Embed Size (px)
DESCRIPTION
March/April 2011 issue of Missoulian Publication: Living Well
Citation preview
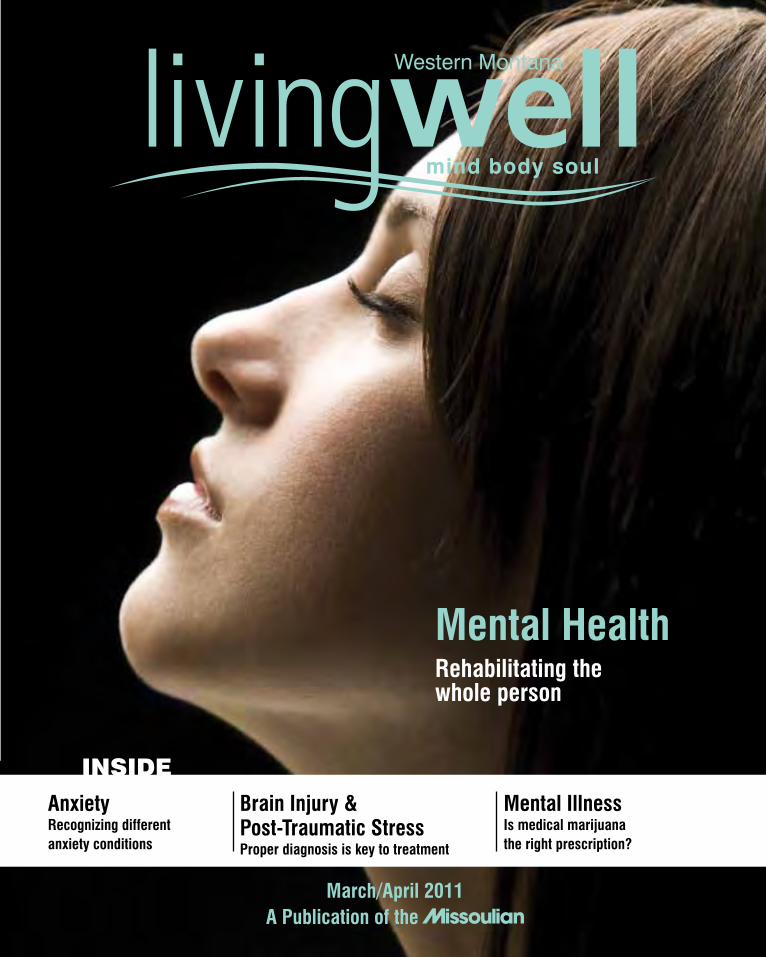
AnxietyRecognizing different anxiety conditions
Brain Injury & Post-Traumatic StressProper diagnosis is key to treatment
Mental IllnessIs medical marijuana the right prescription?
A Publication of theMarch/April 2011
INSIDE
Mental HealthRehabilitating the whole person
Montana’s first and only guide to senior housing.
Copies available now at the Missoulian and other participating locations.
1March/April 2011 ~ livingwell
2 livingwell ~ March/April 2011
publisherStacey Mueller
sales & marketing directorJim McGowan
art directorMichael Lake
graphic designAndrew HendersonDiann KellyMegan Richter
advertising salesHolly Kuehlwein406-523-5223
contributorsDiane Cochran Phillip Holman Kay JenningsCindi LaukesLorna Thackeray
No part of the publication may be reprinted without permission. ©2010 Lee Enterprises, all
rights reserved. Printed in the USA.
A Publication of the
People in Missoula and Western Montana want to feel
good, look good and live well. Available in more than
150 newsstand locations throughout the area, Western
Montana Livingwell is well suited for over 30,000 readers
monthly who want health tips on fitness, nutrition, family,
financial advice, wellness, therapy and beauty.
The opinions, beliefs and viewpoints expressed by the various authors and forum participants in this
publication do not necessarily reflect the opinions, beliefs and viewpoints of the Missoulian or Lee
Enterprises. The author of each article published in this publication owns his or her own words.
L. AUTIOL. LOVEJOY
H. MADDOX
C. MCHOOD
K. LONG
C. SMITHJ. VISSCHER
E. KRESSR. HOOVER
R. WOLFE
S. MCNERNEY
Main Clinic, Broadway Building, 500 W. Broadway, Missoula • 406.721.5600 • 1.800.525.5688 LAR K. AUTIO, MD • KENDRA B. LONG, MD • LISA B. LOVEJOY, MD • HEATHER E. MADDOX, MD • CRAIG H. MCHOOD, MD • CHRISTOPHER B. SMITH, MD • JUDITH K. VISSCHER, MD
Community Medical Center, Physician Center #3, 2835 Ft. Missoula Rd, Missoula • 406.721.5600 REBECCA HOOVER, MD • ERIC J. KRESS, MD • ROCHELLE WOLFE, MD • SARAH MCNERNEY, FNP-BC
Lolo Family Practice,11350 Hwy 93 S, Lolo • 406.273.0045(NOT PICTURED) ELENA FURROW, MD • NED VASQUEZ, MD • LEAH SCHINDLER, FNP-BC
westernmontanaclinic.comServing Missoula since 1922
3March/April 2011 ~ livingwell
March/april 2011 VOl. 2
alSO iN ThiSiSSUE
Depression ~ How to recognize depression at any age. Page 16
suiciDe prevention ~ the top priority. Page 24
smile like You mean it ~ Turn the frown upside down. Page 28
iN ThiSiSSUEmental healthRehabilitating the whole person BraiN
iNjUryand post traumatic stress
aNXiETy what you need to know
page 4 page 12
also
health tip page 32
page 8 page 20
N.a.M.i.national alliance on mental illness
MarijUaNa aNd MENTal illNESS
4 livingwell ~ March/April 2011
Brain Injury & Post-Traumatic
Stress: Common Symptoms and Important Differences
Cindi Laukes, MAMontana Neuroscience Institute

5March/April 2011 ~ livingwell
6 livingwell ~ March/April 2011
Co-occurring brain injuries and post-traumatic stress (PTSD) have recently gained greater national attention due largely to the numbers of Veterans returning home with one or both of these diagnoses. A group of five collaborating federal agencies, recognizing the significance of these overlapping issues, recently published a set of papers in the Archives of Physical Medicine and Rehabilitation to clarify recommendations for more consistency in assessment, diagnoses, research and treatment of brain injuries and PTSD. In Montana, where brain injuries of all levels of severity are common due to motor vehicle accidents, sports concussions, farming accidents and falls, similar issues can arise during the course of everyday living. A frightening, disorienting, violent or life-threatening injury can potentially have similar consequences in all walks of life.
A physical injury to the brain, whether mild or severe, can impact the brain’s ability to function and process information, due to injured nerve cells (neurons), and to delicate damaged tissues of the brain. Injuries to the brain can impact movement, thinking, balance, memory and other daily functions, depending on what part of the brain is involved. What is sometimes less understood is that even mild injuries can also impact emotions, sleep,
concentration and changes in mood, such as increased
7March/April 2011 ~ livingwell
Health Screenings▼
• Cholesterol Checkingin just 10 minutes$30., by appointment
• Free Blood PressureChecksWednesdays, 1–6 pm
• Blood Sugar ScreeningJust $8.
• Prepackaged MedsTaking medications is simple with this time-of-day program
For more informationor to schedule an appointment call us today!
In Eastgate Shopping CenterEast Broadway at VanBuren
549-6163www.eastgatedrug.com
• CholesterolChecking injust10minutes byappointment
• FreeBloodPressure Checks• BloodSugarScreening• PrepackagedMeds Takingmedicationsis simplewiththistime-of dayprogram
• MedBoxes Wesetup&deliver.Let ustaketheworkoutof takingyourmedications.
irritability, anxiety, mood swings or depression. It is primarily in the latter case where some overlapping symptoms common to both brain injury and PTSD may be undiagnosed or misdiagnosed. Following an accident, chronic pain can be another compounding issue, potentially impacting the ability to walk, work, or do simple tasks, and also affecting mood and contributing to irritability, depression, and sleeplessness.
All of these factors combined can make proper diagnosis and treatment of a brain injury and PTSD challenging, but distinguishing differences and similarities may be essential to overall healing. Some symptoms stand out as more clearly related to PTSD, such as persistently re-experiencing the traumatic event through nightmares, flashbacks, a heightened sense of arousal or fearfulness, and an avoidance of any reminders of the trauma. By definition, to meet the criteria for PTSD, these symptoms and others must cause significant disturbances in functioning, and last for at least a month, and typically much longer.
In a milder brain injury, where some symptoms may be similar to those seen in PTSD, such as insomnia, anxiety and irritability, there will often be other physical symptoms such as headache, dizziness, blurred vision
or light intolerance. Depending on the extent and severity of a brain injury, any of these symptoms and others can become compounded, and may also overlap with frightening memories of a life-threatening or disorienting event.
It is possible to treat and rehabilitate both problems if diagnoses are properly made. Some strategies that may be helpful for both include: various structured therapies, anger control and emotional skills, nurturing the hope of recovery, involving the family as a part of the team, relaxation techniques, sleep hygiene, techniques for remembering things, proper medication and pain management, and limiting alcohol and drug use. It is important to receive specialized care for each type of injury, and also to rehabilitate the whole person as they recover from these difficult events and injuries.
If you or a loved one have experienced a brain injury or some of these symptoms, it is best to contact your
physician for further guidance and appropriate referral. For more general information about brain injury
and local resources, feel free to contact the Montana Brain Injury Center at 406-329-5663,
[email protected], or the Brain Injury Association of Montana at 406-541-6442.
It is possible to treat
and rehabilitate
both problems
if diagnoses are
properly made.
8 livingwell ~ March/April 2011
N.A.M.I.National Alliance on Mental Illness
Diane Cochran
“Mental illnesses are treatable
medical conditions.”

9March/April 2011 ~ livingwell
10 livingwell ~ March/April 2011
As a nurse in training fifty years ago, Dorothy Salmonson watched as traumatized veterans were treated with cold showers, insulin shock and other therapies that would be considered inhumane today.
Little was known about mental illnesses then, and Salmonson’s training left her woefully unprepared for the mental health crises that would affect her family in the coming decades.
“What I learned didn’t touch what I needed to know when my daughter had her breakdown,” she said.
Four of Salmonson’s seven children eventually developed mental illnesses, including a son who committed suicide when he was 20 years old. Salmonson and her husband spent years feeling overwhelmed and desperate for help.
They found it through the National Alliance on Mental Illness, or NAMI, a nonprofit organization that provides education and support to people whose lives are affected by mental illnesses.
“Being involved in NAMI has been my salvation,” Salmonson said.
With chapters across the country, including in Missoula, NAMI helps millions of people with local classes and support groups as well as through national advocacy campaigns. The organization was instrumental in convincing scientists to research the brain, which has vastly improved understanding of how mental disorders work.
About 25 percent of Americans experience a mental health disorder in any given year, while 6 percent live with a serious mental illness. Serious mental illnesses include major depression, schizophrenia, bipolar disorder, obsessive-compulsive disorder, panic disorder, post-traumatic stress disorder, and borderline personality disorder.
Mental illnesses are treatable medical conditions. People who develop them are just as sick as are people with a disease like diabetes and just as in
“What I learned didn’t touch what I needed to know”

11March/April 2011 ~ livingwell
need of regular treatment. And, just as a person with diabetes cannot stop her symptoms through willpower, a person with a mental illness cannot stop her symptoms without help.
NAMI helps people with mental illnesses and their loved ones learn about brain disorders and connect to resources. In Missoula, NAMI offers three weekly support groups that focus on coping skills and periodic 12-week courses that provide up-to-date information about disorders and treatments, including medication.
NAMI also works locally and nationally to reduce stigma associated with mental illnesses. That’s why Salmonson shares her family’s story – to let other families struggling with what she calls “the 24-hour rollercoaster ride of mental illness” know that they are not alone and should not be afraid or ashamed to ask for help.
“It’s a good feeling to be part of an organization where we’ll all fighting for the same thing,” Salmonson said.
NAMI Missoula offers three confidential support groups each week.
• 6:30-8 p.m. Tuesdays, Providence Center, Room 107, for family and friends.
• 10 a.m.-noon Thursdays, Providence Center, Room 109, for family and friends.
• 12:30-2 p.m. Fridays, Missoula Public Library, lower level small meeting room, for consumers.
For information about NAMI, call Dorothy at (406) 543-3055 or Mary at (406) 552-5494 or visit www.nami.org
Diane Cochran is a freelance writer and a NAMI member who studies law at the U of M.

12 livingwell ~ March/April 2011
13March/April 2011 ~ livingwell
Marijuana and Mental Illness
Kay Jennings, BSN, MHSA, MSN, APRN-PMH
O n a daily basis, our mental health center is bombarded by clients struggling with mental illness. More and more of these clients are presenting
with medical marijuana cards or attempting to save their money in order to obtain a card. Many have no intention of purchasing a card but use marijuana daily without a prescription. My question to them is always, “If marijuana is working so well, why are you here looking for medication to help your anxiety, voices, depression etc.?”
Not only can these patients not answer that question, most prescribers of psychiatric services struggle with how to advise clients on this topic. As we look at the pros and cons of medical marijuana for people with mental illness, this article will only serve to point things out and not support or endorse the medical use of marijuana. As always, mental health providers need to empower clients to make decisions that help them in their journey of recovery.
14 livingwell ~ March/April 2011
In a study of 302 people who had made serious suicide attempts, 16.2% met the criteria for cannabis dependence or abuse at the time of the attempt, compared with 1.9% of 1,028 randomly selected control subjects (Psychiatric Association).
Some studies suggest that marijuana influences the brain’s stress and reward system in the same way as opiates, nicotine and cocaine.
Chronic marijuana use has long been associated with increased risk of paranoia.
Smoked or burned product increases the risk of certain cancers and pulmonary complications.
Driving under the influence of marijuana poses a significant threat to public safety because of impaired sense of time and perception.
Higher doses of cannabis cause hyper vigilance or paranoia, anxiety and panic, derealization or depersonalization and possible hallucinations.
Employers with drug free work places do not have to accommodate medical marijuana in the work place thus contributing to unemployment of people with mental illness.
Marijuana has the negative effects of smoking on the heart and lungs.
There are few identified interactions with other medications, however, marijuana does have psychoactive effects and should be used with extreme caution in persons suffering from mental illnesses, especially schizophrenia, bipolar disorder and depression.
Drug addiction can happen when prescribers give vulnerable people addictive substances during stressful/vulnerable times in their lives. A question for readers: How is medically driven addiction any different?
15March/April 2011 ~ livingwell
Call for HELP!No Waiting List!
Complete Recovery-Oriented Mental HealthServices and Support
Group Home PlacementsMedicaid Accepted
Call Now! Get Better!406.721.2038
www.windsofchangemontana.com2811 Latimer St • Missoula
16 livingwell ~ March/April 201116
Psychiatry connection:
D e p r e s s i o n

17March/April 2011 ~ livingwell 17
how to recognize DePression at any age
by phillip Holman, MD
s a father of nine children and a husband, I am always concerned about the genetic legacy we pass down to our children. Depression is one of those conditions that can have genetic familial roots and may be part of other ongoing medical diagnoses. Depression is a word we hear bantered around very casually and often, but is never fully defined. It can be a challenge to pinpoint what it means to be depressed. Therefore I have outlined what things to look out for, when you think you might be depressed or see depression in
someone else.Depression in adults can be best described as sadness, feelings of inadequacy and
guilt, tiredness beyond sleep deprivation, events of irritability, pessimism, loss of
D e p r e s s i o n

18 livingwell ~ March/April 2011
DePression is a worD we hear bantereD arounD very casually anD
often, but is never fully DefineD. it can be a challenge to PinPoint what it
means to be DePresseD.

19March/April 2011 ~ livingwell
A 6-week self-management workshop for people with diabetes, high blood pressure, heart disease, arthritis, asthma, chronic pain, mood disorders or other long-term conditions.
• Find practical ways to deal with pain, fatigue and stress.
• Discover better nutrition and exercise choices.• Understand new treatment options.• Learn better ways to talk to your doctor and
family about your health.
For more information call 406-329-5746.
Classes held in Missoula, Polson and the Bitterroot.
Workshops are Facilitated by leaders trained in the Stanford Chronic Disease Self-Management Program who use a standardized,evidence-based curriculum.
Better ChoicesBetter Health™
A Stanford Self-Management Workshop
interest or pleasure, lack of energy and inactivity or everything just seeming to appear hopeless. Depression can present itself in various fluctuations of extremes and intensities of generalized mood numbness, emptiness or sadness. It can be part of another disorder, a result of an illness or an inherited condition. Depression may be short term or long term. It may be associated with Seasonal Affective Disorder (SAD), which is when the number of hours of available natural light diminishes during the winter months. In any case, depression is nothing to be thought of with shame.
It is additionally important to note that depression and depressed moods in children and adolescents present different symptoms. In children and adolescents, one would tend to see behaviors that reflect boredom, sadness and/or irritability.
Teens may have longer periods of feeling depressed that may be associated with changes in weight, sleep disturbances, psychomotor changes, decreased energy, loss of interest in school and activities, suicidal thoughts, feelings of guilt, as well as feelings of worthlessness. Often youth/teens participating in high risk behaviors may be showing identifiers of depression or these high risk behaviors may be a predictor of future depressive moods.
School age children, in general, may show signs of irritability, sad moods, unexplained crying, suicidal thoughts, poor school performance, frequent headaches
or abdominal pain. And pre-school children may look very sad, stop gaining weight, complain of frequent tummy aches and increased crying may be observed.
Furthermore, it is interesting to note that the elderly often do not actually talk about feeling depressed or having depressed moods. The elderly often present a more ambiguous picture of symptoms such as fatigue, insomnia and/or anorexia. As we get older, it may become more difficult to define depression in an individual. There may be no recognizable mood differences and as we age we may naturally feel slowed down somewhat.
It is very important to help loved ones who are suffering with depressed moods. It is important to find a psychiatrist, physician or mental health provider who is a good listener and cares about you and your loved one. Positive treatment plans with the right psychological and medically therapeutic intervention are keys to helping the depressed individual to lead a happy, successful life. It is equally important to have support for those providing support.
A Depression Support Group that I facilitate is offered twice monthly at Community Medical Center in Community Physician Group - Parkside. There is no cost to attend this group. Please call (406) 327-3880 for further information, as well as for dates and times.
Phillip Holman MD is the medical director for psychiatric services for Community Physician Group, part of
Community Medical Center.
20 livingwell ~ March/April 2011
By Phillip Holman, MD
Things you need to know about
Anxiety

21March/April 2011 ~ livingwell
Is it anxiety or something else? What should we be looking for when we think we may be feeling anxious or under stress? How many of you remember feeling
nervous before a test in school? How often did you get that sick sensation as the door opened to your job interview? And what happens when you feel you might have ‘lost it’ under what seemed to be normal circumstances? How do we distinguish generalized anxiety from other disorders such as panic attacks, social anxiety disorder or posttraumatic stress disorder? Let’s have a quick glance at their differences.
Anxiety, as Dr. Sigmund Freud, might have viewed it in Austria over 100 years ago, included clinical presentations of general irritability, anxiety attacks, apprehension/anxious expectations and sometimes phobic avoidance. General anxiety, today, is described frequently as excessive worry, irritability, restlessness, inability to relax, nervousness, expecting bad things to happen or perceiving bad things are about to happen, and the physical manifestation of agitation. Sometimes these symptoms can lead to feelings of dizziness, free floating, increased perspiration, increased sensitivity to pain, higher stress levels and avoidance type behaviors.
22 livingwell ~ March/April 2011
Anxiety is a set of symptoms that can often form a condition, lead to the development of mood disorders such as depression or is concurrent with other medical conditions. Anxiety was initially thought of as learned. However, research illustrates that anxiety is more often an inherited condition.
The following are guidelines from the Diagnostic and Statistical Manual-IV-TR to help you make the distinction between a few of the more recognized types of anxiety conditions, as well as to help you navigate the medical landscape:
1. Generalized anxiety is excessive anxiety and worry. The person finds it difficult to control their worry. This type of anxiety can be associated with restlessness or feeling keyed up or on edge, being easily fatigued, difficulty concentrating or your mind going blank and irritability.
2. Panic attacks are a discrete period of intense fear or discomfort. Symptoms may include palpitations, pounding heart, sweating, trembling or shaking, sensations of shortness of breath, feelings of choking, chest pain, nausea or abdominal stress, feeling dizzy, unsteady, lightheaded, feelings of unreality, fear of losing control or going crazy, fear of dying, numbness or tingling sensations and chills or hot flashes.
3. Social anxiety disorder is avoidance and fear of one or more social or performance situations, generally in a public setting.
4. Posttraumatic stress disorder is a more distant event that is a result of a person witnessing or experiencing an imminent threat of death or serious injury of self and others. The response of the person at that moment involved intense fear, helplessness or horror. As a result, the traumatic occurrence is persistently re-experienced.
In any case, if you have any or all of the above symptoms and feel you are in a physical emergency situation, it is better to rule out a physical crisis and head to the emergency room. And if it is not a medical emergency, then check with your mental health provider to find out more about treating your specific anxiety symptoms. For example, most of us remember having experienced those butterfly feelings as a child before performing in our holiday school plays. So there is no shame in seeking help for a better quality of life for those persistent butterflies.
Phillip Holman M.D., is the medical director of psychiatric services at Community Physician Group at Community Medical Center.
23March/April 2011 ~ livingwell
24 livingwell ~ March/April 2011
Montanans kill themselves at a rate twice the national average, and it’s been that way for decades.
For a least the last 30 years, the Treasure State suicide rate has ranked in the top 10 nationally and often in the top five. Wyoming shares the ignominy with its northern neighbor.
The most recent state listings, compiled in 2007, put Montana’s suicide rate as the second-highest in the country, behind Alaska. Wyoming was fourth-highest. All of the top five were Western states.
Historically, suicide rates for American Indians in Montana tracked just slightly higher than the state’s Caucasian population, according to Karl Rosston, Montana’s suicide prevention coordinator. When he started his job in the Department of Public Health and Human Services three years ago, Montana’s suicide rate was 20 per 100,000 people. The rate for Montana Indians was 21 per 100,000.
“But the gap has widened in the last few years,” Rosston said. “Montana’s rate has stayed the same, but the rate is now 24 for Montana Indians. There have been more suicides among younger Native Americans.”
The Native American population is relatively small, so rates can fluctuate sharply from year to year. The numbers
for 2010 will reflect a cluster of six suicides on the Fort Peck Reservation.
In an awful year that officials at Indian Health Service refuse to talk about in deference to the traumatized tribes, four young people hanged themselves, one used a gun and another stepped in front of a train. The youngest was just 10 years old.
A large cadre of state, federal, tribal and private organizations engaged in a newly energized suicide prevention effort in Indian Country believe that suicide takes too big a toll among Native American youth. It is the second-leading cause of death for those in the 10-to-34 age group and eighth leading cause of death overall for Native Americans.
(In Montana, suicide also ranks as the second leading cause of death for ages 10 to 34 among the Caucasian population and is the ninth leading cause when age groups are combined.)
There are lots of explanations for higher suicide rates among Native Americans, but they all boil down to loss of hope. And that breach in native culture is where the attack has been launched. Programs being implemented on reservations in Montana and Wyoming aim to provide a new generation with skills they need to navigate the dark
Suicide prevention top priorityBy LORNA THACKERAY, Of The Gazette Staff
Billings Gazette, Billings, MT

25March/April 2011 ~ livingwell

26 livingwell ~ March/April 2011

27March/April 2011 ~ livingwell
Home Health of Montana Garners (Yet Another)
Top National Award
541-1800 www.HomeHealthofMontana.com
Home Health of Montana is the only agency in Missoula to consistantly rank in the Top 500 of over 9,000 Medicare-certified agencies surveyed nationanationally.
Why would you settle for less?
Lifeline is a simple, wireless device worn as a pendant or wristband that allows the wearer to summon help with the push of a button, or it can even sense of a button, or it can even sense a fall and automatically call for help.
For about the price of a daily cup For about the price of a daily cup of coffee, Philips Lifeline can help you maintain your independence and give your family peace of mind.
1-800-357-4799
times and see the light of hope beyond.“People who end their life by suicide don’t want to die,
but they don’t see any hope,” said Clayton Small, who teaches a nonprofit program called Native HOPE (Helping Our People Endure).
Small, a Cheyenne who lives in Albuquerque, N.M., has worked on reservations and in school districts across Indian Country using a program that encourages teens to help each other. It teaches participants how to listen to each other, to recognize the signs that someone is contemplating suicide and to reach out and help.
“Eight out of 10 suicides could be prevented if we can break through the ‘code of silence,’ ” he said. “It takes changing attitudes and changing communities to pull them out of the trench they’re in. They need to know you don’t have to keep going down that path into darkness.”
Small has been working with schools on the Fort Peck Reservation, which endured the suicides of six children last year, prompting the tribal council to declare a state of emergency on the northeastern Montana reservation.
It was a traumatizing year for the entire community, but other reservations have suffered similar suicide clusters. Suicide may have first been recognized as an epidemic in this part of the country in 1985, when Wind River Reservation in Wyoming received national attention after nine young men hanged themselves in a two-month period.
“A few years ago it was Flathead,” Rosston said. “Browning and Crow have had bad years, too. They’ve all had their years that seem worse than other years.”
In November, Indian Health Service, the Substance Abuse and Mental Health Services Administration and the Bureau of Indian Affairs launched a series of 10 tribal listening sessions across Indian Country and Alaska seeking input on how to help. Results of the sessions will shape the agenda at a national comprehensive suicide prevention conference later this year.
A report on those meetings will detail suicide prevention needs, concerns, programs and practices in American Indian and Alaska Native communities, said Rose Weakee, director of behavioral health for IHS.
“We want to see how the pieces come together,” she said in a telephone interview. “One piece is very clear to us — we need to work in partnership with the tribes. Everyone has a role to play in suicide prevention.”
Suicides are not a new problem for IHS, Weakee said. Currently federal funds support 127 tribes through IHS’s Methamphetamine and Suicide Prevention Initiative. Along with domestic violence, those two issues were identified by the tribes as top priorities, she said.
HIS is studying programs that show success and passing them on to other tribes.
The White Mountain Apache, for instance, initiated a program that makes suicide data collection uniform among all agencies and then puts it in a shared data base, she said.
“It will help them get a good sense of what’s going on and why,” Weakee said.
28 livingwell ~ March/April 2011
Gretchen Rubin’s life, on the whole, was sunny - handsome husband, delightful daughters, successful career. Maybe it was the rain, but one April day, though nothing had changed,
she realized she wasn’t as happy as she ought to be. Her epiphany led to a yearlong commitment to try to be happier, culminating in an improved outlook and her book, “The Happiness Project” (HarperCollins, 2009), based on her popular blog of the same title.
But what if her life had been like that day’s weather - all storm clouds and no sun? What if she had lost her job or even her home, and the financial pressures were threatening her marriage?
That’s the reality for a lot of folks these days. Can a happiness project work for them?
It depends on their mindset. “Only 10 percent of our long-term happiness is predicted based on externals. The rest is based on the lens through which we view the world,” says Shawn Achor, CEO of Aspirant, a positive psychology consulting firm based in Cambridge, Mass. “It is harder initially to be happy in down times because of our previous expectations, but in the long run, resilient individuals find ways to see possibilities for growth, even in hard times.”
Only at the extreme lows do external circumstances affect happiness, research has shown. For example, poverty and severe illness breed unhappiness, but unless you’re extremely poor or unhealthy, income and health do not affect happiness as much as might be expected, says
personality and quality-of-life researcher William Fleeson, associate professor of psychology at Wake Forest University, Winston-Salem, N.C.
Research also has shown that some people are just happier by nature. “Genes set our initial baseline of happiness,” Achor says. “But we also know you can change your baseline easily by changing your habits and practicing positive mindset. The key is believing your behavior matters.”
Some behaviors shown to boost happiness include listing three things each day for which you are grateful, journaling about one positive experience each day, exercising four times a week, doing yoga, meditating and performing a daily act of kindness, Achor says.
These behaviors, along with principles set forth by philosophers, religious leaders and the likes of Oprah, were tested by Rubin during her yearlong project.
What surprised her most by its efficacy was the scientific finding that trying new things and taking on challenges generally bring happiness. “I was convinced it wouldn’t work for me because familiarity and mastery make me happy. I eat the same foods every day, I hate to travel, and I find comfort in having a routine,” Rubin says.
She did a complete turnaround, though, when the novelty and challenge of keeping a daily blog brought her so much satisfaction.
Keeping a gratitude journal, however, annoyed her. A person can write down that she’s grateful
Smile Like You Mean It
Maybe money can’t buy happiness, but a little time and effort can turn that frown upside-down
By Dawn Klingensmith/CTW Features

29March/April 2011 ~ livingwell
for aged cheddar cheese, but that observation isn’t necessarily edifying. Rubin concedes that just because the gratitude journal didn’t work for her doesn’t mean it won’t prove useful to someone else.
A happiness project, as defined by Rubin, is a three-stage approach to changing your life. First is the preparation stage, when you identify what engages you and brings you satisfaction and joy and what makes you feel guilty, angry, bored or remorseful. Second is the resolution stage, when you identify concrete actions that will boost your happiness. The third stage is putting those resolutions into practice.
A happiness project assumes people play an active role in creating their own satisfaction and inner peace.
“A lot of people see happiness as something that happens to them - if they are fortunate, good things will happen, and they’ll be happy. But that’s not the whole story,” Fleeson says.
The less passive approach is “scary and exhilarating,” he says. “You have to take responsibility for your own unhappiness, but you also have the power to take control and make changes for the better.”
Fleeson’s research has found that acting extroverted - bolder, livelier, more assertive and more social - makes people happier for the time being, even if they are introverts by nature. Generally, “People were able to act extroverted on demand and reported feeling happier in as little as 10 minutes,” he says.
Fleeson has yet to determine whether practicing extroversion until it becomes habitual will bring about a permanent rise in happiness, though.
In down times, “Probably one of the best things you can do is go out and help someone, even if you don’t feel like you have the energy and that the world has taken something from you,” says Los Angeles psychiatrist Dr. Mark Goulston, editor of the Huffington Post column “The Resilient Life.”
“It helps you gain perspective if the person is worse off than you, and the sincere smile you receive will make you feel better,” he adds.
Plus, “What often makes people unhappy is that deep down, they don’t feel like they deserve to be happy,” Goulston says. But by helping someone or thanking someone who’s provided assistance, you “earn” the right to be happy.
Followers of Rubin’s blog report broader success with certain behaviors. For example, most readers said keeping a one-sentence journal was helpful, but longer-form journals were taxing and time-consuming.
A surprising number of readers reported that simply making the bed was a big help. “When you’re facing down times, taking control of the things you can control is very reassuring,” Rubin says. “They don’t need to be gigantic changes. They can be little things.”
In fact, she says, that’s the whole point. “It’s all about what you can do in a normal day. You don’t have to change your life to change your life.”
“Only 10 percent of our long-term happiness is predicted based on externals. The rest is based on the lens through which we view the world.”
30 livingwell ~ March/April 2011
Valley View EstatesA skilled nursing facility in Hamilton providing 24 hour care, full rehabilitation services and a light care wing for those with minor health issues. The only limited memory program with a secured unit offered in the Bitterroot Valley. Complete with Pearls of Life Signature Memory Care Program.225 North 8th, Hamilton • 363-1144
31March/April 2011 ~ livingwell
NAMINational Alliance On Mental Illness, Missoula Affiliate
Support groups held weekly:· Family and Friends: Thurs 10-noon, Providence Center, 543-3055 NEW! Tues. 6:30 p.m, Providence Center, 552-5494· Recoverers: Call Geri 549-9017 for info.www.namimt.org
Rocky Mountain Surgical SolutionsDr. Timothy B. Richards. Providing all your general surgery needs for Intra-Abdominal Problems: Gallbladder, Cancer, Breast Conditions, Hemorroids and Hernia. 2831 Ft Missoula Rd, Suite 104, Bldg 2, Missoula, MT 59804. 406-728-0285.www.RMSSMontana.com
Rocky Mountain Surgical SolutionsDr. Timothy B. Richards. Regional leader in comprehensive vein care. Board certified surgeon specializing in vein treatment. Offering both VenaCure laser and VNUS RF - Radio Frequency closure treatments for varicose vein conditions. 2831 Ft Missoula Rd, Suite 104, Bldg 2, Missoula, MT 59804. 406-728-0285. www.RMSSMontana.com
32 livingwell ~ March/April 2011
How much sodium
is too much?
By Bev Bennett, CTW Features
To reduce sodium • Read the Nutrition Facts panels, compare products
and select the lowest sodium brands.• Switch from processed food to cooked-from-scratch
dishes.• Opt for frozen vegetables, not canned, which usually
have more added sodium.• Don’t use the salt shaker until after you take your first
bite of food.• Be patient.
“It may take as much as 21 days [for your taste buds to adjust]. After that, you’re tasting the flavor of the food, rather than relying on salt for flavor,” says Lyssie Lakatos, a registered dietitian in New York.
But It Doesn’t Taste Salty!Food doesn’t have to taste “salty” to be high in sodium.
The sodium content of these five foods may surprise you:
Food Sodium1 cup creamed cottage cheese with fruit ... 777 milligrams1/2 cup chocolate puddingmade with 2% milk .................................... 417 milligrams1 (3-ounce) can oil-packsardines, drained ....................................... 430 milligrams1 plain (31/2-inch) bagel ........................... 318 milligrams11/4 cups Rice Krispies ............................. 220 milligrams
Cutting back on sodium doesn’t mean bland and boring.
Here are five fun foods that are low in sodium:
Food Sodium1 cup cheese-flavor popcorn ...................... 98 milligrams1 ounce Swiss cheese ............................... 54 milligrams1 corn tortilla ............................................. 12 milligrams1 (41/2-ounce) piña colada ........................ 8 milligrams1/4 cup raisins ........................................... 4 milligrams
Source: U.S. Department of Agriculture Nutrient Data Laboratory
Montana’s first and only guide to senior housing.
Copies available now at the Missoulian and other participating locations.

AnxietyRecognizing different anxiety conditions
Brain Injury & Post-Traumatic StressProper diagnosis is key to treatment
Mental IllnessIs medical marijuana the right prescription?
A Publication of theMarch/April 2011
INSIDE
Mental HealthRehabilitating the whole person