Embed Size (px)
Citation preview

Prof. Ossama Hussein Roshdy

It is a term given to a wide range of disorders all are characterized by cutaneous hypopigmentation.

Melanin is produced from Tyrosine.

Melanocytes in the skin, oral mucosa, and uvea derive from spinal portion of the neural crest.
Melanocytes originate from melanoblasts.
Density of Melanocytes in the skin is the same for all human races.

Tyrosine DOPA DOPA quinone
DOPAchrome
DHI + DHICA Melanin.



INFANCY ( Diffuse-CIRCUMSCRIBED).INFANCY ( Diffuse-CIRCUMSCRIBED).
CHILDHOOD (Diffuse/ CIRCUMSCRIBED).CHILDHOOD (Diffuse/ CIRCUMSCRIBED).
ADULTHOOD (Diffuse/ CIRCUMSCRIBED).ADULTHOOD (Diffuse/ CIRCUMSCRIBED).

INFANCY / DiffuseINFANCY / Diffuse
Eyes, skin & HairEyes, skin & Hair Skin &/or HairSkin &/or Hair
MenkesMenkes Griscelli ‘s – Griscelli ‘s – Elejalde Elejalde
syndromessyndromes
NutritionalNutritionalDeficiencies,Deficiencies,
e.g. Se, e.g. Se, CopperCopper
Sialic aSialic aStorageStorageDiseaseDisease
EECEEC
OCAOCAPhenylketonureaPhenylketonurea
(PKU)(PKU)
11 22 33 Hermansky PudlakHermansky PudlakChediak - HigashiChediak - Higashi
CrossCross
Prader – WilliPrader – WilliAngelmanAngelman

INFANCY / CIRCUMSCRIBEDINFANCY / CIRCUMSCRIBED
Lack of PigmentLack of Pigment Decreased Decreased PigmentPigment
PostPostInfectiousInfectious
Ash leafAsh leafspotsspots
Post-Post-InflammatoryInflammatory
WaardenburgWaardenburg WaardenburgWaardenburg++
HirshsprungHirshsprung
HypomelanosisHypomelanosisOf ItoOf ItoNevusNevus
DepigmentosusDepigmentosus
VitiligoVitiligo PiebaldismPiebaldism

CHILDHOOD / CIRCUMSCRIBEDCHILDHOOD / CIRCUMSCRIBED
PostPostInfectiousInfectious
ChemicalChemicalLeukodermaLeukoderma
Post-Post-TraumaticTraumatic
DiffuseDiffuse
VitiligoVitiligo
Melanoma-Melanoma-AssociatedAssociatedleukodermaleukoderma
VKHVKH
SclerodermaScleroderma
CircumscribedCircumscribed
Post-Post-InflammatoryInflammatory
Total BodyTotal BodyVitiligoVitiligo

ADULTHOODADULTHOOD
PostPostInfectiousInfectious
EczemaEczema
Post-Post-InflammatoryInflammatory
VitiligoVitiligo Post-Post-TraumaticTraumatic
PLC PLC LS & ALS & A
LichenLichenstriatusstriatusPsoriasisPsoriasisAtopic Atopic
dermatitisdermatitis

- White hairs.- Milky white skin.- Blue-grey eyes.
Oculocutaneous Albinism

- Rare syndrome.- Inherited as an autosomal recessive.
Chediak – Higashi SyndromeChediak – Higashi Syndrome

- Bleeding tendency.- Platelet dysfunction.- Progressive neurologic dysfunction.- Severe immunodeficiency.- Marked susceptibility to respiratory
and cutaneous infections.- Uusually fatal before the age of 10
years.- later on from a malignant
lymphoma.


- Autosomal dominant.- Mutatio n on
chromosome 4q11-12.- Since birth.- Mainly forehead,
trunk, and extrimities.- Triangular or diamond
shaped areas.
PiebaldismPiebaldism

- Usually on front of the body.
- Specially on midline distribution.

- Whit forelock.- May be poliosis of eyebrows and
eyelashes.- Treated mainly surgically.

- Rare, autosomal dominant or A. recessive.
- Achromia of hair and/or skin.
- Broad nasal root dystopia canthorum.
- Heterochromia irides.
Waardenburg SyndromeWaardenburg Syndrome


- Congenital deafness.
- Medial eyebrows hyperplasia.

- Superficial fungal infection. - Pityriasis versicolor.
- Unsaturated fatty acids oxidation
products inhibit tyrosinase activity.
Post Infectious lekodermaPost Infectious lekoderma
fungus
Azelaic acid

Others:- Leprosy.- Pinta.- Yaws.- Bejel.- Secondary stage Syphilis.

- It is a misnomer.- Usually present at birth.- Single but may be multiple,
circumscribed.- Rounded, dermatomal or in whorls
and streaks.
Naevus Naevus depigmentosusdepigmentosus


- It is an autosomal dominant disease.- Multiple, irregularly
scattered(ashleaf appearance).
Ash leaf spots (Ash leaf spots (tuberous tuberous sclerosis)sclerosis)

- A disease of unknown etiology.- It affects 4 organs in succession:
1- Meninges encephalitic or meningitic symptoms + lymphocytosis of CSF.
Vogt-Koyanagi syndrome (HARADA)

2- Eyes bilateral uveitis, choroiditis and optic neuritis(some recovery of visual acuity).

3- Inner ears deafness and/or tinnitus (over 50% of cases) completely restored.

4- Skin (permanent changes)
vitiligo (60% of cases), poliosis (80% of cases) and alopecia areata (in 50% of cases).



Positive family member affection in about 25-33% of cases.
No prove of autosomal (recessive-dominant) trait.
Multifactorial inheretance genetic pattern is postulated (on chromosomes 1-2-and 4).

Heterogenous-
Convergence theory

- Association with some auto-immune diseases.
- Antibody activity is more pronounced in active rather than stable disease.
I- Auto-immune theory:

- ↑ Antibodies against melanocyte surface antigens.
- ↑ Antibodies against common tissue antigens (thyroid, gastric parietal cells and adrenal tissue) in 80% of vitiligo cases.
- ↑ Level of anti-tyrosinase antibodies.

- T-cell profiles are abnormal in vitiligo with a decrease in T-helper cells.
- Melanocyte activity Melanocyte death.
II- Auto-cytotoxicity theory:

↑ Melanocyte susceptibility to the precursor molecule (Dopachrome) cell death.
• Inhibition of Thioredoxin reductase enzyme (a free-radical scavenger) ↑accumulation of free radicals.
• ↓Level of catalase (which reduces superoxides).
↑ Dopamine auto-oxidation.
Melanocyte death

• Depigmentation in animal models with injured nerve fibers.• Nerve injury associated absence of vitiligo lesions.
• Segmental dermatomal type of vitiligo.
• Increased adrenergic activity (sweating – vasoconstriction) in vitiligo areas.
III- Neural theory:

Evidenced by:
Elevated levels of in Melanocytes of
vitiligo lesions may suggest neurogenic control.
Neurotensin TNF-α


Vitiligo areas
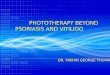
Absent Melanocytes.


Normal skinVitiligo skin

Vitiligo. A melanocyte with a giant melanosome is present at the edge of the
depigmented area. (H&E)

• Cultured Melanocytes at lesion’s peripheries
Evidence of
Poor growth + premature death Degeneration: vacuolizationPyknosismelanosomes aggregation

Sometimes ?? Inflammatory changes at the borders of lesions.


Onset childhood or young adults. in ≈20% develops after severe
sunburn or severe emotional or physical stress.
Incidence ↓ with increasing age.
Gender preponderance in female patients (?? False preponderance).

Prevalence is variable from area to another:
USA → 1%. Denmark →
0.38%. India →
1.13%






According to the extent of involvement:
1- Generalized.2- Universal.3- Acrofacial (distal fingers + facial
orifices).4- Segmental (dermatomal-
asymmetric).5- Focal (localized non-dermatomal).

6- Vitiligo gradata (trichrome type).

7- Vitiligo with raised borders.


8- Drug induced vitiligo – rare type (Chloroquine- Clofazimine).
9- Chemical- induced leukoderma (occupational):
- Phenolic compounds (p-TBP)- monomethyl ether of hydroquinone)
- Sulfhydryls (Sulfanilic acid – Mercaptoethylamine MEA).
- Others: arsenic- corticosteroids – azelaic acid – mercurials.

10- Vitiligo with melanoma:
-Regression or slow progression of melanoma long survival time .-Halo nevus.-Diffuse depigmentation and/or hypo pigmentation (remote from the tumor)


A- Autoimmune diseasaes:- Addison’s disease.- Thyroid disease.- Diabetes.- Alopecia areata.B- Uveitis.C- Auditory problems.D- Vogt-Koyanagi-Harada Syndrome.
CLINICAL SYSTEMIC ASSOCIATIONS

EN
ALU
ATIO
N Wood’s light examinatiuon
TSH level
Complete blood picture
Ophthalmologic examination
Psychological evaluation


TREATMENT
Cosmetic camouflag
e
Topical and systemic steroids
Phototherapy•Psoralen UVA•Narrowband UVB
Surgical treatment

Type of dyes
Sites of application
On exposed areas (face, neck, and hands)
Cover mark- Dermablend – Dermacolor - Dermage
Drawbacks
Personal rejectionSevere reactionNot practical for extensive lesions
I- Cosmetic camouflage

P = Psoralens
UVA = Ultraviolet A
Topical
Systemic
360 nm waveleng
th
PUVA therapy

8 methoxy-psoralen 0.5 mg/kg. Used for extensive vitiligo.
Exposure:• 1.5-2 hours after ingestion of the drug.• 1-2 J/cm2 increments by 0.25 J/cm2 till erythema dose.• 2-3 times / week.

8 methoxy-psoralen 0.05- 0.1% solution.
Used in cases with less than 20% total surface area depigmentation.
Exposure:• Duration before exposure is not important.• 1-2 J/cm2 .• 30 seconds increments by 15-30 seconds up to 10 minutes. • 2-3 times /week.

PUVA increase the size but not the number of Melanosomes.

UV light Psoralen + DNA
photoadducts
(with thymine bases) DNA inhibition
RNA + protein synthesis.
1-photoadducts

Decreasing the antibodies directed against Melanocytes.
2- immunologic :
Cytokines release from keratinocytes:• Interleukin-1 Facilitates binding of α-MSH to keratinocytes.• Leukotriens C4, D4 Stimulate Melanocyte proliferation (in-vitro).• Endothelin-1 Proliferation and differentiation of Melanocytes.Leukotrien C4 + TGF-α Melanocyte migration (in-vitro).

SIDE EFFECTS
IMMEDIATE DELAYED
•Erythema.•Pigmentation.• Fatigue.• Xerosis.• Pruritus.
• Skin aging.•Malignancy (SCC).• Cataract

PUVASOL
Exposure:- We use 5 MOP or TMP.- Dose of 0.3 mg/kg.- 2-4 hours outdoor light exposure (10 AM – 3 PM).- 5-10 minutes increments by 5 minutes/ session for 4 exposures gradual increase up to 2 hours.

Usually 311-312 nm wavelength. Treatment of choice for adults and children
with generalized vitiligo. 250 mJ/ cm2 increments by
15% at each exposure erythema.
2-3 times /week.
1- Can be used in children.2- Can be used in lactating and pregnant
women.3- Can be used in hepatic or kidney dysfunction.
Narrowband UVB (NB-UVB)
Advantages

Repigmentation occurs from hair
follicles.
Upward migration of Melanocytes is influenced by cytokine release from
keratinocytes.

For localized lesions. Face and neck may respond better. High potency topical corticosteroid
preparations (0.1% betamethasone valerate -0.05% clobetasol propionate) are effective.
1-2 months tapering. IM corticotropins may also help.
Topical and systemic steroids

Segmental or localized vitiligo. Non progressive-inctive disease. In areas such as:- Dorsal aspect of fingers.- Forehead.- On hair lines.- Ankles.
Surgical treatment
INDICATIONS

A- Epidermal Grafting
B- Autologus Minigrafting
C- Transplantation of non-cultured Melanocytes
D- Transplantation of cultured Melanocytes
Surgical treatment modalities