Embed Size (px)
DESCRIPTION
LIPIDS: VITAMIN A IN THE EYE & OCULAR LIPID STORAGE DISEASES. Class 9 Vitamin A and lipid storage disease. In this lecture, we take up two diverse topics: the roles of vitamin A in the eye and another set of storage diseases – lipid storage diseases. OUTLINE: - PowerPoint PPT Presentation
Citation preview

LIPIDS: VITAMIN A IN THE EYE &OCULAR LIPID STORAGE DISEASES
Class 9 Vitamin A and lipid storage disease

In this lecture, we take up two diverse topics: the roles of vitamin A in the eye and another set of storage diseases – lipid storage diseases.
OUTLINE:1)Vitamin A and all of its chemical forms2)Uptake and transport of Vitamin A3)Role of Vitamin A in the cornea4)Role of Vitamin A in the retina5)Vitamin A nutrition and toxicology6)More storage diseases: glycolipidoses & sphingolipidoses

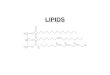
VITAMIN A

The most common forms of vitamin A are shown in the table below:
R
R
NOTE: This is the all-trans form. Most isomerization takes place at carbon 11. 1
3
5
7 9 11 13 15
This is also done at the cell nucleus.

Protonated Schiff base
In addition to the forms just shown, it must be remembered that the aldehydeform must exist in the 11-cis form (figure shown above) in order to be triggeredby light while bound toopsin (as rhodopsin).Note also that the opsin and retinal arebound to each other asa protonated Schiffbase . Just before releasefrom its protein, the11-cis form is isomerizedto the all-trans form. This,in essence, induces aconformational change in the opsinportion of the complexand achieves twogoals: 1) forcedseparation of thetwo molecules; and2) a conformational change in opsin that allows it to interact with the G-proteinknown as transducin.

Vitamin A is taken up as -carotene (fromvegetables) and retinyl esters (from animals). Ultimately converted to retinol, it is re-esterified in the intestine and incorporated into chylomicrons for transport to the liver.
* yellow/ red types: carrots, tomatoes, squash, etc.

Since vitamin A is a lipid soluble vitamin, it shares some of the transport features that are common to other lipids. This was seen in the transport to the liver cells (as shown). However, when vitamin A leaves the liver, it is bound to 2 proteins: a retinol bindingprotein (RBP) and aprealbumin (PA). This isimportant since failureto build up these proteincarriers in vitamin deficient states FAILS tosolve the vitamin deficiency.When vitamin A arrives at itstarget cells (including pigmentepithelial cells) the vitamin is bound to a cell retinol bindingprotein (CRAB) and stored either as an ester or converted toa useful form such as retinoic acid.

How vitamin A is transported within the retina has some importance for preserving vision. Unlike cervonic acid (in either its bound form or as a phospholipid), vitamin A istransported to the PE cell where it is catalyzed to 11-cis retinal before it is transported to the photorecep-tors. The PE cells act as a depotfor vitamin A. They receive vitaminA from both the blood and the photoreceptor. In the diagram, the small (t) indicates that a transport protein moves the vitamin whereas the * indicates an enzyme catalyzed reaction. Not indicated is the existence of inter-photoreceptor retinal binding proteins needed for transport.

The role of vitamin A at the corneal surface:
The destruction of the corneal epithelium (keratomalacia or a melting cornea) has been associated with malnutrition fornearly all of recorded history. A link of this condition to a deficiency in vitamin A malnutrition was made when it was learned that:
1)epithelial proteins were not being synthesized sufficiently;2)vitamin A bound to the DNA which makes these proteins.
Malnutrition related to vitamin A deficiency in underdevelopedcountries and in developed countries (e.g., alcoholics) havecaused over 5 million cases of xeropthalmia (dryness of thecorneal and conjunctiva) and 500,000 cases of blindnessworldwide each year. Specifically, the proteins lacking are:mucins (MUC-1,MUC-4, and MUC-16). This lack causesthe cornea to be both hardened and structurally weakendwhile it also becomes cloudy.

Shown at right is a generalized mucin structurewith oligosaccharides and protein interaction sites. The oligosaccharides give the proteins a viscous property while allowing the surface toremain moist.
In the lower picture areseen the location of threekinds of mucins: MUC-16(red); MUC-4 (green); andMUC-1 (blue). The MUCsprovide an anchor for theaqueous layer (acting asa glycocalyx). These proteins are considered tobecome deficient withdecreased vitamin A.


These are examples of what can happen with extreme vitamin A deficiency.

Vitamin A stimulates protein synthesis in the same manner as steroid hormones and T4 – T3. The vitamin binds to a protein located exclusively in the cell nucleus. After vitamin A binds to its protein (red arrow),the protein binds tothe enhancer regionof DNA. Meanwhile,RNA polymerase binds to its promoterregion (green arrow).The long region ofthe binding protein(blue arrow) bindsto the RNA polymeraseand signals for the beginning of transcription. There are atleast four different receptor proteins for vitamin A in the cornea.

ADDITIONAL INFORMATION ABOUT VITAMIN A:
Just like drugs, vitamin A can be toxic if you ingest too much. This was first discovered by hunters who consumed polar bear livers some years ago. Symptoms include: nausea, vomiting, blurred vision even hair loss and anemia. A question for study: what effect is caused in the retina whenlevels of vitamin A are decreased? This question will appeared in an exam.

LYSOSOMAL STORAGE DISEASESIn addition to mucopolysaccaridoses, there are other storage diseases that involve lipids and glycolipids and also are caused by enzyme defects. They are mentioned since ocular defects may occur with them.

WHAT IS THE “CHERRY RED SPOT” THAT MAY OCCUR IN STORAGE DISEASES INVOLVING LIPIDS?
The area surrounding the red spot is filled with gangliosides that have accumulated in the retina as the result of one of these diseases. Note the whitish area immediately surrounding the red spot (blue arrow). This area is composed of retinal neurons filled with these gangliosides. The red area is the fovea that is normal and has no neurons. It only shows the red circulation of the choroid and appears red.

GAL
hexosaminodase a (deficient)
x
galactosidase
An example is Tay-Sach’s disease. It was discovered in the late 1800’s andusually is the result of a deficiency of hexoaminodase a (HEXA gene). It occursin Ashkenazi Jews, Cajuns and French Canadians. This is a mucolipidoses inwhich GM2 accumulates in neural tissue and destroys neural cells in both the brain and neural retina. The accumulated ganglioside is shown below. The patients begin to experience death of their brain cells by about 6 mos. and usually do not live beyond 5 yr. There is no cure or treatment. The first degradative step is normal and involves the catalytic removal of galactose. Thenext step involves hexosaminodase A. That enzyme is deficient.

I-CELL DISEASE
This disease is a muco-lipidoses that is of interest due to its biochemical mechanism. The disease resembles Hurler’s disease in symptoms and outcome.However, it occurs due to a defect in a “packaging” enzyme that prepares -galactosidase for transport to its lysosome. The enzyme:N-acetylglucosamine 1-phosphotransferase is genetically defective and is needed to add a phsophate group to a mannose sugar on the galactosidase as a signal to move it to lysosomes.

SUMMARY AND STUDY GUIDE:1) What two roles can be assigned to vitamin A in the eye?2) What are the four kinds of vitamin A and their general functions?3) What does isomerization of 11-cis to all-trans vitamin A do to its existence in the rhodopsin molecule?4) Describe the forms and intake of vitamin A into the body and its distribution to its target cells. What carrier proteins are involved?5) Describe the role of pigment epithelial cells in the uptake, storage and distribution of vitamin A in the retina.6) Can you identify each of the following in regard to the deficiency o f vitamin A in the eye? -- keratomalacia; xerophthamia (or xerosis); nyctalopia. 7) What are MUC proteins? What do they do and why is vitamin A of any significance to them?8) Describe the mechanism used to synthesize MUC RNA when controlled by vitamin A.9) Describe the cherry red spot and its surroundings when seen in a fundus photograph. Why is it not seen in a mucopolysaccaridosis?10) What is Tay-Sach’s disease and how does it occur biochemically?11) What is the unusual biochemical pathology of I-cell disease?





![[PPT]Lipid Transport & Storage - qums.ac.ireprints.qums.ac.ir/302/1/Lipid Transport & Storage-86.ppt · Web viewLipid Transport and Storage * Lipid transport & storage * LIPIDS ARE](https://img.pdfslide.us/doc/110x75/5aa076f27f8b9a67178e435e/pptlipid-transport-storage-qumsac-transport-storage-86pptweb-viewlipid-transport.jpg)