Embed Size (px)
Citation preview
LIFE SCIENCES REGULATORY & COMPLIANCE
CODING FOR SUCCESS: ARE YOU MAKING THE MOST OF ICD CLASSIFICATION?
INTRODUCTION
Recent trends in the life sciences industry have seen a shift towards more patient-
centric business models and a drive towards personalised medicine. Life sciences
companies strive for innovative ways to better identify and segment their patient
populations, as well as further advance the understanding of diseases, including disease
progression and management, in order to continue to develop novel therapeutics and
ensure that patients receive the most effective treatments.
In this context, real-world evidence and big data combined with comprehensive data
analytics are vital sources of information to help achieve the overall goal of better
patient outcomes.
THE ICD CLASSIFICATION SYSTEM
The International Classification of Diseases (ICD) classification system, created by the
World Health Organisation (WHO), is an international standard for reporting diseases
and health conditions. The ICD classification system comprises of an index of diseases
categorised by specific codes and has a variety of uses, including:
• identification of global health trends and statistics
• monitoring the incidence and prevalence of disease
• comparison of data across different time periods in the same location
• reimbursement
• used for research purposes to aid in defining diseases
According to the WHO, over 100 countries use the ICD classification system to record
mortality data, with a similar number also using it to record morbidity data, as around
70% of global health expenditures are allocated using the ICD system in reimbursement
and resource allocation procedures1.
1. World Health Organization - Classification of Diseases (ICD) http://www.who.int/classifications/icd/en/

32
HOW LIFE SCIENCES COMPANIES CAN GAIN FROM THE ICD CLASSIFICATION SYSTEM
The ICD classification system is a powerful real-world evidence
tool that, when maximised to its full potential, offers a multitude
of benefits for pharmaceutical and medical device companies,
which include but are not limited to:
• stratifying patient populations for more refined and accurate
recruitment for clinical trials
• ensuring that the right patient gets access to the right
treatment (personalised medicine) through improved and
more precise reporting of their disease state
• enhanced accuracy with reimbursement and pricing
strategies
• better identification and understanding of target patient
populations (e.g. epidemiology), especially in the case of rare
and orphan disease indications
VERSIONS AND MODIFICATIONS OF THE ICD CLASSIFICATION SYSTEM
The version of the ICD system currently in use is the ICD-
10, which came into effect in the early 1990s2. The US has
only recently begun to use ICD-10 as of October 2016 after
a delay of three years3. The next version, ICD-11, is currently
in development with an expected launch date of 2018. It
will incorporate a different coding structure and has been
designed to better support electronic health records and
be more compatible with SNOMED CT, a comprehensive
and standardised multilingual database of medical terms4.
Nonetheless, it is expected that ICD-10 will remain predominant
for the upcoming years, with the earliest use of ICD-11 in country
healthcare systems anticipated to be 20235.
The WHO version of ICD-10 has been translated into over 40
languages and has been modified by certain countries so that
its use for morbidity data can be specifically tailored to fit
with their own healthcare and reimbursement systems. The
main country level modifications can be seen in the figure
below. The key difference between the WHO version and the
different country level modifications are the number of codes
available for use in the classification system. For example, the
ICD-10 WHO version has around 16,000 codes compared to
around 70,000 codes for the ICD-10 CM. Interestingly, country
level modifications are not restricted to the country that has
created them as other countries are freely able to choose which
version/modification of ICD-10 that they want to adopt into
their system. For example, the UK currently uses the ICD-10
WHO version, whereas the Republic of Ireland uses the ICD-10
AM (Australian Modification) and Spain uses the ICD-10 CM
(Clinical/US Modification).
THE ICD REVISION PROCESS
For companies to truly take advantage of the benefits of the ICD system, the relevant
codes need to be present in the classification system. This raises the question: what if
the code required doesn’t exist or is not coded to the degree of specificity needed?
To enable the ICD system to stay relevant and accurately capture advancements in
our understanding of diseases and diagnoses, regular revisions are made to both the
WHO version and the country level modifications. Any individual or organisation is
allowed to submit a proposal for a revision to the ICD WHO version or to the country
level modification, with the exception to the rule being the ICD-10 GM, where only
medical/scientific societies and associations are able to request that a change be made.
This therefore provides companies within the life sciences industry the opportunity
to request for revisions to be made to the ICD-10 classification system. Revisions can
include changes to existing codes and their descriptions and the addition of new codes.
Table 1. List of qualifying reasons for requesting a revision to ICD-10 WHO
1. Need to identify a new disease
2. Need to reflect a change in clinical knowledge
3. Need to reflect a change in clinical terminology
4. Need for compatibility with the WHO Family of Classifications
5. Need for change in rules, guidelines or conventions
6. Need to improve clarity or reduce ambiguity in the tabular list
7. Need to create, delete or correct an index entry
8. Need for greater or less specificity
9. Need to correct typographical errors
Country level modifications add a layer of complexity to the revision process but
also additional strategic opportunities for life sciences companies. As country level
modifications are all derived from ICD-10 WHO, the governing bodies of the country
level modifications usually inclusively incorporate revisions that are implemented at
the WHO level. Revisions can also be made directly at the country level and these are
not immediately implemented back up to the WHO level or into the other country level
modifications unless separate applications are made to each of the other country level
modifications. When deciding which route to choose when submitting a proposal for a
revision, factors that need to be taken into consideration are:
• The specific revision process for the different versions of ICD-10 and their overall
timings, as the timelines from proposal submission to approval and implementation
vary (e.g. ICD-10 CM and GM take an average of one year, whereas ICD-10 WHO
takes between 2 – 5 years)
• The likelihood of the proposed revision being approved
• The market(s) being targeted for the revision or that would benefit most from the
revision
• The key stakeholders involved in the revision process
• The type of revision being requested
ICD-10 WHO VERSION
ICD-10AMAustralian
Modification
ICD-10FRFrench
Modification
ICD-10GMGerman
Modification
ICD-10CACanadian
Modification
ICD-10CMClinical
Modification
Country level modifications
New edition published annually
New edition published biannually
New edition published annually
New edition published annually
New edition published annually
New edition published every 3 years
Figure 1 - Schematic of the current country level modifications of ICD-10
2. World Health Organization - Classification of Diseases (ICD) http://www.who.int/classifications/icd/en/
3. Health Data Management (2016) http://www.healthdatamanagement.com/news/thousands-of-new-icd-10-codes-slated-for-october-release
4. Australian Institute of Health and Welfare. ‘ICD-11 A new way to build the ICD’ (www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=10737419475)
5. ICD10 monitor (2015) ‘ICD-11: A Code Set for the Future’ http://www.icd10monitor.com/enews/item/1399-icd-11-a-code-set-for-the-future

4 5
CASE STUDY 1
Revision to ICD-10 CM proposed by a life sciences company
In 2014, Forest Laboratories LLC, now part of Allergan submitted two proposals requesting that additional codes be added to
the ICD-10 CM. The first proposal put forward was for the addition of the following codes K58.1 - Irritable bowel syndrome with constipation and K58.8 – Other irritable bowel syndrome to be added to irritable bowel syndrome (K58) category. The second
proposal was for the addition of the code K59.04 – Chronic idiopathic constipation to the constipation (K59.0) category.
Forest made the request stating that IBS can be classified into three main subtypes: IBS with constipation (IBS-C), IBS with
diarrhea (IBS-D), a mixture of both constipation and diarrhea (IBS-M) or neither (IBS-U) and that the current ICD-10 coding for
irritable bowel syndrome did not reflect this. As treatment varies for the different patient subtypes, Forest wanted the new codes
implemented for more accurate disease identification for patients. They put forward the same argument for chronic idiopathic
constipation of wanting a more specific code for increased accuracy in disease identification.
At the time the proposal was submitted, Forest had recently received FDA approval in 2012 for their therapeutic Linzess
(linaclotide) to treat patients with irritable bowel syndrome with constipation and chronic idiopathic constipation.
Forest’s proposals were accepted into the next edition of the ICD-10 CM, with a key factor for the approval of their proposals being
the support and backing of their proposal by the American Gastroenterological Association. The addition of a code for mixed IBS
was also added despite not being included in Forest’s original proposal because the revision committee felt that if changes were to
be made to the current coding then this should also be included. At this point in time, these revisions are present only in the ICD-10
CM version6.
ORIGINAL CODES REVISED CODES
CODE CODE DESCRIPTION CODE CODE DESCRIPTION
K58 Irritable bowel syndrome K58 Irritable bowel syndrome
K58.0 Irritable bowel syndrome with diarrhea K58.0 Irritable bowel syndrome with diarrhea
K58.9 Irritable bowel syndrome without diarrhea K58.1 Irritable bowel syndrome with constipation
K59.0 Constipation K58.2 Mixed irritable bowel syndrome
K59.00 Constipation, unspecified K58.8 Other irritable bowel syndrome
K59.01 Slow transit constipation K58.9 Irritable bowel syndrome without diarrhea
K59.02 Outlet dysfunction constipation K59.0 Constipation
K59.09 Other constipation K59.00 Constipation, unspecified
K59.01 Slow transit constipation
K59.02 Outlet dysfunction constipation
K59.03 Drug induced constipation
K59.04 Chronic idiopathic constipation
K59.09 Other constipation
6. http://www.cdc.gov/nchs/data/icd/topic_packet_09_23_2012.pdf
Although submissions are made publicly available for most
versions/modifications, the ICD-10 CM provides the clearest
information on proposals submitted that are reviewed by their
revision committee. At the moment, medical societies make
up the majority of submissions for revisions to changes to the
ICD-10 CM, with less than 10% of submissions in the last 5 years
coming from life sciences companies. Of the submissions made
by life sciences companies, currently there is an approval rate
of just over half. The backing of medical societies appears to be
instrumental in the success of submissions made by life sciences
companies with lack of support being a reason frequently
cited for why their requests were denied. In addition, medical
associations can submit revision proposals directly or indirectly
on the behalf of a life sciences company.
CASE STUDY 2
Example of revision to the ICD-10 CM proposed by medical societies
In September 2012, the American Academy of Ophthalmology (AAO) and the American Society of Retina Specialists (ASRS)
requested that modifications be made to the existing ICD-10 CM codes H35.31 and H35.32 and that new codes be added to better
distinguish the different stages of both wet and dry AMD and the laterality of the disease in the eye. Furthermore, they requested
changes to be made to the codes related to diabetes mellitus with proliferative diabetic retinopathy (E08-E11, E13) to include the
severity levels and laterality of the disease, to enable better tracking of the disease. They also requested changes be made to the
coding for diabetic macular oedema (DME) to reflect the laterality. Finally, they proposed changes to the codes for retinal vein
occlusion (RVO) (H34.8) to also code for the severity of the disease. The purpose of these modifications was to reflect the change
in current standard of care from laser or incisional surgery to treatment with anti-VEGF drugs, such as EYLEA (aflibercept) and
Lucentis (ranibizumab).
Although there is no direct connection between the proposal of these changes to ICD-10 CM by the AAO and the AARS to
Regeneron/Bayer or Genentech/Roche, all the additions and revisions proposed were accepted into the latest version of the ICD-
10-CM and have direct impacts on the reimbursement for EYLEA and Lucentis, both drugs that are approved for all the indications
in which revisions to the coding where suggested. This is because with the new codes reimbursement can now be made for each
individual eye that is treated with anti-VEGF therapy.
This highlights the indirect benefit that life sciences companies can gain when ICD-10 revisions are made to reflect advancements
in the diagnosis and treatment of diseases. It is likely that had Regeneron/Bayer and/or Genentech/Roche submitted the
proposal themselves with the backing of the medical societies then they would have still been successful in having the revisions
implemented. Similarly to the previous case study, the revisions are only present in the ICD-10 CM7.
Medical Societies
Gov
ernm
ent
Other
Pharma/Med
Dev
Revision Approved
Revision Rejected
Figure 2. Submission rate for proposals to revise ICD-10 CM and the success rate for life sciences companies
When deciding to submit a proposal to revise a version/modification of the ICD classification system, it is crucial that all key
stakeholders are aware of the situation and are actively involved and engaged from the early stages. The key stakeholders will vary
depending on the strategy chosen and can include not only medical/scientific associations, but also clinical coders, physicians and
nurses, insurance and reimbursement bodies and government officials.
7. http://www.cdc.gov/nchs/data/icd/topic_packet_for_september_19_2012.pdf
76
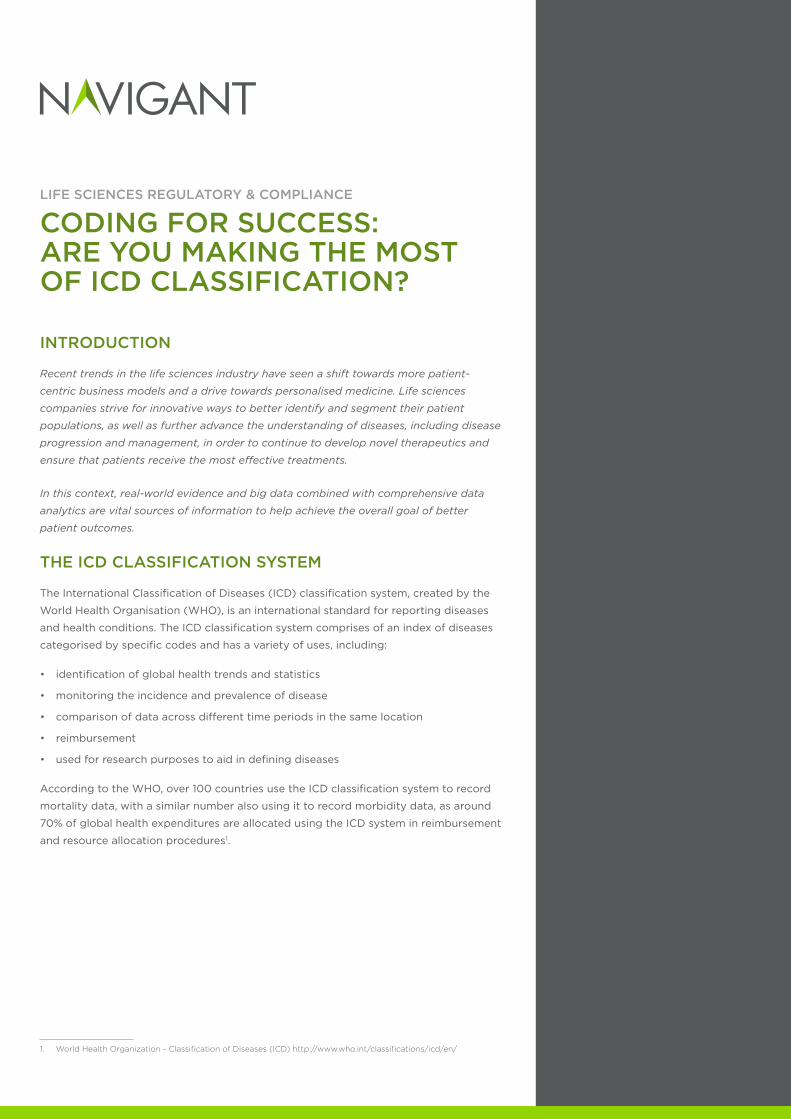
CASE STUDY 4
Example of Revision to the ICD-10 WHO
In 2007, a proposal was submitted to revise the ICD-10 classification system for chronic renal failure (N18) by the Australian ICD-10
committee in order that the ICD-10 WHO version was aligned to the revisions that had already been made to the ICD-10 AM version.
The revisions included modifying the title of the category from chronic renal failure to chronic kidney disease and to add new codes
to reflect the different stages of chronic kidney disease. The argument presented for the revision was that the ICD-10 codes needed
to reflect the current clinically used classification of chronic kidney disease which is frequently used in treatment recommendations.
The proposal was accepted by the WHO and implemented into the 2010 version of the ICD-10 WHO version. These revisions were
subsequently implemented into the country level modifications also9.
ORIGINAL CODES REVISED CODES
CODE CODE DESCRIPTION CODE CODE DESCRIPTION
N18 Chronic Renal Failure N18 Chronic kidney disease
N18.0 End-stage renal disease N18.1 Chronic kidney disease, stage 1
N18.8 Other chronic renal failure N18.2 Chronic kidney disease, stage 2
N18.9 Chronic renal failure, unspecified N18.3 Chronic kidney disease, stage 3
N18.4 Chronic kidney disease, stage 4
N18.5 Chronic kidney disease, stage 5
N18.9 Chronic kidney disease, unspecified
As highlighted in the case study examples, revisions to the ICD-10 classification system that would have a significant impact on
reimbursement have a greater chance of being implemented at the country level modifications compared to the WHO level. This is
because as country level modifications were introduced to ensure more accurate reimbursement, it is possible to present this argument
when submitting a proposal to them; however, this would not be a valid argument for a revision to be made at the WHO level.
CASE STUDY 3
Example of Revision to the ICD-10 GM
In 2006, a proposal was submitted by a member of the Association of Private Health Insurance (Verband der privaten
Krankenversicherung e.V.) to the ICD-10 GM requesting the introduction of additional codes for the different severity levels of
Parkinson’s disease based on the Hoehn and Yahr Scale, as at the time there was only one code specifically for Parkinson’s disease
(G20). The proposal also requested that an additional fifth digit also be added to code for the presence of response fluctuations.
The additions were requested for reimbursement purposes and to aide with accurate resource allocation in the German DRG system
as treatment varies depending on the stage of Parkinson’s that a patient is in. This revision is only present in the ICD-10 GM8.
CODE CODE DESCRIPTION
G20.0[0,1] Parkinson Disease with no to mild disability (Stages 0 to under 3 of the Hoehn and Yahr scale) [without response fluctuations; with response fluctuations]
G20.1[0,1] Parkinson Disease with moderate to severe disability (Stages 3 or 4 of the Hoehn and Yahr scale) [without response fluctuations; with response fluctuations]
G20.2[0,1] Parkinson Disease with severe disability (Stage 5 of the Hoehn and Yahr scale) [without response fluctuations; with response fluctuations]
G20.9[0,1] Parkinson’s Disease, unspecified [without response fluctuations; with response fluctuations]
8. http://www.dimdi.de
9. WHO ICD-10 Revision Platform
CONCLUSION
The benefits of the ICD classification system as a real-world evidence tool for improving
patient outcomes and reimbursement is evident. Pharmaceutical companies seeking to
take advantage of this classification tool will need to understand how to capitalise on it
(including deciding what revisions should be proposed and which versions or country
modifications to target for these proposals), as well as how to access and effectively
analyse the data.
In developing their approach, companies should seek advice from an experienced
expert with a comprehensive understanding of ICD (including both ICD-10, the country
level modifications for ICD-10 and ICD-11) who is well versed in the technical aspects of
the ICD system, the regulatory processes involved with requesting the implementation
of the revision/addition of new codes, potential commercial strategy opportunities, and
global ICD-10 data analysis and interpretation.
Important Notice
The views expressed in this article are those of the authors and do not necessarily
represent the views of Navigant Consulting Inc. or any of our clients.

twitter.com/navigant
linkedin.com/company/navigant
©2017 Navigant Consulting, Inc. All rights reserved. 00006418A
Navigant Consulting, Inc. (“Navigant”) is not a certified public accounting or audit firm. Navigant does not provide audit, attest, or public accounting services. See navigant.com/about/legal for a complete listing of private investigator licenses.
This publication is provided by Navigant for informational purposes only and does not constitute consulting services or tax or legal advice. This publication may be used only as expressly permitted by license from Navigant and may not otherwise be reproduced, recorded, photocopied, distributed, displayed, modified, extracted, accessed, or used without the express written permission of Navigant.
CONTACTS
CHRIS J. HOLMESDirector+44 (0)20 7015 [email protected]
ALEXANDROS CHARITOUAssociate Director+44 (0)20 7015 [email protected]
DEMI DABOR-ALLOHConsultant+44 (0)20 7015 [email protected]
navigant.com
About Navigant
Navigant Consulting, Inc. (NYSE: NCI) is a specialized, global professional services
firm that helps clients take control of their future. Navigant’s professionals apply deep
industry knowledge, substantive technical expertise, and an enterprising approach
to help clients build, manage, and/or protect their business interests. With a focus
on markets and clients facing transformational change and significant regulatory
or legal pressures, the firm primarily serves clients in the healthcare, energy, and
financial services industries. Across a range of advisory, consulting, outsourcing, and
technology/analytics services, Navigant’s practitioners bring sharp insight that pinpoints
opportunities and delivers powerful results. More information about Navigant can be
found at navigant.com.