Embed Size (px)
Citation preview

CLINICAL BRIEF
Linear and Skull Growth in Extremely Low BirthWeight Babies with Rickets of Prematurity
Monika Sharma & Inderpreet Sohi
Received: 27 May 2010 /Accepted: 27 September 2011 /Published online: 14 October 2011# Dr. K C Chaudhuri Foundation 2011
Abstract Preterm birth results in poor accretion of boneminerals and development of rickets of prematurity.Poor skeletal growth is one of the long term morbiditiesof this condition, which is said to have a lesser effecton the skull growth. The present study was a retrospec-tive observational study to compare the effect of ricketsof prematurity on the linear and skull growth in the firstyear of life. In this retrospective analysis, 1 y follow-uprecords of extremely low birth weight (ELBW) babiesborn in five consecutive years and their anthropometricdata were evaluated. ELBW babies with confirmedrickets of prematurity were taken as the study groupand those without were taken as the control group andanthropometric values (head size and length) at variousages in the first year of life were compared usingrelevant statistical software. Both the lengths and headsizes of the babies in the two groups were found to becomparable until the age of 12 mo.
Keywords Rickets of prematurity . Extremely low birthweight babies
Introduction
Extremely low birth weight preterms are born with thedisadvantage of missing the bone mineral accretion in thelast trimester of pregnancy. Delayed breast feeding andproblems requiring prolonged methylxanthines, diuretics
and corticosteroids (which may cause mineral loss),increases the likelihood of developing rickets of prematu-rity (ROP). The incidence of rickets of prematurity is asmuch as 30% in babies born before 28 wk of gestation andup to 50% in babies with birth weights of less than 1,000 g[1]. ROP can present with overt rickets in the first 6 mo oflife and is also linked to myopia of prematurity, persistentrespiratory problems and poor growth in childhood,especially in the first 18 mo of life [2, 3].
ROP can be detected early by performing biochemicaltests like serum calcium, phosphorus and alkaline phospha-tase (ALP). Rise in ALP is considered an early marker andis more important in early detection than a radiologicalexamination [4]. Higher ALP levels have also been linkedwith a worse growth outcome [5]. The exact referencevalues of ALP in the preterm babies (and for various gradesof prematurity) are not available. It has been suggested, thatvalues above 5 times the adult reference values indicateabnormality [6]. ROP is not related to vitamin D deficiencyor a metabolic defect and is managed with appropriatedietary addition of calcium and phosphorus along with lowdose vitamin D supplements [7–9].
Aims and Objectives
To compare the linear and head growth of extremely lowbirth weight babies with and without rickets of prematurityin the first year of life.
Material and Methods
This was a retrospective observational study of theextremely low birth weight babies born in a 5 y period in
M. Sharma (*) : I. SohiDepartment of Pediatrics, Christian Medical College,Brown Road, Ludhiana, Punjab 141008, Indiae-mail: [email protected]
Indian J Pediatr (May 2012) 79(5):655–658DOI 10.1007/s12098-011-0565-z
a tertiary care centre in Punjab. This study was undertakento compare the linear and head growth of extremely lowbirth weight babies with and without rickets of prematurityin the first year of life.
Delivery records were evaluated and all neonates withbirth weight less than 1,000 g noted. Admission records andoutpatient records of all these babies were evaluated andanthropometric data at birth and follow up visits at 1, 2, 4,6, 9 and 12 mo of age were noted. Babies, who died orfailed to follow up after the initial discharge, were excludedfrom the study.
As per hospital protocols a serum alkaline phosphatasewas done at the age of 4 wk and levels five times the
normal adult value considered as an indicator of rickets ofprematurity. Skeletal radiographs were not done as part ofthe initial investigation. Babies diagnosed with rickets ofprematurity were taken as the study group and babies withnormal levels of alkaline phosphatase were considered asthe control group.
Maternal details and perinatal events were also noted.Babies in both the groups received calcium, phosphorussupplements and maintenance doses of vitamin D as percurrent recommendations.
The data thus collected were entered in MS Excel 2003and comparison between groups made using the SPSSsoftware version 12 for windows.
35 Extremely low birth weight babies
2015
1 lost after birth
3 lost after birth
Diagnosed as rickets of prematurity
No ricketsof prematurity
14 Controls17 Cases
Serum ALP at 4 wk age
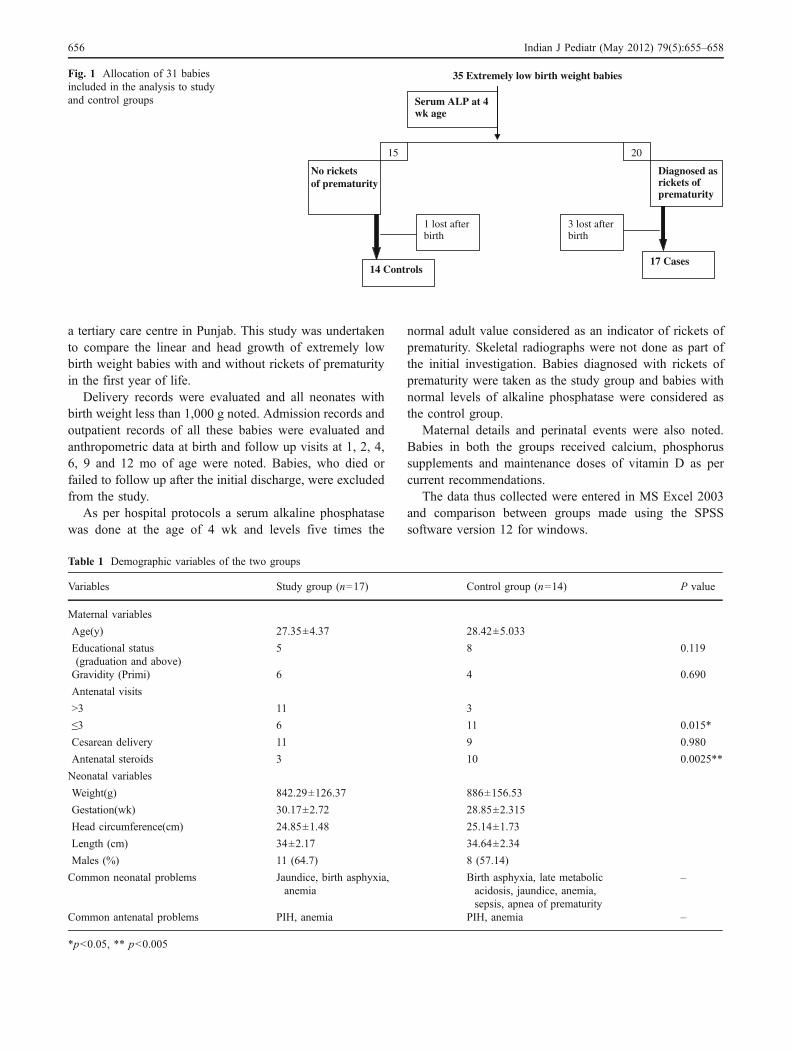
Fig. 1 Allocation of 31 babiesincluded in the analysis to studyand control groups
Table 1 Demographic variables of the two groups
Variables Study group (n=17) Control group (n=14) P value
Maternal variables
Age(y) 27.35±4.37 28.42±5.033
Educational status(graduation and above)
5 8 0.119
Gravidity (Primi) 6 4 0.690
Antenatal visits
>3 11 3
≤3 6 11 0.015*
Cesarean delivery 11 9 0.980
Antenatal steroids 3 10 0.0025**
Neonatal variables
Weight(g) 842.29±126.37 886±156.53
Gestation(wk) 30.17±2.72 28.85±2.315
Head circumference(cm) 24.85±1.48 25.14±1.73
Length (cm) 34±2.17 34.64±2.34
Males (%) 11 (64.7) 8 (57.14)
Common neonatal problems Jaundice, birth asphyxia,anemia
Birth asphyxia, late metabolicacidosis, jaundice, anemia,sepsis, apnea of prematurity
–
Common antenatal problems PIH, anemia PIH, anemia –
*p<0.05, ** p<0.005
656 Indian J Pediatr (May 2012) 79(5):655–658
Results
Of the total of 7,635 live births in the 5 y study period, 35extremely low birth weight babies were born.
Figure 1 shows the allocation of the 31 babies includedin the analysis. The number of babies on regular follow up,in both groups, decreased significantly after 6 mo of life.Maternal and neonatal details recorded are presented inTable 1.
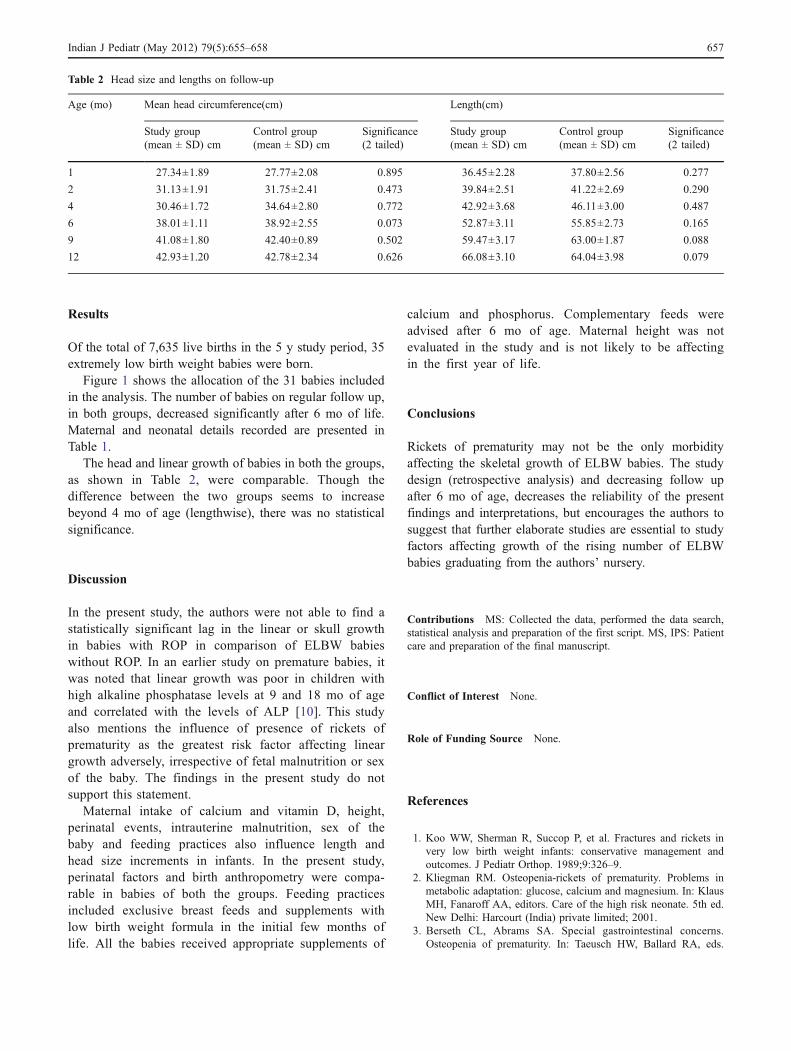
The head and linear growth of babies in both the groups,as shown in Table 2, were comparable. Though thedifference between the two groups seems to increasebeyond 4 mo of age (lengthwise), there was no statisticalsignificance.
Discussion
In the present study, the authors were not able to find astatistically significant lag in the linear or skull growthin babies with ROP in comparison of ELBW babieswithout ROP. In an earlier study on premature babies, itwas noted that linear growth was poor in children withhigh alkaline phosphatase levels at 9 and 18 mo of ageand correlated with the levels of ALP [10]. This studyalso mentions the influence of presence of rickets ofprematurity as the greatest risk factor affecting lineargrowth adversely, irrespective of fetal malnutrition or sexof the baby. The findings in the present study do notsupport this statement.
Maternal intake of calcium and vitamin D, height,perinatal events, intrauterine malnutrition, sex of thebaby and feeding practices also influence length andhead size increments in infants. In the present study,perinatal factors and birth anthropometry were compa-rable in babies of both the groups. Feeding practicesincluded exclusive breast feeds and supplements withlow birth weight formula in the initial few months oflife. All the babies received appropriate supplements of
calcium and phosphorus. Complementary feeds wereadvised after 6 mo of age. Maternal height was notevaluated in the study and is not likely to be affectingin the first year of life.
Conclusions
Rickets of prematurity may not be the only morbidityaffecting the skeletal growth of ELBW babies. The studydesign (retrospective analysis) and decreasing follow upafter 6 mo of age, decreases the reliability of the presentfindings and interpretations, but encourages the authors tosuggest that further elaborate studies are essential to studyfactors affecting growth of the rising number of ELBWbabies graduating from the authors’ nursery.
Contributions MS: Collected the data, performed the data search,statistical analysis and preparation of the first script. MS, IPS: Patientcare and preparation of the final manuscript.
Conflict of Interest None.
Role of Funding Source None.
References
1. Koo WW, Sherman R, Succop P, et al. Fractures and rickets invery low birth weight infants: conservative management andoutcomes. J Pediatr Orthop. 1989;9:326–9.
2. Kliegman RM. Osteopenia-rickets of prematurity. Problems inmetabolic adaptation: glucose, calcium and magnesium. In: KlausMH, Fanaroff AA, editors. Care of the high risk neonate. 5th ed.New Delhi: Harcourt (India) private limited; 2001.
3. Berseth CL, Abrams SA. Special gastrointestinal concerns.Osteopenia of prematurity. In: Taeusch HW, Ballard RA, eds.
Table 2 Head size and lengths on follow-up
Age (mo) Mean head circumference(cm) Length(cm)
Study group(mean ± SD) cm
Control group(mean ± SD) cm
Significance(2 tailed)
Study group(mean ± SD) cm
Control group(mean ± SD) cm
Significance(2 tailed)
1 27.34±1.89 27.77±2.08 0.895 36.45±2.28 37.80±2.56 0.277
2 31.13±1.91 31.75±2.41 0.473 39.84±2.51 41.22±2.69 0.290
4 30.46±1.72 34.64±2.80 0.772 42.92±3.68 46.11±3.00 0.487
6 38.01±1.11 38.92±2.55 0.073 52.87±3.11 55.85±2.73 0.165
9 41.08±1.80 42.40±0.89 0.502 59.47±3.17 63.00±1.87 0.088
12 42.93±1.20 42.78±2.34 0.626 66.08±3.10 64.04±3.98 0.079
Indian J Pediatr (May 2012) 79(5):655–658 657

Avery’s diseases of the Newborn. 7th ed. Printed at Thompsonpress Noida: Harcourt Asia; 2000. pp. 970–3.
4. Glass EJ, Hume R, Hendry GM, Strange RC, Forfar JO. Plasmaalkaline phosphatase activity in rickets of prematurity. Arch DisChild. 1982;57:373–6.
5. James JA, Mayne PD, Barnes IC, Kovar IZ. Growth velocity andplasma alkaline phosphatase activity in the preterm infant. EarlyHum Dev. 1985;11:27–32.
6. Kovar I, Mayne P, Barltrop D. Plasma alkaline phosphataseactivity, a screening test for rickets in preterm neonates. Lancet.1982;1:308–10.
7. McIntosh N, Livesey A, Brooke OG. Plasma 25-hydroxyvitaminD and rickets in infants of extremely low birth weight. Arch DisChild. 1982;57:848–50.
8. Alizade P, Naderi F, Sotoudeh K. A randomized clinical trial ofprophylactic effects of vitamin D on different indices ofosteopenia of prematurity. Iranian J Publ Health. 2006;35:58–63.
9. Greer FR. Vitamin metabolism and requirements in the micro-premie. Clin Perinatol. 2000;27:95–118.
10. Lucas A, Brooke OG, Baker BA, Bishop N, Morley R. Highalkaline phosphatase activity and growth in preterm neonates.Arch Dis Child. 1989;64:902–9.
658 Indian J Pediatr (May 2012) 79(5):655–658