Embed Size (px)
Citation preview
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Leveraging Prior Knowledge inGuiding Pediatric Drug Development
Pravin R JadhavPharmacometrics, Office of Clinical Pharmacology
Office of Translational SciencesCDER,FDA
Workshop on Modeling in Pediatric MedicinesLondon, UK
April 14, 2008The views expressed in this presentation do not necessarily reflect the agency position
[email protected] Pediatric Drug Development 1/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Agenda
1 History of Legislation
2 Retrospective Analysis
3 Impetus
4 CTS Framework
5 Results
6 Conclusions
[email protected] Pediatric Drug Development 2/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Legislation HistoryActive history to obtain good quality pediatric data
1979 Labeling Requirement1994 Pediatric Labeling Rule1997 FDA Modernization Act (FDAMA)1998 Pediatric Rule2002 Best Pharmaceuticals for Children Act (BPCA)2002 Pediatric Rule Enjoined2003 Pediatric Research Equity Act (PREA)2007 FDA Amendments Act of 2007
Pediatric Medical Device Safety and Improvement ActPediatric Research Equity Act (PREA)Best Pharmaceuticals for Children Act (BPCA)
[email protected] Pediatric Drug Development 3/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Legislation HistoryActive history to obtain good quality pediatric data
1979 Labeling Requirement1994 Pediatric Labeling Rule1997 FDA Modernization Act (FDAMA)1998 Pediatric Rule2002 Best Pharmaceuticals for Children Act (BPCA)2002 Pediatric Rule Enjoined2003 Pediatric Research Equity Act (PREA)2007 FDA Amendments Act of 2007
Pediatric Medical Device Safety and Improvement ActPediatric Research Equity Act (PREA)Best Pharmaceuticals for Children Act (BPCA)
[email protected] Pediatric Drug Development 3/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Legislation HistoryActive history to obtain good quality pediatric data
1979 Labeling Requirement1994 Pediatric Labeling Rule1997 FDA Modernization Act (FDAMA)1998 Pediatric Rule2002 Best Pharmaceuticals for Children Act (BPCA)2002 Pediatric Rule Enjoined2003 Pediatric Research Equity Act (PREA)2007 FDA Amendments Act of 2007
Pediatric Medical Device Safety and Improvement ActPediatric Research Equity Act (PREA)Best Pharmaceuticals for Children Act (BPCA)
[email protected] Pediatric Drug Development 3/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Improved Labeling Information for PediatricsA central goal of pediatric exclusivity program
General principles a
Pediatric patients should be given medicines that havebeen appropriately evaluated for their use in thosepopulations
Product development programs should includepediatric studies when pediatric use is anticipated
Shared responsibility among companies, regulatoryauthorities, health professionals, and society as awhole
aICH E-11:http://www.fda.gov/cber/gdlns/ichclinped.htm#id
[email protected] Pediatric Drug Development 4/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Improved Labeling Information for PediatricsA central goal of pediatric exclusivity program
General principles a
Pediatric patients should be given medicines that havebeen appropriately evaluated for their use in thosepopulations
Product development programs should includepediatric studies when pediatric use is anticipated
Shared responsibility among companies, regulatoryauthorities, health professionals, and society as awhole
aICH E-11:http://www.fda.gov/cber/gdlns/ichclinped.htm#id
[email protected] Pediatric Drug Development 4/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Improved Labeling Information for PediatricsA central goal of pediatric exclusivity program
General principles a
Pediatric patients should be given medicines that havebeen appropriately evaluated for their use in thosepopulations
Product development programs should includepediatric studies when pediatric use is anticipated
Shared responsibility among companies, regulatoryauthorities, health professionals, and society as awhole
aICH E-11:http://www.fda.gov/cber/gdlns/ichclinped.htm#id
[email protected] Pediatric Drug Development 4/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Improving Pediatric Dosing through PediatricInitiativesWhat we have learned
Substantive differences in dosing, safety, or efficacy inchildren 1 compared with adults for at least half of theproducts studied
Twenty nine of 131 drugs were concluded to be ineffective
Several oral antihypertensive products that were approvedin adults did not seem to work in children
With rising obesity in children and adolescents, failed trialsfor antihypertensive products have significant public healthimplications
1Rodriguez W, Selen A, Avant D et. al. Improving pediatric dosing through pediatric initiatives: What we have
learned, Pediatrics, 2008; 121(3): 530-9
[email protected] Pediatric Drug Development 5/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Improving Pediatric Dosing through PediatricInitiativesWhat we have learned
Substantive differences in dosing, safety, or efficacy inchildren 1 compared with adults for at least half of theproducts studied
Twenty nine of 131 drugs were concluded to be ineffective
Several oral antihypertensive products that were approvedin adults did not seem to work in children
With rising obesity in children and adolescents, failed trialsfor antihypertensive products have significant public healthimplications
1Rodriguez W, Selen A, Avant D et. al. Improving pediatric dosing through pediatric initiatives: What we have
learned, Pediatrics, 2008; 121(3): 530-9
[email protected] Pediatric Drug Development 5/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Improving Pediatric Dosing through PediatricInitiativesWhat we have learned
Substantive differences in dosing, safety, or efficacy inchildren 1 compared with adults for at least half of theproducts studied
Twenty nine of 131 drugs were concluded to be ineffective
Several oral antihypertensive products that were approvedin adults did not seem to work in children
With rising obesity in children and adolescents, failed trialsfor antihypertensive products have significant public healthimplications
1Rodriguez W, Selen A, Avant D et. al. Improving pediatric dosing through pediatric initiatives: What we have
learned, Pediatrics, 2008; 121(3): 530-9
[email protected] Pediatric Drug Development 5/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Improving Pediatric Dosing through PediatricInitiativesWhat we have learned
Substantive differences in dosing, safety, or efficacy inchildren 1 compared with adults for at least half of theproducts studied
Twenty nine of 131 drugs were concluded to be ineffective
Several oral antihypertensive products that were approvedin adults did not seem to work in children
With rising obesity in children and adolescents, failed trialsfor antihypertensive products have significant public healthimplications
1Rodriguez W, Selen A, Avant D et. al. Improving pediatric dosing through pediatric initiatives: What we have
learned, Pediatrics, 2008; 121(3): 530-9
[email protected] Pediatric Drug Development 5/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Antihypertensive Trial FailuresAnalysis of 6 type C study designs
Six dose-ranging antihypertensive efficacy trials completed forpediatric exclusivity from 1998 to 2005 were reviewed a
Three failed and Three succeeded to demonstrate doseresponse as a primary endpoint
Failed trials included 2-9 fold and Successful trials included20-32 fold dose rangeTwo failed drugs were significantly different compared toplacebo in the 2nd part of the study
Poor dose selection, lack of acknowledgment of differencesbetween adults and pediatrics and lack of suitable pediatricformulations as potential failure reasons
aBenjamin DK, Smith PB, Jadhav PR et. al. Pediatric Antihypertensive Trial Failures: Analysis of End Points and Dose
Range, Hypertension, 2008; 51: 834-840
[email protected] Pediatric Drug Development 6/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Antihypertensive Trial FailuresAnalysis of 6 type C study designs
Six dose-ranging antihypertensive efficacy trials completed forpediatric exclusivity from 1998 to 2005 were reviewed a
Three failed and Three succeeded to demonstrate doseresponse as a primary endpoint
Failed trials included 2-9 fold and Successful trials included20-32 fold dose rangeTwo failed drugs were significantly different compared toplacebo in the 2nd part of the study
Poor dose selection, lack of acknowledgment of differencesbetween adults and pediatrics and lack of suitable pediatricformulations as potential failure reasons
aBenjamin DK, Smith PB, Jadhav PR et. al. Pediatric Antihypertensive Trial Failures: Analysis of End Points and Dose
Range, Hypertension, 2008; 51: 834-840
[email protected] Pediatric Drug Development 6/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Antihypertensive Trial FailuresAnalysis of 6 type C study designs
Six dose-ranging antihypertensive efficacy trials completed forpediatric exclusivity from 1998 to 2005 were reviewed a
Three failed and Three succeeded to demonstrate doseresponse as a primary endpoint
Failed trials included 2-9 fold and Successful trials included20-32 fold dose rangeTwo failed drugs were significantly different compared toplacebo in the 2nd part of the study
Poor dose selection, lack of acknowledgment of differencesbetween adults and pediatrics and lack of suitable pediatricformulations as potential failure reasons
aBenjamin DK, Smith PB, Jadhav PR et. al. Pediatric Antihypertensive Trial Failures: Analysis of End Points and Dose
Range, Hypertension, 2008; 51: 834-840
[email protected] Pediatric Drug Development 6/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Antihypertensive Trial FailuresAnalysis of 6 type C study designs
Six dose-ranging antihypertensive efficacy trials completed forpediatric exclusivity from 1998 to 2005 were reviewed a
Three failed and Three succeeded to demonstrate doseresponse as a primary endpoint
Failed trials included 2-9 fold and Successful trials included20-32 fold dose rangeTwo failed drugs were significantly different compared toplacebo in the 2nd part of the study
Poor dose selection, lack of acknowledgment of differencesbetween adults and pediatrics and lack of suitable pediatricformulations as potential failure reasons
aBenjamin DK, Smith PB, Jadhav PR et. al. Pediatric Antihypertensive Trial Failures: Analysis of End Points and Dose
Range, Hypertension, 2008; 51: 834-840
[email protected] Pediatric Drug Development 6/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Antihypertensive Trial FailuresAnalysis of 6 type C study designs
Six dose-ranging antihypertensive efficacy trials completed forpediatric exclusivity from 1998 to 2005 were reviewed a
Three failed and Three succeeded to demonstrate doseresponse as a primary endpoint
Failed trials included 2-9 fold and Successful trials included20-32 fold dose rangeTwo failed drugs were significantly different compared toplacebo in the 2nd part of the study
Poor dose selection, lack of acknowledgment of differencesbetween adults and pediatrics and lack of suitable pediatricformulations as potential failure reasons
aBenjamin DK, Smith PB, Jadhav PR et. al. Pediatric Antihypertensive Trial Failures: Analysis of End Points and Dose
Range, Hypertension, 2008; 51: 834-840
[email protected] Pediatric Drug Development 6/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Leveraging Prior Quantitative KnowledgeA case study
Drug X to be used for immediate blood pressure (BP) control
The initial study design to obtain exclusivity was fraught withuncertainties
Dose/exposure rangePlacebo durationSample size and primary endpoint
Leveraging prior quantitative knowledge to design a studywith adequate power and improve data quality to deriverational dosing recommendations
[email protected] Pediatric Drug Development 7/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Leveraging Prior Quantitative KnowledgeA case study
Drug X to be used for immediate blood pressure (BP) control
The initial study design to obtain exclusivity was fraught withuncertainties
Dose/exposure rangePlacebo durationSample size and primary endpoint
Leveraging prior quantitative knowledge to design a studywith adequate power and improve data quality to deriverational dosing recommendations
[email protected] Pediatric Drug Development 7/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Leveraging Prior Quantitative KnowledgeA case study
Drug X to be used for immediate blood pressure (BP) control
The initial study design to obtain exclusivity was fraught withuncertainties
Dose/exposure rangePlacebo durationSample size and primary endpoint
Leveraging prior quantitative knowledge to design a studywith adequate power and improve data quality to deriverational dosing recommendations
[email protected] Pediatric Drug Development 7/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Leveraging Prior Quantitative KnowledgeSponsor and FDA conducted clinical trial simulations (CTS) to substantiate thechoice of trial design, dosing regimens and sample size
Information available toSponsor and FDA
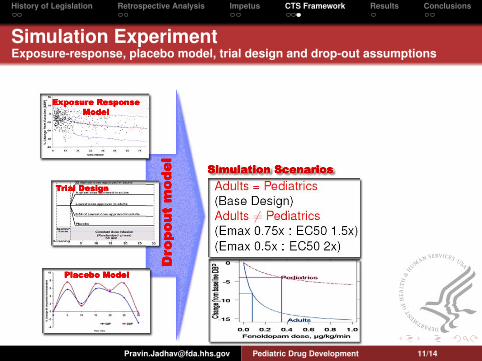
Patient level exposure-response data on drug X in adultsMean exposure-response data on fenoldopam a
FDAPatient level exposure-response data on fenoldopam in adultsand pediatrics
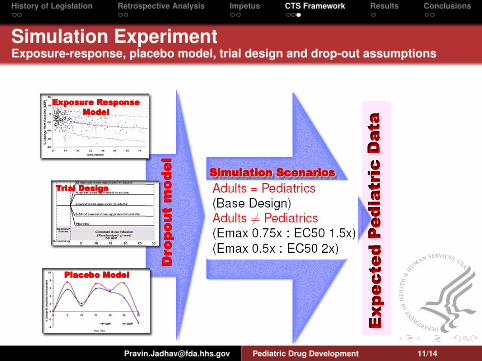
Inputs for CTSExposure response modelPlacebo response modelDrop-out modelTrial design
ahttp://www.fda.gov/cder/foi/label/2004/19922se5-005 colopam lbl.pdf
[email protected] Pediatric Drug Development 8/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Leveraging Prior Quantitative KnowledgeSponsor and FDA conducted clinical trial simulations (CTS) to substantiate thechoice of trial design, dosing regimens and sample size
Information available toSponsor and FDA
Patient level exposure-response data on drug X in adultsMean exposure-response data on fenoldopam a
FDAPatient level exposure-response data on fenoldopam in adultsand pediatrics
Inputs for CTSExposure response modelPlacebo response modelDrop-out modelTrial design
ahttp://www.fda.gov/cder/foi/label/2004/19922se5-005 colopam lbl.pdf
[email protected] Pediatric Drug Development 8/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
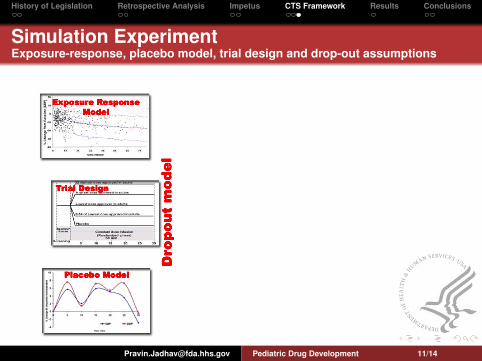
Inputs for CTS
Exposure response modelPatient level adult data for Drug X
Placebo response modelPatient level pediatric data for fenoldopam
Drop-out modelPatient level pediatric data for fenoldopamClinical experience: Subjects with >25% decrease in DBPdiscontinue
[email protected] Pediatric Drug Development 9/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
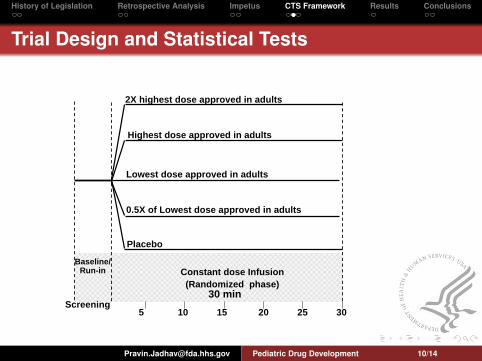
Trial Design and Statistical Tests
Screening
Baseline/Run-in Constant dose Infusion
(Randomized phase)30 min
Placebo
0.5X of Lowest dose approved in adults
Lowest dose approved in adults
2X highest dose approved in adults
Highest dose approved in adults
5 10 15 20 25 30
[email protected] Pediatric Drug Development 10/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
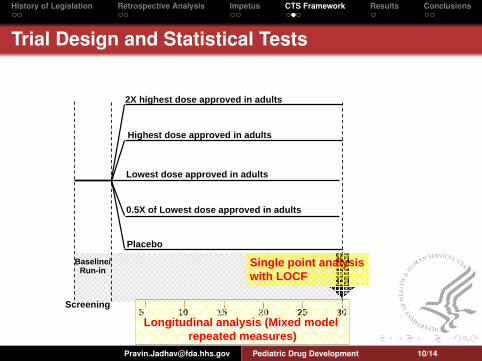
Trial Design and Statistical Tests
Screening
Baseline/Run-in
Placebo
0.5X of Lowest dose approved in adults
Lowest dose approved in adults
2X highest dose approved in adults
Highest dose approved in adults
5 10 15 20 25 30Longitudinal analysis (Mixed model
repeated measures)
Single point analysis with LOCF
[email protected] Pediatric Drug Development 10/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Simulation ExperimentExposure-response, placebo model, trial design and drop-out assumptions
[email protected] Pediatric Drug Development 11/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Simulation ExperimentExposure-response, placebo model, trial design and drop-out assumptions
[email protected] Pediatric Drug Development 11/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Simulation ExperimentExposure-response, placebo model, trial design and drop-out assumptions
[email protected] Pediatric Drug Development 11/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
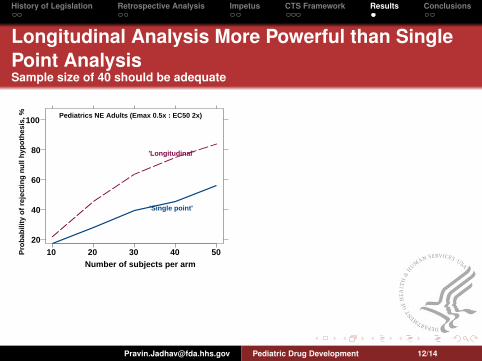
Longitudinal Analysis More Powerful than SinglePoint AnalysisSample size of 40 should be adequate
20
40
60
80
100
10 20 30 40 50
Pediatrics NE Adults (Emax 0.5x : EC50 2x)
'Longitudinal'
'Single point'
Number of subjects per arm
Prob
abili
ty o
f rej
ectin
g nu
ll hy
poth
esis
, %
[email protected] Pediatric Drug Development 12/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
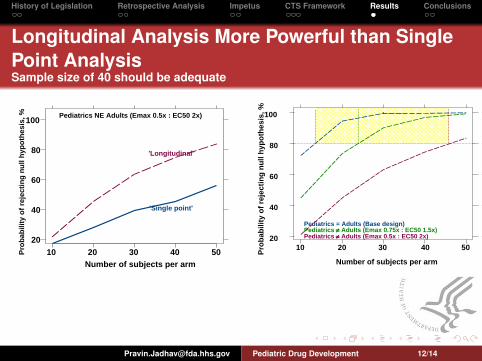
Longitudinal Analysis More Powerful than SinglePoint AnalysisSample size of 40 should be adequate
20
40
60
80
100
10 20 30 40 50
Pediatrics NE Adults (Emax 0.5x : EC50 2x)
'Longitudinal'
'Single point'
Number of subjects per arm
Prob
abili
ty o
f rej
ectin
g nu
ll hy
poth
esis
, %
20
40
60
80
100
10 20 30 40 50
Pediatrics = Adults (Base design)
Pediatrics ≠ Adults (Emax 0.5x : EC50 2x)Pediatrics ≠ Adults (Emax 0.75x : EC50 1.5x)
Number of subjects per armPr
obab
ility
of r
ejec
ting
null
hypo
thes
is, %
[email protected] Pediatric Drug Development 12/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Key FindingsLeveraging prior knowledge allowed us to
effectively use prior knowledge to develop a pediatricwritten request
make informed decisions on dose range, number ofsubjects, sampling scheme and statistical tests
design a study with adequate power and improve dataquality to derive rational dosing recommendations
[email protected] Pediatric Drug Development 13/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Key FindingsLeveraging prior knowledge allowed us to
effectively use prior knowledge to develop a pediatricwritten request
make informed decisions on dose range, number ofsubjects, sampling scheme and statistical tests
design a study with adequate power and improve dataquality to derive rational dosing recommendations
[email protected] Pediatric Drug Development 13/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
Key FindingsLeveraging prior knowledge allowed us to
effectively use prior knowledge to develop a pediatricwritten request
make informed decisions on dose range, number ofsubjects, sampling scheme and statistical tests
design a study with adequate power and improve dataquality to derive rational dosing recommendations
[email protected] Pediatric Drug Development 13/14
History of Legislation Retrospective Analysis Impetus CTS Framework Results Conclusions
AcknowledgmentsInternal and External Experts
Clinical PharmacologyJoga Gobburu PhD, Pharmacometrics, Office of Clinical PharmacologyPatrick Marroum PhD, Office of Clinical PharmacologyMehul Mehta PhD, Office of Clinical Pharmacology
ClinicalNorman Stockbridge MD, Division of CardioRenal Drug ProductsLisa Mathis MD, Pediatric and Maternal Health StaffAbraham Karkowsky MD, Division of CardioRenal Drug Products
StatisticsJialu Zhang PhD, Office of BiostatisticsJim Huang PhD, Office of Biostatistics
OthersCDR Denise Hinton, Project ManagerScientists with the Anonymous Sponsor, Pharmaceutical Industry
[email protected] Pediatric Drug Development 14/14