-
8/3/2019 Local Anesthetic Pharmacology Lec
1/16
Local Anesthetic Pharmacology
Azza Baraka
Professor of Pharmacology, Faculty of Medicine
Alexandria University
-
8/3/2019 Local Anesthetic Pharmacology Lec
2/16
History
Cocaine was the first topical anesthetic, dating backto 3000
B.C.
By 1900 the addictive properties of cocaine were
wellrecognized.
1905: procaine was developed.
-
8/3/2019 Local Anesthetic Pharmacology Lec
3/16
Definition
A local anesthetic (LA) is an agent thatinterrupts pain impulses
in a specific region
of the body without loss of patient
consciousness.
-
8/3/2019 Local Anesthetic Pharmacology Lec
4/16
Chemical Structure LAs consist of a hydrophobic group (often
an
aromatic ring) connected by an intermediate chain
(containing an ester or amide bond) to an ionizable
group (usually a tertiary amine group).
-
8/3/2019 Local Anesthetic Pharmacology Lec
5/16
Administration Routes
Surface anesthesia: topical gel or spray-applied to skin and
mucous membranes.
Infiltration anesthesia: inject subcutaneous around area for
minor surgery. Nerve endings exposed to the anesthetic
solution are quickly rendered unresponsive. Nerve block
anesthesia: Injection of drug around nerve
trunk proximal to the intended area of anesthesia.
Spinal anesthesia: inject into epidural space, diffuses
across
dura into subarachnoid space. LA solution injected into
thesubarachnoid space blocks conduction of impulses along all
nerves with which it comes in contact, although some
nerves are more easily blocked than others.
-
8/3/2019 Local Anesthetic Pharmacology Lec
6/16
-
8/3/2019 Local Anesthetic Pharmacology Lec
7/16
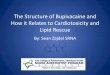
Mechanism of Action
Blocks the sodium channel, from theintracellular side
Must enter the neuron to work Increased lipophilicity is
associated
with increased potency
Increased un-ionized fraction increasespotency
-
8/3/2019 Local Anesthetic Pharmacology Lec
8/16
Site of Action
Local Anesthetic
-
8/3/2019 Local Anesthetic Pharmacology Lec
9/16
Pharmacokinetics
Following injection into the area of nerve fibers to be
blocked, LAs are absorbed into the blood.
Ester-linked LAs are quickly hydrolyzed by cholinesterase
in the blood.
Amide-linked LAs are hydrolyzed by liver microsomal
enzymes. Thus, their half life is significantly longer.
Absorption of LAs is affected by the following factors:
dosage, site of injection, drug-tissue binding, and presence
of vasoconstricting drugs. Presence of vasoconstrictingdrugs
significantly reduces absorption of LAs, thus
enhancing the local drug concentration, prolonging the LA
effect, and reducing blood levels.
-
8/3/2019 Local Anesthetic Pharmacology Lec
10/16
Factors affecting onset, intensity, and
duration of neural blockade
Lipid solubility: a lipophilic LA is more potent and have a
faster
onset of action because it is easier to cross nerve membranes.
Protein binding:LAs with a higher degree of protein binding have
a
prolonged duration of action.
The pKa: The pKa is the pH at which 50% of the LA is in the
ionized
form and 50% is in the unionized form. All LAs are weak bases
withpKa = 8-9:
Thus LAs at physiologic pH will be associated with a greater
fraction of
the molecules existing in the unionized form more
penetration
across nerve membranes faster onset. Local infection (acidosis)
decreases tissue pH , and thus increases the
ionized drug fraction which means less drug will be available
to
penetrate across membranes slower onset.
Dose: Increasing dose of the LA will increase the duration of
theblock.
-
8/3/2019 Local Anesthetic Pharmacology Lec
11/16
Differential sensitivity of nerve fibers to LAs
Fiber diameter: LAs preferentially block small nerve
fibers.Small C fibers (pain signal) are blocked before larger
fibers
(touch, and motor signals)
Myelination: For the same diameter, myelinated nerves will
be
blocked before unmyelinated nerves. Why preganglionic nerves are
blocked before the smaller
unmyelinated C fibers (pain nerves) in spinal anesthesia.
Use-dependent block: Nerves with higher firing frequency are
more sensitive to LA block. This is because LA molecules aremore
likely to access to the binding sites in the open Na+
channel. Pain fibers, have a high firing rate than motor
fibers,
and thus are more sensitive to lower concentrations of LAs.
-
8/3/2019 Local Anesthetic Pharmacology Lec
12/16
Nerve Sensitivity
1. Autonomic
2. Pain
3. Temperature
4. Touch
5. Motor
-
8/3/2019 Local Anesthetic Pharmacology Lec
13/16
Side effects [1] Local:
Irritation and inflammation at the site of administration. LAs
produce vasodilatation but local ischaemia may arise
from a co-administered vasoconstrictor, therefore this
should be avoided in the extremities such as the digits.
Cocaine differs from the other LAs: it blocks norepinephrine
reuptake, resulting in vasoconstriction .Cocaine is
restricted
to topical use in otolaryngeal procedures, to produce
vasoconstriction and reduce mucosal bleeding.
-
8/3/2019 Local Anesthetic Pharmacology Lec
14/16
[2] Systemic:
Toxicity of LAs is mostly related to their inhibitory
effects
on excitable cells such as neurons & cardiac muscle.
CNS: Following absorption, LAs cause stimulation of theCNS,
producing restlessness and tremors that may proceed
to convulsion. Stimulation is caused by inhibition of
inhibitory neuronal activity. At high blood concentrations,
LAs cause depression and even respiratory failure.
CVS: Decrease conduction rate, and force of contraction in
the myocardium. Bupivacaine is more cardiotoxic than
other LAs and may cause cardiovascular collapse andventricular
tachycardia.
Allergic reactions: Ester-linked LAs may cause allergic
reaction in a small population of patients related to their
metabolism to PABA.
-
8/3/2019 Local Anesthetic Pharmacology Lec
15/16
Toxicity of LAs could be prevented by
observing three precautions1. Administer the smallest dose that
will provide
effective anesthesia.
2. Use proper injection technique.
3. Use of a vasoconstrictor containing solution.
-
8/3/2019 Local Anesthetic Pharmacology Lec
16/16
Classification and main differences
between local anestheticsAmidesEsters
Have an amide (-NHCO-) link between
the aromatic group and the amino
terminal.
Have an ester (-COO- ) link
between the aromatic group and the
amino terminal.
Chemistry
Lidocaine: has fast onset
Bupivacaine: dissociate slowly
from cardiac Na+ Channels
risk ofcardiotoxicity.
Procaine: short acting
Tetracaine: long acting
Examples
Few hoursFew minutest1/2
By the liver.By plasma pseudocholinestrase.P-aminobenzoic acid
is a metabolite
Metabolism
RareMoreIncidence ofallergic
reactions




















![[Robert k. Stoelting] Handbook of Pharmacology and Physiology in Anesthetic Practise](https://img.pdfslide.us/doc/110x75/55cf9bb8550346d033a72290/robert-k-stoelting-handbook-of-pharmacology-and-physiology-in-anesthetic.jpg)






