Embed Size (px)
Citation preview
Health Economics: Utilizing Advanced Care Wound Products for Clinical and Cost Effectiveness
Important Pieces of the Research Puzzle Professor Keith Harding
A Retrospective Analysis of the Cost-effectiveness of a Collagen/Oxidized Regenerated Cellulose Dressing in the Treatment of Neuropathic Diabetic Foot UlcersJosé Luis Lázaro-Martínez, PhD; Francisco Javier Aragón-Sánchez, MD, PhD; Esther García-Morales, PhD; Juan Vicente Beneit-Montesinos, MD, PhD; and Máximo González-Jurado, PhD
A Retrospective Study of Sequential Therapy with Advanced Wound Care Products versus Saline Gauze Dressings: Comparing Healing and CostRobert J. Snyder, DPM, CWS; Deborah Richter, RN, CWCA; and Mary Ellen Hill, PT
November 2010, Vol. 56, Issue 11ALLC,
OWMO S T O M Y W O U N D M A N A G E M E N TFROM SCIENCE TO PRACTICE: CONTEMPORARY APPROACHES TO SKIN, WOUND, OSTOMY, AND INCONTINENCE CARE
www.o-wm.com
™
™
SUPPLEMENT TO
This ancillary publication is provided as a courtesy to Ostomy Wound Management readers through a grant from Systagenix Wound Care. This publication was not subject to the Ostomy Wound Management peer-review process.
01_Cover1:Cover1 11/4/10 9:36 AM Page 1

2 OSTOMY WOUND MANAGEMENT NOVEMBER 2010 SUPPLEMENT A
CONTENTSVolume 56, Number 11A, November 2010
Featurespage 3 Important Pieces of the Research Puzzle Professor Keith Harding
page 4 A Retrospective Analysis of the Cost-effectiveness of a Collagen/Oxidized Regenerated Cellulose Dressing in the Treatment of Neuropathic Diabetic Foot Ulcers José Luis Lázaro-Martínez, PhD; Francisco Javier Aragón-Sánchez, MD,PhD; Esther García-Morales, PhD; Juan Vicente Beneit-Montesinos,MD, PhD; and Máximo González-Jurado, PhD
page 9 A Retrospective Study of Sequential Therapy with AdvancedWound Care Products versus Saline Gauze Dressings: Comparing Healing and Cost Robert J. Snyder, DPM, CWS; Deborah Richter, RN, CWCA; and Mary Ellen Hill, PT
EDITORIAL STAFFCLINICAL EDITOR Lia van Rijswijk, RN, MSN,CWCNEDITOR Barbara C. ZeigerASSOCIATE EDITOR Chimere G. HolmesEDITORIAL ASSISTANT Caitlin QuarlesSPECIAL PROJECTS EDITOR Stephanie Wasek
BUSINESS STAFFEXECUTIVE VICE PRESIDENT Peter Norris
VICE PRESIDENT/PUBLISHER Jeremy [email protected]
NATIONAL SALES MANAGER Kristen [email protected]
SALES ASSOCIATES Sydney J. [email protected]
Kelly [email protected]
CIRCULATION MANAGER Bonnie Shannon
HMP COMMUNICATIONS, LLCPRESIDENT Bill NortonCONTROLLER Meredith Cymbor-JonesVICE PRESIDENT SPECIAL PROJECTS Jeff HallCREATIVE DIRECTOR Vic GeanopulosPRODUCTION MANAGER Elizabeth McTamneyPRODUCTION/CIRCULATION DIRECTOR Kathy MurphyAUDIENCE DEVELOPMENT MANAGER Bill MalriatMEETING PLANNER Tracy Blithe, CMPMEETING PLANNER Mary Beth PollartMANAGER OF WEB DEVELOPMENT Tim Shaw
HMP COMMUNICATIONS HOLDINGS, LLCPRESIDENT and CHIEF EXECUTIVE OFFICER Jeff HennessyCHIEF FINANCIAL OFFICER Daniel M. RiceVICE PRESIDENT OF HUMAN RESOURCES Anthony ManciniDIRECTOR OF INFORMATION SYSTEMS David Kang
83 General Warren BoulevardSuite 100 Malvern, PA 19355 (800) 237-7285
Ostomy Wound Management (ISSN 0889-5899) is published monthly byHMP Communications, 83 General Warren Boulevard, Suite 100,Malvern, PA 19355; phone: (800) 237-7285;e-mail: [email protected].
Postmaster: Send address changes to Ostomy Wound Management, 83 General Warren Boulevard.; Suite 100; Malvern, PA 19355 Periodicals postage paid at Malvern, PA and at additional mailing offices.
Change of Address: For change of address, mail your old and new address to:HMP Communications; OWM Subscriptions83 General Warren Boulevard, Suite 100; Malvern, PA 19355or fax to OWM Subscriptions at: (610) 560-0502
Subscriptions: U.S. $75.00 for one year. International $115.00Single or replacement copies: U.S. $14.50; International $17.50Call 1-800-237-7285, ext 5 for the Subscription Dept.or E-mail: [email protected].(Mail subscription requests to the address above)
HMP Communications LLC (HMP) is the authoritative source for compre-hensive information and education servicing healthcare professionals.HMP’s products include peer-reviewed and non-peer-reviewed medicaljournals, national tradeshows and conferences, online programs and cus-tomized clinical programs. HMP is a wholly owned subsidiary of HMPCommunications Holdings LLC. Discover more about HMP’s productsand services at: www.hmpcommunications.com.
© 2010, HMP Communications, LLC, (HMP). All rights reserved. Reproductionin whole or in part prohibited. Opinions expressed by authors, contributors, andadvertisers are their own and not necessarily those of HMP Communications,the editorial staff, or any member of the editorial advisory board. HMP Commu-nications is not r esponsible for accuracy of dosages given in articles printedherein. The appearance of advertisements in this jour nal is not a warranty, en-dorsement or approval of the products or services advertised or of their ef fec-tiveness, quality or safety. HMP Communications disclaims r esponsibility forany injury to persons or property resulting from any ideas or products referredto in the articles or advertisements. Content may not be reproduced in any formwithout written permission. Rights, Permission, Reprint and T ranslation infor-mation is available at www.hmpcommunications.com.
LLC , TM
OWMO S T O M Y W O U N D M A N A G E M E N T
™
02_TOC:TOC 11/4/10 9:37 AM Page 2

NOVEMBER 2010 SUPPLEMENT A OSTOMY WOUND MANAGEMENT 3www.o-wm.com
INTRODUCTION
Wounds and wound healing are complex and challeng-ing for healthcare systems. In recent years, there has
been an e ver-increasing clamor for mor e research to provethat new treatments and systems of care make a difference.At the same time, awareness is growing regarding the diffi-culties associated with undertaking clinical research in thisarea — both in terms of obtaining funding and in the designof research studies. The current state of affairs can be sum-marized by stating that no one sing le piece of research isgoing to provide all of the e vidence required to appreciatewhat is best for patients w ith a par ticular problem but allstructured assessments of intervention add to our under-standing of how to improve patient care.
The two articles in this publication contain new and novelinformation. Lazaro-Martinez et al examine different dress-ing regimens and their impact on healing in a population ofpatients with diabetic foot disease. Treatment including ox-idized regenerated cellulose and collagen appears to make apositive difference. Although this study is not of sufficientsize to prove a statistical sig nificance, the t reatment showspromise. In addition, the authors discuss a number of otheroutcome measures, including effec tiveness and cost-effec-tiveness, which may be as or even more important measures
of success than complete healing. Recognition of the valueof multiple potential outcome measures on patients, care-givers, and healthcare systems is long overdue and merits fur-ther thought and discussion.
Snyder et al performed a retrospective review of morethan 1,000 charts of patients treated with either the cellu-lose-collagen pr oduct or saline-soak ed gauz e. After 2months of treatment, a dramatic difference in healing andcost between the two groups of patients was not ed. Thisstudy is intriguing for both the c oncept of the sequentialuse of wound treatments and the abilit y to demonstratesubstantial cost savings.
Both studies undersc ore the issues clinicians and r e-searchers must consider in understanding ho w to collectinformation, how to consider the use of products in clini-cal practice, and how to measure benefits of using partic-ular treatment regimens. These studies are not intended toprovide all of the answ ers that wound care professionalsneed to improve their pr actice but the y demonstrate theneed for and value of a broad base of approaches to eval-uation that individually provide a small piece of the grad-ually forming complex picture that shows new treatmentsmay convey many benefits. ■
Professor Keith Harding is currenty a Professor of Rehabilitation Medicine (W ound Healing) and the Director of the W ound Healing Research Unit at theUniversity of Wales, College of Medicine.
Important Pieces of the Research PuzzleProfessor Keith Harding
03_Intro:Layout 1 11/5/10 12:04 PM Page 3
4 OSTOMY WOUND MANAGEMENT NOVEMBER 2010 SUPPLEMENT A www.o-wm.com
Increases in life expectancy and the g rowing prevalence ofchronic illnesses such as diabetes mellitus are leading to in-
creased healthcare costs.1 Chronic wound and ulcer treat-ment is one of the major social and medical challenges of the21st century. Diabetic foot, a complication of diabetes melli-tus, may lead to ulceration, infection, or gangrene as a resultof a combination of neuropathy, ischemia, and foot defor -mities; it is the pr incipal cause of nontraumatic lower ex-
tremity amputation.2 These complications come with highcosts3: diabetic foot ulceration (DFU) and amputations wereestimated t o c ost US healthcar e pa yors $10.9 billion in2001.4,5 According to corresponding UK estimates based onthe same methodology, 5% of total national health ser viceexpenditures in 2001 (£3 billion) w ere attributable to dia-betes. The total annual cost of diabetes-related foot compli-cations was estimated to be £252 million.6
A Retrospective Analysis of the Cost-effectiveness of a Collagen/Oxidized Regenerated Cellulose Dressing in the Treatment of Neuropathic Diabetic Foot Ulcers
José Luis Lázaro-Martínez, PhD; Francisco Javier Aragón-Sánchez, MD, PhD; Esther García-Morales, PhD; Juan Vicente Beneit-Montesinos, MD, PhD; and Máximo González-Jurado, PhD
AbstractCollagen/oxidized regenerated cellulose dressings (C/ORC) have shown evidence of clinical effectiveness in the treatmentof neuropathic diabetic foot ulcers (DFUs). A retrospective study to analyze cost-effectiveness was performed using resultsfrom an ear lier, 6-week randomized clinical tr ial carried out on patients (n = 40) with neuropathic DFU treated with anC/ORC dressing. The patients were randomized to two groups: group 1 (n = 20) was treated with an C/ORC dressing andgroup 2 (n = 20), the control group, received wound care in accordance with the standard protocol in use at the authors’healthcare center. Effectiveness was defined as the percentage of patients whose wounds had healed at the end of thestudy. Total cost of care (including staff, ancillary supplies, dressings, and patient transport costs), the number of patientsneeding to treat (NNT), the mean cost, the incremental cost, and the average cost effectiveness were analyzed. NNT was2.11 (95% CI: 1.34-4.96. P = 0.03). Treatment effectiveness was 63% in group 1 and 16% in g roup 2. Incremental cost-effectiveness was $683.18, the amount needed to avoid nonhealing in the control group. Average cost effectiveness was$561.48 in group 1 versus $2,577.65 in group 2 (total cost/effectiveness in each group). Treating neuropathic ulcers withan C/ORC dressing provides an excellent cost-benefit ratio that saves an average of $2,280.13 per patient over 6 weeksof treatment. This saving may be even greater in longer-ter m treatment programs and among patients with ulcers thatshow little tendency to heal.
Key Words: diabetic foot, cost-effectiveness analysis, metalloproteinase, wound healing
Index: Ostomy Wound Management 2010;56(11A):4–8
Potential Conflicts of Interest: none disclosed
Prof. Lázaro-Martínez is Head of the Diabetic Foot Unit, University Podiatry Clinic of Complutense University of Madrid, Madrid, Spain. Dr. Aragón-Sánchez isHead of the Diabetic Foot Unit, La Paloma Hospital, Las Palmas de Gran Canaria, Spain. Prof. García-Morales is a podiatrist, Di abetic Foot Unit at UniversityPodiatry Clinic of Complutense University of Madrid. Prof. Beneit-Montesinos is a physician, Diabetic Foot Unit, University Pod iatry Clinic of ComplutenseUniversity of Madrid. Prof. González-Jurado is a professor, Podiatry College at Complutense University of Madrid. Please address correspondence to: ProfessorJose Luis Lázaro-Martínez, Edificio Facultad de Medicina. Pabellón I., Avda. Complutense s/n, 28040 Madrid, Spain; email: [email protected].
HEALTH ECONOMICS
04-08_Lazaro-Martinez:Layout 1 11/4/10 9:40 AM Page 4
NOVEMBER 2010 SUPPLEMENT A OSTOMY WOUND MANAGEMENT 5www.o-wm.com
HEALTH ECONOMICS
Few studies delineat e the c osts relevant to DFU t reat-ments. The Eurodiale study7 evaluated treatment costs be-tween September 1, 2003 and October 1, 2004 of 821 patientsin a collaborative network of 14 European diabetic foot cen-ters. According to 2005 pr ices, the direct and indirect costsper patient w ith DFU that heals was $9,985.86, which in-creased to $25,779.26 if the wound did not heal w ithin 12months and to $32,406.52 if any amputation at or proximalto the ankle was required. An important element of the costsassociated with the treatment of diabetic foot is the cost in-curred by local treatments7 — specifically, dressing material,staff who perfor med dressing changes, and t ransportation,which represented approximately 20% of the total cost. Top-ical care with wet/dry gauze and topical antiseptic treatmentshas slowly been replaced with dressings that facilitate woundclosure through physical and biological processes.8,9
In this area, growth factors and collagen/oxidized regen-erated cellulose dressings (C/ORC) have shown evidence ofeffectiveness in the t reatment of neuropathic DFU.10-12 Pre-vious cost-effectiveness studies have demonstrated the ad-vantages of these new treatments. In 2002, Ghatnekar13 useda hypothetical cohort of patients thr ough a M arkov statetransition model to estimate the probability of wounds heal-ing, becoming infected, gangrene developing, an ulcer heal-ing after amputation, and death. The study models the resultsof treatment in France, Germany, Switzerland, and the UK.The main objective of this study was to assess the effective-ness and costs of treating nonsuperficial DFU with C/ORCas part of good wound care, compared with good wound carealone. The r esults indicat ed that using C/OR C sa ved$2,569.70 per patient per year in the treatment of deep DFUcompared to good wound care. Other studies14 analyzed theadvantages of a recombinant platelet-derived growth factor.A 1-year decision-analytic model was de veloped and tested
using data from a previously published controlled clinicalstudy in volving 251 peo ple w ith diabet es (124 becapler -min/127 control) and adequate vasculature presenting withan infection-free ulcer that had failed to heal despite appro-priate therapy. At 20-week follow-up, an average saving of$156 was realized, compared to the use of a placebo, at an in-cremental cost of $6 for each additional day of treatment.
However, little cost-effectiveness evidence is available toguide DFU treatment. This study aims to perform a cost-ef-fectiveness analysis using data from a previously conductedrandomized clinical trial15 using C/ORC and control dress-ings in the management of patients with neuropathic DFU.
Material and MethodsThe cost-effectiveness study was c onducted using data
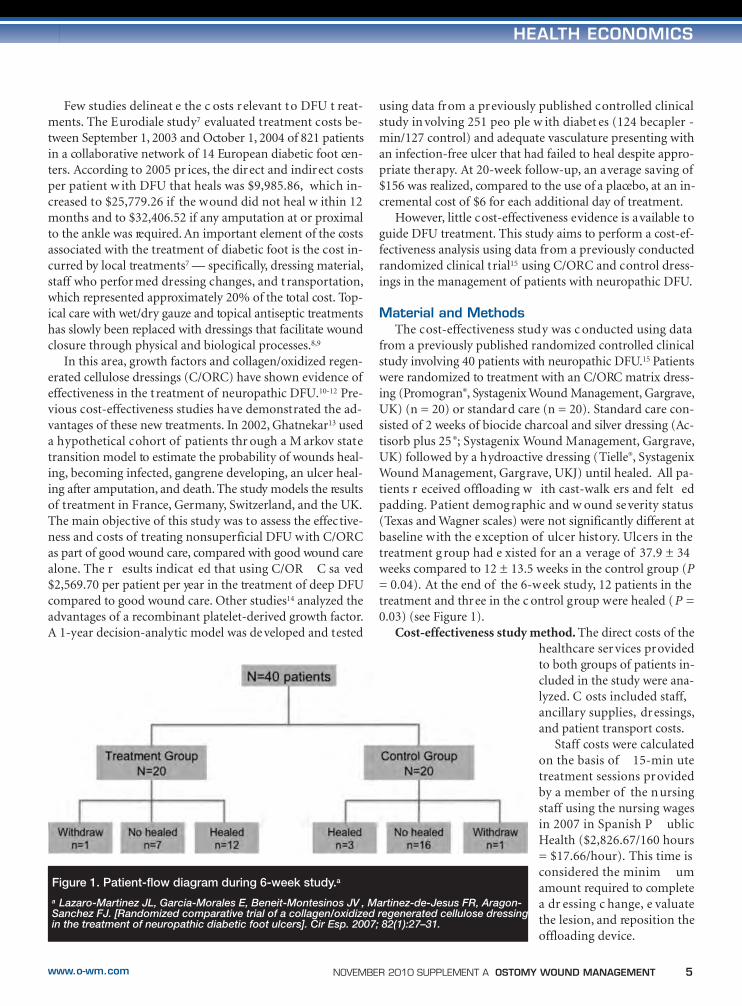
from a previously published randomized controlled clinicalstudy involving 40 patients with neuropathic DFU.15 Patientswere randomized to treatment with an C/ORC matrix dress-ing (Promogran®, Systagenix Wound Management, Gargrave,UK) (n = 20) or standard care (n = 20). Standard care con-sisted of 2 weeks of biocide charcoal and silver dressing (Ac-tisorb plus 25 ®; Systagenix Wound Management, Gargrave,UK) followed by a hydroactive dressing (Tielle®, SystagenixWound Management, Gargrave, UKJ) until healed. All pa-tients r eceived offloading w ith cast-walk ers and felt edpadding. Patient demographic and w ound severity status(Texas and Wagner scales) were not significantly different atbaseline with the e xception of ulcer history. Ulcers in thetreatment g roup had e xisted for an a verage of 37.9 ± 34weeks compared to 12 ± 13.5 weeks in the control group (P= 0.04). At the end of the 6-week study, 12 patients in thetreatment and three in the c ontrol group were healed ( P =0.03) (see Figure 1).
Cost-effectiveness study method. The direct costs of thehealthcare ser vices providedto both groups of patients in-cluded in the study were ana-lyzed. C osts included staff,ancillary supplies, dressings,and patient transport costs.
Staff costs were calculatedon the basis of 15-min utetreatment sessions providedby a member of the nursingstaff using the nursing wagesin 2007 in Spanish P ublicHealth ($2,826.67/160 hours= $17.66/hour). This time isconsidered the minim umamount required to completea dr essing c hange, e valuatethe lesion, and reposition theoffloading device.
Figure 1. Patient-flow diagram during 6-week study.a
a Lazaro-Martinez JL, Garcia-Morales E, Beneit-Montesinos JV , Martinez-de-Jesus FR, Aragon-Sanchez FJ. [Randomized comparative trial of a collagen/oxidized regenerated cellulose dressingin the treatment of neuropathic diabetic foot ulcers]. Cir Esp. 2007; 82(1):27–31.
04-08_Lazaro-Martinez:Layout 1 11/4/10 9:40 AM Page 5
6 OSTOMY WOUND MANAGEMENT NOVEMBER 2010 SUPPLEMENT A www.o-wm.com
HEALTH ECONOMICS
The cost of ancillary supplies included everything requiredfor the patient’s t reatment session according to 2007 pr ices(gloves, tape, antiseptic sol ution, saline sol ution, surg icaldrapes, felted padding, and the like), as well as the cost of thebiocide charcoal dressing with silver (Actisorb plus 25®; Systa-genix Wound Management, Gargrave, UK), the hydroactivedressing (Tielle®, Systagenix Wound Management, Gargrave,UK) in the c ontrol, and the C/OR C matrix dressing in thetreatment group (see Table 1). Most patients were referred bytheir primary healthcare provider, which provided ambulancetransport at a cost of $76.44 as per 2007 Public Health Admin-istrator agreement prices.
Costs were calculated per visit, per week (three visits), andfor the 6-w eek duration of the stud y, regardless of actuallength of treatment. Indirect costs relating to items such as
equipment, inst ruments,fixtures, and appar atuswere not incl uded. Theanalysis also did not in-clude the cost of temporaryoffloading devices such aspostoperative shoes or r e-movable offloading boots.
Of the var ious types ofhealthcare economic analy-sis available, cost-effective-ness was c onsidered mostappropriate because it ismost r elevant t o themicro-economic le vel ofhealthcare management.Its main advantage lies inthe possibility of express-ing effects in the sameunits used in clinical trialsand in daily clinical pr ac-tice.16 Cost-effectivenessmeasures used included
the number of patients needed to treat (NNT), ef-fectiveness, average cost effectiveness, and incre-mental c ost per patient. NNT is anepidemiological measure used in assessing the ef-fectiveness of a healthcare intervention, typicallya treatment with medication.17 The NNT is thenumber of patients who need t o be t reated inorder to prevent one additional bad outcome. AnNNT of 1 means everyone in the treatment groupand nobody in the c ontrol group improves. Thehigher the NNT, the less effec tive the e valuatedtreatment. In this study, effectiveness was definedas the pr oportion of patients whose w oundshealed. Healing was defined as c omplete epithe-lialization of the ulcer.
Data analysis. Average cost effectiveness was calculatedby di viding c ost b y effec tiveness (pr oportion of patientshealed). Incremental cost per patient was determined by cal-culating the difference between cost treatment per patient inthe control and t reatment groups. Average were comparedusing the Student’s t test for independent samples (SPSS ver-sion 15.0 for Windows, SPSS, Chicago, IL). NNT and likeli-hoods w ere calculat ed using the E pi I nfo™ version 3.5.1program (Cent ers for Disease C ontrol and P revention,Dekalb, Georgia).
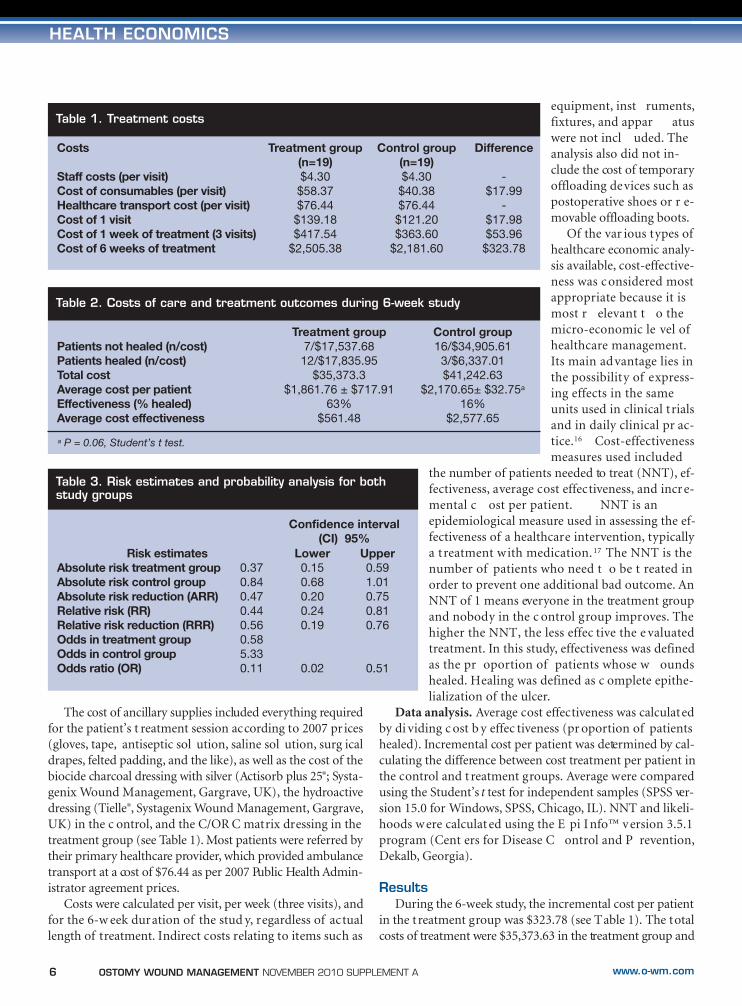
ResultsDuring the 6-week study, the incremental cost per patient
in the t reatment group was $323.78 (see Table 1). The totalcosts of treatment were $35,373.63 in the treatment group and
Table 1. Treatment costs
Costs
Staff costs (per visit)Cost of consumables (per visit)Healthcare transport cost (per visit)Cost of 1 visit Cost of 1 week of treatment (3 visits)Cost of 6 weeks of treatment
Treatment group (n=19)$4.30
$58.37$76.44
$139.18$417.54
$2,505.38
Control group(n=19)$4.30
$40.38$76.44
$121.20$363.60
$2,181.60
Difference
-$17.99
-$17.98$53.96
$323.78
Table 2. Costs of care and treatment outcomes during 6-week study
Patients not healed (n/cost)Patients healed (n/cost)Total costAverage cost per patient Effectiveness (% healed)Average cost effectiveness
Treatment group7/$17,537.68
12/$17,835.95$35,373.3
$1,861.76 ± $717.9163%
$561.48
Control group16/$34,905.613/$6,337.01$41,242.63
$2,170.65± $32.75a
16%$2,577.65
a P = 0.06, Student’s t test.
Table 3. Risk estimates and probability analysis for bothstudy groups
Lower0.150.680.200.240.19
0.02
Upper0.591.010.750.810.76
0.51
0.370.840.470.440.560.585.330.11
Risk estimatesAbsolute risk treatment groupAbsolute risk control groupAbsolute risk reduction (ARR)Relative risk (RR)Relative risk reduction (RRR)Odds in treatment group Odds in control group Odds ratio (OR)
Confidence interval(CI) 95%
04-08_Lazaro-Martinez:Layout 1 11/4/10 9:40 AM Page 6

NOVEMBER 2010 SUPPLEMENT A OSTOMY WOUND MANAGEMENT 7www.o-wm.com
HEALTH ECONOMICS
$41,242.63 in the control group (see Table 2). For both treat-ment groups combined, the average cost of treatment for pa-tients whose ulcers healed compared with those whose ulcersdid not heal was $1,611.52 ± $634.35 (n = 15) versus $2,280.13± $152.31 (n = 23) (P <0.001). The average cost per patient inthe treatment group was lower than the average cost per pa-tient in the c ontrol g roup ($1,861.76 ± $717.91 v ersus$2,170.65 + 32.75, P = 0.06) because the ulc ers healed fasterand in higher proportion in treatment group (see Table 2).
The average cost effectiveness in the treatment group was$561.48 compared to $2,577.65 in the control group. The like-lihood ratio of healing ac cording to the t reatment used isshown in Table 3. Using the treatment protocol reduced therisk of wound healing failure by 47%, and the relative risk re-duction using the treatment protocol was 0.56; thus, the prob-ability of no healing taking place was 5.3 times greater in thecontrol group than in the treatment groups (see Table 3).
NNT was 2.11 (95% CI: 1.34-4.96, P = 0.03), indicatingit would be necessary to manage two patients using the treat-ment protocol in order to avoid one case of nonhealing usingthe control treatment protocol. Based on the NNT value andcompared to the control group, the calculated incrementaleffectiveness c ost per patient was $683.18, the amountneeded to avoid nonhealing in the control group.
DiscussionUsing data from the previously published study, the re-
sults regarding both NNT and the average cost effectivenesssuggest that the c ost benefit r atio of treating neuropathicDFU with an C/ORC matrix dressing instead of a standardprotocol of care is excellent. In this study, the average cost ef-fectiveness associat ed w ith the t reatment pr otocol is$2,016,17 less than when conventional dressings are used. Aninvestment of $683.18 r esulted in an a verage sa ving of$1,596.95 per patient (average cost for patients with no heal-ing [incremental effectiveness cost]). The Eurodiale study,7
which calculat ed w ound t reatment c osts depending onwhether w ounds ar e c omplicated b y infection and/or is-chemia and established an increment linked to the individualor combined presence of these complications, reported thecost of treating a neuropathic ulcer as $5,799.82. In the cur-rent study, using direct costs only, the total cost were lower($2,505.38 in the t reatment and $2,181.60 in the c ontrolgroup). However, these dir ect costs were hig her than the$4,72,82 cited for total direct and other costs (antibiotics, of-floading devices, and hospitalization) in the Eurodiale study,suggesting that nonspecialized treatment was used in the ear-lier research. The cost of healthcare-related transport was in-cluded in this analysis because many patients with DFU havelimited mobility and require transportation. Transportationcosts are high and directly related to the number of visits tothe health center the patient requires before complete healingtakes place.
Independent of the cost-effectiveness ratio, the cost of thetreatment group protocol was lower than that of the controlgroup ($35,373.63 vs. $41,242.63), with a g ross saving of$5,868.99, for 38 patients during 6 weeks of treatment.
The probability of healing , as r eported in the or iginalstudy, was 63% in the t reatment and 16% in the c ontrolgroup during the 6 weeks of treatment even though woundsin the treatment group had existed for an average of 37.9 ±34 weeks before study enrollment. These results are bettercompared with literature relationship with C/ORC dress-ings10,11 but in the current study the length of the monitoringwas 6 weeks. The duration of the period of treatment couldhave affected the cost results because in the majority of sim-ilar studies the treatment period was longer.
LimitationsResults of the Ghatnekar’s study13 indicated that using
C/ORC saved $2,569.70 per patient per y ear in the t reat-ment of deep DFU compared to good wound care. Currentstudy results show these savings may be higher but studycomparisons are limited by the two different cost calcula-tion methods used. However, the pr inciple limitation ofthis study is that the results can be compared only to stud-ies using the same cost-effectiveness model and a differenttopical treatment option. Also, patients in this study wereseen in a referral center for diabetic foot treatment, wherepatients are managed using an integrated treatment model,with offloading of the ulcer a key element in neuropathicwound treatment. This could have affected the results. Forexample, it has been shown that offloading procedures arenot always implemented in the treatment of these patients.A prospective study18 involving 1,232 patients w ith DFUshowed that 77% of patients were not using offloading de-vices or w ere using an inappr opriate method of pressureredistribution.
It is extremely important to bear in mind that the effec-tiveness of this t reatment depends on c orrect use of dress-ings, correct offloading of the ulcer, and correct diagnosis ofany potential complications involved (ischemia and/or in-fection).15,19 The incremental cost per day of treatment was$7.70, similar to the amount reported from a 2003 study bySibbald14 of daily applications of recombinant platelet de-rived growth factor.
The lack of cost-effectiveness studies analyzing new treat-ments for DFU means that purchasing decisions relating todressings for localized treatment are occasionally based onlyon the incremental cost of the treatments. The current studyresults indicate that investment in effective localized treat-ments may reduce the cost of treatment. Additional studies,using larger sample siz es, c omparing differ ent t reatmentmodalities, and including other var iables such as indir ectcosts will provide much-needed knowledge in the field ofcost-effectiveness for DFU treatment.
04-08_Lazaro-Martinez:Layout 1 11/4/10 9:40 AM Page 7

8 OSTOMY WOUND MANAGEMENT NOVEMBER 2010 SUPPLEMENT A www.o-wm.com
HEALTH ECONOMICS
ConclusionA retrospective cost-effectiveness study demonstrates that
use of an effective wound dressing has the potential to reducethe cost of treatment and, compared to standard of care alone,to save patients and payors substantially on care costs. In orderto increase knowledge in the field of cost-effectiveness for DFUtreatment, additional studies with larger samples and compar-ing different alternative treatments are needed. ■
References1. Queen D, Orsted H, Sanada H, Sussman G. A dr essing history. Int
Wound J. 2004;1(1):59–77.2. Apelqvist J, Bakker K, van Houtum WH, Schaper NC. The develop-
ment of global consensus guidelines on the management of the dia-betic foot. Diabetes Metab Res Rev. 2008;24(suppl 1):S116–S118.
3. Albert S. Cost-ef fective management of r ecalcitrant diabetic foot ul-cers. Clin Podiatr Med Surg. 2002;19(4):483–491.
4. Gordois A, Scuffham P, Shearer A, Oglesby A, Tobian JA. The healthcare costs of diabetic peripheral neuropathy in the US. Diabetes Care.2003;26(6):1790–1795.
5. Shearer A, Scuf fham P, Gordois A, Oglesby A. Pr edicted costs andoutcomes from reduced vibration detection in people with diabetes inthe U.S. Diabetes Care. 2003;26(8):2305–2310.
6. Gordois A SP, Shearer A, Oglesby A. The healthcare costs of diabeticperipheral neuropathy in the UK. Diabet Foot. 2003;6:62–73.
7. Prompers L, Huijberts M, Schaper N, et al. Resour ce utilisation andcosts associated with the treatment of diabetic foot ulcers. Prospectivedata from the Eurodiale Study. Diabetologia. 2008;51(10):1826–1834.
8. Fowler EM, Vesely N, Johnson V, Harwood J, T ran J, Amberry T.Wound car e for patients with diabetes. Adv Skin W ound Care .2003;16(7):342–346.
9. Hinchliffe RJ, Valk GD, Apelqvist J, et al. A systematic r eview of theeffectiveness of interventions to enhance the healing of chronic ulcersof the foot in diabetes. Diabetes Metab Res Rev . 2008;24(suppl1):S119–S144.
10. Veves A, Sheehan P, Pham HT. A randomized, controlled trial of Pro-mogran (a collagen/oxidized regenerated cellulose dressing) vs stan-dard treatment in the management of diabetic foot ulcers. Arch Surg.2002;137(7):822–827.
11. Kakagia DD, Kazakos KJ, Xarchas KC, et al. Synergistic action of pro-tease-modulating matrix and autologous growth factors in healing ofdiabetic foot ulcers. A prospective randomized trial. J Diabetes Com-plications. 2007;21(6):387–391.
12. Chow I, Lemos EV, Einarson TR. Management and prevention of dia-betic foot ulcers and infections: a health economic r eview. Pharma-coeconomics. 2008;26(12):1019–1035.
13. Ghatnekar O, Willis M, Persson U. Cost-effectiveness of treating deepdiabetic foot ulcers with Pr omogran in four Eur opean countries. JWound Care. 2002;11(2):70–74.
14. Sibbald RG, Torrance G, Hux M, Attard C, Milkovich N. Cost-effective-ness of becaplermin for nonhealing neur opathic diabetic foot ulcers.Ostomy Wound Manage. 2003;49(11):76–84.
15. Lazaro-Martinez JL, Garcia-Morales E, Beneit-Montesinos JV, Mar-tinez-de-Jesus FR, Aragon-Sanchez FJ. [Randomized comparativetrial of a collagen/oxidized regenerated cellulose dressing in the treat-ment of neuropathic diabetic foot ulcers]. Cir Esp. 2007;82(1):27–31.
16. Weinstein MC. Recent developments in decision-analytic modelling foreconomic evaluation. Pharmacoeconomics. 2006;24(11):1043–1053.
17. Laupacis A, Sackett DL, Roberts RS. An assessment of clinicallyuseful measures of the consequences of treatment. N Engl J Med.1988;318(26):1728–1733.
18. Prompers L, Huijberts M, Apelqvist J, et al. Delivery of care to diabeticpatients with foot ulcers in daily practice: r esults of the Eur odialeStudy, a prospective cohort study. Diabet Med. 2008;25(6):700–707.
19. Armstrong DG, Lavery LA, Nixon BP, Boulton AJ. It’s not what you puton, but what you take off: techniques for debriding and off-loading thediabetic foot wound. Clin Infect Dis. 2004;39(suppl 2):S92–S99.
04-08_Lazaro-Martinez:Layout 1 11/4/10 9:40 AM Page 8
NOVEMBER 2010 SUPPLEMENT A OSTOMY WOUND MANAGEMENT 9www.o-wm.com
Chronic wounds represent a significant medical problemand create huge financial burdens on healthcare systems
globally. Despite the daunting implications of this medicaldilemma, no standard-of-care algorithms have been univer-sally accepted. Topical treatments often are chosen on the basesof local t raditions.1 Wet-to-dry gauze dressings are the mostwidely used primary dressing material in the US2 and may beerroneously considered a standard of care; in a review of theliterature, Ovington3 notes that impeded healing due to localtissue cooling, disruption of angiogenesis by dressing removal,
and increased infection risk from frequent dressing changes,strikethrough, and prolonged inflammation represent goodreasons to abandon this t raditional dressing technique. Thebenefits of moist wound healing are well documented but inpractice the use of gauze, particularly as a wet-to-dry dressing,does not ensure a moist wound environment.4
Collagen/oxidized regenerated cellulose (C/ORC) has beenshown in vitro to reduce elastase, plasmin, and metallopro-teinase activity in chronic wound exudate in patients with di-abetes.5 Results from randomized controlled trials involving
A Retrospective Study of Sequential Therapywith Advanced Wound Care Products versus Saline Gauze Dressings: Comparing Healing and Cost
Robert J. Snyder, DPM, CWS; Deborah Richter, RN, CWCA; and Mary Ellen Hill, PT
AbstractTreating chronic wounds often creates daunting medical and financial challenges — perhaps , in part, because no stan-dard-of-care algorithms have been universally accepted for the provision of care. In a retrospective chart study of patientsreceiving home care ser vices, researchers compared the results on lo wer extremity wound healing of using sequentialtherapy comprising advanced wound care products (collagen/oxidized regenerated cellulose [C/ORC] and collagen/oxi-dized regenerated cellulose + silver/ORC [C/ORC/silver]) versus saline-soaked gauze. Nine hundred, seventy-four (974)persons fit the inclusion criteria; 873 had received C/ORC and C/ORC/silver and 101 had received the saline gauze treat-ment. Demographics were comparable in both groups with regard to age (range 55 to 80 years) and wound type (traumaleading to chronic ulcers, pressure ulcers, neuropathic ulcers in persons with diabetes, postsurgical ulcers, locally infectedulcers, and venous leg ulcers). After 2 months’ treatment, 95% of the C/ORC and C/ORC/silver-treated wounds closed ata total cost of $2,145, compared to 7.2% of the saline gauze-treated group at a total cost of $7,350; 43% of saline-treatedwounds healed by 6 months at a total cost of $22,050. The additional expense incurred was for nursing costs, due mainlyto the need f or more frequent dressing changes . When compared to saline gauz e dressings, sequential therapies andadvanced wound care products may reduce the frequency of nursing visits and optimize wound healing time, subsequentlyreducing healthcare costs; thus, underscoring the need for a paradigm shift in the standard of care f or the treatment ofchronic wounds in the home care environment.
Key Words: chronic wounds, advanced care therapy, home health care, healthcare cost, standard wound care, health economics
Index: Ostomy Wound Management 2010;56(11A):9–15
Potential Conflicts of Interest: Dr. Snyder discloses he is the Medical Director for Systagenix Wound Care, Quincy, MA.
Dr. Snyder is the Medical Director for Systagenix Wound Management, Quincy, MA; and Medical Director, Wound Healing Center at University Hospital, Tamarac,FL. Ms. Richter is a certified nurse wound specialist and Ms. Hill is a physical therapist with a special inter est in wound management, Comprehensive HomeCare of Broward, Ft. Lauderdale, FL. Please address correspondence to: Robert J. Snyder, DPM, CWS, 7301 N. University Drive, Tamarac, FL 33321; email:[email protected].
HEALTH ECONOMICS
09-15_Snyder:Layout 1 11/4/10 9:42 AM Page 9
10 OSTOMY WOUND MANAGEMENT NOVEMBER 2010 SUPPLEMENT A www.o-wm.com
HEALTH ECONOMICS
patients with venous leg ulcers6 and diabetic foot ulcers7,8 haveprovided evidence that C/ORC decreases protease activity inwound exudates and can accelerate healing rates of venous legulcers.9 A randomized, prospective controlled clinical t rial10
involving wounds treated with C/ORC demonstrated bettertissue regeneration and faster time to complete healing whencompared to wounds treated with good wound care alone.
Silver appears to positively effect wound healing, provid-ing antimicrobial and anti-inflammatory benefits to healing.A review of the literature11 reveals that unlike silver nitrateand silver sulfadiazine, which require repeated applica-tions, new technologies allow for consistent silver deliveryover time while maintaining br oad-spectrum antimicro-bial activity against yeasts, molds, and bacteria, including
methicillin-resistant Staphylococcus aureus (MRSA) and van-comysin-resistant Enterococci (VRE). A r andomized con-trolled pilot study by Lanzara et al 12 involving 30 patientswith difficult-to-heal venous leg ulcers showed that 12 weeksof wound treatment using C/OR C and C/OR C/silver andcompression substantially reduced ulcer size compared tocontrol treatment with moist wound healing and compres-sion alone. However, antiseptics such as silver were not de-signed to be utilized indefinitely. A review of the literature13
revealed that eliminating sil ver in favor of other advancedwound products that re-balance the wound microenviron-ment may move wound progression from preparation to clo-sure — using an C/OR C and C/OR C/silver pr otocol hasshown the abilit y to reduce protease activity, scavenge free
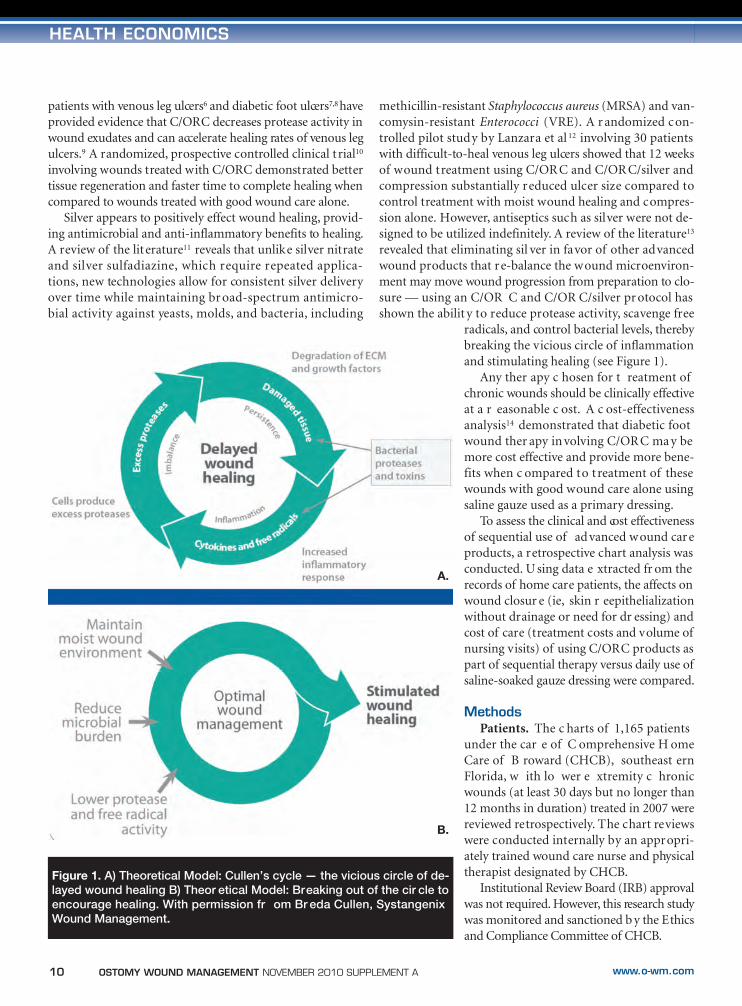
radicals, and control bacterial levels, therebybreaking the vicious circle of inflammationand stimulating healing (see Figure 1).
Any ther apy c hosen for t reatment ofchronic wounds should be clinically effectiveat a r easonable c ost. A c ost-effectivenessanalysis14 demonstrated that diabetic footwound ther apy in volving C/OR C ma y bemore cost effective and provide more bene-fits when c ompared to treatment of thesewounds with good wound care alone usingsaline gauze used as a primary dressing.
To assess the clinical and cost effectivenessof sequential use of advanced wound careproducts, a retrospective chart analysis wasconducted. U sing data e xtracted fr om therecords of home care patients, the affects onwound closur e (ie, skin r eepithelializationwithout drainage or need for dr essing) andcost of care (treatment costs and volume ofnursing visits) of using C/ORC products aspart of sequential therapy versus daily use ofsaline-soaked gauze dressing were compared.
MethodsPatients. The c harts of 1,165 patients
under the car e of C omprehensive H omeCare of B roward (CHCB), southeast ernFlorida, w ith lo wer e xtremity c hronicwounds (at least 30 days but no longer than12 months in duration) treated in 2007 werereviewed retrospectively. The chart reviewswere conducted internally by an appropri-ately trained wound care nurse and physicaltherapist designated by CHCB.
Institutional Review Board (IRB) approvalwas not required. However, this research studywas monitored and sanctioned b y the Ethicsand Compliance Committee of CHCB.
Figure 1. A) Theoretical Model: Cullen’s cycle — the vicious circle of de-layed wound healing B) Theor etical Model: Breaking out of the cir cle toencourage healing. With permission fr om Br eda Cullen, SystangenixWound Management.
A.
B.
09-15_Snyder:Layout 1 11/4/10 9:42 AM Page 10

NOVEMBER 2010 SUPPLEMENT A OSTOMY WOUND MANAGEMENT 11www.o-wm.com
HEALTH ECONOMICS
Data mining procedure. Retrospective analysis was pred-icated upon a search of the database of CHCB for diagnosiscodes (ICD-9). Charts of patients receiving palliative care orusing negative pressure wound therapy (NPWT) or humanskin equivalents and patients w ith severe ischemia, atypicalwounds, and a hiatus in t reatment of more than 1 monthwere excluded. Based on infor mation in the c harts, patientswere divided into two groups: group A received sequentialtherapy using C/ORC/silver and C/ORC (Promogran® MatrixWound Dressing and Promogran Prisma® Wound BalancingMatrix (Systagenix Wound Management, Gargrave, UK) andgroup B received saline gauze dressings.
Sequential therapy. Sequential therapy represents a treat-ment philosophy — ie, when wound appearance changes, itmay be appropriate to change the t ype of dressing used toensure dressing properties rebalance the wound environmentand support healing in an appropriate manner.
For wounds in both groups showing local wound infectionat the commencement of therapy, treatment was initiated withtopical antimicrobial/antiseptic dressings such as hydro-alginateantimicrobial dressing with silver (Silvercel®, Systagenix WoundManagement, Gargrave, UK) or w ith cadexomer iodine alongwith culture-driven systemic antibiotics, if necessary. In keepingwith the sequential ther apy model, these treatments were dis-continued in favor of more appropriate protocols when signsand symptoms of infection cleared. Infection was defined clin-ically based on the pr esence of purulent secretions or at leasttwo signs and symptoms of inflammation.15
Group A patients receiving sequential ther apy were ini-tially t reated w ith C/ORC/silver to decrease the bact erialbioburden and to prepare the wound bed for fur ther treat-ment. When the wound improved clinically (usually within2 to 3 weeks) C/ORC was used to continue treatment of thesewounds, restore the balance within the wound microenvi-ronment, and promote closure.
Group B patients were provided saline-moistened dress-ings changed daily and covered with dry sterile dressings.
Sequential w ound car e pr otocol. C/ORC/silver andC/ORC dr essing c hange fr equency adher ed t o man ufac-turer’s guidelines. These wounds and dressing were preparedas follows:
• Debridement when nec essary, followed by woundsite irrigation in accordance with standard protocols.
• For wounds with little or no exudate, C/ORC/sil-ver and C/ORC were hydrated with saline. Thedressings could be pressed on if needed to breakthe surface tension and help facilitate hydration.
For dressing application:• The dr essing was cut or t orn t o the siz e of the
wound and applied directly to the wound bed• After hydration through exposure to wound exu-
dates or saline, the dressings became gelatinous, cre-ating intimate contact with the wound surface.
• The dressing is biodegradable and will be absorbedinto the body over time
• To maintain a moist w ound environment, thesedressings must be c overed w ith a semi-oc clusivedressing.
Dressing change and removal:• Applied daily or per physician recommendation• Frequency of application depended on le vel of
exudate• It was not necessary to remove any residual material
during dressing changes.Patients in sequential therapy Group A had been provided
nursing visits daily for 1 week, reduced to three times/weekduring week two, and then further reduced to once per weekthereafter, when feasible.
In each case, the principles of wound bed preparation(debridement, infec tion, and moistur e c ontrol, andwound edge pr eparation) and disease-specific w oundmanagement protocols were followed in both G roups Aand B — eg , neuropathic ulcers in persons w ith diabeteswere treated with strict metabolic control, weekly debride-ment and offloading; v enous leg ulc er patients w eretreated with appropriate compression.16,17
Wound he aling assessment. All ulc ers w ere pho-tographed on admission, then monthly, to provide a visualrecord of any changes in appearance. In review of the data-base, healing progress was assessed w eekly by measuringwound length, width, and depth v ia planimetry; however,these data, as well as patient demographics relating to sec-ondary underlying cormorbidities (eg, renal disease, ane-mia, and diabetes) unless otherwise captured as a specificulcer group (eg, neuropathic ulcer in persons with diabetes)could not be g leaned retrospectively; therefore, they werenot included.
The effects of sequential treatment utilizing C/ORC/silverand C/ORC were measured by determining complete woundclosure, defined as skin reepithelialization without drainageor dressing requirement. Results were compared with com-plete wound closure results of Group B of patients t reatedwith saline gauze dressings applied daily.
It is standard policy for CHCB to monitor safety via con-stant surveillance for adverse events during treatment; thiswas reflected in the charts and data reviewed.
Calculation of treatment costs. Dressing costs were basedon the average purchase price to the agency (CHCB). TheC/ORC dressings were priced at $10.00/dressing; gauze andsaline were calculated at $2.50/dr essing. The c ost of eachhome nursing visit in both groups was $120.
Statistical analysis. Data involving average material costs(eg, gloves, saline, gauze, C/ORC/silver, C/ORC, dry steriledressing, tape), nursing costs (taking vital signs; wound eval-uation, measurements, and photos when necessary; dressingchanges; and charting), and number of wounds healed in the
09-15_Snyder:Layout 1 11/4/10 9:42 AM Page 11
12 OSTOMY WOUND MANAGEMENT NOVEMBER 2010 SUPPLEMENT A www.o-wm.com
HEALTH ECONOMICS
measured time frames were extracted to a spreadsheet andanalysis performed using Sigma Plot (10.0 version). Con-fidence intervals (CI, 98%), standard deviations (SD), andvariance were calculated for each group at 2 months and6 months. The level of significance was considered to beP <0.05.
ResultsNine hundred, seventy-four (974) persons fit the inclu-
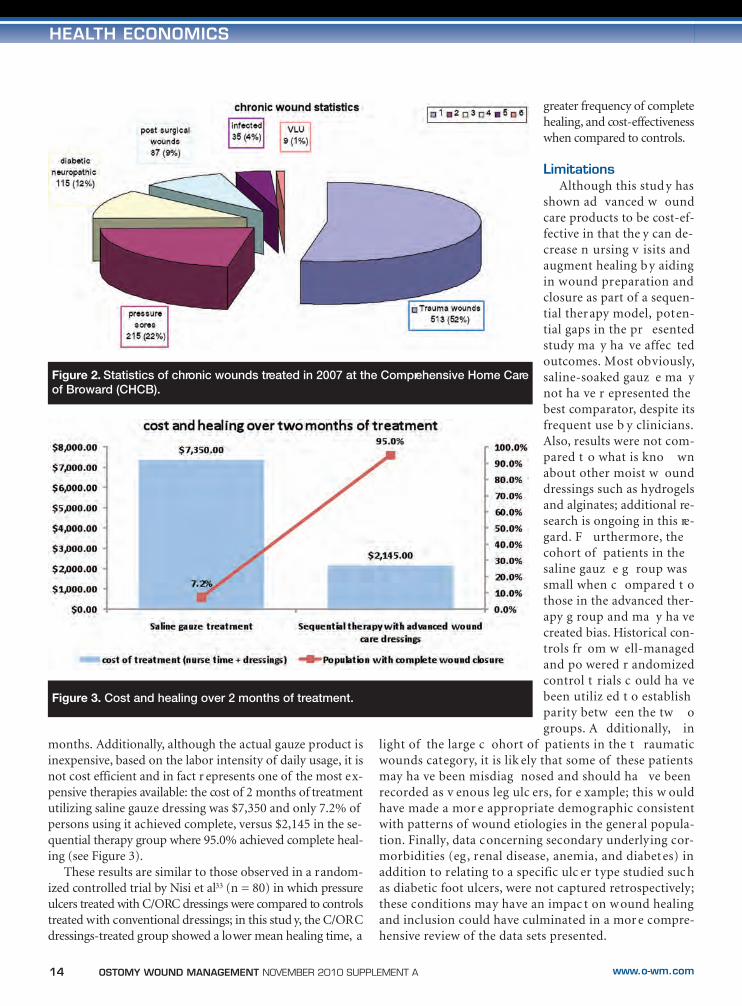
sion criteria; 873 had received C/ORC/silver and C/ORC and101 received saline gauze treatment. The majority of treatedpatients in both g roups was elderly (a verage age 70 y ears;range of 55 to 80 years). A random sampling of the data re-vealed wound sizes ranged from 1 cm2 to 12cm2. Group A in-cluded 463 t rauma leading to chronic wounds (53%), 192pressure ulcers (22%), 102 diabetic foot ulc ers (11%), 78postsurgical wounds (9%), 30 locally infected wounds (4%),and ei ght v enous le g ulcer s (1%). G roup B inc luded 53trauma leading to chronic wounds (53%), 22 pressure ulcers(22%), 12 diabetic foot ulc ers (12%), nine postsurg icalwounds (8%), four locally infected wounds (4%), and one ve-nous leg ulcer (1%).
Wound he aling. In g roup A, 95.0% of the w oundsachieved complete wound closure in 38.6 days (95% CI; SD4.62; variance 21.33; population SD 4.54567; variance pop-ulation SD 20.66). During the same time per iod, 7.2% pa-tients in group B achieved complete wound closure (95% CI;SD 0.72; variance 0.52; population SD 0.66; variance popu-lation SD 0.44); after 6 months of treatment, a total of 43%of group B wounds achieved complete wound closure (95%CI; SD 4.25; variance SD 18.07; population SD 4.09; variancepopulation SD 16.7).
Local infection not appar ent on initial e valuation andthus presumed to have occurred during the treatment phasewas the only adverse effect observed. However, this condition
was classified as mild to moder-ate and presented in <1% of pa-tients in each group.
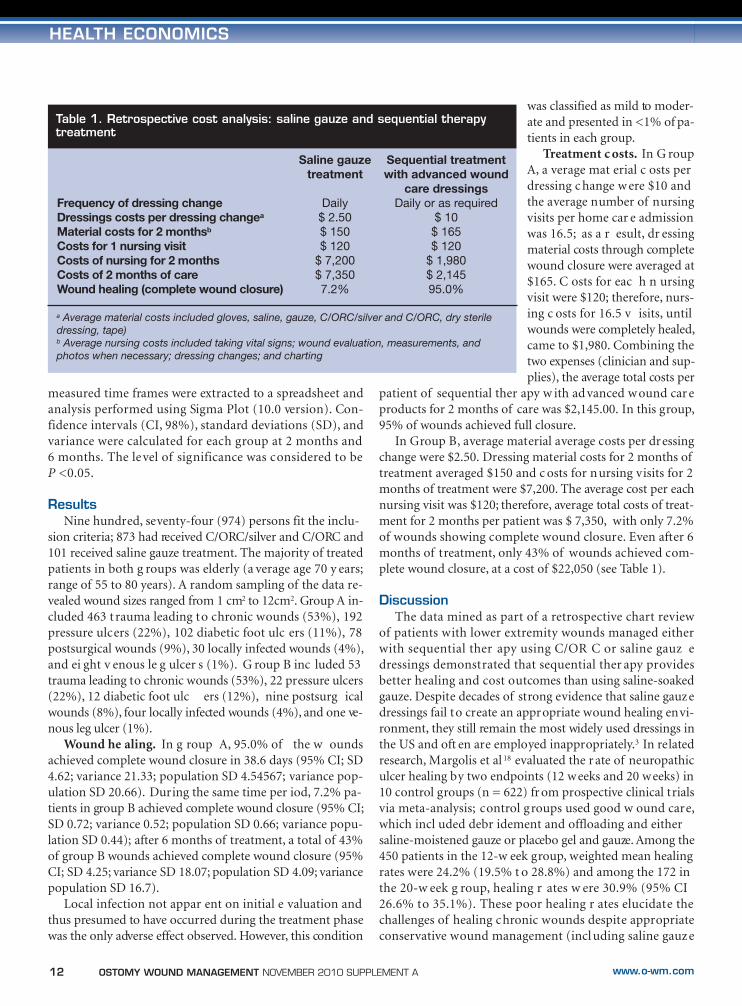
Treatment c osts. In G roupA, a verage mat erial c osts perdressing c hange w ere $10 andthe average number of nursingvisits per home car e admissionwas 16.5; as a r esult, dr essingmaterial costs through completewound closure were averaged at$165. C osts for eac h n ursingvisit were $120; therefore, nurs-ing c osts for 16.5 v isits, untilwounds were completely healed,came to $1,980. Combining thetwo expenses (clinician and sup-plies), the average total costs per
patient of sequential ther apy w ith ad vanced w ound car eproducts for 2 months of care was $2,145.00. In this group,95% of wounds achieved full closure.
In Group B, average material average costs per dressingchange were $2.50. Dressing material costs for 2 months oftreatment averaged $150 and c osts for nursing visits for 2months of treatment were $7,200. The average cost per eachnursing visit was $120; therefore, average total costs of treat-ment for 2 months per patient was $ 7,350, with only 7.2%of wounds showing complete wound closure. Even after 6months of treatment, only 43% of wounds achieved com-plete wound closure, at a cost of $22,050 (see Table 1).
DiscussionThe data mined as part of a retrospective chart review
of patients with lower extremity wounds managed eitherwith sequential ther apy using C/OR C or saline gauz edressings demonstrated that sequential ther apy providesbetter healing and cost outcomes than using saline-soakedgauze. Despite decades of strong evidence that saline gauzedressings fail to create an appropriate wound healing envi-ronment, they still remain the most widely used dressings inthe US and oft en are employed inappropriately.3 In relatedresearch, Margolis et al 18 evaluated the r ate of neuropathiculcer healing by two endpoints (12 weeks and 20 weeks) in10 control groups (n = 622) fr om prospective clinical trialsvia meta-analysis; control groups used good w ound care,which incl uded debr idement and offloading and eithersaline-moistened gauze or placebo gel and gauze. Among the450 patients in the 12-w eek group, weighted mean healingrates were 24.2% (19.5% t o 28.8%) and among the 172 inthe 20-w eek g roup, healing r ates w ere 30.9% (95% CI26.6% to 35.1%). These poor healing r ates elucidate thechallenges of healing chronic wounds despite appropriateconservative wound management (incl uding saline gauze
Table 1. Retrospective cost analysis: saline gauze and sequential therapytreatment
Frequency of dressing changeDressings costs per dressing changea
Material costs for 2 monthsb
Costs for 1 nursing visitCosts of nursing for 2 monthsCosts of 2 months of careWound healing (complete wound closure)
Saline gauzetreatment
Daily$ 2.50$ 150$ 120
$ 7,200$ 7,3507.2%
Sequential treatment with advanced wound
care dressingsDaily or as required
$ 10$ 165$ 120
$ 1,980$ 2,14595.0%
a Average material costs included gloves, saline, gauze, C/ORC/silver and C/ORC, dry steriledressing, tape)b Average nursing costs included taking vital signs; wound evaluation, measurements, and photos when necessary; dressing changes; and charting
09-15_Snyder:Layout 1 11/5/10 12:15 PM Page 12

NOVEMBER 2010 SUPPLEMENT A OSTOMY WOUND MANAGEMENT 13www.o-wm.com
HEALTH ECONOMICS
dressing) and proliferate the notion that advanced woundcare products may be considered more costly and are oftenunavailable to the clinician, especially in the acute hospitalsetting where patients may be admitted only for a few days.As such, advanced wound therapies often are not utiliz edbut may be required to treat ulcers that fail to progress withgood w ound car e alone. R esearch17 shows that when awound fails to progress by at least 50% in the first 4 weeksdespite implementation of disease-specific ther apies, it isunlikely it w ill heal in 12 w eeks. Ther efore, when goodwound care does not pr oduce a desir ed result, advancedtherapies should be considered.
Impediments to healing. Chronic wounds fail to followthe normal pattern of wound repair; the pathogenesis ofchronic wounds is characterized by persistent inflammationand an imbalance in protease/protease-inhibitor levels.19 Per-sistent inflammation and ongoing proteolysis of matrix pro-teins, such as fibronectin, laminin, various collagens, and lowlevels of growth factors and growth factor receptors impedegranulation and epithelialization in c hronic wounds.20,21 Inaddition, a review of the literature22-24 reveals that a high per-centage of w ounds w ith dela yed healing ha ve bact erialbiofilms that host antibodies, inflammatory cells, antibiotics,and disinfectants cannot eradicate.
Sequential therapy.The importance of wound bed preparation. Knowing these
biochemical variables, many wound care specialists have em-braced moist w ound healing and the r ecent c oncept ofwound bed preparation (WBP) as the under pinning in fa-cilitating healing. Falanga25 defined this hypothesis as themanagement of a wound in order to accelerate endogenoushealing or to facilitate the effectiveness of other therapeuticmeasures. This model e xtends the holistic appr oach t owound management, removing barriers to healing, establish-ing healthy granulation tissue, and stimulating a well-vascu-larized w ound bed. An understanding of w ound healingscience and inherent differences between acute and chronicwounds remain mandatory in facilitating these changes andmaking appropriate treatment choices.16
WBP combines a number of important concepts, includ-ing debr idement, t reatment of infection, management ofmoisture balanc e, and w ound edge pr eparation. Thismethodology fosters removal of healing impediments whileinitiating the repair process and restoring healthy granula-tion tissue over time. This encourages the sequential use oftherapeutic products in order to reduce infection and bacte-rial bioburden, rebalance wound biochemistry, and encour-age growth factor production while stimulating wound edgeepithelialization and addressing senescent cells. Treatmentwith saline gauze remains ineffective in this regard.3
The role of timing, products, and cost. In a review of the lit-erature, Frantz and Gardner26 hypothesize that changes inwound care must be based on changing wound parameters,
as well as timely, complete, and accurate wound assessment.This review represents the foundation for sequential use ofproducts and therapies appropriate to the changing woundenvironment. A literature review by Hanson1 concluded thatif a wound can be re-dressed at longer intervals and if healingcan occur more quickly, advanced product usage can be costeffective; Metzer’s27 review of the literature found that “bestpractice” wound management included moist wound heal-ing and the use of advanced products that promote efficientuse of nursing time. Similarly, Horch et al’s 28 review of theliterature found that despit e higher daily costs, some alter-native wound therapies turn out to be more cost efficientwhen all economic factors are considered. A qualitative studyinvolving 65 pr ofessionals c onducted b y Armstrong andPrice29 revealed that barriers to the use of modern productsdid not appear t o be associated with availability or knowl-edge and experience of use — cost was the most frequentlycited barrier. Although it is true that modern dressing prod-ucts have a higher unit cost, they require fewer changes thangauze, making them more cost effective. If other issues, suchas time to healing and quality of life, are included, cost effec-tiveness should be a major force for change.3
C/ORC/silver. The product used in the cur rent contains1% silver ORC salt, which equates to a release of 0.25% ionicsilver. When compared to other available silver dressings, thiswould be c onsidered a “lo w-dose” v ehicle; ho wever, theproduct has been shown to provide significant reductions inbacterial counts in a standard in vitro assay of antimicrobialactivity without harming host cells in vitro.30 In a pilot ran-domized controlled study with 30 venous leg ulcer patients,Lanzara et al 12 demonstrated that 12 w eeks of treatment ofwounds with C/ORC/silver resulted in ulcer size reduction.
The use of low- versus high-dose silver is controversial. Inresults of a literature review, Drosou et al31 postulate that thestrongest argument against the use of antiseptics in woundsis that these substances, using primarily in vitro models, maybe cytotoxic to cells essential to wound healing; however, thiscytotoxicity appears to be concentration-dependant. Severalantiseptics in low concentrations may not be cy totoxic, al-though they retain their antibacterial activity in vitro; for ex-ample, sil ver ions at lo w par ts per million (ppm)concentrations have been shown to be bactericidal againstmost planktonic bacteria.32 However, in vitro research doesnot always correlate to the patients’ bedside and most treat-ment strategies still remain intuitive. It remains likely that ahigher does of silver, such as those used in the initial phaseof treatment in this stud y, may be required in the pr esenceof overt infection. Additional in vivo research is needed t ofurther investigate this issue
Cost-effectiveness. The current study helps dispel se v-eral myths regarding the effectiveness and cost benefits ofsaline gauze dressing. It is clear from this study that salinegauze is ineffecti ve; healing r ates ar e ab ysmal e ven at 6
09-15_Snyder:Layout 1 11/4/10 9:43 AM Page 13
14 OSTOMY WOUND MANAGEMENT NOVEMBER 2010 SUPPLEMENT A www.o-wm.com
HEALTH ECONOMICS
months. Additionally, although the actual gauze product isinexpensive, based on the labor intensity of daily usage, it isnot cost efficient and in fact r epresents one of the most ex-pensive therapies available: the cost of 2 months of treatmentutilizing saline gauze dressing was $7,350 and only 7.2% ofpersons using it achieved complete, versus $2,145 in the se-quential therapy group where 95.0% achieved complete heal-ing (see Figure 3).
These results are similar to those observed in a random-ized controlled trial by Nisi et al33 (n = 80) in which pressureulcers treated with C/ORC dressings were compared to controlstreated with conventional dressings; in this stud y, the C/ORCdressings-treated group showed a lower mean healing time, a
greater frequency of completehealing, and cost-effectivenesswhen compared to controls.
LimitationsAlthough this stud y has
shown ad vanced w oundcare products to be cost-ef-fective in that the y can de-crease n ursing v isits andaugment healing b y aidingin wound preparation andclosure as part of a sequen-tial therapy model, poten-tial gaps in the pr esentedstudy ma y ha ve affec tedoutcomes. Most obviously,saline-soaked gauz e ma ynot ha ve r epresented thebest comparator, despite itsfrequent use b y clinicians.Also, results were not com-pared t o what is kno wnabout other moist w ounddressings such as hydrogelsand alginates; additional re-search is ongoing in this re-gard. F urthermore, thecohort of patients in thesaline gauz e g roup wassmall when c ompared t othose in the advanced ther-apy g roup and ma y ha vecreated bias. Historical con-trols fr om w ell-managedand po wered r andomizedcontrol t rials c ould ha vebeen utiliz ed t o establishparity betw een the tw ogroups. A dditionally, in
light of the large c ohort of patients in the t raumaticwounds category, it is lik ely that some of these patientsmay ha ve been misdiag nosed and should ha ve beenrecorded as v enous leg ulc ers, for e xample; this w ouldhave made a mor e appropriate demographic consistentwith patterns of wound etiologies in the general popula-tion. Finally, data concerning secondary underlying cor-morbidities (eg, renal disease, anemia, and diabetes) inaddition to relating to a specific ulc er type studied suc has diabetic foot ulcers, were not captured retrospectively;these conditions may have an impac t on w ound healingand inclusion could have culminated in a mor e compre-hensive review of the data sets presented.
Figure 2. Statistics of chronic wounds treated in 2007 at the Comprehensive Home Careof Broward (CHCB).
Figure 3. Cost and healing over 2 months of treatment.
09-15_Snyder:Layout 1 11/4/10 9:43 AM Page 14

NOVEMBER 2010 SUPPLEMENT A OSTOMY WOUND MANAGEMENT 15www.o-wm.com
HEALTH ECONOMICS
Conclusions Despite the limitations of this r etrospective study, the
analysis of data shows that utilizing advanced wound careproducts such as C/ORC/silver and C/ORC in lower ex-tremity ulcers applied sequentially ma y better optimizewound healing when c ompared to saline gauze and mayreduce the fr equency of n ursing v isits and subsequenthealthcare c osts. The data suggest that t reatment w ithsaline gauze dressing applied daily may be 10 times mor ecostly than advanced therapies and provide fewer benefits.These results should foster a change in practice away from“traditional” saline gauze dressings and encourage a para-digm shift in the standar d of care for the t reatment ofchronic lower extremity wounds in the home care environ-ment, w ith pot ential far -reaching implications in theglobal wound care community. ■
References1. Hansson C. Interactive wound dressings: a practical guide to their use
in older patients. Drugs Aging. 1997;11(4):271–284.2. McCallon ST, Knight CA, Vallulus P, et al. Vacuum–assisted closure
versus saline-moistened gauze in the healing of post-operative dia-betic foot wounds. Ostomy Wound Manage. 2000;46(8):28–34.
3. Ovington LG. Hanging wet to dry dr essing out to dry . Home HealthNurse. 2001;19(8):1–11.
4. Bolton LL, Monte K. Moisture and healing beyond the jargon. OstomyWound Manage. 2000;46(1A):S51–S62.
5. Cullen B, Smith R, McCulloch E, Silcock D, Morrison L. Mechanism ofaction of PROMOGRAN, a protease modulating matrix, for the tr eat-ment of diabetic foot ulcers. Wound Rep Reg. 2002;10:16–25.
6. Smeets R, Ulrich D, Unglaub F, Wöltje M, Pallua N. Effect of oxidisedregenerated cellulose/collagen matrix on proteases in wound exudateof patients with chr onic venous ulceration. Int W ound J .2008;5:195–203.
7. Lobmann R, Schultz G, Lehnert H. Pr oteases and the diabetic footsyndrome: mechanisms and therapeutic implications. Diabetes Care.2005;28:461–71.
8. Veves A, Sheehan P, Pham HT. A randomized, controlled trial of Pro-mogran (a collagen/oxidized regenerated cellulose dressing) vs stan-dard treatment in the management of diabetic foot ulcers. Arch Surg.2002;137:822–827.
9. Vin F, Teot L, Meaume S. The healing pr operties of Promogran in ve-nous leg ulcers. J Wound Care. 2002;11:335–41.
10. Lázaro-Martínez JL, Gar cía-Morales E, Beneit-Montesinos JV ,Martínez-de-Jesús FR, Aragón-Sánchez FJ. Randomized comparativetrial of a collagen/oxidized regenerated cellulose dressing in the treat-ment of neuropathic diabetic foot ulcers. Cir Esp. 2007;82:27–31.
11. Demling R, DeSanti, L. Ef fects of silver on wound management.Wounds. 2001;13(suppl A):4–15
12. Lanzara S, Tacconi G, Gianesini S, et al. A Pilot Randomized T rial toDetermine the Effects of a New Active Dressing on Wound Healing ofVenous Leg Ulcers. Oral presentation at the EWMA 2008 Conference.Lisbon Portugal. May14-16, 2008.
13. Gibson D, Cullen B, Legerstee R, Harding KG, Schultz G. MMPs madeeasy. Wounds International. 2009;1(1): Available at: www.woundsin-ternational.com. Accessed September 1, 2010.
14. Ghatnekar O, Willis M, Persson U. Cost effectiveness of treating deepdiabetic foot ulcers with Pr omogran in four Eur opean countries. JWound Care. 2002;11:70–74.
15. Lipsky BA, Berrendi AR, Deery HG, et al. Diagnosis and tr eatment ofdiabetic foot infections. Clin Infect. 2004;39:885–910.
16. Snyder RJ. Rationale for sequential use of topical wound pr oducts-preparing and closing the wound. Podiatry Manage. 2007;June/July:3–6.
17. Snyder RJ, Cardinal M, Dauphinee D, Stavosky J. Diabetic Foot Ul-cers: Less Than 50% Closure in 4 Weeks Predicts Failure to Heal by12 Weeks. Poster presented at the Diabetic Limb Salvage Symposium,Washington, DC. 2009.
18. Margolis D, Kantor J, Berlin J. Healing of neur opathic ulcers: resultsof a meta-analysis. Diabetes Care. 1999;22:692–695.
19. McDaniel HB, Marston WA, Farber MA, Mendes RR, Owens LV, YoungML, Daniel PF, Keagy BA. Recurrence of chronic venous ulcers on thebasis of clinical, etiologic, anatomic, and pathophysiologic criteria andair plethysmography. J Vasc Surg. 2002;35:723–728.
20. Nwomeh BC, Yager DR, Cohen IK. Physiology of the chronic wound.Clin Plast Surg. 1998;25:341–356.
21. Owen CA, Campbell EJ. The cell biology of leukocyte-mediated pr o-teolysis. J Leukoc Biol. 1999;65:137–150.
22. James GA, Swogger E, Wolcott R, et al. Biofilms in chr onic wounds.Wound Rep Reg. 2008; 16(1): 37–44.
23. Costerton JW, Stewart PS, Gr eenberg EP. Bacterial biofilms: a com-mon cause of persistent infections. Science. 1999;284:1318–1322.
24. Costerton JW, Stewart PS. Battling biofilms. Sci Am. 2001;285:74–81.25. Falanga V (ed). New Concepts in Wound Bed Preparation. Berlin, Ger-
many: Springer-Verlag GmbH & Co;2003.26. Frantz RA, Gardner S. Elderly skin car e: principles of chronic wound
care. J Gerontol Nurs. 1994;20(9):35–44. 27. Metzger S. Clinical and financial advantages of moist wound manage-
ment. Home Health Nurs. 2004;22(9):586–590.28. Horch RE, Nord D, Augustin M, et al. Economic aspects of sur gical
wound therapies. Chirurg. 2008;79(6):518–525. 29. Armstrong MH, Price P. Wet-to-dry gauze dressings: fact and fiction.
Available at: www.woundsresearch.com/article/2284. Accessed Sep-tember 20, 2009.
30. Serena TE. Managing the wound micr oenvironment. Wounds.2005;8(suppl. A):7–11.
31. Drosou A, Falabella A, Kirsner R. Antiseptics on wounds: an ar ea ofcontroversy. Wounds. 2003;15(5 ):149–166.
32. Russell AD, Hugo WB. Antimicrobial activity and action of silver. ProgMed Chem. 1994;31:351–370.
33. Nisi G, Brandi C, Grimaldi L, Calabro M, DÁniello C. Use of a protease-modulating matrix in the tr eatment of pr essure sor es. Chirug Ital .2005;57(4):465–468.
09-15_Snyder:Layout 1 11/4/10 9:43 AM Page 15

LLC , TM
83 General Warren Blvd., Suite 100Malvern, PA 19355
www.hmpcommunications.com
Copyright 2010 ©
SYS/GLO/260/1110
SYS130-106
16_Cover4:Layout 1 11/5/10 9:46 AM Page 2