Embed Size (px)
Citation preview
Life course perspectiveson coronary heart disease,
stroke and diabetes
WHO/NMH/NPH/02.1ORIGINAL: ENGLISH
DISTR.: GENERAL
Ageing and Life CourseDepartment of Noncommunicable Diseases Prevention and Health Promotion
Noncommunicable Diseases and Mental Health Cluster
WORLD HEALTH ORGANIZATION
The evidence and implicationsfor policy and research
AC
CU
MU
LATE
D N
CD
RIS
K
AGE
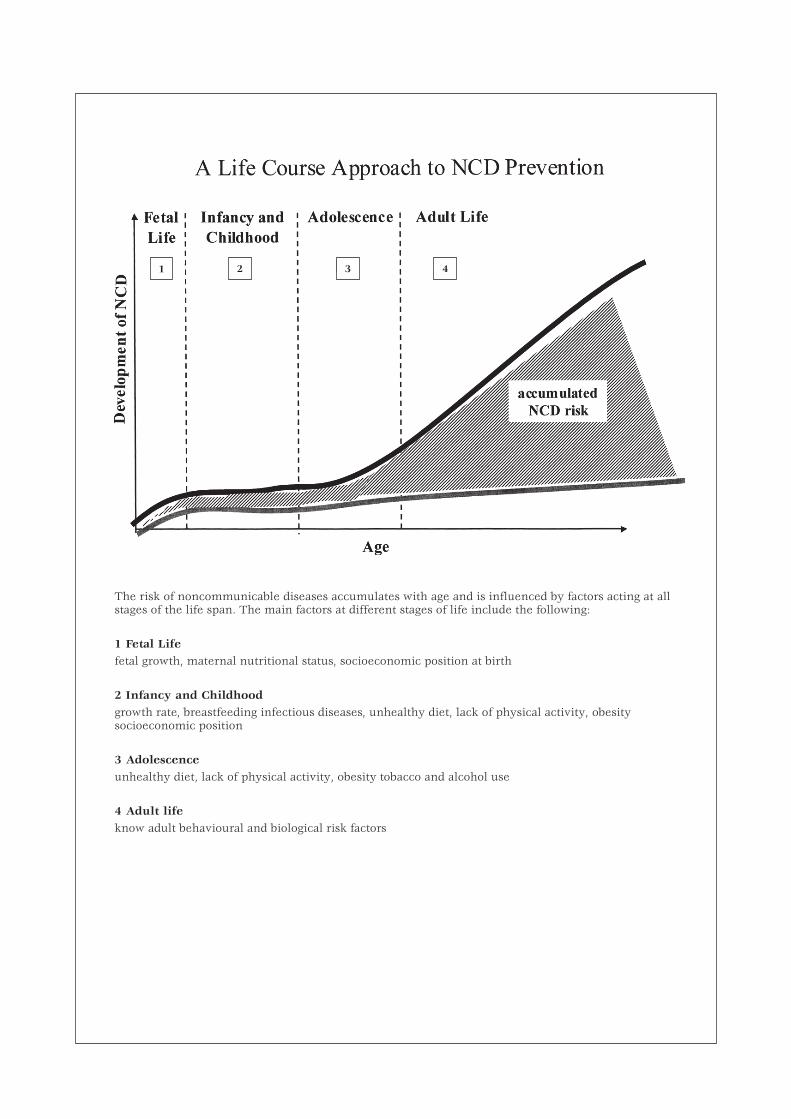
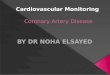
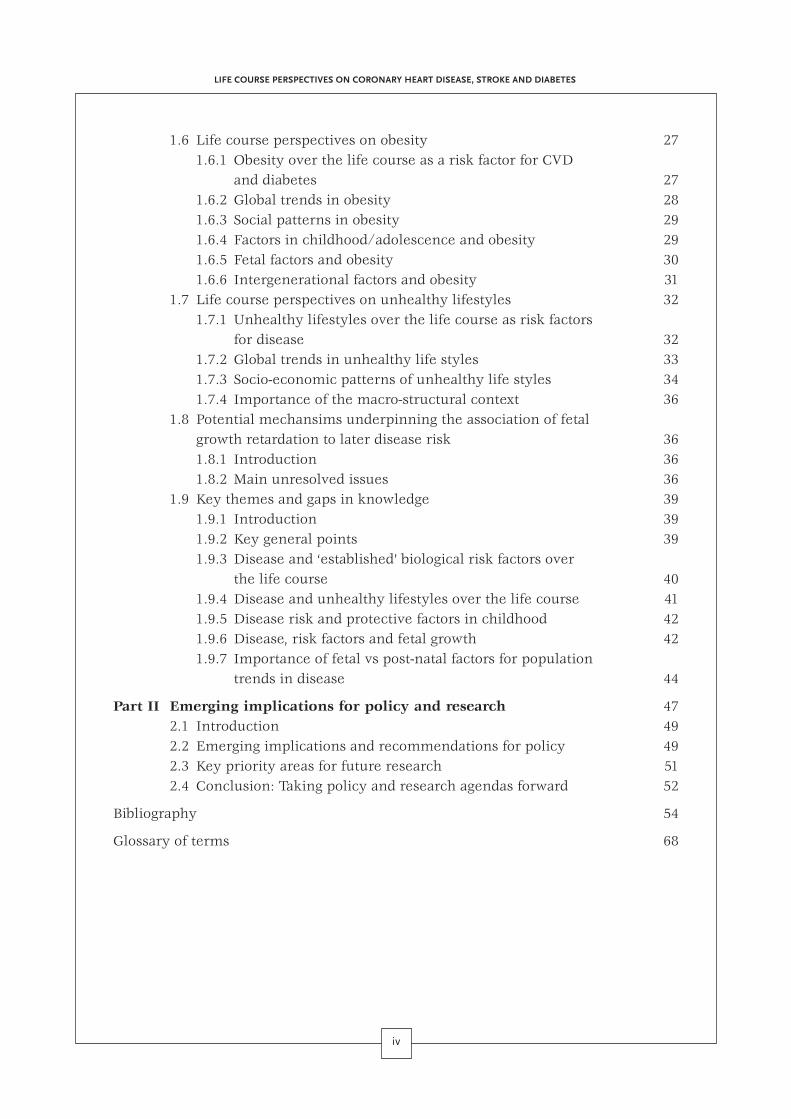
The risk of noncommunicable diseases accumulates with age and is influenced by factors acting at allstages of the life span. The main factors at different stages of life include the following:
1 Fetal Lifefetal growth, maternal nutritional status, socioeconomic position at birth
2 Infancy and Childhoodgrowth rate, breastfeeding infectious diseases, unhealthy diet, lack of physical activity, obesitysocioeconomic position
3 Adolescenceunhealthy diet, lack of physical activity, obesity tobacco and alcohol use
4 Adult lifeknow adult behavioural and biological risk factors
31 2 4
Life course perspectiveson coronary heart disease,
stroke and diabetesThe evidence and implications
for policy and research
WHO/NMH/NPH/02.1 • ORIGINAL: ENGLISH • DISTR.: GENERAL
Ageing and Life CourseDepartment of Noncommunicable Diseases Prevention and Health Promotion
Noncommunicable Diseases and Mental Health Cluster
WORLD HEALTH ORGANIZATIONGeneva
Acknowledgements
The World Health Organization wishes to acknowledge the support from the Government of Japanfor the organization of the first meeting of experts on life course and health and the finalization ofthis report.
Copies can be obtained from:
Ageing and Life CourseDept. of Noncommunicable Diseases Prevention and Health PromotionNoncommunicable Diseases and Mental Health ClusterNMH/NPH/ALC20 Avenue Appia1121 Geneva 27SwitzerlandFax: +41 (22) 7914839e-mail: [email protected]
Suggested Citation:
Aboderin, I., Kalache, A., Ben-Shlomo, Y., Lynch, J.W., Yajnik, C.S., Kuh, D., Yach, D. (2002) LifeCourse Perspectives on Coronary Heart Disease, Stroke and Diabetes: Key Issues and Implications forPolicy and Research. Geneva, World Health Organization
© World Health Organization 2002
This document is not a formal publication of the World HealthOrganization (WHO), and all rights are reserved by the Organization.The document may, however, be freely reviewed, abstracted,reproduced or translated, in part or in whole, but not for sale nor foruse in conjunction with commercial purposes.
The views expressed in documents by named authors are solely theresponsibility of those authors.
Designed by minimum graphicsPrinted in Switzerland
Contents
iii
Executive Summary 1
Introduction: The life course perspective and NCD prevention:potential and challenge 2
Part I Life course impacts on risk of CHD, stroke and diabetes:the state of the art evidence 5
1.1 Introduction 71.2 Established life course factors associated to CHD, stroke,
and diabetes 71.2.1 Established adult risk factors 71.2.2 Factors in fetal life 81.2.3 Factors in infancy and childhood 91.2.4 Interactions between early and later factors 101.2.5 Developing a deeper understanding of the associations
of life course factors to adult disease 111.3 Life course perspectives on blood pressure 12
1.3.1 Blood pressure over the life course as a risk factor for CVD 121.3.2 Global trends in blood pressure 131.3.3 Social patterns of blood pressure 131.3.4 Factors in childhood/adolescence and blood pressure 141.3.5 Fetal factors and blood pressure 151.3.6 Intergenerational factors and blood pressure 17
1.4 Life course perspectives on dyslipidaemias and impairedglucose tolerance (IGT) 171.4.1 Dyslipidaemia and IGT over the life course as risk factors
for CVD and diabetes 171.4.2 Global trends in dyslipidaemias and IGT 181.4.3 Social patterns in dyslipidaemas and IGT 181.4.4 Factors in childhood/adolescence and dyslipidaemias and IGT 191.4.5 Fetal factors and dyslipidaemias and IGT 201.4.6 Intergenerational factors and IGT 23
1.5 Life course perspectives on height 231.5.1 Short stature as a risk factor for disease 231.5.2 Secular trends in height 241.5.3 Height as a marker of early life factors 241.5.4 Possible factors mediating the association of short stature
to disease 25
1.6 Life course perspectives on obesity 271.6.1 Obesity over the life course as a risk factor for CVD
and diabetes 271.6.2 Global trends in obesity 281.6.3 Social patterns in obesity 291.6.4 Factors in childhood/adolescence and obesity 291.6.5 Fetal factors and obesity 301.6.6 Intergenerational factors and obesity 31
1.7 Life course perspectives on unhealthy lifestyles 321.7.1 Unhealthy lifestyles over the life course as risk factors
for disease 321.7.2 Global trends in unhealthy life styles 331.7.3 Socio-economic patterns of unhealthy life styles 341.7.4 Importance of the macro-structural context 36
1.8 Potential mechansims underpinning the association of fetalgrowth retardation to later disease risk 361.8.1 Introduction 361.8.2 Main unresolved issues 36
1.9 Key themes and gaps in knowledge 391.9.1 Introduction 391.9.2 Key general points 391.9.3 Disease and ‘established’ biological risk factors over
the life course 401.9.4 Disease and unhealthy lifestyles over the life course 411.9.5 Disease risk and protective factors in childhood 421.9.6 Disease, risk factors and fetal growth 421.9.7 Importance of fetal vs post-natal factors for population
trends in disease 44
Part II Emerging implications for policy and research 472.1 Introduction 492.2 Emerging implications and recommendations for policy 492.3 Key priority areas for future research 512.4 Conclusion: Taking policy and research agendas forward 52
Bibliography 54
Glossary of terms 68
iv
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES

1
Executive Summary
The Life Course and Health Perspective con-siders chronic disease in terms of the
social and physical hazards, and the consequentbiological, behavioural and psychosocial proc-esses, that operate across all stages of the lifespan to cause or modify risk of disease.
This perspective carries a substantial poten-tial for identifying the most appropriate and ef-fective policies for NCD prevention and healthpromotion—a potential that is yet to be fullyrealized in public health policy.
Through the preparation for, and the conductof a meeting of experts on life course and health(2–4 May, 2001), the WHO Department ofNoncommunicable Diseases Prevention andHealth Promotion (NPH) made a first step to-wards harnessing the potential of the life courseapproach for policy.
The meeting has established the state of theart knowledge regarding life course impacts onrisk of coronary heart disease, stroke and dia-betes and, on the basis of this, has identifiedemerging agendas for policy and research. Thelimited initial focus on three diseases wasdeemed necessary for the task to remain man-ageable. However, it provides a starting pointupon which future assessments of life courseand other NCDs can build.
The emerging policy recommendations fol-low a hierarchy according to the firmness ofavailable evidence. The strongest recommenda-tion, currently, is to continue the focus on the
major known risk factors. In doing so particu-lar attention should be paid to primordial/pri-mary prevention strategies to counter theemergence of risk factors and behaviours inchildhood or adolescence, particularly in devel-oping countries. Most importantly, such strate-gies must take into account the varied processesby which urbanisation and ‘westernisation’ canlead to risk behaviours and factors in differentsocio-economic contexts and populations. It isimportant to recognize the cultural, economicand social circumstances within which suchbehaviours and risks emerge, and that these maybe specific to different countries in differentstages of economic development. Thus, researchto inform the development of such preventivestrategies in individual countries is urgentlyneeded.
Despite the high profile of evidence linkingearly life factors such as reduced fetal growthto later disease, evidence is still insufficient forfirm policy recommendations to be made. Fur-ther research is urgently needed to establish therelative role and importance of early life expo-sures, and the mechanisms by which they af-fect future risk of disease. Key priority areas forresearch have been identified.
NPH is taking forward the policy and researchagendas emerging in light of current evidenceon life course, through collaborative work andconsultation across departments within WHO,and with outside institutions.
2
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
The WHO initiative on life course and health,the scientific foundation for which was
consolidated in a meeting of experts on lifecourse, 2–4 May 2001, is situated within andis a central aspect of the work of the Depart-ment of Noncommu-nicable Disease (NCD)Prevention and Health Promotion (NPH). Thedepartment’s overall goal is to prevent noncom-municable diseases and thus to reduce prema-ture morbidity, mortality and disability causedby them. Particular focus is given to most com-mon NCDs such as cardiovascular diseases(CVD) and diabetes, as they cause much humansuffering, pose substantial threats to the econo-mies of individual countries, and are importantin the increasing health inequalities betweencountries and within popu-lations worldwide.
Global trends in CVDand diabetes
Although already high, the bur-den of CVD and diabetes is ex-pected to rise further in thecoming decades—above all indeveloping countries, i.e. thosecountries with the least re-sources to effectively deal withthem (see e.g. Murray andLopez, 1996):
• In developed countries,cardiovascular diseases areand will remain the first cause of death anddisability, despite the gradual decline indisease rates experienced in most of themin the last few decades. In 2000, 48.6% ofdeaths were caused by CVD. By 2020, still46.4% of all deaths are expected to be at-tributable to CVD. Meanwhile, the numberof those suffering from diabetes will haverisen from 51 million in 1995 to 72 millionin 2025.
• In the developing world, CVD will soonbecome the main cause of death and dis-ability: by 2020, a third (33.8%) of all deaths
Although alreadyhigh, the burden of CVDand diabetes is expected
to rise further in thecoming decades—above allin developing countries,i.e. those countries with
the least resources toeffectively deal
with them
Introduction: Life course as a central partof WHO’s work on NCD prevention and
health promotion
are expected to be due to CVD. The numberof those with diabetes will increase morethan 2.5 times, from 84 million in 1995 to228 million in 2025.
• It is projected that by 2020 71% of ischae-mic heart disease (IHD) deaths, 75% ofstroke deaths and 70% of diabetes deathswill occur in developing countries.
• The current ‘epidemic’ in adult and child-hood obesity, not just in developed but alsoin many developing countries may indicateeven sharper rises in the burden of CVDand diabetes.
The spectre of rising CVD and diabetesunderscores the imperative need to developeffective and appropriate prevention policies,especially in poor and marginalized populations.
Such policies, as has long beenrecognized, need to address themajor risk factors predisposingto disease (the current focus ison the behavioural risk factorssmoking, physical inactivity andunhealthy diet), and take intoconsideration underlying eco-nomic, social, gender, political,behavioural, and environmentalfactors that foster disease risk.
However, what the most valu-able concrete strategies are indifferent contexts and popula-
tions, whom they should be targeted at, whenand how, remains to be firmly established andwill depend in large part on the cultural, socialand economic conditions.
This represents the core charge of NPH’swork and is the reason why NPH has adoptedthe life course as the underpinning perspectiveof its work. In doing so, WHO recognizes thepotential of the life course perspective to en-able policymakers to identify the most effectiveand appropriate prevention strategies and togain maximum leverage for interventions whereprevention resources may be scarce.

3
processes, that act across all stages of the lifespan—gestation, infancy, childhood, adoles-cence, young adulthood and midlife—to affectrisk of disease later on. It considers, in particu-lar, the existence of both “critical” and “sensi-tive” periods throughout life where exposuresare deterministic or especially powerful in pre-
disposing to, or lessening riskof disease later on. The term“critical period” implies expo-sures that must occur in somespecified window(s) of time andoften involve exposures thatalter normal biological develop-ment. “Sensitive period” expo-sures refer to a broader class ofinfluences that may havegreater impact on later out-comes if they occur in certainperiods than in others. In em-pirical terms, both critical andsensitive period exposures im-ply time by exposure interac-
tions. Better understanding of critical andsensitive period exposures thus offers thepotential for identifying the most appropriateand effective interventions or strategies for dis-ease prevention or health promotion. In addi-tion, a life course perspective on NCDs invokesconcepts of “accumulation” of both correlatedor uncorrelated exposures that over timeadditively increase the risk of adverse outcomes.
The major challenge in harnessing thepotential of the life course perspective for pub-lic health policy is to fully elucidate the path-ways and mechanisms by which, in differentpopulations and at different historical periods,factors or exposures in earlier and later life actto determine subsequent risk of disease. Of par-ticular importance is to identify the relative roleof—and interaction between—earlier and laterfactors, and the critical periods and exposuresthat may shape chronic disease risk later on.
So far, and on the basis of available evidence,several theoretical models have been advancedto explain the possible ways in which factorsover the life course may act to cause chronicdisease (Ben-Shlomo and Kuh, 1999)
1. A critical period model—where an insultduring a specific period of growth or devel-opment has a lasting, life long effect on physi-cal functioning or structure thus resulting indisease later on.
INTRODUCTION. LIFE COURSE AS A CENTRAL PART OF WHO’S WORK ON NCD PREVENTION AND HEALTH PROMOTION
The life course perspective—potential and challenge
The current epidemiological focus on a lifecourse approach to chronic disease emerged inthe 1980s. However, the notion that experiencesin early life shape adult health is not new. Itwas, in fact, a prominent perspective in publichealth in the first half of the cen-tury, but was superseded by the“life style” model of chronic dis-ease which focused almost exclu-sively on adulthood risk factors.This was, largely, a result of thesuccess of cohort studies in con-firming, for example, smoking orhigh cholesterol levels as majorrisk factors for several chronicdiseases.
The current revived emphasison a life course perspective hasarisen against a background ofincreasing evidence, especiallyfrom revitalised historical cohorts, maturingbirth or child-cohort studies, that the risk ofmany NCDs such as CVD or diabetes is not justdetermined by risk factors in mid-adult life, butalready begins in childhood or adolescence—andpotentially even earlier during fetal develop-ment.
Specifically, it has been boosted by promi-nence given to (a) the increasing evidence onthe ‘tracking’ of conventional risk factors fromchildhood to adulthood from large and extendedcohort studies such as the Bogalusa Heart Study(e.g. Bao et al. 1994); (b) the rise of ‘program-ming’ as a model of disease aetiology, inparticular the fetal origins of adult diseasehypothesis (Barker, 2000a); and (c) emergingevidence to indicate that some early risk fac-tors may act across generations thus increasingcardiovascular risk in offspring (Sterne et al.2001; Davey Smith et al.2000a).
Whilst consideration of early life factors orexposures is a main focus of the life course per-spective, it is much broader than that. Its aim isto transcend the dichotomy between traditional‘adult lifestyle’ and ‘early origins’ models of adultdisease, both of which, on their own, are un-able to fully explain individual risk as well asgeographical, social, and temporal variations indisease patterns (Kuh and Ben-Shlomo, 1998).
Thus, the life course perspective considersthe social and physical hazards, and the result-ing behavioural, biological and psychosocial
Thus, the life courseperspective considers the
social and physicalhazards; and the resulting
behavioural, biologicaland psychosocial
processes, that act acrossall stages of the life
span—gestation, infancy,childhood, adolescence,young adulthood and
midlife—to affect risk ofdisease later on.

2. A critical period with later effect modi-fiers—where later factors may modify sucha risk earlier incurred.
3. Accumulation of risk with independentand uncorrelated results—where separateand independent risk factors at each stage oflife combine to raise disease risk.
4. Accumulation of risk with correlatedresults—where risk factors cluster in sociallyor biologically patterned ways, and may raisethe risk of disease through social and/or bio-logical chains (or pathways) of risk. That is,where one adverse (or protective) experiencewill tend to lead to another adverse (or pro-tective) experience in a cumulative way.
Disentangling the ways in which factors ateach stage of life act or interact to shape dis-ease risk is, obviously, complex and difficult.This is added to by the fact that explanationsare not only disease specific, butmay also vary from one cohort,population, or context to an-other. It is crucial to understandthat the effects of early life ex-posures on later disease risk arelikely to be highly contextu-alized in both time and space.For example, being born intopoverty in Bangladesh in 2000is likely to be associated with very different earlylife exposures than being born into poverty inthe USA in the 1950s. The social meaning of pov-erty and its life course links to particular typesof exposures, as well as the prevailing diseaseenvironment will all influence the potential forearly life factors to be expressed in different ad-verse outcomes later in life.
Despite the complexity and difficulty of thechallenge, and despite the fact that work is onlyin its early stages, a critical mass or body of evi-dence, in particular from developed countries,has accumulated over the last decade.
The time is thus now ripe for taking a firststep towards capturing some of the potential ofthe life course perspective for policy—by tak-ing stock of what knowledge has accumulated,by considering what policy implications are al-ready emerging, and by pinpointing the key gapsin knowledge that need to be addressed by fu-ture research.
Structure of the report
The remainder of this report is divided into twoparts:
Part I provides an overview of the state of theart knowledge and evidence regarding lifecourse impacts on risk of CHD, stroke and dia-betes, as established at the meeting of experts,2–4 May 2001. It begins by outlining the asso-ciations between early or later life factors and
CHD, stroke and diabetes thathave been firmly established orare highly suggestive. The sub-sequent sections examine in de-tail the nature and factorsunderpinning these associations.They do this by considering, inturn, each of the key biologicalor lifestyle related domains dis-cussed, whilst pointing out areas
of overlap between them. A final section drawstogether the emerging key themes, issues, andthe main gaps in knowledge regarding the in-fluence of earlier and later life factors on dis-ease risk.
Part II describes the main implications for re-search and policy that emerge from the currentstate of knowledge on life course and later dis-ease. Recommendations for public health policyare made and priority areas for future researchare identified.
Disentangling the waysin which factors at each
stage of life act or interactto shape disease risk is,
obviously, complexand difficult.
4
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
PART I
Life course impacts onrisk of CHD, stroke and diabetes
– the state of the art evidence

1.1 Introduction
This first part of the report provides anoverview of the state of the art evidence on
early and later life course impacts on risk ofCHD, stroke and diabetes—as established by theexperts in the their written comments prior to,and their discussions at the May 2001 meeting.Throughout, the points and issues raised by theexperts are substantiated with key referencesfrom the literature.
Most of the relevant evidence comes eitherfrom historical or retrospective cohort studies,or from ongoing or recently established prospec-tive birth or child cohort studies. A selection ofsome of the former studies, which are mostlyfrom developed countries, include:
• UK—the 1946 and 1950 birth cohorts; theHertfordshire, Sheffield, and Caerphilly co-horts (see Leon and Ben-Shlomo, 1997); theGlasgow University Students cohort(McCarron et al. 1999), and the Boyd Orrcohort (Gunnell et al. 1998a)
• US—the Harvard Alumni Studies(Paffenbarger and Williams, 1967) or JohnsHopkins Precursor Study (e.g. Klag et al.1993)
• Finland—the Helsinki Central HospitalCohort (Eriksson et al. 1999)
• Netherlands—the Dutch Famine Cohort(e.g. Ravelli et al. 2000)
• Russia—the Leningrad Siege Cohort(Stanner et al. 1997)
• Sweden—the Uppsala cohort (e.g. Leon etal. 1996, 1998)
A few such cohorts have, however, also beenstudied in developing countries, for example inMysore, India (Stein et al. 1996; Fall et al. 1998)or Beijing, China (Mi et al. 2000).
Prospective child or adolescent cohort stud-ies, too, are predominantly from developedcountries, e.g
US—the Bogalusa Heart Study (Berenson etal. 1991)
UK—the ALSPAC Study (ALSPAC, 2001)Finland—the Young Finns Study (Åkerblom
et al. 1999).
However, several developing country childcohort studies do exist including,
India—the Pune Birth Cohort (Bavdekar etal. 1999) and the Pune Maternal NutritionStudies (Fall et al. 1999)
South Africa—the Birth to Ten Study (Yachet al. 1991).
A few retrospective child cohort studies, suchas for example in Jamaica (Forrester et al. 1996),the Gambia (Margetts et al. 1991), Zimbabwe(Woelk et al. 1998), or the Democratic Republicof Congo (Longo-Mbenza et al. 1999), have pro-vided further evidence on early life course riskfactors in developing populations.
Additional developing world insights come,moreover, from child health and nutrition sur-veys such as the CEBU Longitudinal Health andNutrition Survey in the Philippines (CLHNS)(Cebu Study Team, 1991) or the INCAP Nutri-tion Supplementation Trial in Guatemala(Martorell, 1995). Whilst these studies did notspecifically set out to investigate life course im-pacts on chronic disease risk, some of their find-ings are, nevertheless, relevant.
The first of the following sections outlinesthose associations between life course factorsand disease that are firmly established or highlysuggestive. Given that these associations havemainly been demonstrated in developed coun-tries it, moreover, considers the extent to whichthey are generalizable to other populations, par-ticularly in the developing world.
The subsequent six sections, which follow thestructure of the discussions at the May 2001meeting, examine the nature and basis of theobserved associations between early or later fac-tors and disease. They do so by exploring indetail the life course determinants and interac-tions of the main known risk domains: HighBlood Pressure, Dyslipidaemias and Im-paired Glucose Tolerance, Obesity, Height,and Unhealthy Lifestyles, and by discussingthe potential mechanisms underpinning theassociation of fetal factors to disease risk.
A final section draws together the mainstrands emerging from the explorations of theindividual domains. It considers the cross-cutting themes and issues, and pinpoints themain gaps in our understanding of how lifecourse factors shape risk of CHD, stroke, anddiabetes.
1.2 Established life course factorsassociated to disease
1.2.1 Factors in adulthood
a. The ‘established’ risk factors
The most firmly established associations be-tween CVD or diabetes and factors in the life
7
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE

8
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
span are those between disease and the majorknown ‘adult’ risk factors—tobacco use, obes-ity, physical inactivity, cholesterol, highblood pressure, and alcohol. (see e.g. Godlee,1999; Elisaf, 2001 for review)
These are the factors confirmed to lead toincreased risk of CHD, stroke, and diabetes.Some of the associations are con-sidered causal and reversible:
• high blood pressure forCHD or stroke (e.g. Mc-Mahon et al. 1990; Kannelet al. 1996)
• high cholesterol (diet) forCHD (e.g.Hu et al. 2000;Hooper et al. 2001; Ander-son et al.1987)
• tobacco use for CHD (e.g.Doll et al. 1994; Lopez, 1999)
Other associations are robustand consistent, though they havenot necessarily been shown to be reversible:
• obesity (physical inactivity) for CHD, dia-betes, stroke (e.g. Jousilahti et al. 1996;Shaper et al.1997; Davey Smith et al. 2000c;Wannamethee et al.1998a)
• heavy and/or binge drinking for CHD andstroke (e.g.Kaukanen et al. 1997; Lopez,1999)
Although most of the evidence establishingthe link of these factors to disease is from de-veloped countries, it is generally believed thatthese associations can be generalized with someconfidence to other populations. Supportingevidence from developing countries is begin-ning to emerge.
This includes the confirmed link in India oftobacco use, history of hypertension, diabetes,and abdominal adiposity to acute myocardialinfarction (AMI) (Pais et al. 1996); the associa-tion of high serum cholesterol levels to CHD inChina (Chen et al. 1991); as well as the clearlyestablished link of tobacco use to overall andCVD specific mortality in large-scale studies inIndia (Gupta and Mehta, 2000) and China (Liuet al. 1998; Niu et al. 1998). Further efforts todetermine the major risk factors specifically forCHD in developing countries are being begunby the WHO Interheart Study (Ounpuu et al.2000).
b. Low socio-economic position
In developed countries, various indicators of lowsocio-economic position (SEP) have clearly beenshown to be associated with a higher risk of car-diovascular disease and diabetes (Davey Smith,1997). Recent evidence from the UK, moreoversuggests that although overall CVD rates are fall-
ing, these inequalities in diseaseare persisting or even increas-ing, (e.g. Harding et al. 1998).However, such rising social in-equality in CVD is not necessar-ily a feature in all developedcountries.
The effect of SEP on risk ofCVD or diabetes in developingcountries is poorly understood,given the paucity of cause-spe-cific mortality and morbiditydata. However, what little evi-dence is available suggests thatthere has been an initial prepon-
derance of CVD among the higher socio-economic groups, but that in some populationshigher risk of CVD is, in fact, associated withlower SEP (e.g. Gupta et al. 1994). The particu-lar nature of the social inequalities in CVD de-pends upon how lower socioeconomic positionwithin a particular country affects the socialdistribution of risk factors for CVD, such assmoking, unhealthy diet and physical inactiv-ity.
It is generally assumed, though not as yetverified, that as the ‘epidemic’ of chronic dis-ease in developing countries advances, the so-cial distribution of adverse risk facors and theburden of disease, as it has done in the West,will progressively shift to the lower socialclasses.
1.2.2 Factors in fetal life
a. Intrauterine growth retardation (IUGR)
In addition to the major adult risk factors, thereis firm evidence, mostly from developed coun-tries, that intrauterine growth retardation(IUGR) is associated with an increased risk ofCHD, stroke, and diabetes.
Evidence from revitalized historical cohortsor retrospective studies shows clear associationsbetween retarded fetal growth (indexed by smallsize at birth), and risk of CHD (Leon and Ben-Shlomo, 1997; Leon et al. 1998; Eriksson, et al.1999; Forsén et al. 1999); risk of diabetes (Barkeret al. 1993a; Lithell et al. 1996; McKeigue, 1997,
The most firmlyestablished associations
between CVD ordiabetes and factors in the
life span are thosebetween disease and themajor known ‘adult’ risk
factors—tobacco use,obesity, physical
inactivity, cholesterol,high blood pressure,
and alcohol.

9
b. Overnutrition in utero
Just as there is evidence for an association be-tween small size at birth and later disease, thereis also evidence to show that large size at birth(macrosomia), i.e. fetal overnutrition, is associ-ated with increased risk of diabetes and CVD.
In Sweden, for example, birth weight wasshown to have an inverse ‘J’ relationship withCHD, indicating that heavy babies, too, are atincreased risk (Leon et al. 1998). Among PimaIndians, diabetes was found to have a U-shapedrelationship with birth weight, again indicatinga greater risk also among those heavy-born(McCance et al. 1994).
The role of fetal overnutrition is importantto be borne in mind, particularly in view of thegeneral emphasis and prominence currentlygiven to the fetal undernutrition as a determi-nant of later disease, as encapsulated in the fe-tal origins hypothesis (Barker, 2000a).
c. Intergenerational factors
There is some evidence of intergenerationaltransmission of CVD risk associated with fetalgrowth in humans. For example, several stud-ies have shown low birth weight in offspring tobe related to parental cardiovascular mortality
(Davey Smith et al. 1997, 2000a;Sterne et al. 2001).
In some populations, moreo-ver, maternal gestational diabe-tes (GDM), has been shown tolead to large birth weight and aconsequent risk of diabetes aswell as gestational diabetes inthe offspring (Pettit andKnowler, 1998). Further evi-dence of such intergenerationaltransmission of risk, over sev-eral generations, comes fromanimal models. However, the
mechanisms for such intergenerational trans-mission of CVD and diabetes risk remain un-clear.
1.2.3 Factors in infancy and childhood
a. Retarded postnatal growth in weight
In addition to showing an association betweenretarded fetal growth and coronary heart dis-ease, evidence from the developed world alsoindicates an association between low growth inearly infancy (low weight at 1 year) and an in-creased risk of CHD, irrespective of size at birth.
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
Forsén et al. 2000a; Rich-Edwards et al. 1999);and risk of stroke (Martyn et al.1996; Leon et al1998; Rich-Edwards et al. 1997).
Low birth weight, while clearly an imperfectmarker, is the most commonly used (and mostwidely available) indicator for retarded fetalgrowth. Some research, however, has also in-vestigated the associations of more specific in-dices of fetal growth, such as birth weightcorrected for gestational age (Leon, et al., 1998).Other research has examined indicators of in-utero growth retardation such as birth length,head circumference, or ‘thinness’ i.e. ponderalindex (weight/length)3 with later disease.
The findings of such research show impor-tant differences in the strength of associationsbetween disease and different kinds of fetalgrowth retardation (Barker, 1995), and highlightthe limited value of birth weight alone in cap-turing the range of relevant fetal exposures.
Further evidence for an association betweenIUGR and later disease comes from ‘famine stud-ies’ which explore the risk of disease in cohortsexposed to famine during gestation. The DutchFamine Study exploring the effects of the DutchHunger Winter 1944–45, for example, has shownthat exposure to famine in early gestation is as-sociated with an increased riskof heart disease (Roseboom et al.2000a). No such effect, however,was found in the Russian faminestudy examining the impact ofthe Leningrad Siege 1941–1944(Stanner et al. 1997).
Only two studies in the devel-oping world, both in India, haveso far examined the associationbetween fetal growth and dis-ease, and their results suggestsimilarities and discrepancieswith those in the developedworld. An association between low birth weightand CHD was found in one study (Stein et al.1996). However, diabetes was not found to berelated to low birth weight, but rather to fatness(higher ponderal index) at birth (Fall et al. 1998).
These diverging findings and possible popu-lation differences clearly suggest that there isnot sufficient evidence to confirm a link be-tween retarded fetal growth and adult chronicdisease across all populations at all times andso can not yet be generalized to developingcountry populations.
Only two studiesin the developing world,
both in India,have so far examined
the association betweenfetal growth and disease,
and their resultssuggest similarities
and discrepancies withthose in the developed
world.
10
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
(Barker et al. 1989; Osmond et al. 1993; Erikssonet al. 2001). This association suggests the im-portance also of immediate post-natal factors inshaping disease risk.
Again, no research to demonstrate such as-sociation has yet been conducted in the devel-oping world, and thus no inferences can bemade.
b. Retarded childhood growth in height(short stature)
There is clear evidence from the developedworld that short stature or childhood leg length(both indices of socio-economic deprivation inchildhood) is associated with anincreased risk of CHD, stroke,and to some extent diabetes (e.g.Hart et al. 2000; McCarron et al.2000b, 2001a; Marmot et al. 1997;Rich-Edwards et al. 1997; Njolstadet al. 1996; Davey Smith et al.2000b; Wannameethee et al. 1998;Jousilahti et al. 1998, 2000;Forsén et al. 2000b; Gunnell et al.1998a).
Given that short stature, andspecifically short leg-length areparticularly sensitive indicators of early socio-economic deprivation (Gunnel et al. 1998c),their association to disease, very likely reflectsan association between poor early SEP and in-creased risk of disease. (Davey Smith, 1998).
Only indicative data exists so far on the linkof stature (or early SEP) to disease risk in devel-oping countries, and firm inferences can hencenot yet be made.
1.2.4 Interactions between earlyand later factors
In addition to the robust evidence on independ-ent associations of IUGR, infancy, and adulthoodfactors with later disease, there are increasingindications that the interaction between someof these early and later factors may lead to aparticularly high risk of disease.
a. Interaction between IUGRand adult obesity
Existing evidence from the developed worldshows that the interaction between retardedfetal growth and obesity in adulthood can beimportant in raising risk disease.
For example, IUGR (low birth weight),
followed by subsequent adult obesity has beenshown to impart a particularly high risk of CHD(Frankel et al. 1996), as well as of diabetes (e.g.Lithell et al. 1996).
Only indicative evidence of such an effectexists as yet for the developing world, and firmgeneralization can not yet be made.
b. Interaction between IUGR andenhanced growth in weight inchildhood/adolescence
Further evidence for an interactive effect be-tween IUGR and post-natally gained weight isprovided by studies in developed countries,
showing an interaction betweenrapid catch-up growth in weightand IUGR in raising risk of dis-ease.
In Finland, for example,among men and women, thehighest risk of CHD or meta-bolic syndrome was found to beassociated to IUGR (small sizeat birth) followed by rapidgrowth to above average weightin childhood. (Eriksson et al.,1999, 2001; Forsén et al. 2000a).
The precise period during childhood in whichrapid weight growth is detrimental is yetunclear. Evidence so far would seem to giveconflicting indications.
Considerable, but only indicative evidence onsuch an effect of catch up growth on disease isavailable from the developing world, suggest-ing that no firm generalizations can yet be made.
c. Interaction between IUGR andenhanced growth in height inchildhood/adolescence
In addition to evidence of an interaction be-tween enhanced IUGR and enhanced growth inweight, there are indications of such an effectalso for rapid growth in height in raising dis-ease risk.
In Finland, for example, short length at birthfollowed by enhanced growth in height to be-come average or tall, was found to be associ-ated with an increased risk of CHD in women(in contrast, tallness in girls with long birthlength was associated with lower risk) (Forsénet al. 1999). Similarly, among men and women,increased stroke risk was shown to be associ-ated with small size at birth followed by accel-erated growth in height to reach average levelsin later childhood (Eriksson et al. 2000a).
There is clear evidencefrom the developed world
that short stature orchildhood leg length
(both indices of socio-economic deprivation inchildhood) is associatedwith an increased risk ofCHD, stroke and to some
extent diabetes

11
Very little indicative evidence on such aneffect of enhanced growth in height on CVD ordiabetes risk factors is present from the devel-oping world, and generalizations can not yet bemade.
d. Possible interpretations of the inter-action between IUGR and later growth
The apparent detrimental interaction betweenIUGR and enhanced later growth in weight orheight—which, as the subsequent sections willdiscuss, has also been shown to be linked toraised blood pressure, dyslipidaemia and IGT,is not yet fully understood. However, four (notmutually exclusive) interpreta-tions are possible:
i. It represents a negative effectof enhanced growth in child-hood or adolescence per se. Inother words, acceleratedgrowth in weight (or height)itself could have negative con-sequences.
ii. It is the difference in size between birth andthe later stage that better defines detrimen-tal impaired early growth: the higher thedifference, the higher the risk. (see e.g. Lucaset al. 1999)
iii.Obesity reveals/activates underlying suscep-tibility induced by impaired early growth and,vice versa, low birth weight enhances the riskassociated to obesity. I.e. obesity is particu-larly harmful in those with early growth re-tardation.
iv. The effect of enhanced growth in height inIUGR babies may reflect a failure of the fetusto realize its genetic growth potential in utero,possibly due to placental failure. It may bethis insult on fetal growth, not an effect ofpost-natal growth, that underlies the in-creased risk of disease (e.g. Leon et al. 1996)
Whilst the particular interpretation maydepend on the specific disease or risk factor con-cerned, each indicates the importance of anadequate post-natal nutritional environment inbringing to the fore a risk associated with fetalgrowth retardation.
1.2.5 Developing a deeper under-standing of the associations of lifecourse factors to adult disease:individual risk domains andpotential mechanisms
The established or highly suggestive associationsdescribed above demonstrate the undoubtedclear importance of early life—as well as adult-hood factors in influencing risk of CHD, strokeand diabetes.
What is less clear however, is the nature andbasis of these associations. What is the basis ofthe association between retarded fetal or infant
growth and later disease? Whatis the nature and the basis of theapparent interaction betweenretarded fetal growth and highweight (or height) gained post-natally in raising risk of disease?What are the biological mecha-nisms underpinning theseassociations and interactions?What is the influence of socio-economic conditions? What is
the relative importance of earlier versus adult-hood risk factors in causing disease?
The following sections will examine what isknown in relation to these complex questions.They do this, first, by exploring in detail the lifecourse determinants of the five main riskdomains:
High blood pressure, dyslipidaemias andimpaired glucose tolerance, height, obesity,and unhealthy lifestyles (tobacco use, physi-cal activity, and unhealthy diet).
Discussion of each risk domain, as indicatedearlier, will specifically assess the following twoaspects:
• the global, secular trends in both developedand developing countries, and what is knownon the prevalence patterns with respect togender, ethnicity and socio-economic status.
Particular attention is paid to examining theextent to which prevalence patterns followthe classically assumed distribution, i.e. thathigher risk levels are associated with lowsocio-economic status in industrialized coun-tries, and with high socio-economic status indeveloping populations.
• what is known of the determinants of eachbiological/lifestyle related factors in:
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
There are increasingindications that the
interaction between someof these early and
later factors may lead to aparticularly high risk
of disease.

12
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
— fetal life— infancy— childhood— adolescence— intergenerationally
Of the four biological risk factor domains dis-cussed, obesity will be discussed last, becauseof the central importance of obesity in the de-velopment of the other biological riskfactors (Berenson et al. 1991; Pi-Sunyer, 1991);because of its apparent importance in raisingthe disease risk related to impaired fetal growth;and because of the growingglobal health burden relatedto obesity.
Following the examinationof the individual risk do-mains, the discussion willturn to exploring what isknown about the potentialmechanisms that underpinthe associations of fetal fac-tors to later disease risk. Thisincludes questions regarding:
• the relative role of genetic versus ‘environ-mental’ factors as the basis of the associationsbetween fetal growth and later disease
• the specific role of intergenerational andintrauterine factors (e.g. maternal or fetalnutrition) in the association between fetalgrowth and later disease
• the role of programming of endocrine, insu-lin or stress (HPA) pathways in the associa-tion between early growth and later disease
• the role of post-natal factors such as infec-tions or childhood diet in underpinningassociations, for example, between childhoodsocio-economic position and later disease
The final section will draw together the mainstrands emerging from the individual domainand mechanism discussions. It will highlight thecross-cutting themes and issues, and pinpointthe main gaps that remain in our understand-ing of the life course impacts on disease risk.
1.3 Life course perspectives onblood pressure
1.3.1 Blood pressure over the life courseas a risk factor for CVD
High blood pressure—usually measured in mid
or later life—has been established as a main riskfactor for cardiovascular diseases—stroke andcoronary heart disease. (e.g.Psaty et al. 2001).
No serial data exists, however, on the rela-tionship of blood pressure at different points ofthe life span to later disease, including bloodpressure at one year prior to the disease out-come. Such data, however, would be necessaryto determine whether long term average expo-sure to raised blood pressure is important or,perhaps, simply an acute high transient level.
Nevertheless, some long-term cohort studies(e.g. the Harvard AlumniStudy, the Chicago Heart As-sociation Detection Project orthe Glasgow University Stu-dents Study) have shown thathigh blood pressure already inadolescence or young adult-hood is strongly related to riskof stroke or CHD, independ-ently of blood pressure in midlife (Paffenbarger and Wing,1969, 1971; Paffenbarger andWilliams, 1967; Thorne et al.
1968; Miura et al. 2001; McCarron et al. 2000a).In other words, risk of CVD through high bloodpressure already starts well before middle age.
Whether, however, elevated blood pressurein early life is a stronger predictor of diseasethan high blood pressure in mid adulthood hasnot yet been established, with existing evidencebeing sparse and conflicting. Data from theHarvard Alumni study point to high blood pres-sure in midlife as a stronger indicator of risk ofnon-fatal stroke than high blood pressure inyouth. Other evidence, however, suggests anequally important effect of high blood pressurein earlier life (Navas-Nacher et al. 2001).
Indirect evidence for the importance ofexposure to high blood pressure from early lifecomes, moreover, from the Bogalusa HeartStudy which shows that high blood pressure,tracking from childhood to adulthood, is relatedto the onset of early atherosclerosis (e.g. Bao etal. 1995; Berenson et al. 1998a). More evidenceon the actual strength of the association betweenearly and prolonged high blood pressure andlater CHD or stroke will emerge as study co-horts, such as in the Bogalusa study, continueto age.
Cohort studies have shown thathigh blood pressure already in
adolescence or youngadulthood is strongly related to
risk of stroke or CHD,independently of blood pressure
in mid life. In other words,risk of CVD, through high
blood pressure already startswell before middle age.

13
1.3.2 Global trends in blood pressure
a. A word of caution
A word of caution is necessary prior to out-lining the trends and patterns in blood pressure.This concerns the current limitations in meth-odology and measurement of blood pressurewhich make international comparisons difficult,and limit the accuracy of blood pressure esti-mates within populations. The particular limi-tations include:
i. differences in measurements and methodol-ogy between national surveys
ii. a lack of data on blood pressure levels espe-cially from developing countries
iii.fundamental difficulties in the accurate meas-urement of blood pressure and hypertensiondue to the acute variability of blood pressure.Experience from the Bogalusa Heart Study,for example, has shown that estimates ofhypertension can yield up to 10–20% falsepositives. Ambulatory measures have, more-over, revealed the inadequacy of singlemeasurements as an index of‘typical blood pressure ’(Berenson, personal communi-cation).
iv. indications that ‘normal ’levels of blood pressure maydiffer between populations orage groups. In India, for exam-ple, levels appear to be lowerthan in other countries, andlevels among children arelower than among adults. Cor-rect identification of hypertension in popu-lations thus requires the establishment ofappropriate population norms of blood pres-sure.
These limitations not withstanding, severalbroad patterns and trends in blood pressure areidentified.
b. Secular trends in blood pressure
Developed world
Evidence from multi-country studies such asWHO MONICA show that in most developedcountries, mean population blood pressurelevels have decreased over the past decades (e.g.Dobson et al. 1998; Kuulasmaa et al. 2000). Manysurveys from individual countries further sup-port this general picture. In Denmark, for ex-
ample, blood pressure levels shifted towardslower values between 1964 and 1991 (Sjol et al.1998). In Finland, similar shifts at least in systo-lic blood pressure were observed between 1982and 1997 (Kastarinen et al. 2000), and in the U.K.between 1984 and 1993 (Bartley et al. 2000).
However, not all countries show this generaltrend. In Japan, for example, more complextrends have been observed. Whereas systolic anddiastolic blood pressure levels had decreaseduntil the early 1990s, they have plateaued dur-ing the last ten years, showing cyclical oscilla-tions (Hasegawa and Oshima, 2001).
Developing world
In contrast to the largely declining trends inblood pressure in the developed world, the lit-tle available evidence suggests that blood pres-sure levels in developing countries are rising.In China, for example, WHO MONICA and otherstudies have found significant increases in bothdiastolic and systolic blood pressure over thepast decades (Dobson et al. 1998; Gao et al. 1999),one study documenting such adverse trends par-
ticularly in the younger popu-lation (aged 15–34) (Yu et al.1999).
In general, the prevalence ofhypertension seems to rise withGNP, i.e. the higher the level ofeconomic ‘development’ thehigher the prevalence of hyper-tension (Fuentes et al. 2000).
Hypertension—though rec-ognized as a public health prob-lem since the 1970s in some
nations—is now, clearly, a problem in most de-veloping countries (Fuentes et al. 2000). Highblood pressure is particularly found to be a prob-lem in Sub-Saharan Africa, consonant with thehigher rates of stroke and susceptibility to hy-pertension observed among black populations(Pickering, 2001).
1.3.3 Social patterns of blood pressure
Developed countries
In developed countries, the prevalence of highblood pressure and other cardiovascular riskfactors has generally been found to have asocial gradient, with higher prevalence amongthose with lower socio-economic positions(Bartley et al. 2000; Marmot 1989; Luepker et al.1993; Lynch et al. 1996; Myllykangas et al. 1995,Manhem et al. 2000; Colhoun et al. 1998).
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
In contrast to thelargely declining trends in
blood pressure in thedeveloped world, the little
available evidencesuggests that bloodpressure levels in
developing countriesare rising.

14
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
Apart from low adult socio-economic posi-tion, low childhood socio-economic position,too, has often but not always been found to beassociated with higher blood pressure in laterlife (Blane et al. 1996; Lynch et al. 1997; Brunneret al. 1999). Evidence suggests, however, thatits effect is weaker than that of adult socio-economic position (Blane et al. 1996).
Despite applying overall, it is important tobear in mind that the generally observed socialgradient pattern may not apply to all ethnic orpopulation groups. For example, among blacksin the US no significant differences in bloodpressure levels were found between socio-economic groups (Resnicow et al. 2001).
Developing countries
In developing countries, blood pressure patternsare usually assumed and typically found to showmarked rural/urban differences with levelsconsiderably higher in urban populations, andamong higher socio-economicgroups (e.g. Colhoun et al. 1998)
In India, for example, the CRI-SIS study (Coronary Risk of In-sulin Sensitivity in IndianSubjects) found hypertensionprevalence to be highest amongurban middle class population(12.4%), much lower prevalencein urban slum dwellers (3.8%),and the lowest prevalence in ru-ral populations (2.4%) (Lubree et al. 2001). Simi-lar urban-rural and socioeconomic groupdifferences in blood pressure and hypertensionlevels have been found in China (Gao et al. 1999;Yu et al. 2000).
Evidence from Nigeria, Tanzania and theGambia, similarly shows significantly higherlevels of hypertension in urban compared torural areas (Kaufman et al. 1999; van der Sandeet al. 2000; Ministry of Health Tanzania, 1997).In urban Nigeria and in Tanzania, moreover, thehighest rates of hypertension were found in thehigher socioeconomic groups (Olatunbosun etal. 2000; Ministry of Health Tanzania, 1997).
Although this general pattern prevails inmany cases, it is again important to bear in mindthat it may not always hold. In urban China, forexample, blood pressure was found to be high-est among those with lowest socio-economicpositions (Yu et al. 2000). In South Africa, simi-larly, blood pressure levels were not found tosimply rise with degree of urbanization. Rather,
the highest levels were found among newcom-ers to cities living in informal settlements. Thelowest levels were, in fact, found in the mosturbanized group (van Rooyen et al. 2000).
1.3.4 Factors in childhood andadolescence and blood pressure
a. High blood pressure originsin childhood
High blood pressure and essential hypertensioncan emerge in childhood.
Contrary to the long held assumption thathigh blood pressure emerges in mid adulthood,evidence from the developed world (e.g. theBogalusa Heart Study) shows that it is alreadypresent in children. Some evidence also showsthat blood pressure ‘tracks’ from childhood topredict hypertension in adulthood, though thestrength of tracking to adulthood varies depend-ing on age, with stronger tracking seen at older
ages in childhood or adolescence(see Whincup and Cook, 1997).Virtually no evidence exists yeton the emergence and develop-ment of high blood pressure inchildren in developing coun-tries.
As the developed world evi-dence further shows, high bloodpressure in childhood (in com-bination with other risk factors),
moreover, causes target organ and anatomicalchanges associated with cardiovascular risk,such as reduction in artery elasticity, increasedleft ventricular size and mass, haemodynamicincrease in cardiac output, and peripheralresistance. These effects are seen already atlevels lower than the conventional 140/90 cut-off point used to define adult hypertension(Berenson et al. 1991, 1998a; Bao et al. 1995).
High blood pressure in children is stronglyassociated to obesity, in particular central obes-ity. It moreover clusters and tracks with anadverse serum lipid profile (especially LDL-c)and glucose intolerance (Berenson et al. 1991,Tershakovec et al. 1998). Such clustering andtracking has also been shown in non-westernindustrialized populations, for example inJapan (Tan et al. 2000).
Within this general picture, however, someracial differences have also been observed insome studies. These include the higher bloodpressure rates and rises found in black children,especially boys; and the stronger relationship
Low childhoodsocio-economic positiontoo, has often but not
always been found to beassociated with higher
blood pressure inlater life.

15
of blood pressure to obesity in white children(Berenson et al. 1991). In a recent cross-sectionalstudy of more than 47,000 children and adoles-cents in the US, few substantive differences inblood pressure were observed between African-Americans and Whites. The racial differencesin blood pressure that did emerge were oftenexplained by differences in BMI. Interestingly,at lower levels of BMI black children and ado-lescents tended to have higher blood pressureand more hypertension, but athigher levels of BMI, the reversewas true (Rosner et al. 2000).
The presence and tracking ofblood pressure in children andadolescents occur against a back-ground of unhealthy lifestyles.These include excessive intake oftotal and saturated fat, choles-terol and salt, inadequate intakeof potassium, and reduced physical activity, of-ten accompanied by high amounts of televisionviewing. In older children habitual alcohol andtobacco use moreover contributes to blood pres-sure (Berenson et al. 1991; Okasha et al. 2000).
Breastfeeding and blood pressure
Just as diet in childhood is important, there areindications that breastfeeding in infancy too hasan effect on later blood pressure levels.
There is specific evidence from recent pro-spective studies and trials, for example in theUK, showing that among term and pre-terminfants, breastfeeding was associated withsignificantly lower blood pressure levels in child-hood (Wilson et al. 1998; Singhal et al. 2001).
Other studies on older cohorts, however, forexample in the UK (Fall et al. 1998) or the DutchFamine Study (Ravelli et al. 2000) have shownno such association, possibly reflecting cohortor population variations relating to modes orduration of breast feeding.
The mechanisms that may underlie a ben-eficial effect of breastfeeding on blood pressureare not yet understood. Virtually no evidenceexists, moreover, on the effects of breast feed-ing on blood pressure in developing countrypopulations.
1.3.5 Fetal factors and blood pressure
a. IUGR and high blood pressure
In addition to its determinants in childhood,there is consistent evidence that high blood pres-
sure, in particular high systolic blood pressurein adulthood is associated with retarded fetalgrowth (as measured by low birth weight)(Huxley et al. 2000; Eriksson et al. 2000a; Leonet al. 2000). It is not yet clear, however, whetherthis association mediates the link between IUGRand CVD.
Most of the evidence showing this associa-tion comes from studies in developed countries,though some also comes from the developing
world, for example from China(Mi et al. 2000) or South Africa(Levitt et al. 2000).
Blood pressure in childhoodhas equally been found to be as-sociated to low birth weight. Theevidence comes from studies onchild cohorts in both the devel-oped and developing world,for example in Sweden, Chile,
Guatemala, China (Law et al. 2001); the UK(Whincup et al. 1999); Zimbabwe (Woelk et al.1999); South Africa (Levitt et al. 1999); theDemocratic Republic of Congo (Longo-Mbenzaet al., 1999); Jamaica (Walker et al. 2001); andIndia (Bavdekar et al. 1999).
In contrast to the bulk of evidence, some de-veloping country studies, among children inJamaica (Gaskin et al. 2000) and Nigeria (Lawet al. 2001), and among adults in India (Kumaranet al. 2000) and Hong Kong (Cheung et al. 2000)do not find an association between small size atbirth and higher blood pressure. The latter,rather, find greater length at birth to be associ-ated to higher blood pressure.
Similarly, findings from the two natural ‘fam-ine’ studies—the Leningrad Siege Study, and theDutch Famine Study, show no association be-tween exposure to famine at any stage in gesta-tion and higher blood pressure in adulthood(though in the Dutch cohort, exposure late ingestation was associated with lower birthweight) (Stanner et al. 1997; Roseboom et al.2001).
These divergent findings clearly highlight twoimportant points:
• First, they indicate the possible existence ofpopulation and cohort differences in the re-lationship of fetal growth to blood pressure.It has been suggested that this relationshipmay be specifically different in blackpopulations.
• Second, they indicate that the associationwith higher blood pressure may depend on
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
Just as diet in childhoodis important, there are
indications thatbreastfeeding in infancytoo has an effect on later
blood pressure levels.

16
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
the type of growth retardation or impairmentexperienced in utero, with birth weight toocrude an index to distinguish between suchdifferent factors
b. Issues relating to the link betweenIUGR and high blood pressure
A mediating effect of obesity or enhancedweight gain in childhood/adolescence?
Just as evidence has indicated a possible inter-acting effect of obesity or gained weight in en-hancing the risk of CHD ordiabetes associated with im-paired fetal growth, severalindications also point to such apossible effect for blood pres-sure:
i. A mediating effect of obesity(high BMI)
Some evidence on the associa-tion between low birth weightand adult blood pressure, for ex-ample from Sweden, demon-strates an apparent mediatingeffect of obesity (high BMI). It shows that theeffect of low birth weight on higher blood pres-sure increased with rising adult BMI, being sig-nificantly stronger in the highest than in thelower tertile of BMI (Leon et al. 1996). Con-versely, the association of current BMI to bloodpressure was enhanced in those with low birthweight.
Such an effect of fatness has been replicatedin other studies though not in all. In the studyamong 11–12 year old children in Jamaica, forexample, blood pressure levels were found tobe highest in those with retarded fetal growthand greater weight gain between the ages of 7and 11 (Walker et al. 2001). Similarly, in the childcohort study in India (Bavdekar et al. 1999),blood pressure was highest in those with lowbirth weight and highest fat mass at age 8,though the interaction term was not statisticallysignificant. These children also had the highestcentral adiposity.
Further studies on the body composition oflow birth weight Indian babies have revealedthat these, e.g. in contrast to newborns in theUK, these have a distinct phenotype character-ized by poor muscle but high fat preservation.It is this ‘thin-fat’ phenotype, which persiststhrough the post-natal period and is associatedwith increased central adiposity in childhood,
and the higher risk of raised blood pressure (Fallet al. 1999; Yajnik, 2000, 2001).
ii. Adjustment for current size (BMI)
In most studies, the association between lowbirth weight and high blood pressure has beenfound to be particularly strong if adjusted forcurrent size (BMI), suggesting the importanceof weight gain after birth on the association(Lucas et al. 1999).
As discussed in the previous section, the ap-parent effect of post-natallygained weight is as yet poorlyunderstood, and several possibleinterpretations exist. What isclear, however, is that it signalsthe importance of the postnatalcontext of nutrition and growthin shaping the association be-tween impaired fetal growth andhigher blood pressure later in life.
A mediating effect of enhancedgrowth in height in childhood/adolescence?
In addition to the possible mediating effect ofobesity, there is evidence to suggest an interac-tion between small size at birth and acceleratedgrowth in height in raising risk of disease.
In Sweden, for example, low birth weight fol-lowed by enhanced growth in height to becometall in adulthood was found to be associated withhighest blood pressures (Leon et al. 1996). InFinland, similarly, shortness and thinness atbirth combined with accelerated growth inheight (as well as weight) to reach average lev-els was associated with increased risk of hyper-tension (Eriksson et al. 2000b).
The nature and factors underlying thiseffect of height growth are not yet fully under-stood. However, again, they point to the impor-tance of the post-natal (nutritional) environmentin shaping the association between retardedfetal growth and blood pressure.
Underlying mechanisms—genetic?environmental?
The mechanism underpinning the observedassociation between retarded fetal growth (lowbirth size) and higher blood pressure remainspoorly understood. The most important ques-tion concerns the relative role played by genetictraits as opposed to environmental exposuresin utero.
Just as evidence hasindicated a possibleinteracting effect of
obesity or gained weightin enhancing the risk of
CHD or diabetesassociated with impaired
fetal growth, severalindications also point tosuch a possible effect for
blood pressure.

17
As has been proposed for insulin resistance(IR), the association may reflect the action ofgenetic feature that simultaneously affects birthweight (fetal growth) as well as physiologicalcomponents predisposing to high blood pressure(Hattersley et al. 1998; Hattersley and Tooke,1999). Alternatively, the association may reflectthe effect of exposures in utero, for example as aresult of maternal nutrition or stress, which leadto fetal adaptations which in turn lead to higherblood pressure later on.
Although several twin studies have exploredthe relationship between impaired fetal growthand blood pressure, they have failed to producea particularly clear picture, perhaps partly as aresult of methodological problems.
Their findings as they stand have not pro-duced particularly convincing evidence for anenvironmental effect (Dwyer et al. 1999; Poulteret al. 1999; Ijzerman et al. 2000; Baird et al. 2001;Rassmussen (unpublished).
Little support for the role specifically of ma-ternal undernutrition in causing high blood pres-sure comes, moreover, from the famine studies.(Roseboom et al. 2001 ; Stanner et al. 1997)
Inadequacy of low birth weightas an index of IUGR
The Dutch famine study’s find-ing of an association betweenhigh blood pressure and expo-sure to famine in early gestation(an exposure that was not associ-ated with low birth weight)clearly indicates the limitation oflow birth weight in capturing the range of po-tentially important exposures in utero.
1.3.6 Intergenerational factorsand blood pressure
a. Maternal birth weight
Some recent evidence from the UK suggests apossible intergenerational effect on risk of bloodpressure associated with maternal fetal growth.The data shows that blood pressure levels inadult offspring were inversely related to mater-nal fetal growth, i.e. low maternal birth weightwas associated with higher blood pressurelevels in the offspring, independent of the rela-tion between offspring’s own birth weight andblood pressure (Barker et al. 2000b). The mecha-nisms underlying such an intergenerationalassociation are as yet poorly understood.
1.4 Life course perspectives ondyslipidaemias and impairedglucose tolerance (IGT)
1.4.1 Dyslipidaemias and IGT over thelife course as risk factors for CVDand diabetes
Dyslipidaemias and impaired glucose tolerance(IGT) are commonly considered together as el-ements of the metabolic syndrome or ‘syndromeX’. Syndrome ‘X’—the clustering in the popula-tion of physiological disturbances associatedwith insulin resistance, i.e. hyperinsulinaemia,IGT, hypertension, elevated plasma triglycerideand low high density lipoprotein cholesterol(HDL-c)—is considered a distinct condition thatis related to diabetes and atherosclerotic cardio-vascular disease (Reaven, 1988; De Fronzo et al.1991).
The clustering of these risk variables alreadyoccurs in childhood and adolescence and is as-sociated with atherosclerosis in young adult-hood, and thus risk of later cardiovasculardisease (Bao et al. 1994; Berenson et al. 1998a).In some though not all cases, moreover, such
clustering of risk factors inchildhood is shown to lead onto diabetes, suggesting thatthere may be several differentsubtypes of ‘syndrome X ’(Berenson, personal communica-tion).
Raised serum cholesterol lev-els on their own in middle agehave also been established as a
clear risk factor for cardiovascular disease (e.g.Davey Smith et al. 1992; Neaton and Wentworth1992).
Raised serum cholesterol in early life, too, isshown to be already associated with anincreased risk of disease later on. The JohnsHopkins Precursor Study, for example, hasshown that among white males serum choles-terol levels in adolescence or young adulthoodwere strongly related to subsequent risk of CVDmorbidity and mortality. An increased risk ofCVD, especially for CHD, was found even forhigher cholesterol levels in the ‘normal’ range,indicating that serum cholesterol levels inhealthy young adults are a strong predictor ofdisease in mid-life (Klag et al. 1993).
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
Some recent evidencefrom the UK suggests a
possible intergenerationaleffect on risk of blood
pressure associated withmaternal fetal growth

18
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
1.4.2 Global trends in dyslipidaemiasand IGT
a. Secular trends in serum lipid levels
Developed countries
Evidence from multi-country (e.g. WHOMONICA) and national surveys suggest favour-able trends in serum lipid levels in most devel-oped countries over the past decades. WhilstWHO MONICA found little overall change inpopulation cholesterol levels in most of the 20developed world countries studied during the1980s (Dobson et al. 1998), na-tional surveys, for example inthe US or Finland have shownconsistent reductions as well asreductions in the incidence ofhypercholesterolaemia (e.g.Szklo et al. 2000; Johnson et al.1993; Kastarinen et al. 2000).
Developing countries
Very little evidence is available on trends in li-pid levels in developing countries, in particularin Africa, Latin America and South Asia. Thelittle evidence that is available suggests an un-favourable trend, contrasting with the situationin the developed world.
Secular increases in dyslipidaemia have beenindicated for several developing countrypopulations. In China, for example, Sino-MONICA has shown rises in cholesterol levelsin mid aged adults between 1984/86 and 1988/89 (Yao et al. 1993; Dobson et al. 1998). Similarrises have been observed in other Chinesepopulations with one study finding them in par-ticular among younger age groups (e.g. Gao etal. 1999).
b. Secular trends in impairedglucose tolerance
Whilst comprehensive data on global trends andpatterns in IGT is sparse, some data and projec-tions on diabetes prevalence as measured byvenous post-load plasma glucose are available.(King et al. 1998) These data show that preva-lence of diabetes is currently higher in devel-oped and than in developing countries, and willremain so by 2025. However, the proportionalincrease will be greater in the developing world,greatest in China and India.
1.4.3 Social patterns in dyslipidaemiasand impaired glucose tolerance
a. Social patterns in serum lipid levels
Developed countries
Adverse lipid levels, as most other cardiovascu-lar risk factors are, currently, generally shownto have a social gradient, with higher prevalenceamong those with lower socio-economic posi-tion. (Bartley et al. 2000; Brunner et al. 1999;Marmot 1989; Luepker et al. 1993; Lynch et al.1996; Myllykangas et al. 1995; Perova et al. 2001).
An opposite gradient, interest-ingly, was found a few decadesago in the UK, highlighting thefact that socio-economic pat-terns of disease risk factors maybe cohort specific. The WhitehallI study in the late 1960s, for ex-ample, found higher adverselipid levels among higher rank-ing UK civil servants (Smith et
al. 1992), indicating that a social gradient re-versal in dyslipidaemia levels has occurred overthe past three decades. A similar reversal is pre-dicted for non-industrialised countries as theyprogressively develop and urbanize.
In addition, adverse lipid levels have some-times but not always been shown to be linkedto poor childhood socio-economic position. Inthe West of Scotland Collaborative Study amonga cohort of employed men, for example, serumcholesterol was related to poor adult and poorchildhood SEP, though the effect of the latterwas weaker (Blane et al. 1996). The Whitehall IIstudy, however, only found childhood SEP to belinked to adverse HDL-c levels in women(Brunner et al. 1999). A recent study of men inEastern Finland similarly found a detrimentalimpact of low childhood SEP. Compared to menwho had been born into advantaged childhoodcircumstances and had gone on to high incomepositions later in life, men who had come frompoorer backgrounds but achieved the same levelof adult income had significantly higher LDL-clevels. However, no socio-economic differencesin HDL-c were observed (Lynch, 2000).
Despite the broad overall pattern of moreadverse lipid profiles among the lower socialstrata, it is clear that this social gradient maynot hold in all developed countries. In Russiaand Poland, for example, an opposite gradientwas found, with adverse lipid levels increasingdirectly with years of education (Perova et al.2001).
In addition, adverselipid levels have
sometimes but not alwaysbeen shown to be linkedto poor childhood socio-
economic position.

19
Furthermore, the expected social gradientmay not apply in specific ethnic groups. Amongblacks in the US, for example, no significantdifferences in cholesterol levels were foundbetween socio-economic groups (Resnicow et al2001).
Developing countries
In the developing world, the prevalence ofdyslipidaemias is generally assumed to followan opposite pattern to that in the developedworld, i.e. levels are assumed to increase withsocio-economic position and to be highest in theaffluent, urban population.
The little evidence available from develop-ing countries suggests that in most cases levelsfollow this general pattern. In China, for exam-ple, the prevalence of adverse lipid profilesamong men was found to increase directly withyears of education (Perova et al. 2001).Dyslipidaemia prevalence in Taiwan has simi-larly been shown to be higher in higher socio-economic groups (Lee et al.2000).
In Jamaica, serum cholesterollevels among children and ado-lescents were found to show asimilar social gradient withhigher levels in those of highersocio-economic back ground(Forrester et al. 1996).
In India, as expected, choles-terol and triglyceride levels have been found tobe highest among middle class urbanpopulations, followed by urban slum dwellers,and lowest in rural samples (Lubree et al. 2001).Similar rural-urban distributions in hyperlipi-daemia were found in the Gambia (van derSande et al. 2000).
Evidence suggests, however, that the preva-lence of dyslipidaemias does not always followthe expected pattern or gradients. In Tanzania,for example, cholesterol levels were found to besignificantly higher in affluent rural areas thanin urban areas (Ministry of Health Tanzania,1997). Blood cholesterol concentrations in SouthAfrica, similarly, were found not to rise withdegree of urbanization (Steyn et al. 1997).
b. Social patterns in impairedglucose tolerance
Developed countries
In developed countries, impaired glucose toler-ance, just as dyslipidaemias, is generally found
to be higher among the poor socio-economicstrata. However, it has not so far been found tobe associated to poor childhood socioeconomicposition (e.g. Brunner et al. 1999; Wannametheeet al. 1996).
Developing countries
Very little data exists on the social patterns ofimpaired glucose tolerance or diabetes in de-veloping countries. However, diabetes or IGT,just as the other risk factors, are again assumedto be higher among the more affluent, urban,‘westernised’ population.
The little information available suggests thatin many cases this pattern holds.
In India (Lubree et al. 2001) and the Gambia(van der Sande, 2000), for example, diabetesprevalence has been shown to be considerablyhigher in urban than in rural areas and, in thecase of India, has also been found to be signifi-cantly higher among the more affluent popula-tion.
Despite the rural urban dif-ferentials, however, it is impor-tant to note that in many casesdiabetes or IGT prevalence inthe rural population is alreadysubstantial. In India, for exam-ple, rural prevalence was foundto stand at almost 10%.
In China, similarly, rural lev-els are found to be almost as
high as those in the urban population (van derSande, 2000).
1.4.4 Factors in childhood/adolescenceand dyslipidaemias and IGT
a. Origins of IGT and dyslipidaemiasin childhood
Developed country evidence, for example fromthe Bogalusa Heart Study, the Young FinnsStudy, and Japan, shows that impaired glucosetolerance and an adverse lipid profile alreadyemerge in childhood or adolescence, where theytypically appear clustered together with higherblood pressure and relate strongly to obesity, inparticular central obesity (e.g. Berenson et al.1991; Raitakari et al. 1994 a,b; Twisk et al. 1999;Tan et al. 2000). Virtually no evidence exists yeton the emergence and development of thesefactors in children in the developing world.
Evidence moreover shows that obesity inchildhood is the driving force behind the emer-gence of both IGT and dyslipidaemias, and their
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
Evidence suggests,however, that the
prevalence ofdyslipidaemias does not
always follow the expectedpattern or gradients.

20
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
tracking through adolescence into early adult-hood (e.g. Berenson et al. 1991).
Within this broad pattern, race and genderdifferences have been observed in the emer-gence and development of obesity. These in-clude the development of a markedly moreadverse profile of triglycerides and HDL-c inwhite boys, and the weaker relationship of obes-ity to dyslipidaemia in black girls (Berenson etal. 1991).
As is the case with blood pressure, IGT anddyslipidaemia in children and adolescents is ac-companied by unhealthy lifestyles, includingthe excessive intake of total and saturated fat,cholesterol and salt, inadequate intake of po-tassium or fibre, as well as lack of exercise, of-ten due to television viewing. Inolder children habitual alcoholand tobacco use moreover con-tributes to blood pressure(Berenson et al. 1991; Raitakariet al. 1994c; 1997; Boulton, et al.1995; Ludwig et al. 1999).
The importance of a low satu-rated fat diet in lowering choles-terol levels in children hasrecently been demonstrated in a recentrandomized controlled trial in Finland (Simellet al. 1999).
b. Breastfeeding and dyslipidaemiasand IGT
In contrast to the relatively solid evidence for abeneficial effect of breastfeeding on blood pres-sure, evidence on its effects on dyslipidaemiasand IGT is conflicting (Berenson et al. 1991).
Whilst data from the Dutch Famine Studyshowed exclusive breastfeeding in the first fewweeks to be associated to a lower risk of IGTand a more favourable lipid profile (Ravelli etal. 2000), studies on younger cohorts, for exam-ple in the Bogalusa Heart Study, or a recentstudy in the UK (Leeson et al. 2001) as well ason a historical cohort (Fall et al. 1995), find nosuch beneficial effect of breastfeeding on dyslipi-daemias (Leeson et al. 2001).
Virtually no evidence exists on the long termeffects of breastfeeding on lipid levels and IGTin developing country populations.
1.4.5 Fetal factors, dyslipidaemiaand IGT
In addition to its determinants in childhood,evidence in western populations has shown a
strong association between reduced fetal growthand increased risk of metabolic syndrome(measured as an aggregate of all componentstaken as a single binary trait) in middle life(Barker et al. 1993b).
However, the association of fetal growth toIGT or those dyslipidaemias most stronglyassociated to CVD risk (i.e. high triglyceride andlow HDL-c levels) is less clear cut.
a. Fetal factors and dyslipidaemias
Current evidence on the relationship betweenfetal growth and serum lipid levels is somewhatconflicting and difficult to interpret.
In developed countries, several studies havefound relationships between small size at birth
and adverse serum total choles-terol (TC) or LDL-c levels(Barker et al. 1993b; Tenhola etal. 2000). Some have, moreover,found associations betweensmall size at birth and triglycer-ide levels in youth (Donker et al.1997; Morley et al. 2000). Others,however, have found no associa-tion between reduced fetal
growth (small size at birth) and adverse triglyc-eride (TG) or HDL-c levels (Lithell et al. 1996;Phillips et al. 1995; Valdez et al. 1994).
Data from the Dutch Famine Study similarlyfails to show a significant association betweenexposure to famine in utero and adverse HDL orTG levels. However it does show a significantassociation between exposure to famine in earlypregnancy (not related to lower size at birth)and a more adverse lipid profile (a higherLDL:HDL ratio) (Roseboom et al. 2000b).
The finding of the Dutch study conflicts withthat of the Russian Famine Study which foundno effect of exposure to famine in utero on lipidlevels (Stanner et al. 1997).
In contrast to the developed world, evidencefrom developing countries so far has consist-ently shown an association between small sizeat birth and adverse lipid levels. In China, forexample, an association has been shown be-tween low birth weight and higher triglyceridelevels in adults (Mi et al. 2000).
In Jamaica, among 6–16 year olds, a relation-ship was found between length at birth and to-tal cholesterol levels (Forrester et al. 1996).Similarly, the recent child cohort study in Indiahas found a link between low birth weight andadverse total serum cholesterol and LDL-c lev-els in 8 year old children (Bavdekar et al. 1999).
Current evidence on therelationship between fetalgrowth and serum lipid
levels is somewhatconflicting and difficult
to interpret.

21
b. Fetal factors and impaired glucosetolerance
Developed countries
In contrast to the limited evidence regarding alink between reduced fetal growth and lipid lev-els, considerably clear evidence shows an asso-ciation between IUGR and IGT—at least inwestern populations that are at comparativelylow risk of diabetes.
A consistent association between small sizeat birth and IGT in adulthood has been found inhistorical cohort studies. Typically this relation-ship has been found more strongly withponderal index (‘thinness’) at birth than withbirth weight (Hales, et al. 1991; Phipps et al.1993). An association between low ponderal in-dex and IGT in children has been shown, forexample, in the UK (Law et al. 1995).
Further evidence for an association betweenIUGR and IGT comes from the Dutch FamineStudy. This has shown an increased risk of IGTin those adults who were exposed to famine inlate gestation. The highest risk was found inthose who had become obese as adults (Ravelliet al. 1998).
The Dutch finding again conflicts with thatof the Russian Famine Study which found noeffect of exposure to famine in utero on risk ofimpaired glucose tolerance (Stanner et al. 1997).
Developing countries
Much of the sparse evidence from developingcountries also indicates an association betweenretarded fetal growth and impaired glucosetolerance.
In China, for example, an as-sociation between low birthweight and IGT was foundamong a cohort of adults (Mi etal. 2000).
Child cohort studies in devel-oping countries, for example inIndia and South Africa, haveshown a similar association be-tween IGT and small size atbirth, with the link being strongest in those whohad become fat or tall in childhood (Yajnik et al.1995; Bavdekar et al. 1999; Crowther et al. 1998).In Jamaica an association to IGT was found onlywith short length at birth among prepubertalchildren (Forrester et al. 1996).
No clear association between IUGR and IGT,however, has been found among adults in someethnic populations, such as Indians or Pima
Indians who are at high risk of diabetes.In India, among adults (and in contrast to the
relationship found among children) an associa-tion was found between IGT and high ponderalindex (i.e. fatness) at birth (Fall et al. 1998). InPima Indians, a U-shaped relationship to birthweight was found; among Mexican Americansthe relationship was found to be flat (McCanceet al. 1994; Valdez et al. 1994).
A possible interpretation has been that thesedivergent results reflect a high prevalence of ma-ternal gestational diabetes (GDM) in thesepopulations which, in turn, leads to macrosomia(large size at birth), hyperinsulinaemia andchanged glucose metabolism in the fetus, in turnpredisposing to diabetes in later life (McKeigue,1997).
c. Issues relating to the relationshipbetween fetal growth and IGT
The current findings regarding the associationbetween fetal growth and IGT highlight severalimportant issues regarding the role, nature ofthe relationship, and the mechanisms that un-derpin it.
Insulin resistance or insulin deficiency?
Evidence is as yet unclear as to whether theobserved association between fetal growth andlater impaired glucose tolerance in manypopulations is underpinned by insulin resist-ance or insulin sensitivity (insulin deficiency).
In the developed world, most evidence so farsuggests that insulin resistance rather than in-sulin deficiency is involved (McKeigue, 1997;
Phillips et al. 1994; Lithell et al.1996; Ravelli et al. 1998), al-though some studies find no in-dication of insulin resistance(Robinson et al. 1992; Law et al.1995).
In the developing world, too,most evidence points to the in-volvement of insulin resistance(Bavdekar et al. 1999; Valdez et
al. 1994; Mi et al. 2000). However, the studyamong Indian adults showing an associationbetween fatness and IGT, implicates insulin sen-sitivity as the underpinning process, indicating,perhaps a very different kind off association.
Population differences?
The conflicting evidence regarding the associa-tion between fetal growth and serum lipid
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
Much of the sparseevidence from developingcountries also indicatesan association between
retarded fetal growth andimpaired glucose
tolerance.

22
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
levels, especially for triglyceride levels suggeststhat there may be important population differ-ences in the way fetal growth relates to or im-pacts on lipid metabolism.
Evident population differences are shown inthe association between small size at birth andIGT. As mentioned, these are thought to per-haps reflect the effect of a high population preva-lence of maternal gestational diabetes.
Cohort differences—importance of the post-natal environment?
The conflicting findings regarding the relation-ship between IUGR and IGT among children andadults in India may indicate the existence ofimportant cohort differences in the impact thatreduced fetal growth has on subsequent risk.These differences may reflect changes in thepost-natal environment for the two cohorts, asa result of rapid social change in India.
A mediating effect of obesityor enhanced weight gain inchildhood/adolescence
As in the case of blood pressure,there are indications that therelationship of IUGR to IGT ordyslipidaemia may be mediatedby the degree of weight gainedpost-natally:
i. A mediating effect of high BMI
One study in the developedworld has shown that the adverse effect of re-duced fetal growth on risk of IGT was largest inthose with highest adiposity. At the same time,the IUGR and later adiposity showed a signifi-cant interaction such that the risk of IGT washighest in those who had low birth weight butwho had become obese as adults (Lithell et al.1996).
A similar effect of IUGR and fatness gainedon IGT risk has been shown in child cohorts inSouth Africa (Crowther et al. 1998) and India(Bavdekar et al. 1999). In the latter, insulin re-sistance and dyslipidaemia were highest in thosewho had low birth weight but had highest fatmass at 8 years, though the interaction betweenIUGR and current size was only significant forIR (Bavdekar et al. 1999). As in the case of bloodpressure, the raised risk of IR and dyslipidaemiain these children was linked to their increasedcentral adiposity driven by the distinct thin-fatphenotype of IUGR Indian babies (Fall et al.1999; Yajnik, 2000, 2001).
ii. Adjustment for current BMI
In addition to the observed effect of obesity, theapparent role of weight gained in mediating thelink between IUGR and disease risk is indicatedby the fact that most studies find a significantor strong link only after adjustment for currentweight or BMI (Yajnik et al. 1995; Bavdekar etal. 1999, Crowther et al. 1998).
A mediating effect of high post-natal growthin height?
Some indicative evidence of a mediating effectalso of height gained post-natally, as has beensuggested for blood pressure, comes from theIndian child cohort study.
This shows that highest insulin resistancelevels were found in children who had low birthweight but had subsequently grown tall at 8years. Among these children, insulin resistancewas highest in those who had short parents
(Bavdekar et al. 1999).As in the case of blood pres-
sure, the apparent effect of post-natally gained weight or heighton the link between IUGR andrisk is as yet poorly understood.However, it again signals theimportance of the post-natalnutritional context in shapingthe association between im-paired fetal growth and higherblood pressure.
Differential effect of starvation in utero:importance of the post-natal nutritionalenvironment
A final strand of evidence indicating the impor-tance of the post-natal nutritional environmentin bringing out the risk attached to reduced fe-tal growth, are the discrepant findings betweenthe Dutch and the Russian Famine studies.
The fact that the Russian study has failed tofind any effect of exposure to famine on laterrisk of disease, whereas the Dutch study has,may suggest that nutritional deprivation in uteromay only be detrimental if it is followed by ad-equate or plenty nutrition after birth. This wasthe case in the Dutch famine which endedabruptly after 5–6 months and was followed bya period of adequate nutrition and increasingaffluence. In contrast, the Leningrad siege lasted28 months (1941–1944) with extreme under-nutrition lasting from July 1941 through 1942.Thus, children exposed to undernutrition inutero continued to be inadequately nourished.
As is the case for bloodpressure, the mechanisms
underpinning theobserved association
between retarded fetalgrowth (low birth size)and risk of impairedglucose tolerance or
dyslipidaemia remainpoorly understood.
23
In this context, exposure to undernutrition inutero did not confer an increased risk of IGT ordyslipidaemia.
Underlying mechanisms—genetic?environmental?
As is the case for blood pressure,the mechanisms underpinningthe observed association be-tween retarded fetal growth (lowbirth size) and risk of impairedglucose tolerance or dyslipi-daemia remain poorly under-stood. The most fundamentalquestion concerns the relativerole played by genetic traits as opposed to envi-ronmental exposures in utero.
Some evidence and a specific hypothesis havebeen advanced to argue for a genetic base, re-lated to glucokinase deficiency, of the associa-tion between retarded fetal growth and IGT(Hattersley et al. 1998; Hattersley and Tooke,1999).
Results from the few twin studies conductedso far as well as from migrant studies also pro-vide no particularly convincing evidence for anenvironmental effect (Baird et al. 2001;McKeigue, 1997; Poulsen et al. 1997).
In contrast, the link found between exposureto famine and IGT in the Dutch Famine Studywould seem to point to a role of intrauterineexposures (Stanner et al. 1997).
1.4.6 Intergenerational factors and IGT
Several strands of existing evidence suggest thatrisk of IGT related to fetal growth may be trans-mitted intergenerationally.
a. Maternal gestational diabetesmellitus (GDM)
Evidence from animal models suggests thatexposure to maternal gestational diabetes or hy-perglycaemia in utero results in IGT in the off-spring, and that this effect is transmissible fromone generation to the next (see McKeigue, 1997)
Among Pima Indians, a similar effect isobserved. Findings suggest that exposure tomaternal gestational diabetes is associated to ahigher risk of IGT in the offspring, as well as ahigher risk of developing GDM, independentlyof offspring’s weight (Pettit and Knowler, 1998).
Evidence from other populations indicatesthat the risk of developing GDM is enhancedby maternal obesity (Martorell et al. 2001) as
well as by short stature (Kousta et al. 2000;Anastasiou et al. 1998; Jang et al. 1998) whichin turn may be linked to intergenerational proc-esses of risk transmission.
The possible mechanisms that underpin thedevelopment of GDM and its association to
fetal growth and later risk of off-spring across generations arenot understood. A fundamentalquestion relates again to therelative influence of genetictraits as opposed to factors as-sociated to the uterine environ-ment.
1.5 Life course perspectives on height
1.5.1 Short stature as a risk factorfor disease
a. Developed countries
Adult Height
As mentioned in section 2.1, evidence fromdeveloped countries has consistently shownshort adult height to be associated to a higherrisk of CHD, stroke, and probably also of adultonset diabetes. In addition, short stature hasbeen linked to a higher risk of stomach cancer,suicide, and respiratory disease (e.g.McCarronet al. 2000b; Marmot et al. 1997; Rich-Edwardset al. 1997; Njolstad et al. 1996; Davey Smith etal. 2000b; Wannameethee et al. 1998b; Jousilahtiet al. 1998, 2000; Forsén et al. 2000b).
In contrast, adult height has been found tohave a positive relationship with some diseasessuch as the sex-hormone dependent cancers(prostate, colorectal and breast cancer), possi-bly through processes involving growth factorlevels (e.g. Gunnell et al. 1998b; Davey Smith etal. 1998).
The association off short adult stature tostroke is particularly strong for haemorrhagicstroke suggesting that the relationship of heightto disease is not just disease specific but alsodiffers with respect to subtypes of disease(McCarron et al. 2001a).
Little is known about the association of adultheight to disease in eastern developed countries,such as Japan, though research is currentlyongoing (Hasegawa, personal communication).
Height in childhood
In addition to its association with short adultheight, CHD has also been found to be linked toshorter height in childhood, for example in two
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
Several strands ofexisting evidence suggestthat risk of IGT related to
fetal growth may betransmitted
intergenerationally.

24
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
historical cohorts from the UK and Finland(Gunnell et al. 1998a; Eriksson et al. 2001). Can-cer, in contrast, was found to be positively re-lated to childhood leg length (Gunnel et al.1998b).
b. Developing countries
Adult height
Very little evidence exists on the relationshipof adult stature to chronic disease in develop-ing countries. However, emerging indicationsare that the relationships may be similar to thosefound in the West.
Very recent research in Korea, for example,has found short stature to be associated with anincreased risk of haemorrhagic stroke, thoughnot with ischaemic stroke. No association how-ever has been found with CHD (of which levelsare very low in Korea), suggesting perhaps thatthe association may be dependent on the pres-ence of other factors (Davey Smith, personalcommunication).
A few other developing country studies in-vestigating the relationship of stature to bloodpressure and impaired glucose tolerance, e.g.in Brazil and Nigeria, have found some, thoughnot compelling indications of an associationwith short stature (Sichieri et al.2000; Olatun-bosun and Bella,2000).
Finally, short adult height isalso indicated to have an adverseeffect on disease risk in the nextgeneration. In India, shorterparental height was associatedwith a significantly higher riskof insulin resistance in chil-dren—especially in those children who hasthemselves grown tall, i.e. who had a highgrowth velocity (Bavdekar et al. 1999).
Childhood height
Virtually nothing is known about the relation-ship of childhood height or leg length to chronicdisease in developing countries. However, indi-rect evidence for an association comes from theearlier described observed relationship betweenchildhood stunting and risk of adiposity in sev-eral developing countries. A relationship of shortstature to risk of IGT and raised cholesterollevels was moreover found among children inJamaica (Forrester et al. 1996).
1.5.2 Secular trends in height
a. Developed countries
In industrialised countries, height has generallyshown clear secular increases over the past cen-tury. Generally these increases are thought toreflect improvements in nutrition and hygiene.
In most populations the increases in heightseem to have slowed down or even stopped inthe last decade or so. In some countries how-ever, such as in the Netherlands or the US, indi-cations are that height is continuing to increase,in the US specifically among middle class sub-jects. In Japan, height is, and has been increas-ing particularly strongly from 1975 onwards,mainly due to increases in leg length. (Evelethand Tanner, 1990)
The secular increases in height in the devel-oped world seem to be consistent with the trendsin disease that have occurred over the past dec-ades. Those diseases related to short stature—CVD, respiratory disease etc.—have showndeclines, whereas those positively associated toheight—i.e. breast, prostate and colorectal can-cer—are increasing.
b. Developing countries
The little data that exists suggests that secularincreases in height have alsooccurred in many developingcountries mainly in LatinAmerica and East Asia. As inindustrialised countries, theseincreases are attributed to eco-nomic and dietary improve-ments. In other parts of thedeveloping world however, par-ticularly in Sub-Saharan Africa,
height levels seem not to have increased, possi-bly reflecting the persisting economic and nu-tritional deprivation (Eveleth and Tanner, 1990;Davey Smith, personal communication).
1.5.3 Height as a marker ofearly life factors
The significance of the association betweenshort stature and CVD or diabetes lies in thefact that short stature in childhood and adult-hood is a marker of socio-economic (and psy-chosocial) circumstances in childhood, as wellas of fetal growth (Peck and Lundberg, 1995).In other words, the association between shortstature and disease illustrates the potential im-portance of factors acting in early life that may
In addition to itsassociation with shortadult height, CHD hasalso been found to be
linked to shorter heightin childhood.

25
affect attainment of the full genetic potentialfor adult height.
a. Short stature as a marker for earlychildhood deprivation
Most importantly short stature in childhood andadulthood, in particular short leg length, indi-cates socio-economic (or psychosocial) depriva-tion in childhood. (Peck and Lundberg, 1995).Thus, among children today, for example, slowgrowth and short stature is found most often inchildren living in long-term poverty (Miller andKorenman, 1994)
The association between shortstature and disease is thus con-sistent with the inverse associa-tion that has been found betweenearly socio-economic positionand later disease or mortality (Kuh et al. 1997; Davey Smith,1997, Dedman et al. 2001)
A marker of nutritional deprivationand infectious load
Height or leg length, much more than trunklength is thought to be an especially sensitiveindicator of childhood socioeconomic circum-stances, because of the specific effect of under-nutrition on long bone growth. (Gunnell et al.1998c). Though it may also reflect aspects suchas housing conditions, it is considered mainlyas an index of early nutritional deprivation andof infectious load. Infection in early childhood,as for example measles, slows down the rate ofgrowth in height.
If, following infection, nutrition is adequate,subsequent catch-up growth rapidly restores thechild to its normal growth curve. If the avail-able nutrition is unable to meet the high en-ergy intake needed to sustain catch-up growth,stunting occurs. (Eveleth and Tanner, 1990)Moreover, poor nutrition in general causes areduced growth in height. No conclusive evi-dence exists yet on which nutrients are of par-ticular relevance to height growth, however itis clear that more calories alone are insufficient.
A marker for psychosocial deprivation
In addition to reflecting nutrition and infectiousload, short stature is assumed to be an indicatorof psychosocial deprivation in childhood. Evi-dence has shown fairly severe psychologicalstress to cause a failure to grow among somechildren (e.g. Peck and Lundberg, 1995; Zimet
et al. 1997) and it is generally assumed that psy-chological deprivation causes a failure to grow,possibly through affecting growth hormones.
b. Fetal growth and height
In addition to being an indicator of childhoodconditions, height is also a reflection of fetalgrowth. Short stature has consistently beenshown to be related to low birth weight andheight (regardless of SEP, gender, or race). Thus,most low birth weight and length babies remainshort into adult life. (Martorell et al. 1998, 2001,
Adair, 1998, Bavdekar et al. 1999;Sørensen et al. 1999).
Moreover, evidence suggeststhat where low birth weight ba-bies grow up in good nutritionalconditions they may catch up inheight in childhood, but thismay be a reflection of earliermaturation rather than overallincrease in height. In girls it has
been observed to lead to earlier onset of me-narche (e.g. Cooper et al. 1996).
c. Genetic influences
Genetic factors undoubtedly influence earlygrowth and stature. The nature and role of possi-ble genetic determinants is not yet well under-stood, but evidence indicates that their relativeinfluence (as opposed to environmental factors)depends on the general socio-economic condi-tions in the population. As evidence suggests,the role of genetic factors in shaping differencesin height is likely to be greater, the higher andmore evenly distributed the living standards are(Silventoinen et al. 2000).
Thus, the importance of height as an indica-tor of childhood living conditions is likely to varybetween cohorts and populations, depending onthe prevailing level of ‘development’.
1.5.4 Possible factors mediatingthe association of shortstature to disease
The association between short stature and riskof disease may reflect an effect of early socio-economic conditions in childhood, of retardedfetal growth, or of short stature itself.
However, what the relative importance or roleof each of these is, or what the factors are thatmediate the association between height (or theearly exposures it is a marker for) and later dis-
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
Short stature in childhoodand adulthood is a marker
of socio-economic (andpsychosocial) circum-
stances in childhood, aswell as of fetal growth.

26
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
ease or, indeed, to disease risk in offspring arenot yet fully understood.
The involvement of several factors or proc-esses, however, is indicated by the availableevidence.
a. Short stature as a reflection of theeffects of child socioeconomic deprivation
i. Poor childhood SEP andrisk behaviours
To some extent the associationbetween short stature (as amarker for poor childhood socio-economic position) and later dis-ease may be mediated by therelationship between childhooddeprivation and higher risk behaviour discussedin the previous section. However, it is clear thatthis relationship can not fully explain the asso-ciation between short stature or child SEP to dis-ease.
ii. Childhood infections and disease
The relationship of short stature to disease maypossibly reflect the effect of exposure to infec-tious agents in early childhood.
Two specific bacterial pathogens, Helicobacterpylori and Chlamidia pneumoniae, which are as-sociated with poorer conditions, have been in-dicated to possibly play a role in causing longterm risk of CVD. C. pneumoniae, for example,has been shown to be present in atheroscleroticlesions, and there has been a preliminary suc-cessful antibiotic prevention trial. However, evi-dence so far is difficult to interpret and far fromconclusive (Leon and Ben-Shlomo, 1997;Leinonen and Saikku, 2000; Danesh et al. 1997).
A further, possibly infectious but yet uniden-tified factor may explain the particularly con-sistent association that is seen between poorchildhood SEP and haemorrhagic stroke.
iii. Nutritional stunting and risk of obesity
A possible, though probably less important wayin which short stature may, to some extent,mediate the association between early nutri-tional deprivation and later disease, especiallyin developing countries, may be through theearlier discussed higher risk of (abdominal) adi-posity associated to stunting, particularly severestunting.
b. Adverse outcomes of short stature itself
i. Short stature and adverse body function
The association of short stature to disease couldbe an outcome simply of body function. Heightcorrelates with lung function and coronary ar-tery size, and thus shorter height means reducedlung function and smaller arteries. However,
though there is still debate, grow-ing indications are that lungfunction is not involved in thelink between short height andCVD.
An important role of lungfunction, for example, is not eas-ily reconcilable with the fact thatthe association between short
stature and CHD is much stronger than that withrespiratory disease. Moreover, it is leg length(not trunk length) that is shown to be particu-larly strongly related to heart disease. Lung func-tion however, shows a greater correlation withtrunk length (Davey Smith et al. 2001a).
ii. Short stature and poor social outcomes
Short stature itself, just like obesity, has beenshown in developed countries to be associatedwith a poorer socio-economic trajectory and itmay be this that links it to disease. For exam-ple, short stature is linked with downwardsocial mobility, a higher risk of adult unemploy-ment, and lower educational achievement,which in turn are associated with higher ratesof disease (Peck, 1992; Montgomery et al.1996;Power and Matthews, 1997).
In contrast, larger height, together with be-ing healthier and of higher intelligence, has beenshown to be associated with upward socialmobility.
In addition, short stature among men is as-sociated with a reduced chance of getting mar-ried, which again is associated to poorer healthoutcomes.
In developing countries short children havebeen shown to have both lower intellectual func-tioning and work capacities (Martorell, 1995).Short stature is moreover associated with loweducational attainment.
c. Short stature as a reflection ofretarded fetal growth
The association of short stature to disease maybe an expression of the effect of retarded fetalgrowth. Since short stature correlates with lowbirth weight (as well as ponderal index and birth
Like adult obesity,obesity in childhood and
adolescence is alreadyrelated to risk of later
CHD or diabetes.

27
length), its link to disease could reflect the welldocumented and earlier discussed associationbetween intra-uterine growth retardation andlater CVD and diabetes.
However, indications are that this may notbe the case. The fact that size at birth is equallystrongly related to both leg and trunk length,but only leg length is closely linked to disease(Gunnel et al. 1999), indicates that fetal factorsmay not underlie the association between shortstature and disease. Rather, factors affectingpost-natal growth may be more important in un-derstanding the link between short stature anddisease.
d. Genetic determinants
Finally, the association between short adultheight and later disease may reflect the actionof genetic traits. However, virtually nothing isyet known about the extent or role of such agenetic influence. Evidence from some researchamong dizygotic and monozygotic twins, so far,indicates that the relationship of shorter heightto later disease may not be genetically deter-mined (e.g. Vagero and Leon, 1994). More twinstudies are required to provide more solidinsights.
e. Factors mediating the association ofadult short stature to risk of disease inoffspring
As discussed in the earlier sec-tion, the factors mediating theindicated intergenerational ef-fect of parental short stature onthe risk of insulin resistance inoffspring are not yet understoodat all, but are thought to possi-bly involve either geneticmechanisms related to the func-tion of insulin as a growth hor-mone; or to reflect intrafamilialenvironmental factors relating topoor nutrition and acting on fetal growth anddevelopment (Bavdekar et al. 1999). The ob-served association (discussed above) betweenshort maternal stature and increased risk of de-veloping GDM (which in turn is linked to ahigher risk of obesity and related disease riskin offspring), may speak to this.
1.6 Life course perspectiveson obesity in relationto CVD and diabetes
1.6.1 Obesity over the life course as arisk factor for CVD and diabetes
Obesity, in particular abdominal obesity inadults is one of the main risk factors for CHD,stroke, and diabetes (WHO, 2000).
The adverse health consequences of obesityin adults are influenced by the degree of over-weight, the location of body fat, (with higherrisk associated to abdominal fat rather than fatin thigh and hips), the magnitude of weight gainduring adulthood, and a sedentary life style(Bray, 1996)
Like adult obesity, obesity in childhood andadolescence is already related to risk of laterCHD or diabetes (Freedman et al. 1999; WHO,2000).
Evidence from the Harvard Growth Study, forexample, shows that obesity in adolescence sig-nificantly increases (2 fold) the risk of CHDdeath, independently of weight in adulthood.The risk associated to adolescent obesity is,moreover, found to be even stronger than thatassociated to obesity in adulthood (Must et a.1992).
The link of obesity in childhood to diabetesis illustrated by the fact that it has been a majorfactor underpinning the recent 10-fold rise in
the incidence of diabetes amongadolescents (Pinhas-Hamiel etal. 1996).
Social consequences of obesity
Obesity early in life may alsohave long-term indirect impactson disease, by leading to poorersocio-economic trajectorieswhich in turn are linked to anincreased risk of CVD incidenceand mortality. Data from the
Bogalusa Heart Study has shown overweight inadolescence to be associated with lower levelsof socioeconomic attainment seven years later,especially in women. The US National Longitu-dinal Survey of Youth found obesity in lateadolescence to be related to lower rates of mar-riage, fewer years of education completed, lowerfamily incomes and higher rates of poverty(Gortmaker et al. 1993).
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
Obesity early in lifemay also have long-term
indirect impacts ondisease, by leading to
poorer socio-economictrajectories which in turnare linked to an increased
risk of CVD incidenceand mortality.

28
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
Which carries a greater risk? Childhood oradult obesity?
Evidence on whether childhood or adult obes-ity is more important in developing disease isinconclusive and the relative importance ofearly vs. later obesity may be disease specific.
The Harvard Growth Study findings, for ex-ample, indicate that for CHD, earlier obesitymay be more important. In contrast, evidencefrom Finland regarding the risk of insulin re-sistance syndrome, suggests that childhoodobesity, on its own, has little effect. If persist-ing into adulthood, however, (thus causinglonger periods of insulin resistance) it has animportant enhancing effect onthe risk associated with the adultobesity (Vanhala et al. 1998).
1.6.2 Global trends inobesity
a. A note of caution
At the outset, before describingthe global trends of obesity, aword of caution is necessary.This relates to several methodological con-straints that seriously hamper the estimation ofcomparable trends and patterns on obesity.
These constraints include the dearth ofnationally representative, especially seculardata, particularly from developing countries; alack of standardisation in age groups, periodsof data collection, and measurements of obes-ity (WHO, 2000).
An additional limitation exists because BMI,the most commonly used index of obesity, doesnot adequately measure adiposity and relateddisease risk (see WHO, 2000; Guo and Chumlea,1999). BMI does not distinguish between weightassociated with muscle and with body fat; thusa given BMI may not correspond to the samedegree of fatness across populations. For exam-ple blacks tend to have a lower fat percentagethan whites. In contrast, people of South Asiandescent have a higher percentage especially ofabdominal fat for a given level of BMI (WHO,2000, McKeigue, 1996).
The estimation of obesity in childhood oradolescence is limited by an even greater lackof agreement regarding its classification andmeasurement, as well as by serious technicaland biological problems in the referencepopulations and charts used so far.
Despite these limitations, several trends andpatterns are clearly emerging.
b. A global ‘epidemic’ in obesity
A global epidemic of obesity is currentlyunderway. Obesity in both children and adultsis increasing at an alarming rate in many devel-oped and developing countries (WHO, 2000,Mokdad et al. 2001; Dietz, 2001). In the US forexample, adult obesity has increased from 12.0%in 1991 to 18.9% in 1999—a 57% increase in just8 years (Mokdad et al. 2001). Among pre-schoolchildren in the UK, obesity has increased by 70%in just 9 years from 1989 to 1998 (Bundred et al.2001). Data from the US also show importantrace/ethnic and gender differences in obesitytrends among children and adolescents, with the
temporal increases being espe-cially large among young blackgirls (NCHS, 2000).
In the developing world, obes-ity, especially in women, butalso in children, is already be-coming a serious problem inmany of the more affluent coun-tries in Latin America and theCaribbean, the Middle East andNorth Africa, though levels are
still relatively low in Sub-Saharan Africa andAsia (see WHO, 2000; Martorell et al. 2000a, b;de Onis and Bloessner, 2000). It is assumed thatas GNP and ‘westernisation’ increase, with itsattendant changes in diet and physical activity,obesity will become a problem also in the poorercountries (Martorell et al. 2000a).
The epidemic increase in obesity threatenseven higher than expected future increases inCVD and diabetes in the developing world. Inthe developed world, the rise in obesity threat-ens to undermine some of the progress that hasbeen made in reducing the rates of other riskfactors. Indeed, the growth in obesity prevalenceis seen as a main factor underpinning the re-cent slow-down in the reduction of CVD ratesin developed countries.
The reason for the recent drastic rise in obes-ity is unlikely to be related to changes in thegene pool. Rather, it is most likely a result ofenvironmental and cultural changes (in the de-veloping world termed ‘nutrition transition’)related to physical inactivity and shifts towardsa diet high in saturated fats, sugar and refinedfoods which, possibly in interaction with geneticsusceptibilities, promote the development ofobesity (see Dietz, 2001a; Popkin 1994, 2001;Martorell et al. 2000a).
A global epidemic ofobesity is currently
underway. Obesity inboth children and adults
is increasing at analarming rate in many
developed and developingcountries.

29
1.6.3 Social patterns of obesity
In both developed and developing populations,the prevalence of obesity and overweight showssome clear socio-economic and ethnic patterns.
Developed countries
In industrialised countries obesity is generallyshown to be associated with lower socio-economic position (e.g. Sobal and Stunkard,1989; Braddon et al., 1986; Power et al. 1988;Kimm et al. 1996; Greenlund et al. 1996; Croft etal. 1992).
However, such a straightforward relationshipclearly does not hold in all cases. Among manyethnic groups, for example African, Mexican orCuban Americans, no such social gradient hasbeen demonstrated (e.g. Crawford et al. 2001;Stettler et al. 2000, Maurer et al. 1985).
Racial differences moreover exist in theprevalence rates of obesity. In the US, for ex-ample, child, adolescent, and adult obesity ishigher in African Americans than it is in whiteor Hispanic Americans (e.g. Troiano et al. 1995;Flegal et al. 1998; Srinivasan et al. 2001; Kimmet al. 2001; Crawford et al. 2001).
Developing countries
The relationship between obesity and SEP es-pecially in poorer developing countries is gen-erally assumed, and in most cases found to beopposite to that in the developed world: i.e. obes-ity is higher in the more affluent, urbanpopulations (Sobel and Stunkard, 1989, Martorellet al. 2000a, 2000b, Bavdekar et al. 1999). Inricher developing countries, obesity prevalenceis higher and more equally dis-tributed in the population. Thesepatterns are assumed to reflectthe influence of increasing ur-banisation, westernisation andrising national income on lifestyles.
Urbanisation and nationaleconomic development, how-ever, do not always have thesame uniform impact on social patterns of obes-ity. Rather, the patterns vary depending on theparticular macro-structural context—the prevail-ing economic, market, social and cultural forcesthat determine, amongst others, cost and mean-ing of unhealthy diet and exercise.
For example, in many Latin American devel-oping countries, against a context of increasingincome inequality, obesity is emerging as a
serious disease specifically among the poor. Poorpeople, in these countries, simply cannot afforda ‘healthy’ diet, but must choose low cost, high-fat, high-sugar, high-calorie foods. At the sametime they have less access to the necessary re-sources, health promotion messages and scopefor systematic physical exercise (Pena andBacallao, 2000). At the same time, obesity amonghigher socioeconomic classes, for exampleamong women in Brazil, has shown some re-ductions, possibly as a result of intensive me-dia driven health promotion programmes(Monteiro et al. 2000).
1.6.4 Factors in childhood andadolescence and obesity
a. Emergence of obesity in childhood andtracking through to adulthood
Evidence from the developed world clearlyshows that obesity, and the related disease risk,already emerge in childhood. Comprehensivedeveloping country evidence on the develop-ment of obesity in childhood is virtually non-existent.
In developed countries, as the Bogalusa Heartstudy has demonstrated, obesity, especially ab-dominal obesity in childhood drives the devel-opment of high blood pressure, dyslipidaemiaand impaired glucose tolerance in children,adolescents and through to adulthood (Freed-man et al. 1999, 2001; Mahoney et al. 1991). Thehigher the rate of increase in adiposity duringchildhood and adolescence, the more adversethe changes in cardiovascular risk factor pro-files (Srinivasan et al. 2001).
Within this broad picture,however, some race and genderdifferences exist. The associa-tion of obesity to developmentof other risk factors is strongerin white than in black children,and is strongest in white boys.The weakest association is seenin black girls (Berenson et al.1991).
The presence of obesity in children is linkedto their dietary and physical activity patterns,with the recent rise in obesity being under-pinned by growing total and saturated fat, saltand sugar intake, excess calorie intake and lackof physical activity (Berenson et al. 1991, 1998b;Muller et al. 1999; Burke et al. 2001). In the US,for example, childhood obesity has been shownto be specifically related to decreased physical
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
In both developed anddeveloping populations,the prevalence of obesity
and overweight showssome clear socio-
economic and ethnicpatterns.

30
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
activity due to television viewing, as well asincreased consumption of sugar-sweeteneddrinks (Gortmaker et al. 1996, Robinson, 1999,2001; Ludwig et al. 2001).
Recent developing country evidence, e.g.from Thailand and Mexico, has similarly foundobesity in children to be linked to physicalinactivity. In Mexico, specifically TV viewingwas found to be a risk factor (Hernandez et al.1999; Mo-suwan et al. 2000).
Obesity that emerges in childhood or adoles-cence generally tracks into adulthood, with allthe associated health risks. Tracking is especiallylikely if obesity is present by late childhood oradolescence—the odds ratio is found to riselinearly with age (Guo et al. 1994; Guo andChumlea, 1999).
In fact, adolescence is a critical period fordevelopment of obesity that persists into adult-hood, especially in girls. The reasons for thisare not yet fully understood, but are thought torelate to changes in the location of body fat dur-ing puberty, with particular risk associated toearlier menarche (Dietz, 1997, Kimm et al. 2001).
A second period in early life that is indicatedto be critical in the development of obesity thatpersists into adulthood is the ‘adi-posity rebound’ (AR)—i.e. the ageat which BMI increases after itsnadir in early childhood (6–8yrs).An early adiposity rebound hasbeen shown to be associated withhigher BMI in childhood, adoles-cence, and young adulthood, anda substantially increased risk ofadult obesity (as defined by BMI)(Dietz, 1997).
The mechanisms of, reasons for, and signifi-cance of the effect of AR are still unclear (ques-tions remain, for example, regarding the extentto which the higher BMI reflects increases inbody fat), as are the determinants of an earlieradiposity rebound (Dietz, 2000).
There are conflicting findings regarding theinfluence of high protein or dietary intakes onthe timing of AR, nor has any evidence demon-strated an association with SEP. However, thereis evidence to suggest that parental obesity, aswell as exposure to maternal gestational diabe-tes in utero are associated with an earlieradiposity rebound (Dorosty et al. 2000).
b. Stunting and obesity
Increasing evidence from several developingcountries suggests that stunting, especially se-vere stunting in childhood (a result of nutritionaldeprivation) may be associated with an in-creased risk of developing obesity (high BMI)or abdominal fatness, especially in rural-urbanmigrants (Sawaya et al. 1995,1999; Popkin et al.1996, Sichieri et al. 2000; Schroeder et al. 1999;Bénéfice et al. 2000).
It s thought, though not yet fully understood,that stunting may increase people’s susceptibil-ity (in terms of weight gain) to high-fat ‘urban’diets, possibly through mechanisms related toinefficient fat oxidation (Sawaya et al. 1999;Hoffman et al. 2000).
Such an increased susceptibility is potentiallyof great concern to developing world popula-tions where malnutrition is common but coex-ists with rapid socio-economic development (i.e.ongoing nutritional transition) and urbanmigration (Schroeder et al. 1999).
c. Breast feeding and obesity
There is increasingly strong evidence from stud-ies in developed countries to suggest that
breastfeeding is associated witha lower risk of developing obes-ity (e.g. Kramer et al. 1981; vonKries et al. 2001; Gillman et al.2001). Indications are that themagnitude of this protective ef-fect may be directly related tothe length of exclusive breast-feeding; and that it does notbecome evident until after a
certain age (Dietz, 2001b).The mechanisms underpinning the appar-
ently protective effect of breastfeeding onobesity are not yet understood and there is noevidence on the long term effects of breastfeed-ing on obesity from the developing world.
1.6.5 Fetal factors and obesity
a. Interactions of obesity and IUGR andrisk of disease
In many cases, as described in previous sections,obesity (or fatness) in adults or children hasbeen found to mediate or enhance the risk ofdisease or risk factor prevalence associated withretarded fetal growth. In addition obesity hasbeen shown to interact with retarded fetalgrowth to create a particularly high risk of dis-ease.
There is increasinglystrong evidence fromstudies in developed
countries to suggest thatbreastfeeding is associated
with a lower risk ofdeveloping obesity.

31
b. IUGR and risk of obesity
In view of the apparent importance of obesityin influencing the risk of disease associated toIUGR, the question of whether IUGR enhancesthe risk of obesity itself is crucial.
The available evidence so far, however, isconflicting and difficult to interpret (Dietz, 1997;Whitaker and Dietz, 1998; Martorell et al. 2001).
Most studies in developed and developingcountries show no association between IUGR(low birth weight) and later risk of high BMI (orin one study % body fat). Instead, they find aconsistent, often linear, positive relationship ofBMI with birth weight (Martorell et al. 2001),i.e. a particularly high risk of obesity in thosewith large birth weights (macrosomic babies).
In contrast, a few studies do find a link be-tween low birth weight (or exposure to faminein early gestation) and BMI. Others, again inboth developed and developingcountries, find a relationshipbetween small size at birth andcentral adiposity (WHR orSS:TR), though only after adjust-ment for current size (Martorellet al. 2001; Bavdekar et al. 1999).Recent evidence from theALSPAC study in the UK, moreo-ver, has shown lower size atbirth to be associated to highercatch-up growth between birth and two years,and higher fatness at age five (Ong et al. 2000)
The consistent positive, often linear relation-ship between birth weight and later BMI (andthus, presumably, increased risk of disease) onthe one hand, and the association between lowbirth weight and risk of central adiposity anddisease on the other, seemingly present a para-dox.
This paradox may be explained by the inabil-ity of BMI to adequately measure adiposity.Recent evidence has shown that the larger BMIassociated with larger birth weight is due to in-crements in muscle rather than fat. Conversely,the lower BMI linked with low birth weight isassociated with lower muscularity, but a higherpercentage of body fat.
This is assumed to lead to lower expenditureof energy, a consequent higher risk of a posi-tive energy balance and development of adiposetissue, and a reduced responsiveness to insulin(insulin resistance) (Kahn et al. 2000; Hedigeret al. 1998). Thus, the lack of an associationbetween low birth weight and high BMI maydisguise an important relationship between low
birth weight and greater risk of body fat, per-haps especially central body fat. In the case ofIndian low birth weight babies such a link hasbeen demonstrated. This is mediated by the dis-tinct poor muscle-high fat phenotype of IUGRinfants that persists through the poast-natalperiod and is associated with increased centraladiposity (Yajnik, 2001).
1.6.6 Intergenerational factorsand obesity
There are clear indications that parental factorsmay have a significant impact on the risk ofobesity of their offspring.
a. Parental obesity
Growing evidence from developed countriessuggests that parental body composition, in par-
ticular parental adiposity is animportant predisposing factor forthe development of obesity inchildren (Whitaker et al. 1997;Stettler et al. 2000; Burke et al.2001; Magarey et al. 2001; Par-sons et al. 2001). One study in theUS, for example, found parentalobesity to lead to a 4-fold in-crease in the risk of obesity in
children aged 3–5 (Hediger et al. 2001). In Aus-tralia, maternal obesity was found to be associ-ated with an independent eight-fold risk ofobesity in adolescent daughters (Burke et al.2001). A further study, finally, indicates thatparental obesity may be even more importantthan large birth weight in predicting risk of obes-ity in adolescents (Frisancho, 2000). Little isknown about the effects of parental obesity indeveloping countries.
The mechansims underpinning the effect ofparental obesity are poorly understood but arethough to involve both genetic, environmental,and behavioural influences. One possiblemechanism may be through the developmentof gestational diabetes. Obese women have ahigher risk of developing GDM, and this in turnis associated with a higher risk of obesity in off-spring (Martorell et al. 2001).
b. Maternal gestational diabetes mellitus(GDM) and obesity
Evidence from developed countries clearlyshows that fetal exposure to GDM (though onlyinsulin requiring GDM), increases the off-
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
Most studies in developedand developing countries
show no associationbetween IUGR (low birthweight) and later risk of
high BMI (or in onestudy % body fat).

32
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
spring’s risk of developing obesity in childhoodand adolescence (Weintrob et al. 1996). Again,little is known about the impact of GDM in de-veloping countries.
GDM is known to lead to fetal overnutrition,hyperglycaemia, hyperinsulinaemia and thus alarge size at birth. It may thus partly explainthe consistent relationship between large birthweight and obesity (Whitaker and Dietz, 1998;Martorell et al. 2001). Moreover, GDM is indi-cated to be associated to an earlier adiposity re-bound, which as described above is clearlyassociated to a higher risk of obesity. (seeDorosty et al. 2000)
The precise mechanisms, however, by whichGDM leads to an increased obesity risk in off-spring remain poorly understood. Some evi-dence suggests that its effect is independent ofmaternal fatness but is a function of the meta-bolic intrauterine experience associated withdiabetes. Other evidence, however, throwsdoubts on the importance of the uterine envi-ronment pointing instead to the role of geneticdeterminants (Velho et al. 2000).
What leads to GDM?
As the previous sections have discussed, thedeterminants of GDM are not yet well under-stood. However, several factors have been shownto be linked to GDM, at least in somepopulations. These include obesity, own expo-sure to GDM, and short stature.
a. Maternal birth weight
Recent evidence also points toa possible intergenerational ef-fect on risk of obesity associatedwith maternal birth weight. Forexample, findings from theALSPAC birth cohort study inthe UK found that low mater-nal birth weight was associatedwith lower size at birth, height-ened post-natal catch-up growth, and subse-quently higher fatness, i.e. risk of obesity at age5 in offspring. The genetic or environmentalmechanisms underlying these associations areas yet poorly understood (Ong et al. 2000).
1.7 Life course perspectives onunhealthy lifestyles
1.7.1 Unhealthy lifestyles of the lifecourse as risk factors for disease
The lifestyle behaviours of unhealthy diet, inparticular a diet high in saturated fat, refinedfoods, salt and sugar, physical inactivity, andtobacco use are some of the most firmly estab-lished adult risk factors for obesity, high bloodpressure, dyslipidaemia and IGT and, conse-quently CHD, stroke, and diabetes in adults.They are shown to be significant at both the in-dividual and population level.
Whilst most of the evidence establishing theserisk factors so far comes from developed coun-tries, evidence demonstrating their associationto disease in developing country populations isaccumulating. The clear link of tobacco use toCVD specific and overall mortality, for exam-ple, has been demonstrated in large-scale co-hort and case-control studies in China (Liu etal. 1998; Niu et al. 1998) with similar evidenceemerging from India (e.g. Gupta and Mehta,2000).
Changes in lifestyles—especially towardsunhealthy diet (what has been termed the ‘nu-tritional transition’) in the developing world andphysical inactivity in the West—are believed tounderpin the recent alarming global rises ofobesity and related disease risk among adults
and children (Dietz, 2001a;Popkin, 1994; Fung et al. 2000).
Similarly, differences in life-styles are shown to be respon-sible for differences in riskfactor prevalence betweenmore and less ‘westernised’populations—for example,between blacks in Africa, theCaribbean and the USA(Okosun et al. 1999).
Early uptake of unhealthy lifestyles
Unhealthy lifestyles do not just emerge in adult-hood. They are already taken up in childhoodand adolescence and, as for example theBogalusa Heart Study has shown, drive the earlydevelopment of obesity, dyslipidaemia, highblood pressure, impaired glucose tolerance andassociated disease risk (Berenson et al. 1991,1998b; Yang et al. 1999; Twisk et al. 2000). In theUS, for example, much of the rise in obesity hasbeen specifically related to decreased physical
Whilst most of the evidenceestablishing these risk
factors so far comes fromdeveloped countries,
evidence demonstratingtheir association to disease
in developing countrypopulations isaccumulating.

33
activity due to television viewing (Gortmakeret al. 1996).
Unhealthy lifestyles in early life, e.g. physi-cal inactivity or smoking, have also been shownto independently predict CHD and stroke inlater life, regardless of their presence in midadulthood (Lee and Paffen-barger, 1998;Paffenbarger and William, 1967; Thorne et al.1968; Paffenbarger and Wing, 1969, 1971;Deckers et al. 1990; McCarron et al. 2001b).
In addition, unhealthy lifestyles, in particu-lar smoking, have a direct effect also on thehealth of the next generation. Smoking in preg-nancy, for example, has been shown to bestrongly linked to low birth weight, and the as-sociated morbidity and mortality risk in off-spring. Parental smoking, moreover, by exposingchildren to environmental to-bacco smoke and reducing theamount of breastfeeding, hasbeen found to increase children’sdisease risk. It specificallycauses reduced lung function-ing, asthma, and risk of infec-tions in offspring (see WHO,2001a).
Children and adolescents take up unhealthybehaviours largely as a result of massive mar-keting and media pressures which are reinforcedthrough peer pressure as well as through par-ents’ own health behaviours.
Parents’ physical inactivity, for example, hasbeen shown to be strongly linked to children’slack of physical activity and consequent obes-ity (Fogelholm et al. 1999). Likewise, unhealthyparental diet has been found to be linked to un-healthy dietary intake and overweight in chil-dren (e.g. Cutting et al. 1999; Burke et al. 2001).Parental tobacco use and quitting have an im-portant influence on the uptake of smokingespecially by younger children (see WHO,2001a,b).
Little is so far known about the processesleading to early adoption of unhealthy diet andphysical inactivity in developing countries.However, the alarming exposure of the youngto tobacco advertising and their consequent up-take of tobacco use in many developing coun-tries is beginning to be documented by theWHO/UNICEF supported Global Youth TobaccoSurvey (GYTS) (e.g. Warren et al. 2000).
1.7.2 Global trends in unhealthylife styles
As with the biological risk factors, perhaps evenmore so, quality data on trends and patterns inunhealthy lifestyles is seriously lacking—in par-ticular in the developing world. The little datathat is available from developing countries isusually from scattered, non representative sur-veys on selected populations. Nevertheless,some very broad features are discernible.
Developed world
Physical inactivity
In the developed world, indications are thatphysical inactivity is on the increase, especiallyamong the young. In the US, for example, par-
ticipation in physical activityclasses among high school stu-dents has declined over the pastdecade (YBRFSS, 2000). In lei-sure time, too, as indicatedabove, physical activity has de-clined mainly due to increasedtelevision viewing (Gortmaker etal. 1996).
Unhealthy diet
Intake of unhealthy foods, too, is showing ris-ing trends, particularly among the young.
Among 18–29 year olds in the U.S. for exam-ple, there has been a sharp increase in the con-sumption of hidden high fat foods such as pizza,French fries, burgers, Mexican and Chinese fastfood (Popkin et al. 2001). Similarly, between 1977and 1996, there has been a significant rise insnacking (high fat and high sugar snacks) among2–18 year olds (Jahns et al. 2001).
Smoking
In contrast to the adverse trends in diet andphysical activity, smoking in many developedcountries, including the US, UK, Finland andAustralia, has declined over the past decades,particularly among adults. In other countrieshowever, adverse trends are seen. These in-clude, for example, the rising prevalence ofsmoking among women in Germany or Japan,and in many countries the alarming rise insmoking among teenagers, especially girls.Whereas in the past smoking rates among girlswere always considerably lower, in several coun-tries they now exceed those of boys (HBSC, 1998,Corrao et al. 2000).
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
In the developed world,indications are that
physical inactivity is onthe increase, especially
among the young.

34
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
The most worrying trends are currently seenin Central and Eastern European countrieswhere smoking rates are rising among both menand women with prevalence rates higher than45% in some countries (Corrao et al. 2000).
Developing world
Physical inactivity
Virtually no information existson the trends in physical activ-ity patterns in the developingworld.
Diet
The scanty information that ex-ists on trends in diet suggeststhat they are unfavourable. In Asia overall therehas been a fall in the percentage of diet energyderived from complex carbohydrates and anincrease in the proportion contributed by fat(Lang, 1997). In China the percentage of house-holds consuming a relatively high fat diet hasbeen found to have increased sharply from 1989to 1993 (Peto, 1996).
Similar increases in the intake of dietary fathave been observed in Latin American Coun-tries as for example in Brazil (WHO, 1990). Vir-tually no information on diet trends is availablefrom Africa.
Smoking
The data that exists on smoking the developingworld shows very divergent trends dependingon region and country. In some regions likeSouth East Asia, Latin America, the Caribbean,and some Middle Eastern countries tobacco useis generally high and in many countries, for ex-ample China, is on the increase. In others, how-ever, such as India or Hong Kong, rates areshown to be falling (Corrao et al. 2000; Shah,personal communication). In Africa and someMiddle Eastern countries, in contrast, smokingprevalence is generally low, and in some coun-tries, for example South Africa, Ghana, Zimba-bwe or Kuwait, is falling.
A particularly worrying trend especially inmany Asian countries is the increase in the tra-ditionally low rates of tobacco use in women.In some Caribbean countries, alarmingly highrates of smoking are also seen among youth. Inthe Dominican Republic, for example, ratesstand at 35% (Corrao et al. 2000).
1.7.3 Socio-economic patterns ofunhealthy life styles
Unhealthy lifestyles are directly influenced byindividuals’ motivations and attitudes which inturn are shaped, to greater or lesser extents, byfamily, friends, peer groups, the school, andbroader social environment.
In addition, the prevalence of unhealthy life-styles shows clear variationsbetween race, gender, andsocio-economic groups, indicat-ing the important influencethat social or economic deter-minants have on the choice ofdiet, smoking and the extent ofphysical activity.
a. Patterns in developed countries
Current SEP and unhealthy lifestyles
In developed countries the prevalence of un-healthy lifestyles generally shows a clear socialgradient with higher rates in those of poorersocio-economic position.
For example, studies in many countries haveshown physical inactivity among adults andyouth to be highest in poor income or occupa-tional strata (Luepker et al. 1993; Lynch et al.,1997; NCHS, 1998; NLSCY, 2000; Brunner et al.1999). Smoking and unhealthy diets are simi-larly found to be associated to lower occupa-tional or income level (Blane et al. 1996; Brunneret al. 1999). In Finland, for example, salt con-sumption, binge drinking, total calorie and satu-rated fat intake, and little intake of fresh fruitand vegetables have all been shown to be high-est in the poorer socio-economic strata (Lynchet al. 1997).
This clustering of unhealthy behaviours inthe lower socio-economic groups is consistentwith, but does not fully explain, the observedinequalities in health and disease rates indeveloped countries (Lynch et al. 1997).
Earlier SEP and unhealthy lifestyles
At the same time as they are related to currentSEP, unhealthy lifestyles in adults in developedcountries are often also related to their earliersocio-economic position—i.e. to lower levels ofeducation and poorer background in childhood.
In Finland, for example, unhealthy diet hasbeen shown to be linked not just to adult but tolow childhood SEP (Lynch et al. 1997). Risk ofsmoking, similarly, and less successful smok-
Virtually no informationexists on the trends in
physical activity patternsin the developing world.

35
ing cessation has been linked to lower educa-tional level in many countries (Lynch, personalcommunication) (NCHS, 1995). A similar link hasbeen shown between lower education and in-creased physical inactivity (Luepker et al. 1993).
This influence of early SEP suggests that earlydisadvantage may increase risk of later diseasethrough development processes where childrenadopt particular detrimental behaviours and at-titudes.
Important variations in the influence of SEPover the life course
It is crucial to bear in mind that the impact ofearly and later SEP on risk behaviours clearlydoes not always follow the general social gradi-ents described above. Rather, different relation-ships are found in different populations and thenature and extent of associations varies depend-ing on cohort, gender, race, or the life trajecto-ries involved.
The impact of subsequent life trajectory isillustrated, for example, by the effect of child-hood SEP on physical activity in Finnish men.The risk of physical inactivity among high in-come men, was highest if they had had a lowchildhood SEP. In contrast, among low incomeadult men, a high childhood SEP conferred anincreased risk, perhaps indicating an effect ofdownward social mobility(Lynch et al. 1997; Lynch 2000).
The influence of life trajec-tory and cohort is illustrated, forexample, in the effects of childand adult SEP on smoking in theAlameda County cohort in theU.S. In 1965, the greatest cumu-lative life course disadvantagewith respect to smoking was inadults in high income stratawhose fathers had been manualworkers, i.e. who had moved up-wards. In 1994, by contrast, the highest cumu-lative risk was in those who came from lowoccupational class origins and had remained ina low income strata as adults (Davey Smith etal. 2001b).
Cohort differences are also illustrated in theimpact of family income on ‘snacking’ in youngUS adults. Whereas in 1977, low income familybackground was protective of snacking among18–29 year olds, in 1994–1996 it no longer hadsuch a protective effect, with little differentia-tion between low and high income strata (Zizza
et al. 2001). A similar pattern was found in arecent child cohort in the UK where less healthyfood choices—convenience, snack and fingerfoods—were found in children with less edu-cated mothers, but also in children from sociallyadvantaged backgrounds (North et al. 2000).
Finally, cohort and gender differences aredemonstrated, for example, in the impact ofeducational level on smoking in Switzerland.Among older cohorts of women, higher levelsof education were associated with a higher riskof starting smoking early, whereas among menhigher education had no effect. In contrast,among younger cohorts, higher education inmen had come to be protective of starting smok-ing early, whereas among women it no longerhad an effect (Curtin et al. 1997). A similarswitch in the effect of higher socio-economic oreducational level has been observed in Spainaround 1988/92 (Borras et al. 2000).
These variations indicate the crucial impor-tance of the prevailing historical, social, eco-nomic and cultural context in shaping the effectthat lifecourse SEP, race/ethnicity, or gender (orethnic group) may have on risk behaviours.
b. Patterns in developing countries
The social gradient of unhealthy lifestyles indeveloping countries, just as that of the biologi-
cal risk factors, is generally as-sumed to be opposite to that indeveloped countries, i.e. un-healthy diet, physical inactivityand smoking are assumed to behigher in the more affluent,‘westernised’ urban populations.
The available evidence sug-gests that this urban-rural andSEP gradient often holds. InChina, for example, tobacco use,fat and meat intake, as well asreduced vegetable intake and
physical inactivity has been found to be associ-ated with higher income level and urban resi-dence (Popkin et al. 1995; Peto, 1996; Paeratakulet al. 1998; Gao et al. 1999; Yu et al. 2000).
Evidence from Latin America, similarly, sug-gests that physical activity and energy expendi-ture is much higher in rural than in urban areas(Torun, 2000). However, the evidence alsoclearly indicates that in many cases the patternsof risk behaviours do not follow this classicalpattern. In Brazil, for example, the intake of ahigh-fat, high-sugar diet is particularly high
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
At the same time as theyare related to current SEP,
unhealthy lifestyles inadults in developed
countries are often alsorelated to their earlier
socio-economic position—i.e. to lower levels ofeducation and poorer
background in childhood.
36
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
among the poor population, who simply can notafford a healthier diet, especially in cities (Penaand Bacallao, 2000).
Similarly, smoking in urban China has beenfound to be highest in the lower socio-economicgroups, in particular the lowest educationalgroups (Yu et al. 2000). Finally in India, con-trary to assumptions, smoking rates among mostage groups have been found to be much higherin rural than in urban areas (Shah, personal com-munication).
These variations indicate that in the devel-oping world, too, the impact of SEP on healthbehaviours is shaped by the prevailing socio-economic or cultural context, and that ‘urbani-sation’ or ‘westernisation’ cannot simply beassumed to have uniform impacts on diseaserisk patterns.
1.7.4 Importance of the macro-structural context
The significant population, gender, and cohortvariations in the relationship between early andlater SEP and unhealthy lifestyles in developedand developing countries have highlighted thecrucial importance of the prevailing macro-structural context—i.e. the main social, eco-nomic, cultural and political forces—in shapingthe social determinants and trends in risk be-haviour.
It is the macro-context that determines theresources available to different groups; the re-sources necessary for opting forhealthy (or unhealthy) lifestyles;the exposure to risk factors, andthe social meaning that risk be-haviours (for example smoking)have for different populationgroups.
Specific forces that are of par-ticular importance in this regard include:
i. The macroeconomic and political factors thatdetermine level of income, poverty and in-come inequality
ii. Legislation, such as anti-smoking laws orfiscal policies, which have been shown to suc-cessfully curb smoking in several developed,but also in some developing countries, e.g.in South Africa (Corrao et al. 2000)
iii.The extent of advertising, for example of un-healthy as opposed to healthy foods
iv. The level of influence, market control andexpansion of the fast food industry (Schlosser,2001).
1.8 Potential mechansimsunderpinning the association ofintrauterine growth retardationto later disease risk
1.8.1 Introduction
The previous sections have illustrated the evi-dently important associations that exist, in manypopulations, between intrauterine growth retar-dation (small size at birth or exposure to fam-ine in utero) and risk of adult disease or riskfactor prevalence.
This section aims to explore in some detailwhat is known about the mechanisms under-pinning these associations.
A first point to emphasize at the outset is thatthese mechanisms are still extremely poorlyunderstood, with research only at the beginning.
A second point is that the development of abetter understanding of the mechanisms has,to some degree, been hampered by the limita-tions in the currently used measures of fetalgrowth retardation. Low birth weight, as theprevious sections have indicated, is too crude amarker to capture the range of possible uterineexposures and experiences that may relate todisease risk.
At the same time, the somewhat haphazarduse of several other measures ofsize at birth, e.g. head circum-ference or length at birth, haslimited the comparability andinterpretation of findings (seeKramer and Joseph, 1996).
Efforts to develop and system-atically use more specific meas-
ures of important exposures in utero are thus akey requisite for developing a better understand-ing of the mechanisms that link fetal growth tolater disease.
The remainder of this section considers themain unresolved issues and questions regard-ing these mechansims.
1.8.2 Main unresolved issues
a. Underlying determinants—geneticor environmental?
A fundamental unresolved question pertains tothe relative role of genetic versus environmen-
However in many casesthe patterns of risk
behaviours do not followthis classical pattern.

37
tal factors in underpinning the associationbetween IUGR and later disease risk. In otherwords, is the association due to an environmen-tal exposure in utero, or due to a genetic traitwhich causes changes that leadto disease risk and at the sametime to retarded fetal growth?
Evidence from existing stud-ies, including twin studies—which are generally though to bethe best equipped to answerquestions relating to the relativeimportance of genetic versus en-vironmental factors—providesinconclusive evidence, pointingat times to a dominant role of en-vironmental, at other times to genetic traits asthe determinants. Evidence from twin studies,moreover, is partly limited by difficulties in as-signing birth weights. Furthermore, there aremore fundamental questions as to the extent towhich conclusions can be drawn from differ-ences in disease concordance between mono-and dizygotic twin pairs (e.g. Phillips, 1993).
What seems clear is that the interaction ofboth genetic and environmental factors is in-volved and that the relative importance of oneor the other may also vary depending on theparticular disease risk concerned. For example,a specific hypothesis has been advanced (thoughonly very weak supporting evidence exists) toindicate a possible genetic determinant of theassociation between retarded fetal growth andimpaired glucose tolerance.
b. The nature of intergenerationaltransmission
Related to the issue regarding the relative roleof genetic versus environmental determinants,is the question of the nature and basis of theapparent intergenerational effects on risk trans-mission associated with fetal growth. Particularquestions in this respect relate to the possiblerole of maternal gestational diabetes or of pa-rental height, weight, and nutritional history,sub-clinical pathology, and the specific mecha-nisms by which parental obesity leads to obes-ity in offspring.
c. The fixedness of early programming
A further question relates to the extent to whichearly ‘programming’ of disease risk is fixed or ismodifiable by later interventions. The markedsuccess of several high risk life style interven-
tions in reducing risk of diabetes and CVD inmiddle aged individuals, combined with thelarge secular changes in major risk factors forCVD (smoking, unhealthy diet, hypertension)
suggests that, perhaps, program-ming of risk is more flexible thanpreviously assumed. For exam-ple, a recent randomized con-trolled trial in Finland showedthat weight reduction and im-provement of diet led to a 58%reduction in diabetes over 3.2years of follow up (Tuomilehtoet al. 2001).
d. Which possible exposureslead to detrimental fetal growth? What isthe role of maternal nutrition in this?
A fourth area that remains poorly understoodconcerns the possible environmental exposuresin utero that may cause retarded fetal growth oradaptations that lead to later risk of disease.
It is commonly assumed that such adapta-tions and retarded fetal growth occur in situa-tions in which the fetus’ nutrient demand ishigher than the placental supply. The resultingundernutrition leads to hypoxaemia which inturn leads to changes in blood distribution,placentation, metabolic and endocrine changes.
However, it is not yet known which exposuresor factors cause such detrimental fetal growthor development. Particular questions regard therole that maternal nutrition plays in this. It isbecoming increasingly clear that maternal nu-trition is not necessarily the same as fetal nu-trition (Harding, 2001). For example, maternalnutritional supplementation interventions havebeen shown to have very little effect on off-spring’s birth weight (e.g. Kramer, 1987). It isthus assumed that other, non-nutritional factorsrelating to fetal nutrition or placental function-ing may be of importance.
e. What is the importance of timing ofinsults during pregnancy?
A further unresolved question relates to thepossible importance of the timing of insults inutero for subsequent risk of disease. That tim-ing may be important has been indicated by thefindings of the Dutch Famine Study which hasshown that exposures in early and later gesta-tion can have very different effects. These dif-ference may, moreover, depend on theparticular disease concerned.
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
Efforts to develop andsystematically use more
specific measures ofimportant exposures in
utero are thus a keyrequisite for developing abetter understanding of
the mechanisms that linkfetal growth to later
disease.

38
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
f. Which adaptations may occur in uteroin response to stress?
It is assumed, for example by the fetal originsof disease hypothesis, that exposure to stress orundernutrition in utero leads to endocrine andmetabolic adaptations or processes that thenlead to development of later disease risk.
Although the particular metabolic and endo-crine processes are not yet understood, severalpossible processes that may be involved havebeen suggested.
i. Elastin
The laying down of elastin, avital component for the elastic-ity of arterial walls, occurs onlyonce, early in life. Its half life of30 to 40 years means that by mid-life, half of the elastin in bloodvessels has disappeared, thusrendering them less elastic. Proc-esses in utero which restrict the laying down ofelastin could potentially increase the risk of car-diovascular disease later in life (e.g.Martyn andGreenwald 1997).
ii. Programmable hormonal systems
There is some evidence to show that severalhormonal systems may be programmable inutero and could thus potentially be involved inthe mechanisms leading to enhanced risk oflater disease. These include:
— Adrenocortical Steroids (e.g. Cortisol)— The Sympathoadrenal System— GH/IGF-1 Axis— Pituitary-Thyroid Axis— Gonadal Steroids— Insulin Secretion
Programming of the HPA axis (i.e. the sys-tem of adrenocortical steroids (cortisol)), inparticular, is indicated to possibly play an im-portant role. Evidence from human and animalstudies shows that low birth weight is associ-ated with higher cortisol levels, and that stress-ful experiences such as deprivation in utero canact to prime the HPA system in such a way as toincrease the magnitude of subsequent responsesto stress and adverse circumstances later in life.In other words, the degree of adult responsive-ness (cortisol levels secreted) to stresses in adultlife (e.g low socioeconomic position, job con-trol, self-esteem, or social support) may be de-termined by events in utero. At the same time,
evidence from physiological studies shows in-creased stress response to be associated withatherosclerosis and increased left ventricularmass, and in follow up to predict hypertension.Cross-sectional and case-control study datafurthermore shows higher levels of cortisol,especially in conjunction with obesity, to be as-sociated to higher blood pressure, IGT and IR,and dyslipidaemia. However, no link of elevatedstress response to CVD or diabetes has yet been
demonstrated (e.g. Sapolsky,1996; Brunner, 1997; Phillips,1999; Reynolds et al.2000,Bjorntorp, 1997), though someprospective evidence exists fora link between CVD and psycho-social factors such as anxiety ordepression (which may involveheightened stress responses)(e.g. Hemingway and Marmot,1999). The particularly adverse
effect of stress in conjunction with obesity maybe of importance in terms of the apparent me-diating effect of obesity on the risk of diseaseassociated to retarded fetal growth.
A role of a raised stress response in liftingthe risk of CVD may be of particular significancefor developing countries where people frompoor origins (i.e. likely to have been exposed toundernutrition in utero) increasingly move tostressful urban environments.
g. Which mechanisms underlie theobserved mediating effect of enhancedgrowth in weight?
The mechanisms underlying the apparent in-teraction between retarded fetal growth and in-creased post-natal growth in weight or fatnessin increasing disease risk, are just as little un-derstood as the association between IUGR andlater disease risk in general.
A first question pertains to the timing of en-hanced growth in weight. Is such growth onlydetrimental if it occurs in a certain period orstage of childhood? Existing evidence is not yetable to give solid insights to this.
A second questions concerns the physiologi-cal mechanisms that may underpin the in-creased risk of disease associated with retardedfetal growth followed by rapid growth in weight.These mechanisms, which are likely to differdepending on the particular outcome con-cerned, again are not understood. However, apotential process, at least relating to increasedrisk of insulin resistance, has been proposed.
The risk of developingCHD, stroke or diabetes isinfluenced by biologicalor social factors acting at
all stages of the lifecourse—in fetal life,
childhood, adolescence,and adulthood.

39
This builds on the increasing evidence thatbabies who are small or thin at birth have rela-tively less muscle compared to those of normalor high birth weight (Kahn et al.2000; Hedigeret al.1998)—a phenotype shown to be particu-larly marked in Indian IUGR babies (Fall et al.1999; Kinare et al. 2000)—and evidence that thisdeficiency persists after birth. The critical pe-riod for muscle growth is around 30 weeks inutero; there is little cell replication thereafterand later muscle cell hypertrophy may be in-sufficient to compensate for this deficiency(Widdowson et al. 1972; Bassey et al. forthcom-ing).
The idea is that if IUGR babies develop a highbody mass index in childhood they may have adisproportionately high fat mass, as low mus-cle means less energy expenditure, more likeli-hood of achieving a positive energy balance, andthus increased rate of adipose tissue gain. Highfat mass (and low muscle mass), in turn, willlead to an increased risk of development of in-sulin resistance, as lower muscle mass may alsoresult in lower overall muscle responsivenessto a given insulin signal (Kahn et al. 2000). InIndian IUGR babies, the marked thin-fatphenotype has been shown to persist throughthe post-natal period and to be associated inparticular with high central adiposity (Yajnik,2001).
h. Which mechansims underpin theobserved mediating effect of enhancedgrowth in height?
As is the case for growth in weight, the mech-ansims underpinning the apparent effect ofenhanced growth in height in childhood oradolescence on risk of disease are poorly un-derstood.
A potential mechanism thathas been proposed is that slowgrowth in utero resulting in shortlength at birth may involve a per-manently reduced number ofcells for example in the kidney,with no further cell replicationafter birth. Post-natal catch-up could be delete-rious either because overgrowth disrupts cellfunction, or because large body size imposes ex-cessive metabolic demand which in case of thekidney may lead to cycles of nephron death andthus increased blood pressure (e.g Eriksson etal. 2000; Forsén et al.1999; Lever andHarrap,1992).
1.9 Key themes and key gapsin knowledge
1.9.1 Introduction
The previous sections in this part of the reporthave sought to set out the evidence on the in-fluence of life course impacts on risk of CHD,stroke and diabetes. The discussions have shownthe complexity in trying to disentangle the vari-ous life course influences that shape the risk ofCVD and diabetes later on. They have high-lighted, in particular, the limitations imposedby the serious lack of evidence from develop-ing countries.
However, the discussions have also shownthat much knowledge has already accumulated,and we are some way (though still at the begin-ning) towards understanding how factorsthroughout the life course impact on later dis-ease risk.
The aim of this final section of Part I is firstto draw together the major strands—the mainthemes and issues—emerging from the previ-ous individual domain discussions and, in do-ing so, to pinpoint the important gaps inknowledge that remain and that need to be ad-dressed by research.
1.9.2 Key general points
Three general, but extremely important issuesregarding the use of the life course perspectivefor policy, warrant re-emphasis at the outset.
a. Risk of disease is influenced by factorsat all stages of the life course
The risk of developing CHD, stroke or diabetesis influenced by biological or social factors act-
ing at all stages of the lifecourse—in fetal life, childhood,adolescence, and adulthood.
Life time risk, however, can-not simply be understood as anadditive model: Earlier and laterfactors are likely to interact, andthe consequences of some influ-
ences may depend on events at earlier (or later)critical stages of development. For example,negative consequences of fetal growth retarda-tion appear especially in conjunction with highpost-natal weight gains. The relative importanceof early and later factors in causing later dis-ease, however, is not yet fully understood.
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
Life course impacts ondisease cannot simply
be generalised from onepopulation to the next.

40
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
b. Life course influences aredisease specific
CHD, stroke and diabetes are likely not theresults of the same processes and exposuresacting over the life course. The life course in-fluences on risk are specific for each disease, oreven subtype of disease—as, for example, forhaemorrhagic and ischaemic stroke—thus pos-ing important challenges for research and forintegrated policy development.
c. Life course impacts on disease arepopulation (and cohort) specific
Life course impacts on diseasecannot simply be generalizedfrom one population to the next,or from one cohort to the next.Important differences appear toexist, reflecting either geneticdifferences and/or differingsocial, economic, cultural andnutritional contexts, and differ-ences in the manner of gene ex-pression across a variety ofenvironmental conditions.What determines population orcohort differences, particularly what the rela-tive role is of different social contexts, is notwell understood, but is a key area for future re-search.
1.9.3 Disease and ‘established’ riskfactors over the life course
a. ‘Known’ risk factors remain the mostfirmly established link to disease
The risk behaviours of unhealthy diet, lack ofexercise, and tobacco use, and the associatedbiological risk factors of high blood pressure,obesity and dyslipidaemia, remain the mostfirmly established risk factors for CHD, strokeand diabetes.
Efforts to disentangle the life course impactson- and effects of these risk factors, especiallyin developing countries, are seriously hamperedby the dearth of, and methodological limitationsin the existing studies on their prevalence andsocial patterning and trends. The latter includethe inability of body mass index (BMI), as themost commonly used index of obesity, to ad-equately distinguish between lean and fat tis-sue; the methodological difficulties of accuratelyidentifying hypertension; and the lack of appro-priate population norms for both blood pressureand adiposity.
Nevertheless, several key issues can be iden-tified.
b. Rising risk factor trends: obesityand tobacco use
The little evidence that exists shows that in thedeveloping world, the prevalence of the majorrisk factors obesity and tobacco use is rising.
In developed and developing populations theprevalence of obesity among both adults andchildren has shown sharp increases, somewhatoff-setting the progress made with some of theother biological risk factors in many countries.
The rise in obesity particularly,is a reflection of the increasedmarketing and availability of awesternised diet rich in refinedfoods, saturated fats, sugar andsalt (‘nutritional transition’), aswell as changes in lifestylestowards decreased physicalactivity.
Tobacco use, though declin-ing in some, mainly developedcountry populations, is showingalarming rates or increases in
others. A particularly worrying trend is themarked rise in smoking amongst women andteenagers in many developing and developedcountries.
c. Major biological risk factors emergeand act in early life
Contrary to what was long assumed, high bloodpressure, dyslipidaemia, impaired glucose tol-erance (IGT), and obesity already emerge inchildhood and adolescence, and are often clus-tered together. Obesity, especially abdominaladiposity, seems to play a central role in thedevelopment of the other factors, although somerace and gender differences in the clustering ofrisk factors do appear to exist.
Three critical periods or exposures in earlylife appear to increase the risk of developingobesity that persists into adulthood: 1) exposureto gestational maternal diabetes and high birthweight; 2) an early adiposity rebound (the ageat which BMI increases after its nadir in earlychildhood), and 3) development of obesity inadolescence. The mechanisms underpinningthese apparent associations are not yet under-stood.
The presence of risk factors early in life al-ready influences risk of later disease, either
The risk behaviours ofunhealthy diet, lack of
exercise, and tobacco use,and the associated
biological risk factors ofhigh blood pressure,
obesity and dyslipidaemia,remain the most firmly
established risk factors forCHD, stroke and diabetes.

41
through the social and biological tracking ofthese behaviours over time, and /or throughtheir direct biological effects. Obesity, high bloodpressure and dyslipidaemia track from child-hood through to adolescence and young adult-hood, where they lead to atherosclerosis and,in many cases, diabetes. The presence of riskfactors in adolescence or young adulthood (e.g.high blood pressure) has additionally beenshown to independently predict an increasedrisk of CVD later on.
The relative predictive power of risk factorspresent in childhood, compared to risk factorsin mid-life will depend on the disease con-cerned. In many cases, however, it is indicatedto be equal, if not stronger, than that of riskfactor presence in mid-adulthood.
What is not yet understood, for example inthe case of blood pressure, is the relative im-portance of long-term exposures to raised lev-els as opposed to acute high transient levels. Inthe case of obesity and insulin resistance syn-drome it appears that long-term exposure toobesity has an aggravating effect.
Risk factors in early life, particularly tobaccouse and obesity, moreover, not only affect one’sown later health but also the health of the nextgeneration.
Obesity, especially in mothers, for example,clearly increases the risk of obesity and, conse-quently, disease risk in their offspring.
Similarly, tobacco use during pregnancy isstrongly linked to low birthweight and associated diseaseor mortality risk in the off-spring. Parental smoking,moreover, exposes children toenvironmental tobacco smoke(ETS), and thus an increasedrisk of asthma, certain infec-tions and reduced lung func-tioning.
1.9.4 Disease and unhealthy lifestylesover the life course
a. Unhealthy lifestyles drive theemergence of disease risk in early life
Unhealthy lifestyles—tobacco use, physical in-activity and unhealthy diet (a diet high in sugar,saturated fat, salt and calorie content)—arealready taken up by children, leading to theearly development of obesity, high blood pres-sure, dyslipidaemia, IGT and the associated dis-ease risk. In addition, unhealthy lifestyles in early
life, for example physical inactivity, are shownto independently predict later CVD—regardlessof their presence in mid or late adulthood.
Unhealthy lifestyles are taken up by childrenor adolescents largely as a result of massivemarketing and media pressures, as well as par-ents’ own health behaviours. Parents’ lifestyles,for example, have an important impact onchildren’s dietary habits, level of physical activ-ity, and uptake of tobacco use.
b. Socioeconomic position over the lifecourse influences risk factor development
The prevalence of behavioural or biological riskfactors is clearly influenced by socio-economicposition (SEP) over the life course. In adults,for example, the prevalence of risk factors is notjust determined by adult SEP, but also by theirsocioeconomic position in childhood and the dif-ferent social trajectories that individuals traverseas they become educated, enter the labour mar-ket, generate income, change jobs, and gatherassets.
In developed countries, prevalence of riskbehaviours and factors among adults, just asprevalence of disease, is generally higher amongthose from lower socio-economic strata. Simi-larly, it is typically poorer childhood SEP that isassociated with more risk behaviour, suggest-ing that early socio-economic disadvantage mayincrease later disease risk through developmen-tal processes whereby children adopt particu-
lar detrimental behaviours andattitudes.
Poor early SEP can also haveintergenerational effects on dis-ease risk. Among young femalesin Japan, for example, raising SEPthrough education has beenshown to not only decrease theirown risk of disease, but also thatof their offspring in the next gen-
eration. (Hasegawa, personal communication).The general developed country pattern of low
SEP=high risk, however, clearly does not holdin all cases. The effect, detrimental or protec-tive, of SEP on risk behaviours can differ con-siderably between populations, ethnic groups,cohorts and genders. For example, among olderwomen cohorts, low early SEP was shown toprotect against smoking, whereas amongyounger cohorts at present it is associated withan increased risk.
In developing countries the social gradientof disease risk is commonly assumed, and
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
Risk factors in early life,particularly tobacco use
and obesity, moreover, notonly affect one’s own laterhealth but also the health
of the next generation.
42
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
often found to be opposite to that in developedcountries. Risk factors are often highest in thosepopulation groups that are the most western-ised or modern—i.e. the affluent, urban popu-lation. However, the patterns of risk are at timesmore complex and do not follow this uniformpattern. Obesity, for example, is emerging as aserious problem among the poor in LatinAmerica. In India, smoking rates are found tobe higher in rural than in urban areas.
c. Importance of the macro-structuralcontext
The specific socio-economicand rural-urban risk factor pat-terns that prevail in differentpopulations are shaped, to alarge degree, by the underlyingmacro-structural context—theprevailing social, economic, po-litical and cultural forces. Theseforces determine the exposureto risk inducing environments,the resources necessary and available to opt forhealthy lifestyles, and the social meaning thatrisk behaviours have for different populationgroups.
For the developing world in particular, thismeans that the processes by which ‘urbanisa-tion’ and ‘development’ lead to increased riskcannot simply be assumed to be the same acrossdifferent societies.
d. Additional influence of poorchildhood SEP
The relationship of poor early SEP to risk fac-tors or behaviours only partly explains its asso-ciation to later disease. The clear link of lowerearly SEP to CHD and stroke, which is reflectedin the consistent association shown betweenshort stature (i.e. impaired linear growth) andthese diseases, is possibly mediated by two otherfactors.
Infectious factors
A first factor thought to possibly underpin theassociation of poor childhood SEP to CVD isearly exposure to infectious agents. The specificbacterial pathogens that appear linked to poorconditions and have so far been implicated in-clude Helicobacter pylori and Chlamidiapneumoniae, though evidence is far from con-clusive.
A further, possibly infectious but yet uniden-tified factor is assumed to underpin the particu-larly consistent association that is seen betweenpoor childhood SEP and haemorrhagic stroke.
The possible role of other infectious agentsin the development of chronic disease risk,especially in developing countries where infec-tious disease is still pervasive, has not yet beenexplored.
Nutritional factors
A further indirect way in which childhood dep-rivation, especially nutritional deprivation, may
be associated to a raised diseaserisk, is through the apparent as-sociation between stunting(especially severe stunting) andan increased risk of (abdomi-nal) adiposity. This associationis possibly due to impaired fatoxidation in stunted childrenand a consequent increased sus-ceptibility (in terms of weight
gain) to high fat ‘urban’ diets.A link between stunting and risk of central
adiposity would be of particular importance inthose developing countries who have recentlyor are currently undergoing the ‘nutrition tran-sition.
1.9.5 Disease risk and protectivefactors in childhood
a. Breastfeeding
In contrast to the detrimental effects of un-healthy diet and lack of exercise in childhood,breastfeeding is indicated to have a protectiveeffect on the development of disease risk.
Apart from its well-established short termbenefits for child health and development,breastfeeding is increasingly indicated to con-fer a lower risk of high blood pressure, as wellas of dyslipidaemia and obesity. However, thisprotective effect is not yet unequivocally estab-lished, as some weak evidence of a long-termnegative impact of breastfeeding on CVD riskexists.
1.9.6 Disease, risk factors andfetal growth
In addition to factors in childhood and adoles-cence, factors relating to fetal growth are clearlyinvolved in shaping risk of disease.
The processes by which‘urbanisation’ and
‘development’ lead toincreased risk cannot
simply be assumed to bethe same across different
societies.

43
a. Fetal growth and later disease
In many populations intrauterine growth retar-dation (IUGR) (as indexed by small size at birthor exposure to famine in gestation) is shown tobe associated with a higher risk of CHD, strokeand diabetes. This association forms the basisof the ‘Barker’ or the ‘Fetal Origins of AdultDisease’(FOAD) hypothesis. Some evidence sug-gests moreover that this risk may be transmit-ted intergenerationally.
At the same time, however, large size at birth,too, is found to be linked to an increased risk ofdiabetes or CVD. Thus, the relationship of fetalgrowth to later disease is, in fact, U-shaped. Thiseffect of fetal overnutrition is important to bearin mind, particularly in view of the currentprominence of the FOAD hypothesis.
b. Fetal growth, blood pressure,dyslipidaemias and impaired glucosetolerance (IGT)
In addition to its link to adult disease, IUGR isclearly found, in both adults and children, to beassociated to a higher risk of high blood pres-sure and impaired glucose tolerance. Its asso-ciation to the most important dyslipidaemias(i.e. high triglyceride and low HDL-c levels) isless clear cut.
At least in a statistical sense, the associationof IUGR to these biological risk factors does notappear to mediate its link to CVD, though thismay reflect the limitations of available data. Inthe case of diabetes, a mediating effect of theassociation to IGT seems more indicated.
c. Population and cohort differences:importance of the post-natal context
Though associations between IUGR and diseaserisk are found in most populations studied, someevidence shows conflicting results, indicatingthe existence of important population and co-hort differences in the relationship of fetalgrowth to later disease. Examples include theapparent lack of an association between smallsize at birth and diabetes in Indians; the absenceof a relationship between IUGR and blood pres-sure in some black populations; and the diver-gent relationship between IUGR and impairedglucose tolerance in children and adults inIndia.
These population and cohort differences mayreflect underlying genetic differences, expres-sion of genes, and/or the impact of divergentpost-natal contexts and environments. The
latter may reflect differences in a particularpopulations’ stage of the epidemiological or nu-tritional transition or, between cohorts of thesame population, the result of rapid social andeconomic change.
d. Interaction between IUGR and laterweight or height gained: importance ofpost-natal nutrition
Increasing evidence indicates the associationbetween IUGR and later disease risk is some-how mediated or enhanced by the rate of growthin weight or height in childhood or adolescence.
The apparent role of growth in weight orheight is indicated by three factors:
— in most cases significant associations be-tween low size at birth and later diseaserisk factor are only found after adjustmentfor current weight
— in many cases the association betweenlow birth weight and disease risk is strong-est in those with highest BMI or fatness
— in some studies the association betweenIUGR and disease risk is shown to be high-est in individuals who have had acceler-ated growth in height to become tall.
It is not yet clear how this apparent effect ofpost-natally gained weight or height is to beinterpreted, but four (not mutually exclusive)interpretations are possible:
i. It represents a negative effect of enhancedgrowth in childhood or adolescence per se.In other words, accelerated growth in weight(or height) itself could have negative conse-quences.
ii. It is the difference in size between birth andthe later stage that better defines detrimen-tal impaired early growth: the higher the dif-ference, the higher the risk (see e.g. Lucas etal. 1999).
iii.Obesity reveals/activates an underlying sus-ceptibility induced by impaired early growthand, vice versa, low birth weight enhancesthe risk associated to obesity, i.e. obesity isparticularly harmful in those with earlygrowth retardation.
iv. The effect of enhanced growth in height inIUGR babies may reflect a failure of the fetusto realise its genetic growth potential in utero,possibly due to placental failure. It may bethis insult on fetal growth that underlies the
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
44
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
increased risk of disease (e.g. Leon et al.1996).
Whilst the particular interpretation maydepend on the specific disease or risk factor con-cerned, they all indicate the importance of anadequate post-natal nutritional environment inbringing to the fore a risk associated with fetalgrowth retardation.
Further evidence for this comes from the dis-crepant findings of the two existing famine stud-ies. Whereas an associations between exposureto famine and later disease risk were found inthe Dutch famine, which was followed by aperiod of adequate nutritional supply, no asso-ciation was found in the Russian famine, whichwas followed by a long period of inadequate nu-tritional supply. Another indication of the im-portance of the post-natal nutritional context arethe marked rural-urban differences in CVD anddiabetes risk, for example in India. While lowbirth weight is more common in rural areas,disease risk is much higher in the nutritionallymore adequate urban areas (e.g. Yajnik, 2000).
e. IUGR and increased risk of obesity—a paradox?
The crucial question of whether IUGR also en-hances the risk of obesity in a nutritionally richpost-natal environment (i.e. the thrifty pheno-type hypothesis) is still unresolved.
The available evidence is inconclusive andpresents a paradox by consistently showing apositive, often linear, relationship between birthweight and obesity (BMI) which is difficult toreconcile with the association between low birthweight and higher risk of disease.
A possible explanation of this paradox maylie in the inadequacy of BMI to adequately meas-ure fatness, thus disguising a possibly impor-tant relationship between low birth weight andgreater risk especially of central body fat.
f. Mechanisms underpinningthe association of fetalgrowth to disease risk
The mechanisms and processesunderpinning the association be-tween retarded fetal growth andlater disease risk remain poorlyunderstood.
The generation of a greaterunderstanding has, amongst oth-ers, been hampered by the somewhat haphaz-ard use of multiple measures of birth size, and
by the limitations of low birth weight (the cur-rently most commonly used index of fetalgrowth retardation) as an adequate marker tocapture the range of possibly important expo-sures or birth outcomes.
The main unresolved issues include the fol-lowing:
• the relative role of environmental versusgenetic exposures
• the nature and role of intergenerationaltransmission of risk, including the role ofmaternal gestational diabetes, and paren-tal body size and nutritional history
• the nature of the exposures that may leadto detrimental fetal growth retardation inparticular the role of maternal nutrition inthis
• the potential importance of the timing ofinsults in utero
• the potential endocrine, metabolic andhaemodynamic adaptations that may oc-cur in the fetus in response to insults, inparticular the population relevance of theapparently important adaptations in thecortisol stress response system.
• the nature and significance of the appar-ent mediating effect of rapid post-natalweight and height gain, including the ques-tions as to why catch-up growth is detri-mental? and whether it has to occur in aspecific period to be detrimental?
1.9.7 Importance of fetal vs. post-natalfactors for population trends indisease
a. A greater importance ofpost-natal factors
The clear association of both fetal and of post-natal factors (incl. the classicalestablished risk factors) to risk ofCHD, stroke and diabetes raisesthe crucial question as to the rela-tive importance of fetal vs. laterfactors in determining popula-tion patterns and trends in dis-ease.
The evidence so far points toa limited role of fetal factors. Se-
rious doubts exist concerning the causality oftheir association to disease, and indications arethat their population attributable risk is small.
The mechanisms andprocesses underpinningthe association between
retarded fetal growthand later disease risk
remain poorlyunderstood.

45
The rapid increases as well as the social pat-terns of risk factors, CVD, and diabetes in de-veloping countries are clearly not explained bychanges in fetal growth. Impaired fetal growth(low birth weight) has been pervasive for a longtime whereas the epidemic in CVD and diabe-tes are a recent occurrence. In most countries,moreover, disease rates are much higher in ur-ban areas although birth weights are much lowerin rural areas.
The temporal trends and patterns of risk fac-tors and disease in populations thus seemlargely related to changes in post-natal lifestyleand environment. The period in which thetrends, for example of CVD indeveloping countries, haveevolved is too short for anychanges in the gene pool to ac-count for them.
b. Interaction (potentiatingeffect) between fetal andpost-natal effects
Despite questions over the lim-ited direct role of fetal factors indetermining trends and patterns
of disease, they may nevertheless have a po-tentially important influence if their effects de-pend in part on interactions with exposures inlater life. The association of IUGR to riskfactor development as well as its apparentinteraction with obesity to enhance risk of dis-ease suggests that, in many populations, fetalundernutrition may increase susceptibility tothe adverse effects of life style or environmen-tal change. In addition, it may have apotentiating effect on the risk of disease asso-ciated with obesity. These effects, given the ap-parent intergenerational transmission of riskassociated to fetal growth, may last not just for
one, but for several generations.A potentiating effect of fetal
growth retardation (which in sta-tistical analyses would manifestin steeper slopes in the link be-tween obesity and disease foundin developing compared to de-veloped countries) would havegrave implications for the ex-pected future rates of disease inthe developing world.
PART I. LIFE COURSE IMPACTS ON RISK OF CHD, STROKE AND DIABETES – THE STATE OF THE ART EVIDENCE
In many populations,fetal undernutrition mayincrease susceptibility tothe adverse effects of lifestyle or environmentalchange. In addition, it
may have a potentiatingeffect on the risk ofdisease associated
with obesity.

PART II
Emerging implications forpolicy and research

2.1 Introduction
In light of the evidence on the influences of lifecourse factors on the risk of CHD, stroke, anddiabetes, several implications for policy and forresearch have been identified by the experts,and a set of firm recommendations have beenmade.
This second part of the report presents firstthe emerging recommendations for policy, andthen the recommended research agenda.
2.2 Emerging implications andrecommendations for policy
Whilst carrying a great potential for disease pre-vention, the move from research to policy basedon the life course impacts on disease presents agreat challenge. The disease specific nature oflife course impacts on diseaserisk means that integration ofpolicies may be difficult. Thereare no simple models such as, forexample, in the case of tobacco.
Policies specifically geared toreducing the risk of one disease,may have no, or even adverseeffects on the risk of another.Policies may, moreover, havedifferent effects in different set-tings and cohorts, and couldhave possible unintended detri-mental outcomes in the short term.
Much more, therefore, needs to be knownabout the life course influences on various dis-eases, in particular what aspects may be com-mon to them, what trade-offs exist between shortand possible long-term outcomes, and what ef-fects prevail in different environmental contextsand in different cohorts. This notwithstanding,however, some clear implications and recom-mendations for policy already emerge.
Given that the scientific knowledge on lifecourse and disease is still evolving, these rec-ommendations are placed in a hierarchy accord-ing to the firmness of currently availableevidence.
1. Firm positive recommendationsfor policy
• Continue focus on major known risk factors
The major known risk behaviours—unhealthydiet, physical inactivity and tobacco use—andthe associated biological risk factors of obesity,high blood pressure, dyslipidaemias, remain the
most firmly established causal factors for CHD,stroke and diabetes. These factors should there-fore remain the focus of prevention policy.
Fetal factors, given their potential importancein shaping risk of disease, also need to be con-sidered. Above all, efforts are needed to developa fuller understanding of the nature and basisof their effect.
Prevention policies should specifically focuson tobacco use and obesity.
Prevention of tobacco use and, perhaps moreimportantly, reductions in total exposure tosmoking over the life course by encouragingyoung adults to stop, must be a priority givenits clear and reversible link to CVD and certaincancers; its alarming and rising prevalenceamong women and youth in many countries;and its detrimental effect not only on the health
of those who use tobacco butalso of the next generation.
A focus on obesity preventionis needed in view of the alarm-ing global rises in its prevalence;its central role in the develop-ment of other risk factors; its po-tential interaction with retardedearly growth to enhance diseaserisk; and finally its adverse ef-fect also on the health of thesubsequent generation.
In developing countries, obes-ity prevention policies must go hand in handwith strategies to prevent undernutrition.
• Need for strategies of primary andprimordial prevention
Given that risk behaviours and factors are morecommonly established in childhood and adoles-cence and ‘track’ through to adulthood, andgiven the difficulty of reversing especially obes-ity in adulthood, strategies of primary andprimordial prevention are of utmost impor-tance—though high risk lifestyle interventionstrategies can clearly also be effective.
Primary prevention strategies should beaimed particularly at children, and preferablyinvolve school-based health education and pro-motion programmes, focusing on behaviouraland psychosocial components and aimed at pro-moting healthy diets, exercise and reducedtobacco use. Such strategies must be appropri-ate and responsive to the particular setting andto the prevailing cultural perceptions, for exam-ple regarding body weight.
PART II. EMERGING IMPLICATIONS FOR POLICY AND RESEARCH
49
The major known riskbehaviours—unhealthydiet, physical inactivity
and tobacco use—and theassociated biological riskfactors of obesity, high
blood pressure,dyslipidaemias shouldremain the focus ofprevention policy.
50
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
Targeting primary prevention policies at thefollowing groups may be beneficial:
• Young girls or women. Preventing tobaccouse will not just reduce their own risk ofdisease but also the risk of low birthweight and later disease risk in their off-spring. In the same vein, preventing obes-ity in girls or young women will not justbenefit their own health, but also the riskof obesity and associated disease in theirchildren. Given the critical effect ofobesity development inadolescence, policies mayperhaps focus particularlyon pre-puberty girls
• Those socially or biologi-cally disadvantaged fromearly life, for example,those with low birth weight, stunting, orexposed to gestational maternal diabetes,or with parents who are obese
• Youth at those ages where particular ‘life-styles’ are adopted, i.e. where ‘program-ming of lifestyle’ occurs
• Adolescents and young adults who alreadysmoke should be specifically targeted byefforts to help them quit smoking—theearlier one quits the greater the benefit
Primary prevention strategies must be under-pinned and complemented by policies of pri-mordial prevention. Such policies must addressthe various macro-structural social, economic,and cultural forces that influence and determine(or protect from) the uptake of risk behavioursamong different populations in different set-tings, in particular in the developing world. Spe-cifically, such policies should aim at:
• Reduction of advertising or positivecultural representations of known riskfactors—e.g. tobacco or unhealthy foods
• Wide use of smoke-free environments
• Fiscal policies to reduce smoking
• Promotion of public healthy food policies
• Reduction of the influence of big food cor-porations, especially on the young
• Encouragement of public and private part-nerships. This is the most realistic andpromising way to move forward on creat-ing healthy developmental environments,
in particular with regard to adoption ofrisk behaviours such as tobacco use, poordiet and lack of physical activity.
• Reduction of poverty
Reducing poverty and increasing education willimprove children’s health trajectories both inrelation to infectious and non-communicablediseases. Among girls, such strategies will notjust improve their own health trajectories, butalso that of their offspring in the next genera-
tion.Policies, specifically to pre-
vent severe undernutrition andstunting—as have already beensuccessfully pursued in somepopulations—are likely to in-crease work capacity, intellectualfunctioning and educational
achievement, and reduce risk of developing cen-tral adiposity. By additionally lowering the riskof low birth weight in offspring, such interven-tions may also reduce disease risk in the nextgeneration. Concrete interventions, thus, couldthus take the form of public support for nutri-tion programmes from infancy through school.
2. Unspecified recommendations
• No clear direction regarding fetal growth
Despite the high profile of evidence linkingearly life factors such as impaired fetal or child-hood growth to risk of later disease, no firmpolicy recommendations can yet be made.
First, there are potentially important shortand long-term negative effects and trade-offs ofstrategies to increase fetal growth. For increasedfetal growth these include, in the short term, araised risk for obstetric complications throughgrowing larger babies in many developingpopulations. In the long term, they may causea possibly increased risk of other chronic dis-eases: higher birth weight and stature, for ex-ample, are associated with a higher risk of someneoplasms.
Second, the U-shaped relationship betweensize at birth and risk of later diabetes or CVD,as well as the existence of apparent populationand cohort differences in the association be-tween fetal growth and later disease, indicatethat no clear direction can yet be given in termsof what is the ‘optimum’ birth size to target for.
Third, current evidence casts serious doubton the feasibility and effectiveness of currently
Strategies of primaryand primordial
prevention are of utmostimportance.
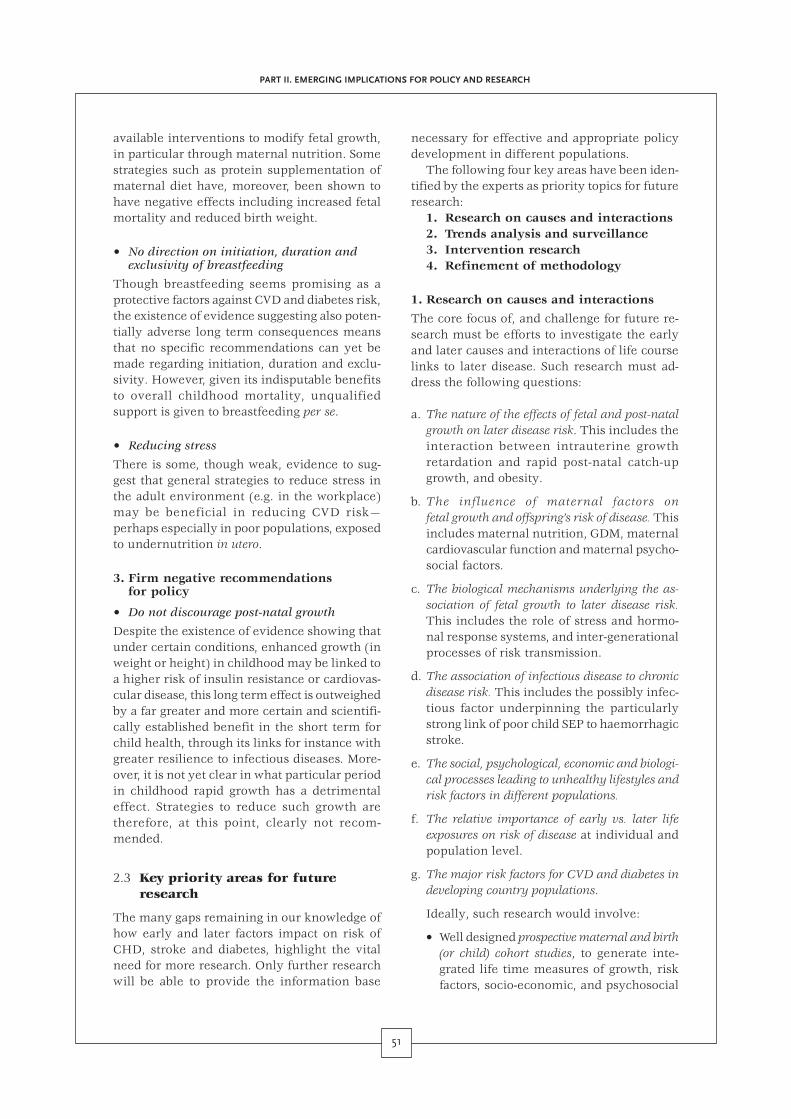
51
available interventions to modify fetal growth,in particular through maternal nutrition. Somestrategies such as protein supplementation ofmaternal diet have, moreover, been shown tohave negative effects including increased fetalmortality and reduced birth weight.
• No direction on initiation, duration andexclusivity of breastfeeding
Though breastfeeding seems promising as aprotective factors against CVD and diabetes risk,the existence of evidence suggesting also poten-tially adverse long term consequences meansthat no specific recommendations can yet bemade regarding initiation, duration and exclu-sivity. However, given its indisputable benefitsto overall childhood mortality, unqualifiedsupport is given to breastfeeding per se.
• Reducing stress
There is some, though weak, evidence to sug-gest that general strategies to reduce stress inthe adult environment (e.g. in the workplace)may be beneficial in reducing CVD risk—perhaps especially in poor populations, exposedto undernutrition in utero.
3. Firm negative recommendationsfor policy
• Do not discourage post-natal growth
Despite the existence of evidence showing thatunder certain conditions, enhanced growth (inweight or height) in childhood may be linked toa higher risk of insulin resistance or cardiovas-cular disease, this long term effect is outweighedby a far greater and more certain and scientifi-cally established benefit in the short term forchild health, through its links for instance withgreater resilience to infectious diseases. More-over, it is not yet clear in what particular periodin childhood rapid growth has a detrimentaleffect. Strategies to reduce such growth aretherefore, at this point, clearly not recom-mended.
2.3 Key priority areas for futureresearch
The many gaps remaining in our knowledge ofhow early and later factors impact on risk ofCHD, stroke and diabetes, highlight the vitalneed for more research. Only further researchwill be able to provide the information base
necessary for effective and appropriate policydevelopment in different populations.
The following four key areas have been iden-tified by the experts as priority topics for futureresearch:
1. Research on causes and interactions2. Trends analysis and surveillance3. Intervention research4. Refinement of methodology
1. Research on causes and interactions
The core focus of, and challenge for future re-search must be efforts to investigate the earlyand later causes and interactions of life courselinks to later disease. Such research must ad-dress the following questions:
a. The nature of the effects of fetal and post-natalgrowth on later disease risk. This includes theinteraction between intrauterine growthretardation and rapid post-natal catch-upgrowth, and obesity.
b. The influence of maternal factors onfetal growth and offspring’s risk of disease. Thisincludes maternal nutrition, GDM, maternalcardiovascular function and maternal psycho-social factors.
c. The biological mechanisms underlying the as-sociation of fetal growth to later disease risk.This includes the role of stress and hormo-nal response systems, and inter-generationalprocesses of risk transmission.
d. The association of infectious disease to chronicdisease risk. This includes the possibly infec-tious factor underpinning the particularlystrong link of poor child SEP to haemorrhagicstroke.
e. The social, psychological, economic and biologi-cal processes leading to unhealthy lifestyles andrisk factors in different populations.
f. The relative importance of early vs. later lifeexposures on risk of disease at individual andpopulation level.
g. The major risk factors for CVD and diabetes indeveloping country populations.
Ideally, such research would involve:
• Well designed prospective maternal and birth(or child) cohort studies, to generate inte-grated life time measures of growth, riskfactors, socio-economic, and psychosocial
PART II. EMERGING IMPLICATIONS FOR POLICY AND RESEARCH
52
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
parameters. One opportunity in this re-spect would be extension of the WHO roadto health studies of child health and growthstudies, beyond the age of five.
• Historical cohort studies with availabledata sets on early growth parameters.Possible examples include the Bambui orPelotas longitudinal study cohorts inBrazil, or possibly a cohort from the 1956famine in India. Potentially valuable co-horts may also be identified from pastmonitoring studies on maternal and/orchild growth and development, especiallyin developing countries. Efforts are neces-sary, in this respect, to preserve and makesuch existing data sets accessible.
• Multi-generational studies, especially ofmigrants (and those remaining in the coun-try of origin). The by now three genera-tions of Asian migrants in the U.K., as wellas Japanese migrants in Brazil may pro-vide important opportunities for this.
2. Trends analysis and surveillance
Investigations of causes and interactions of lifecourse links to later disease must be comple-mented by research to establish and analysetrends in risk factors and disease This wouldspecifically involve:
a. Surveillance of trends and socioeconomic pat-terns in major risk factors
b. Surveillance of trends and patterns in maternaland child health, nutrition and growth
3. Intervention research
Investigations of causes and interactions andsurveillance and analysis of trends must be com-plemented by research to assess the potentialeffectiveness and impact of interventions. Thisspecifically includes:
a. Comprehensive policy reviews on actions tar-geting under- and over-nutrition in developingcountries
b. Investigation of the efficacy, long and short termeffects (on both mother and child) of interven-tions to increase birth weight
c. Investigation of the short and long-term out-comes of enhanced early growth for infants bornsmall
d. Establishment of the long term effects ofbreastfeeding with regard to non communicablediseases
e. Research to identify ways of applyingcurrent knowledge to prevention programmes
4. Methodological issues
Finally, for life course research to be as effec-tive as possible, efforts are necessary to improveon existing, or foster certain methodologies. Thisinvolves:
a. Improvement of measures of intra-uterinegrowth retardation (alternatives to low birthweight). These must reflect new born bodycomposition and fetal exposures that may notnecessarily be expressed in birth size.
b. Improvement of measures of early socioeconomicdisadvantage and psychosocial experiences
c. Improvement of measures for adiposity, andestablishment of appropriate population normsacross the life course
d. Improvement of reliability and accuracy of meas-ures for blood pressure and establishment ofappropriate population norms
e. Development of specific measures for underly-ing pathophysiological factors, e.g. endothelialdysfunction
f. Conduct of comparative research betweenpopulations at different stages of theepidemiological/nutritional transition, as wellas between cohorts.
Comparative analyses can powerfully illumi-nate the role of the postnatal environment inshaping disease risk in interaction with earlygrowth experiences.
3.4 Conclusion: Taking policy andresearch agendas forward
The experts’ recommendations on policy andresearch in light of current evidence on the lifecourse links to CHD, stroke and diabetes presenta vital starting point for harnessing the poten-tial of the life course perspective to identify themost appropriate and effective prevention poli-cies in different populations.
WHO, together with the group of experts whoare committed to guiding and supporting itsefforts, is taking steps to foster this life courseinitiative, through collaborative work and con-

53
sultation across departments within WHO andwith partner institutions.
A specific focus of this work will be the de-velopment, in consultation with the experts, ofa protocol for a multi-centre comparative studyto address some of the key gaps in knowledgeon life course and NCD risk in differentpopulations—especially in developing countries.
PART II. EMERGING IMPLICATIONS FOR POLICY AND RESEARCH

54
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
Bibliography
Barker, D.J.P., Hales, C.N., Fall, C.H.D., Osmond,C., Phipps, K., Clark, P.M.S. (1993a) “Type 2 (Non-Insulin –Dependent) Diabetes Mellitus, Hyperten-sion and Hyperlipidaemia (Syndrome X): Relationto Reduced Fetal Growth” Diabetologia 36: 62–67
Barker, D.J.P., Martyn, C.N., Osmond, C., Hales,C.N., Fall, C.H.D. (1993b) “Growth In Utero andSerum Cholesterol Concentrations in Adult Life”BMJ 307: 1524–1527
Barker, D.J.P. (1995) “Fetal Origins of CoronaryHeart Disease” BMJ 311: 171–174
Barker, D.J.P. (ed.) (2000a) Fetal and Infant Originsof Adult Disease. London: BMJ Books
Barker, D.J.P., Shiell, A.W., Barker, M.E., Law, C.M.(2000b) “Growth in Utero and Blood PressureLevels in the Next Generation” J Hypertens 18: 843–846
Barros, F.C., Victora, C.G., Vaughan, J.P., Tomasi,E., Horta, B.L., Cesar, J.A., Menezes, M.B.,Halpern, R., Post, C.L., del Mar Garcia, M. (2001)“The Epidemiological Transition in Maternal andChild Health in a Brazilian City, 1982–93: a Com-parison of Two Population-Based Cohorts” PediatrPerinat Epidemiol 15: 4–11
Bartley, M., Fitzpatrick, R., Firth, D., Marmot, M.(2000) “Social Distribution of Cardiovascular Dis-ease Risk Factors: Change Among Men 1984–1993”J Epidemiol Community Health 54: 806–814
Bassey, E.J., Aihie Sayer, A., Cooper, C. (forthcom-ing) “A Life-Course Approach to MusculoskeletalAgeing in Women: Muscle Strength, Osteoporosisand Osteoarthritis” in D. Kuh and R. Hardy (eds)A Life Course Approach to Women’s Health. OUP(in press)
Bavdekar, A., Yajnik, C.S., Fall, C.H.D., Bapat, S.,Pandit, A.N., Deshpande, V., Bhave, S., Kellingray,S.D., Joglekar, C.V. (1999) “Insulin Resistance in 8year old Indian Children” Diabetes 48: 2422–2429
Bénéfice, E., Garnier, D., Simonson, K.B., Malina,R.M. (2001) “Relationship between Stunting inInfancy and Growth and Fat Distribution DuringAdolescence in Senegalese Girls” Eur J Clin Nutr55: 50–58
Ben-Shlomo, Y., Kuh, D. (1999) “A Life CourseApproach to Chronic Disease Epidemiology”Paper presented at International Workshop ‘Synthetic
Aboderin, I., Kalache, A., Ben-Schlomo, Y., Lynch,J.W., Yajnik, C.S., Kuh, D., Yach, D. (2001) LifeCourse Perspectives on Coronary Heart Disease,Stroke and Diabetes: Key Issues and Implcations forPolicy and Research. Geneva, World Health Organi-zation.
Adair, L.S. (1998) “Filipino Children Exhibit Catch-Up Growth from Age 2 to 12 Years” J Nutr 129:1140–1148
Åkerblom, H.K., Viikari, J., Raitakari, O.T., Uhari,M. (1999) “Cardiovascular Risk in Young FinnsStudy: General Outline and Recent Developments”Ann Med 31 Suppl.1: 45–54
ALSPAC (2001) “ALSPAC: The Avon LongitudinalStudy of Parents and Children: Aims and StudyDesign” [Internet—WWW, URL] http://www.ich.bris.ac.uk/ALSPACext/MainProtocol/Default.htm (28th February, 2001)
Anastasiou, E., Alevizaki, M., Grigorakis, S.J.,Phillipou, G., Kyprianou, M., Souvatzoglou, A.(1998) “Decreased Stature in Gestational DiabetesMellitus” Diabetologia 41: 997–1001
Anderson, K.M., Kastelli, W.P., Levy, D. (1987)“Cholesterol and Mortality: 30 Years of Follow-Upfrom the Framingham Study” JAMA 257: 2176–2180
Baird, J., Osmond, C., McGregor, A., Snieder, H.,Hales, C.N., Phillips, D.I. (2001) “Testing the FetalOrigins Hypothesis in Twins: The BirminghamTwin Study” Diabetologia 44: 33–39
Bao, W., Srinivasan, S.R., Wattigney, W.A.,Berenson, G.S. (1994) “Persistence of MultipleCardiovascular Risk Clustering Related to Syn-drome X from Childhood to Young Adulthood: theBogalusa Heart Study” Arch Intern Med 154: 1842–1847
Barker, D.J.P. (ed.) (1992) Fetal and Infant Originsof Adult Disease. London: BMJ Books
Bao, W., Threefoot, S.A., Srinivasan, S.R., Berenson,G.S. (1995) “Essential Hypertension Predicted byTracking of Elevated Blood Pressure from Child-hood to Adulthood: The Bogalusa Heart Study” AmJ Hypertens 8: 657–665
Barker, D.J.P., Osmond, C., Winter, P.D., Margetts,B., Simmonds, S.J. (1989) “Weight Gain in Infancyand Death from Ischaemic Heart Disease” Lancet2: 577–580

55
Biographies: State of the Art and Developments’, 6–9June, San Miniato (Pisa), Italy
Berenson, G.S., Srinivasan, S.R., Webber, L.S.,Nicklas, T.A., MacD.Hunter, S., Harsha, D.W.,Johnson, C.C., Arbeit, M.L., Dalferes, E.R.,Wattigney, W.A., Lawrence, M.D. (1991) Cardiovas-cular Risk in Early Life: The Bogalusa Heart Study.Current Concepts Series. Kalamazoo, Michigan:Upjohn
Berenson, G.S., Srinivasan, S.R., Bao, W., Newman,W.P., Tracy, R.E., Wattigney, W.A. (1998a) “Asso-ciation Between Multiple Cardiovascular Risk Fac-tors and Atherosclerosis in Children and YoungAdults” NEJM 338: 1650–1656
Berenson, G.S., Srinivasan, S.R., Nicklas, T.A.(1998b) “Atherosclerosis: A Nutritional Disease ofChildhood” Am J Cardiol 82: 22T–29T
Bjorntorp, P. (1997) “Stress and CardiovascularDisease” Acta Physiol Scand Suppl 640: 144–148
Blane, D., Hart, C.L., Davey Smith, G., Gillis, C.R.,Hole, D.J., Hawthorne, M. (1996) “Association ofCardiovascular Disease Risk with SocioeconomicPosition During Childhood and During Adulthood”BMJ 313: 1434–1438
Borras, J.M., Fernandez, E., Schiaffino, A., Borrell,C., La Vecchia, C. (2000) “Pattern of Smoking Ini-tiation in Catalonia, Spain, from 1948 to 1992” AmJ Publ Health 90: 1459–1462
Boulton, T.J.C., Magarey, A.M., Cockington, R.A.(1995) “Serum Lipids and Apolipoproteins from 1to 15 Years: Changes with Age and Puberty, andRelationships with Diet, Parental Cholesterol andFamily History of Ischaemic Heart Disease” ActaPaediatr 84: 1113–1118
Braddon, F.E., Rogers, B., Wadsworth, M.E., Davies,J. (1986) “Onset of Obesity in a 36 Year BirthCohort Study” BMJ 293: 299–303
Bray, G. (1996) “Coherent Preventive and Manage-ment Strategies for Obesity” in D.J. Chadwick andG.C. Cardew (eds) The Origins and Consequencesof Obesity. Chichester: Wiley, pp228–254 (CibaFoundation Symposium 201)
Brunner, E., Shipley, M.J., Blane, D., Davey Smith,G., Marmot, M. (1999) “When Does Cardiovascu-lar Risk Start? Past and Present SocioeconomicCircumstances and Risk Factors in Adulthood”J Epidemiol Community Health 53: 757–764
Bundred, P., Kitchiner, D., Buchan, I. (2001) “Preva-lence of Overweight and Obese Children Between1989–1998: Population Based Series of Cross Sec-tional Studies” BMJ 322: 326–328
Burke, V., Beilin, L.J., Dunbar, D. (2001) “FamilyLifestyle and Parental Body Mass Index as Predic-tors of Body Mass Index in Australian Children: a
Longitudinal Study” Int J Obes Relat Metab Disord25: 147–157
Cebu study team (1991) “Underlying and Proxi-mate Determinants of Child Health: The CebuLongitudinal Health and Nutrition Study” Am JEpidemiol 133: 185–201
Cheung, Y.B., Low, L., Osmond, C., Barker, D.,Karlberg, J. (2000) “Fetal Growth and Early Post-natal Growth Are Related to Blood Pressure inAdults” Hypertension 36 (5) 795–800
Chen, Z., Peto, R., Collins, R., MacMahon, S., Lu,J., Li, W. (1991) “Serum Cholesterol Concentrationand Coronary Heart Disease in population WithLow Cholesterol Conctentrations” BMJ 303: 276–282
Colhoun, H.M., Hemingway, H., Poulter N. (1998)“Socio-Economic Status and Blood Pressure: AnOverview Analysis” J Hum Hypertens 12: 91–110
Cooper, C., Kuh, D., Egger, P., Wadsworth, M.,Barker, D. (1996) “Childhood Growth and Age atMenarche” Br J Obstet Gynaecol 103: 814–817
Corrao, M.A., Guindon, G.E., Sharma, N.,Shokoohi, D.F. (eds) (2000) Tobacco Control Coun-try Profiles. American Cancer Society, Atlanta,Georgia, USA
Crawford, P.B., Story, M., Wang, M.C., Ritchie, L.D.,Sabry, Z.I. (2001) “Ethnic Issues in the Epidemiol-ogy of Childhood Obesity” Pediatr Clin North Am48: 855–878
Croft, J.B., Strogatz, D.S., James, S.A., Keenan,N.L., Ammerman, A.S., Malarcher, A.M., Haines,P.S. (1992) “Socioeconomic and Behavioural Cor-relates of Body Mass Index in Black Adults: ThePitt County Study” Am J Publ Health 82: 821–826
Crowther, N.J., Cameron, N., Trusler, J., Gray, I.P.(1998) Association Between Poor Glucose Toler-ance and Rapid Post Natal Weight Gain in Seven-year-old Children” Diabetologia 41 (10) 1163–1167
Curtin, F., Morabia, A., Bernstein, M. (1997) “Smok-ing Behaviour in a Swiss Urban Population: theRole of Gender and Education” Prev Med 26: 658–663
Danesh, J., Collins, R., Peto, R. (1997) “ChronicInfections and Coronary Heart Disease: Is Therea Link? Lancet 350: 430–436
Davey Smith, G., Shipley, M.J., Marmot, M.G.,Rose, G. (1992) Plasma Cholesterol Concentrationand Mortality: the Whitehall Study” JAMA 267: 70–76
Davey Smith, G. (1997) “Socioeconomic Differen-tials” in D. Kuh and Y. Ben-Shlomo (eds) A LifeCourse Approach to Chronic Disease Epidemiology.Oxford: Oxford University Press, pp242–273
BIBLIOGRAPHY
56
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
Davey Smith, G., Hart, C., Ferrell, C., Upton, M.,Hole, D., Hawthorne, V., Watt, G. (1997) “BirthWeight of Offspring and Mortality in the Renfrewand Paisley Study: Prospective ObservationalStudy” BMJ 315: 1189–1193
Davey Smith, G., Shipley, M., Leon, D.A. (1998)“Height and Mortality from Cancer Among Men:Prospective Observational Study” BMJ 317: 1351–1352
Davey Smith, G., Harding, S., Rosato, M. (2000a)“Relation Between Infants’ Birth Weight and Moth-ers’ Mortality: Prospective Observational Study”BMJ 320: 839–840
Davey Smith, G., Hart, C., Upton, M., Hole, D.,Gillis, C., Watt, G., Hawthorne, V. (2000b) “Heightand Risk of Death among Men and Women: Aetio-logical Implications of Associations with Cardiores-piratory Disease and Cancer Mortality” J. ofEpidemiol Community Health 54: 97–103
Davey Smith, G., Shipley, M.J., Batty, G.D., Mor-ris, J.N., Marmot, M. (2000c) “Physical Activity andCause Specific Mortality in the Whitehall Study”Public Health 114: 308–315
Davey Smith, G., Greenwood, R., Gunnell, D.,Sweetnam, P., Yarnell, J., Elwood, P. (2001a) “LegLength, Insulin resistance, and Coronary HeartDisease Risk: The Caerphilly Study” J EpidemiolCommunity Health 55: 867–872
Davey Smith, G., Ben-Shlomo, Y., Lynch, J.W.(2001) “Life Course Approaches to Inequalities inCoronary Heart Disease Risk” in S. Stansfeld andM.Marmot (eds) Stress and Heart Disease. London:BMJ Books, in press
Dedman, D.J., Gunnell, D., Davey Smith, G.,Frankel, S. (2001) “Childhood Housing Conditionsand Later Mortality in the Boyd Orr Cohort”J Epidemiol Community Health 55: 10–15
DeFronzo, R.A., Ferrannini, E. (1991) “Insulin Re-sistance: a Multifaceted Syndrome Responsible forNIDDM, Obesity, Hypertension, Dyslipidaemia,and Atherosclerotic Cardiovascular Disease” DiabetCare 14: 173–194
DeOnis, M., Bloessner, M. (2000) “Prevalence andTrends of Overweight Among Preschool Childrenin Developing Countries” Am J Clin Nutr 72: 1032–1039
Dietz, W.H. (1997) “Periods of Risk in Childhoodfor the Development of Adult Obesity—What DoWe Need to Learn?” J Nutr 127: 1884S–1886S
Dietz, W.H. (2000) “’Adiposity Rebound’: Reality orEpiphenomenon” Lancet 356: 2027–2028
Dietz, W.H. (2001a) “The Obesity Epidemic inYoung Children” BMJ 322: 313–314
Dietz, W.H. (2001b) “Breastfeeding May Help Pre-vent Childhood Overweight” JAMA 285: 2506–2507
Dobson, A.J., Evans, A., Ferrario, M., Kuulasmaa,K.A., Moltchanov, V.A., Sans, S., Tunstall-Pedoe,H., Tuomilehto, J.O., Wedel, H., Yarnell, J. (1998)“Changes in Estimated Coronary Risk in the 1980s:Data from 38 Populations in the WHO MONICAProject” Ann Med 30: 199–205
Doll, R., Peto, R., Wheatley, K., Gray, R., Suther-land, I. (1994) “Mortality in Relation to Smoking:40 Years’ Observation on Male British Doctors” BMJ309: 901–911
Donker, G.A., Labarthe, D.R., Harrist, R.B., Selwyn,B.J., Srinivasan, S.R., Wattigney, W., Berenson, G.S.(1997) “Low Birth Weight and Serum Lipid Con-centrations at Age 7–11 Years in a Biracial Sam-ple” Am J Epidemiol 145: 398–407
Dorosty, A.R., Emmet, P.M., Cowin, S.D., Reilly,J.J. (2000) “Factors Associated with Early Adipos-ity Rebound. ALSPAC Study Team” Pediatrics 105:1115–1118
Dwyer, T., Blizzard, L., Orley, R., Ponsonby, A.L.(1999) “Within Pair Association Between BirthWeight and Blood Pressure at 8 in Twins from aCohort Study” BMJ 319: 1325–1329
Elisaf, M. (2001) “The Treatment of Coronary HearDisease: An Update. Part 1: An Overview of theRisk Factors for Cardiovascular Disease” Curr MedRes Opin 17: 18–26
Eriksson, J.G., Forsén, T., Tuomilehto, J., Winter,P.D., Osmond, C. (1999) “Catch–up Growth inChildhood and Death from Coronary Heart Dis-ease: A Longitudinal Study” BMJ 318: 427–431
Eriksson, J.G., Forsén, T., Tuomilehto, J., Osmond,C., Barker, D.J.P. (2000a) “Early Growth, Adult In-come, and Risk of Stroke” Stroke 31: 869–874
Eriksson, J., Forsén, T., Tuomilehto, J., Osmond,C., Barker, D. (2000b) “Fetal and Childhood Growthand Hypertension in Adult Life” Hypertension 36:790
Eriksson, J., Forsén, T., Tuomilehto, J., Osmond,C., Barker, D.J.P. (2001) “Early Growth and Coro-nary Heart Disease in Later Life: LongitudinalStudy” BMJ 322: 949–953
Eveleth, P.B., Tanner, J.M. (1990) Worldwide Varia-tion in Human Growth. 2nd edition, Cambridge:Cambridge University Press
Fall, C.H.D., Osmond, C., Barker, D.J.P., Clark,P.M.S., Hales, C.N., Stirling, Y., Meade, T.W. (1995)“Fetal and Infant Growth and Cardiovascular RiskFactors in Women” BMJ 310: 428–432
Fall, C.H.D., Stein, C.E., Kumaran, K., Cox, V.,Osmond, C., Barker, D.J.P., Hales, C.N. (1998) “Size
57
at Birth, Maternal Weight, and Type 2 Diabetes inSouth India” Diabet Med 15: 220–227
Fall, C.H.D, Yajnik, C.S., Rao, S., Coyaji, K.J. (1999)“The Effects of Maternal Body Composition BeforePregnancy on Fetal Growth: The Pune MaternalNutrition Study” In P.M.S. O’Brien, T.Wheeler,D.J.P. Barker (eds) Fetal Programming Influences onDevelopment and Disease in Later Life. London:RCOG Press, pp231–245
Flegal, K.M., Carroll, M.D., Kuczmarski, R.J.,Johnson, C.L. (1998) “Overweight and Obesity inthe United States: Prevalence and Trends, 1960–1994” Int J Obes Relat Metab Disord 22: 39–47
Fogelholm, M., Nuutinen, O., Pasanen, M.,Myohanen, E., Saatela, T. (1999) “Parent-ChildRelationship of Physical Activity Patterns andObesity” Int J Obes Relat Metab Disord 23: 1262–1268
Forrester, T.E., Wilks, R.J., Bennett, F.I., Simeon,D., Osmond, C., Allen, M., Chung, A.M., Scott, P.(1996) “Fetal Growth and Cardiovascular Risk Fac-tors in Jamaican Schoolchildren” BMJ 312: 156–160
Forsén, T., Eriksson, J.G., Tuomilehto, J., Osmond,C., Barker, D.J.P. (1999) “Growth in Utero andDuring Childhood in Women Who Develop Coro-nary Heart Disease: A Longitudinal Study” BMJ319: 1403–1407
Forsén, T., Eriksson, J., Tuomilehto, J., Reunanen,A., Osmond, C., Barker, D. (2000a) “The Fetal andChildhood Growth of Persons Who Develop Type2 Diabetes” Ann Intern Med 133(3): 176–182
Forsén, T., Eriksson, J., Qiao, Q., Tervahauta, M.,Nissinen, A., Tuomilehto, J. (2000b) “Short Stat-ure and Coronary Heart Disease: A 35 Year Fol-low-up of the Finnish Cohorts of the SevenCountries Study” J. of Internal Medicine 248: 326–332
Frankel, S., Elwood, P., Sweetnam, P., Yarnell, J.,Davey Smith, G. (1996) “Birthweight, Body MassIndex in Middle Age and Incident Coronary HeartDisease” Lancet 348: 1478–1480
Freedman, D.S., Dietz, W.H., Srinivasan, S.R.,Berenson, G.S. (1999) “The Relation of Overweightto Cardiovascular Risk Factors Among Childrenand Adolescents: The Bogalusa Heart Study”Pediatrics 103: 1175–1182
Freedman, D.S., Khan, L.K., Serdula, M.K.,Srinivasan, S.R., Berenson, G.S. (2000) “SecularTrends in Height among Children During 2 Dec-ades: The Bogalusa Heart Study” Arch PediatrAdolesc Med 154: 155–161
Freedman, D.S., Khan, L.K., Dietz, W.H.,Srinivasan, S.R., Berenson, G.S. (2001) “Relation-
ship of Childhood Obesity to Coronary Heart Dis-ease Risk Factors in Adulthood: the Bogalusa HeartStudy” Pediatrics 108: 712–718
Frisancho, A.R. (2000) “Prenatal Compared withParental Origins of Adolescent Fatness” Am J ClinNutr 72: 1186–1190
Fuentes, R., Ilmaniemi, N., Laurikainen, E.,Tuomilehto, J., Nissinen, A. (2000) “Hypertensionin Developing Economies: A Review of Population-Based Studies Carried Out from 1980 to 1998”J Hypertens 18: 521–529
Fung, T.T., Hu, F.B., Yu, J., Chu, N.-F., Spiegelman,D., Tofler, G.H., Willett, W.C., Rimm, E.B. (2000)“Leisure-Time Physical Activity, Television Watch-ing, and Plasma Biomarkers of Obesity and Car-diovascular Disease Risk” Am J Epidemiol 152:1171–1178
Gao, M., Ikeda, K., Hattori, H., Miura, A., Nara, Y.,Yamori, Y. (1999) “Cardiovascular Risk FactorsEmerging in Chinese Populations UndergoingUrbanization” Hypertens Res 22: 209–215
Gaskin, P.S., Walker, S.P., Forrester, T.E., Grantham-McGregor, S.M. (2000) “Early Linear Growth andLater Blood Pressure” Eur J Clin Nutr 54: 563–567
Gillman, M.W., Rifas-Shiman, S.L., Camargo, C.A.,Berkey, C.S., Frazier, L., Rockett, H.R.H., Field,A.E., Colditz, G.A. (2001) “Risk of OverweightAmong Adolescents Who Were Breastfed as In-fants” JAMA 285: 2461–2467
Godlee, F. (1999) Clinical Evidence. London: BMJBooks
Gortmaker, S.L., Must, A., Perrin, J.M., Sobol, A.M.,Dietz, W.H. (1993) “Social and Economic Conse-quences of Overweight in Adolescence and YoungAdulthood” NEJM 329: 1008–1012
Gortmaker, S.L., Must, A., Sobol, A.M., Peterson,K., Colditz, G.A., Dietz, W.H. (1996) “TelevisionViewing as a Cause of Increasing Obesity amongChildren in the United States, 1986–1990” ArchPediatr Adolesc Med 150: 356–362
Greenlund, K.J., Liu, K., Dyer, A.R., Kiefe, C.I.,Burke, G.L., Yunis, C. (1996) “Body Mass Index inYoung Adults: Associations With Parental Body Sizeand Education” Am J Publ Health 86: 480–485
Gunnell, D.J., Davey Smith, G., Frankel, S.,Nanchahal, K., Braddon, F.E.M., Pemberton, J.,Peters, T.J. (1998a) “Childhood Leg Length andAdult Mortality: Follow Up of the Carnegie (BoydOrr) Survey of Diet and Health in Pre-war Britain”J Epidemiol Community Health 52: 142–152
Gunnell, D.J., Davey Smith, G., Holly, J.M.P.,Frankel, S. (1998b) “Leg Length and Risk of Can-cer in the Boyd Orr Cohort” BMJ 317: 1350–1351
BIBLIOGRAPHY
58
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
Gunnell, D.J., Davey Smith, G., Frankel, S.J.,Kemp, M., Peters, T.J. (1998c) “Socio-economic andDietary Influences on Leg Length and TrunkLength in Childhood: A Reanalysis of the Carnegie(Boyd Orr) Survey of Diet and Health in PrewarBritain (1937–39” Pediatric and Perinatal Epidemi-ology 12 (Suppl. 1): 96–113
Gunnell, D., Davey Smith, G., McConnachie, A.,Greenwood, R., Upton, M:, Frankel, S. (1999) “Sepa-rating in-utero and Postnatal Influences on LaterDisease” Lancet 354: 1256–1257
Guo, S.S., Roche, A.F., Chumlea, W.C., Gardner,J.D., Siervogel, R.M. (1994) “The Predictive Valueof Childhood Body Mass Index Values for Over-weight at Age 35y” Am J Clin Nutr 59: 810–819
Guo, S.S., Chumlea, W.C. (1999) “Tracking of BodyMass Index in Children in Relation to Overweightin Adulthood” Am J Clin Nutr 70: 145–148
Gupta, R., Gupta, V.P., Ahluwalia, N.S. (1994) “Edu-cational Status, Coronary Heart Disease and Coro-nary Risk Factor Prevalence in a Rural Populationin India” BMJ 307: 1332–1336
Hales, C.N., Barker, D.J.P., Clark, P.M.S. , Cox, L.J.,Fall, C., Osmond, C.M., Winter, P.D. (1991) “Fetaland Infant Growth and Impaired Glucose Toler-ance at Age 64” BMJ 303: 1019–1022
Hales, C.N. and Barker, D.J.P. (eds) (1992) “Type 2(non-insulin-dependent) Diabetes Mellitus: TheThrifty Phenotype Hypothesis” Diabetologia 35:595–601
Harding, S., Bethune, A., Maxwell, R. et al. (1998)“Mortality Trends Using the Longitudinal Study”in F. Drever and M. Whitehead (eds) HealthInequality. London: HMSO, pp 143–155
Harding, J.E. (2001) “The Nutritional Basis of theFetal Origins of Adult Disease” Int J Epidemiol 30:15–23
Hart, C.L., Hole, D.J., Davey Smith, G. (2000)“Influence of Socioeconomic Circumstances inEarly and Later Life on Stroke Risk among Men ina Scottish Cohort” Stroke 31: 2093–2097
Hasegawa, T., Oshima, M. (2001) “Non-LinearTrends in the Blood Pressure of Japanese Adults”Hypertens Research 24: (3) 215–219
Hattersley, A.T., Beards, T., Ballantyne, E.,Appleton, M., Harvey, R., Ellard, S. (1998) “Muta-tions in the Glucokinase Gene of the Fetus Resultin Reduced Birth Weight” Nat Genet 19: 268–270
Hattersley, A.T., Tooke, J.E. (1999) “The Fetal In-sulin Hypothesis: An Alternative Explanation ofthe Association Between Low Birthweight withDiabetes and Vascular Disease” Lancet 353: 1789–1792
Hediger, M.L., Overpeck, M.D., Kuczmarski, R.J.,McGlynn, A., Maurer, K.R., Davis, W. (1998) “Mus-cularity and Fatness of Infants and Young Chil-dren Born Small-or Large-for Gestational Age”Pediatrics 102: E1204
Hediger, M.L., Overpeck, M.D., Kuczmarski, R.J.,Ruan, J. (2001) “Association Between InfantBreastfeeding and Overweight in Young Children”JAMA 285: 2453–2460
Hemingway, H., Marmot, M. (1999) “PsychosocialFactors in the Aetiology and Prognosis of CoronaryHeart Disease: Systematic Review of ProspectiveCohort Studies” BMJ 318: 1460–1467
Hoffman, D.J., Sawaya, A.L., Verreschi, I., Tucker,C.L., Roberts, S.B. (2000) “Why Are NutritionallyStunted Children at Increased Risk of Obesity?Studies of Metabolic Rate and Fat Oxidation inShantytown Children from Sao Paulo, Brazil” Am JClin Nutr 72: 702–707
Hooper, L., Summerbell, C.D., Higgins, J.P.T.,Thompson, R.L., Clemets, G., Capps, N., DaveySmith, G., Riemersma, R.A., Ebrahim, S. (2001)“Reduced or Modified Dietary Fat for PreventingCardiovascular Disease” Cochrane Database forSystematic Reviews, Issue 3
Hu, F., B., Rimm, E.B., Stampfer, M.J., Asciero, A.,Spiegelman, D., Willett, W.C. (2000) “ProspectiveStudy of Major Dietary Patterns and Risk of Coro-nary Heart Disease in Men” Am J Clin Nutr 72:912–921
Huxley, R.R., Shiell, A.W., Law, C.M.(2000) “TheRole of Size at Birth and Postnatal Catch-Up Growthin determining Systolic Blood Pressure: A System-atic Review of the Literature” J Hypertens 18: 815–831
Ijzerman, R.G., Stehouwer, C.D., Boomsma, D.I.(2000) “Evidence for Genetic factors Explaining theBirth Weight—Blood Pressure Relation” Hyperten-sion 36: 1008–1012
Jahns, L., Siega-Riz, A.M., Popkin, B.M. (2001) “TheIncreasing Prevalence of Snacking Amongst USChildren from 1977 to 1996” J Pediatr 138: 493–498
Jang, H.C., Min, H.K., Lee, H.K., Cho, N.H.,Metzger, B.E. (1998) “Short Stature in KoreanWomen: A Contribution to the MultifactorialPredisposition to Gestational Diabetes Mellitus”Diabetologia 41: 778–783
Johnson, C.L., Rifkind, B.M., Sempos, C.T., Carroll,M.D., Bachorik, P.S., Briefel, R.R., Gordon, D.J.,Burt, V.L., Brown, C.D., Lippel, K. et al. (1993)“Declining Serum Total Cholesterol Levels amongUS Adults: The National Health and Nutrition Ex-amination Surveys” JAMA 269: 3002–3008
59
Jousilahti, P., Tuomilehto, J., Vartiainen, E.,Pekkanen, J., Puska, P. (1996) “Body Weight, Car-diovascular Risk Factors, and Coronary Mortality.15-Year-Follow-Up of Middle-Aged Men andWomen in Eastern Finland” Circulation 93: 1372–1379
Jousilahti, P., Vartiainen, E., Tuomilehto, J.,Pekkanen, J., Puska, P. (1998) “Role of Known RiskFactors in Explaining the Difference in the Risk ofCoronary Heart Disease between Eastern andSouthwestern Finland” Ann Med. 30(5): 481–487
Jousilahti, P., Tuomilehto, J., Vartiainen, E.,Eriksson, J., Puska, P. (2000) “Relation of AdultHeight to Cause-Specific and Total Mortality: AProspective Follow-up Study of 31, 199 Middle-agedMen and Women” Am. of Epidemiol. 151(11): 1112–1120
Kahn, H.S., Narayan, K.M., Williamson, D.F.,Valdez, R. (2000) “Relation of Birth Weight to Leanand Fat Thigh Tissue in Young Men” Int J ObesRelat Disord 24: 667–672
Kannel, W.B., (1996) “Blood Pressure as a Cardio-vascular Risk Factor: Prevention and Treatment” JAm Med Assoc 275: 1571–1576
Kastarinen, M.J., Nissinen, A.M., Vartiainen, E.A.,Jousilahti, P.J., Korhonen, H.J., Puska, P.M.,Tuomilehto, J. (2000) “Blood Pressure Levels andObesity Trends in Hypertensive and Normoten-sive Finnish Population from 1982 to 1997”J Hypertens 18: 255–262
Kauhanen, J., Kaplan, G., Goldberg, D.E., Salonen,J.T. (1997) “Beer Binging and Mortality. Resultsfrom the Kuopio Ischaemic Heart Disease RiskFactor Study, a Prospective Population BasedStudy” BMJ 315: 846–851
Kimm, S.Y., Obarzanek, E., Barton, B.A., Aston,C.E., Similo, S.L., Morrison, J.A., Sabry, Z.I.,Schreiber, G.B., McMahon, R.P. (1996) “Race, So-cioeconomic Status, and Obesity in 9- to 10-Year-Old Girls: The NHBLI Growth and Health Study”Ann Epidemiol 6: 266–275
Kimm, S.Y., Barton, B.A., Obarzanek, E., McMahon,R.P., Sabry, Z.I., Waclawiw, M.A., Screiber, G.B.,Morrison, J.A., Similo, S., Daniels, S.R. (2001) “Ra-cial Divergence in Adiposity During Adolescence:The NHBLI Growth and Health Study” Pediatrics107: E34
King, H., Aubert, R.E., Herman, W.H. (1998) “Glo-bal Burden of Diabetes, 1995–2025” Diabetes Care141: 1414–1431
Kitange, H.M., Swai, A.B.M., Masuki, G., Kilima,P.G., Alberti, K.G.M.M., McLarty, D.G. (1993)“Coronary Heart Disease Risk Factors in SubSaharan Africa: Studies in Adolescents” J EpidemiolPubl Health 47: 303–307
Klag, M.J., Ford, D.E., Mead, L.A., He, J., Whelton,P.K., Liang, K.Y., Levine, D.M. (1993) “Serum Cho-lesterol in Young Men and Subsequent Cardiovas-cular Disease” NEJM 328: 313–318
Kousta, E., Lawrence, N.J., Penny,A., Millauer,B.A., Robinson, S., Johnston, D.G., McCarthy, M.I.(2000) “Women With a History of Gestational Dia-betes of European and South Asian Origin areShorter than Women with Normal Glucose Toler-ance in Pregnancy” Diabetes 17: 792–797
Kramer, M.S. (1981) “Do Breast-Feeding and De-layed Introduction of Solid Foods Protect AgainstSubsequent Obesity?” J Pediatr 98: 883–887
Kramer, M.S. (1987) “Determinants of Low BirthWeight: Methodological Assessment and Meta-Analysis” Bull World Health Organ 65: 663–737
Kramer, M.S., Joseph, K.S. (1996) “Enigma ofFetal/Infant Origins Hypothesis” Lancet 348: 1254
Kuh, D., Power, C., Blane, D., Bartley, M. (1997)“Social Pathways Between Childhood and AdultHealth” in D.Kuh and Y. Ben-Shlomo (eds) A LifeCourse Approach to Chronic Disease Epidemiology.Oxford: Oxford University Press, pp 169–198
Kuh, D., Ben-Shlomo, Y. (1998) “A Life CourseApproach to Chronic Disease Epidemiology—What ’s New?” Paper Presented at AmericanEpidemiological Society, March 26, Boston,Massachussetts
Kumaran, K., Fall, C.H.D., Martyn, C.N.,Vijayakumar, M., Stein, C., Shier, R. (2000) “BloodPressure, Arterial Compliance, and Left Ventricu-lar Mass: No Relation to Small Size at Birth in SouthIndian Adults” Heart 83 (3) 272–277
Kuulasmaa, K., Tunstall-Pedoe, H., Dobson, A.,Fortmann, S., Sana, S., Tolonen, H., Evans, A.,Ferrario, M., Tuomilehto, J. (2000) “Estimation ofContribution of Changes in Classic Risk Factors toTrends in Coronary Event Rates across WHOMONICA Project Populations” Lancet 355: 675–687
Lang, T. (1997) “The Public Health Impact ofGlobalisation and Food Trade” in P.S. Shetty andK. McPherson (eds) Diet, Nutrition and ChronicDisease: Lessons from Contrasting Worlds. Chiches-ter, U.K.: Wiley, pp 173–187
Law, C.M., Barker, D.J.P., Osmond, C., Fall, C.H.D.,Simmonds, S.J.(1992) “Early Growth and Abdomi-nal Fatness in Adult Life” J Epidemiol CommunityHealth 46: 184–186
Law, C.M., Gordon, G.S., Shiell, A.W., Barker, D.J.P.,Hales, C.N. (1995) “Thinness at Birth and GlucoseTolerance in Seven Year Old Children” Diabet Med12: 24–29
Law, C.M., Egger, P., Dada, O., Delgado, H.,Kylberg, E., Lavin, P., Tang, G-H., von Hertzen,
BIBLIOGRAPHY
60
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
H., Shiell, A.W., Barker, D.J.P.(2001) “Body Size atBirth and Blood Pressure Among Children inDeveloping Countries” Int J Epidemiology 30: 52–57
Lee, I.M., Paffenbarger, R.S. Jr (1998) “PhysicalActivity and Stroke Incidence: The HarvardAlumni Health Study” Stroke 29: 2049–2054
Leeson, C.P., Kattenhorn, M., Deanfield, J.E.,Lucas, A.(2001) “Duration of Breastfeeding andArterial Distensibility in Early Adult Life: Popula-tion Based Study” BMJ 322: 643–647
Leinonen, M., Saikku, P. (2000) Infections andAtherosclerosis” Scand Cardiovasc J 34: 12–20
Leon, D.A., Koupilova, I., Lithell, H.O., Berglund,L., Mohsen, R., Vagero, D., Lithell U-B., McKeigue,P.M. (1996) “Failure to Realise Growth Potential inUtero and Adult Obesity in Relation to Blood Pres-sure in 50 year Old Swedish Men” BMJ 312: 401–406
Leon, D.A., Ben-Shlomo, Y. (1997) “Preadult Influ-ences on Cardiovascular Disease and Cancer” inD.Kuh and Y. Ben-Shlomo (eds) A Life CourseApproach to Chronic Disease Epidemiology. Oxford:Oxford University Press, pp.45–77
Leon, D.A., Lithell, H.O., Vagero, D., Koupilova,I., Mohsen, R., Berglund, L., Lithell, U.B.,McKeigue, P.M. (1998) “Reduced Fetal Growth Rateand Increased Risk of Death from Ischaemic HeartDisease: Cohort Study of 15000 Swedish Men andWomen born 1915–29” BMJ 317: 241–245
Leon, D.A., Johansson, M., Rasmussen, F. (2000)“Gestational Age and Growth Rate of Fetal Massare Inversely Associated with Systolic Blood Pres-sure in Young Adults: an Epidemiologic Study of165,136 Swedish Men Aged 18 Years” Am JEpidemiol 152: 597–604
Lever, A.F., Harrap, S.B. (1992) “Essential Hyper-tension, a Disorder of Growth With Origins inChildhood?” J Hypertens 10: 101–120
Levitt, N.S., Steyn, K., de Wet, T., Morrell, C.,Edwards, R., Ellison, G.T., Cameron, N. (1999) “AnInverse Relation Between Blood Pressure and BirthWeight Among 5 year old Children from Soweto,South Africa” J Epidemiol Community Health 53:264–268
Levitt, N.S., Lambert, E.V., Woods, D., Hales, C.N.,Andrew, R., Seckl, J.R. (2000) “Impaired GlucoseTolerance and Elevated Blood Pressure in LowBirth Weight, Nonobese, Young South AfricanAdults: Early Programming of Cortisol Axis” JEndocrinol Metab 85 (12) 4611–4618
Lithell, H.O., McKeigue, P.M., Berglund, L.,Mohsen, R., Lithell, U-B., Leon, D.A. (1996) “Rela-tion of Size at Birth to Non-Insulin Dependent Dia-
betes and Insulin Concentrations in Men aged 50–60 Years” BMJ 312: 406–410
Longo-Mbenza, B., Ngiyulu, R., Bayekula, M., Vita,E.K., Nkiabungu, F.B., Seghers, K.V., Luila, E.L.,Mandundu, F.M., Manzanza, M. (1999) “Low BirthWeight and Risk of Hypertension in African SchoolChildren” J Cardiovasc Risk 6: 311–314
Lopez, A. (1999) “Alcohol and Smoking as RiskFactors” in Health and Mortality Issues of GlobalConcern XVII: 374–411
Lubree, F.H., Rege, S.S., Bhat, D.S., Raut, K.N.,Panchanadikar, A.S., Joglekar, C.V., Yajnik, C.S.,Shetty, P., Yudkin, P. (2001) “Body Fat and Cardio-vascular Risk Factors in Men in Three Geographi-cal Locations” Ann Nutr Metab 45 (suppl) : 358
Lucas, A., Fewtrell, M.S., Cole, T.J. (1999) “FetalOrigins of Adult Disease—The Hypothesis Revis-ited” BMJ 319: 245–249
Ludwig, D.S., Pereira, M.A., Kroenke, C.H., Hilner,J.E., Van Horn, L., Slattery, M.L., Jacobs, D.R.(1999) “Dietary Fiber, Weight Gain, and Cardiovas-cular Disease Risk Factors in Young Adults” JAMA282: 1539–1549
Ludwig, D.S., Peterson, K.E., Gortmaker, S.L.(2001) “Relation Between Consumption of Sugar-Sweetened Drinks and Childhood Obesity: aProspective, Observational Analysis” Lancet 357:505–508
Luepker, R.V., Rosamond, W.D., Murphy, R.,Sprafka, J.M., Folsom, A.R., McGovern, P.G.,Blackburn, H. (1993) Socioeconomic Status andCoronary Heart Risk Factor Trends. The Minne-sota Heart Survey” Circulation 88: 2171–2179
Lynch, J.W. (2000) “Socioeconomic Factors in theBehavioral and Psychosocial Epidemiology ofCardiovascular Disease” in: N. Schneiderman, J.Gentry, J.M. da Silva, M. Speers, and H. Tomes(eds.) Integrating Behavioral and Social Sciences withPublic Health. Washington, DC.: APA Press, pp: 51–71.
Lynch, J.W., Kaplan, G.A., Cohen, R.D.,Tuomilehto, J., Salonen, J.T. (1996) “Do Cardio-vascular Risk Factors Explain the Relation BetweenSocioeconomic Status, Risk of All-Cause Mortal-ity, Cardiovascular Mortality, and Acute Myocar-dial Infarction?” Am J Epidemiol 144: 934–942
Lynch, J.W., Kaplan, G.A., Salonen, J.T. (1997)“Why do Poor People Behave Poorly? Variation inAdult Health Behaviours and Psychosocial Char-acteristics by Stages of the SocioeconomicLifecourse” Soc Sci Med 44: 809–819
MacMahon, S., Peto, R., Cutler, J., Collins, R.,Sorlie, P., Neaton, J., Abbott, R., Godwin, J., Dyer,A., Stamler, J. (1990) “Blood Pressure, Stroke, and
61
Coronary Heart Disease. Part 1. Prolonged Differ-ences in Blood Pressure: Prospective ObservationalStudies Corrected for the Regression Dilution Bias”Lancet 335: 765–774
Magarey, A.M., Daniels, L.A., Boulton, T.J.,Cockington, R.A. (2001) “Does Fat Intake PredictAdiposity in Healthy Children and AdolescentsAged 2–15 y? A Longitudinal Analysis” Eur J ClinNutr 55: 471–481
Mahoney, L.T., Lauer, R.M., Lee, J., Clarke, W.R.(1991) “Factors Affecting the Tracking of CoronaryHeart Disease Risk Factors in Children. TheMuscatine Study” Ann N Y Acad Sci 623: 120–132
Manhem, K., Dotevall, A., Wilhelmsen, L.,Rosengren, A. (2000) “Social Gradients in Cardio-vascular Risk Factors and Symptoms of SwedishMen and Women: The Goteborg MONICA Study” JCardiovasc Risk 7: 259–368
Margetts, B.M., Rowland, M.G.M., Foord, F.A.,Cruddas, A.M., Cole, T.J., Barker, D.J.P. (1991) “TheRelation of Maternal Weight to the Blood Pressureof Gambian Children” Int J Epidemiol 20: 938–943
Marmot, M. (1989) “Socioeconomic Determinantsof CHD Mortality” Int J Epidemiol 18: (3 suppl 1)S196–S202
Marmot, M.G., Bosma, H., Hemingway, H.,Brunner, E., Stansfield, S. (1997) “Contributions ofJob Control and Other Risk Factors to Social Vari-ations in Coronary Heart Disease Incidence”Lancet 350: 235–239
Martorell, R. (1995) “Results and Implications ofthe INCAP Follow-up Study” J Nutr 125 (suppl.4)1127S–1138S
Martorell, R., Ramakrishnan, U., Schroeder, D.G.,Melgar, P., Neufeld, L. (1998) “Intrauterine GrowthRetardation, Body Size, Body Composition andPhysical Performance in Adolescence” Eur J ClinNutr 51: S43–S53
Martorell, R., Kettel-Khan, L., Hughes, M.L.,Gummer-Strawn, L.M. (2000a) “Obesity in Womenfrom Developing Countries” Eur J Clin Nutr 54:242–252
Martorell, R., Kettel-Khan, L., Hughes, M.L.,Gummer-Strawn, L.M. (2000b) “Overweight andObesity in Preschool Children from DevelopingCountries” Int J Obes Relat Disord 24: 959–967
Martorell, R., Stein, A.D., Schroeder, D.G. (2001)“Early Nutrition and Later Adiposity” J Nutr 131:874S–880S
Martyn, C.N., Barker, D.J.P., Osmond, C.(1996)“Mother’s Pelvic Size, Fetal Growth and Death fromStroke and Coronary Heart Disease in Men in theUK” Lancet 348: 1264–1268
Martyn, C.N., Greenwald, E.S. (1997) “ImpairedSynthesis of Elastin in Walls of Aorta and LargeConduit Arteries During Early Development as anInitiating Event in Pathogenesis of Systemic Hy-pertension” Lancet 350: 953–955
Maurer, K.R. (1985) “Plan and Operation of theHispanic Health and Nutrition Examination Sur-vey, 1982–84. United States Department of Healthand Human Services, Centers for Disease Controland Prevention, National Center for Health Statis-tics” Vital Health Stats 1:19 (PHS) 85–1321
McCance, D.R., Pettitt, D.J., Hanson, R.L., Jacob-son, L.T.H., Knowler, W.C., Bennett, P.H. (1994)“Birthweight and Non-Insulin dependent Diabetes:Thrifty Genotype, Thrifty Phenotype or SurvivingSmall Baby Genotype?” BMJ 308: 942–945
McCarron, P., Davey Smith, G., Okasha, M.,McEwen, J. (1999) “Life Course Exposure and LaterDisease: A Follow-up Study Based on Medical Ex-aminations Carried Out in Glasgow University(1948–1968) Public Health 113: 265–271
McCarron, P., Smith , G.D., Okasha, M., McEwen,J. (2000a) “Blood Pressure in Young Adulthood andMortality from Cardiovascular Disease” Lancet 355:1430–1431
McCarron, P., Greenwood, R., Ebrahim, S., Elwood,P., Davey Smith, G. (2000b) “Adult Height is In-versely Associated with Ischaemic Stroke. TheCaerphilly and Speedwell Collaborative Studies”J. of Epidemiol Community Health 54: 239–240
McCarron, P., Hart, C.L., Davey Smith, G. (2001a)“The Relation Between Adult Height andHaemmorrhagic and Ischaemic Stroke in theRenfew/Paisley Study” J Epidemiol CommunityHealth 55: 404–405
McCarron, P., Davey Smith, G., Okasha, M.,McEwen, J. (2001b) “Smoking in Adolescence andYoung Adulthood and Mortality in Later Life: Pro-spective Observational Study” J Epidemiol Commu-nity Health 55: 334–335
McKeigue, P.M. (1996) “Metabolic Consequencesof Obesity and Body Fat Pattern: Lessons fromMigrant Studies” in D.J. Chadwick and G.C.Cardew (eds) The Origins and Consequences ofObesity. Chichester: Wiley, pp54–67 (Ciba Foun-dation Symposium 201)
McKeigue, P.M. (1997) “Diabetes and InsulinAction” in D. Kuh and Y. Ben-Shlomo (eds) A LifeCourse Approach to Chronic Disease Epidemiology.Oxford: Oxford University Press, pp. 78–100
Mi, J., Law, C.M., Zhang, K-L., Osmond, C., Stein,C.E., Barer, D.J.P. (2000) “Effects of InfantBirthweight and Maternal Body Mass Index in Preg-nancy on Components of the Insulin ResistanceSyndrome in China” Ann Intern Med 132: 253–260
BIBLIOGRAPHY
62
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
Miller, J.E., Korenman, S. (1994) “Poverty andChildren’s Nutritional Status in the United States”Am J Epidemiol 140 (3) 233–243
Ministry of Health, Tanzania (1997) “Policy Impli-cations of Adult Morbidity and Mortality: End ofPhase 1 Report. Ministry of Health, Dar-es-Salaam,Tanzania, August, 1997
Miura, K., Daviglus, M.L., Dyer, A.R., Liu, K.,Garside, D.B., Stamler, J., Greenland, P. (2001) “Re-lationship of Blood Pressure to 25-Year MortalityDue to Coronary Heart Disease, CardiovascularDiseases and All Causes in Young Adult Men” ArchIntern Med 161: 1501–1508
Mokdad, A.H., Bowman, B.A., Ford, E.S., Vinicor,Marks, J.S., Koplan, J.P. (2001) “The ContinuingEpidemics of Obesity and Diabetes in the UnitedStates” JAMA 286: 1195–1200
Monteiro, C.A., Mondini, L., Medeiros de Souza,A.L., Popkin, B.M. (2000) “Shifting Obesity Trendsin Brazil” Eur J Clin Nutr 54: 342–346
Montgomery, S.M., Bartley, M.J., Cook, D.G.,Wadsworth, M.E.J. (1996) “Health and Social Pre-cursors of Unemployment in Young Men in GreatBritain” J. of Epidemiology and Community Health50: 415–422
Morley, R., Harland, P.S.E.G., Law, C.M., Lucas,A. (2000) “Birthweight and Social Deprivation: In-fluences on Serum Lipids and Fibrinogen” ActaPaediatr 89: 703–707
Muller, M.J., Koertzinger, I., Mast, M., Langnase,K., Grund, A., Koertzinger, I. (1999) “Physical Ac-tivity and Diet in 5 to 7 years Old Children” PublicHealth Nutr 2: 443–444
Murray, C.J.L., Lopez, A.D. (eds) (1996) TheGlobal Burden of Disease. A ComprehensiveAssesment of Mortality and Disability from Disease,Injury and Risk Factors in 1990 and Projected to 2020.World Health Organization, Geneva
Must, A., Jacques, P.F., Dallal, G.E., Bajema, C.J.,Dietz, W.H. (1992) “Long-Term Morbidity and Mor-tality of Overweight Adolescents. A Follow-Up ofthe Harvard Growth Study” NEJM 327: 1350–1355
Myllykangas, M., Pekkanen, J., Rasi, V., Haukkala,A., Vahtera, E., Salomaa, V. (1995) “Haemostaticand Other Cardiovascular Risk Factors, and Socio-economic Status Among Middle Aged FinnishMen” Int J Epidemiol 24: 1110–1116
Navas-Nacher, E.L., Colangelo, L., Beam, C., Green-land, P. (2001) “Risk Factors for Coronary HeartDisease in Men 18 to 39 Years of Age” Ann InternMed 134: 433–439
Neaton, J.D., Wentworth, D. (1992) “Serum Cho-lesterol, Blood Pressure, Cigarette Smoking, and
death from Coronary Heart Disease: Overall Find-ings and Differences by Age for 316, 099 WhiteMen” Arch Intern Med 152: 56–64
Njølstad, I., Arnesen, E., Lund-Larsen, P.G. (1996)“Body Height, Cardiovascular Risk Factors, andRisk of Stroke in Middle-aged Men and Women”Circulation 94(11): 2877–2882
North, K., Emmett, P., and the Avon LongitudinalStudy of Pregnancy in Childhood (ALSPAC) StudyTeam (2000) “Multivariate Analysis of the DietAmong Three-Year-Old Children and Associationswith Socio-Demographic Characteristics” Eur J ClinNutr 54: 73–80
Okasha, M., McCarron, P., McEwen, J., DaveySmith, G. (2000) “Determinants of AdolescentBlood Pressure: Findings from the Glasgow Uni-versity Student Cohort” J Hum Hypertension 14:117–124
Okosun, I.S., Forrester, T.E., Rotimi, C.N.,Osotimejin, B.O., Muna, W.F., Cooper, R.S. (1999)“Abdominal Adiposity in Six Populations of WestAfrican Descent : Prevalence and Population At-tributable Fraction of Hypertension” Obes Res 7:453–462
Olatunbosun, S.T., Bella, A.F. (2000) “RelationshipBetween Height, Glucose Intolerance, and Hyper-tension in an Urban African Black Adult Popula-tion: A Case for the ‘Thrifty Phenotype ’Hypothesis?” J Natl Med Assoc 92 (6) 265–268
Ong, K.L., Ahmed, M.L., Emmett, P.M., Preece,M.A., Dunger, D.B., and the ALSPAC Study Team(2000) “Association Between Postnatal Catch-UpGrowth and Obesity in Childhood: ProspectiveCohort Study BMJ 320: 967–971
Osmond, C., Barker, D.J.P., Winter, P.D., Fall,C.H.D., Simmonds, S.J. (1993) “Early Growth andDeath from Cardiovascular Disease in Women”BMJ 307: 1519–1524
Ounpuu, S., Negassa, A., Yusuf, S. (2000) “INTER-HEART: A Global Strategy for Risk Factors for AcuteMyocardial Infarction” Am. Heart J 141: 711–721
Paffenbarger, R.S., Williams, J.L. (1967) “ChronicDisease in Former College Students V. Early Pre-cursors of Fatal Stroke” Am J Public Health 57: 1290–1299
Paffenbarger, R.S., Wing, A.L. (1969) “Chronic Dis-ease in Former College Students X. The Effects ofSingle and Multiple Characteristics on Risk of Fa-tal Coronary Heart Disease” Am J Epidemiol 90:527–535
Paffenbarger, R.S., Wing, A.L. (1971) “Chronic Dis-ease in Former College Students XI. Early Precur-sors of Nonfatal Stroke” Am J Epidemiol 94 (6) :524–530

63
Pais, P., Pogue, J., Gerstein, H., Zachariah, E.,Savitha, D., Jayprakash, S., Nayak, P.R., Yusuf,S.(1996) “Risk Factors for Acute Myocardial Infarc-tion in Indians: A Case-Control Study” Lancet 348:358–363
Parsons, T.J., Power, C., Manor, O. (2001) “Fetaland Early Life Growth and Body Mass Index fromBirth to Early Adulthood in 1958 British Cohort”BMJ 323: 1331–1335
Peck, M.N. (1992) “Childhood Environment,Intergenerational Mobility and Adult Health: Evi-dence from Swedish Data” J Epidemiol CommunityHealth 46: 71–74
Peck, M.N. and Lundberg, O. (1995) “Short Statureas an Effect of Economic and Social Conditions inChildhood” Soc Sci Med 41: 733–738
Pena, M., Bacallao, J. (2000) Obesity and Poverty.A New Public Health Challenge. PAHO, Washington
Perova, N.V., Davis, C.E., Tao, S., Pajak, A., Stein,Y., Broda, G.B., Li, Y., Tyroler, H.A. (2001) “Multi-Country Comparison of Plasma Lipid Relationshipto Years of Schooling in Men and Women” Int JEpidemiol 30: 371–379
Peto, R. (1996) “Tobacco: The Growing Epidemicin China” JAMA 275: 1683–1684
Pettit, D.J., Knowler, W.C. (1998) “Long-TermEffects of the Intrauterine Environment, BirthWeight, and Breast Feeding in Pima Indians” Dia-betes Care 21: B138–B141
Phillips, D.I.W. (1993) “Twin Studies in MedicalResearch: Can They Tell Us Whether Diseases AreGenetically Determined?” Lancet 341: 1008–1009
Phillips, D.I.W., Barker, D.J.P., Hales, C.N., Hirst,S., Osmond, C. (1994) “Thinness at Birth and In-sulin Resistance in Adult Life” Diabetologia 37: 592–596
Phillips, D.I.W., McLeish, R., Osmond, C., Hales,C.N.(1995) “Fetal Growth and Insulin Resistancein Adult Life: Role of Plasma Triglyceride andNonesterified Fatty Acids” Diabet Med 12: 796–801
Phillips, D.I.W. (1999) “The ‘Fetal Origins’ Hypoth-esis: Role of Programming of Adrenocortical andSympathoadrenal Function” in P.M.S. O’Brien,T.Wheeler and D.J.P. Barker (eds) Fetal Program-ming: Influences on Development and Disease in laterLife. London: RCOG Press, pp 414–423
Phipps, K., Barker, D.J.P., Hales, C.N., Fall, C.H.D.Osmond, C., Clark, P.M.S. (1993) “Fetal Growth andImpaired Glucose Tolerance in Men and Women “Diabetologia 36: 225–228
Pickering, T.G. (2001) “Why is Hypertension MoreCommon in African Americans?” J Clin Hyperten-sion 3: 50–52
Pinhas-Hamiel, O., Dolan, L.M., Daniels, S.R.,Standiford, D., Khoury, P.R., Zeitler, P. (1996)“Increased Incidence of Non-Insulin-DependentDiabetes Mellitus Among Adolescents” J Pediatr128: 608–615
Pi-Sunyer, F.X. (1991) “Health Implications of Obes-ity” Am J Clin Nutr 53 (Suppl) 1595S–1603S
Popkin, B. (1994) “The Nutrition Transition in LowIncome Countries: an Emerging Crisis” Nutr Rev52: 285–298
Popkin, B.M., Richards, M.K., Monteiro, C.A. (1996)“Stunting is Associated with Overweight in Chil-dren of Four Nations that are Undergoing theNutrition Transition” J Nutr 126: 3009–3016
Popkin, B.M. (2001) “The Nutrition Transition andObesity in the Developing World” J Nutr 131: 871S–873S
Poulsen, P., Vaag, A.A., Kyvik, K.O., Moller Jensen,D., Beck-Nielsen, H. (1999) “Low Birth Weight isAssociated with NIDDM in Discordant Monozy-gotic and Dizygotic Twin Pairs” Diabetologia 40:439–446
Poulter, N.R., Chang, C.L. “MacGregor, A.J.,Snieder, H., Spector, T.. (1999) “Association Be-tween Birth Weight and Adult Blood Pressure inTwins: Historical Cohort Study” BMJ 319: 1330–1333
Power, C., Moynihan, C. (1988) “Social ClassChanges and Weight-for-Height Between Child-hood and Early Adulthood” Int J Obesity 12: 445–453
Power, C., Matthews, S. (1997) “Origins of HealthInequalities in a National Population Sample”Lancet 350: 1584–1589
Psaty, B.M., Furberg, C.D., Kuller, L.H., Cushman,M., Savage, P.J., Levine, D., O’Leary, D.H., Bryan,R.N., Anderson, M., Lumley, T. (2001) “Associa-tion Between Blood Pressure Level and the Riskof Myocardial Infarction, Stroke and Total Mortal-ity: The Cardiovascular Health Study” Arch InternMed 161: 1183–1192
Raitakari, O.T., Porkka, K.V., Viikari, J.S., Ronnema,T., Akerblom, H.K. (1994a) “Clustering of Risk Fac-tors for Coronary Heart Disease in Children andAdolescents. The Cardiovascular Risk in YoungFinns Study” Acta Paediatr 83: 935–940
Raitakari, O.T., Porkka, K.V., Rasanen, L.,Ronnema, T., Viikari, J.S. (1994b) “Clustering ofRisk Factors for Coronary Heart Disease in Chil-dren and Adolescents. The Cardiovascular Risk inYoung Finns Study” Acta Paediatr 83: 935–940
Raitakari, O.T., Porkka, K.V., Rasanen, L., Viikari,J.S. (1994c) “Relations of Life-Style with Lipids,Blood Pressure and Insulin Adolescents and Young
BIBLIOGRAPHY

64
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
Adults. The Cardiovascular Risk in Young FinnsStudy” Atherosclerosis 111: 237–246
Raitakari, O.T., Taimela, S., Porkka, K.V., Telama,R., Valimaki, I., Akerblom, H.K., Viikari, J.S. (1997)“Associations Between Physical Activity and RiskFactors for Coronary Heart Disease: the Cardio-vascular Risk in Young Finns Study” Med Sci SportsExerc 29: 1055–1061
Ravelli, A.C.J., van der Meulen, J.H.P., Michels,R.P.J., Osmond, C., Barker, D.J.P., Bleker, O.P.(1998) “Glucose Tolerance in Adults After Prena-tal Exposure to Famine” Lancet 351: 173–177
Ravelli, A.C., van der Meulen, J.H., Osmond, C.,Barker, D.J.P., Bleker, O.P. (2000) “Infant Feedingand Adult Glucose Tolerance, Lipid Profile, BloodPressure, and Obesity” Arch Dis Child 82: 248–252
Reaven, G.M. (1988) “Role of Insulin Resistancein Human Disease” Diabetes 37: 1595–1607
Resnicow, K., Wang, T., Dudley, W.N., Jackson, A.,Ahluwalia, J.S., Baranowski, T., Braithwaite, R.L.(2001) “Risk Factor Distribution amongSociodemographically Diverse African AmericanAdults” J Urban Health 78: 125–140
Reynolds, R.M., Walker, B.R., Syddall, H.E.,Andrew, R., Wood, P.J., Whorwood, C.B., Phillips,D.I.W. (2000) “Altered Control of Cortisol Secre-tion in Adult Men with Low Birth Weight and Car-diovascular Risk factors” J Clin Endocrinol Metab86: 245–250
Rich-Edwards, J.W., Stampfer, M.J., Manson, J.E.,Rosner, B., Hankinson, S.E, Colditz, G.A., Willett,W.C., Hennekens, C.H. (1997) “Birth Weight andRisk of Cardiovascular Disease in a Cohort ofWomen Followed Up since 1976” BMJ 315: 396–400
Rich-Edwards, J.W., Colditz, G.A., Stampfer, M.J.,Willett, W.C., Gillman, M.W., Hennekens, C.H.,Speizer, F.E., Manson, J.E. (1999) “Birth Weight andthe Risk of Type 2 Diabetes Mellitus in AdultWomen” Ann Intern Med 130: 278–284
Robinson, S., Walton, R.J., Clark, P.M., Barker,D.J.P., Hales, C.N., Osmond, C. (1992) “The Rela-tion of Fetal Growth to Plasma Glucose in YoungMen” Diabetologia 35: 444–446
Robinson, T.N. (1999) “Reducing Children’s Televi-sion Viewing to Prevent Obesity: a RandomizedControlled Trial” JAMA, 282: 1561–1567
Robinson, T.N. (2001) “Television Viewing andChildhood Obesity” Pediatr Clin North Am 48: 1017–1025
Roseboom, T.J., van der Meulen, J.H.P., Osmond,C., Barker, D.J.P., Ravelli, A.C.J., Schroeder-Tanka,J.M., van Montfrans, G.A., Michels, R.P.J., Bleker,
O.P. (2000a) “Coronary Heart Disease After Pre-natal Exposure to the Dutch Famine 1944-45” Heart84(6):595–598
Roseboom, T.J., van der Meulen, J.H., Osmond,C., Barker, D.J., Ravelli, A.C., Bleker, O.P. (2000b)“Plasma Lipid Profiles in Adults after Prenatal Ex-posure to the Dutch Famine” Am J Clin Nutr 72:1101–1106
Roseboom, T.J., van der Meulen, J.H:, vanMontfrans, G.A., Ravelli, A.C., Osmond, C., Barker,D.J., Bleker, O.P. (2001) “Maternal Nutrition Dur-ing Gestation and Blood Pressure in Later Life” JHypertens 19: 29–34
Rosner B., Prineas R., Daniels S.R., Loggie J. (2000)“Blood Pressure Differences Between Blacks andWhites in Relation to Body Size Among US Chil-dren and Adolescents” Am J Epidemiol. 151:1007–1019
Sapolsky, R.M. (1996) “Why Stress Is Bad for YourBrain” Science 273: 749–750
Sawaya, A.L., Dallal, G., Slymos, G.M., Souza,M.H., Ventura, M.L., Roberts, S.B., Sigulem, D.M.(1995) “Obesity and Malnutrition in a ShantytownPopulation in the City of Sao Paulo, Brazil” ObesRes 3 (suppl. 2) 107S–115S
Sawaya, A.L., Grillo, L.P., Verreschi, I., da Silva,A.C., Roberts, S.B. (1999) “Mild Stunting is Associ-ated with Higher Susceptibility to the Effects ofHigh Fat Diets: Studies in a Shantytown Popula-tion in Sao Paulo, Brazil” J Nutr 128: 415S–420S
Schlosser, E. (2001) Fast Food Nation. London: Pen-guin
Schroeder, D.G., Martorell, R., Flores, R. (1999)“Infant and Child Growth and Fatness and Fat Dis-tribution in Guatemalan Adults” Am J Epidemiol149: 177–185
Shaper, A., Wannamethee, S.G., Walker, M. (1997)“Body Weight. Implications for the Prevention ofCoronary Heart Disease, Stroke and DiabetesMellitus in a Cohort of Middle-Aged Men” BMJ 314:1311–1317
Sichieri, R., Siqueira, K.S., Moura, A.S. (2000)“Obesity and Abdominal Fatness Associated withUndernutrition Early in Life in a Survey in Rio deJaneiro” Int J Obes Relat Metab Disord 24: 614–618
Silventoinen, K., Kaprio, J., Lahelma, E.,Koskenvuo, M. (2000) “Relative Effect of Geneticand Environmental Factors on Body Height: Dif-ferences Across Birth Cohorts Among Finnish Menand Women” Am J Public Health 90 (4): 627–630
Simell, O., Niinikoski, H., Viikari, J., Rask-Nissilä,L., Tammi, A., Rönnemaa, T. (1999) “Cardiovascu-lar Disease Risk Factors in Young Children in theSTRIP Baby Project” Ann Med 31 Suppl. 1: 55–61
65
Singhal, A., Cole, T.J., Lucas, A. “Early Nutritionin Preterm Infants and Later Blood Pressure: TwoCohorts After Randomized Trials” Lancet 357: 413–419
Sjol, A., Thomsen, K.K., Schroll, M. (1998) “Secu-lar Trends in Blood Pressure Levels in Denmark1964–1991” Int J Epidemiol 27: 614–622
Sobal, J., Stunkard, J. (1989) “Socioeconomic Sta-tus and Obesity. A Review of the Literature”Psychol Bull 105: 260–275
Sorensen, H.T., Sabroe, S., Rothman, K.J., Gillman,M., Steffensen, F.H., Fischer, P., Sorensen, T.I.(1999) “Birth Weight and Length as Predictor forAdult Height” Am J Clin Nutr 149: 726–729
Srinivasan, S.R., Myers, L., Berenson, G.S. (2001)“Rate of Change in Adiposity and Its Relationshipto Concomitant Changes in Cardiovascular RiskVariables Among Biracial (Black-White) Childrenand Young Adults: The Bogalusa Heart Study”Metabolism 50: 299–305
Stanner, S.A., Bulmer, K., Andrés, C., Lantsena,O.E., Borodina, V., Poteen, V.V., Yudkin, J.S. (1997)“Malnutrition in Utero as a Determinant of Diabe-tes and Coronary Heart Disease in Adult Life: TheLeningrad Siege Study” BMJ 315: 173–177
Stein, C.E., Fall, C.H.D., Kunaran, K., Osmond, C.,Cox, V., Barker, D.J.P. (1996) “Fetal Growth andCoronary Heart Disease in South India” Lancet 348:1269–1273
Sterne, J.A.C., Davey Smith, G., Leon, D.A.,Tynelius, P., Rasmussen, F. (2001) “Fetal Growth isAssociated with Parents’ Cardiovascular Mortality:Record Linkage Study” Pediatric Research (in press)Supplement, Abstract FC9/4.
Stettler, N., Tershakovec, A.M., Zemel, B.S.,Leonard, M.B., Boston, R.C., Katz, S.H., Stallings,V.A. (2000) “Early Risk Factors for Increased Adi-posity: A Cohort Study of African American Sub-jects Followed From Birth to Young Adulthood” AmJ Clin Nutr 72: 378–383
Szklo, M., Chambless, L.E., Folsom, A.R., Gotto,A., Nieto, F.J., Patsch, W., Shimakawa, T., Sorlie,P., Wijnberg, L. (2000) “Trends in Plasma Choles-terol Levels in the Atherosclerosis Risk in Com-munities (ARIC) Study” Preventive Medicine 30:252–259
Tan, F., Okamoto, M., Suyams, A., Miyatomo, T.(2000) “Tracking of Cardiovascular Risk Factors anda Cohort Study on Hyperlipidemia in Rural School-children in Japan” J Epidemiol 10: 255–261
Tenhola, S., Martikainen, A., Rahiala, E., Herrgard,E., Halonen, P., Voutilainen, R. (2000) “SerumLipid Concentrations and Growth Characteristics
BIBLIOGRAPHY
in 12-Year-Old Children Born Small for GestationalAge” Pediatr Res 48: 623–628
Tershakovec, A.M., Jawad, A.F., Stallings, V.A.,Cortner, J.A., Zemel, B.S., Shannon, B.M. (1998)“Age-Related Changes in Cardiovascular DiseaseRisk Factors of Hypercholesteraemic Children”J Pediatr 132: 414–420
Thorne, M.C., Wing, A.L., Paffenbarger, R.S. (1968)“Chronic Disease in Former College Students VII.Early Precursors of Nonfatal Coronary Heart Dis-ease” Am J Epidemiol 87: 520–529
Torun, B. (2000) “Physical Activity Patterns in Cen-tral America” in M. Pena and J. Bacallao (eds)Obesity and Poverty. A New Public Health Challenge.PAHO, Washington, pp29–38
Troiano, R.P., Flegal, K.M., Kuczmarski, R.J.,Campbell, S.M., Johnson, C.L. (1995) “OverweightTrends and Prevalence for Children and Adoles-cents. The National Health and Nutrition Exami-nation Survey” Arch Pediatr Adolesc Med 149:1085–1091
Tuomilehto, J., Lindstrom, J., Eriksson, J.G., Valle,T.T., Hamalainen, H., Ilanne-Parika, P., Keinanen-Kiukaanniemi, S., Laakso, M., Louheranta, A., Ras-tas, M., Salminen, V., Uusitupa, M., Aunola, S.,Cepaitis, Z., Moltchanov, V., Hakumaki, M.,Mannelin, M., Martikkala, V., Sundvall, J. (2001)“Prevention of Type 2 Diabetes Mellitus byChanges in Lifestyle Among Subjects with Im-paired Glucose Tolerance” NEJM 344: 1343–1350
Twisk, J.W., Boreham, C., Cran, Savage, J.M.,Strain, J., van Mechelen, W. (1999) “Clustering ofBiological Risk Factors for Cardiovascular Diseaseand the Longitudinal Relationship with Lifestyleof an Adolescent Population: the Northern IrelandYoung Hearts Project” J Cardiovasc Risk 6: 355–362
Twisk, J.W.R., Kemper, H.C.G., van Mechelen, W.(2000) “Tracking of Activity and Fitness and theRelationship with Cardiovascular Disease RiskFactors” Med Sci Sports Exerc 32: 1455–1461
Vagero, D., Leon, D. (1994) “Ischaemic Heart Dis-ease and Low Birth Weight: a Test of the Fetal-Ori-gins Hypothesis from the Swedish Twin Registry”Lancet 343: 260–263
Valdez, R., Athens, M.A., Thompson, G.H.,Bradshaw, B.S., Stern, M.P. (1994) “Birthweight andAdult Health Outcomes in a Biethnic Populationin the USA” Diabetologia 35: 444–446
van der Sande, M.A., Milligan, P.J., Nyan, O.A.,Rowley, J.T., Banya, W.A., Ceesay, S.M., Dolmans,W.M., Thien, T., McAdam, K.P., Walraven, G.E.(2000) “Blood Pressure Patterns and Cardiovascu-lar Risk Factors in Rural and Urban Gambian Com-munities” J Hum Hypertension 14: 489–496
66
LIFE COURSE PERSPECTIVES ON CORONARY HEART DISEASE, STROKE AND DIABETES
Vanhala, M., Vanhala, P., Kumpusalo, E., Halonen,P., Takala, J. (1998) “Relation Between Obesity fromChildhood to Adulthood and the Metabolic Syn-drome: Population Based Study” BMJ 317: 319
Velho, G., Hattersley, A.T., Froguel, P. (2000) “Ma-ternal Diabetes Alters Birth Weight in Glucokinase-Deficient (MODY2) Kindred but Has no Influenceon Adult Weight, Height, Insulin Secretion or In-sulin Sensitivity” Diabetologia 43: 1060–1063
Von Kries, R:, Koletzko, B., Sauerwald, T., vonMutius, E., Barnert, D., Grunert, V., von Voss, H.(1999) “Breat Feeding and Obesity: Cross SectionalStudy” BMJ 319: 147–150
Walker, S.P., Gaskin, P., Powell, C.A., Bennett, F.I.,Forrester, T.E., Grantham-McGregor, S. (2001) “TheEffects of Birth Weight and Postnatal LinearGrowth on Blood Pressure at Age 11–12 Years”J Epidemiol Community Health 55: 394–398
Wannamethee, S.G., Whincup. P.H., Shaper, G.,Walker, M. (1996) “Influence of Fathers’ Social Classon Cardiovascular Disease in Middle Aged Men”Lancet 348: 1259–1263
Wannamethee, S.G., Shaper, A.G., Walker, M.(1998a) “Changes in Physical Activity, Mortalityand Incidence of Coronary Heart Disease in OlderMen” Lancet 351: 1603–1608
Wannamethee, S.G., Shaper, A.G., Whincup, P.H.,and Walker, M. (1998b) “Adult Height, Stroke andCoronary Heart Disease” Am. J. of Epidemiology148(11) 1069–1076
Warren, C.W., Riley, L., Asma, S., Eriksen, M.P.,Green, L., Blanton, C., Loo, C., Batchelor, S., Yach,D. (2000) “Tobacco Use by Youth: a SurveillanceReport from the Global Youth Tobacco SurveyProject” Bull World Health Organization 78: 868–876
Weintrob, N., Karp, M., Hod, M. (1996) “Short-andLong-Range Complications in Offspring of DiabeticMothers” J Diab Complications 10: 294–301
Whincup, P., Cook, D. (1997) “Blood Pressure andHypertension” in D.Kuh and Y. Ben-Shlomo (eds)A Life Course Approach to Chronic Disease Epide-miology. Oxford: Oxford University Press, pp.121–144
Whincup, P., Bredow, M., Payne, F., Sadler, S.,Golding, J., and the ALSPAC Study Team (1999)“Size at Birth and Blood Pressure at 3 Years of Age.The Avon Longitudinal Study of Pregnancy andChildhood (ALSPAC)” Am J Epidemiol 149: 730–739
Whitaker, R.C., Wright, J.A., Pepe, M.S., Seidel,K.D., Dietz, W.H. (1997) “Predicting Obesity inYoung Adulthood from Childhood and ParentalObesity” N Engl J Med 337: 869–873
Whitaker, R.C., Dietz, W.H. (1998) “Role of the Pre-natal Environment in the Development of Obes-ity” J Pediatr 132: 768–776
WHO (1990) Consultation for the First Global Analy-sis of Diet in Relation to Chronic Diseases. WorldHealth Organization Technical Report, Ser 1990;797
WHO (2000) Obesity: Preventing and Managing theGlobal Epidemic. Report of a WHO Consultation.World Health Organization, Geneva
WHO (2001a) Women and The TobaccoEpidemic.Challenges for the 21st Century. WorldHealth Organization, Geneva
WHO (2001b) Advancing Knowledge on RegulatingTobacco Products. World Health Organization, Ge-neva
Widdowson, E.M., Crabb, D.E., Milner, R.D.G.(1972) “Cellular Development of Some HumanOrgans Before Birth” Arch Dis Child 47: 652–655
Willett, W.C. (1994) “Diet and Health: What ShouldWe Eat?” Science 264: 532–537
Wilson, A.C., Forsyth, J.S., Greene, S.A., Irving,L., Hau, C., Howie, P.W. (1998) “Relation of InfantFeeding to Adult Serum Cholesterol Concentrationand Death From Ischaemic Heart Disease” BMJ316: 21–25
Woelk, G.B., Emanuel, I., Weiss, N.S., Psaty, B.M.(1998) “Birthweight and Blood Pressure AmongChildren in Harare, Zimbabwe” Arch Dis Child Fe-tal Neonatal Ed 79: F119–F122
Yach, D., Cameront, N., Padayachee, N., Wagstaff,L., Richter, L., Fonn, S. (1991) “Birth to Ten: ChildHealth in South Africa in the 1990s. Rationale andMethods of a Birth Cohort Study” Pediatr PerinatalEpid 5: 211–233
Yajnik, C., Fall, C.H., Vaidya, U., Pandit, A.N.,Bavdekar, A., Bhat, D.S., Osmond, C., Hales, C.N.,Barker, D.J.P. (1995) “Fetal Growth and Glucoseand Insulin Metabolism in 4 Year Old Indian Chil-dren” Diabet Med 12: 330–336
Yajnik, C.S. (2000) “Interactions of Perturbationsof Intrauterine Growth and Growth During Child-hood on the Risk of Adult-Onset Disease” Proc NutrSoc 59: 257–265
Yajnik, C.S. (2001) “The Insulin Resistance Epi-demic in India: Fetal Origins, Later Lifestyle, orBoth?” Nutr Rev 59: 1–9
Yang, X., Telama, R., Leino, M., Viikari, J. (1999)“Factors Explaining the Physical Activity of YoungAdults: the Importance of Early Socialization”Scand J Med Sci Sports 9: 120–127

67
BIBLIOGRAPHY
Yao, C., Wu, Z., Wu, J. (1993) “The Changing Pat-tern of Cardiovascular Diseases in China” WorldHealth Stat Q 46: 113–118
Yu, Z., Song, G., Guo, Z., Zheng, G., Tian, H.,Vartiainen, E., Puska, P., Nissinen, A (1999)“Changes in Blood Pressure, Body Mass Index andSalt Consumption in a Chinese Population” PrevMed 29: 165–172
Yu, Z., Nissinen, A., Vartiainen, E., Song, G., Guo,Z., Zheng, G., Tuomilehto, J., Tian, H. (2000) “As-sociation Between Socioeconomic Status and Car-diovascular Risk Factors in an Urban Populationin China” Bull World Health Organ 78: 1296–1305
Zimet, G.D., Owens, R., Dahms, W., Cutler, M.,Litvene, M., Cuttler, L. (1997) “Psychosocial Out-come of Children Evaluated for Short Stature”Arch Pediatr Adolesc Med 151: 1017–1023
Zizza, C., Siega-Riz, A.M., Popkin, B.M. (2001) “Sig-nificant Increases in Young Adults’ Snacking Be-tween 1977–78 and 1994–96 Represents a Causefor Concern! Prev Med 32: 303–319
Glossary of terms and abbreviations
68
AR Adiposity Rebound
BMI Body Mass Index
BP Blood Pressure
CAH Child and Adolescent Health
CHD Coronary Heart Disease
GDM Gestational Maternal Diabetes Mellitus
HDL-c High Density Lipoprotein Cholesterol
IGT Impaired Glucose Tolerance
IR Insulin Resistance
ID Insulin Deficiency
IUGR Intrauterine Growth Retardation
LBW Low Birth Weight
LDL-c Low Density Lipoprotein Cholesterol
NCD Noncommunicable Diseases
NPH Department of Noncommunicable Diseases Prevention & Health Promotion
SEP Socioeconomic Position
TG Triglycerides
WHR Waist to Hip Ratio
Ageing and Life CourseDepartment of Noncommunicable Diseases Prevention and Health Promotion
World Health OrganizationAvenue Appia 20
1211-Geneva-27Switzerland
e-mail: [email protected]: +41-22 791 3405
Fax: +41-22 791 4839