Embed Size (px)
Citation preview
Levercirrhose, hand-out college
Jan F. Monkelbaan,
Internist en MDL-arts
Afdeling MDL UMCU
Indeling
1. Anatomie2. Fysiology 3. Steatose4. Fibrose5. Cirrhose6. Complicaties van cirrhose7. Therapie8. Leverfalen
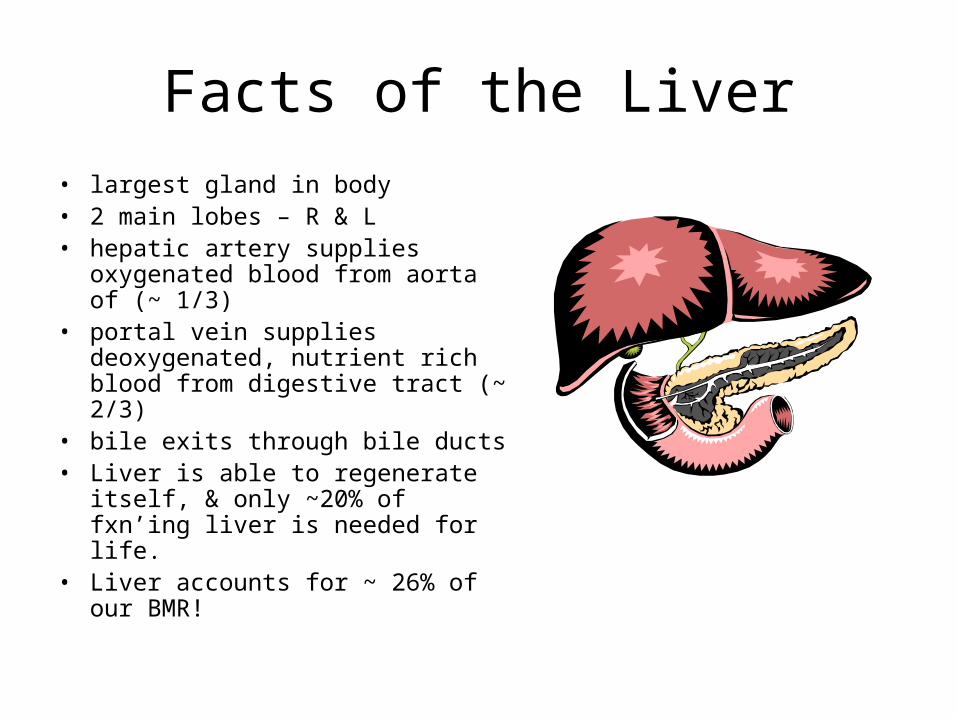
Facts of the Liver
• largest gland in body• 2 main lobes – R & L• hepatic artery supplies oxygenated
blood from aorta of (~ 1/3)• portal vein supplies deoxygenated,
nutrient rich blood from digestive tract (~ 2/3)
• bile exits through bile ducts • Liver is able to regenerate itself, &
only ~20% of fxn’ing liver is needed for life.
• Liver accounts for ~ 26% of our BMR!
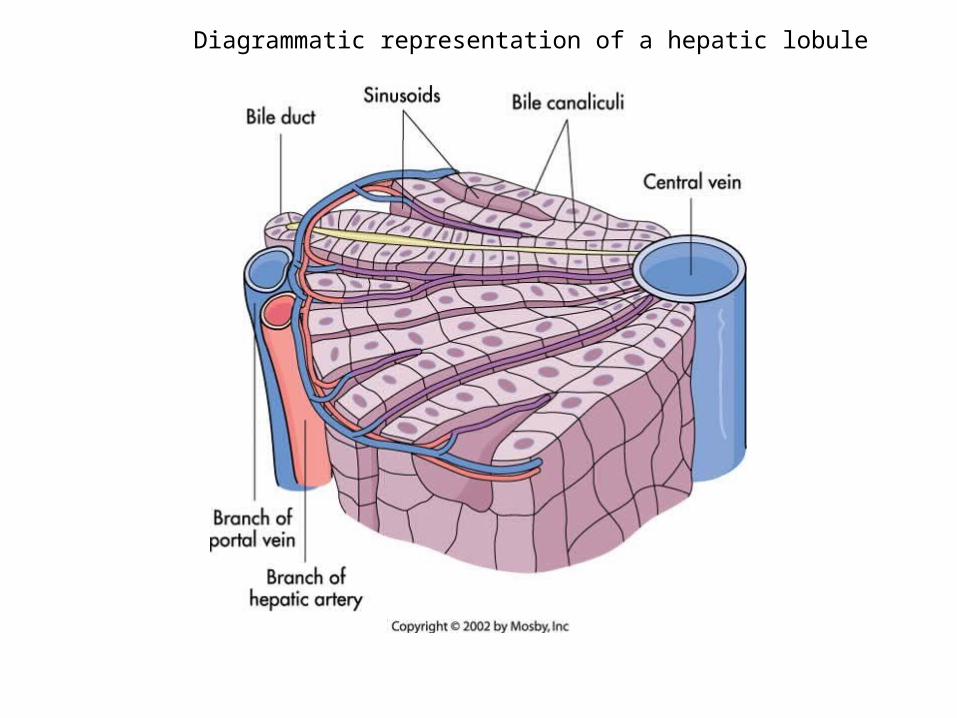
Diagrammatic representation of a hepatic lobule
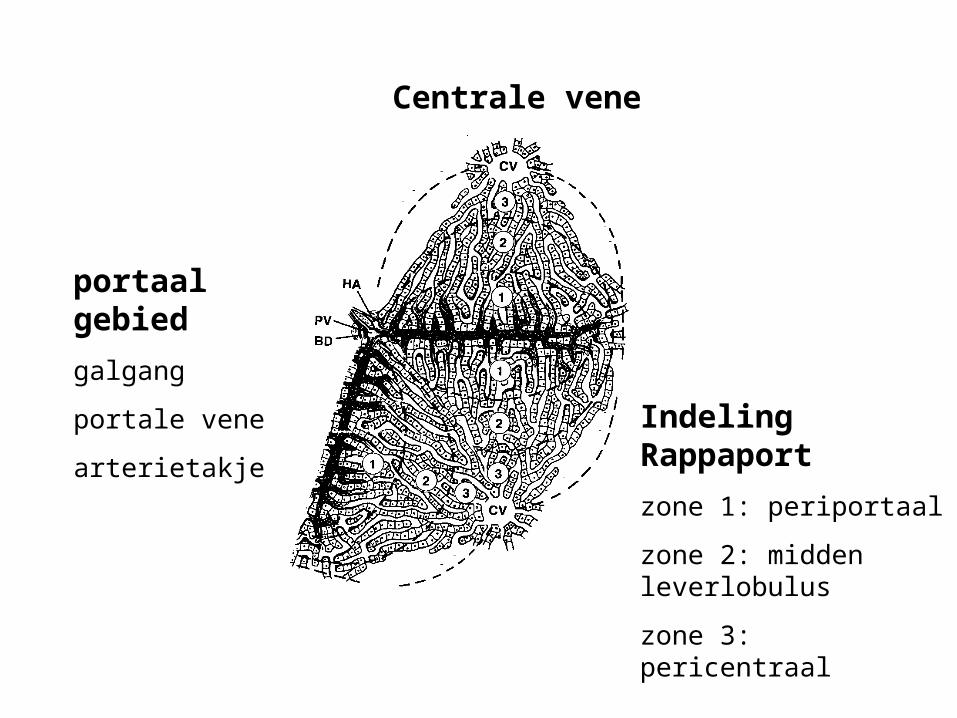
portaal gebied
galgang
portale vene
arterietakje
Centrale vene
Indeling Rappaport
zone 1: periportaal
zone 2: midden leverlobulus
zone 3: pericentraal
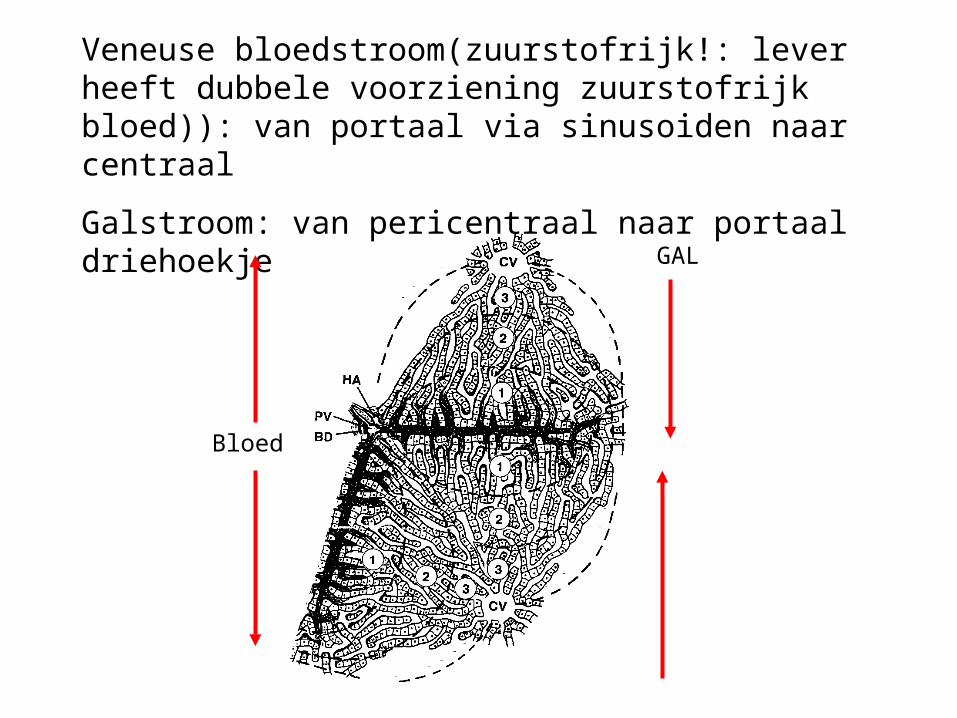
Veneuse bloedstroom(zuurstofrijk!: lever heeft dubbele voorziening zuurstofrijk bloed)): van portaal via sinusoiden naar centraal
Galstroom: van pericentraal naar portaal driehoekje
GAL
Bloed
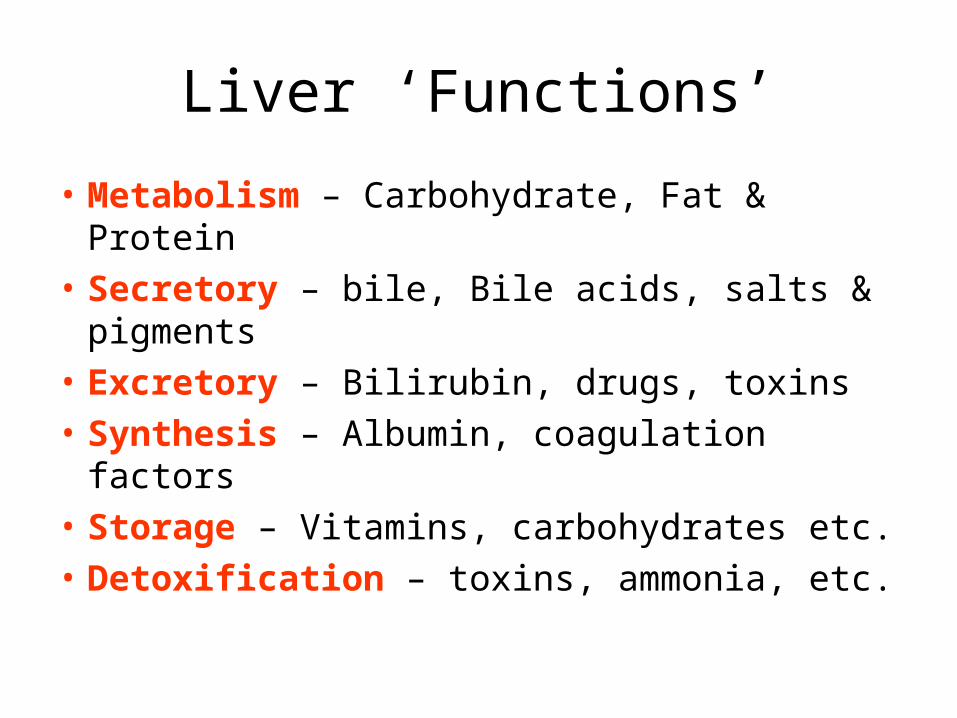
Liver ‘Functions’
• Metabolism – Carbohydrate, Fat & Protein
• Secretory – bile, Bile acids, salts & pigments
• Excretory – Bilirubin, drugs, toxins
• Synthesis – Albumin, coagulation factors
• Storage – Vitamins, carbohydrates etc.
• Detoxification – toxins, ammonia, etc.
Physiology of the Liver• produces ~ 1 quart of bile (water,
bile acids, bile salts, cholesterol, lecithin & billirubin)
• toxins are stored or detoxified, & steroids hormones are metabolized
• carbohydrate metabolism– glycogenesis– glycogenolysis– gluconeogenesis (from AA and
lactic acid)• lipid metabolism
– stores exogenous triglycerides– f.a. & TGA synthesis from glucose
and AA’s -oxidation– ketogenesis– lipoprotein synthesis for transport
of TAG & cholesterol– cholesterol synthesis (for
production of bile salts)
• protein metabolism– deamination of AA– conversion of ammonia (NH3) into
urea for excretion– synthesis of plasma proteins
(albumin, prothrombin, fibrinogen, transferrin, etc.)
– transamination (for synthesis of non-essential AA)
• storage– vitamin A– vitamin B12– vitamin D– vitamin E– vitamin K– iron & copper– zinc & magnesium
• activation of Vitamin D, vitamin A, & folate
• phagocytosis – of worn-out rbs & wbc & some bacteria
Common Laboratory Tests for Liver Function
• Hepatic excretion—Total serum
bilirubin, urine bilirubin
• Cholestasis tests—Serum alkaline
phosphatase• Hepatic enzymes
—ALT, AST
• Serum proteins—PT, PTT, serum
albumin• Markers of specific liver
diseases—Serum ferritin,
ceruloplasmin• Specific tests for viral
hepatitis—IgM anti-HAV, anti-
HBS, HCV-RNA
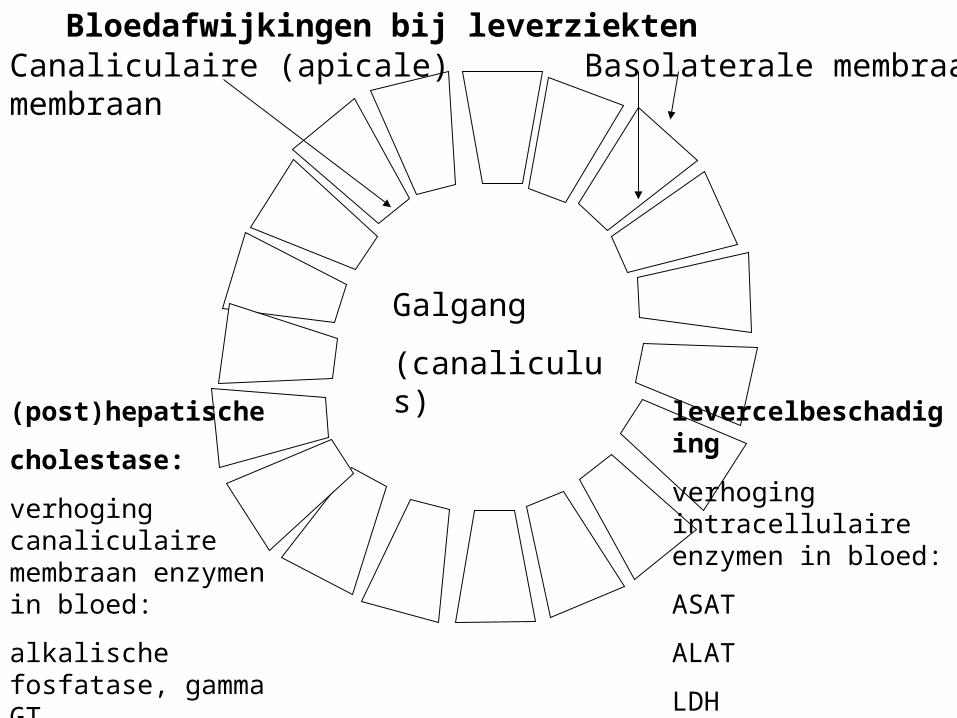
Galgang
(canaliculus)
Canaliculaire (apicale) membraan Basolaterale membraan
(post)hepatische
cholestase:
verhoging canaliculaire membraan enzymen in bloed:
alkalische fosfatase, gamma GT
(bilirubine)
levercelbeschadiging
verhoging intracellulaire enzymen in bloed:
ASAT
ALAT
LDH
(bilirubine)
Bloedafwijkingen bij leverziekten
Lever beschadiging
• Begrippen:• Hepatitis• Steatose• Fibrose• Cirrose
Fibrosis
• Response to inflammation or direct toxic insult• Initially, may be portal, pericentral, or sinusoidal• Eventually, fibrous tendrils link areas of the liver,
called bridging• Fibrosis is potential reversible; continuing injury
and fibrosis lead to nodules of regenerating hepatocytes surrounded by fibrous bands, termed CIRRHOSIS.
• Cirrosis is irreversible.
Pathophysiology Fibrose
• Slow, insidious, progressive, chronic• Fibrous bands replace normal liver
structure• Cell degeneration occurs• Liver attempts to regenerate cells but cells
are abnormal and disorganized• Causes abnormal blood and lymph flow• Results in more fibrous tissue formation
Levercirrose: is geen oorzaak maar een gevolg van diverse leverziekten
• Sterke verbindweefseling in de lever – door diverse oorzaken (meest hepatisch)– met vorming regeneratienoduli– waardoor portaal bloed niet goed meer door lever
heen kan (portale hypertensie: ascites, slokdarmvarices)
– en uiteindelijk ook de leverfunctie achteruitgaat (stollingsstoornis, laag albumine)
Definition:
1. Diffuse disorder of liver characterised by;
2. Complete loss of normal architecture,
3. Replaced by extensive fibrosis with,
4. Regenerating parenchymal nodules.
Etiology of Cirrhosis
• Alcoholic liver disease 60-70%
• Viral hepatitis 10%
• Biliary disease 5-10%
• Primary hemochromatosis 5%
• Cryptogenic cirrhosis 10-15%
• Wilson’s, 1AT def rare
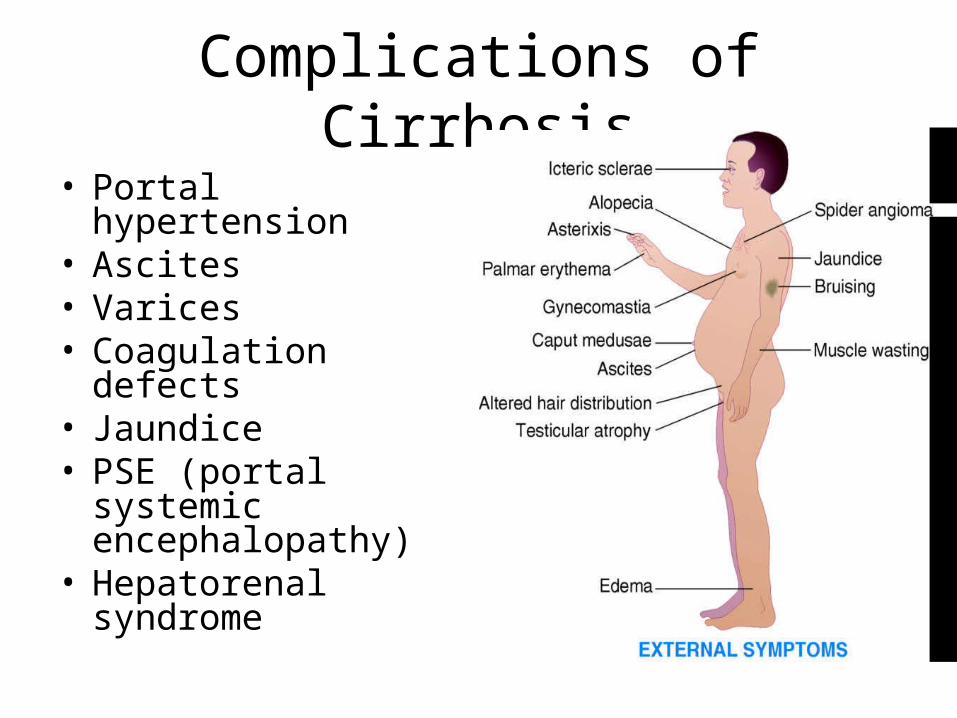
Complications of Cirrhosis
• Portal hypertension• Ascites• Varices• Coagulation defects• Jaundice• PSE (portal systemic
encephalopathy)• Hepatorenal
syndrome
Icterus
• Yellow discoloration of skin & sclera due to excess serum bilirubin. >40umol/l, (3mg/dl)
• Conjugated & Unconjugated types
• Obstructive & Non Obstructive (clinical)
• Pre-Hepatic, Hepatic & Post Hepatic types
• Jaundice - Not necessarily liver disease *
Portal Hypertension
• Increased pressure in the portal venous system. • Normal portal pressure is 5 to 10 mm Hg (7 to 14 cm
H2O), which exceeds inferior vena caval pressure by 4 to 5 mm Hg (the portal venous gradient).
• Higher values are defined as portal hypertension. • Portal hypertension is asymptomatic; • clinical findings result from its complications. The
most important is acute variceal bleeding,• usually from the distal esophagus, less often from the
gastric fundus, and only rarely from other sites. • Portal-systemic encephalopathy and ascites are the
other major consequences of portal hypertension.
Hepatic Failure/ESLD/ Hepatic Encephalopathy
Stage Symptom
I Mild confusion, agitation, irritability, sleep disturbance, decreased attention
II Lethargy, disorientation, inappropriate behavior, drowsiness
III Somnolence but arousable, incomprehensible speech, confusion, aggression when awake
IV Coma
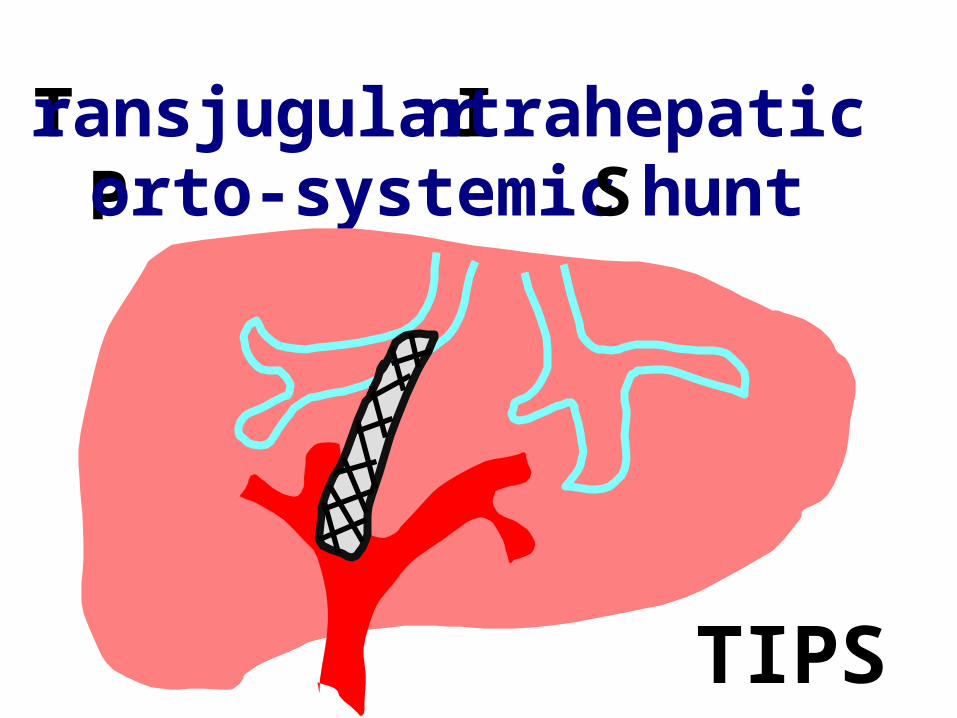
Transjugular Intrahepatic Porto-systemic S hunt
TIPS