-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
1/20
Linking Six Sigma to simulation:a new roadmap to improve the
quality of patient careGiovanni Celano, Antonio Costa and Sergio
Fichera
Dipartimento di Ingegneria Industriale e Meccanica, University
of Catania,Catania, Italy, and
Giuseppe TringaliAzienda Ospedaliero Universitaria Policlinico
Vittorio Emanuele,
Catania, Italy
AbstractPurpose Improving the quality of patient care is a
challenge that calls for a multidisciplinaryapproach, embedding a
broad spectrum of knowledge and involving healthcare professionals
fromdiverse backgrounds. The purpose of this paper is to present an
innovative approach that implementsdiscrete-event simulation (DES)
as a decision-supporting tool in the management of Six Sigma
qualityimprovement projects.
Design/methodology/approach A roadmap is designed to assist
quality practitioners and healthcare professionals in the design
and successful implementation of simulation models within
thedefine-measure-analyse-design-verify (DMADV) or
define-measure-analyse-improve-control (DMAIC)Six Sigma
procedures.
Findings A case regarding the reorganisation of the flow of
emergency patients affected by vertigosymptoms was developed in a
large town hospital as a preliminary test of the roadmap. The
positivefeedback from professionals carrying out the project looks
promising and encourages further roadmap
testing in other clinical settings.
Practical implications The roadmap is a structured procedure
that people involved in qualityimprovement can implement to manage
projects based on the analysis and comparison of
alternativescenarios.
Originality/value The role of Six Sigma philosophy in
improvement of the quality of healthcareservices is recognised both
by researchers and by quality practitioners; discrete-event
simulationmodels are commonly used to improve the key performance
measures of patient care delivery. The twoapproaches are seldom
referenced and implemented together; however, they could be
successfullyintegrated to carry out quality improvement programs.
This paper proposes an innovative approach tobridge the gap and
enrich the Six Sigma toolbox of quality improvement procedures with
DES.
Keywords Quality improvement, Six sigma, Modelling, Discrete
event simulation, Simulation,Health services
Paper type Research paper
The current issue and full text archive of this journal is
available at
www.emeraldinsight.com/0952-6862.htm
The authors wish to thank the anonymous referees for valuable
suggestions which allowedimprovement of the quality of the final
paper. Furthermore, the authors are grateful toDr G. Brown, PhD
(Department of Psychology, Royal Holloway, University of
London),and Dr F Messineo, PhD (Kent School of Law, University of
Kent), who gave valuable supportduring the editing process of this
paper.
IJHCQA25,4
254
Received 9 September 2010Revised 15 December 2010Accepted 27
December 2010
International Journal of Health Care
Quality Assurance
Vol. 25 No. 4, 2012
pp. 254-273
q Emerald Group Publishing Limited
0952-6862
DOI 10.1108/09526861211221473
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
2/20
IntroductionContinuous quality improvement of patients care is
recognised as essential forachieving excellence in the healthcare
service delivery. In the last 20 years, Six Sigma(6s) has received
a lot of attention among the several quality management
philosophies. Six Sigma is a rigorous, focused and highly
effective implementation ofproven quality principles and
techniques, which aims at virtually error free businessperformance
(Pyzdek, 2003). In the 1980s, Six Sigma was initially implemented
in theindustrial setting by Motorola; it subsequently attracted
much attention among peopleworking in the service sector, including
healthcare professionals. In 1998, KentuckysCommonwealth Health
Corporation was the first healthcare organisation which
fullyembraced the Six Sigma philosophy the US; successively, Six
Sigma was implementedwithin several US organisations (Sehwail and
DeYong, 2003). A survey of Six Sigmaprograms in 56 US healthcare
organisations conducted by means of questionnaires ispresented by
(Feng and Manuel, 2008). Six Sigma improvement programmes
andpersonnel training have also been employed in European
healthcare organisations.Some case studies presenting Six Sigma
implementation in the nursing department atthe Red Cross Hospital
of Beverwijk (The Netherlands) are discussed in Van denHeuvel et
al. (2004); the annual savings obtained in the same hospital by
means of theimplementation of quality improvement projects are
presented in Van Den Heuvel et al.(2005). A review about the Six
Sigma methodology application to healthcareorganisations is
proposed in Taner et al. (2007). More recently, Taner and Sezen
(2009)have proposed the implementation of the Six Sigma toolbox to
study the turnoverproblem of doctors in medical emergency services
and paramedic backup. However, allof these case studies show that a
strong financial and organisational effort is needed tocarry out a
successful Six Sigma project in the healthcare field. This is a
barrier to itsdeployment within organisations with a limited budget
capacity or which are alreadyimplementing another quality
management philosophy like, for example, the ISO 9000
family of standards. The question arises if there are ways to
introduce the Six Sigmatechniques within budget-conscious
healthcare organisation while retaining aneffective outcome.
Based on several years of experience about the implementation of
Six Sigmaprogrammes, Magnusson et al. (2003) claim that there are
three main approaches todeploy Six Sigma within a company. The
first approach assumes that Six Sigma can beinitiated as a
company-wide strategy at the highest level and deployed throughout
theentire organisation under the full senior management commitment.
This approachrequires a strong company effort to achieve
breakthrough quality-improvementobjectives which should be
supported by a well defined organisational structure,(Glickman et
al., 2007). Alternatively, the second approach assumes that Six
Sigma canbe implemented as an improvement programme by one or more
organisational units
and, if successful, extended to the other areas of the company.
Finally, accordingly tothe third approach Six Sigma can be adopted
as a toolbox into specific projects forimprovement with a
particular focus to problem solving: this third approach does
notrequire the commitment from senior management or a large company
involvement.This third vision and approach to Six Sigma will be
adopted in this paper; it fits withthe definition of Six Sigma
given in (Linderman et al., 2003), who consider Six Sigma asan
organised and systematic problem-solving method for strategic
systemimprovement and new product and service development based on
statistical methods.
Linking SixSigma to
simulation
255
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
3/20
Hundreds of papers and several research journals show the
implementation ofoperations research (OR) tools in the field of
healthcare service. Operations Research isapplied to problems that
concern how to conduct and coordinate the operations (i.e.
theactivities) within an organisation. Among the OR tools,
discrete-event simulation
(DES) allows for the complexity of stochastic systems to be
modelled which cannot becaught by a pure mathematical model
(Hillier and Lieberman, 2005). Healthcaresettings, like those
investigated in the case study discussed in this paper, are
oftencomplex stochastic systems. These are characterised by random
variables describingthe times to complete activities; complex flow
of patients to be managed throughout thedepartments, random patient
interarrival times; shared resources availability amongseveral
departments. Thus, describing all these aspects by means of a
puremathematical model is often a prohibitive task; otherwise, they
can be efficiently (andquite easily) modelled through DES. A
comprehensive review of discrete-eventsimulation models applied to
healthcare problems is reported in Jun et al. (1999): thispaper
surveys the application of discrete-event simulation modelling to
healthcareclinics and systems of clinics, i.e. hospitals,
outpatient clinics, emergency departments,and pharmacies. A second
more recent review (Fletcher and Worthington, 2009) isfocused on
the simulation of emergency patient flows and provides for
exhaustivereferences to papers related to the study of accident and
emergency (A&E)departments, bed management, surgery, critical
care and diagnostics and other specificenvironments.
Often the key performance measures (KPM) optimised by means of a
discrete-eventsimulation model can coincide with the critical to
quality (CTQ) parameters selected toachieve quality-improvement
within a Six Sigma programme. Thus, trying to get asynergy between
Six Sigma and DES techniques seems to be appropriate and
deservesattention from the researchers and quality practitioners.
In light of this, a recent paper(Tang et al., 2007) suggests as a
major strengthening for Six Sigma to expand its
toolbox through the integration of the OR techniques in the
training courses for SixSigma Black Belts.In this paper, a
theoretical framework based on a roadmap facilitating the
process
of embedding discrete-event simulation as a decision tool within
a Six Sigmaquality-improvement project is discussed. The roadmap is
built as a structured andhierarchical procedure to achieve quality
improvement in a general setting. A casestudy showing the first
in-hospital implementation of the roadmap is presented to
thereaders.
In the next section, the proposed roadmap is discussed in
detail. Then, thedevelopment of a DES based quality-improvement Six
Sigma programme is presentedto show the implementation of the
roadmap in practice. This was a programme aimedat reorganising the
flow of emergency patients affected by vertigo symptoms.
Successively, the lessons learned from the case study and the
potential benefits fromthe proposed approach are discussed.
Finally, conclusions and future researchopportunities complete the
paper.
Linking Six Sigma to simulation: definition of a roadmapSix
Sigma quality practitioners select, develop and validate a
quality-improvementproject by selecting and implementing a
define-measure-analyse-improve-control(DMAIC) or, alternatively, a
define-measure-analyse-design-verify (DMADV) five step
IJHCQA25,4
256
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
4/20
procedure. Whenever process improvement should be investigated
by comparing anexisting configuration to alternative scenarios, the
DMAIC methodology is adopted.When new processes, products or
services should be designed, the DMADVmethodology is adopted
instead; for further details, readers can refer to (Pyzdek,
2003).
Often, the comparison among different scenarios or testing new
product or processconfigurations can only be performed by means of
simulation because of the complexmanagement issues and associated
costs required in the performance of real trial runs.
The design of a simulation model is a structured five-step
procedure working asfollows. First, the process requires mapping
and a clear definition of its boundaries: areview and application
of several visual techniques to map processes in the
healthcarefield can be found in (Guglielmino et al., 2009). Then,
the stochastic process data arecollected to define the base of
knowledge needed to design the model. The third stepconsists of
analysing these data to get a good statistical fit of their
variability. Then,the simulation model logic can be designed and
developed. Finally, the model isvalidated through a set of trial
runs. After the simulation model has been validated, itcan be used
to compare the current configuration, if it exists, against
hypothesised newscenarios in order to find the optimum with respect
to one or more pre-selected keyperformance measures. This five-step
procedure has been adapted in Seppanen et al.(2005) to fit it with
the DMAIC procedure.
A roadmap extending this approach is proposed here as a
theoretical framework tomanage Six Sigma projects aimed at
improving the quality of a service: it merges boththe DMADV and
DMAIC methodologies to achieve a hierarchical procedure able
tomanage an ongoing Six Sigma quality-improvement project of an
existing servicebased on a discrete-event simulation model. We
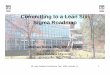
denote it as the DMAIC-DMADVroadmap. Similarly, if the Six Sigma
improvement project is focused on new serviceconfigurations to be
investigated, the double DMADV2 roadmap should be considered.Figure
1 shows the flow chart of the DMAIC-DMADV roadmap.
The roadmap description intentionally refers to a generic
process, thus assuring ahigh degree of generality and a wide
applicability of the framework either to a serviceor a
manufacturing environment. In the proposed hierarchical approach,
the DMAICmethodology defines the five steps for the
quality-improvement project and containsthe DMADV methodology
related to the DES model design and development. Thus, inFigure 1,
the upper (lower) case notation and plain (dashed) line boxes
denote a phaseand the activities belonging to the outer DMAIC
(inner DMADV) methodology,respectively. Of course, given the
parental relationship between the two methodologies,each activity
belonging to the inner DMADV methodology is also part of the
outerDMAIC methodology. In the next Sub-sections a brief
description of each phase of theroadmap is presented.
DefineThe first phase of the outer DMAIC methodology consists of
the sequence of stepsaimed at deciding if a quality-improvement
project is suitable to be carried out byfollowing the proposed
roadmap. First, the quality-improvement project should beselected:
the expected quality improvement of patient care and, possibly,
cost savingsare drivers to the selection; then, the work team
should be formed by involving, ifneeded, external consultants and
people from the quality assurance and the otherdepartments affected
by the project. To implement the proposed approach, the
Linking SixSigma to
simulation
257
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
5/20
prerequisites are: the need to test one specific process
scenario or comparing differentprocess (service) configurations;
the need to implement the simulation tool to model theprocess
because of the massive presence of random variables and
uncertainty, multipleflows of information and activities, several
interactions between resources and the
Figure 1.The roadmap linking 6sand the discrete-eventsimulation
modeldevelopment
IJHCQA25,4
258
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
6/20
difficulty of performing trial runs. Once the presence of these
prerequisites has beenconfirmed, the project continues by starting
the inner define phase aimed atmodelling the process. The clear
understanding about which department is involvedand, for each
department, what the resources and the areas to be modelled are
allows
for the boundaries of the process to be defined. This represents
the starting milestoneto define the cross-functional process maps
and the value added stream of activities.Software allowing the
visualisation and analysis of complex information, systems
andprocesses and common spreadsheets are useful during this phase.
For each activitydefined within a cross-functional process map the
following information should berecorded: upstream and downstream
activities, required resources, time to completionand associated
costs. The outcomes of this phase are one or more detailed
processflowcharts and a partially complete database of records each
containing an activity tobe performed and its related information.
Some empty fields of these records, like timeand costs to perform
the activities, cannot be filled at this step of the roadmap.
Thus,the measurement of the available historical data or the
on-line collection of new data isrequired: to accomplish this
information, the measure phase should be started.
MeasureAssuming that a measurement system is already present and
active, during this phasethe project development proceeds with the
model building. Data retrieved from theorganisations databases
and/or hardcopy registries should be checked and filtered toremove
errors. The data should also be formatted for the subsequent
roadmap phases.Sometimes, it is not possible to retrieve
information about some categories of data. Inthose cases, the only
ways to gather knowledge about them are direct sampling orreliable
estimates based on interviews with those directly involved in the
servicedelivery. Usually, the data to be collected to simulate a
healthcare service includestandard costs and time schedules related
to the involved resources, i.e. nurses,technicians and physicians;
costs and times needed to perform exams and/or
surgicalinterventions; transportation times between departments,
and so on. Basic informationabout patients includes volumes,
arrival rates at each time of day (TOD), type andseverity of
illness, length of stay. The outcomes of this phase are
spreadsheetscollecting the data to be analysed.
AnalyseOnce collected and pre-processed, the data should be
classified and analysed. Standardcosts can be retrieved from the
organisations accounting system: usually, they have adeterministic
value. Conversely, a statistical distribution fitting is required
for all therandom data: for example, times to perform a
consultation, to complete an exam, or to
perform a surgical intervention are stochastic and should be
statistically modelled.Usually lognormal, normal or triangular
distributions are adopted. The patientsarrival times are modelled
as a non-stationary Poisson process with exponentialinterarrival
times. The final step of this phase assigns costs and times to a
specificactivity area of the process coinciding with each
department included within themodel. The outcome of this phase is a
set of deterministic data and statisticaldistributions completing
the information contained within the database of theactivities.
Then, the project can proceed with the DES model building.
Linking SixSigma to
simulation
259
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
7/20
ImproveThis phase of the project coincides with the
formalisation of different processconfigurations to be compared. In
the proposed roadmap, Improve is the core phasebecause it involves
the DES model design and validation: that is, it includes the
design
and verify phases belonging to the inner DMADV procedure, see
Figure 1. For eachscenario, the model logic is built within a
specific simulation software environment byreferring to the
cross-functional process maps drawn during the define phase.
Eachblock of the simulation model is defined by loading the
quantitative data modelledduring the Analyse phase. Finally, the
critical to quality parameters, which weredefined so as to compare
the different process configurations, are embedded within theDES
model as variables or expressions to be triggered during the
simulation. This stepends the design phase for the DES model. Then,
during the verify phase the DES modellogic is tested and validated
through a set of pilot simulation runs to demonstrate
itsconsistency with real process data. Once the DES model has been
validated, anexperimental plan can be designed by setting at
different levels the factors influencingthe quality of service
delivery: usually, these factors may include processconfigurations,
amount of available resources capacity and costs. For
eachexperimental run, the CTQs are the response variables to be
optimised. Each run ofthe DES model performed with a specific
combination of factors represents areplication of the experimental
study. A statistical analysis allows the best processconfiguration
to be selected. The outcomes of this phase are the simulation
models ofthe different process configurations and a report
presenting the results of the statisticalanalysis. Then, the last
phase of the quality-improvement project can be initiated.
ControlOnce the best scenario is selected, all the cost and time
savings are computed anddocumented for each activity area. Finally,
the quality-improvement project requires
the documentation and dissemination of the results throughout
the involved areas ofthe organisation and, if required, outside the
organisation. Brainstorming meetingsshould be scheduled to share
opinions about the results and to organise theimplementation the
best process configuration.
An in-hospital implementation of the roadmapA first in-hospital
test of the roadmap has been performed in the emergencydepartment
of a large town public hospital in southern Italy to compare two
differentprocedures designed to manage the flow of emergency
patients affected by vertigosymptoms illness (later denoted as VSI
patients). This quality-improvement projectdevelopment has been
carried out by academic staff from the University of Catania andby
staff from the emergency department and the other departments
involved in the
vertigo patients flow reorganisation. The hospital has an ISO
9000 standardcertification, and it has never implemented a Six
Sigma project in the past. The SixSigma approach was not adopted to
carry out quality improvement programs withinthe hospital
organisation for two main reasons. First, a cultural issue arising
from theapproach to quality based on the ISO 9000 standard. This
puts more emphasis oncorrect management of documentation,
procedures description and bookkeeping,rather than to promote
efforts reducing variability and improving processes by meansof
sharply focused projects. Second, an operational issue: the lack of
internal resources
IJHCQA25,4
260
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
8/20
having a strong background on the Six Sigma techniques rendered
theirimplementation difficult.
Getting a diagnosis for a walk-in emergency patient affected by
vertigo symptomsrequires the execution of several exams and
consultations from different departments.
Thus, the time to diagnosis can be extremely long and high rates
of light symptomspatients leave the service. The objective of the
quality-improvement projectimplementation in the ED has been to
eliminate unnecessary exams and to reducethe time and cost needed
to get the VSI patients diagnosis leading to ward admission ortheir
discharge. To achieve the Six Sigma improvement project goals, a
new procedure(scenario B) for the management of VSI patients in the
emergency department has beendesigned and compared to the current
procedure, denoted here as scenario A. Bothprocedures are described
below and graphically detailed in Figures 2 and 3.
The combined DMAIC-DMADV roadmap served as the framework problem
solvingtool. In Table I, each step of the roadmap is presented with
reference to the project. Thedefine phase started by deciding to
compare the time to diagnosis and the associatedcosts by means of
two DES models describing the currently adopted procedure(scenario
A) and the alternative procedure (scenario B). Implementing DES
modelsallowed to cope with the VSI patient flow complexity and to
avoid the raising of projectcosts associated to real trial runs.
Historical data about VSI patients were availablefrom the emergency
department registries. At the beginning of the inner define
phasethe process boundaries have been defined: the team developing
the project decided thatall but the ED activities required for VSI
patients should be included within the models.This strong
simplification avoids to simulate all the ED activities, i.e. an
overwhelmingtask far from the project objectives. As a consequence,
the results from the simulationruns have been considered as the
lower bound values corresponding to a limitingcondition where all
resources are unlimited, i.e. not shared with other
emergencypatients. After a cycle of meetings and interviews with
the chairs from the departments
involved in the project, two cross-functional process maps
related to scenario A(current procedure) and scenario B
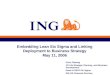
(alternative procedure) have been generated, seeFigures 2 and 3,
respectively.
In the two figures, a rectangular box corresponds to a
value-added activity to beconsidered in the value stream analysis
as well as in the database recordinginformation about resources
needed to perform each activity. The term value-addedactivity means
an operation (a physician consultation or an exam
specificallyperformed for that patient) which adds information to
the patient diagnosis profile. Theset of value-added activities for
the VSI patients has been defined by means ofinterviews with people
from the departments involved in the project.
Both scenarios start with the triage nursing assessment and
colour code assignmentto a patient, which ranges through the
following three levels: white, yellow and green
colour from the less to the most severe assessment. The two
scenarios significantlydiffer in the route whereby yellow and green
patients are examined across the hospitaldepartments.
Accordingly to the current procedure (scenario A), see Figure 2,
only white codepatients (those having apparently light symptoms)
immediately undergo anotoneurologic examination, whose outcome
decides for their admission or discharge.Yellow and green code
patients immediately receive a complete medical assessmentand
undergo a full blood count. If no internal pathologies are
diagnosed, then the
Linking SixSigma to
simulation
261
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
9/20
patient path continues with a cardiological EGC examination and
the study of bloodcardiac markers. If abnormal cardiac conditions
are diagnosed, the patient is admittedto the cardiology ward,
otherwise further exams are started to diagnose suspectneurologic
pathologies: a computer assisted tomography (CAT) exam is
performed.The presence of a pathological condition immediately
calls for the ward admission to astroke unit or a
neurologic/neurosurgery department If the CAT exam does not
revealany pathology, then the patient is sent to the audiology
department to undergo an
Figure 2.Cross-functional processmap of the current VSIpatient
path (scenario A)
IJHCQA25,4
262
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
10/20
otoneurologic exam. The outcome of this exam decides for his/her
admission ordischarge.
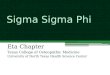
The new procedure (scenario B), see Figure 3, maintains the same
patient flow forthe white code patients as scenario A. However,
yellow and green patients immediatelyreceive a clinical assessment
with questionnaires to detect an abnormal brain diffuse
Figure 3.Cross-functional process
map of the alternative VSI
patient path (scenario B)
Linking SixSigma to
simulation
263
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
11/20
DMAIC
DMADV
Step
Tool
Outcome
Define
***
Selectthequality-improvementproject
Brainstormingmeetings
Managingtheflowofemergency
patientsaffectedbyvertigo
symptoms
illness(VSIpatients)
***
Shouldoneormorescenariosbe
considered?
Brainstormingmeetings
Twoscenarios:thecurrent
andone
alternativeproceduremana
gingVSI
patients
***
Istheareaofimprovementacomplex
process?
Brainstormingmeetings
Yes.Involvementofseveral
departments.Complexpatientpathway
***
Checkavailabilityofexistinghistorical
dataorpossibilityofestimation
Brainstormingmeetings
Yes.Existenceofpatientsr
ecordsand
unitarycosts
Define
Definetheprocessboundaries
Brainstorming,meetings
Studyrestrictedtotheflow
ofpatients
affectedbyVSIbetweenED
entrance
andadmission/discharge
Define
Observe,documentandmapprocess
stepsandflow
BrainstorminginterviewsMicro
soft
Visio
Cross-functionalprocessmapsforthe
twoscenarios
Define
Definethevaluestream
BrainstormingMicrosoftExcel
Databaseofactivitiesforeachinvolved
Departmenttobecompleted
Measure
Measure
Collecthistoricalprocessdata
DataminingtechniquesMicrosoftExcelRawDatabasesofhistoricaldata
Measure
Pre-processhistoricalprocessdata
DataminingtechniquesMicrosoftExcelCleanedDatabasesofhistoricaldata
Measure
Gatherunbiasedestimatesoffurther
data
InterviewssamplingMicrosoftExcel
Estimatesandconfidenceintervalsof
furtherdata
Analyse
Analyse
Stratificationoftheavailabledata
DataminingtechniquesMicrosoftExcelFortheVSIPatients:intera
rrivaltimes
perdayandmonthRatesofpatients
leavingtheserviceProbabilityforeach
colourcodeassignedatthe
triageVSI
PatientsIllnessdiagnosisoccurrencies
Analyse
Distributionfittingofthegrouped
samplesofdata
Statisticalinferenceminitab
Triangulardistributionsfittingtimesto
performeachactivity
Analyse
Classificationofthevalueadded
operationsintoactivityareas
Resourceallocationtools
Completedatabaseofactivitiesforeach
involvedDepartment
(continued)
Table I.The proposed roadmapfor the VSI patient
flowquality-improvementproject
IJHCQA25,4
264
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
12/20
DMAIC
DMADV
Step
Tool
Outcome
Improve
Design
DefinetheDESmodellogicfromthe
processmap
RockwellARENA
Logicdefinitionforthesimulation
modelsofthetwoscenarios
Design
Addtheinformationabouttheavailable
datatotheDESmodel
RockwellARENA
Characterisationofeachobjectmodelfor
thesimulationofthetwoscenarios
Design
DefinetheproperCTQparametersin
the
DESmodel
BrainstormingRockwellARENA
CTQs:Expectedoverallcos
tperyear
ExpectedDepartmentalcos
tsperyear
FlowtimesforeachcategoryofVSI
patient
Verify
ChecktheDESModelLogic
TestingproceduresRockwellARENA
Correctmodellogicforeachscenario
Verify
ValidatetheDESmodel
TestingproceduresinterviewsR
ockwell
ARENA
DESmodelsforthetwoscenarios
validatedandreadytoberunfor
comparisonpurposes
Improve
***
Designtheexperimentalplan
Minitab/designexpertRockwell
ARENA
CTQsassumedasresponse
variables
Factorspossiblyaffectinge
achscenario
configurationDesignofthe
experiment
***
RuntheDESmodelreplications
RockwellARENA
ValuesoftheCTQsforeachrun
***
PerformastatisticalanalysisonCTQ
sto
comparethescenarios
Minitab/designexpertRockwell
ARENA
Empiricaldistributionsand
parameters
fortheCTQs
***
Selectthebestperformingscenario
BrainstormingRockwellARENA
Bestscenarioandoptimalv
aluesforthe
CTQs
Control
***
Estimatecost/timesavingsandresource
utilisation
RockwellARENA
Reportsaboutcostandtimedataand
resourceutilisation
***
Document,communicateandvisualise
results
Meetings
Presentationanddissemina
tionofthe
results
Table I.
Linking SixSigma to
simulation
265
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
13/20
perfusion: if a perfusion is suspected, then cardiological exams
are immediatelystarted. The outcome of these exams supports
decisions about the ward admissiondestination of a patient. If the
abnormal brain diffuse perfusion is not suspected for ayellow/green
patient, then the otoneurologic examination is immediately
conducted.
The patient flow continues with the admission within the
audiology ward or therequest of a neurologic visit including a CAT
exam.
When the suspicion of neurological pathologies is excluded, a
complete medicalassessment with blood count is started to detect
the presence of internal organpathologies. Scenario B significantly
increases the audiology department workloadbecause the
otoneurologic examination is scheduled at the beginning of the
patientflow, whatever the patient colour code. It calls for a 24
hours presence or availability ofa specialised physician. However,
at the moment of designing scenario B professionalsinvolved in the
project believed this would reduce the overall number of
examsrequired to get a diagnosis for a patient and consequently the
associated times andcosts.
The VSI patients completing the path to diagnosis and needing to
be hospitalisedhave been categorised into one of the following four
groups, depending on thedepartment wherein the ward admission is
decided: audiology (AD), cardiology (CD),medicine (MD),
neurology/neurosurgery/stroke unit (ND). Based on the information
inthe cross-functional process maps, the development of a
spreadsheet containing thedatabase of activities completed the
define phase.
During the measure phase, historical data was collected from the
emergencydepartment. Information about every VSI patient arriving
at the ED in 2007 wasretrieved and coded into spreadsheets. When a
service characterised by multiple flowsof patients is to be
modelled, the transportation time estimation and the
relativeresources availability should be carefully investigated by
practitioners becausedifferent hospital configurations can lead to
sensibly different patient flow times. Thus,
further information has been gathered by means of time study and
interviews with EDnurses and professionals about the times required
to perform exams and to directpatients from one department to
another. With the exception of the audiologydepartment, all the
other departments and wards involved in the case study are
locatedat different floors in the same building. This location of
the departments significantlyreduces the transportation times to a
few walking minutes. Finally, unit costs ofresources and exams have
been retrieved from the hospital IT system.
During the analyse phase, a statistical distribution has been
fitted to each family ofsampled data by means of the Minitabw
commercial software: patients inter-arrivaltimes have been modelled
through exponential distributions; the times to completemedical
exams and to transport patients between departments have been
modelledthrough triangular and normal distributions. The explicit
values of times and costs for
each exam and patient transfer are not reported here for the
sake of brevity. Table IIpresents the stratified historical data
about the VSI patients.
The improve phase of the roadmap has been started by designing
the DES modelscorresponding to the two scenarios within the
Rockwell ARENAw simulationenvironment: the cross functional process
maps presented in Figures 2 and 3 helpedconsultants in designing
the models. Several activity areas each coinciding with adepartment
have been introduced in the two models to get explicit cost
estimation foreach involved department, (Kelton et al., 2007).
Model logic was animated by means of
IJHCQA25,4
266
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
14/20
suitable pictures to facilitate comprehension during the results
dissemination. Then, the
CTQs to be collected by the DES models have been selected.
According to the project
objectives, a set of departmental yearly costs have been
identified to quantify the service
effectiveness for each scenario. Similarly, the service
efficiency for each scenario has been
quantified through the computation of the mean flow time for
each category of VSI
patient, from the emergency department entrance to the ward
admission or discharge.
Overall, ten response variables have been considered (see Table
III).
Model logic checking and validation was achieved through several
trial runs. A
direct comparison with the available historical data did not
show any anomaly. The
two scenarios have been assumed as potential factors affecting
the service CTQs. Foreach scenario model, 1,000 replications have
been run. Table IV shows the replication
statistics of the CTQs for both scenarios. An empirical
distribution fitting of the yearly
costs based on the Anderson Darling test led to model them as
Gamma distributed
random variables. Thus, in Table IV, for each cost the expected
value, the scale
parameter uand the shape parameter k of the fitting Gamma
distribution are reported.
Interarrival rates of VSI patients showing at the ED(exponential
distrib.)2.25 patients/day 8 a.m.-3 p.m.
3 p.m.-8p.m.8 p.m.-8a.m.
0.966 patients/day0.495 patients/day0.788 patients/day
Incidence of colour codes for VSI patientsWhite (%) 9.4Yellow
(%) 10.3Green (%) 80.3
VSI patients completing the path to diagnosis (%) 68
VSI patients needing admission (%) 31
Incidence of each in-patient groupAudiology (%) 33Cardiology (%)
15Medicine (%) 43
Neurol./neurosurg./stroke unit (%) 9
Table II.Historical data observed
for the VSI patients
during year 2007
CTQs
CTOT [e/year] Total cost to deliver the service to VSI
patientsCED [e/year] Cost at the emergency department
CAD [e/year] Cost at the audiology departmentCLD [e/year] Cost
at the laboratory test departmentCRD [e/year] Cost at the radiology
department
FTAD [h ] Mean flow time of the patients admitted within the
audiology department wardFTCD [h ] Mean flow time of the patients
admitted within the cardiology department wardFTMD [h ] Mean flow
time of the patients admitted within the medicine department
wardFTND [h ] Mean flow time of the pat. adm. within the
neurology/neurosurg./stroke unit dept.
wardFTDP [h ] Mean flow time of the discharged patients
Table III.The critical to quality
parameters (CTQs)selected for the case
study
Linking SixSigma to
simulation
267
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
15/20
CTOT
CED
CAD
CLD
CRD
FTAD[h]
Scen.
[e/year]
[e/year]
[e/year]
[e/year]
[e/year]
White
Y/G
FTC
D[h]
FTMD[h]
FTND[h]
FTDP[h]
A
98285
63318
8507
16368
10092
3.25(0.87)
4.57(0.66)
1.7
3(0.07)
1.14(0.02)
2.22(0.15)
2.51(0.14)
u
36014
23178
3216
5990
3790
k
2.729
2.732
2.645
2.732
2.663
B
65209
42261
20279
835
1834
1.50(0.56)
1.71(0.51)
1.2
9(0.02)
1.29(0.01)
2.23(0.62)
1.67(0.3)
u
24136
15634
7533
324.5
672
k
2.702
2.703
2.692
2.574
2.729
DC%
2
33.7
233.3
138.4
2
94.9
2
81.8
DT%
2
53.8
2
62.6
2
25.4
13.2
0.4
2
33.5
Table IV.Comparison of scenario Bvs scenario A. Resultsfrom the
simulation runs
IJHCQA25,4
268
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
16/20
The control phase of the project started with the evaluation of
the cost and flow timesavings obtained by simulating the B
scenario. Cost comparisons presented in Table IVimmediately show
that the effectiveness of scenario B clearly overcomes that
ofscenario A:
. The yearly expected cost saving to deliver the service to VSI
patients equals 33.7per cent.
. The yearly expected cost saving in the emergency department
equals 33.3 percent.
. As expected by the project development team, the number of
seized exams in theaudiology department is significantly increased:
thus, the yearly expected costincreases of 138.4 per cent.
. The largest cost savings are achieved in the laboratory test
department, (DC percent 294.7 per cent), and the radiology
department, (DC per cent 281.8 percent); this means that the
currently adopted procedure calls for a significantlylarger number
of blood and CAT exams than required.
Finally, the availability of empirical distributions for each of
the investigated costsallows decision makers to take decisions
about provisional budgets for the servicedelivery based on reliable
data estimation.
Table IV also presents within parentheses the mean and the
standard deviation ofthe flow times for each category of patients
and the flow time percentage reduction DTper cent obtained by
implementing scenario B as opposed to scenario A. Theperformance of
scenario B in terms of efficiency is better than that of scenario
A. Inparticular, it has been found that:
. The expected flow times for patients who need to be admitted
in the audiologydepartment ward reduce of more than 50 per cent
whereas those admitted in the
cardiology department reduce their flow time of more than 25 per
cent.. The expected flow time increases for those to be admitted in
the medicine
department (13.2 per cent), and remains quite unchanged for
patients having apathological condition to be treated within the
neurology/neurosurgery/strokeunit departments.
Thus, the project demonstrates that scenario B looks promising
both in terms ofservice efficiency and in terms of efficacy and
that it is worth choosing it for furtherinvestigation and the
implementation of real trial runs. Dissemination of results
toprofessionals working in the hospital and a cycle of informative
meetings with peoplefrom other hospitals completed the project.
Lessons learned and benefits from the proposed approachThe
implementation of the roadmap to the in-hospital case study allowed
somestrength points of the proposed theoretical framework to be
experienced. First,getting a precise definition of the
cross-functional process maps and the value-addedstream analysis at
the early steps of the project i.e. during the design phase was
demonstrated to be a key factor in stating the problem correctly
andsuccessfully developing the project. During the brainstorming
meetings, doctors,nurses and technicians were stimulated to
re-think every step of the service in
Linking SixSigma to
simulation
269
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
17/20
which they operate as resources; a shared view about the way
service is deliveredand the awareness about eliminating unnecessary
activities can be progressivelyachieved through this problem
solving approach. Some bugs have been detected inthe hospitals
information system during the measure and analyse phase aimed
at
collecting and fitting the historical data: these have been
progressively corrected oreliminated. The improve phase required
the design and validation of the twosimulation models. The trial
tests on the models were performed at the presence ofthe chairs of
the involved departments: the graphical representation of the
patientflows during the simulation runs helped professionals from
the hospital to visualisethe entire flows and detect the presence
of bottlenecks increasing flow times;statistical distribution
fitting for the expected costs allowed budgeting forecasts tobe
prepared; the evaluation of percentage costs savings and flow times
reductionprovided with a quantitative basis of knowledge to promote
further investigation ofscenario B. Finally, dissemination of the
results inside and outside the hospitalduring meetings and seminars
received a positive feedback from operators,
especially in terms of interest to the roadmap implementation to
other healthcaresettings. In particular, during seminars the
interest was originated by the
opportunity that such a procedure gives to people in achieving
self-awareness aboutthe activities they are requested to do in
their organisation. In those seminars wheredeveloping part of the
design procedure was proposed as a classroom exercise forsmall
groups, great emphasis was put by the attendees in the process of
visualisingthe procedures they usually follow in their
organisations through process maps. Thecommon feeling was that
getting precise process maps allowed for a re-thinking
andquestioning of apparently well-structured practices and finding
useless activities.Sharing different points of view further
enriched this process. Showing thegraphical interface of the DES
models during the simulation running increasedinterest in the
classroom. Costs and time estimates based on simulated data
gavepeople more confidence to figure out workload and budgeting for
each involveddepartment.
It is worth noting that by linking the Six Sigma quality
perspective to theoperational research toolbox, the proposed
roadmap can serve as an operationalframework to create
opportunities for starting innovative Lean Six Sigma experiencesin
the healthcare organisation (George, 2003; De Koning et al., 2006):
its intrinsicstructure allows both activities control and the
identification and elimination of wasteand non-value added
activities, i.e. the muda, as commonly known by the lean
thinkingpractitioners. Further investigation is suggested in this
direction.
Lastly, it is also important to speak about some shortfalls of
the proposedframework. First, there are many situations where some
prerequisites required to start
the synergy are not respected. Second, as stated in (Jackson,
2003), problem contextswithin an organisation can be different
depending on the combination of the followingtwo dimensions: the
nature of the investigated system/organisation, i.e. simple
orcomplex, and the attitude of participants: unitary or pluralist
or coercive. Qualitymanagement in the service sector, and in
particular healthcare organisations, can coverall of these problem
contexts depending on the level of the organisation it
impacts.Given this perspective, the proposed roadmap supporting
sharply-focusedquality-improvement projects is particularly suited
to support system thinking and
IJHCQA25,4
270
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
18/20
problem solving when a simple unitary combination is present.
This is the field ofapplication of what is called hard system
thinking.
ConclusionsThis paper has presented a theoretical framework
based on a roadmap defining anapproach integrating Six Sigma and
discrete-event simulation during the developmentof a
quality-improvement project. The roadmap merges DMAIC/DMADV
orDMADV/DMADV Six Sigma procedures in a hierarchical approach aimed
atdeveloping the Six Sigma project and the simulation model. The
roadmap has beentested to carry out a project focused on the
re-organisation of the flow of emergencypatients affected by
vertigo symptoms. The implementation of the proposed roadmapallowed
the following potential benefits to be identified:
. The design of a DES model aimed at simulating and comparing
differentscenarios is significantly enhanced by the adoption of the
roadmap, whichsimplifies the formalisation and execution of the
successive steps to get a correctmodel.
. Conversely, the Six Sigma quality improvement project cost can
be significantlyreduced if DES simulation can be adopted: in fact,
real trial runs are not neededto get results about different
process configurations.
. Discussion and dissemination of results inside and outside an
organisation isfacilitated by the roadmap because it can serve as a
structured approach to befollowed during presentations.
Visualisation of the different scenarios throughDES models
stimulates the interest of people and makes the comprehension
andmotivation of results easier.
The positive outcome from the practice has demonstrated the
effectiveness of the
proposed roadmap in the healthcare field and calls for further
investigation in otherclinical settings. Thus, research will be
continued in this direction to enhance theproposed framework and to
create potential opportunities for Lean Six Sigmaimplementation in
healthcare.
References
De Koning, H., Verver, J.P.S., Van den Heuvel, J., Bisgaard, S.
and Does, R.J.M.M. (2006), LeanSix Sigma in healthcare, Journal for
Healthcare Quality, Vol. 28, pp. 4-11.
Feng, Q. and Manuel, C.M. (2008), Under the knife: a national
survey of Six Sigma programs inus healthcare organizations,
International Journal of Health Care Quality Assurance,Vol. 21, pp.
535-47.
Fletcher, A. and Worthington, D. (2009), What is a generic
hospital model? A comparison ofgeneric and specific hospital models
of emergency patient flows, Health Care
Management Science, Vol. 12, pp. 374-91.
George, M.L. (2003),Lean Six Sigma for Service: How to Use Lean
Speed and Six Sigma Quality toImprove Services and Transactions,
McGraw-Hill, New York, NY.
Glickman, S.W., Baggett, K.A., Krubert, E.D., Peterson, E.D. and
Schulman, K.A. (2007),Promoting quality: the health-care
organization from a management perspective,
International Journal for Quality in Healthcare, Vol. 19 No. 6,
pp. 341-8.
Linking SixSigma to
simulation
271
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
19/20
Guglielmino, M.G., Celano, G., Costa, A. and Fichera, S. (2009),
Modelling a radiologydepartment service using a VDL integrated
approach, Journal of Health Organisation and
Management, Vol. 23 No. 4, pp. 376-95.
Hillier, F.S. and Lieberman, G.J. (2005), Introduction to
Operations Research, 8th ed.,
McGraw-Hill, Singapore.Jackson, M.C. (2003), Systems Thinking:
Creative Holism for Managers, Wiley, Chichester.
Jun, J., Jacobson, S. and Swisher, J . (1999), Application of
discrete-event simulation in health careclinics: a survey, Journal
of the Operational Research Society, Vol. 50, pp. 109-23.
Kelton, D.V., Sadowski, R.P. and Sturrock, D.T. (2007),
Simulation with Arena, 4th ed.,McGraw-Hill, New York, NY.
Linderman, K., Schroeder, R.G., Zaheer, S. and Choo, A.S.
(2003), Six Sigma: a goal theoreticperspective, Journal of
Operations Management, Vol. 21 No. 2, pp. 193-203.
Magnusson, K., Kroslid, D. and Bergman, B. (2003), Six Sigma The
Pragmatic Approach,2nd ed., Studentlitteratur, Lund.
Pyzdek, T. (2003), The Six Sigma Handbook, McGraw-Hill, New
York, NY.
Sehwail, L. and DeYong, C. (2003), Six Sigma in health care,
International Journal of HealthCare Quality Assurance Incorporating
Leadership in Health Services, Vol. 16 No. 4, pp. 1-5.
Seppanen, M.S., Chandra, C. and Kumar, S. (2005), Process
Analysis and Improvement: Tools andTechniques, McGraw-Hill Irwin,
New York, NY.
Taner, M.T. and Sezen, B. (2009), An application of Six Sigma
methodology to turnoverintentions in health care, International
Journal of Health Care Quality Assurance, Vol. 22No. 3, pp.
252-65.
Taner, M.T., Sezen, B. and Antony, J. (2007), An overview of Six
Sigma applications inhealthcare industry, International Journal of
Health Care Quality Assurance, Vol. 20 No. 4,pp. 329-40.
Tang, L.C., Goh, T.N., Lam, S.W. and Zhang, C.-W. (2007),
Fortification of Six Sigma: expanding
the DMAIC toolset, Quality and Reliability Engineering
International, Vol. 23 No. 1,pp. 3-18.
Van den Heuvel, J., Does, R.J.M.M. and Vermaat, M.B. (2004), Six
Sigma in a Dutch hospital:does it work in the nursing department?,
Quality and Reliability Engineering International,Vol. 20 No. 5,
pp. 419-26.
Van Den Heuvel, J., Does, R.J.M.M. and Verver, J.P.S. (2005),
Six Sigma in healthcare: lessonslearned from a hospital,
International Journal of Six Sigma and Competitive Advantage,Vol. 1
No. 4, pp. 380-8.
About the authorsGiovanni Celano received his PhD in 2003 from
the University of Palermo defending a thesis on
the sequencing of mixed model assembly lines. He is currently
Assistant Professor at theUniversity of Catania (Italy). His
research is focused on statistical quality control,
productionscheduling and operations management applied to both
industrial and service sector. He iscurrently a member of the
European Network of Business and Industry Statistics (ENBIS),
andthe International Institute for Innovation, Industrial
Engineering and Entrepreneurship (I4e2). Hehas authored/co-authored
about 85 papers in international journals and in the proceedings
ofnational and international conferences. Dr Celano is Associate
Editor ofQuality Technology andQuantitative Management. Giovanni
Celano is the corresponding author and can be contacted
at:[email protected]
IJHCQA25,4
272
-
7/27/2019 Linking Six Sigma to simulation a new roadmap to
improve the quality of patient care
20/20
Antonio Costa holds a PhD in Structural Mechanics from the
University of Catania. He iscurrently Assistant Professor in
Technology and Manufacturing Systems at the University ofCatania
(Italy) and a Senior Member of the Associazione Italiana di
Tecnologia Meccanica(AITeM). His research involves supply chain
network management, mixed model assembly line
sequencing and heuristic optimisation applied to manufacturing
systems. He is a co-author ofabout 45 papers published in
international journals and in the proceedings of national
andinternational conferences.
Sergio Fichera is an Associate Professor in Technology and
Manufacturing System at theDipartimento di Ingegneria Industriale e
Meccanica of the University of Catania, (Italy). He holdsa MS
degree from the University of Catania and MBA degree from the
Schools of Management atthe University of Turin. His research
interests are in production scheduling, statistical qualitycontrol,
optimisation of machining processes. He is a member of the
Associazione Italiana diTecnologia Meccanica (AITeM). He has
co-authored about 80 papers in international journalsand in the
proceedings of national and international conferences.
Giuseppe Tringali is the head of the Audio-Vestibolo-Fonologia
Unit at the Vittorio Emanuelehospital, Catania (Italy). He
frequently collaborates with the University of Catania to
developquality improvement and service re-engineering projects in
the healthcare field.
Linking SixSigma to
simulation
273
To purchase reprints of this article please e-mail:
[email protected] visit our web site for further
details: www.emeraldinsight.com/reprints