Embed Size (px)
Citation preview

UNITED REPUBLIC OF TANZANIA
MINISTRY OF HEALTH, COMMUNITY DEVELOPMENT, GENDER, ELDERLY AND CHILDREN
NATIONAL TUBERCULOSIS LABORATORY STRATEGIC PLAN (2018–2022)
MAY 2018

Table of contents
List of figures...................................................................................................................................... iiiForeword............................................................................................................................................. ivAcknowledgments................................................................................................................................vExecutive summary............................................................................................................................viAbbreviations.....................................................................................................................................vii1.0 Vision and mission statements......................................................................................................1Vision...................................................................................................................................................1Mission.................................................................................................................................................12.0 Situational analysis........................................................................................................................22.1 The TB specific contextual analysis:..............................................................................................2
a) Epidemiological situation for tuberculosis............................................................................2b) Laboratory objectives and targets according to the NTLP strategic plan and the National
health laboratories TB-specific objectives............................................................................2c) National TB diagnostic and treatment guidelines and current linkages with the NTLP........2d) Linkages with supra-national reference laboratories...........................................................1e) Linkages with the NTLP and general health system (including private health sector).........2f) Linkages with Private Sector................................................................................................2g) Regulatory, legal, political and economic issues..................................................................2
2.2 TB specific tests currently available and coverage........................................................................32.3 Structure of the TB laboratory network.........................................................................................32.4 Infrastructure of the TB laboratory network..................................................................................52.5 Human resources for the TB laboratory network...........................................................................62.6 Maintenance and validation of TB laboratory equipment..............................................................62.7 Laboratory quality management systems.....................................................................................72.8 Management of laboratory commodities and supplies..................................................................72.9 Laboratory information and data management.............................................................................82.10 Specimen referral system for the TB laboratory network............................................................82.11 Operational research regarding the TB laboratory network........................................................92.12 Legal and Policy review...............................................................................................................92.13 Finances for TB laboratory services.............................................................................................93.0 Development of the national TB Laboratory Strategic Plan.........................................................113.1 The purpose of the National TB Laboratory Strategic Plan..........................................................113.2 Methodology for the development of Strategic Plan....................................................................114.0 Strengths, weaknesses, opportunities and threats (SWOT) analysis...........................................125.0 Key priority intervention areas and main activities in priority order...........................................16
ii

List of figures
Figure 1: Tanzania National Tuberculosis Diagnostic Algorithm (No Onsite GeneXpert Instrument)...11Figure 2: Tanzania National Tuberculosis Diagnostic Algorithm (Onsite GeneXpert Instrument)........12
iii

Foreword
This is the first-ever National Tuberculosis Laboratory Network Strategic Plan for the United Republic of Tanzania. The plan has been developed based on the National Tuberculosis and Leprosy Program (NTLP) Strategic Plan, National Health Laboratory Strategic Plan, Health Sector Strategic Plan IV, the Mid Term Expenditure Framework of the Ministry Of Health, Community Development, Gender, Elderly and Children (IV) the World Health Organization/Global Laboratory Initiative TB Laboratory Guidelines, and the Maputo Declaration.
The main purpose of this strategic plan is to enable the Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) laboratory services to effectively carry out TB-related functions as stipulated by the ministry’s mandate, and to strategically mobilize, coordinate and allocate available resources by prioritizing functions with effective impact in line with the National Health Policy.
This plan will be used as a management resource and national operational guidelines for public and private TB laboratories, TB laboratory-dependent health programs, and donor organizations interested in filling resource gaps on TB laboratory services. This document details results of an assessment of the current laboratory situation in Tanzania, specific strategic approaches, planned activities, and goals to be achieved by the end of 2022.
The objectives of the current National TB Laboratory Strategic Plan are as follows:1. Increase access to quality-assured AFB microscopy2. Improve the diagnosis of TB among AFB-negative cases especially among people
living with HIV3. Increase access to rapid laboratory diagnosis among presumptive and TB patients
considered at risk for M/XDR-TB.4. Establish Laboratory Quality Management Systems.
These objectives were identified by assessing the gap between the current service provision and the country’s goals for the future.
Through these objectives, the NTLP will create affordable and sustainable system of high-quality TB laboratory services accessible to all citizens with reliable results to provide guide in clinical decision-making throughout the country.
The implementation of this five-year plan will be monitored using the results framework and midterm and end-of-period reviews. These reviews will result in appropriate adjustments.
Dr. Zainab ChaulaPermanent Secretary - HealthMay 2018
iv

Acknowledgments
This first National Tuberculosis (TB) Laboratory Network Strategic Plan was completed by the National Tuberculosis and Leprosy Programme (NTLP) of the Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) in close collaboration with other National and International consultants and Development Partners.
The development of this strategic plan involved many people who offered advice and support. Sincere thanks go to the Director for Preventive Services Dr. Leonard Subi, the NTLP Programme Manager Dr. Beatrice Mutayoba and the Deputy Programme Manager Dr. Liberate Mleoh for their readiness, tireless efforts and guidance towards the development of this document. Special gratitude goes to Ms. Basra Doulla the Head of the Central Tuberculosis Reference Laboratory, who provided the preliminary stimulus by initiating and preparing the first draft. Heartfelt thanks goes to Dr. Valentina Anisimova, the KNCV consultant for her technical support during development of the plan.
The Ministry also appreciates the contributions from the research scientists and laboratory staff from NTLP, NIMR, CTRL, KIDH and IHI who thoroughly and critically reviewed the plan and provided vital feedback and relevant inputs used to improve the document. Special appreciation goes to Dr. N. Range, Dr. A.M. Kilale, Mr. E. Luhanga, Dr. V. Mahamba , Mr. T. Chonde, Mr. P.H. Ngowi, Mr. H. Mbega, Mr. G. Mrema and Mr. S. Mfaume, Dr. J. Hella, Dr. K. Said, Mr. R. Shirima, Dr. I. Lekule, Mr. A. Mrutu and Mr. A. Kingalu for their valuable inputs.
It is not possible to mention each and every individual who provided inputs into this strategic plan, but I must extend my thanks to Prof. Moses Joloba, Department of Microbiology, Makerere University, Kampala, Uganda, who was part of the consultants during development of this document.
Lastly my sincere appreciation goes to The Global Health Bureau, Office of Health, Infectious Disease and Nutrition (HIDN), US Agency for International Development, financially supports development and printing of National Tuberculosis (TB) Laboratory Network Strategic Plan through Challenge TB under the terms of Agreement No. AID-OAA-A-14-00029. This National Tuberculosis Laboratory Strategic plan has been made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents do not necessarily reflect the views of the USAID or the United States Government.
Prof. Muhammad Bakari KambiChief Medical Officer
v

Executive summary
The current TB laboratory strategic plan was developed in October 2013 and required updates as there have been a few developments in TB control and TB laboratory network since then. Thus, the NTLP has developed a number of guiding documents; to mention a few, i) NTLP strategic plan 2015 – 2020, ii) GeneXpert MTB/RIF implementation and roll-out plan (2015), iii) Framework for decentralization of PMDT services and others.
In late 2013, the WHO had endorsed a handbook for developing strategic plans for TB laboratories developed by KNCV in partnership with The Union, CDC Atlanta and MSH supported by USAID through TB CARE (http://www.tbcare1.org/publications). This handbook guided the development of the existing strategic plan.
The current strategic plan gives a strong emphasis on four major laboratory objectives and NTLP strategic plan (2015–2020) targets. It refers to the National Health Laboratory objectives and the situational analysis of TB epidemiological situation in the country. The plan contains a section showing the structure of the TB laboratory network and its infrastructure. A clear explanation of the linkages with the general health system, supra-national reference laboratories, private sector laboratories, regulatory, legal, political and economic issues have also been made.
The current strategic plan includes; information on the available TB specific tests and their coverage, TB laboratory network human resources, maintenance and validation of the TB laboratory equipment, laboratory quality management systems and laboratory commodities and supplies.
The development of this plan unveils key priority intervention areas and main activities in precedence.
vi

Abbreviations
ADDS Assistant Director of Diagnostic ServicesAFB Acid-fast bacilliAIDS Acquired Immunodeficiency SyndromeASP Authorized service providerCDC Centers for Disease Control and PreventionCPC Cetyl Pyridinium ChlorideCTRL Central Tuberculosis Reference LaboratoryDHIS2 District Health Information System 2DOTS Directly Observed Therapy, Short CourseDRS Drug Resistance SurveyDST Drug Susceptibility TestingDTHC District Tuberculosis and HIV CoordinatorDTLC District Tuberculosis and Leprosy CoordinatorEMS Expedited Mail ServiceEQA External Quality AssessmentFIND Foundation for Innovative New DiagnosticsGLI Global Laboratory Initiative (STOP TB Partnership-World Health Organization)HIV Human Immunodeficiency VirusHRH Human Resource for HealthISO International Organization for StandardizationIT Information TechnologyIHI Ifakara Health InstituteKIDH Kibong’oto Infectious Disease HospitalKNCV Koninklijke Nederlandse Centrale Vereniging tot bestrijding der TuberculoseLED FM Light-Emitting Diode Fluorescence MicroscopyLIS Laboratory Information SystemLPA Line Probe AssayLQAS Laboratory Quality Assurance SystemM&E Monitoring and EvaluationMDR TB Multidrug-resistant tuberculosisMOCGEC Ministry of Health Community Development, Gender, Elderly and ChildrenMSD Medical Stores DepartmentMTB Mycobacterium tuberculosisNGO Non-Government OrganizationNIMR National Institute for Medical ResearchNLMIS National Laboratory Management Information SystemNTLP National Tuberculosis and Leprosy ProgrammeNTLSP National Tuberculosis Laboratory Strategic PlanOR Operational ResearchHF Health facilityPATH Program for Appropriate Technology in HealthPHL-IdC Public Health Laboratory – Ivo de CarneriPPE Personal protective equipmentPPP Public Private PartnershipPPM Planned preventive maintenance
vii

QMS Quality Management SystemRIF RifampicinRLT Regional Laboratory TechnologistRTLC Regional Tuberculosis and Leprosy CoordinatorSLMTA Strengthening Laboratory Management towards AccreditationSNRL Supra-National Reference LaboratorySWOT Strengths, weaknesses, opportunities and threatsTA Technical AssistanceTB Tuberculosis TBCAP Tuberculosis Control Assistance ProgramTLCU Tuberculosis and Leprosy Central UnitIUATLD International Union Against Tuberculosis and Lung DiseaseUSAID US Agency for International DevelopmentWHO World Health OrganizationXDR TB Extensively drug-resistant tuberculosisZN Ziehl Neilsen
viii

1.0 Vision and mission statements
Vision
Well-coordinated, high-quality, sustainable, nationwide TB laboratory services accessible and affordable to all.
Mission
Ensure high-quality, efficient TB laboratory services at all levels of public and private laboratories, functioning according to acceptable national standards.
1

2.0 Situational analysis
2.1 The TB specific contextual analysis:
a) Epidemiological situation for tuberculosis
Tuberculosis is still a major public health problem in Tanzania. The country is among the 30 high burden countries as described in the 2017 Global TB report. The first-ever national TB prevalence survey was completed in November 2012, and revealed higher TB burden with the prevalence of 295 per 100,000 populations among adults ≥ 15 years and a case detection rate of 42 – 54. However, the most recent WHO modelled estimates in 2015 show that the prevalence of all forms stands at 528 per 100,000 with incidence of 327 per 100,000 and case detection rates determined at 79%. In 2016, however, Tanzania notified a total of 65,902 cases of all forms of TB. Using WHO 2015 estimates, Tanzania is missing approximately 16,268 TB cases of all forms each year.
TB treatment success rate for smear positive TB cases stood at 90% in 2015, with regional variations between 71% and 98%. Treatment outcomes for new smear positive TB/HIV co-infected patients were lower than in HIV negative. Overall treatment success and death rates for co-infected patients were 83.2% and 8.4% respectively in 2015 (NTLP annual report 2016).
b) Laboratory objectives and targets according to the NTLP strategic plan and the National health laboratories TB-specific objectives
The current National Strategic Plan V for Tuberculosis and Leprosy Program (NSPV) was reviewed in 2014 for the period of 2015–2020. This TB Laboratory Strategic Plan has been formulated based on the NSPV. It has four objectives which include; increase access to quality-assured AFB smear microscopy; Improve the diagnosis of TB among AFB-negative cases especially among people living with HIV; Increase access to rapid laboratory diagnosis among presumptive and TB patients considered at risk for M/XDR-TB; and Establish Laboratory Quality Management.
c) National TB diagnostic and treatment guidelines and current linkages with the NTLP
TB services in Tanzania are in line with WHO and the UNION recommendations which are specific for particular countries. In the country, there is a strong network coverage of diagnostic laboratories for sputum smear microscopy services, although the level of function of the laboratories are different i.e., central, zonal, region, district, heath center and dispensary. These laboratories are fully integrated into the general health care delivery system, including private and public health institutions.
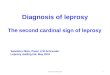
The diagnosis of pulmonary TB is primarily dependent on the Acid Fast Bacilli (AFB) microscopy (Figure 1). For high-work load centers, light-emitting diode (LED) fluorescence microscopy (FM) is recommended. However, the extent of FM coverage is not adequate. In-
2

depth assessment is needed in order to establish realistic demands of LED FM countrywide in relation to the WHO recommendations.
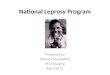
Furthermore, diagnostic guidelines for detection of pulmonary TB and DR TB depend on availability of new diagnostic tools such as Xpert MTB/RIF (Figure 2). In settings with GeneXpert laboratories, Xpert MTB/RIF test is recommended as an initial test for detection of both drug sensitive TB and DR TB with a single spot sputum specimen. In all other areas AFB microscopy remains an initial test for detection of TB. In this case two sputum samples are to be submitted: spot and early morning sample.
Laboratory tests recommended for detection of extra-pulmonary TB (EPTB) are smear microscopy, molecular tests (Xpert MTB/RIF and LPA) and culture. Laboratory diagnosis of pediatric TB is the same as for adults with an exception that replacement of microscopy with Xpert MTB/RIF is recommended for diagnosis of TB in children wherever possible while HIV (human immunodeficiency virus) positive status is not among the criteria for priority testing with Xpert MTB/RIF according to the algorithm in the Xpert MTB/RIF roll-out plan. Xpert MTB/RIF is the main test for detection of MDR TB.
3

Figure 1: Tanzania National Tuberculosis Diagnostic Algorithm (sites with no GeneXpert machine)
1

Figure 2: Tanzania National Tuberculosis Diagnostic Algorithm (site with GeneXpert machine)
2

Bacteriologically confirmed TB is defined as TB case from whom a biological specimen is positive by smear microscopy, culture or molecular test (LPA, Xpert MTB/RIF). International definition of smear positive case is used depending on the type of microscopy used when there is presence of AFB in only one sputum sample. Monitoring of treatment is done using one sputum (morning) sample. Smear negative tuberculosis is detected by repeated clinical assessment and chest X-Ray.
In Tanzania, drug susceptibility testing (DST) is done primarily for routine surveillance of drug resistance. Culture and first line (FLD) anti-TB DST are recommended for Xpert MTB/RIF positive cases and for smear positive cases at high risk for MDR TB. Second line (SLD) anti-TB drugs DST is prescribed for cases at high risk for MDR TB with confirmed resistance to rifampicin (RIF) by Xpert MTB/RIF.
d) Linkages with supra-national reference laboratories
The CTRL maintains close linkage with the private sector and regulatory bodies to ensure smooth and integrated implementation of NTLP activities in the country. CTRL also maintains a close collaboration with the World Health Organization (WHO), the International Union Against Tuberculosis and Lung Disease (IUATLD) and the Supra-National Reference Laboratory (SNRL). The Central TB Reference Laboratory (CTRL) is officially linked to the Supranational Reference Laboratory (SNRL) in Belgium (Department of Biomedical Sciences, Mycobacteriology Unit, Prince Leopold Institute of Tropical Medicine, Nationalestraat 155, 2000, Antwerp) and Supranational Reference Laboratory in Uganda. This ensures smooth linkage and participation in global initiatives and collaborations.
Term of reference of the linkage includes:
Programmatic1. Liaise with Global Laboratory Initiative (GLI) technical partners, the Central TB Reference
Laboratory and the NTLP to facilitate implementation of WHO policy guidance on TB diagnostics and laboratory norms and standards
2. Support the integration of quality TB diagnostic services within national laboratory policies and strategic plans incorporating cross cutting laboratory issues including quality management systems, supply management, specimen transport and referral and human resource development
3. Advocate for TB laboratory worker protection with use of current WHO TB biosafety recommendations
4. Support the implementation of an appropriate data management system.5. Provide guidance on quality management systems for a process towards achieving
laboratory accreditation to international standards
1

TechnicalServe as the focal point for coordination of technical assistance to CTRL (or equivalent) to enable:
1. Monitoring of the proficiency of drug susceptibility testing of M. tuberculosis2. Implementation of quality assured AFB microscopy (including external quality
assessment) in laboratory networks3. Development of capacity and proficiency in performing conventional and new WHO
endorsed technologies including:a. Microscopy methodsb. Culture and identification methodsc. Drug susceptibility testing (phenotypic and molecular methods)
4. Development of laboratory components of drug resistance survey (DRS) protocols, data validation, and quality assurance as required
5. On-site technical training or in-house training of laboratory staff as needed6. Review of laboratory proposals in Global Fund applications7. Conduct operational research, as relevant, including the introduction of new laboratory
tools
e) Linkages with the NTLP and general health system (including private health sector)
The Central TB Reference Laboratory (CTRL) is part of the Tuberculosis and Leprosy Central Unit (TLCU) which is under the Unit of Epidemiology and Disease control in the Department of Preventive Services of the Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC). The TB laboratories at the zonal, regional, district and peripheral levels are part of the National Health Laboratory (NHL) system which is under Diagnostic Services Section of the MoHCDGEC.
f) Linkages with Private Sector
The private sector is a potential resource for the expansion of TB laboratories services in Tanzania. However, linkages between private and public TB laboratory network need to be strengthened. Specific strategies have been detailed in the NTLP Strategic plan in order to engage the Private sector in the delivery of the TB related services in line with the national PPP policy and health sector PPP strategy.
g) Regulatory, legal, political and economic issues
TB diagnosis in Tanzania is controlled by the NTLP and the CTRL. Quality assurance at the national level is regulated by the National Health Laboratory Quality Assurance (QA). Tanzania Bureau of Standards (TBS) is responsible for laboratory techniques and accreditation based on ISO17025 and ISO 15189.
2

2.2 TB specific tests currently available and coverage
There are 1,200 microscopy centers in the country (2.4/100,000 population). However, about 30% of them are not functional due to various reasons. Fluorescent microscopy (FM) is implemented in 14% of laboratories. The vast majority of the FM laboratories use LED (Light Emitting Diode) technology. Smears are prepared direct from specimens except for few culture laboratories.
There are eight culture laboratories (CTRL, Kibong’oto, Mbeya, Dodoma, Pemba, and Bugando) and two for Research purposes which are KCRI and IHI. All of them perform culture on solid media (LJ, Lowenstein-Jensen) and two (the CTRL and Mbeya) on liquid media (MGIT - Mycobacterium Growth Indicator Tube). Specimen processing for culture uses NALC (N-Acetyl-L-Cysteine) procedure. Identification of MTB (Mycobacteria Tuberculosis) is done by rapid immune-chromatographic tests. NTM (Non-Tuberculous Mycobacteria) are identified using line probe assays.
First line DST (isoniazid [INH], rifampicin [RIF], streptomycin [STR] and ethambutol [EMB]) uses the proportion method both on solid (LJ) and liquid (MGIT) media. Second line DST (kanamycin [KM] and ofloxacine [OFX]) is conducted on solid (LJ) media. The concentrations of the drugs used for testing are in the line with the international recommendations. FLD DST is performed in two laboratories (the CTRL and Mbeya) and SLD DST in the CTRL only.
Molecular tests implemented in Tanzania are Xpert MTB/RIF) and line probe assay (LPA). There are 200 GeneXpert sites in the country. The instruments are located in higher to lower level heath facilities. The NTLP plans to scale up GeneXpert sites to 300 by 2022. Currently there are three laboratories that perform Line Probe Assays, planned to be scaled up to all the Zonal TB Laboratories.
2.3 Structure of the TB laboratory networkTB laboratory network in Tanzania is organized into four main levels according to the type of services provided:
1. National: Central Tuberculosis Reference Laboratory (1)2. Intermediate: Zonal Tuberculosis Reference Laboratories (5)3. Regional/referral (32) and district (169) hospital laboratories4. Peripheral: Health centers and dispensaries (993)
Specific responsibilities of the TB laboratory network levels
National: The Central Tuberculosis Reference Laboratory1. Conducts appropriate TB bacteriology tests, including AFB microscopy, molecular tests,
culture, susceptibility, and species identification tests on sputum specimens of new and retreatment patients received from districts and Zonal Tuberculosis Reference Laboratories (ZTRL)
3

2. Conducts slit skin smears for AFB microscopy for referred leprosy patients3. Develops policies, guidelines, and standards regarding AFB microscopy, molecular tests,
culture, drug susceptibility testing, and other novel diagnostic technologies4. Plans and carries out surveillance of resistance of Mycobacterium tuberculosis5. Plans, trains, supervises, and carries out regular quality control of AFB microscopy and
molecular test activities6. Collects, compiles, and analyzes data on smear and culture results from ZTRLs7. Disseminates and uses data on AFB microscopy and MDR TB surveillance for TB and
leprosy care and control activities8. Ensures availability of laboratory equipment, reagents, supplies and stationaries at all
levels in line with the NTLP guidelines9. Initiates, coordinates, and collaborates in operational research of relevant TB and leprosy
control activities
Zonal Tuberculosis Reference Laboratories1. Conducts TB bacteriology testing, including ensuring that all positive culture slopes are
sent to the CTRL as soon as possible (within 14 days) for susceptibility and species identification tests
2. Ensures that quality control procedures for smear and culture slopes are carried out and results are recorded accurately
3. Ensures that all smear and culture equipment and facilities are taken care of and maintained properly
4. Plans, trains, supervises, and carries out regular quality control of AFB microscopy and molecular testing activities
5. Participates in supervision of AFB microscopy in the zone and training of laboratory workers involved in AFB microscopy, in collaboration with the RTLC (Regional TB and Leprosy Coordinator)
6. Conducts slit skin smears for AFB microscopy for referred leprosy patients7. Initiates, coordinates, and collaborates in operational research of relevant TB and leprosy
control activities
Regional hospital laboratories1. Plans and supervises AFB smear microscopy and molecular testing in the region and
organizes training of laboratory workers involved in AFB microscopy, in collaboration with the RTLC
2. Ensures availability of a three-month supply of laboratory reagents and other supplies, in collaboration with the RTLC and the regional pharmacist
3. Participates in external quality assessment (EQA) of AFB smear microscopy
District hospital laboratories1. Supervises and ensures the quality of AFB microscopy in the district2. Collects, stores, and transports sputum specimens for culture and sensitivity testing at
the reference laboratory, in collaboration with the DTLC (District TB and Leprosy Coordinator)
4

3. Ensures that sufficient, quality-controlled stains and reagents are supplied to health facilities
4. Assists in AFB microscopy training programs5. Participates in EQA of AFB smear microscopy
Health centers and dispensaries1. Facilitates proper sputum specimen collection (spot, early morning) and registration2. Performs proper smear microscopy and recording of results in the NTLP laboratory
request form and register3. Ensures that sufficient laboratory reagents are available, in collaboration with the District
Laboratory Technician (DLT) and the DTLC4. Ensures the safe disposal of infected materials (e.g., sputum containers, microscopic
slides)5. Retains all examined slides for EQA in line with the NTLP guidelines6. Ensures proper care, use, and safety of the microscope7. Implements recommended corrective action for improvement of services
The levels of the network are linked through a two-way system: the lower level reports to the next higher level and higher levels supervise the lower levels. Exclusion is that the zonal level is not systematically involved in supervision.
2.4 Infrastructure of the TB laboratory networkThere is a national guidance for laboratory structure within the MoHCDGEC which guides the design and lay-out of the laboratories at different levels; however, this document is for general laboratories and not specific for TB. TB laboratories are equipped according to their levels of responsibility. Infrastructure of zonal and regional laboratories is mainly of good quality. Some TB culture laboratories are equipped with negative air pressure (the CTRL – processing room, in Mbeya and in Dodoma – the whole TB laboratory). Currently, the infrastructure of the CTRL facility does not allow proper flow of samples; only one small room is equipped with negative air pressure. In six out of eight TB laboratories processing of specimen and paperwork are done in the same room. All culture laboratories have biological safety cabinets (BSC). At the CTRL, Mwanza and Mbeya the BSCs are ducted to outside. A few district laboratories are equipped with BSCs. Other major equipment for culture (e.g., centrifuges, inspissators and incubators) and for LPA (e.g., thermocyclers, twincubators) is available.
All microscopy centers have microscopes; however, some of the facilities are not functional due to broken microscopes. Some laboratories are renovated to accommodate LPA and GeneXpert services. Some GeneXpert laboratories are equipped with air conditioners, generators and have access to tap water while some are powered with solar panels. However, many GeneXpert laboratories have not been renovated for the purpose; do not have air conditioners and are not protected from dust. There are frequent fluctuations of voltage in electrical power lines. Infrastructure of most of the district and peripheral laboratories buildings are old and are not well maintained.
5

The national, zonal, regional and district facilities use incinerators for waste disposal while many of peripheral facilities are not equipped with incinerators and bury or burn waste.
2.5 Human resources for the TB laboratory network
Tanzania as other developing countries is facing critical shortage of skilled health workers. Bottlenecks exist not only at production side but also the capacity to absorb the trained personnel is very limited at all departments including laboratory services. The distribution of trained personnel is also mismatched with the rural and remote areas facing major shortage. The National Health Strategic Plan (IV) has earmarked the Human Resource for Health (HRH) population ratio for laboratory services to be very low below the expectation and hence strategies are in place for the improvement. The strategies are stipulated in the HSSPIV, HRH Strategy and the BRN strategy.
There are six medical schools in the country which provide the pre-service training for TB microscopy. Several in-service training are provided with guidance and supervision of the National and zonal Trainers. The CTRL conducts hands on training of technicians for zonal laboratories to culture, DST and LPA. Additionally, there are TB bacteriology courses in Arusha, SADC (South Africa Development Community); a course on culture and DST in Ethiopia and ACILT (African Center for Integrated Laboratory Training) in South Africa.
2.6 Maintenance and validation of TB laboratory equipment
According to the national policy on medical laboratory equipment, introduction of technologically new equipment should be approved by the PHLB (Private Health Laboratory Board) which is authorized to verify of suitability of new equipment. The CTRL guides procurement of equipment based on the international standard specifications. There are no national standard specifications for TB laboratory equipment. A national procedure guides procurement of equipment through MSD (Medical Stores Department). Each laboratory is responsible for verification of any new equipment before routine use.
Professional preventive maintenance and repairs are inconsistent in frequency and turnaround times mainly due to the lack of service contracts and no budget lines specifically for service of equipment. The MoHCDGEC has established zonal workshops for maintenance of medical equipment; however, there is no national capacity for maintenance of the major TB laboratory equipment and microscopes. There is no national database for TB laboratory equipment and a plan for equipment services.
Laboratory staffs are trained in routine maintenance of microscopes, GeneXpert (Xpert MTB/RIF) systems and other relevant equipment during technical trainings. Routine maintenance is also inconsistent; it is either not done (sometimes due to lack of tools) or not recorded (sometimes due to lack of stationary).
6

2.7 Laboratory quality management systemsThe Quality Management System is aligned with National guidelines. There is an EQA program for AFB microscopy; however, there is no written plan or procedures which are described in training materials for EQA only. Safety aspects in TB laboratories are also addressed in every aspect of laboratory management. There is no national biosafety guideline for TB laboratories.
The total number of laboratories participating in the general SLMTA (Stepwise Laboratory Management Towards Accreditation) in the country is 45; in most of them the TB section is not part of the program. Six laboratories in the country are involved in TB SLMTA (the CTRL, Mbeya Referral, Kibong’oto Hospital, Public Health laboratory Pemba, Bugando Medical Centre and Dodoma Hospital) with support from FIND (Foundation for Innovative New Diagnostics). There is no existing structured plan for enrollment or preparation for enrollment of TB laboratories into the SLMTA program.
The EQA program for microscopy involves all three components: PT (proficiency testing), blinded re-checking (BR) of slides and on- site supervision visits. The total coverage of the laboratories by EQA is approximately 50%. Some laboratories are subscribed to PT panels from abroad e.g., UK-NEQAS (United Kingdom National External Quality Assessment Service). At the national level, PT for AFB microscopy is prepared and distributed by the National Health Quality Assurance Laboratory and Training Centre (NHQALTC) at laboratories request. Blinded re-checking is performed for district, health centers and dispensaries laboratories. The weakness of BR is there is no controller of the re-checker.Internal quality control (QC) for microscopy includes the use of positive and negative controls routinely (at least twice a week) and for freshly prepared stains and reagents.
Two culture laboratories (the CTRL and Mbeya) are supported by the SNRL (PTs and support supervision visits). PT for LPA is received from the UK-NEQAS. Zonal culture laboratories (except for Mbeya) do not receive proficiency testing for culture.
Proficiency testing for 100 GeneXpert laboratories was received from CDC (Centers for Disease Control and Prevention in Atlanta, USA) in 2017.
2.8 Management of laboratory commodities and suppliesSpecifications for procurement of supplies and equipment are provided by the CTRL based on the international standards.
Currently there are two operational procurement channels;a) Procurement done by the MSD (supplies for microscopy), andb) Procurement done by the NTLP in collaboration with partners (supplies for culture,
DST and molecular tests).At the moment, reagents for culture, DST and molecular tests are not in the MSD procurement list. The overall, quality standards are respected by the procuring bodies.
7

The MSD procures supplies centrally and distributes to the zonal branches of the MSD. The zonal MSDs distribute supplies to the district level and large hospitals. The Faith Based Hospitals and NGOs (Non-Government Organization) can procure supplies and commodities directly from the MSD. The MSD is equipped with cold chain delivery tools, very good storage facilities at the national and zonal levels and an electronic management system which can be used for placing orders. The supplies procured by the NTLP are distributed by the NTLP itself in collaboration with partners through the RTLCs and the DTLCs. At the regional and district level supplies are stored at pharmacies; some of them are not adequate for storage.
2.9 Laboratory information and data managementThe laboratory information system comprises of paper and electronic data capture tools. The paper based information tools consist of forms and registers at all facilities. The electronic system exists for the GeneXpert Management from facility to National level and TBLis at CTRL. In addition, NTLP has introduced a case based electronic TB and Leprosy registration (ETL) system.
2.10 Specimen referral system for the TB laboratory networkSpecimen collection and transportation are described in the NTLP manual for management of TB and Leprosy, TB microscopy handbook and Xpert MTB/RIF roll out plan. Sample collection manual is available at the CTRL and other health facilities i.e., Regional and District levels. Sample referral SOPs are available in a number of laboratories implementing QMS.
There are three systems for delivery of samples to laboratories: referral of patients, referral of slides (fixed sputum smears) prepared by community sputum fixers and referral of specimens. Specimens are referred to the zonal laboratories for culture. MTB Isolates are referred from Zonal TB labs to CTRL for DST. GeneXpert sites receive samples via contracted motorcyclists, other sites patients are referred. Referral of fixed sputum smears is not consistent throughout the country and is dependent on availability of funds. The Global Fund (GF) supports sputum fixers and referral of slides in 16 regions. Seven regions are supported by the Challenge TB project. Referral of specimens for culture is conducted by the DTLCs as requested from clinicians.
Specimens are transported by either facility vehicles or by the EMS (Expedited Mail Service) company. The EMS reaches as far as district headquarters but not peripheral levels. A revised EMS contract has been signed to include services in zonal TB laboratories and regional laboratories in transportation of samples. Occasionally, the Tanzania Post Office is also used for transportation of samples. The service reaches as far as the peripheral level but it has low capacity and the turnaround times are long. Culture specimens from sites that will have a transit time of more than 4 days can be transported in the presence of 1% CPC (Cetyl Pyridinium Chloride). Triple packaging is used for transportation of specimens and isolates;
8

however, biohazard signs are not always available to comply with requirements. Similarly, the use of cool boxes is not consistent.
Microscopy and Xpert MTB/RIF results are either collected by motorcyclists, patients, relatives or nurses or sent to the requesting facilities using the same channels as for specimen transportation. Culture and DST results are sent to the RTLCS who pass the results to the DTLCs (after recording the results) or to the requesting clinicians. The CTRL emails MDR TB results to the RTLCs and to the MDR TB focal person at the NTLP. Xpert MTB/RIF resistant results are reported directly via emails, SMS through the GxAlert system or called by the laboratory. Other GeneXpert laboratories that are yet not linked to the GxAlert system, inform the RTLCs and the DTLCs by phone calls or through SMSs using their private phones and airtime.Results on paper are sent by the CTRL via the EMS to the RTLCs and the RTLCs send the results to the DTLCs.
2.11 Operational research regarding the TB laboratory networkFollowing TB being among the top ten causes of morbidity and mortality in the country, it was included in health and research priorities set by the MoHCDGEC through the National Institute for Medical Research (NIMR) in 2013. The NTLP has the overall responsibility to support and utilize operational TB research findings to improve its performance. CTRL that is under the NTLP provides technical support in health research and involved in routine diagnosis and surveillance of drug resistant TB. Approximately 20% of the CTRL capacity is used for research projects and 80% for routine work. The CTRL provided technical support to the national prevalence survey (2012) and the ongoing DRS. The CTRL closely collaborates with stakeholders such as the NIMR, Ifakara Health Institute, Liverpool School of Tropical Medicine and other implementing partners such as KNCV. The laboratory participates in the World Bank (WB) multi-center research project on NTM for the East African Public Health Laboratory Network. CTRL is also part of UNDP (United Nations Development Program) led partnership on research on neglected diseases that also includes MDR-TB. Challenge TB supports the national TWG (Technical Working Group) coordinated by the CTRL to guide and advice on the performance of TB laboratories in Tanzania.
2.12 Legal and Policy reviewCTRL is under preventive services department of the Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC), all plans and operational guidelines are approved by MoHCDGEC.
2.13 Finances for TB laboratory servicesTB laboratory services are funded mostly by the government and development partners. Government funding is realized through Medium Term Expenditure Framework (MTEF) of MoHCDGEC, PO-RALG and CCHP of Local Government Authorities (LGA). The development
9

partners fund the services through Health Basket funds and individual Health initiatives. The Global Fund and PEPFAR are the major global initiatives that finance TB control interventions, laboratory services included. Some of the PEPFAR funds are channeled directly to support TB diagnostic activities however; most of the PEPFAR funds are channeled through international and local implementing partners such as KNCV and FIND. FIND provides technical assistance (TA) to roll-out of GeneXpert, procurement of instruments and supplies for GeneXpert and SLMTA process. KNCV through Challenge TB provides TA, GeneXpert instruments, cartridges and trainings in seven regions. It also seconded quality, safety and EQA officers to the CTRL to facilitate accreditation.
The Government’s contribution towards TB control is about 7% according to the Global TB report 2015. It supports human resources, infrastructure and supplies for TB microscopy; and in some regions maintenance of vehicles used for supervision. Finance for TB laboratory is managed by the NTLP and partners.
10

3.0 Development of the national TB Laboratory Strategic Plan
3.1 The purpose of the National TB Laboratory Strategic Plan
The National TB laboratory Strategic Plan (NTLSP) has been developed in support to strengthening, sustaining and maximizing input of TB laboratory network to TB control in Tanzania. The NTLSP is based on the “National Strategic plan (2015 – 2020) for Tuberculosis and Leprosy”, National Laboratory Strategic Plan, NTLP reports, prevalence surveys study - 2012, Drug Resistance Surveillance (DRS) 2007, Global TB reports and international guidelines. The TB Laboratory Strategic Plan represents a platform for coordinated support of TB laboratory strengthening by the government, partners and stakeholders.
3.2 Methodology for the development of Strategic PlanThe NTLSP (2018 – 2022) was developed through broad engagement of stakeholders at all levels of the TB laboratory network. The team was represented by the MoHCDGEC, NTLP, the CTRL, zonal, regional and district laboratories, RTLCs and DTLCs and partners (CDC, FIND, KNCV, PharmAccess). Technical support to the development was provided by KNCV TB laboratory consultant through Challenge TB project of the United States Agency for International Development (USAID). The Planning Tool: A Practical Handbook for National TB Laboratory Strategic Plan Development developed by TB CARE I/USAID in 2011 – 2012 was used as a template and a guide to the development of the first National TB Laboratory Strategic Plan 2018 - 2022 for Tanzania.
Based on the recommendations of the guide and review of the mentioned national guidelines, four objectives for the strategic plan were agreed upon by TB laboratory experts and stakeholders as follows:
1. Increase access to quality-assured AFB microscopy2. Improve the diagnosis of TB among AFB-negative cases especially among people
living with HIV3. Increase access to rapid laboratory diagnosis among presumptive and TB patients
considered at risk for M/XDR-TB4. Establish Laboratory Quality Management Systems
11

4.0 Strengths, weaknesses, opportunities and threats (SWOT) analysis
This section presents main findings of the SWOT analysis. For details refer to the resource documents file Annex 1.
Strength
1. Well-spread structured TB laboratory network (national, zonal, regional/ district and peripheral levels); CTRL is connected to SNRL in Antwerp
2. Good coverage of microscopy network (2.4 laboratories per 100,000 population); LED FM is implemented in 14.2% laboratories
3. Rapid molecular techniques implemented at national, zonal, regional and district levels
4. There are eight culture laboratories among them, two are conventional DST laboratories Second line drug testing is done in the country
5. Three culture laboratories equipped with negative pressure6. TB laboratories are equipped according to their levels; major equipment for culture
and DST is available7. Most of facilities are equipped with generators and tap water 8. EQA program established at all levels (strong system for blinded rechecking of
slides and existence of supervisory structure); private labs are included in EQA program
9. All culture/DST laboratories are building QMS; two zonal TB laboratories are accredited
10. Routine quality control is performed 11. Full time Quality Officers and Safety Officers at central, zonal, regional and district
levels12. Most of TB laboratory staff are governmental13. At least one staff in each of microscopy laboratories was formally trained; trained
staff at culture/DST and GeneXpert laboratories s are available 14. There are pool of ToTs and GeneXpert super-users at the national and regional
levels15. Standard national training materials, TB microscopy manual (ZN and FM) are
available16. Quality microscopes are procured from reliable manufacturers (e.g., Olympus) with
enough back-up equipment and spare parts.17. Some major equipment have service contracts and calibration of majority of
GeneXpert machines is routinely done.18. There were no major interruptions in microscopy and culture services due to
shortage of supplies in the recent few years; international standards are used for procurement
12

19. National data collection tools (request/report form and registers) are available and used
20. Culture laboratories are equipped with LIS; GxAlert monitoring system is being implemented
21. Triple packaging for sample transportation is used throughout the country; contracts for specimen transportation are available at central and some zones
22. CTRL developed research agenda for 5 years and conducts routine resistance surveillance
23. CTRL has strong links with research institutions and has capacity to provide technical support on operational research
24. There are general laboratory QMS auditors in the country
Weaknesses1. Large proportion (30%) of non-functional microscopy centers; low LED FM coverage 2. Limited access to culture and DST (molecular and conventional)3. Not all levels of the TB laboratory network function up to their scope (zonal
laboratories do not function yet for regions within the zones, only for the hospitals catchment areas)
4. Highly centralized supervision (high load on CTRL)5. Low coverage of microscopy laboratories by EQA (less than 50%)6. Inadequate communication and coordination in between levels of the network 7. Inadequate infrastructure of some culture laboratories e.g., limited space, testing is
done in the same room as office work, no negative pressure in five culture laboratories
8. Many GeneXpert laboratories and microscopy centers are not renovated and located in poorly maintained facilities
9. Many facilities do not have access to tap water, generators and incinerators; similarly few facilities are with unstable power voltage and water supply.
10. There is lack of national regulatory documentation: standards for infrastructure of TB laboratories, equipment and supplies; QA manual and EQA program; national SOPs
11. Training and re-training are not regular12. No mentorship program for new supervisors13. Routine and professional preventive maintenance are inconsistent (most of major
equipment do not have service contracts)14. There is no equipment database and maintenance plan for most of TB laboratories15. Quality laboratory performance indicators are mostly not monitored16. There is no national EQA program for culture, GeneXpert, LPA and DST laboratories17. Inadequate supervision of culture laboratories18. There is no structured plan of enrollment of TB laboratories into SLMTA program
13

19. Weak management of supplies (shortages and expiries due to poor quantifications and forecasting) and some supplies such as liquid culture, LPA are not in MSD list.
20. No electronic data flow at all levels in the network; the existing eLIS are not linked21. Long turnaround times for referral tests (delivery of specimens and reporting
results)22. Weak referral system in between periphery and district and in between districts23. Lack of standardized referral register for TB samples24. Transportation of isolates to CTRL do not meet biosafety requirements (no hard
box, not sealed etc.,)25. Knowledge gap of laboratory personnel on proposal writing and conducting OR
Opportunities
1. Wide coverage of diagnostic HFs at all levels2. Partners support and government commitment3. Involvement and ownership of Local Government in TB program (some local
governments authorities procure microscopes and involved in EQA activities)4. Existence of private laboratories for diagnosis of TB5. Existence of national quality assurance laboratory and Tanzania bureau of
standards6. Availability of development partners to support laboratory networks in the country7. Availability of reference materials and opportunities for training and technical
assistance8. National Health laboratory has standards for infrastructure of medical laboratories9. Availability of renovation plans at district health councils10. Establishment of workshops for medical equipment maintenance at zonal level and
existence of maintenance unit at MoHCDGEC11. A school for bioengineers is established12. Pre-service medical schools and universities which exists within the country13. Roll-out of SLMTA/SLIPTA program in the country14. Government supply system (MSD and zonal branches)15. Logistician at NTLP and laboratory officer at MSD are available16. DTLCs (monthly) and RTLCs (quarterly) visit health facilities and could be involved in
collection of sample based data17. Availability of various electronic means of communication in the market and
expansion of internet services in the country (most of the adult population has mobile phones)
18. Existence of national post and courier services, e.g., EMS (operates at regional level), private courier companies; postal services operate at district level while buses exists at the peripheral levels
19. Existence of parallel sample referral networks, e.g. early infant diagnosis and viral load (DNA, PCR)
14

20. District health information system is being implemented in all districts21. Existence of collaboration between NTLP/CTRL and other stakeholders such as
academic, research programs/institutions.22. Presence of national TWG
Threats
1. Cross border transmission of TB2. Excessive dependence on donors support and inadequate financing from the
Government3. Shortage of funds at district health councils for renovations and maintenance of
laboratory infrastructure4. No specific budget lines for CTRL and the network in the NTLP/Partners plan
(internet, airtime, landline telephone); lack of a system for laboratory petty cash for emergency issues
5. Lack of exit/sustainability plans of partners support6. Inadequate support to facilitate Zonal engineers to maintain TB Laboratory
equipment7. Certification of BSc using in country engineers are expensive than from abroad8. No Cepheid Authorized Service Provider (ASP) in the country9. Curriculum for TB training in pre-service personnel is inadequately updated based
on Global updates.10. High staff turnover and no lab staff retention plan11. Most courier services do not reach peripheral level12. Lack of internet connectivity in remote areas13. Lack local suppliers for TB reagents 14. There is no unique identifier for Tanzania citizen and for Presumptive TB.; same
person can get more than one Presumptive TB number15. National standards for lab infrastructure do not include specifications for TB labs
15

5.0 Key priority intervention areas and main activities in priority order
This section presents summary of priority areas and main activities derived from situational analysis framework by key challenges and specific areas with potential solutions. For details refer to resource documents file Annex 2.
Objective 1: Increase access to quality-assured AFB microscopy
Key priority intervention area: Increase microscopy capacity and accessibility through expansion of the network
TB microscopy network will be expanded through regaining of functionality of the existing non- functional laboratories and engaging private laboratories. Currently approximately 30% of the existing microscopy centers are not providing microscopy services. By 2022, 300 microscopy laboratories will be revived. Inventory (mapping) of the TB laboratory network will be conducted to establish coverage by regions and districts. Data on numbers of private and government laboratories in the areas will be received from the Tanzania association of private laboratories and the MoHCDGEC. The inventory data will be used for development of databases (infrastructure including biosafety issues, equipment, human resource etc.), planning (expansion, training, maintenance) and upgrading of the existing functional laboratories.
Infrastructure of laboratories will be upgraded through minor renovations including water, power supply (solar panels in the areas without access to electricity), incinerators and installation of furniture. Biosafety will be ensured by optimizing airflow (natural and/or mechanical). Electronic means for reporting of results will be implemented.
Quality of microscopy services will be enhanced through development of national manual for FM microscopy and internal quality assurance, establishing zonal training centers and harmonization of training curricular for AFB microscopy at medical laboratory colleges and universities. Data management plan and procedures will be developed and disseminated to improve data flow and troubleshooting. Capacity for preventive maintenance and small repair of microscopes will be increased through training of supervisors and provision of tools.
Key priority intervention area: Expand and improve EQA program for AFB microscopy by improving supervision through mentorship (pool of mentors)
EQA program for AFB microscopy will be re-structured through decentralization along the network. EQA services will be established at zonal laboratories to provide support to regions. Coverage of EQA program will be increased up to 95% by 2022. Expansion of the network will be guided by roll-out plan based on thorough nationwide assessment of the program. Quality of the program will be ensured through development of guidelines, SOPs, training, improved data flow and analysis at all levels and mentorship of supervisors. Infrastructure of
16

EQA centers will be improved by provision of furniture, office equipment, stationary and access to electronic means of communication.
17

Objective 2: Improve the diagnosis of TB among AFB-negative cases especially among people living with HIV
Key priority intervention area: Use of rapid techniques
The number of laboratories performing rapid testing with the use of GeneXpert MTB/RIF technology will be increased up to 300 by 2022. The laboratories will be placed in renovated facilities which will be equipped with back-up power supply and furniture. Biosafety will be improved by optimizing airflow (natural and/or mechanical) and provision of mobile incinerators. Training will be standardized in all areas through the use of the national training materials. Management of supplies and commodities for GeneXpert will be enhanced through centralization of quantification, procurement and distribution (leading role of NTLP and engaging MSD) and quantification of consumption-based management. Routine and professional maintenance of GeneXpert systems will be improved through monitoring and provision of service contracts (warranties) based on maintenance procedures and plans. Data management will be improved through expansion of the use of GxAlert remote monitoring technology. The use of the data collected will be improved by routine regular monitoring and troubleshooting at all levels guided by M&E plan and SOPs. Supervision of GeneXpert laboratories will be strengthened through mentorship approach.
Key priority intervention area: Establish reliable specimen referral system at all levels
National regulatory documentation for specimen collection and transportation will be developed and disseminated. A situational analysis will be conducted on availability transportation services at all levels (peripheral health facility – district/big hospital where GeneXpert laboratories are located) including hospital vehicles. Specimen transportation means and schedules specific for districts will be developed. Performance of the transportation channels will be monitored through turnaround times by facilities and districts. Service contracts will be procured wherever available and fuel to facilities vehicles will be provided. Electronic means will be used for reporting of positive and resistant results.
18

Objective 3: Increase access to rapid laboratory diagnosis of drug-resistant TB among presumptive and TB patients considered at risk of M/XDR-TB
Key priority intervention area: Capacity building)
A standardized training curriculum for new technologies (LPA, GeneXpert, etc.,) have been developed with materials endorsed by the MoHCDGEC in 2017. In addition to this implementation of quarterly targeted supervision and mentorship should be re-enforced and scaled up until proficiency is sustained for identification and linkage of patients considered at high risk of M/XDR - TB.
Key priority intervention area: Supply chain management
Laboratory commodities and supplies needed for rapid tests should be procured and planned for calibration and maintenance services timely. Currently procurement of laboratory commodities, supplies and equipment of new technologies is done vertically at the programme level. During this next strategic period of 2018 - 2022, NTLP should incorporate procurement and supply of commodities needed for rapid tests (LPA, GeneXpert) into the normal national procurement and supply system. This intervention area is further described in objective 2 above.
Objective 4: Establish Laboratory Quality Management Systems
Key priority intervention area: Accreditation of TB laboratories
Currently there is one public TB laboratory (Mbeya) that has been accredited. In this strategic plan 2018 – 2022, CTRL and all zonal TB laboratories should implement QMS in order to be accredited. In addition, the laboratory network (AFB microscopy laboratories) will aim to improve the standards to reach GLI standards needed for accreditation.
Key priority intervention area: Optimize the existing laboratory information system
In this plan, the QMS should be optimized to capture all TB laboratory indicators from the peripheral level to the national level. Also create linkage and network for monitoring of all laboratory indicators within the TB network i.e., peripheral, regional, zonal and national.
Key priority intervention area: Conduct operational research
Conduct OR based on QMS to address key issues affecting quality delivery of TB diagnostics rolled out based on the need/ gaps identified within the network e.g., microscopy, culture, DST and new technologies. These OR will be reviewed and contribute to improve service delivery in the country.
19