Embed Size (px)
Citation preview

CoC-trained
consultants on staff
Toni Hare, RHIT, CTR CoC-trained Consultant
Vice President, CHAMPS Oncology November 27, 2012
Leveraging Your Cancer Registry: A Strategy for Survey Success
Georgia’s Best and Promising Practices In Quality Cancer Care: Meeting the 2012
Commission on Cancer Standards

Learning Objectives
Distinguish how registry data is applied to decisions affecting
planning
Demonstrate how registry is utilized to validate patient care
and outcomes
Identify steps to evaluate adherence to multiple accreditations
and certifications

The Evolution of Cancer Registry Data in Cancer Control
Traditional: Data Reporting
Past
Current:
Quality Care Measures & Improvement Strategies
Present Future
Future Trends:
Information for Financial Incentives, Regulation and Policy

Healthcare Innovators for Quality of Cancer Care
•Access to up-to-date comprehensive quality care close to home
•Plan, monitor and evaluate programs and services continuously
Healthcare Providers
•Collect and analyze cancer incidence for a specific population or geographic area
•Measures progress in cancer prevention and control
Government and Federal Agencies
•Explore trends in cancer care
•Create regional and state benchmarks for participating hospitals
•Serve as the basis for quality improvement
National Organizations
• Incentivize programs that monitor performance Primary Payers
Cancer Registry - First Source of Information
Develop administrative and marketing
plans
Support infrastructure
decisions
Evaluate clinical performance
Meet accreditation standards

Administrative & Marketing Plans Enhance
oncology service offerings
Monitor existing services
Establish population trends and
referral patterns
Apply for grants

Enhance Oncology Services
Market Analysis: Building Oncology
Center
Incidence Primary Cancer Sites
Stratify Primary Sites by Zip Code
and County
Identify physician Referral Patterns
Stratify by Managing Physician
Identify Practice Patterns
Stratify by Medical and Radiation
Oncology
Compare with the State Registry
Data

Enhance Oncology Service Offerings

Monitor Existing Services
Market Analysis: Treatment Trends
Incidence all Cancer Sites
Stratify by Accession Year
Trending Referral Patterns
Stratify by Accession Year &
Class of Case
Identify Practice Patterns
Stratify by Medical & Radiation
Oncology

Class of Case for Trending Reports
Initial diagnosis at reporting facility
00 Initial DX at the reporting facility AND all treatment or a decision not to treat was done elsewhere
10 Initial DX at the reporting facility or in a staff physician’s office AND part or all of 1st course RX or a decision not to treat was at the reporting facility, NOS
11 Initial DX in staff physician’s office AND part of first course treatment was done at the reporting facility
12 Initial DX in staff physician’s office AND all 1st RX or a decision not to treat was done at the reporting facility
13 Initial DX at the reporting facility AND part of 1st course RX was done at the reporting facility; part of 1st course RX was done elsewhere
14 Initial DX at the reporting facility AND all 1st course treatment or a decision not to treat was done at the reporting facility
Initial diagnosis elsewhere
20 Initial DX elsewhere AND all or part of 1st course RX was done at the reporting facility, NOS
21 Initial DX elsewhere AND all 1st course RX or a decision not to treat was done at the reporting facilityRX was done elsewhere
22 Initial DX in staff physician’s office AND part of first course treatment was done at the reporting facility
Analytic Classes of Case (required by CoC) from FORDS http://www.facs.org/cancer/coc/fordsmanual.html

Diagnosis & Treatment Patterns
36 51 39
26 31
362
313
348
315 321
230 234 210
168 170
0
50
100
150
200
250
300
350
400
2005 2006 2007 2008 2009
DX only
DX & TX
TX Only
-20%

Population Trends & Referral Patterns
Market Analysis: Treatment
Trends
Incidence of Top 5 Cancer
Sites
Stratify by Class of Case
(10-14 & 20-22)
Trending Population
Patterns
Stratify by Zip Code & County
Compare with State Data

Population Trends & Referral Patterns
Applying for Funding & Grants
Market Analysis: Disparities of
Breast
Incidence of Breast Cancer
Stratify by Accession Year
(5 yrs)
Patient Demographics
Stratify by Race, Ethnicity, Insurance
& Stage at DX
Survival Comparison with
NCDB
Stratify by Stage at Dx
Developed Programs from Grant Funding
B.R.E.A.S.T Program Amigas Unidas
MetroHealth Breast Center http://www.metrohealth.org/body.cfm?id=3522&oTopID=3522

Support Infrastructure Decisions
Identify staffing needs
Recruit physicians
Estimate revenue by disease site
Analyze costs and utilization
of ancillary services

Utilization of Ancillary Services
Radiation Therapy
Radiology
Laboratory
Medical Admissions
Inpatient Surgery
Outpatient Surgery
All I II III IV
16.6 2.3 16.3 19.7 22.0
All I II III IV
14.3 14.5 18.1 13.7 14.4
All I II III IV
28.6 25.1 27.6 27.8 43.1
All I II III IV
2.2 1.2 1.8 2.1 2.9
All I II III IV
1.6 1.0 1.1 1.5 2.7
All I II III IV
2.9 1.7 1.2 3.3 6.9
Average Number of visits per patient by stage

Evaluate Clinical Performance
Utilizing Quality
Improvement Methodology
PDCA Plan, Do,
Check, Act
FADE Focus,
Analyze, Develop, Execute
FMEA Failure mode and effects
analysis
Six Sigma
How does your
registry utilize
quality
improvement
methodologies
to evaluate
clinical
performance?

Quality Improvement Activities
• Measure effectiveness of improvement
• Implement the improvement
• Develop and implement potential solution or improvement
• Identify & analyze problem
Plan Do
Check Act
How does your
registry connect
to the quality
process in your
facility?

Registry Study Improves Clinical Care
• Decrease wait time from radiation consult to initial treatment for prostate cancer patients
Study Topic: (patients identified from cancer registry)
• Dx date, Consult date (User Defined field), Date Radiation Tx Started
Analysis: (data captured in cancer registry database)
• Average wait time – 20% above national benchmark Outcome: (quantitative report provided by cancer registry)
• Purchased and installed IMRT
• Additional 1 hour added to RT Clinic schedule Action: Implement solution
• Improvement - 29 days Monitor the effectiveness of action plan implemented

Multiple Cancer Program Accreditations & Certifications
Mastering the
Juggling Act
CoC
NAPBC
TJC
QOPI

Commission on Cancer (CoC)
• CoC-accredited Cancer Programs demonstrate the following services: – Comprehensive care with state of the art services and equipment
– Multidisciplinary team approach to coordinate treatment options
– Clinical trial information and education
– Access to patient-centered services: psychosocial distress, navigation
– Ongoing monitoring and improvement of care
– Assessment of treatment planning based on evidence-based guidelines
– Follow-up care including survivorship care plan
– Cancer information collection (Cancer Registry)
National Accreditation Program for Breast Centers (NAPBC)
• Centers demonstrate the following services:
– Multidisciplinary team approach to coordinate the best care and treatment options available
– Access to breast cancer-related information, education, and support
– Breast cancer data collection on quality indicators
– Identifies and references evidence-based guidelines
– Ongoing monitoring and improvement of care
– Clinical trials information and new treatment options

The Joint Commission Certification (TJC): Disease-Specific Care
• Develop a Multidisciplinary Site-specific Advisory Team
• Compliance with consensus-based national standards which include: – Program management
– Clinical information management
– Delivering or facilitating care
– Supporting self-management
– Measuring and improving performance
• Effective integration of Clinical Practice Guidelines to manage and optimize care
• Collects and analyzes performance measure data and drive improvement activities

ASCO: Quality Oncology Practice Initiative (QOPI)
• Quality assessment and improvement program for US-based outpatient hematology-oncology practices
• Data analyses on nationally recognized guidelines
• Practice-specific and aggregate comparison data for data-driven

Strides to Success
Is there a shared vision
within the cancer services?
Is that shared vision
supported by senior
leadership?
Is the Cancer Committee
aware of the latest
standards?
Are there adequate and
useful communication
tools to promote a successful
feedback loop?
Is the cancer registry acting as a strategic
partner to the cancer care
team?

Step # 1: Strategic Plan & Goal Setting
Assess Current Internal Resources
Available
Compare Standards and
Guidelines
Create Leadership Infrastructure
Develop a Communication
Tool

Standards Comparison Matrix

Step #2: Form Dedicated Teams
Establish subcommittees with disease-specific focus
Identify key stakeholders from cancer committee
membership
Agree on goals that align with cancer
program
Reports regularly to the Cancer
Committee

Hospital Subcommittee Members Required Member
Cancer Committee
Breast Program Leadership
Lung Cancer Advisory Group
Surgeon
Pathologist
Radiologist
Medical Oncologist
Radiation Oncologist
Navigator
Administrator
Oncology Nurse
Social Worker
Quality Improvement Coordinator
Data Manager
Other members as assigned

Step #3: Create Quality Scorecard
Identifies quality indicators
Organized by accreditation
Track each data set YTD comparison,
target, current status, monthly progress
Create reporting schedule
Assign responsibility

Current NQF Performance Measures
• BCS/RT- Breast conserving surgery with radiation
• MAC- Combination Chemo within 120 days Stage II & III ER/PR
• HT- Tamoxifen w/in 1 year Stage II & III ER/PR+
Breast
• ACT- Adjuvant chemo w/in 120 days Stage III
• 12 RLN- 12 lymph nodes removed Colon
• ADJ RT- Radiation w/in 180 days Stage III Rectal

Breast Cancer Quality Metrics Indicators Benchmark Reference Responsibility
Surgery: Mastectomy vs. breast conservation surgery rate - to ensure that women with stage 0-II BC are offered BCT
>50% NAPBC standard 2.3 Cancer Registry
Surgery: Needle biopsy vs open biopsy rate
>74.2% CoC 2008 NAPBC standard 2.9 NQF #0221
Cancer Registry
Med Onc: combo chemo given within 120 days of dx for pt <70 with AJCC T1cN0M0, or stage II or III, ER/PR - (CP3R)
100%
100% for CoC CMS has proposed reporting this quarterly NQF #0559
Cancer Registry
Med Onc: Tamoxifen or AI tx is initiated within 365 days of dx with AJCC T1cN0M0, or stage II or III, ER/PR + (CP3R)
97% 95% CoC NQF #0220 CMS has proposed reporting
Cancer Registry
Rad Onc:Is Rad. Tx administered within 365 days of dx for <70 receiving BCT (C3PR)
98% 95% CoC NQF #0219
Cancer Registry
Surgery: Mastectomy vs. breast conservation surgery rate - ensure stage 0-II are offered BCT
>50% NAPBC standard 2.3 Cancer Registry

Breast Scorecard for NAPBC & CoC System Metrics Benchmark Report
Nov 2012
Report Feb 2013
Report May 2013
Report Aug 2013
Jan-Mar 2012 cases
Apr-June 2012 cases
July-Sept 2012 cases
Oct-Dec 2012 cases
Surgery: Breast conservation surgery vs Mastectomy, to ensure that women with stage 0-II breast cancer are offered BCT
>50% NAPBC
Surgery: needle biopsy vs open biopsy rate >74.2% NAPBC
Med Onc: Is combo chemo considered or given within 120 days of dx for women <70 with AJCC T1cN0M0, or stage II or III, ER/PR - (CP3R)
100% COC
Med Onc:Tamoxifen or AI tx is considered or initiated within 365 days of dx for women with AJCC T1cN0M0, or stage II or III, ER/PR + (CP3R)
97% CoC
Rad Onc:Is Rad. Tx administered within 365 days of dx for <70 receiving BCT for (C3PR)
98% CoC
Evaluation of the axilla for patients with early stage breast cancer (I-IIB) via sentinel node biopsy at time of surgery (lumpectomy or mastectomy)
75% Intermountain
Timeliness of treatment (screening-path) 8 days (OH)
Survival by stage (0, I, II, III, IV), by hospital and OH, compared to NCDB

Lung Cancer Quality Metrics Indicators Benchmark Reference Responsibility
Diagnosis by initial stage compared internally by hospital & state and with NCDB
Cancer Registry
Risk adjust morbidity after lobectomy for lung cancer (% of patients undergoing elective lobectomy for lung cancer that have a length of stay > 14 days.)
NQF #0459 (Society for Thoracic Surgeons)
Quality Dept.
Risk adjusted morbidity & mortality for lung resection (specific list of post-op complications such as need for trach, ARDS, PE and more)
NQF #1790 (Society for Thoracic Surgeons)
Quality Dept.
% of lung cancer surgeries with >4 mediastinal lymph node stations dissected
100% NCCN Cancer Registry
% of prophylactic cranial irradiation in limited or extensive stage small cell celllung cancer
100% NCCN Cancer Registry
Survival by stage, compared with NCDB and internally by hospital and system
Compare to the National Cancer Database by hospital, by system
Cancer Registry

Lung Scorecard for TJC: Disease Specific Care
System Metrics Benchmark Report Nov 2012
Report Feb 2013
Report May 2013
Report Aug 2013
Jan-Mar 2012 cases
Apr-June 2012 cases
July-Sept 2012 cases
Oct-Dec 2012 cases
Diagnosis by initial stage compared internally by hospital & state and with NCDB. NSCLC Only
Diagnosis by initial stage compared internally by hospital & state and with NCDB. SCLC Only
Risk adjust morbidity (% of pts undergoing elective lobectomy for length of stay > 14 days.) NQF 0459
<6.2% (for 74th percentile)
% of surgeries for NSCLC with >4 mediastinal lymph node stations dissected (NCCN)
100%
% of prophylactic cranial irradiation given in limited stage small cell (NCCN-adv group set %)
80%
Recording of clinical stage prior to resection (% of all surgical patients undergoing treatment procedures for lung cancer that has clinical TNM staging provided)
98.2% (for 75th percentile)
Survival by stage compared by hospital and system with NCDB as possible. NSCLC Only
Survival by stage compared by hospital and system with NCDB as possible. SCLC Only

Colorectal Cancer Quality Metrics Indicators Benchmark Reference Responsibility
Colon/Surgery: At least 12 regional lymph nodes are removed and pathologically examined for resected cancer for staging completeness for stage I, II, III.
81.50% NQF #0225 80% CoC
Cancer Registry
Colon/Med Onc: Is adjuvant chemotherapy considered or given wtihin 120 days of diagnosis in pts <80 with stage III colon cancer? (CP3R)
100%
NQF #0223. 100% for CoC CMS has proposed reporting this quarterly
Cancer Registry
Rectal/Rad Onc: Radiation therapy given for stage III rectal CA in pts <80, under 6 mths of DX. (C3PR)
100% CoC C3PR Cancer Registry
Rectal: Endorectal ultrasound or pelvic MRI is performed prior to TX for rectal cancer.
100% NCCN version 3.2012 (colorectal cancer) Cancer Registry
Colorectal Survival Compare to the National Cancer Database by hospital, by system
Cancer Registry

Colorectal Scorecard for CoC System Metrics Benchmark Report
Nov 2012
Report Feb 2013
Report May 2013
Report Aug 2013
Jan-Mar 2012 cases
Apr-June 2012 cases
July-Sept 2012 cases
Oct-Dec 2012 cases
COLON CANCER
Colon/Surgery: At least 12 regional lymph nodes are removed and pathologically examined for resected cancer for staging completeness for stage I, II, III. (C3PR)
81.5%
Colon/Med Onc: Is adjuvant chemotherapy considered or given wtihin 120 days of diagnosis in pts <80 with stage III colon cancer? (CP3R)
100%
RECTAL CANCER
Rectal/Rad Onc: Is radiation therapy considered or given for stage III rectal CA in patients <80, under 6 months of diagnosis. (C3PR metric)
100%
Rectal/Endorectal ultrasound or pelvic MRI is performed prior to trt for rectal cancer.
100%
COLON & RECTAL CANCER
Colorectal Survival (separately) - this is 5-year survival, thus the most recent complete year is 2011.
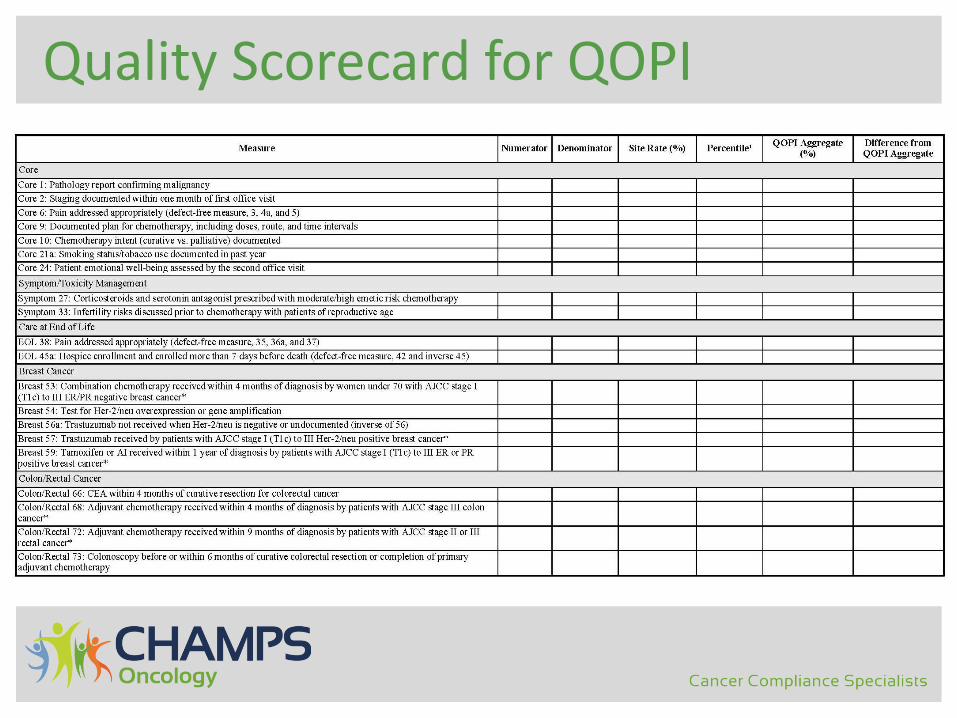
Quality Scorecard for QOPI

Quality Scorecard Sample

Step # 4: Invest in Quality & Informatics
Identify Sources of Cancer Information
• Cancer Registry-First Source
• Clinical Trial Databases
• Patient Navigation Databases
Utilize IT Support Services
• AutoMerge from Electronic Health Record
• Data Warehousing
• SQL Reporting

Don’t Reinvent the Wheel
Multi-disciplinary Cancer Care
Team
Standard Guidelines
Clinical Practice
Guidelines
Performance Measures
Data Analytics

Thank You!
• Questions? Contact:
– Toni Hare, RHIT, CTR CoC-trained Consultant Vice President CHAMPS Oncology [email protected] 216.255.3716
www.champsoncology.com