Embed Size (px)
Citation preview

Lecture Outline
• Type 1 diabetes– Changes in lipid metabolism are a
CONSEQUENCE of diabetes
• Type 2 diabetes– Changes in lipid metabolism may be a
CAUSE of diabetes AND– Changes in lipid metabolism are a
CONSEQUENCE of diabetes

Normal Pancreatic Function
• Exocrine pancreas aids digestion– Bicarbonate– Lipase– Amylase– Proteases
• Endocrine pancreas (islets of Langerhans)– Beta cells secrete insulin– Alpha cells secrete
glucagon – Other hormones

Type 1 Diabetes Mellitus:Background
• Affects ~1 million people
• Juvenile onset
• Genetic component
• Autoimmune/environmental etiology

Type 1 Diabetes:Hallmarks
• Progressive destruction of beta cells
• Decreased or no endogenous insulin secretion
• Dependence on exogenous insulin for life

Diabetes: General Information
• Juvenile Diabetes Research Foundation– www.jdf.org
• American Diabetes Association– www.diabetes.org

Type 1 Diabetes:Presenting Symptoms
• Polyuria• Polydipsia• Hyperphagia• Growth retardation• Wasting

Insulin Stimulates Cellular Glucose Uptake
LiverSkeletal Muscle
Adipocytes
Intestine & Pancreas
InsulinInsulin
Insulin

Absence of Insulin
• Glucose cannot be utilized by cells
• Glucose concentration in the blood rises
• Blood glucose concentrations can exceed renal threshold
• Glucose is excreted in urine

Presenting Symptoms of Type 1 Diabetes
• Polyuria: Glucose excretion in urine increases urine volume
• Polydipsia: Excessive urination leads to increased thirst
• Hyperphagia: “Cellular starvation” increases appetite

Growth Retardation
• Insulin required for normal growth
• Necessary for normal amino acid and protein metabolism
• Stimulates synthesis, inhibits degradation

Wasting
• Calories are inefficiently stored as fat
• Adipose stores are depleted

Normal
LPL
Triglyceride
LipolysisGlycerol
Free fatty acids
Free fatty acids
Glucose
Synthesis
Insulin
Insulin

Triglyceride
LPL
Type 1 Diabetes Mellitus
LipolysisGlycerol
Free fatty acids
Free fatty acids
Glucose
Synthesis

Clinical Chemistry
• Normal– Fasting blood glucose
< 100 mg/dL
– Serum free fatty acids ~ 0.30 mM
– Serum triglyceride ~100 mg/dL
• Uncontrolled Type 1– Fasting blood glucose
up to 500 mg/dL
– Serum free fatty acids up to 2 mM
– Serum triglyceride > 1000 mg/dL

Adipocyte Fatty Acid Uptake Decreased
• Lipoprotein lipase– Synthesized by adipocytes– Secreted to capillary endothelium– Hydrolyzes circulating triglyceride
• Fatty acid transporter– CD36, FABPpm
– Facilitates movement of free fatty acids from extracellular to intracellular space

Adipocyte Triglyceride Synthesis Decreased
Glycerol-3-P
Lysophosphatidic acid
Phosphatidic acid
Diglyceride
Triglyceride
FACoA
FACoA
FACoA
Pi

Antilipolysis
AC
Gs Gi
IRS
ATP cAMP
PKAHSLAMP
PDE
PI3K
PKB
AC

Enhanced Lipolysis: Consequences in Liver
• Liver partitions fatty acids:
– Triglyceride synthesis (VLDL)
– Oxidation
– Ketogenesis

Insulin Regulation of Hepatic Fatty Acid Partitioning
FA-CoA
TG ATP, CO2 -hydroxybutyrate
acetoacetate
Mitochondrion

In Liver:FFA Entry into Mitochondria is Regulated by
Insulin/Glucacon
FA-CoA
Mitochondrial membranes
outer
inner
CPT-I CPT-II
carnitine
FA-CoA
carnitine
ATP, CO2 HB, AcAc
Malonyl CoA
TG

Malonyl CoA is a Regulatory Molecule
• Condensation of CO2 with acetyl CoA forms malonyl CoA
• First step in fatty acid synthesis
• Catalyzed by acetyl CoA carboxylase
• Enzyme activity increased by insulin

Ketone Bodies
• Hydroxybutyrate, acetoacetate• Fuel for brain• Excreted in urine
• At 12-14 mM reduce pH of blood• Can cause coma (diabetic
ketoacidosis)

Type 1 Diabetes
Summary• Lack of insulin prevents storage of
lipid in adipose tissue
• Unstored lipid circulates as lipoproteins and free fatty acids
• Free fatty acids are oxidized by liver to form ketone bodies

Type 2 Diabetes Mellitus
• 16 million estimated affected• Genetic component• Associated with obesity• Previously maturity-onset• Progressive

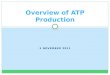
How is Glucose Tolerance Measured?
• Oral Glucose Tolerance Test (OGTT)– Fasting state– 75 gm oral glucose load– Blood sampled before and at intervals
for 2-4 hr.– Serum glucose measured clinically– Serum insulin measured experimentally

Oral Glucose Tolerance Test
0
100
200
300
0 30 60 90 120
Time Post Glucose Load (min)
Blood
Glucos
e (mg
/dL)
Normal • Normal– Low basal glucose– Small, transient
rise in glucose
– Low basal insulin, two-phase, transient increase in insulin

Oral Glucose Tolerance Test
0
100
200
300
0 30 60 90 120
Time Post Glucose Load (min)
Blood
Glucos
e (mg
/dL)
I nsulin Resistant • Insulin Resistant– Tissues unresponsive
to insulin
– Basal hyperinsulinemia
– First phase insulin release blunted
– Blood glucose curve looks normal

Oral Glucose Tolerance Test
0
100
200
300
0 30 60 90 120
Time Post Glucose Load (min)
Blood
Glucos
e (mg
/dL)
Normal IGT • Impaired Glucose Tolerance– Deterioration in ability
to handle glucose
– Basal and stimulated hyperinsulinemia
– Fasting plasma glucose >100, <126 mg/dL
– 2 hr glucose >140, <200 mg/dL

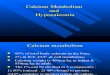
Oral Glucose Tolerance Test
0
100
200
300
0 30 60 90 120
Time Post Glucose Load (min)
Blood
Glucos
e (mg
/dL)
Normal IGT T2DM • Diabetes Mellitus– Hyperinsulinemia can’t
compensate for insulin resistance
– Fasting blood glucose >126 mg/dL
– 2 hr glucose >200 mg/dL
– Insulin resistance increases

Ectopic deposition of lipid contributes to the etiology and progression of T2DM.
“Lipotoxicity” hypothesis

Bad Places for Excess Lipid
Liver
Pancreas
Skeletal Muscle
Heart Muscle

Primary Defect in Type 2
• Study healthy 1st degree relatives of patients with type 2
• Measure ability of body to use glucose
• Find defects in muscle glucose uptake before any symptoms develop

Insulin
1. Infuse insulin to induce hyperinsulinemia
2. Measure blood glucoseevery 2 min
150 mg/dLGlucose
3. Adjust glucose infusion rate to maintain euglycemia.

Clamp Data
• The amount of glucose infused is a measure of insulin sensitivity.
• More glucose = more sensitive
• Less glucose = less sensitive
McGarry 2002, Fig 2B

Findings from Clamp Studies
• Glucose disposal is decreased 60% in some healthy young people with family history of type 2.
• Defect is in ability of insulin to stimulate glucose transport into the cell.

Why is Glucose Transport Reduced?
• Mitochondrial phosphorylation decreased 30%
• Intramyocellular lipid is increased 80%
• Ectopic fat may hinder insulin-stimulation of glucose transport.

Lipids as Signaling Molecules
Fatty acyl CoA esterified to diglyceride
Diglyceride activates protein kinase C theta
Protein kinase C theta serine-phosphorylates and inactivates insulin receptor substrate 1

What is consequence of muscle insulin resistance?
• Pancreas compensates > hyperinsulinemia
• Hyperinsulinemia exacerbates insulin resistance in adipose tissue.

Consequences of Insulin Resistance in Adipose Tissue
• Similar to insulin deficiency
• Reduced TG synthesis
• Enhanced lipolysis
• Net increase in FA availability to non-adipose tissues

Effect of excess free fatty acids on insulin sensitivity
0
2
4
6
8
10
12
Control Intralipid
Infusion
Glu
cose
Dis
posa
l

Consequences of Insulin Resistance FFA in Muscle
• Increased intramyocellular lipid
• Hypothetical: inhibition of insulin signaling by diglyceride
• Reduction in glucose uptake by muscle

Consequences of Insulin ResistanceFFA in Liver
• Increased triglyceride synthesis
• Increased oxidation
• Increased gluconeogenesis
• Hepatic glucose output contributes to hyperglycemia

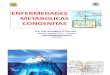
Consequences of Insulin ResistanceFFA in Pancreas
• Animal models of diabetes
• Lipid droplets accumulate in beta cells
• Beta cells undergo apoptosis
• Reduced beta cell mass
• Decreased circulating insulin

Pancreatic Histology
Control Diabetic

Timeline: Development of Type 2
Genetic
predisposition
Environmental
insult
Insulin
resistance
Increased
lipolysis
Ectopic fat
deposition
Compromised
pancreatic function
Fasting
Hyperglycemia
Beta cell
failure

Diet and Exercise
• Goal– Reduce caloric intake– Increase exercise
• Purpose– Reduce size of adipose stores– Improve insulin sensitivity– Increase lean body mass

Insulin-releasing Drugs
• Goal– Stimulate pancreas to produce more
endogenous insulin
• Purpose– Overcomes insulin resistance
– Plasma glucose is taken up and oxidized appropriately

Hepatic Insulin Sensitizers
• Goal– Work selectively on the liver
– Inhibit glycogenolysis and gluconeogenesis
• Purpose– Reduce hepatic glucose output
– Reduce blood glucose concentration

Thiazolidinediones: new class of drugs
• Goal– Peripheral insulin sensitizers– Enhance muscle insulin
sensitivity
• Purpose– Reduce blood glucose, insulin

Thiazolidinediones: new class of drugs
• Unintended consequences
– Increase lipid storage in adipose tissue
– Reduce lipid storage in muscle, pancreas
– Preserve beta cell mass

Summary
• Insulin deficiency perturbs lipid metabolism in type 1 diabetes.
• Prevention– Under investigation
• Treatment – Insulin replacement– Management of carbohydrate intake

Summary, cont.
• Dysregulated lipid metabolism may contribute to the development of type 2 diabetes.
• Prevention– Eat less, exercise more really works
• Treatment– Depends on stage of disease