· List of Allergies: MEDICATIONS: Do you take any medications or vitamins regularly? Yes PAST...
6
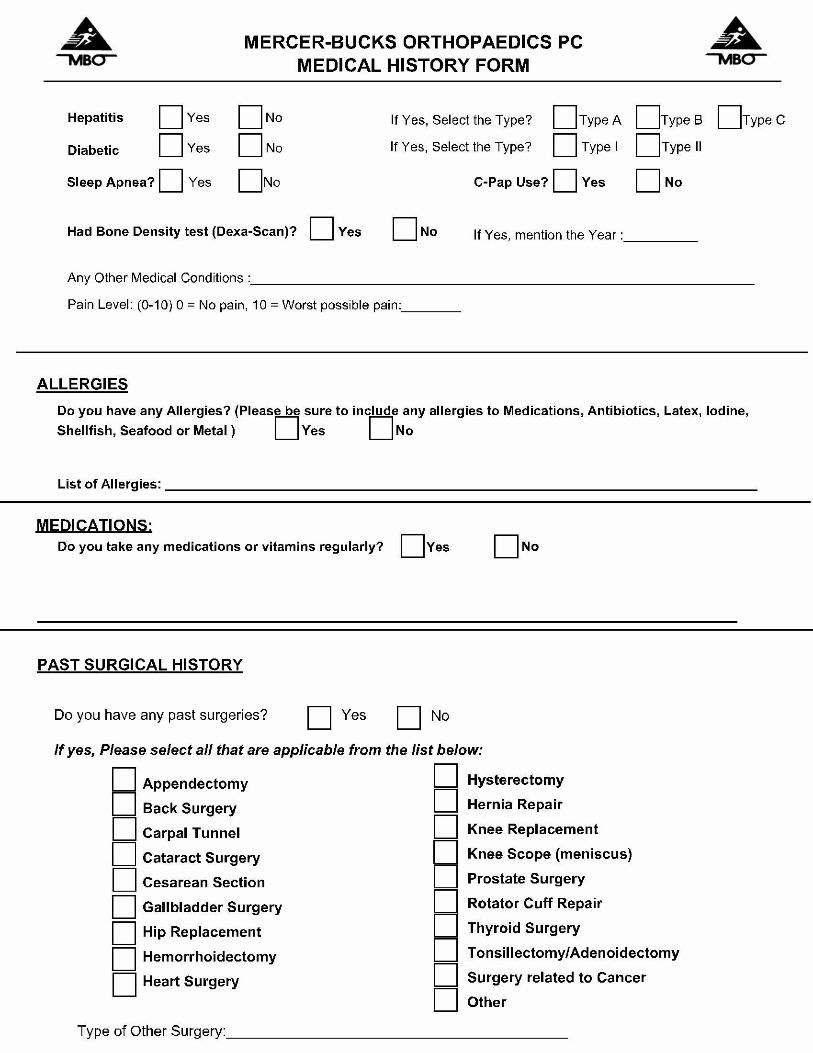
· List of Allergies: MEDICATIONS: Do you take any medications or vitamins regularly? Yes PAST SURGICAL HISTORY Do you have any past surgeries? Yes If yes, Please select all that