Embed Size (px)
Citation preview

1
LITHUANIAN UNIVERSITY OF HEALTH SCIENCES
MEDICAL ACADEMY
FACULTY OF PUBLIC HEALTH
DEPARTMENT OF PREVENTIVE MEDICINE
PRASHANTH PRAKASH
QUALITY OF LIFE IN RELATION TO ORTHODONTIC PROBLEMS
AMONG ADOLESCENT CHILDREN
IN THE CITY OF CHENNAI, INDIA.
Master Thesis
Thesis supervisor:
Prof. Dr.Apolinaras Zaborskis
KAUNAS 2014

2
SUMMARY
Quality of life in relation to orthodontic problems among adolescent children in the city of
Chennai, India.
Prashanth Prakash
Academic supervisor, Prof.Dr.Apolinaras Zaborskis, Professor, Department of Preventive
Medicine, Faculty of Public Health, Lithuanian University of Health Sciences.
Kaunas, 2014
AIM: To evaluate the prevalence of orthodontic problems and quality of life in relation to
orthodontic problems among adolescent children in the city of Chennai, India.
OBJECTIVES: To analyze the differences in the need for orthodontic treatment among
children in the public and private schools; to analyze the need for orthodontic treatment among
the various socioeconomic groups; to evaluate the Quality of Life (QoL) among the children; to
analyze the relationship between Quality of Life (QoL) and the need for orthodontic treatment.
METHODS: 200 children participated in the study, out of which 100 were from the private
school and 100 from the public school from the city of Chennai, India. Two sets of
questionnaires were used for the study, one was filled by the children and the other was filled by
the researchers and trained dental assistants after doing a thorough dental examination and
asking questions from the participants. This was carried out according to the recommendations of
WHO oral health assessment. Statistical data was collected, recorded and analyzed using the
software SPSS 17.0 for Windows.
RESULTS: The private school children had more orthodontic problems than the public school
children (49% and 44% respectively). The need for Orthodontic Treatment was the highest in
children under the rich category (56.4%), followed by the children under the poor category
(45.3%) and is least among the children under the average category (44.4%). The Quality of Life
was found to be better among children in private schools than in public schools (90.6% and
89.0% respectively). Children who did not have a good quality of life had little or no need for

3
orthodontic when compared to children who had a good quality of life (60.0% and 53.4%
respectively).
CONCLUSION: Children from the private school who were mostly from the rich socio-
economic group had more orthodontic problems and need for orthodontic treatment. Inspite of
the quality of life being better among children from the private school, they still had a definitive
need for orthodontic treatment. A low quality of life and socio-economic status does not have a
significant impact on the prevalence and need for orthodontic treatment.

4
LIST OF ABBREVIATIONS
IOTN – Index for Orthodontic Treatment Need
QoL – Quality of Life
OHRQol – Oral Health Related Quality of Life
WHO – World Health Organization
SES – Socio-economic ststus
DAI – Dental Aesthetic Index
ICON – Index of Complexity Outcome and Need
AC – Aesthetic Component

5
CONTENTS
INTRODUCTION………………………………………………………………….6
1. AIM AND OBJECTIVES………………………………………………………9
2. REVIEW OF LITERATURE……………………………………………….....10
2.1. Orthodontic problems among adolescent children…………………………..10
2.2. Reasons for orthodontic problems in adolescent children……………..........10
2.3. Different types of orthodontic problems among adolescent children………12
2.4. Quality of Life (QoL)………………………………………………………...13
2.5. Orthodontic oral self-perceptions……………………………………………15
2.6. Index for Orthodontic Treatment Need (IOTN)…………………………….17
3. MATERIALS AND METHODOLOGY……………………………………...18
3.1. Study population……………………………………………………………..18
3.2. Organizing the survey………………………………………………………..18
3.3. Implementing the survey…………………………………………………….19
3.4. Measurement criteria………………………………………………………...20
4. RESULTS AND DISCUSSION……………………………………………....22
4.1. Variables used to record the need for orthodontic treatment
Index for Orthodontic Treatment Need (IOTN)……………………………23
4.2. Difference in the need for orthodontic treatment among
children in public and private schools and among boys and girls ………...25
4.3. The need for orthodontic treatment among
the various socio-economic status groups………………………………….28
4.4. Quality of Life (QoL) among the children…………………………………31
4.5. Relationship between Quality of Life (QoL) and
the Need for Orthodontic Treatment (IOTN)………………………………33
4.6. Binary logistic regression analysis…………………………………………35
CONCLOSION……………………………………………………………...38
PRACTICAL RECOMMENDATIONS…………………………………….39
LIST OF REFERENCES……………………………………………………40
QUESTIONNARIES………………………………………………………..45

6
INTRODUCTION
The oral-facial region is usually an area of significant concern for the individual
because it draws the most attention from other people in interpersonal interactions and is the
primary source of vocal, physical, and emotional communication. Orthodontic anomalies have
been associated with psychosocial distress poor oral health condition and impaired chewing
function and so should be regarded as a health problem. As a result, patients who seek orthodontic
treatment are concerned with improving their appearance and social acceptance often more than
they are with improving their oral function or health. Enhancing these aspects of quality of life is
an important motive for undergoing orthodontic treatment. Oral health can affect the general
health, well-being, education and development of children. In many of the countries, especially
the developing and under developed, a large number of parents and children are unaware of the
causes, occurrence and prevention of most of the common oral diseases. Among the oral diseases,
the most common dental problems in mankind along with dental caries, gingival disease and
dental fluorosis is orthodontic problems and malocclusion (Dhar V et al, 2007). Scientific research
shows that orthodontic anomalies are one of the most common dental pathologies among children
and adolescence as this age group between 12 to 15 years is when the permanent teeth begin to
take its place (after the milk teeth fall) in the jaws it becomes common for the teeth to erupt in an
irregular manner. The main expected benefits of orthodontic treatment relate to improvements
appearance of the teeth and oral functions that will lead to improved psychological and social
well-being. Diagnosis of orthodontic anomalies among children usually implies the detection of
morphologic changes by the dental health professional. However, such an investigation is
relatively expensive, and therefore cheaper alternatives are considered when trying to tackle
orthodontic issues at public health level (Aiste K et al, 2010). Subjective, self-reported oral health
measures are successfully employed in research among adult populations (Jarvinen S et al, 2001;
Jokovic A et al,1997). Such measures are being successfully implemented in research on children
also. Recent studies suggest that age-adjusted questionnaires for children are relatively valid and
proper instruments for evaluation of oral health, demonstrating that 12-year-old children are

7
sufficiently aware about their oral health and its related factors (Gherunpong S et al, 2004).
Information from self-reports by children in the form of questionnaires might help in planning
effective strategies to promote oral health. Questions are usually based on socio-demographics,
self-reports of behavior, knowledge and oral problems and a single-item measuring self-reported
state and satisfaction with appearance of teeth. Several studies have provided evidence that with
the use of schoolchildren’s surveys, valuable information on dental issues including orthodontic
problems, malocclusions, their prevalence, associations with socio-demographic factors, and
potential needs for dental care, could be obtained (Aiste K et al, 2010). Such data are valuable in
planning the needs of treatment of orthodontic pathology, possible workload of orthodontists in
municipalities, and setting priorities for care in sensitive social groups to reduce health
inequalities. According to World Health Organization, the main oral diseases should be subjected
to periodic epidemiological surveys. The epidemiological data on orthodontic treatment need is of
interest for dental public health programs, clinical treatment, screening for treatment priority,
resource planning and third party funding (Brito DI et al, 2009). Appraisal of distribution of
malocclusion and other orthodontic problems in childhood can facilitate efforts to prevent such a
disorder and its consequences and make it possible to reduce the complexity of costly orthodontic
treatment.
In a country like India where inequalities exist within society, there is a clear
demarcation between the various socio-economic groups in aspects such as awareness of health
related issues and attitudes towards seeking treatment for the same due to factors such as financial
stability and quality of life. Also, the availability of the public health facilities for treatment
especially when it comes to dental needs such as orthodontic problems are very scarce and
underdeveloped and hence people have to seek such treatment in the private hospitals which are
dominant and very expensive. Children attending private schools hail from the middle and upper
socio-economic group and those studying in the public schools are from the lower socio-economic
group and hence there is a clear difference between awareness and seeking treatment for
orthodontic problems among these children. This becomes a public health issue as children in the
adolescent age group are more prone to develop orthodontic problems which require them to seek
treatment which involves correction of this problem. Orthodontic treatment is very expensive and
cannot be sought by those from the lower socio-economic group and hence it is very important to

8
evaluate factors such as quality of life, awareness, prevalence and the need for orthodontic
treatment to plan for programs and treatment need for all without any discrimination.
Hence the aim of this study is to find out the existence of orthodontic problems and the
Quality of Life in relation to these orthodontic problems among and the need for orthodontic
treatment among adolescent children in the city of Chennai, India.

9
1. THE AIM AND OBJECTIVES
Aim
The aim of the present study was to ascertain the prevalence of orthodontic problems and quality
of life in relation to orthodontic problems among adolescent children.
Objectives
The main objectives of this study are:
1) To analyze the differences in the need for orthodontic treatment among children in the
public and private schools.
2) To analyze the need for orthodontic treatment among the various socioeconomic groups.
3) To evaluate the Quality of Life (QoL) among the children.
4) To analyze the relationship between Quality of Life (QoL) and the need for orthodontic
treatment.

10
2. REVIEW OF LITERATURE
2.1. Orthodontic problems among adolescent children
Initiation of the adolescent phase in human beings is accompanied by several
physical developmental changes that characterize puberty which are mirrored in a person’s oral
cavity (mouth). This stage in the life of an individual, is a unique time, in terms of dental
considerations, during which, dental caries rates increase from childhood; the first signs of
periodontal disease occur (Casamassimo P et al, 1979); up to a third of facial growth occurs
during a relatively short growth spurt; and the need for orthodontic therapy occurs. These
changes brought about in the adolescent phase
2.2. Reasons for orthodontic problems in adolescent children
Three types of changes which are particularly important are, the transition from
primary to permanent teeth; skeletal and facial growth; and hormonal change. Between the ages
of 10 and 12, a person’s entire set of primary teeth has been replaced with permanent successors,
second permanent molars erupt, and only the third molars remain to develop and erupt (Finn
SB,1973). By ages 12 or 13, an individual’s permanent teeth are usually stable. The face grows
significantly during adolescence, leading to skeletal changes, completing almost all of the
vertical growth that affects tooth position, facial contour, and space available for teeth. During
this phase, it is common to undergo orthodontic treatment (Rarity DM,1980). This is that time in
life of an individual when appearance begins to be important. Children often desire orthodontic
treatment, at this stage as they begin to get conscious about changes in their aesthetic appearance
and their parents perhaps even more so for their child. On the other hand some children, in spite
of obvious facial appearances do not prefer to undergo treatment due to lack of awareness and
access to dental care (in underdeveloped and developing countries) and fear to visit the dentist.
The individual has also reached an age when she or he is considered to have achieved autonomy
and is able to desire or decline orthodontic treatment. Hence, dentists with the patient and the
parents, play the most important role in the decision process. Also, the role of public health
services play an important role in educating the citizens about the importance of orthodontic
treatment.

11
Orthodontics includes the study of the growth and development of the jaws and face
particularly, and the body generally as influencing the position of teeth; the study of action and reaction
of internal and external influences on the development and the prevention and correction of arrested and
perverted development (Milton B et al, 1990).
The benefits of orthodontic treatment are prevention of tissue damage,
improvement in aesthetics and physical function. The uptake of orthodontic treatment is
influenced by the desire to look attractive, self-esteem and self -perception of dental appearance
(Mandeep KB et al, 2012). In every country, there is a need to identify the awareness levels of
children with respect to oral health and the orthodontic treatment as children play an important
role in inculcating healthy lifestyle practices to last for a lifetime. Pre-adolescents and
adolescents would be benefitted with the knowledge about orthodontic treatment since early
orthodontic treatment could be advantageous in preventing further malocclusion complications.
Orthodontic problems which commonly occur in adolescents include: Malocclusion, Crowding
of teeth, Changes in aesthetic appearance and profile. Such orthodontic problems worsen, and
others become apparent later in adolescence (Roopa S et al, 2013).
According to the American Dental Association, Public Dental Health is defined
as the science and art of preventing and controlling dental disease and promoting dental health
through community effort. When public orthodontic care of children and adolescents is
evaluated, especially in developing countries, it is important to take a lot of factors into
consideration. The most important being, education of the individual; awareness of the need for
orthodontic treatment; socio-economic status; the availability and access to dental services;
parents education level, income and awareness about the importance of dental care for their
children; scarcity of dental services especially in rural areas; lack of public health services,
facilities and personnel; lack of sources and interventions to seek a knowing about such
problems. Hence it becomes important to study both the changes in orthodontic services as such
and the perspective of the entire dental health care in a public health point of view.

12
2.3. Different types of orthodontic problems among adolescent children
Malocclusion is the malpositioning of maxillary (upper jaw bone) and
mandibular (lower jaw bone) teeth, a condition that can have both esthetic, functional, and
emotional implications on an individual. Malocclusion is not a disease, but a morphological
variation which may or may not be associated with a pathological condition (Nashashibi S et al,
1983). Pain and miseries are seldom acute in malocclusion and has a greater impact on society
and individual in terms of quality of life, discomfort, social and functional limitations.( Ansai T
et al,1993; Mclain JB et al,1985). The reasons to develop malocclusion could be genetic or
environmental and/or combination of both the factors along with various local factors such as
adverse oral habits, tooth anomalies, form and developmental position of teeth can cause
malocclusion. (Miitchell L et al, 2001). Data from the World Health Organization show that
malocclusion is the third most important condition in the ranking of oral health problems,
outranked only by caries and periodontal disease (Mausner JS et al, 1985). Several studies have
evaluated the prevalence of malocclusion in various populations and have reported different
prevalence rates (39-98%). Prevalence of malocclusion varies from country to country and
among different age and sex group. The prevalence of malocclusion in India varies from 20% -
43%.
(Sureshbabu AM et al, 2005). In such a diverse and vast country like India, a large
variation in prevalence of malocclusion exists in varying regions of the country. This can be due
to variations in ethnicity, nutritional status, religious beliefs, and dietary habits (Kharbanda OP et
al, 1991). There is a definite ethnic trend in the prevalence of the type of malocclusion in India
from north to south of India. The prevalence of malocclusion in southern India is about 5%, and
is much lower compared to the north which is 10—15% in. In addition, the southern population
has an ethnic affinity for bimaxillary protrusion (Kharbanda OP, 2009).
Studies on the prevalence of malocclusion in public health provide important
epidemiological data to assess the type and distribution of occlusal characteristics of a given
population, its treatment need and priority and the resources required to offer treatment. It is
essential to identify and localize the wide range of deviations from occlusal development that
may arise and that must be intercepted before the end of the active growth stage. As well as
problems of a functional nature that arise from these morphological changes, which may become
more complex skeletal problems in the future, aesthetic impairment often occurs, with serious
psychosocial consequences for the developing individual. Assessment of malocclusion and

13
treatment needs for public health purposes are instrumental in determining the priorities for
treatment in publicly subsidized dental services and to properly estimate the number of
professionals to be recruited as well as the financial resources necessary to provide this treatment
(Marcos AVB et al, 2010). The recognition of malocclusion as an important problem in the
public dental health services for children implies a need for rational planning of preventive and
therapeutic orthodontic measures. It is necessary to carry out epidemiologic studies of
malocclusion in groups of boys and girls at various stages of development and from different
socio-economic groups and geographic areas. Analysis of the prevalence rates of malocclusion in
such groups may also contribute to an understanding of the causes of malocclusion (Helm S,
1968). In a developing country like India, malocclusion is still not considered to be a dental
problem because more priority is given to the treatment of dental caries and periodontal diseases
due to pain experienced by them. Most malocclusion cases are still not treated properly due to
ignorance of patients, parents, inadequacy of resources, lack of knowledge about malocclusion
and other influencing factors like literacy rate and socio-economic status. The level of dental
health knowledge, positive dental health attitude, and dental health behavior are interlinked and
associated with the level of education and income.
Malocclusion results in various problems in the affected individuals, including lack of
satisfaction with facial appearance, problems associated with the function of the masticatory
system, dysfunction of the temporomandibular joint, problems with swallowing and speech,
susceptibility to facial traumatic injuries and development of caries and periodontal problems
(Proffit WR et al, 2007). In addition, the individuals with malocclusion will not be satisfied with
their facial appearance, resulting in inappropriate social responses and development of emotional
and mental problems. In other words, Oral Health-Related Quality of Life is disturbed in a large
proportion of affected individuals (Azuma SH et al, 2008).
2.4. Quality of Life (QoL)
The quality of life is defined as a subjective judgment of an individual of his/her health
status and in fact satisfaction or dissatisfaction with specific aspects of life, which are important
for the individual (Kok VY et al, 2004). Disturbances in the normal somatic, psychosomatic and
social functioning of individuals are considered important considerations in the evaluation of oral
health. QoL is a somewhat intangible entity and there has been much debate as to how to define

14
it. QoL reflects physical, social, and psychologic functioning, Inability of commonly used tools
to evaluate and quantify oral health, such as evaluation of the ability of patients to chew food and
enjoy the taste of food items, has resulted in a new direction and attitude toward evaluation of
oral health by new quantification tools such as OHQoL.
Oral Health Related Quality of Life (OHRQoL) has important implications for clinical
practice in dentistry and dental research. OHRQoL is an integral part of general health and well-
being and is recognized by the WHO as an important segment of the Global Oral Health Program
(WHO, 2003). This concept of health status embraces the biopsychosocial model of health into
which symptoms, physical functioning, emotional and social well-being are incorporated
(Kleinman, 1988). Quality of life (QoL), or individuals’ “perceptions of their position in life in
the context of culture and value systems in which they live, and in relation to their goals,
expectations, standards, and concerns” (WHOQOL, 1995), is now recognized as a valid
parameter in patient assessment in nearly every area of physical and mental healthcare, including
oral health. Further, the opportunity arose to consider how oral health affects aspects of social
life, including self-esteem, social interaction, school and job performance, etc, all of which are
parameters to access the Quality of Life of an individual. Researchers began to postulate how
oral health is related to health-related quality of life (HRQoL) (Gift and Atchison, 1995) and to
understand the interrelationships between and among traditional clinical variables (like
diagnosis), data from clinical examinations, and person-centered, self-reported health experience.
With increasing focus of health policy to address health promotion and disease prevention,
HRQoL and OHRQoL have come to incorporate both positive and negative perceptions of oral
health and health outcomes (Broder and Wilson-Genderson, 2007). Thus, assessments of oral
health can reflect both negative impact and enhancement of self and well-being. For example,
people may seek oral healthcare for preventive (e.g., cleanings) or elective (e.g., orthodontics)
treatment.
Assessment of OHRQoL allows for a shift from traditional medical/dental criteria to
assessment and care that focus on a person’s social and emotional experience and physical
functioning in defining appropriate treatment goals and outcomes (Christie et al., 1993).
Finally, OHRQoL is important because of its implications for oral health disparities and access
to care. Unfortunately, socioeconomic and racial/ethnic oral health disparities constitute a major
social problem (Petersen et al., 2005). Health disparities can be explained, in part, by limited

15
access to care. Locations within developing countries may have minimal dental health
professionals, and rural areas often lack facilities offering dental services. In developed
countries, treatment access is limited by high costs and sometimes by transportation difficulties
(Sisson, 2007). OHRQoL can be useful in measuring the impact of oral health disparities on
overall health and QoL.
OHRQoL is utilized in health services research to examine trends in oral health and
population-based needs assessment. Epidemiological survey research has examined trends in
OHRQoL (e.g., dental caries, orthodontic treatment etc), identified individual and environmental
characteristics that affect OHRQoL (e.g., income, education, etc.), and aided in needs assessment
and health planning for population-based policy initiatives. OHRQoL has a multitude of
substantive applications for the field of dentistry, healthcare, and dental research as we move
from bench to applied science and person-centered approaches to measure treatment needs and
efficacy of care. Patient-oriented outcomes like OHRQoL will enhance our understanding of the
relationship between oral health and general health and demonstrate to clinical researchers and
practitioners that improving the quality of a patient’s well-being goes beyond simply treating
dental maladies. OHRQoL research can be used to inform public policy and help eradicate oral
health disparities (Sischo L and Bordre HL, 2011).
2.5. Orthodontic oral self-perceptions
A variety of social, cultural, psychological and personal factors influences the
perception of dental appearance (Graber LW et al, 1980). Dissatisfaction with dental appearance
is the main factor associated to the decision to undergo orthodontic treatment (Bos et al., 2003).
It has been estimated that 80% of orthodontic patients seek services out of a concern for
aesthetics rather than for reasons related to health or function (Albino et al., 1981). Thus, an
individual’s self-perceived dental aesthetics affects normative assessments regarding the need for
orthodontic treatment (de Oliveira et al, 2004). Malocclusion has an impact on the quality of life
among school children because of which the aesthetic facial appearance may be altered, hence
such children have a negative self-perception on their aesthetic appearance and perceive the need
for orthodontic treatment. A number of authors have suggested that children especially teenagers
have developed a perceptual awareness towards their facial appearance and oral health. Facial
appearance has shown to have a major impact on the psychological well-being of an individual.

16
People vary in their perceptions of their physical self and have emotional reactions to these
perceptions (Pertschuk et al,1982). In determining the potential benefits of orthodontic treatment
for an individual, the relation between physical appearance of an aesthetic deviation and the
impact of such a deviation on self esteem and body image are important factors (Birkeland et al,
2000).The assessment of potential benefits of orthodontic treatment to the individual should
include greater awareness towards the individuals psychosocial functioning and the patients own
perspective on the need for orthodontic treatment. Some studies showed that, children with less
perceptual awareness tend to be dissatisfied with their dental appearance and showed a greater
need for orthodontic treatment. Some other studies showed opposite perception levels. Hence it
can be drawn to a conclusion that whilst people seemed to be more aware of their orthodontic
problems they did not perceive a need for orthodontic treatment to the same extent as the
orthodontist. Despite the patients awareness level, the dentist or orthodontist’s was seen to have a
more critical view to consider whether treatment was needed. In a study among both adolescents
and young adults, only 50–65 percent of those normatively assessed as in need of orthodontic
treatment actually perceived such a need (Koochek et al, 2001). And these figures were nearly
identical to those derived from studies of orthognathic surgery patients, in which 50–60 percent
of those clinically assessed as requiring treatment reported that they perceived such a need for
treatment (Bell R et al, 1985).
A variety of social, economic, and cultural factors like, esthetic judgment, income,
and availability of providers, may influence personal perception of the need for orthodontic
treatment (N’Gom et al, 2005). However, in developing countries, public healthcare services do
not offer orthodontic treatment, making it inaccessible to a large proportion of the population
who fall under the lower socioeconomic strata as they cannot afford expensive treatment in a
private dental clinic and also lack of awareness which the public health services do not provide .
In such a situation, not much is known regarding the effects of malocclusion on social and
psychological wellbeing among individuals who cannot enjoy the benefits of orthodontic
treatment and how such individuals perceive aesthetic alterations arising from malocclusion.
Thus, it is important to gain a better understanding of the biopsychosocial aspects of
malocclusion and its effect on quality of life among such individuals, addressing the issue as a
public health problem. Information in this regard would favor a better assessment of treatment

17
needs and priorities as well as allowing a better planning of the resources needed to offer the
population access to orthodontic treatment (Marques LS et al, 2009).
2.6. Index for Orthodontic Treatment Need (IOTN)
Orthodontic research has traditionally focused on “hard clinician-driven outcome
measures at the expense of subjective patient-driven measures”. Based on this a number of
orthodontic need indices, such as the Dental Aesthetic Index (DAI), the Index of Orthodontic
Need (IOTN), and the Index of Complexity Outcome and Need (ICON), have been developed
and used for assessing orthodontic treatment need (Georgios Tsakos, 2008). Majority of these
indices assess not only severity of dental occlusion but also include evaluation of the aesthetics.
The aesthetic component of the indices is more subjective and less readily measurable than the
morphological characteristics. The subjectivity of indices used to record orthodontic anomalies,
their questionable validity and reliability may contribute to inconsistency of results. An
alternative approach to the use of indices is a registration of measurable occlusal characteristics
such as overjet, overbite, crowding, crossbite (Antanas S; Kristina L, 2009).
The Index of Orthodontic Treatment Need (IOTN), described by Brook and Shaw
(1989) has been gaining national and international recognition as a method of objectively
assessing treatment need. The IOTN is employed to determine the normative need in the
population .This index ranks malocclusion in terms of the significance of various occlusal traits
for the person's dental health and perceived aesthetic impairment with the intention of identifying
those persons who would be most likely to benefit from orthodontic treatment. The Aesthetic
Component (AC) of this indicator is recorded by visual clinical examination and photographs.
This indicator shows the different levels of dental attractiveness from the scale of 1 to 10, with 1
being the most attractive and 10 the least attractive, according the arrangement of teeth. The
principle is that any individual can be identified and rated according to this scale.
The Dental Health Component of this indicator categorizes the detrimental effects of
the various occlusal traits like overcrowding of teeth, gap between the teeth, problems in
occlusion etc, in order of severity. All these occlusal traits have to be examined clinically and
recorded separately. This component was developed to ensure validity and consistency in
reporting the need for orthodontic treatment.

18
MATERIALS AND METHODOLOGY
3.1. Study population.
The survey was conducted in the city of Chennai, India. A total of 200 children
participated in the survey between the age groups of 13 to 14 years. In each of these age groups
an attempt was made to include equal number of male and female subjects. Out of these 200
children, 100 were from the private school which is situated in the city and 100 were from the
public school which is located in the suburbs. The schools were selected based on the socio-
economic status. Children belonging to the low socio-economic groups were those studying in
the public school and the high socio-economic group comprised of children studying in private
school. The consent for examining of the children was obtained from the respective head master.
The criteria for selection of the study subjects were that the children should be permanent
residents of Chennai and should be full time students enrolled in the school.
Depending on the conditions of the school, the exact arrangement for conducting the
examination was determined. The subjects were examined on an upright chair in adequate
natural light. A torch light was used to examine the oral cavity (mouth). Examination of the child
was done by only one examiner to avoid inter-examiner variability. Recording of data was done
by a two trained dental assistants who assisted throughout the study. Prior to the examination for
orthodontic problems and dental caries, a questionnaire was filled by the subject to find out the
personal data and oral hygiene habits. Tooth surface was dried and examination of the oral cavity
was made using a dental mouth mirror, and dental probe.
Calibration procedures were performed prior to and during the study to ensure that a
consistent standard of the diagnosis was maintained. Re-examinations were carried out on
approximately one in ten children selected at random to have a constant check on the inter
examiner variability. The data was recorded on a performa and were entered into a computer.
3.2. Organizing the survey
3.2.1. Obtaining ethical clearance and permission from the concerned authorities. The
ethical clearance for the present study was obtained from the Lithuanian university of health
science, Kaunas Lithuania, The Dental council of India and the Principals of the public and

19
private schools. The required official permission for the study was obtained from Health &
Family Welfare Office of Chennai Tamil nadu and local medical officers of Primary Health
Centers and Sub-centers. For examination of children in the rural areas, co-operation and oral
consent was taken from school principle heads.
3.2.2. Scheduling. The present study was conducted from June 2013 to August 2013. A detailed
monthly schedule of the survey was prepared well in advance and the concerned authorities were
informed regarding examination place, date and timings. On an average 20 subjects were
interviewed and examined on each day. Examination of each individual took approximately 8-
10minutes.
3.3. Implementing the survey
3.3.1. Informed consent. Consent from each study subject was taken after explaining the
nature of the study.
3.3.2. Data collection. The data included questions related to socio-demographic characteristics,
oral hygiene practices, adverse oral habits, some other habits like brushing teeth, frequency of
dental visits etc.
3.3.3. Armamentarium. The following instruments and supplies were used for the study:
1) Plane dental mouth mirrors
2) Dental Explorers.
3) Dental Tweezers
4) Containers
5) Surgical scrub
6) Disposable tumblers
7) Chemical disinfectants
8) Towels
9) Gauze
10) Gloves and Mouth Masks
11) Survey Proforma
Adequate number of sterilized instruments was made available during the survey and
current recommendations and standards were followed for infection control.

20
3.4. Measurements and criteria:
Table 1: Distribution between the number and percentage among gender, school and socio-
economic status:
N %
Gender
Boys 112 56.0
Girls 88 44.0
School
Private 100 50.0
Public 100 50.0
Table 1, shows that 100 (50.0%) children from the public school and 100 (50.0%)
from the private school participated in the study, out of which, 112 (56.0%) boys and 88 (44.0%)
were girls. Out of the 200 children who took part in the study, 86 (43.0%) were from the poor
socio-economic group, 72 (36.0%) were from the average and 37 (18.5%) were fro the rich
socio-economic group.
Orthodontic problems such as aesthetic component, crowding, spacing between the
teeth, cross-bite, open incisor bite, incisal overlap, upper and lower posterior teeth ratio of the
sagittal direction (right and left). All the above variables were included in a new variable called
Index for Orthodontic Treatment (IOTN).
Socio-economic
status
Poor 86 43.0
Average 72 36.0
Rich 37 18.5
Missing 5 2.5

21
Factors such as car, bedroom, holiday, family, father’s and mother’s job was
included in socio-economic determinants and were recorded using self administered
questionnaires.
We have chosen to record the general quality of life to assess the impact of
orthodontic problems and treatment procedures on the satisfaction in life, happiness level and
health status according to their assessment. Factors such as health, happy and life were
considered in Quality of Life and these factors were sub categorized into ‘High’ (excellent, very
good and good) and was indicated with the score “0” and ‘Low’ (fair and poor) was indicated
with score “1”. This was recorded using self administered questionnaires.
Orthodontic problems were grouped under Index for Orthodontic Treatment Need
and were grouped as follows: Index for Orthodontic Treatment (IOTN) which was categorized
into ‘No or Little need for treatment’ (<7) and ‘Definitive need for treatment’ ( >7) groups.
Variables such as aesthetic component, crowding and spacing between teeth, cross bite, open
incisor bite and incisor overlay, upper and lower posterior teeth saggital ratio of the right and left
side were recorded for each subject to evaluate the necessity for the need of orthodontic
treatment.
3.5. Statistical analysis:
The data collected was analyzed using Statistical Package for Social Sciences for
Windows, version 17 (SPSS Inc., Chicago, IL). Descriptive statistics (mean, proportion, standard
deviation) were used to describe the characteristics of the sample. The chi-square test was used
to explore the relationship between orthodontic problems and socio-economic status .The
statistical significance was considered as P ≤ 0.05.

22
4. RESULTS AND DISCUSSION
This cross sectional study was conducted to assess the prevalence of orthodontic
problems and the orthodontic treatment need using the Index for Orthodontic Treatment Need
(IOTN) among 13 to 15 years old school children of Chennai city, India. In this event, 200
children were selected, out of which 100 belonged to the private school and 100 were from the
public school. 112 boys and 88 girls were examined in this study. The reason for selecting the
two categories of schools are because children from the lower socio-economic strata attend the
public schools which are mostly located in the suburban areas and children attending the private
schools were from the higher socio-economic strata which are located within the city. Children
in the city would be more exposed to a varied lifestyles and would be more aware in terms of
dental health and the need for treatment as compared to children who live in the suburbs. In this
way it was easy to make a clear association between socio-economic status and orthodontic
problems including the need for treatment. This is in agreement with similar studies which were
conducted in India (Tak M et al, 2013). The present study was conducted among 12 years and 15
years age group as both the age groups are the index age group of pathfinder survey as per WHO
Basic Oral Health Survey method. The 12 years age group was selected because this age is
considered as a global monitoring age for caries for international comparisons and monitoring of
disease trends. The 15 years age group was selected because at this age, the permanent teeth have
been exposed to the oral environment for 3-9 years. This age is also important for the assessment
of periodontal disease indicators in adolescents (WHO,1999). The present study seek to advocate
the need to include an orthodontic focus in the public dental health services. In the studies of
prevalence of orthodontic problems, one should always choose a well-defined sample, subjects
with no prior history of orthodontic treatment and objective data collection (Thilander B et al,
2001). The present study could not fulfill such criteria as the sample size was very small. To
calculate the difference in orthodontic problems among children in public and private schools,
the Index for Orthodontic Treatment Need (IOTN) was used.

23
4.1.Variables used to record the need for orthodontic treatment – Index for
Orthodontic Treatment Need (IOTN)
According to the IOTN index it is necessary to record variables such as aesthetic
component, crowding and spacing between teeth, cross bite, open incisor bite and incisor
overlay, upper and lower posterior teeth saggital ratio of the right and left side for each subject to
evaluate the necessity for the need of orthodontic treatment.
Table 2. Index for orthodontic treatment need (IOTN) variables
According to table 2, the difference between boys and girls when it came to the variables such as
aesthetic component, cross bite, open incisor bite and incisor overlay showed statistically
significant results. 40.7% of boys and 67.8% girls showed crowding and spacing between their
IOTN
COMPONENT
GENDER TOTAL
(N%)
P VALUE
Boys (N%) Girls (N%)
Aesthetic
component
1 (0.9) 1 (1.1) 2 (1.0) < .005
Crowding and
spacing between
teeth
46 (40.7) 59 (67.8) 105 (52.5) .852
Cross bite 17 (15.0) 3 (3.4) 20 (10.0) < .001
Open incisor bite 20 (17.7) 11 (12.6) 31 (15.5) .007
Upper posterior
teeth saggital
ratio right side
and Lower
posterior teeth
saggital ratio left
side
29 (25.7) 13 (14.9) 42 (21.0) .327

24
teeth, the difference was not statistically significant. 25.7% of boys and 14.9% of girls showed a
saggital ratio difference between the posterior teeth but the difference was not statistically
significant.
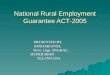
Figure 1: Differences among the IOTN variables between boys and girls.
Figure 1 shows most of the orthodontic problems to be related to crowding and
spacing which were more among girls (67.8%) than boys (40.7%).
Many studies which have evaluated the need for orthodontic treatment among school
children have used the IOTN index for Orthodontic Treatment Need (Col Prassana Kumar et al,
2012; Nicky A. Mandall et al, 2005).
The IOTN has been gaining international recognition as a method of objectively
assessing treatment need (Neslihan U and Esra E, 2001). Comparing all the orthodontic indices,
it was found that IOTN was a reliable and user friendly index, which can be used for orthodontic
surveys (Col Prasanna Kumar et al, 2013).
0.9%
40.7%
15% 17.7% 25.7%
1.1%
67.8%
3.4%
12.6% 14.9%
Aesthetic component
crowding and spacing
cross bite open incisorbite and incisor
overlay
upper and lower teeth sagittak ratio rightside and left side
Boys Girls

25
4.2. Difference in the need for orthodontic treatment among children in public and private
schools and among boys and girls
The need for orthodontic treatment was analyzed between children from the private
and public school and among boys and girls using the Index for Orthodontic Treatment Need
(IOTN). A total of 200 children were examined out of which 100 were from the private school
and 100 were from the public school. 113 boys and 87 girls were examined.
Table 3. Distribution in the need for orthodontic treatment among school type and gender
Table 3 shows that out of the 100 children examined in the public school, it was found
that 56.0% were healthy and had no orthodontic problems that needed treatment, while 44.0%
had orthodontic problems and needed treatment. Out of the 100 children examined in the private
school, it is found that 51.0% were healthy and did not have any orthodontic problems that
needed treatment, while 49.0% had orthodontic problems and needed treatment. Hence in this
study, it is observed that children in the private school had more orthodontic problems than those
in the public school. However the difference was not statistically significant.
Out of the 200 participants in both the public and private schools, 69.0% of the girls
did not have any orthodontic problems and 31.0% had orthodontic problems. 41.6% of boys did
not have any orthodontic problems and 58.4% had orthodontic problems. Boys had more
orthodontic problems than girls. The difference was statistically significant.
TOTAL
IOTN
P
VALUE
No or little
need (N%)
Definitive
need (N%)
SCHOOL Private 100 51 (51.0) 49 (49.0) .285
Public 100 56 (56.0) 44 (44.0)
GENDER Boys 113 47 (41.6) 66 (58.4) < .001
Girls 87 60 (69.0) 27 (31.0)

26
Figure 2: Differences in the need for orthodontic treatment among the private and public
school
Figure 2 shows that the children from the private school had a definitive need for orthodontic
treatment (49%) when compared to the public school (44%).
Figure 3: Differences in the need for orthodontic treatment among boys and girl
51%
56%
49%
44%
Private Public
No or little need Definitive need
41.6%
58.4%
69%
31%
No or little need Definitive need
Boys Girls

27
Figure 3, shows that the boys had a definitive need for orthodontic treatment
(58.4%) when compared to girls (31%).
Literature comparing the Need for Orthodontic Treatment among public and
private school children in India, is very limited as this differentiation is made to bring about the
differences in socio-economic status. However there is a lot of literature among gender
differences and the need for orthodontic treatment. The distribution with respect to males and
females for orthodontic treatment need has been studied by several researchers. Hedayati and
co-workers showed more findings of need for orthodontic treatment in males than females in
Iranian children (Hedayati et al, 2007). Sanjeev S and his colleagues, also found that the
difference between the IOTN values among boys and girls indicated that boys represented more
need to treatment than girls but the difference was not statistically significant (Sanjeev S et al,
2007). Burden and co-workers, in their study used the IOTN index and found that significantly
more males were in need of orthodontic treatment than females (Burden et al, 1994). These
findings were in line with the present study. The reason why girls had lesser need for orthodontic
treatment in our study when compared to boys may be because they gave more importance to
their dental aesthetic appearance and took care of their teeth well. In a study by Shaw et al
(1991), they found that the parents pay more attention to girls than boys concerning dental
aesthetics.
Neus Puertes-Fernández and co-workers, in their epidemiological study
conducted in West Saharan school children found that there was no significant difference
between the need for orthodontic treatment and gender among children (Neus Puertes et al,
2010). Also, a study done by Venkatesh B and his co-worker showed no correlation with the
treatment needs and gender of (Venkatesh B and Gopu H, 2011). Another study done by Aiste
Kavaliauskine and co-workers, demonstrated that girls reported orthodontic problems more often
than boys (Aiste K et al, 2010). The findings of these studies were in contradiction with the
present study.
Generally in majority of the studies, when interpreting results, it was noted that
in the study population, none of the children had been orthodontically treated. In most
epidemiological studies, individuals with a previous or current history of orthodontic treatment
were systematically excluded from the sample (Barnabe E et al, 2006; Seema D et al, 2013). Our
study did not have this exclusion criteria, as the study population included children who have

28
previously undergone, undergoing and not undergone orthodontic treatment. Children who were
undergoing or had already undergone orthodontic treatment were considered as those not having
a need for treatment.
Most of the studies have been performed by selecting schools randomly and
examining its children, hence results interpreted are in general representing the entire study
population. But in the present study we have included two categories of schools and
differentiated the need for treatment based on the IOTN index.
The existence of orthodontic problems with orthodontic treatment need and the
perception of such need by the children reinforce the importance of including orthodontic
treatment in public health policies. Such inclusion assumes adequate resource allocation, better
use of human resources and professional creativity, and institutional liaison between public and
private institutions.
4.3. The need for orthodontic treatment among the various socio-economic status groups
According to the socio-economic status, the children from both the public and
private schools were divided into three categories: poor, average and rich.
Table 4. Index for Orthodontic Treatment Need among the various socio-economic groups
Socio-economic
status - SES
(Scores)
Total (N%)
IOTN groups
P value No or little
need (N%)
Definitive need
(N%)
Poor (0-1) 86 (44.1) 47 (54.7) 39 (45.3)
0.429
Average (2-4) 72 (36.9) 40 (55.6) 32 (44.4)
Rich (5-7) 37 (19.0) 16 (43.2) 21 (56.8)

29
According to table4, 43.2% of children under the rich category did not need orthodontic
treatment and 56.8% needed orthodontic treatment. 55.6% of children under the average
category do not need orthodontic treatment and 44.4% needed orthodontic treatment. 54.7% of
children under the poor category needed orthodontic treatment and 45.3% do not need
orthodontic treatment. However the difference was not statistically significant.
Figure 4: The need for orthodontic treatment among the various socio-economic groups.
According to figure 4, the need for orthodontic treatment is the highest in children
under the rich category (56.4%), followed by the children under the poor category (45.3%) and is
least among the children under the average category (44.4%).
Some studies have demonstrated that the need for orthodontic treatment (IOTN)
did not significantly differ between subjects from different areas of living or socioeconomic
backgrounds (Heidi Kerosuo et al, 2004; Ruhi Nalcaci et al, 2012). Other studies have revealed
that the need for orthodontic treatment was greater among the deprived or lower socio-economic
54.7% 55.6%
43.2% 45.3% 44.4%
56.8%
Poor Average Rich
No or little need Definitive need

30
status group (Tickle M et al, 1999; Prabu D et al, 2008). In the present study, children from the
average socio-economic group had no need for orthodontic treatment followed by the low socio-
economic group. Children from the higher or rich socio-economic group had a definitive need
for orthodontic treatment. The reason for this may be due to the easy availability and
consumption of unhealthy diet and junk food among the children residing in the cities who study
in the private school and hail from the higher socio-economic group. Since they consume more
junk foods in an early stage, they are more prone to the development of dental caries resulting in
the early loss of deciduous teeth and subsequent drifting and crowding of the permanent teeth
when they erupt.
When it comes to creating an awareness and planning of public health programs,
more importance is given to targeting the lower socio-economic group, but according to the
findings of the present study, importance should also be given to children from the higher socio-
economic group.

31
4.4. Quality of Life (QoL) among the children
The Quality of Life was analyzed among boys and girls and among the private and
public schools.
Table 5: Distribution of Quality of Life among school type and gender
Table 5, shows that the Quality of Life (QoL) is higher for girls (98.4%) when compared
to boys (86.4%). However, the difference is not statistically significant. The Quality of Life
(QoL) is higher among children in private schools (90.6%) than in public schools (89.0).
However the difference is not statistically significant.
Quality of Life (QoL)
P value
Gender
High
(N%)
Low
(N%)
Boys 95 (86.4) 15 (13.6)
0.05
Girls 81 (94.2) 5 (5.8)
School
0.44 Private 87 (90.6) 9 (9.4)
Public 89 (89.0) 11 (11.0)

32
Figure 5: Quality of Life (QoL) among gender and school.
Figure 5 shows that the Quality of Life (QoL) is higher for girls and among children
in private schools.
Studies done by Abu A et al and Kok YV et al have also shown similar results, with
no statistical significance. In a study done by Navabi et al, they observed no significant
relationship between gender and QoL in the subjects (Navabi N et al, 2012). de Oliveria and
Sheiham reported that sex significantly affects the impact of orthodontic problems on QOL, and
women were 1.22 times more likely to have an impact than men. They have concluded that,
gender differences cannot be considered as predicting factors for QoL (de Oliveira CM and
Sheiham A 2004).
One study has evaluated the Quality of Life among Sudanese school children
attending the public and private school and have found that children from the private schools had
a better quality of life compared to children attending the public school (Nazik MN et al,2010).
Girls seemed to exhibit a better general quality of life as they may seem to be more
happier and take care of their health and well being when compared to boys. The quality of life
seemed to be better in private schools as most of them hail from the higher socio-economic status
group, their parents are well educated and are financially sound and they seemed to have a better
lifestyle when compared to children from public schools who hail from the lower socio-
86.4%
94.2% 90.6% 89%
13.65
5.8% 9.4% 11%
Boys Girls Private Public
Quality of life -high Quality of life -Low

33
economic group who comparatively do not have a better lifestyle. Hence quality of life is a very
important factor when it comes to conducting public health programs, as more focus should be
given to improving the quality of life and health situation, aiming at providing free health care.
4.5. Relationship between Quality of Life (QoL) and the Need for Orthodontic Treatment
(IOTN)
The association between quality of life and the need for orthodontic treatment has
been shown. Children who have a good quality of life have been recorded as high and those
having a poor quality of life have been recorded as low.
Table 6: Association between Quality of Life and Need for Orthodontic Treatment
QoL
IOTN
P value No or little
need
Definitive
need
High 94 (53.4) 82 (46.6)
0.375 Low 12 (60.0) 8 (40.0)
In table 6, children who did not have a good quality of life, had little or no need for
orthodontic treatment (60%), when compared to children who had a good quality of life (53.4%).
Whereas children who had a good quality of life had a definitive need for orthodontic treatment
(46.6%) when compared to those who did not have a good quality of life (40.0%). However, the
difference was not statistically significant.

34
Figure 6: Association between quality of life and the need for orthodontic treatment
Most of the studies have shown that, children who had a need for orthodontic
treatment had a significantly worse Qol score compared to those who did not need treatment
(O’Brien et al, 1998; Mandall N et al, 2001; Fox D et al, 2000; Kok YV et al, 2000). Study done
by Navabi et al (2012), have shown an improvement in function and appearance of the child and
an improvement in quality of life who had previously undergone orthodontic treatment. In
contrast, Taylor believes despite the fact that orthodontic treatment improves appearance, oral
functions and the social health of the patients, it does not seem to exert a significant influence on
their general quality of life (Taylor et al, 2009).
It has long been recognized that people seek and undergo orthodontic treatment not
because of the anatomic irregularities or to prevent the destruction of tissue within the oral
cavity, but because of the consequences of the aesthetic impairment caused by orthodontic
problems and malocclusion. Thus, malocclusion and orthodontic care have become a quality-of-
life (QoL) issue. Some studies have shown that self-consciousness and embarrassment and the
general feeling of less satisfaction in life were significantly associated with higher orthodontic
treatment need in both males and females. On the other hand it did not affect the ability of the
patient to do their job or function effectively. Therefore it may be assumed that patients with
53.4%
60%
46.6%
40%
Quality of life-High Quality of life-Low
No or little need Definitive need

35
orthodontic problems may suffer from aesthetic and social problems which is related to quality
of life rather than impairment of daily activities.
4.6. Binary logistic regression analysis:
Table 7: Socio-Economic Status, School, Quality of Life and Index for Orthodontic
Treatment.
N% Crude model
Odds ratio (CI)
Adjusted model
Odds ratio (CI)
GENDER:
Girls
Boys
87
113
Ref
3.12(1.73-5.62)
Ref
1.83(0.04-77.76)
SCHOOL:
Private
Public
99
99
Ref
0.81(0.46-1.42)
Ref
0.85(0.34-2.09)
SOCIO-ECONOMIC STATUS:
Poor
Average
Rich
86
72
37
Ref
0.63(0.29-1.37)
0.61(0.27-1.35)
Ref
0.91(0.38-2.20)
1.07(0.33-3.43)
QUALITY OF LIFE (QoL):
High
Low
176
20
Ref
0.76(0.29-1.96)
Ref
0.55(0.20-1.50)
The relative risk of the need for orthodontic treatment adjusted for confounding is
estimated for the various categories of gender, school type, socio-economic status and quality of
life.
The evaluation of socio-economic status revealed insignificant differences among the
subgroups in low, average, and rich categories, 45.3%, 44.40%, and 56.8% of schoolchildren,
respectively, reported for the need for orthodontic treatment ( df=1;P=0.429). However, children
from the rich socio-economic status group, reported a definitive need for orthodontic treatment

36
when compared to the average and poor groups .The relative risk of the need for orthodontic
treatment is calculated for the average and rich socio-economic group, keeping the poor socio-
economic group as reference category. No elevation in risk is observed in the average group.
The relative risk is 0.91(0.38-2.20). However, there is a slight elevation in risk for the rich socio-
economic group. The relative risk is 1.07(0.33-3.43).
The evaluation for gender revealed significant differences among boys and girls, 58.4%
and 31.0% of boys and girls, respectively, reported for the need for orthodontic treatment ( df=1;
P<0.001). Boys reported a definitive need for orthodontic treatment when compared to girls. The
relative risk of the need for orthodontic treatment is calculated for girls keeping boys as the
reference category. No elevation in the risk is observed. The relative risk is 0.32(0.17-0.59).
The evaluation for school type revealed insignificant differences among private and public
schools, 49.0% and 44.0% of private and public school children, respectively, reported for the
need for orthodontic treatment ( df=1; P=0.285). Private school children reported a definitive
need for orthodontic treatment when compared to public school children. The relative risk of the
need for orthodontic treatment is calculated for public school keeping private school as the
reference category. No elevation in the risk is observed. The relative risk is 0.85(0.34-2.09).
The evaluation for Quality of Life (QoL) revealed insignificant differences among high
and low groups. 46.6% and 40.0% of school children from the high and liw groups, respectively,
reported for the need for orthodontic treatment (df=1; P=0.375). The high group reported a
definitive need for orthodontic treatment when compared to the low group. The relative risk of
the need for orthodontic treatment is calculated for girls keeping boys as the reference category.
No elevation in the risk is observed. The relative risk is 0.32(0.17-0.59).
The association between the need for orthodontic treatment and gender, school type,
socioeconomic factors and quality of life was analyzed more in detail employing binary logistic
regression model (Table 8). The analysis involving gender, school type, socio-economic factors
and quality of life revealed that the prevalence of orthodontic treatment need was significantly
associated only with gender where boys were 1.83 times more likely in need of orthodontic
treatment when compared to girls. Other factors were not significantly associated with
orthodontic treatment needs.

37
However, our study had some limitations. In most epidemiological studies, individuals with a
previous or current history of orthodontic treatment are systematically excluded from the sample
(Bernabé and Flores-Mir, 2006; Manzanera et al., 2008). This leads to underestimation of the
real treatment need of the population being studied, a fact that needs to be taken into account
when making comparisons.

38
CONCLUSSIONS
1. Children from the public school had a lower need for orthodontic treatment than those in
the private school and girls had a lower need for orthodontic treatment than boys.
2. Children from the average socio-economic status category had a lower need for
orthodontic treatment followed by the poor and finally by the rich socio-economic status
category.
3. Girls had a better Quality of Life when compared to boys and children from the private
schools had a better Quality of Life than those from the public school.
4. Children who have a good quality of life had lower need for orthodontic treatment when
compared to children who do not have a good quality of life.

39
PRACTICAL RECOMMENDATIONS
1. Monitoring. Orthodontic problem are very common especially among adolescent children. In
India, awareness of orthodontic problems and the need for treatment is less especially in the sub-
urban and rural areas compared to the city. The schools pay attention towards awareness and
education among both private and public schools. Monitoring in routine basis should be done
every month. The need and demand of orthodontic treatment is important for planning public
orthodontic and dental services.
2. Health education. The lessons of health education should be implemented into teaching
curriculum starting from kindergarten and primary schools and higher secondary schools. It is
important to provide for children the appropriate knowledge and skills. The education of
children, parents and teachers regarding orthodontic problems and when to undertake treatment
is important.
3. Schools. The role of school health service should be increased. They should
concentrate more on oral health promotion programs on nutrition .The school can incorporate
oral health promotion as an integral part of schools curricula
4. Oral health. Oral health professional can plan, propose and implement school oral health
promotion activities as part of building up oral health promotion in schools.
5. Parents and family health services. Parents need more health education on the matters
related with nutrition, dental problem etc so that they could take the responsibility towards their
children regarding treatment. Family dentist also should take integrated efforts with school
health services to educate and instruct parent’s on health promotion matters of their children.

40
LIST OF REFERENCES
1. Abdolreza Jamilian, Mitra Toliat, Sahara Etezad. Prevalence of Malocclusion and Index
of Orthodontic Treatment Need in Children in Tehran. Oral Health and Preventive
Dentistry 2010; 8: 339-343.
2. Aiste Kavaliauskiene, Antanas Sidlauskas, Apolinaras Zaborskis. Demographic and
social inequalities in need for orthodontic treatment among school children in Lithuania.
Medicina (Kaunas) 2010;46(11):767-773.
3. Ansai T, Miyazaki H, Katoh Y, Yamashita Y, Takehara T, Jenny J. Prevalence of
malocclusion in high school students in Japan according to the Dental Aesthetic Index.
Community Dental Oral Epidemiology 1993; 21:303-5.
4. Bell R, Kiyak HA, McNeil RW, Wallen TR. Perceptions of facial profile and their
influence on the decision to undergoorthognathicsurgery. AmJ Orthod1985;88(4):323–32
5. Bernabé E and Flores-Mir C. Orthodontic treatment need in Peruvian young adults
evaluated though Dental Aesthetic Index. The Angle Orthodontist 2006; 76: 417–421.
6. Broder HL, Wilson-Genderson M. Reliability and convergent anddiscriminant validity of
the Child Oral Health Impact Profile (COHIP Child’s version). Community Dental Oral
Epidemiology, 2007; 35(1):20-31.
7. Brook PH, Shaw WC. The development of an index of orthodontic treatment priority.
European Journal of Orthodontics 1989;11(3):309–20.
8. Christie M, French D, Sowden A, West A. Development of childcentered, disease-
specific questionnaires for living with asthma. Psychosomatic Medicine 1993;55:541-
548.
9. Dhar V, Jain A, Kohli A. Prevalence of gingival diseases, malocclusion and fluorosis in
school-going children of rural areas in Udaipur district . Journal of the Indian Society of
Pedodontics and Preventive Dentistry 2007; 25:103 – 105.

41
10. Diwan S, Kumar S, Saxena V, Goel D. Assessment of orthodontic treatment needs
among children in Doiwala region, Uttarakhand (India). National Journal of Community
Medicine 2013; 4(2): 208-211.
11. Finn S.B. Clinical Pedodontics, 4th ed. (Philadelphia, PA: W.B. Saunders Co., 1973).
12. Rarity, D. M., Synopsis of Craniofacial Growth (New York NY: Appleton-Century-
Crofts, 1980).
13. Gift HC, Atchison KA . Oral health, health, and health-related quality of life. Medical
Care 1995; 33(11):57-77.
14. Graber LW, Lucker GW. Dental esthetic self-evaluation and satisfaction. American
Journal of Orthodontics 1980; 77:163-173.
15. Georgios Tsakos. Combining Normative and Psychosocial Perceptions for Assessing
Orthodontic Treatment Needs. Journal of Dental Education 2008;72 (8): 855-876.
16. Hedayati Z, Fattahi H R, Jahromi S B. The use of index of orthodontic treatment need in
an Iranian population. Journal of International Society of Pedodontic and Preventive
Dentistry 2007;25:10-14.
17. Heidi Kerosuo, Salem Al Enezi, Eero Kerosuo, Ebrahim Abdulkarim. Association
between normative and self-perceived orthodontic treatment need among Arab high
school students. American Journal of Orthodontics and Dentofacial Orthopedics, Vol.25,
Issue 3, March 2004.
18. Hemapriya S, Ingle NA, Chaly PE, Reddy VC. Prevalence of Malocclusion and
Orthodontic Treatment Needs Among 12 and 15 Years Old Rural School Children in
Kancheepuram District,Tamilnadu. Journal of Oral and Community Dentistry 2013; 7(2):
84-90.
19. Jaideep Sharma, Ruchi Dhir Sharma. Assessment of Orthodontic Treatment Need for
children in Moradabad, North India. OHDM - Vol. 13 - No. 1 - March, 2014.
20. Jose A, Joseph M R. Prevalence of dental health problems among school going children
in rural Kerala.
21. Kalyani Trivedi, Tarulatha R Shyagali, Jigar Doshi, Yagnesh Rajpara. Reliability of
Aesthetic component of IOTN in the assessment of subjective orthodontic treatment
need. Journal of advanced Dental Research 2011, 2(1): 61-66.

42
22. Kok YV, Mageson P, Harrudine NW, Sprod AJ. Comparing a quality of life measure and
the Aesthetic Component of the Index of Orthodontic Treatment Need (IOTN) in
assessing orthodontic treatment need and concern. Journal of Orthodontics 2000;
31(4):312-8.
23. Koochek AR, Yeh MS, Rolfe B, Richmond S. The relationship between index of
complexity, outcome, and need and patients’ perceptions of malocclusion: a study in
general dental practice. British Dental Journal 2001;191(6):325–9.
24. Mandeep Kaur Bhullar, Ashutosh Nirola. Malocclusion pattern in Orthodontic Patients.
Indian Journal of Dental Sciences 2012; 4(4); 20-22.
25. Mandall NA, McCord, Blinkhorn AS, Worthington HV, O’Brien KD. Perceived
aesthetic impact of malocclusion and oral self-perceptions in 14-15-year-old Asian and
Caucasian children in Greater Manchester. European journal of Orthodontics 1999; 21:
175-183.
26. Marcos AVB, Andre WM. An overview of the prevalence of malocclusion in 6 to 10-
year-old children in Brazil. Journal of Orthodontics 2010; 15(6).
27. Marques CR, Couto GB, Orestes CS. Assessment of orthodontic treatment need in
Brazilian schoolchildren according to the Dental Aesthetic Index (DAI). Community
Dental Health 2007; 24: 145–148.
28. Mausner JS, Kramer S. Epidemiology - An Introductory Text. 2nd
edition. Philadelphia:
Saunders; 1985.
29. Mclain JB, Proffitt WR. Oral health status: Prevalence of malocclusion. Journal of Dental
Education 1985;49:386-96.
30. Miitchell L, Carter NE, Doubleday B. An introduction to orthodontics. 2nd edition.
Oxford University Press; 2001.
31. Milton B, Asbell A. A brief history of orthodontics. American Journal of Orthodontics
1990; 98(3): 206-13.
32. N. Navabi, H. Farnudi, H. Rafiei, M. Tahmasbi Arashlow. Orthodontic Treatment and the
Oral Health-Related Quality of Life of Patients. Journal of Dentistry, Tehran University
of Medical Sciences, Tehran, Iran 2012; Vol. 9, No.3

43
33. Nazik M Nurelhuda, Mutaz F Ahmed, Tordis A Trovik, Anne N Astrom. Evaluation of
oral health-related quality of life among Sudanese schoolchildren using Child-OIDP
inventory. Health and Quality of Life Outcomes 2010, 8:152.
34. N’gom PI, Brown R, Diagne F, Normand F, Richmond S.A. Cultural comparison of
treatment need. European Journal of Orthodontics 2005; 27: 597-600.
35. Neslihan U, Esra E. The use of the Index of Orthodontic Treatment Need (IOTN) in a
school population and referred population. Journal of Orthodontics 2001; Vol.28: 45-52.
36. Neus Puertes-Fernández, José María Montiel-Company, José Manuel Almerich-Silla and
David Manzanera. Orthodontic treatment need in a 12-year-old population in the Western
Sahara. European Journal of Orthodontics 2010.
37. Roopa Siddegowda1, Rani. M.S. An Epidemiological Survey on Awareness towards
Orthodontic Treatment in South Indian School Children. Open Journal of Dentistry and
Oral Medicine 1(1): 5-8, 2013
38. Ruhi Nalcaci, Serhat Demirer, Firat Ozturk, Burcu A. Altan, Oral Sokucu, Vildan
Bostanci. The Relationship of Orthodontic Treatment Need with Periodontal Status,
Dental Caries, and Sociodemographic Factors. The Scientific World Journal 2012.
39. Paul S.Casamassimo, Jimmy R.Pinkham and Daniel Steinke. Dental Health Needs of the
Adolescent. Pediatric Dentistry 1979; 1(2):129-137.
40. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C (2005). The global
burden of oral diseases and risks to oral health. Bulletin of World Health Organization.
83:661-669.
41. Prabu D, Naseem B et al. A relationship between socioeconomic status and orthodontic
treatment need. Virtual Journal of Orthodontics 2008; 8 (2): 1-7.
42. Shaw WC, Richmond S, O'Brien KD, Brook P, Stephens CD. Quality control in
orthodontics: Indices of treatment need and treatment standards. Br Dent J 1991;9:107-
12.
43. KM Shivakumar, GN Chandu, VV Subba Reddy, MD Shafiulla
.Prevalence of
malocclusion and orthodontic treatment needs among middle and high school children of
Davangere city, India by using Dental Aesthetic Index. Journal of Indian Society of
Pedododontic and Preventive Dentistry 2009;27:211-8.

44
44. Sischo.L and Broder HL. Oral Health-related Quality of Life: What, Why, How, and
Future Implications. Journal of Dental Research 2011; 90(11):1264-1270.
45. Sisson KL. Theoretical explanations for social inequalities in oral health. Community
Dental and Oral Epidemiology 2007; 35:81-88.
46. Sudaduang Gherunpong, Georgios Tsakos and Aubrey Sheiham. The prevalence and
severity of oral impacts on daily performances in Thai primary school children. Health
and Quality of Life Outcomes 2004; 2:57.
47. Susan J Cunningham, Nigel P Hunt. Quality of life and its importance in Orthodontics.
British Orthodontic Society 2001; 28 (2): 152-158.
48. Taylor KR, Kiyak A, Huang GJ, Greenlee GM, Jolley CJ, King GJ. Effects of
malocclusion and its treatment on the quality of life of adolescents. American Journal of
Orthodontics and Dentofacial Orthopedics. 2009; 136(3):382-392.
49. Tak M, Nagarajappa R, Sharda AJ, Asawa K, Tak A, Jalihal S, Kakatkar G. Prevalence
of malocclusion and orthodontic treatment needs among 12-15 years old school children
of Udaipur, India. Eur J Dent 2013;7(1):45-53.
50. Thilander B, Pena L, Infante C, Parada SS, de Mayorga C. Prevalence of malocclusion
and orthodontic treatment need in children and adolescents in Bogota, Colombia. An
epidemiological study related to different stages of dental development. European Journal
of Orthodontics 2001; 23:153-167.
51. Tickle M, Kay EJ, Bearn D. Socio-economic status and orthodontic treatment need.
Community Dental Oral Epidemiology 1999; 27: 413-418.
52. Venkatesh Babu , Gopu H. Assessment of Orthodontic Treatment Needs According to
Dental Aesthetic Index. Journal of Dental Sciences and Research 2011; 2(2): 1-5.

45
QUESTIONNARIES
CHILDREN'S ORAL HEALTH AND RELATED QUALITY OF LIFE
INVESTIGATION
FORM TO BE FILLED BY STUDENTS
Dear students,
Thank you for participating in this study. In response to this questionnaire, it will help us learn more about
children's oral health. This will allow dentists and researchers to explore, deeper children's teeth and other oral
diseases organ to disclose their reasons for selecting the best treatment. This will be useful as healthy teeth are very
important for good health and your happiness.
How to fill in the questionnaire?
Carefully read each question. In response to it, the box, which is near or below the most likes you the answer. For
each question tick only one box, otherwise we will not be able to count your answers. If it is difficult to choose a
single answer, so think, at that moment which answer is accurate. In other cases, write a response to the points
marked.
Please reply to the questions yourselves. After filling the form, insert it in an envelope, stick and give it yourself to
the school visiting doctors. We promise that no one at school and parents (guardians) will know your answers.
Thank you in advance for honesty and sincerity.
The study by the Lithuanian University of Health Sciences
The study coordinator
Prashanth Prakash

46
1) Today's date: Day..... Month..................... Year 201…..
Questions about yourself
2) When were you born?
I was born on: Day..... Month..................... Year ….................
3) Who are you: a boy or a girl?
4) Which class do you study in?
In brackets, write the letter and class, for example, 7 (A) class, if any.
I am studying in ........................... (..........) classroom
5) Where do you live?
Questions about General health and happiness
6) How would you describe your health?

47
7) In general, how you feel thinking about your current life?
8) The picture drawn ladder: At the top of the ladder is score 10 – if you are most satisfied with your life, at
the bottom is 0 – if you are least satisfied with your life.
Where on the ladder do you feel you standing now?
Mark the box that best reflects your position.
10 Most satisfied
with life
9
8
7
6
5
4
3
2
1

48
0 least
satisfied with life
Oral health status and complaints
9) How would you describe your oral health?
Mark one box for each row
very good well average poor very bad
a) Dental
b) Lip
c) Gum
d) Stomatitis
e) Jaws and joints
10) During the past three months as part of a mouth organ Thee plagued health disorders?
Mark one box for each row
Just not a
trouble
A little
distressed
somewhat
distressed weary
It is very
tiring
a) Dental
b) Lip
c) Gum
d) Stomatitis
e) Jaw and joints

49
11) In the last three months of the dry felt an organ pain?
Mark one box for each row
never
once or
twice sometimes often
almost
every day
a) Dental
b) Lip
c) Gum
d) Stomatitis
e) Jaw and joints
12) During the past three months has your mouth had such problems?
Mark one box for each row
Never
once or
twice Sometimes often
almost
every day
a) When cleaning your
teeth, do your gums
bleed
b) Sores or wounds on
the lips
c) Mouth sores or
wounds
d) Bad breath from
mouth
e) Does food get caught
between your teeth
f) Are your teeth
sensitive to hot, cold
or sweets

50
13) During the past 3 months due to dental or oral condition, do you ...?
Mark one box for each row
Never
Once or
twice Sometimes Often
Almost
every day
a) Tear and chew solid
food like apple and
meat
b) Take longer time
than others to chew
the food
c) Could not drink or
eat anything hot or
cold
d) Could not drink
through a straw
e) Could not be opened
wide
14) During the past 3 months due to dental or oral condition you ...? Mark one box for each row
If this was not associated with dental or oral condition, note the answer "Never"
Never
Once or
twice Sometimes Often
Alm ost
every day
a) Breathing through
the mouth
b) Could not form
words
c) Blogs slept
d) headaches
e) In general, you feel
ill (nausea, felt
fatigue, etc.).
Questions about your feelings and emotions
15) During the past 3 months due to dental or oral condition
You are ...? Mark one box for each row
If this was not associated with dental or oral condition, note the answer "Never"

51
Never
Once or
twice sometimes often
Almost
everydy
a) Cries, suddenly
excited
b) Lack of courage,
self-confidence
c) You were
embarrassed, felt
ashamed
d) Were you nervous,
irritable, angry
e) you feel lonely
f) Do you feel,others
are thinking badly
about your teeth or
mouth
g) Do you feel,your
teeth or mouth does
not look as nice as
the other
h) Do you feel, your
teeth or mouth are
not as healthy as
other
i) Did you feel
dejected because of
their teeth or mouth
j) Do you feel,you
stand out from the
rest thanks to their
teeth or mouth
appearance

52
Questions about school, friends and leisure time
16) During the past 3 months due to dental or oral condition
You are ...? Mark one box for each row
If this is not related to the teeth or mouth, note the answer "Never
Never
Once or
twice Sometimes Often
Almost
every day
a) Avoiding school
b) Could not
concentrate at school
c) Could not concentrate
with homework
d) Avoid loud talking in
class or read
e) Avoid attending
sports, choir or other
circles, get-togethers
or school trips
f) Avoid talking with
your friends
g) Avoid eating when
other people were
around
h) Avoid smile or laugh
when you are around
other children were
i) In general, avoid
being with other
children
j) It was hard to play
wind musical
instruments (if you
play)

53
17) During the past 3 months due to dental or oral condition ...?
Mark one box for each row
If this is not related to the teeth or mouth, note the answer "Never"
Never
Once or
twice sometimes often
Once or
twice
a) Other kids made fun of
You
b) Other children avoid
you
c) Other children asked
what happened to your
teeth or mouth
How do you take care of their teeth and mouth
Remember the last 3 months
18) How often do you brushing your teeth with a toothbrush and toothpaste?
19) Have you noticed that brushing your teeth with a toothbrush and toothpaste, it is difficult to clean your teeth?
(eg dental remains of food)

54
20) What kind of toothbrush you use?
1 A simple one
al
21) What kind of toothpaste you use?
22) Do you rinse your mouth with mouthwashes?
1 Never
2 Sometimes
23) Do you use sanitary thread (floss) between the teeth to clean?
1 Never
2 Sometimes
ften
24) Do you use toothpicks to clean between the teeth?
1 Never
2 Sometimes
ften

55
Treatment / Healing
25) Do you have a filled tooth?
1 Yes
2 No
26) Do you have rotten teeth that need to be treated?
doctor
27) Over the last 12 months, you visited the dentist?
28) If "Yes", visited the why? Mark all that apply. If "No", skip this question.
undergo prophylactic
.......................................... ...........................
29) How much do you fear dental treatment?

56
30) Have you ever noticed that your teeth are irregularly placed, or did you notice a bad bite?
31) Do you wear / wore dentures?
ore. Write how much time wore: ..............................
How long have wearing ............................................. ....
32) Do you wear / wore braces?
.........
33) If you wear / wore dentures or braces, how much do you think this treatment has helped you (improved health,
appearance or other)?
plate or braces

57
Diet and smoking
Remember the last 3 months
34) How often do good or eat these foods?
Mark one box for each line.
Never
Less than
once a week Weekly
2-4 days a week
5-6 days a week
Every day,
once a day
Every day, several
times a day
a) fruit
b) green vegetables
c) cooked vegetables
d) Candies, chocolate
e) Cakes, brownies, cookies
f) Coca-Cola and other carbonated soft drinks
g) various energy drinks
h) Milk, yogurt, cottage cheese, cheese and other dairy product
35) Have you ever smoked (at least one cigarette)?
1 Yes
2 Not
36) How often do you smoke?

58
Questions about your parents and family
37) How often do you talk to parents about your dental and oral health?
Mark one box for each row
Veryeasy Easy It is
difficult
It is very
difficult
Do not
have or
see this
person
a) The father
b) The stepfather (sponsor)
c) with mom
d) The stepmother (Patron)
38) Overall, how easy is it to talk to your parents, about the different things that are important to you and made you
worried about?
Mark one box for each row
Very easy Easy It is
difficult
Very
difficult
Do not
have or
see this
person
a) The father
b) The stepfather
(sponsor)
c) with mom
d) The stepmother
(Patron)
39) Does your family have a computer?

59
40) Does your family have a car?
1 .No
41)How many times in the past 12 months you together with your family, went on trips (vacation)?
1. Never
4 more than 2 times
42) Do you have your own room?
1. yes
2. no
43) How well off do you think your family is?
1
2
3
4
5 not at all well off
44) Does your father have a job?

60
44). Does your mother have a job?
2 No
Questions about your abilities
45) The table shows the wide variety of claims about your abilities. After reading each statement, note how many
agree with him or disagree
Mark one box for each line.
Strongly
agree Agree Disagree
Strongly
disagree
a) I feel that I am inferior to other
b) It seems to me that I have more
good qualities
c) Overall, I think that I am a loser
d) I am able to everything as well
as many other
e) I feel that I have little to be
proud of
f) About myself I feel good
g) Overall, I am a self-satisfied
h) I prefer a more self-respect
i) Sometimes, I feel to be useless
to anyone
j) Sometimes I think that I am
nothing?

61
CHILDREN’S ORAL HEALTH RELATED QUALITY OF LIFE
RECORD FORM FOR
ORAL HEALTH EXAMINATION
SCHOOL ...................................... CLASS.............
ID ..................................................................
1. Today‘s date: ________ / _________ / 201____
DAY MONTH YEAR
2. Date of birth: ________ / _________ / _______
DAY MONTH YEAR
3. Gender
1 Boy
2 Girl
4. Ask the child if the following questionnaires were completed:
A. For child himself B. For parents (guardians)
1 Yes
1 Yes
2 No 2 No

62
A.
Den
tal
bo
ne
con
dit
ion
To
p /
Lef
t
Bo
tto
m /
Lef
t
7 –
sea
l
8 –
sea
l +
act
ive
dec
ay
9 –
sea
l +
sta
bil
ized
dec
ay
10
– e
xtr
act
ed t
oo
th d
ecay
on
11
– e
xtr
act
ed t
oo
th fo
r o
rth
od
on
tic
pu
rpo
ses
12
– r
eta
ined
to
oth
13
– s
eala
nts
2
8
38
27
37
26
36
25
35
24
34
23
33
22
32
21
31
11
41
0 –
wh
ole
su
rfa
ce i
s h
ealt
h
1 –
in
tact
su
rfa
ce a
ctiv
e d
ecay
(sm
ear)
2 –
act
ive
dec
ay
, th
e su
rfa
ce e
na
mel
def
ect
3 –
act
ive
dec
ay
, d
eep
en
am
el d
enti
ne
def
ect
4 –
in
tact
su
rfa
ce s
tab
iliz
ed d
eca
y (
smea
r)
5 –
sta
bil
ized
dec
ay
, th
e su
rfa
ce e
na
mel
def
ect
6 –
sta
bil
ized
dec
ay
, d
eep
en
am
el d
enti
ne
def
ect
12
42
13
43
14
44
15
45
16
46
17
47
18
48
M
O
D
B
L
۞
M
O
D
B
L
۞
To
p /
Rig
ht
Bo
tto
m /
Rig
ht

63
A1. Oral Hygienic Index (by Silness & Loe) 4 points assessment
0
No plaque
1 The small amount of plaque at cervical region
2 Plaque is clearly visible at cervical region and interdental space
3 Thick deposits of plaque on the surface of the tooth to the gum and
interdental spaces which are clearly visible and run through probe
A2. Assessment of periodontal status (CPITN index)
0 – Healthy
1 – Bleeding on probing
2 – Stones
3 – A pocket of 4-5 mm
4 – 6 mm pockets and deeper
5 – Missing sextant
A3. Dental fluorosis classification (by Thylstrup & Fejerskov)
The upper jaw The lower
jaw
Central incisors
Lateral incisors
Canines
First premolars
Second premolars
First molars
Second molars
A4. Discoloration or damaged tooth
Discoloration
Hipoplasia
Tetracycline
Erosion
Attrition

64
B. Tooth position and occlusal evaluation
B1. Lateral teeth ratio (Angle class):
Ratio of the first molars:
Right Left
1 Angle I
1 Angle I
2 Angle II 2 Angle II
3 Angle III 3 Angle III
B2. Ratio of the canines
1 Angle I
1 Angle I
2 Angle II 2 Angle II
3 Angle III 3 Angle III
B3. No teeth (solving of adentae, ectopic and retained teeth)
Mark observed disturbances
Classification Criteria
0 No changes
1 Retained tooth
(excluding third
molars)
5.i Did not spring up teeth due to crowding,
dislocation, overcomplement tooth, ankylosing
deciduous teeth, and other pathological reasons
2 Mild hipodontia 4.h Missing one tooth in any quadrant and required
orthodontic treatment prior to restorations or
gaps closing to avoid the prosthesis
3 Severe hipodontia 5.h Missing more than one tooth in any quadrant
and required orthodontic treatment prior to
restorations
4 Partially appearance
of teeth 4.t Partially appearance of teeth, leaning and
blocked the adjacent tooth

65
B3. No teeth (solving of adentae, ectopic and retained teeth)
Mark observed disturbances
5 Overcomplement
tooth
4.x Extra teeth
6 Milk tooth
ankylosis
5.s
B4. Horizontal mouth overlay (HMO): ........................... mm
Classification Criteria
1 A small positive,
competent lips
2.a 3.5 mm <HMO ≤ 6 mm, lip competent
2 A small positive
incompetent lips 3.a 3.5 mm <HMO ≤ 6 mm, lip incompetence
3 Medium positive 4.a 6 mm <HMO ≤ 9 mm
4 Bright positive 5.a HMO > 9 mm
5 Slightly negative 2.b -1 mm ≤ HMO < 0 mm
6 Average negative free
speech and chewing
problems
3.b -3.5 mm ≤ HMO < -1 mm, no speech and
chewing problems
7 Bright negative free
speech and chewing
problems
4.b HMO < -3.5 mm, no speech and chewing
problems
8 On average, the
negative, with a speech
and chewing problems
4.m -3.5 mm ≤ HMO < -1 mm, is a speech and
chewing problems
9 Bright negative, with
speech and chewing
problems
5.m HMO < -3.5 mm, is a speech and chewing
problems
B5. Lips
0 Competent

66
B5. Lips
1 Incompetent
B6. Chewing disorders
0 No
1 Yes
B7. Speech disorders
0 No
1 Yes
B8. Cross-bite (CB)
0 No
1 Yes
B9. CB: .......................................... mm
Measured distance (CB) between the retruded contact surface and the
intermound surface
B10. CB location B11. CB functional disorders
1 Front
0 No
2 Right side 1 Yes
3 Left side
4 Single tooth

67
B12. Classification Criteria
0 No changes
1 A small front or side 2.c CB ≤ 1 mm
2 Average front or side 3.c 1 mm < CB ≤ 2 mm
3 Bright front or side 4.c CB > 2 mm
4 Lateral lingual 4.l One-sided or double-sided lateral lingual CB
without functional occlusal contacts
B13. Displacement of the contact points (DCP): ........................... mm
(crowding). Measured distance between the two most crowded permanent teeth
Classification Criteria
0 No changes
1 Small 1.- DCP ≤ 1 mm
2 Noticeable 2.d 1 mm < DCP ≤ 2 mm
3 Quite a bit 3.d 2 mm < DCP ≤ 4 mm
4 Bright 4.d DCP > 4 mm (pronounced shift in the
point of contact)

68
B14. Vertical moth overlay (VMO): ............................. mm
Classification Criteria
0 No changes
1 Increased OB, deep
bite
2.f VMO ≥ 3.5 mm no contact with the gums
2 Increased OB, deep
bite 3.f Deep bite, reaching the gums or palate, no
injuries
3 Increased OB, deep
bite 4.f Deep bite, reaching the gums or palate with
trauma
4 Front or side open
bite
2.e 1 mm < VMO ≤ 2 mm
5 Front or side open
bite
3.e 2 mm < VMO ≤ 4 mm
6 Front or side open
bite
4.e VKP > 4 mm
B15. Lip or cleft palate and other anomalies
1 No
2 Yes (5.p)
B16. Pre-normal or post-normal occlusion without other abnormalities
1 No
2 Yes (2.g)
B17. Photo
1 Was made
2 Was not made

69
B18. Aesthetic component (1.....10)
.....................................................................
Dental component of the ICON index
3 A. Open incisors bite B. Incisors overlay
0 Edge to edge
0 <1/3
1 < 1 mm
1 From 1/3 to 2/3
2 From 1.1 to 2 mm
2 From 2/3 to the full
3 From 2.1 to 4 mm
3 Full
4 > 4 mm
4 The upper and lower posterior teeth ratio from front to back (in arrow direction):
Right Left
0
The upper lateral teeth in contact with the protuberance of
lower teeth:
Angle I, II, III
0
1 Any tuberosity ratio but not in thalamus to the thalamus 1
2 Thalamus to the thalamus 2
1 A. Crowding B. Spaces between the teeth
0 < 2 mm
0 < 2 mm
1 From 2.1 to 5 mm
1 From 2.1 to 5 mm
2 From 5.1 to 9 mm
2 From 5.1 to 9 mm
3 From 9.1 to 13 mm
3 > 9 mm
4 From 13.1 to 17 mm
5 > 17 mm
5 Retained teeth

70
PHOTOGRAPHS
Public school
Private school