Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Lipid-peroxidation and peroxiredoxin-overoxidationin the erythrocytes of non-insulin-dependent type 2diabetic men during acute exercise
Christian Brinkmann • Jenny Blossfeld • Martin Pesch • Bastian Krone •
Kathrin Wiesiollek • Dario Capin • Georgina Montiel • Martin Hellmich •
Wilhelm Bloch • Klara Brixius
Received: 1 July 2011 / Accepted: 30 September 2011 / Published online: 18 October 2011
� Springer-Verlag 2011
Abstract Single bouts of exercise induce an acute state of
oxidative stress. It is largely unknown what this means in the
context of diseases which are associated with increased
oxidative stress, e.g., type 2 diabetes mellitus (T2DM). Free
radicals can destroy the structure of erythrocytes and reduce
their deformability. Antioxidative peroxiredoxins are highly
abundant in erythrocytes. Therefore, we immunohisto-
chemically examined whether the free radical-induced
erythrocyte lipid-peroxidation measured by 8-iso-prosta-
glandin-F2a (8-Iso-PGF) as well as the erythrocyte con-
tents of overoxidized peroxiredoxins (PRDX-SO2–3)
differ between overweight/obese T2DM men (n = 15,
years = 59 ± 10 (mean ± SD)) and overweight/obese
non-diabetic control subjects (n = 12, years = 53 ± 4)
during acute exercise (WHO-step test). We further studied
whether physical training affects the oxidative stress
response to acute exercise. Seven men belonging to the
diabetic group took part in a moderate intensity cycling
endurance training. Erythrocyte 8-Iso-PGF significantly
increased during acute exercise and decreased in the 30-min
recovery phase in untrained diabetic and non-diabetic men
(P B 0.05). Increases/decreases in 8-Iso-PGF in relation to
exercise/recovery time were similar in both groups. A sig-
nificant exercise-induced increase in the contents of eryth-
rocyte PRDX-SO2–3 was only observed in T2DM men
(P B 0.05). PRDX-SO2–3 contents were not reduced during
recovery. Following physical training, the magnitude of
exercise-induced increases in 8-Iso-PGF (relative to exercise
time) was significantly lower in the erythrocytes of T2DM
men (P B 0.05), whereas increases in PRDX-SO2–3 were
significantly higher (P B 0.05). Exercise-induced erythro-
cyte lipid-peroxidation is similar in untrained overweight/
obese T2DM patients and overweight/obese control sub-
jects, while antioxidative mechanisms differ. Physical
training might improve oxidative stress in T2DM men’s
erythrocytes during acute exercise.
Keywords Oxidative stress � Exercise � Type 2 diabetes �Erythrocytes � Lipid-peroxidation � Peroxiredoxin
Introduction
In patients suffering from type 2 diabetes mellitus (T2DM),
oxidative stress (the imbalance between free reactive oxygen
species (ROS) and the antioxidative defense capacity) can
induce/potentiate different secondary complications, e.g.,
cardio-vascular illnesses (Rains and Jain 2011).
The increased autoxidation of glucose, an intensified
formation of advanced glycation products, an elevated
activation of the polyol-pathway, mitochondrial ROS-pro-
duction as well as the increased activity of NADPH-oxi-
dases can be responsible for a considerable amount of free
radicals in T2DM subjects (Brownlee 2001; Inoguchi et al.
Communicated by Susan A. Ward.
C. Brinkmann (&) � J. Blossfeld � M. Pesch � B. Krone �K. Wiesiollek � D. Capin � W. Bloch � K. Brixius
Department of Molecular and Cellular Sport Medicine,
Institute of Cardiovascular Research and Sport Medicine,
German Sport University Cologne, Am Sportpark
Mungersdorf 6, 50933 Cologne, Germany
e-mail: [email protected]
G. Montiel
Department of Preventive and Rehabilitative Sport Medicine,
Institute of Cardiovascular Research and Sport Medicine,
German Sport University Cologne, Cologne, Germany
M. Hellmich
Institute of Medical Statistics, Informatics and Epidemiology,
University of Cologne, Cologne, Germany
123
Eur J Appl Physiol (2012) 112:2277–2287
DOI 10.1007/s00421-011-2203-x
2000; Kaneto et al. 2010; Wolff and Dean 1987). In
addition, there is growing evidence that the antioxidative
capacity is weakened in patients exhibiting T2DM, since
reduced activity of antioxidative enzymes, e.g., of super-
oxide dismutase (SOD), catalase (CAT) and glutathione
peroxidase (GPX) has been reported (Bhatia et al. 2003;
Memisogullari et al. 2003).
Thus, numerous publications have demonstrated
increased systemic oxidative stress levels in T2DM
patients in blood plasma compared with non-diabetic
control subjects (Collier et al. 1992; Osuntokl et al. 2007;
Pandey et al. 2010; Sato et al. 1979).
Single exercise bouts can increase oxidative stress,
among others, probably attributable to a rise in mitochon-
drial ROS-production, as well as in the ROS-generation
resulting from the autoxidation of oxyhemoglobin, oxy-
myoglobin, catecholamines or the activity of xanthine- and
NADPH-oxidases (Cooper et al. 2002; Fisher-Wellman and
Bloomer 2009).
Red blood cells are confronted with ROS generated by
the intracellular autoxidation of hemoglobin or coming
from the extracellular plasma. In the situations of high
oxidative stress, the structure of erythrocytes can be neg-
atively affected and their deformability which is essential
to pass through small capillaries can be reduced (Minetti
et al. 2007). Moreover, Minetti et al. argue that red blood
cells could turn into harmful ‘‘pro-oxidant bullets’’
spreading oxidative stress throughout the entire body when
ROS are not sufficiently buffered by the antioxidative
system. To protect themselves from oxidative damage,
erythrocytes are characterized by a strong endogenous
antioxidative capacity. It has, therefore, been asserted that
red blood cells can even help lower systemic oxidative
stress by taking up and metabolizing peroxides from the
extracellular plasma (Cho et al. 2010; Winterbourn and
Stern 1987).
Peroxiredoxins are highly abundant antioxidative pro-
teins in erythrocytes. Most of them are only slowly recy-
cled/reduced by the thioredoxin system (Low et al. 2008).
It has, thus, been demonstrated in erythrocytes in vitro that
peroxiredoxins can be overoxidized in the situations of
high amounts of free radicals (Cho et al. 2010). To date,
little is known about the activity of these antioxidative
enzymes in T2DM patients’ red blood cells.
In accordance with the abovementioned aspects, Villa-
Caballero et al. (2000) hypothesized that exercise with an
incremental workload induces an increase in oxidative
stress in both T2DM and non-diabetic control subjects,
with more rapid and higher increases observable in T2DM
patients. This might be harmful, especially for the exer-
cising diabetic subjects. However, training was thought to
reduce exercise-induced increases in oxidative stress in
T2DM patients especially due to an up-regulation of the
antioxidative capacity in the long-term. This topic has thus
far been researched quite sparsely and no research group, to
our knowledge, has examined oxidative stress levels in red
blood cells of T2DM patients during acute exercise,
although erythrocytes have been assigned a central role for
the redox homeostasis in the cardio-vascular system
(Nikolaidis and Jamurtas 2009).
Therefore, the aim of the present study was to examine
the influence of acute exercise on erythrocyte oxidative
stress in untrained/trained T2DM patients and non-diabetic
control subjects. We performed immunohistochemical
stainings using antibodies for the lipid-peroxidation marker
8-iso-prostaglandin-F2a (8-Iso-PGF) which has been
established as being a valid marker for oxidative stress
and free radical-dependent cell damages (Basu 1998; Pra-
tico et al. 2004; Roberts and Morrow 2000). In addition,
exercise-induced changes in the contents of overoxidized
peroxiredoxins (PRDX-SO2–3) were quantified immuno-
histochemically to better understand the functioning of
peroxiredoxins as very important antioxidants in red blood
cells.
Methods
The protocol for the research project was approved by a
suitably constituted Ethics Committee of the German Sport
University before the investigation. It conformed to the
provisions of the Declaration of Helsinki. Written informed
consent was obtained from all subjects.
Subjects
Male subjects were recruited via a newspaper ad. The
inclusion criteria required the subjects to belong to an age
group of around 50 years and be overweight/obese. The
diabetic patients were to exhibit non-insulin-dependent
type 2 diabetes (diagnosed by the family physician (crite-
ria: fasting glucose values C126 mg/dl, HbA1c value C6%
and/or 2 h oral glucose tolerance test indicating glucose
levels C200 mg/dl)). Finally, a total of 15 diabetic men
took part in the study. They declared that neither diabetic
complications nor any cardio-vascular diseases (apart from
well-controlled hypertension, n = 11) had ever been
diagnosed. The duration of the diabetic disease had been
6 ± 7 years (self-report). Within the control group, 12
non-diabetic men were studied for comparison. The sub-
jects’ characteristics are presented in Table 1. Diabetic and
non-diabetic control subjects did not significantly differ in
age, body mass index (BMI) or physical fitness in order to
exclude the influence of age, overweightness, physical fit-
ness when analyzing oxidative stress between the two
groups and to focus on the influence of type 2 diabetes.
2278 Eur J Appl Physiol (2012) 112:2277–2287
123

Fasting glucose values in blood serum indicating the cur-
rent glycemic status were significantly higher in the dia-
betic than in the control group. Most of the subjects were
taking medications during the investigation period. Medi-
cation intake and the subjects’ health condition are shown
in Table 2. It was determined by questionnaire that none of
the subjects had regularly exercised during the last 3 years
before the commencement of the study.
Study design
The erythrocyte oxidative stress response to an acute bout
of exercise was compared between untrained T2DM men
and non-diabetic control subjects. Accordingly, venous
blood was collected before, immediately after the WHO-
step test on a bicycle ergometer and 30-min post-exercise.
In addition, venous blood that was collected under resting
conditions was used to compare basal oxidative stress in
the erythrocytes of T2DM men with that of non-diabetic
control subjects. Furthermore, the effect of regular physical
activity on exercise-induced erythrocyte oxidative stress
was investigated. The subjects of the diabetic group were
asked to participate in a cycling endurance training for 3
months. The training program started 3 days after the
initial performance test. The patients were instructed not to
change their dietary habits and medication-intake during
the training intervention. The WHO-step test was per-
formed once again 3 days after the end of the training
period. Venous blood was collected in accordance with the
same principles as before the training.
Endurance training
Seven diabetic patients (Table 3) took part in the endur-
ance training program. The exercise regimen was designed
based on experiences from previous studies involving
training for diabetic subjects (Sigal et al. 2004). Accord-
ingly, the diabetic subjects were instructed to take part in a
supervised cycling endurance training 3 times a week on
non-consecutive days. Subjects were encouraged to train
on their own (walking or Nordic walking after initial pro-
fessional instruction) when they missed a training session.
We documented that patients participated in at least 90% of
the training sessions. The training intensity was about 75%
of the maximal heart rate (220-age beats/min). The training
bouts (effective time of performance) continuously
increased from a duration of 25 min in the first week to
50 min in the last.
Performance diagnostics
An endurance test was performed on the upright bike
‘‘Ergometrics900’’ (Ergoline, Bitz, Germany) coupled with
an ECG (‘‘Ergoscript EK3012’’, Ergoline). During exer-
cise, respiratory gas measurement was done using the
‘‘ZAN 600 USB’’ system (nSpire Health, Longmont, Col-
orado, USA). Subjects were tested with the following
stopping criteria: muscular exhaustion, angina pectoris,
ischemia, paleness, cyanosis, arrhythmia, respiratory
insufficiency, hypertension (systolic blood pressur-
e [250 mmHg or diastolic blood pressure [115 mmHg),
aberration, dizziness and/or co-ordination problems. Start-
ing at 25 W resistance, the intensity gradually increased by
25 W every 2 min (WHO-step test). VO2peak was deter-
mined as the highest oxygen uptake during performance.
The consumption of caffeine was not permitted within 12 h
before testing. The subjects were always tested at the same
time of day and were instructed not to engage in physically
exhausting activities 24 h before the measuring.
Erythrocyte preparation and immunohistochemistry
Immunohistochemistry is a standard procedure used in cell
biology that has proven successful in the semiquantitative
analysis of proteins in erythrocytes (Fischer et al. 2007; Suhr
et al. 2009). Both the protocol for the fixation of erythrocytes
as well as the standard immunohistochemical protocol were
similar to those used by Suhr et al. (2009). Immunohisto-
chemical stainings were carried out with the following pri-
mary antibodies in the main fields of cell-covered slides:
8-Iso-PGF IgG polyclonal (Acris, Hiddenhausen, Germany)
as the lipid-peroxidation marker and PRDX-SO2–3 IgG
monoclonal (AbFrontier, Seoul, Korea) detecting two forms
of overoxidized peroxiredoxins, those with the cysteine
Table 1 Subjects’ characteristics: comparison of data from non-diabetic male control subjects (CON) and men suffering from type 2 diabetes
mellitus (T2DM)
Age (years) BMI (kg/m2) Fasting glucose (mg/dl) VO2peak (ml/min/kg)
Untrained CON 53 ± 4 30 ± 2 94 ± 9 23.9 ± 5.4
Untrained T2DM 59 ± 10 32 ± 4 163 ± 43* 22 ± 4.9
Values are means ± SD
BMI body mass index, VO2peak highest oxygen consumption
* Significantly different from control subjects (P B 0.05)
Eur J Appl Physiol (2012) 112:2277–2287 2279
123
sulfinic acid (CP-SO2H) and those with the cysteine sulfonic
acid (CP-SO3H). The antibodies were used with a dilution of
1:1,500 (8-Iso-PGF) and 1:200 (PRDX-SO2–3). The primary
antibodies were absent for a negative immunohistochemical
control (IHC-C) which was separated from the main field on
the slides. For the intensity analysis of immunostaining, the
gray values [DU = density unit] of at least 40 erythrocytes
from at least 5 randomly selected areas of each slide were
measured in the main field. At least 10 erythrocytes from at
least 2 randomly selected areas were measured in the IHC-C.
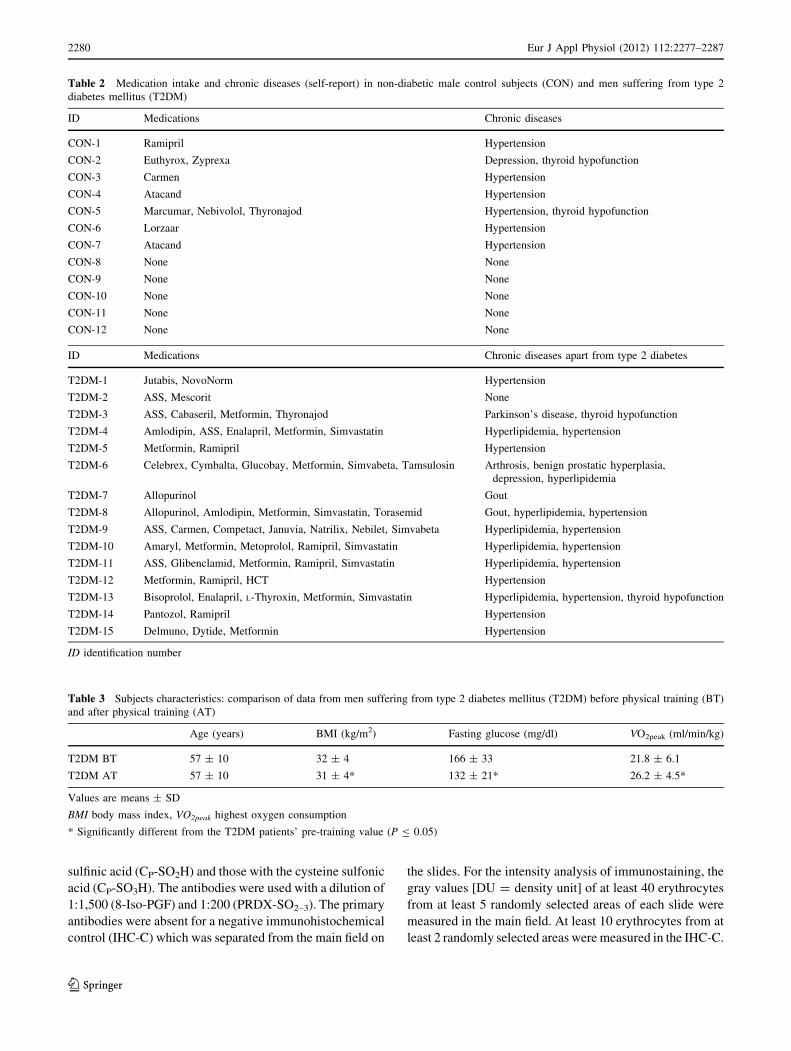
Table 2 Medication intake and chronic diseases (self-report) in non-diabetic male control subjects (CON) and men suffering from type 2
diabetes mellitus (T2DM)
ID Medications Chronic diseases
CON-1 Ramipril Hypertension
CON-2 Euthyrox, Zyprexa Depression, thyroid hypofunction
CON-3 Carmen Hypertension
CON-4 Atacand Hypertension
CON-5 Marcumar, Nebivolol, Thyronajod Hypertension, thyroid hypofunction
CON-6 Lorzaar Hypertension
CON-7 Atacand Hypertension
CON-8 None None
CON-9 None None
CON-10 None None
CON-11 None None
CON-12 None None
ID Medications Chronic diseases apart from type 2 diabetes
T2DM-1 Jutabis, NovoNorm Hypertension
T2DM-2 ASS, Mescorit None
T2DM-3 ASS, Cabaseril, Metformin, Thyronajod Parkinson’s disease, thyroid hypofunction
T2DM-4 Amlodipin, ASS, Enalapril, Metformin, Simvastatin Hyperlipidemia, hypertension
T2DM-5 Metformin, Ramipril Hypertension
T2DM-6 Celebrex, Cymbalta, Glucobay, Metformin, Simvabeta, Tamsulosin Arthrosis, benign prostatic hyperplasia,
depression, hyperlipidemia
T2DM-7 Allopurinol Gout
T2DM-8 Allopurinol, Amlodipin, Metformin, Simvastatin, Torasemid Gout, hyperlipidemia, hypertension
T2DM-9 ASS, Carmen, Competact, Januvia, Natrilix, Nebilet, Simvabeta Hyperlipidemia, hypertension
T2DM-10 Amaryl, Metformin, Metoprolol, Ramipril, Simvastatin Hyperlipidemia, hypertension
T2DM-11 ASS, Glibenclamid, Metformin, Ramipril, Simvastatin Hyperlipidemia, hypertension
T2DM-12 Metformin, Ramipril, HCT Hypertension
T2DM-13 Bisoprolol, Enalapril, L-Thyroxin, Metformin, Simvastatin Hyperlipidemia, hypertension, thyroid hypofunction
T2DM-14 Pantozol, Ramipril Hypertension
T2DM-15 Delmuno, Dytide, Metformin Hypertension
ID identification number
Table 3 Subjects characteristics: comparison of data from men suffering from type 2 diabetes mellitus (T2DM) before physical training (BT)
and after physical training (AT)
Age (years) BMI (kg/m2) Fasting glucose (mg/dl) VO2peak (ml/min/kg)
T2DM BT 57 ± 10 32 ± 4 166 ± 33 21.8 ± 6.1
T2DM AT 57 ± 10 31 ± 4* 132 ± 21* 26.2 ± 4.5*
Values are means ± SD
BMI body mass index, VO2peak highest oxygen consumption
* Significantly different from the T2DM patients’ pre-training value (P B 0.05)
2280 Eur J Appl Physiol (2012) 112:2277–2287
123

Finally, the intensity of immunostaining (for all erythrocytes
of an individual) was determined as follows:
Arbitrary gray value¼ 1
40
X40
i¼1
ðerythrocyte gray valuemain field i
� background gray valuemain field iÞ
� 1
10
X10
j¼1
ðerythrocyte gray valueIHC�Cj
� background gray valueIHC�CjÞ
The background gray value was measured in a cell-free
area of the slide. For comparative analyses, only values of
erythrocytes incubated in the same immunostaining
procedure (under identical conditions) were chosen. For
staining intensity detection, a light microscope (‘‘Axiophot’’,
Zeiss, Jena, Germany) coupled to a video camera (‘‘3CCD’’,
Sony, Tokio, Japan) was used together with the ‘‘KS300’’
software (Zeiss). The analysis was conducted using the
software ‘‘Image J’’ (National Institutes of Health, Bethesda,
Maryland, USA). The magnification was 4009.
Statistical analyses
Data are presented as mean values ± standard deviations
(SD). Non-parametric (rank-based) hypotheses tests
were used throughout as normality of continuous data
distributions seemed questionable (skewness, outliers).
Specifically, the Friedman ANOVA was performed for
repeated measures. If found statistically significant,
implemented post-hoc tests for multiple pairwise compar-
isons were conducted (Bonferroni corrected). Moreover,
unpaired samples of diabetic and non-diabetic men were
compared by the Mann–Whitney U test, paired data (pre-
vs. post-training values) using the Wilcoxon signed rank
test. P values B0.05 were found to indicate statistical
significance. All statistical analyses were carried out using
the ‘‘SPSS 18.0’’ program (PASW Statistics, SPSS Inc.,
Chicago, Illinois, USA).
Results
Exercise-induced lipid-peroxidation and peroxiredoxin-
overoxidation in the erythrocytes of untrained non-
insulin-dependent T2DM patients and
untrained non-diabetic control subjects
We first examined how lipid-peroxidation (as measured by
8-Iso-PGF) as well as the peroxiredoxin-overoxidation
(PRDX-SO2–3) in the erythrocytes of T2DM men change
during acute exercise. In both type 2 diabetic and non-
diabetic men, statistical analysis revealed significant
changes in erythrocyte 8-Iso-PGF contents over time
(Fig. 1): the density of 8-Iso-PGF significantly increased
during acute exercise and significantly decreased in the
Fig. 1 a Density of 8-Iso-PGF and PRDX-SO2–3 at rest, immedi-
ately after the WHO-step test and at 30-min recovery in non-diabetic
male control subjects (CON) and men suffering from non-insulin-
dependent type 2 diabetes mellitus (T2DM). Values are means ± SD.
�Significantly different from at rest (P B 0.05). �Significantly differ-
ent from immediately after exercise (P B 0.05). b Original photos of
the 8-Iso-PGF and PRDX-SO2–3 immunohistochemical stainings
Eur J Appl Physiol (2012) 112:2277–2287 2281
123

following 30-min recovery nearly to the level before
exercise. The density of overoxidized peroxiredoxins
(PRDX-SO2–3) significantly changed over time in T2DM
patients’ erythrocytes, but not in non-diabetic control
subjects’ red blood cells (Fig. 1). We observed a significant
increase in PRDX-SO2–3 contents during acute exercise in
T2DM men. Following a 30-min recovery period, PRDX-
SO2–3 levels were still increased compared with the levels
at resting conditions. Neither increases in erythrocyte
8-Iso-PGF levels during the WHO-step test (in relation to
the individual exercise time during the WHO-step test) nor
decreases in 8-Iso-PGF levels during recovery significantly
differed between T2DM patients and control subjects
(Fig. 2).
We were interested in determining whether the detected
similarities/differences in the oxidative stress response
during acute exercise between T2DM men and non-dia-
betic control subjects were possibly associated with simi-
larities/differences in the basal oxidative stress status.
Therefore, we examined 8-Iso-PGF levels in the erythro-
cytes and found no significant differences for erythrocyte
8-Iso-PGF in T2DM patients and control subjects at resting
conditions (Fig. 3).
Exercise-induced lipid-peroxidation and peroxiredoxin-
overoxidation in the erythrocytes of non-insulin-
dependent T2DM patients before and after
physical training
To determine whether regular physical training can affect
acute exercise-induced lipid-peroxidation and peroxir-
edoxin-overoxidation in the erythrocytes of T2DM
patients, we immunohistochemically analyzed erythrocytes
from blood taken after 3 months of endurance training. As
presented in Table 3, physical fitness improved after the
training period.
8-Iso-PGF increased in the erythrocytes of T2DM men
during an acute bout of exercise and decreased in the
recovery period similar to the observations before training
(Fig. 4). Furthermore, we found significant changes in
erythrocyte PRDX-SO2–3 levels during acute exercise
which were also similar to changes before training: PRDX-
SO2–3 contents increased from at rest to immediately after
exercise and were not reduced in the 30-min recovery
period (Fig. 4).
Nevertheless, there were some changes in the oxidative
stress response to acute exercise after the training period
(Fig. 5). Following physical training, increases in erythro-
cyte 8-Iso-PGF levels (in relation to exercise time) were
significantly decreased during the WHO-step test.
Decreases in 8-Iso-PGF in the recovery phase did not differ
between untrained and trained men. Increases in PRDX-
SO2–3 contents (in relation to exercise time) were signifi-
cantly higher in the erythrocytes of T2DM men following
physical training.
To discuss changes in the oxidative stress response to an
acute bout of exercise pre- versus post-training, we wanted
to determine whether oxidative stress at rest was also
affected by physical training. We observed a significant
reduction in 8-Iso-PGF in the erythrocytes of T2DM men
following physical training based on immunohistochemical
analyses (Fig. 3).
Discussion
The present study revealed a similar exercise-induced
oxidative stress response in the erythrocytes of T2DM
patients relative to non-diabetic control subjects as mea-
sured by 8-Iso-PGF. However, we observed increased
contents of overoxidized peroxiredoxins only in T2DM
patients during strenuous exercise. Physical training low-
ered oxidative stress (8-Iso-PGF) at rest and reduced
exercise-induced increases in 8-Iso-PGF contents (in rela-
tion to exercise time) in the erythrocytes of T2DM patients.
Furthermore, peroxiredoxin-overoxidation was increased
during acute exercise following physical training in the
erythrocytes of T2DM men.
Fig. 2 Increases/decreases in
8-Iso-PGF density during acute
exercise and at 30-min recovery
(in relation to exercise/recovery
time) in non-diabetic male
control subjects (CON) and men
suffering from non-insulin-
dependent type 2 diabetes
mellitus (T2DM). Values are
means ± SD
2282 Eur J Appl Physiol (2012) 112:2277–2287
123

Exercise-induced lipid-peroxidation and peroxiredoxin-
overoxidation in the erythrocytes of untrained non-
insulin-dependent T2DM patients and untrained non-
diabetic control subjects
Single bouts of exercise can increase the amount of free
radicals in the short-term. This has already been demon-
strated by Ashton et al. (1998) using electron spin reso-
nance spectroscopy as early as in 1998 (the signal was
fourfold increased post- vs. pre-exercise).
Erythrocytes are confronted with ROS from blood plasma
as well as with ROS resulting from the autoxidation of
hemoglobin. It can be assumed that this cell-internal ROS-
generation is also increased during acute exercise (Cooper
et al. 2002). High amounts of free radicals can reduce the red
blood cell deformability and even lead to their destruction
(Minetti et al. 2007; Dikmenoglu et al. 2008).
The demonstration that the activity of antioxidative
enzymes SOD, CAT and GPX in the erythrocytes of T2DM
subjects can be decreased (Bhatia et al. 2003; Memisogullari
Fig. 3 a Density of 8-Iso-PGF
in the erythrocytes of non-
diabetic male control subjects
(CON) and men suffering from
non-insulin-dependent type 2
diabetes mellitus (T2DM) as
well as of T2DM men before
physical training (BT) and after
physical training (AT) at rest.
Values are means ± SD.
*Significantly different from the
pre-training value (P B 0.05).
b Original photos of the 8-Iso-
PGF immunohistochemical
stainings
Fig. 4 a Density of 8-Iso-PGF and PRDX-SO2–3 at rest, immedi-
ately after the WHO-step test and at 30-min recovery in men suffering
from non-insulin-dependent type 2 diabetes mellitus before physical
training (BT) and after physical training (AT). Values are
means ± SD. �Significantly different from at rest (P B 0.05).�Significantly different from immediately after exercise (P B 0.05).
b Original photos of the 8-Iso-PGF and PRDX-SO2–3 immunohisto-
chemical stainings
Eur J Appl Physiol (2012) 112:2277–2287 2283
123

et al. 2003) raises the question whether T2DM patients’
erythrocytes are more defenceless against exercise-induced
free radicals and whether there are more rapid and higher
increases in oxidative stress during acute exercise than in
non-diabetic subjects.
Our results indicate similar changes in lipid-peroxidation
as measured by 8-Iso-PGF. Erythrocyte 8-Iso-PGF levels
increased during exercise and decreased in the following
30-min recovery phase in T2DM men and non-diabetic
control subjects. Increases and decreases (in relation to
exercise/recovery time) were also similar in both groups.
The data are in line with the findings of Miyazaki et al.
(2001) who found an increased lipid-peroxidation in the
erythrocyte membrane of healthy subjects immediately
after acute exercise compared with values at rest.
The finding that the contents of overoxidized peroxire-
doxins only increased in the diabetic group, but not in non-
diabetic men during acute exercise is particularly interesting.
It has been shown experimentally in different cell types,
e.g., in HeLa and yeast cells, that peroxiredoxins can
overoxidize in the presence of high amounts of hydrogen
peroxides (Lim et al. 2008; Seo et al. 2009). Consequently,
the peroxiredoxin system is ‘‘overloaded’’ and overoxida-
tion occurs (Low et al. 2008). Cho et al. (2010) recently
confirmed this mechanism in human erythrocytes and
found overoxidized peroxiredoxins when exposing red
blood cells to high hydrogen peroxide levels in vitro.
What could be the reason for an increase in the contents
of overoxidized peroxiredoxins in vivo to only occur in
T2DM men and not in non-diabetic control subjects under
increased oxidative stress as is the case during acute
exercise?
It can be suggested that the peroxiredoxin system
becomes more relevant in diabetes to buffer hydrogen per-
oxides in the erythrocytes if the activity of other enzymes
(e.g., of erythrocyte CAT, GPX) is reduced under patho-
logical conditions (Bhatia et al. 2003; Memisogullari et al.
2003). Furthermore, it can be speculated that the thioredoxin
system which is responsible for reducing oxidized perox-
iredoxins is negatively influenced by hyperglycemia (Minn
et al. 2005; Schulze et al. 2004). Moreover, it can be
hypothesized that the regulation of the activity of peroxire-
doxins through posttranslational modification (Seo et al.
2009; Jang et al. 2006) is different between the two groups.
However, increases in lipid-peroxidation, as measured by
8-Iso-PGF (relative to exercise time), were similar between
the diabetic and non-diabetic group. Therefore, the ratio of
exercise-generated free radicals and the total antioxidative
capacity seem to be similar in the patients of both our groups,
whereas antioxidative mechanisms obviously differ.
Finally, we examined whether T2DM men have
increased erythrocyte oxidative stress levels at rest relative
to non-diabetic subjects. In this case, exercise-induced
increases in oxidative stress would probably sum up to a
higher level of oxidative stress during acute exercise
compared with control subjects.
Different processes including hyperglycemia-dependent
mechanisms can be responsible for an elevated amount of
free radicals in T2DM subjects (Brownlee 2001; Inoguchi
et al. 2000; Kaneto et al. 2010; Wolff and Dean 1987).
Fig. 5 Increases/decreases in
8-Iso-PGF and PRDX-SO2–3
density during acute exercise
and at 30-min recovery (in
relation to exercise/recovery
time) in men suffering from
non-insulin-dependent type 2
diabetes mellitus before
physical training (BT) and after
physical training (AT). Values
are means ± SD. *Significantly
different from the pre-training
value (P B 0.05)
2284 Eur J Appl Physiol (2012) 112:2277–2287
123

In this context, Memisogullari et al. (2003) identified
increased oxidative stress in the erythrocytes of T2DM
men indicated by an increased concentration of malondi-
aldehyde (MDA). In our study, 8-Iso-PGF levels did not
significantly differ between overweight/obese T2DM and
overweight/obese non-diabetic men. It must be noted that
most of the diabetic subjects in our study took medications,
which, in part, are known to reduce ROS-production
(Ouslimani et al. 2005). Furthermore, the control subjects
were overweight/obese (BMI-matched) and it is accepted
that overnutrition increases systemic oxidative stress
(Urakawa et al. 2003). Therefore, it might be plausible that
oxidative stress is already increased in the erythrocytes of
overweight/obese men, and it is possible that arising T2DM
does not further increase oxidative stress levels, at least not
considerably.
A 30-min recovery period suffices to reduce the contents
of erythrocyte 8-Iso-PGF close to the basic level in both
diabetic as well as non-diabetic men. Nevertheless, the
contents of overoxidized peroxiredoxins were not signifi-
cantly reduced in the erythrocytes of the diabetic patients.
The peroxidatic cysteine of peroxiredoxins can be over-
oxidized to the sulfinic (CP-SO2H) and further on to the
sulfonic (CP-SO3H) acid form. The sulfinic form is
reversible and can be reduced by sulfiredoxin that is
expressed in red blood cells (Cho et al. 2010), whereas the
sulfonic form is probably irreversible (Seo et al. 2009).
Whether the sulfiredoxin system in the erythrocytes was
negatively affected by diabetes or whether peroxiredoxins
in the erythrocytes of the T2DM men in our study were
primarily overoxidized to the irreversible form remains
open. Further research on these questions is necessary.
Exercise-induced lipid-peroxidation and peroxiredoxin-
overoxidation in the erythrocytes of non-insulin-
dependent T2DM patients before and after
physical training
Several human studies have revealed a positive effect of
physical training on the activity/contents of antioxidative
enzymes, for example, of SOD, CAT, GPX in erythrocytes
or in skeletal muscle in the long-term (Ennezat et al. 2001;
Linke et al. 2005; Miyazaki et al. 2001; Ohno et al. 1988).
An up-regulation of antioxidative enzymes/proteins can
also be expected in the erythrocytes of the T2DM men in
our study, since we have revealed a decrease in basal
erythrocyte 8-Iso-PGF contents at rest as well as lower
increases in exercise-induced erythrocyte oxidative stress
(8-Iso-PGF in relation to exercise time) after training
compared with before training.
In line with our study, Miyazaki et al. (2001) examined
the influence of physical training on the oxidative stress
response in the erythrocytes of healthy men. They reported
a decreased magnitude of the increases in lipid-peroxida-
tion (thiobarbituric acid reactive substances (TBARS)) in
the erythrocyte membrane after acute exercise following
physical training. Miyazaki et al. also found an increase of
antioxidative enzyme activities at rest as well as a
decreased free radical production by neutrophils during
acute exercise following training. Consequently, it can be
deduced that regular physical activity can contribute to the
protection of erythrocytes from oxidative damage at rest
and during acute exercise.
Looking at our 8-Iso-PGF data, it could be possible that
the documented decreases in 8-Iso-PGF during the WHO-
step test following training are largely due to an increased
exercise time following physical training. When analyzing
absolute rather than relative increases (i.e., not in relation
to exercise time), no significant change is in fact obser-
vable pre- versus post-training. However, our data indicate
that less oxidative stress arises at the same workload pre-
versus post-training, i.e., oxidative stress increases more
slowly during the WHO-step test after the training
intervention.
Surprisingly, the magnitude of increases in overoxidized
peroxiredoxins was higher after than before training.
As a possible explanation it can be assumed that training
increases PRDX contents in the erythrocytes and, further-
more, the ratio of PRDX contents relative to other anti-
oxidative components. As a result, the probability of
peroxiredoxin oxidation and overoxidation increases in the
presence of high amounts of free radicals. This hypothesis
may be accepted, especially when the thioredoxin system is
weakened and/or sulfiredoxin activity/contents are reduced
in T2DM.
Of course the question is whether a high concentration
of overoxidized peroxiredoxins can be useful for the
erythrocytes of T2DM patients in any way. It has been
described in the literature that overoxidized peroxiredoxins
can convert into high-molecular-weight complexes (no
longer scavenging hydrogen peroxides) and act as chap-
erones which might protect proteins from (oxygen radical-
mediated) denaturation (Rhee et al. 2007).
Limitations
The use of only one measure (8-Iso-PGF) to determine the
presence of oxidative stress can be considered a limitation
of the study. The ratio of oxidized/reduced glutathione,
TBARS or other indicators for the redox state of the
erythrocytes should be examined in future studies (also
using other methods as well). It would also be particularly
interesting to compare the effect of physical training
between overweight/obese type 2 diabetic men and over-
weight/obese non-diabetic subjects to better elucidate the
effect of training on the type 2 diabetic organism,
Eur J Appl Physiol (2012) 112:2277–2287 2285
123

independent of obesity. It is, however, not too easy to
clearly determine the extent of the influence of diabetes
(before and after training) on oxidative stress variables,
because most of the subjects in our study also exhibited
other risk factors such as hyperlipidemia or hypertension,
which can affect the oxidative stress situation (Alexander
1995; Araujo et al. 1995).
Conclusions
The oxidative stress response to an acute bout of exercise,
measured as 8-Iso-PGF in the erythrocytes, is similar in
untrained overweight/obese non-diabetic control subjects
and T2DM patients, while antioxidative mechanisms
obviously differ. Regular physical activity can contribute to
the lowering of erythrocyte lipid-peroxidation (8-Iso-PGF)
at resting conditions as well as during acute exercise in
T2DM men. Therefore, cycling endurance training as
performed in our study can be considered a beneficial
strategy in diabetes to efficiently counteract ROS in
erythrocytes and prevent oxidative damage.
Acknowledgments The study was funded by the German Sport
University Cologne. The authors would like to thank A. Voss,
M. Ghilav and B. Collins for technical assistance.
Conflict of interest There is no conflict of interest for any of the
authors.
References
Alexander RW (1995) Hypertension and the pathogenesis of athero-
sclerosis. Oxidative stress and the mediation of arterial inflam-
matory response: a new perspective. Hypertension 25:155–161
Araujo FB, Barbosa DS, Hsin CY, Maranhao RC, Abdalla DS (1995)
Evaluation of oxidative stress in patients with hyperlipidemia.
Atherosclerosis 117:61–71
Ashton T, Rowlands CC, Jones E, Young IS, Jackson SK, Davies B,
Peters JR (1998) Electron spin resonance spectrometric detection
of oxygen-centred radicals in human serum following exhaustive
exercise. Eur J Appl Physiol 77:498–502
Basu S (1998) Radioimmunoassay of 8-iso-prostaglandin F2alpha: an
index for oxidative injury via free radical catalysed lipid
peroxidation. Prostaglandins Leukot Essent Fatty Acids
58:319–325
Bhatia S, Shukla R, Venkata Madhu S, Kaur Gambhir J, Madhava
Prabhu K (2003) Antioxidant status, lipid peroxidation and nitric
oxide end products in patients of type 2 diabetes mellitus with
nephropathy. Clin Biochem 36:557–562
Brownlee M (2001) Biochemistry and molecular cell biology of
diabetic complications. Nature 414:813–820
Cho CS, Lee S, Lee GT, Woo HA, Choi EJ, Rhee SG (2010)
Irreversible inactivation of glutathione peroxidase 1 and revers-
ible inactivation of peroxiredoxin II by H2O2 in red blood cells.
Antioxid Redox Signal 12:1235–1246
Collier A, Rumley A, Rumley AG, Paterson JR, Leach JP, Lowe GD,
Small M (1992) Free radical activity and hemostatic factors in
NIDDM patients with and without microalbuminuria. Diabetes
41:909–913
Cooper CE, Vollaard NB, Choueiri T, Wilson MT (2002) Exercise,
free radicals and oxidative stress. Biochem Soc Trans
30:280–285
Dikmenoglu N, Ileri E, Seringec N, Ercil D (2008) Melatonin
prevents lipid peroxidation in human erythrocytes but augments
deterioration of deformability after in vitro oxidative stress. Clin
Hemorheol Microcirc 40:235–242
Ennezat PV, Malendowicz SL, Testa M, Colombo PC, Cohen-Solal A,
Evans T, LeJemtel TH (2001) Physical training in patients with
chronic heart failure enhances the expression of genes encoding
antioxidative enzymes. J Am Coll Cardiol 38(1):194–198
Fischer UM, Schindler R, Brixius K, Mehlhorn U, Bloch W (2007)
Extracorporeal circulation activates endothelial nitric oxide
synthase in erythrocytes. Ann Thorac Surg 84:2000–2003
Fisher-Wellman K, Bloomer RJ (2009) Acute exercise and oxidative
stress: a 30 year history. Dyn Med 8:1
Inoguchi T, Li P, Umeda F, Yu HY, Kakimoto M, Imamura M, Aoki
T, Etoh T, Hashimoto T, Naruse M, Sano H, Utsumi H, Nawata
H (2000) High glucose level and free fatty acid stimulate
reactive oxygen protein kinase C-dependent activation of
NAD(P)H oxidase in cultured vascular cells. Diabetes
49:1939–1945
Jang HH, Kim SY, Park SK, Jeon HS, Lee YM, Jung JH, Lee SY,
Chae HB, Jung YJ, Lee KO, Lim CO, Chung WS, Bahk JD, Yun
DJ, Cho MJ, Lee SY (2006) Phosphorylation and concomitant
structural changes in human 2-Cys peroxiredoxin isotype I
differentially regulate its peroxidase and molecular chaperone
functions. FEBS Lett 580:351–355
Kaneto H, Katakami N, Matsuhisa M, Matsuoka TA (2010) Role of
reactive oxygen species in the progression of type 2 diabetes and
atherosclerosis. Mediat Inflamm 2010:453892
Lim JC, Choi HI, Park YS, Nam HW, Woo HA, Kwon KS, Kim YS,
Rhee SG, Kim K, Chae HZ (2008) Irreversible oxidation of the
active-site cysteine of peroxiredoxin to cysteine sulfonic acid for
enhanced molecular chaperone activity. J Biol Chem
283:28873–28880
Linke A, Adams V, Schulze PC, Erbs S, Gielen S, Fiehn E, Mobius-
Winkler S, Schubert A, Schuler G, Hambrecht R (2005)
Antioxidative effects of exercise training in patients with chronic
heart failure: increase in radical scavenger enzyme activity in
skeletal muscle. Circulation 111:1763–1770
Low FM, Hampton MB, Winterbourn CC (2008) Peroxiredoxin 2 and
peroxide metabolism in the erythrocyte. Antioxid Redox Signal
10:1621–1630
Memisogullari R, Taysi S, Bakan E, Capoglu I (2003) Antioxidant
status and lipid peroxidation in type II diabetes mellitus. Cell
Biochem Funct 21:291–296
Minetti M, Agati L, Malorni W (2007) The microenvironment can
shift erythrocytes from a friendly to a harmful behavior:
pathogenetic implications for vascular diseases. Cardiovasc
Res 75:21–28
Minn AH, Hafele C, Shalev A (2005) Thioredoxin-interacting protein
is stimulated by glucose through a carbohydrate response
element and induces beta-cell apoptosis. Endocrinology
146:2397–2405
Miyazaki H, Oh-ishi S, Ookawara T, Kizaki T, Toshinai K, Ha S,
Haga S, Ji LL, Ohno H (2001) Strenuous endurance training in
humans reduces oxidative stress following exhausting exercise.
Eur J Appl Physiol 84:1–6
Nikolaidis MG, Jamurtas AZ (2009) Blood as a reactive species
generator and redox status regulator during exercise. Arch
Biochem Biophys 490:77–84
Ohno H, Yahata T, Sato Y, Yamamura K, Taniguchi N (1988)
Physical training and fasting erythrocyte activities of free radical
2286 Eur J Appl Physiol (2012) 112:2277–2287
123

scavenging enzyme systems in sedentary men. Eur J Appl
Physiol Occup Physiol 57:173–176
Osuntokl AA, Fasanmade OA, Adekola AO, Amira CO (2007) Lipid
peroxidation and erythrocyte fragility in poorly controlled type 2
diabetes mellitus. Nig Q J Hosp Med 17:148–151
Ouslimani N, Peynet J, Bonnefont-Rousselot D, Therond P, Legrand
A, Beaudeux JL (2005) Metformin decreases intracellular
production of reactive oxygen species in aortic endothelial cells.
Metabolism 54:829–834
Pandey KB, Mishra N, Rizvi SI (2010) Protein oxidation biomarkers
in plasma of type 2 diabetic patients. Clin Biochem 43:508–511
Pratico D, Rokach J, Lawson J, FitzGerald GA (2004) F2-isopros-
tanes as indices of lipid peroxidation in inflammatory diseases.
Chem Phys Lipids 128:165–171
Rains JL, Jain SK (2011) Oxidative stress, insulin signaling, and
diabetes. Free Radic Biol Med 50:567–575
Rhee SG, Jeong W, Chang TS, Woo HA (2007) Sulfiredoxin, the
cysteine sulfinic acid reductase specific to 2-Cys peroxiredoxin:
its discovery, mechanism of action, and biological significance.
Kidney Int Suppl 106:S3–S8
Roberts LJ, Morrow JD (2000) Measurement of F(2)-isoprostanes as
an index of oxidative stress in vivo. Free Radic Biol Med
28:505–513
Sato Y, Hotta N, Sakamoto N, Matsuoka S, Ohishi N, Yagi K (1979)
Lipid peroxide level in the plasma of diabetic patients. Biochem
Med 21:104–107
Schulze PC, Yoshioka J, Takahashi T, He Z, King GL, Lee RT (2004)
Hyperglycemia promotes oxidative stress through inhibition of
thioredoxin function by thioredoxin-interacting protein. J Biol
Chem 279:30369–30374
Seo JH, Lim JC, Lee DY, Kim KS, Piszczek G, Nam HW, Kim YS,
Ahn T, Yun CH, Kim K, Chock PB, Chae HZ (2009) Novel
protective mechanism against irreversible hyperoxidation of
peroxiredoxin: Nalpha-terminal acetylation of human peroxire-
doxin II. J Biol Chem 284:13455–13465
Sigal RJ, Kenny GP, Wasserman DH, Castaneda-Sceppa C (2004)
Physical activity/exercise and type 2 diabetes. Diabetes Care
27:2518–2539
Suhr F, Porten S, Hertrich T, Brixius K, Schmidt A, Platen P, Bloch
W (2009) Intensive exercise induces changes of endothelial
nitric oxide synthase pattern in human erythrocytes. Nitric Oxide
20:95–103
Urakawa H, Katsuki A, Sumida Y, Gabazza EC, Murashima S,
Morioka K, Maruyama N, Kitagawa N, Tanaka T, Hori Y,
Nakatani K, Yano Y, Adachi Y (2003) Oxidative stress is
associated with adiposity and insulin resistance in men. J Clin
Endocrinol Metab 88:4673–4676
Villa-Caballero L, Nava-Ocampo AA, Frati-Munari A, Ponce-Monter
H (2000) Oxidative stress, acute and regular exercise: are they
really harmful in the diabetic patient? Med Hypotheses 55:43–46
Winterbourn CC, Stern A (1987) Human red cells scavenge
extracellular hydrogen peroxide and inhibit formation of hypo-
chlorous acid and hydroxyl radical. J Clin Invest 80:1486–1491
Wolff SP, Dean RT (1987) Glucose autooxidation and protein
modification. Biochem J 245:243–250
Eur J Appl Physiol (2012) 112:2277–2287 2287
123














![ERYTHROCYTES [RBCs]](https://img.pdfslide.us/doc/110x75/56813dc0550346895da78963/erythrocytes-rbcs-56ea22b2e2743.jpg)












![ERYTHROCYTES [RBCs]](https://img.pdfslide.us/doc/110x75/568130b1550346895d96c651/erythrocytes-rbcs-5687466751123.jpg)