Embed Size (px)
Citation preview

Clinical Radiology (1994) 49, 252-255
Life-Threatening Arterial Haemorrhage: Results of Treatment by Transcatheter Embolization Using Home-Made Steel Coils S. SHARMA, S. S. KOTHARI*, M. RAJANI and P. V E N U G O P A L t
Departments of Cardiovascular Radiology, *Cardiology and ~Cardiothoracic and Vascular Surgery, All India Institute of Medical Sciences, New Delhi, India
Major arterial haemorrhage can be fatal. Its management by percutaneous embofization using commercially available embolizing agents is well established. We describe the use of home- made steel coils in the treatment of five patients. These coils were designed during the procedure in order to conform to the dimension of the bleeding artery. The group included two patients with life-threatening haemoptysis after surgical correction for tetralogy of Fallot; one patient each with exsanguinating haemorrhage from a branch of the left profunda femoral artery following violent trauma; massive haematuria due to an inoperable hypernephroma; and haemoptysis due to post-tubercular bronchiectasis. The bleeding vessel was evaluated by selective angiography in each patient. After assessing its length and diameter, steel coils of desired dimensions were made by utilizing a conventional 0.032-in wide guidewire and these were released into the bleeding artery. Occlusion of the bleeding vessel was obtained in all patients, without complication. Fabrication of coils of desired length and diameter can be done within a few minutes during the procedure. These coils provide an effective method of treating fife-threatening arterial haemorrhage in selected cases. Sharma, S., Kothari, S.S., Rajani, M. & Venugopal, P. (1994). Clinical Radiology 49, 252-255. Life-Threatening Arterial Haemorrhage: Results of Treatment by Transcatheter Embolization Using Home-Made Steel Coils
Accepted for Publication 20 September 1993
The technique and role of therapeutic arterial emboliza- tion are well established in many clinical conditions [l-5]. A number of new embolic agents and delivery systems have been reported recently [6-8]. Commercially avail- able steel coils are widely used for transcatheter occlusion of blood vessels. But these are expensive and not always readily available, especially in an emergency. In this report we describe the technique of fabricating steel coils of desired dimensions. These coils were designed during the angiographic procedure and successfully used to treat exsanguinating arterial haemorrhage in five patients.
PATIENTS AND M E T H O D S
Five patients with massive arterial haemorrhage were treated by this method. The group included two patients with haemoptysis on the third and sixth post-operative day following total surgical correction in tetralogy of Fallot, one patient each with haemorrhage from a branch of the left profunda femoral artery following violent trauma, haematuria from an inoperable hypernephroma, and haemoptysis secondary to post-tubercular bronchi- ectasis. All the patients were males and the age ranged between 4 and 49 years (mean, 25 years). Table 1 gives the demographic information about these patients.
In each patient, the systemic blood pressure was stabilized by supportive management, including matched blood transfusion. Informed, written consent was obtained from each patient. At the beginning of the procedure, a complete angiogram was obtained by utiliz-
Correspondence to: Dr Sanjiv Sharma, Department of Radiodiagno- sis, All India Institute of Medical Sciences, New Delhi 110029, India.
ing digital subtraction or cine angiography on a commer- cially available Polydiagnost C (Philips Medical Systems, The Netherlands) or Angiotron CMP (Siemens, Ger- many) unit, Multi-purpose or Picard catheters (William Cook Company, Australia) and an ionic, iodinated, water-soluble contrast medium (Urografin 76%, Schering AG, Germany) to provide full vascular mapping. The bleeding artery was selectively catheterized and the length and diameter of the bleeding artery were measured on the angiogram.
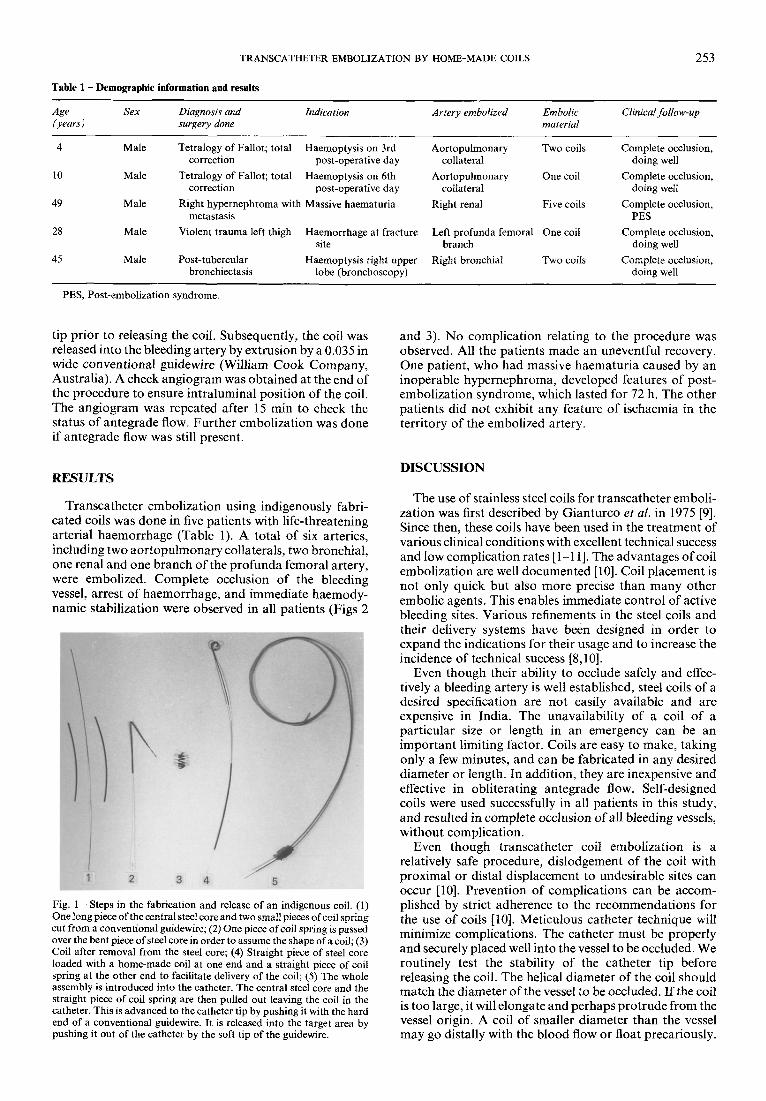
The coil was made from a conventional 0.032-in wide guidewire. The steps are illustrated in Fig. 1. The two ends of the guidewire were cut by a scissors to remove the central steel core and the fine safety wire from the outer coil spring. Two 20-cm long pieces were cut from the central steel core. One of them was kept for introducing the coil into the catheter. The other piece was bent at an acute angle 5 cm from its tip. A 5-10 cm long piece of the coil spring was introduced over this bent piece of steel core from the straight end. Upon withdrawal from the bent end, it assumed the shape of a coil. We observed that the diameter of this coil was directly proportional to the angle of the bend of the steel core. The length of the coil was shortened, if necessary to suit the dimensions of the bleeding vessel. The two ends of the coil were trimmed and blunted by using sand paper, previously sterilized by ethylene dioxide gas. This coil was loaded on the straight piece of steel core and backed up by a straight piece of coil spring for releasing into the catheter (Fig. 1). It took about 5-10 min to make coils in this manner.
The selective position of the catheter was checked by contrast injection before releasing the coil. A conven- tional guidewire was passed through the catheter into the bleeding artery in order to test the stability of the catheter
TRANSCATHETER EMBOLIZATION BY HOME-MADE COILS
Table 1 - Demographic information and results
253
Age Sex Diagnosis and Indication Artery embotized Embotic Clinical follow-up (years) surgery done material
4 Male Tetralogy of Fallot; total Haemoptysis on 3rd Aortopulmonary Two coils Complete occlusion, correction post-operative day collateral doing well
10 Male Tetralogy of Fallot; total Haemoptysis on 6th Aortopulmonary One coil Complete occlusion, correction post-operative day collateral doing well
49 Male Right hypernephroma with Massive haematuria Right renal Five coils Complete occlusion, metastasis PES
28 Male Violent trauma left thigh Haemorrhage at fracture Left profunda femoral One coil Complete occlusion, site branch doing well
45 Male Post-tubercular Haemoptysis right upper Right bronchial Two coils Complete occlusion, bronchiectasis lobe (bronehoscopy) doing well
PES, Post-embolization syndrome.
tip prior to releasing the coil. Subsequently, the coil was released into the bleeding artery by extrusion by a 0.035 in wide conventional guidewire (William Cook Company, Australia). A check angiogram was obtained at the end of the procedure to ensure intraluminal position of the coil. The angiogram was repeated after 15 min to check the status of antegrade flow. Further embolization was done if antegrade flow was still present.
RESULTS
Transcatheter embolization using indigenously fabri- cated coils was done in five patients with life-threatening arterial haemorrhage (Table 1). A total of six arteries, including two aortopulmonary collaterals, two bronchial, one renal and one branch of the profunda femoral artery, were embolized. Complete occlusion of the bleeding vessel, arrest of haemorrhage, and immediate haemody- namic stabilization were observed in all patients (Figs 2
Fig. 1 - Steps in the fabrication and release of an indigenous coil. (1) One long piece of the central steel core and two small pieces of coil spring cut from a conventional guidewire; (2) One piece of coil spring is passed over the bent piece of steel core in order to assume the shape of a coil; (3) Coil after removal from the steel core; (4) Straight piece of steel core loaded with a home-made coil at one end and a straight piece of coil spring at the other end to facilitate delivery of the coil; (5) The whole assembly is introduced into the catheter. The central steel core and the straight piece of coil spring are then pulled out leaving the coil in the catheter. This is advanced to the catheter tip by pushing it with the hard end of a conventional guidewire. It is released into the target area by pushing it out of the catheter by the soft tip of the guidewire.
and 3). No complication relating to the procedure was observed. All the patients made an uneventful recovery. One patient, who had massive haematuria caused by an inoperable hypernephroma, developed features of post- embolization syndrome, which lasted for 72 h. The other patients did not exhibit any feature of ischaemia in the territory of the embolized artery.
DISCUSSION
The use of stainless steel coils for transcatheter emboli- zation was first described by Gianturco et al. in 1975 [9]. Since then, these coils have been used in the treatment of various clinical conditions with excellent technical success and low complication rates [1-11]. The advantages of coil embolization are well documented [10]. Coil placement is not only quick but also more precise than many other embolic agents. This enables immediate control of active bleeding sites. Various refinements in the steel coils and their delivery systems have been designed in order to expand the indications for their usage and to increase the incidence of technical success [8,10].
Even though their ability to occlude safely and effec- tively a bleeding artery is well established, steel coils of a desired specification are not easily available and are expensive in India. The unavailability of a coil of a particular size or length in an emergency can be an important limiting factor. Coils are easy to make, taking only a few minutes, and can be fabricated in any desired diameter or length. In addition, they are inexpensive and effective in obliterating antegrade flow. Self-designed coils were used successfully in all patients in this study, and resulted in complete occlusion of all bleeding vessels, without complication.
Even though transcatheter coil embolization is a relatively safe procedure, dislodgement of the coil with proximal or distal displacement to undesirable sites can occur [10]. Prevention of complications can be accom- plished by strict adherence to the recommendations for the use of coils [10]. Meticulous catheter technique will minimize complications. The catheter must be properly and securely placed well into the vessel to be occluded. We routinely test the stability of the catheter tip before releasing the coil. The helical diameter of the coil should match the diameter of the vessel to be occluded. If the coil is too large, it will elongate and perhaps protrude from the vessel origin. A coil of smaller diameter than the vessel may go distally with the blood flow or float precariously.
254 CLINICAL RADIOLOGY
(a)
(b)
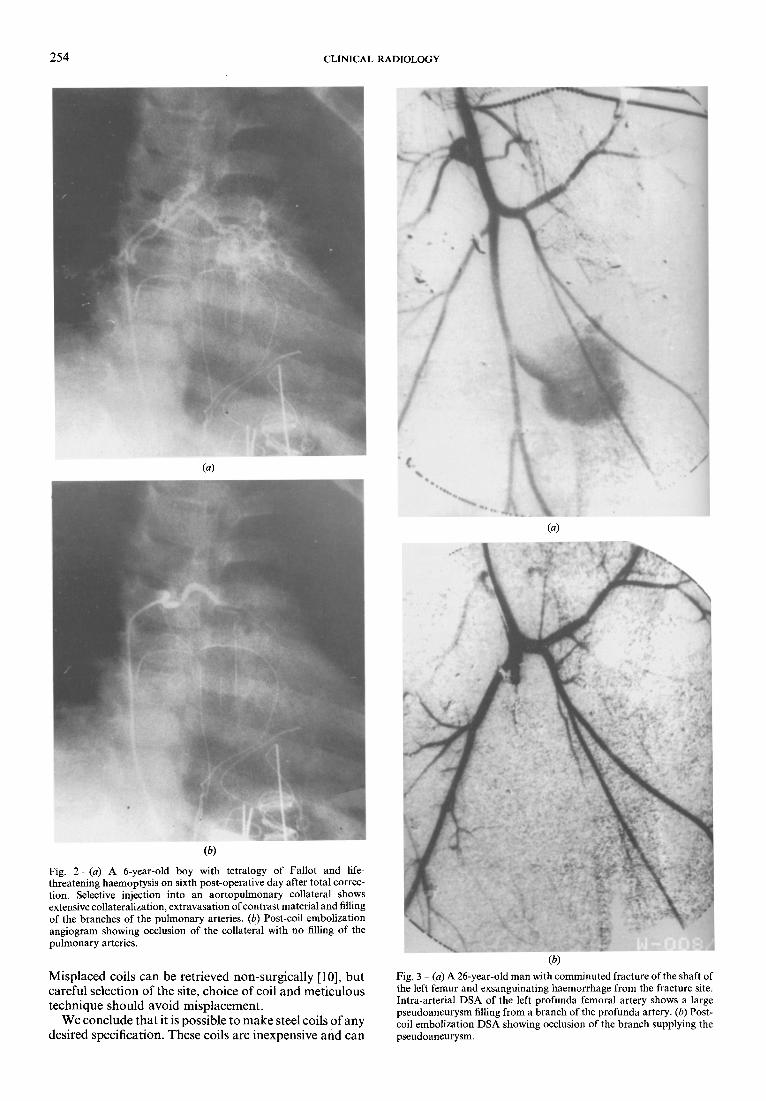
Fig. 2 - (a) A 6-year-old boy with tetralogy of Fallot and life- threatening haemoptysis on sixth post-operative day after total correc- tion. Selective injection into an aortopulmonary collateral shows extensive collateralization, extravasation of contrast material and filling of the branches of the pulmonary arteries. (b) Post-coil embolization angiogram showing occlusion of the collateral with no filling of the pulmonary arteries.
Misplaced coils can be retrieved non-surgically [10], but careful selection of the site, choice of coil and meticulous technique should avoid misplacement.
We conclude that it is possible to make steel coils of any desired specification. These coils are inexpensive and can
(a)
(b)
Fig. 3 (a) A 26-year-old man with comminuted fracture of the shaft of the left femur and exsanguinating haemorrhage from the fracture site. Intra-arterial DSA of the left profunda femoral artery shows a large pseudoaneurysm filling from a branch of the profunda artery. (b) Post- coil embolization DSA showing occlusion of the branch supplying the pseudoaneurysm.

TRANSCATHETER EMBOLIZATION BY HOME-MADE COILS 255
b e e x t r e m e l y use fu l in t he e m e r g e n c y m a n a g e m e n t o f life- t h r e a t e n i n g a r t e r i a l h a e m o r r h a g e in p laces a n d a t t i m e s w h e n c o m m e r c i a l co i l s a r e n o t a v a i l a b l e .
Acknowledgements. We are grateful to Dr Sunil Jain, Associate Professor, Department of Radiology, SGPGI, Lucknow, for his help in the fabrication of these coils, and to Dr Sairtri Shrivastava, for her help in the treatment of one of these patients.
REFERENCES
I Stoll JF, Bettmann A. Bronchial artery embolization to control haemoptysis: a review. Cardiovascular and lnterventional Radiology 1988; 11:263-269.
2 Widlus DM, Murray RR, White RI et al. Congenital arteriovenous malformations: tailored embolotherapy. Radiology 1988;169:51l 516.
3 Palmaz JC, Newton TH, Reuter SR, Bookstein JJ. Particulate intraarterial embolization in pelvic arteriovenous malformations. American Journal of Roentgenology 1981;137:117 122.
4 Hemingway AP, Allison DJ. Complications ofembolization: analy- sis of 410 patients. Radiology 1988;166:669-672.
5 Allison DJ. In: Grainger RG & Allison DJ, eds. Diagnostic radiology. Edinburgh: Churchill Livingstone, 1986:2146 2158.
6 Berenstein A, Kricheff II. Catheter and material selection for transarterial embolization: technical considerations. I. Radiology 1979;132:619 630.
7. Berenstein A, Kricheff II. Catheter and material selection for transarterial embolization: technical considerations. II. Radiology 1979; 132:631-639.
8. Olliff S, Thomas S, Karani J, Waiters H. Superselective emboliza- tion using a coaxial catheter technique. British Journal of Radiology 1990;63:197~01.
9 Gianturco C, Anderson JH, Wallace S. Mechanical device for arterial occlusion. American Journal of Roentgenology 1975; 124:428-435.
10 Chuang VP, Wallace S, Gianturco C, Sos CS. Complications of coil embolization: prevention and management. American Journal of Roentgenology 1981;137:809-813.
11 Szarnicki R, Krebber H J, Wack J. Wire coil embolization of systemic-pulmonary artery collaterals following surgical correction of pulmonary atresia. Journal of Thoracic and Cardiovascular Surgery 1981;81:124-126.





























