-
Loa loa infection in a patient with thymoma
Pierre Landrya,*, Cecile Bassib, Brigitte Christenc
aLausanne University Medical Policlinic, Lausanne,
SwitzerlandbHopital des Cadolles in Neuchatel, Neuchatel,
SwitzerlandcInstitut Neuchatelois dAnatomie Pathologique,
Neuchatel, Switzerland
Received 24 November 2003; received in revised form 16 February
2004; accepted 17 February 2004
Available online 20 April 2004
KEYWORDSLoa loa infection;
Thymoma
Summary An exceptional observation of a Loa loa infection
occurring in a short termtraveller with a thymoma is described in
details. We discuss the implications of theimmunodeficiency induced
by a thymoma on a concomitant parasitic infection.q 2004 Elsevier
Ltd. All rights reserved.
Case report
A 73-year-old Caucasian woman with no relevantprevious medical
history spent 12 days in SouthernCameroon in May 2000 and five
months laterdeveloped migrating oedema first of a calf andthen of
wrists and forearms, painless and non-itching. No diagnosis was
made and the lesionsdisappeared spontaneously. In March 2002,
shecomplained of difficulties swallowing and oesopha-gal
candidiasis diagnosed by gastroscopy wassuccessfully treated by
seven days of fluconazole.
Three months later, following the appearance ofshortness of
breath and 10 kg weight loss, sheconsulted again. A chest X-ray
showed an extensiveright pleural effusion which was confirmed by
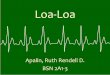
CTscan, with the presence of an anterior mediastinalmass of 8 5
cm2, but no lymph node enlargementsuspect of malignancy (Fig. 1).
Thoracentesis wasperformed and numerous sheathed
microfilaria,diagnosed as Loa loa were found in the pleural
effusion, which contained 70% lymphocytes, 10%granulocytes, 10%
macrophages and 10% mesothe-lial cells. There were no cancerous
cells and noMycobacterium tuberculosis bacilli, neither ondirect
smear nor after culture. Cultures for otherbacteria remained
sterile too. The peripheral bloodeosinophilia was increased (910
cell/mm3 (13%))and the blood contained 2500 microfilaria/ml(midday
blood sample). Serology for filaria waspositive but negative for
strongyloidosis, schistoso-miasis, and HIV. Stool examination
showedTrichuris trichiuria eggs. A needle biopsy of themediastinal
mass revealed a T cell predominantinflammation tissue containing
many microfilaria(Fig. 2), and excluded lymphoma.
A review of the literature on hypereosinophilia,pleural effusion
and mediastinal mass led to thepossible diagnosis of a reactive
tumor to filarialinfection. Therefore, immediate thoracotomy
waspostponed and, after exclusion of oncocerciasis(negative skin
snips), treatment with diethylcarba-mazine (DEC) was initiated
under corticosteroidscover in hospital. The patient received in
stepwisefashion up to 1 mg/kg of DEC for 21 days with noside
effect. The eosinophil count returned tonormal value, and the
microfilaria disappearedfrom blood one week after the start of DEC.
Her
1477-8939/$ - see front matter q 2004 Elsevier Ltd. All rights
reserved.doi:10.1016/j.tmaid.2004.02.009
Travel Medicine and Infectious Disease (2004) 2, 8587
www.elsevierhealth.com/journals/tmid
*Corresponding author. Address: Place Pury 9, 2000Neuchatel,
Switzerland. Tel.: 41-32-724-5533; fax: 41-32-724-5534.
E-mail address: [email protected]
-
general health status improved, she regained 5 kgand resumed her
normal activities.
Unfortunately 2 months later the pleural effusionincreased again
and a new CT scan confirmed thestill present mediastinal mass. A
sternotomy andresection of the tumor were performed.
Histologyconfirmed a type B1 (or predominant cortical)invasive
thymoma infiltrating the pericardium andthe right lung (CD3
reaction for T cells and CD99reaction for thymus T cells were
strongly positive,whereas CD20 for B cells was scarcely
positive).No parasite was found in the tumor and in theperipheral
blood, but a few live microfilaria wereseen in the still present
pleural effusion. A secondtreatment against Loa loa infection was
initiated,
this time with albendazole 2 200 mg/day for 21days at the end of
which the eosinophil countreached 660 cell/mm3. At that stage the
patienthad lost some weight again, but was still
active.Immunological analysis showed no hypogammaglo-bulinemia
(gammaglobulins 8.8 g/l (6.013.0)), butmild lymphocytopenia (1105
cells/mm3) affectingT lymphocytes mainly (764 (69.1%) CD3 T
cells/mm3
(13502350), 598 CD4 T cells/mm3 (8251575)and 168 CD8 T cells/mm3
(4751025), 341 (30.9%)B cells/mm3. The CD4/CD8 ratio was not
invertedbut increased to 3.6.
At more than 14 months of follow-up, the patientis well, her CT
scan shows no residual pleuraleffusion, and no sign of recurrence
of the tumor.Her white blood cell count is normal, but the
totallymphocyte count is gone down to 815 cells/mm3
(550 CD3 T cells/mm3, 436 CD4 cells/mm3 and 111CD8 cells/mm3),
with immunoglobulins in thenormal range (IgA 1.45 g/l (0.74.0), IgG
9.00 g/l(7.016.0), IgM 0.9 g/l (0.4012.3).
Discussion
Thymoma are intrathoracic tumors of variableepithelial and
lymphoid content. About 44% ofthem are linked to myasthenia gravis,
21% tovarious levels of cytopenia, 6% to hypogammaglo-bulinemia,
and some cases to various autoimmunedisorders. A thymoma related
immunodeficiencysyndrome (Good syndrome) has been
describedcombining low or absent B cells in the peripheralblood,
hypogammaglobulinemia and variablydemonstrable cell-mediated
immunity defect,especially reduced CD4 T cells.1 On the otherhand,
a common variable immunodeficiency syn-drome (CVID) combines
variable antibodydeficiency and some cellular immune defects, butno
reduced levels of B cells.1 Various infectionsrelated to the
immunodepression associated withthymoma have been described, upper
respiratoryinfections2 being the commonest, but also oeso-phagal
candidiasis and a variety of viral (CMV,herpes) infections. But
data on parasitic disease arescarce with a few cases of
strongyloidosis,3 tox-oplasmosis4 and Pneumocystis carinii
infections.1
Except for an accidental infection by dirofilaria, nocase of
filarial infection has been published inpatients with
immunodeficiency or Good syndrome.
Loasis is a parasitic disease acquired in CentralWest Africa
only, usually in people with a normalimmune status. Following the
bite of a tabanid fly ofthe genus Chrisops, the infective larvae
burrow inthe skin where they develop into adults moving
Figure 1 Thoracic CT scan showing a mediastinal mass.A: aorta;
H: heart; PA: pulmonary atelectasia; PE: pleuraleffusion; T:
thymoma.
Figure 2 Loa microfilaria in the biopsy of the mass.
P. Landry et al.86
-
in the connective tissues and producing numerousmicrofilaria
found in the blood. Clinical featuresare migrating subcutaneous
swellings (Calabaroedema) most commonly on the wrists and
ankles,lasting from a few hours to a few days, sometimeswith
pruritus and arthralgia. The adult filarial canoccasionally be seen
passing under the skin or theconjunctiva, rarely resulting in
serious compli-cations when invading the central nervous system,or
other organs. In expatriates hypereosinophilia iscommon.
In this case, the initial presentation, e.g. apleural effusion
with loasis and an intrathoracicmass suggested a reactive tumor due
to the possiblepresence of an adult parasite in the thorax.
Twocases of filarial infection causing a mediastinal masshave been
reported, one over 50 years ago, with Loaloa5 and a more recently
one due to Wucherariabancrofti.6 Both resolved after
antiparasitictherapy. Some cases of pleural effusion or pulmon-ary
infiltrates with high contents in eosinophils havebeen associated
to loasis.7 In the case we describeeosinophil counts in the pleural
effusion and in thebiopsy of the mediastinal mass were not
increased.At the time of surgical removal of the type B1thymoma,
the Loa loa infection was still present,although less intense,
despite a three weeks courseof DEC. It is known that T Helper cells
responsive-ness play an important role in the clearanceof
parasites.8,9 Thus this relative failure of treat-ment could be
related to some degree ofimmunodeficiency.
There was no immunoglobulin deficiency and
nohypogammaglobulinemia, but T lymphocytopenia,affecting both the
CD4 and CD8 subsets, whichremained after removal of the tumor.
Theseabnormalities do not qualify for CVID or for Goodsyndrome, but
the patient clearly has immunode-ficiency. The decrease in T
lymphocytes a year or soafter the tumorectomy, although without
symp-toms, is consistent with published data of thepersistence of
immunological abnormalities evenafter removal of the tumor.1
Looking for opportu-nistic infections as in Good syndrome or CVID
ismandatory. Noteworthy is a published case ofsevere
strongyloidosis and thymoma with no
hypogammaglobulinemia either.3 Organ involve-ment of loasis is
well known, especially in kidney,heart, brain and lungs, but of
interest, we found noreference to unusual manifestations of
loasisrelated to HIV infection, although both diseasesare frequent
in Central Africa. Rare studies haveanalyzed the effect of steroids
in the clinical aspectof this infection.10
In summary, thymoma are tumors which aresometimes related to
some degree of immunodefi-ciency, leading to complicated infections
includingparasitic ones. We described the possible first caseof
thymoma and loasis, in a short-term traveler.
References
1. Tarr PE, Sneller MC, Mechanic LJ, et al. Infections in
patientswith immunodeficiency with thymoma (Good syndrome).Report
of 5 cases and review of the literature.
Medicine2001;80:123133.
2. Granel B, Gayet S, Christides C, et al. Thymoma
andhypogammaglobulinemia. Goods syndrome: a propos of acase and
review of the literature. Rev Med Interne 1999;20:347349.
3. Godoy P, Camargos Campos ChM, Costa G, et al. Associationof
thymoma and severe intestinal strongyloidiasis. Rev SocBras Med
Trop 1998;31(5):481485.
4. Shaikh BS, Schwab IR, Morse LS. Association of
oculartoxoplasmosis and thymoma. Retina 1997;17(4):354356.
5. Madell SH, Spingam CL. Unusual thoracic manifestations
infilariasis due to Loa loa. Am J Med 1953;15:272280.
6. Gilbert H, Hartman BJ. Short report: a case of
fibrosingmediastinitis caused by Wucheraria bancrofti. Am J TropMed
Hyg 1996;54(6):596599.
7. Boornazian JS, Fagan MJ. Tropical pulmonary
eosinophiliaassociated with pleural effusions. Am J Trop Med Hyg
1985;34(3):473475.
8. Baize S, Wahl G, Soboslay PT, et al. T helper
responsivenessin human Loa loa infection; defective specific
proliferationand cytokine production by CD4 T cells from
microfilar-aemic subjects compared with amicrofilaraemic. Clin
ExpImmunol 1997;108:272278.
9. Ungeheuer M, Elissa N, Morelli A, et al. Celullar responses
toLoa loa experimental infection in mandrills (Mandrillussphinx)
vaccinated with irradiated infective larvae. ParasiteImmunol
2000;22:173183.
10. Wanji S, Tendongfor N, Vuong PN, et al. The migration
andlocalization of Loa loa infective and fourth stage larvae
innormal and immunosuppressed rodents. Ann Trop MedParasitol
2002;96:823830.
Loa loa infection in a patient with thymoma 87
Loa loa infection in a patient with thymomaCase
reportDiscussionReferences

![Parathyroid Adenoma/Thymoma Case Reportadenoma and thymoma without mention of sestamibi uptake by the thymoma (whether such imaging was performed or not). Byrne et al. [13] demonstrated](https://img.pdfslide.us/doc/110x75/5e2f040ac0577556e1278f0b/parathyroid-adenomathymoma-case-adenoma-and-thymoma-without-mention-of-sestamibi.jpg)