Embed Size (px)
Citation preview
Leukemia
History
• Means “white blood” in Greek
• Discovered by Dr. Alfred Velpeau in France, 1827
• Named by pathologist Rudolf Virchow in Germany, 1845
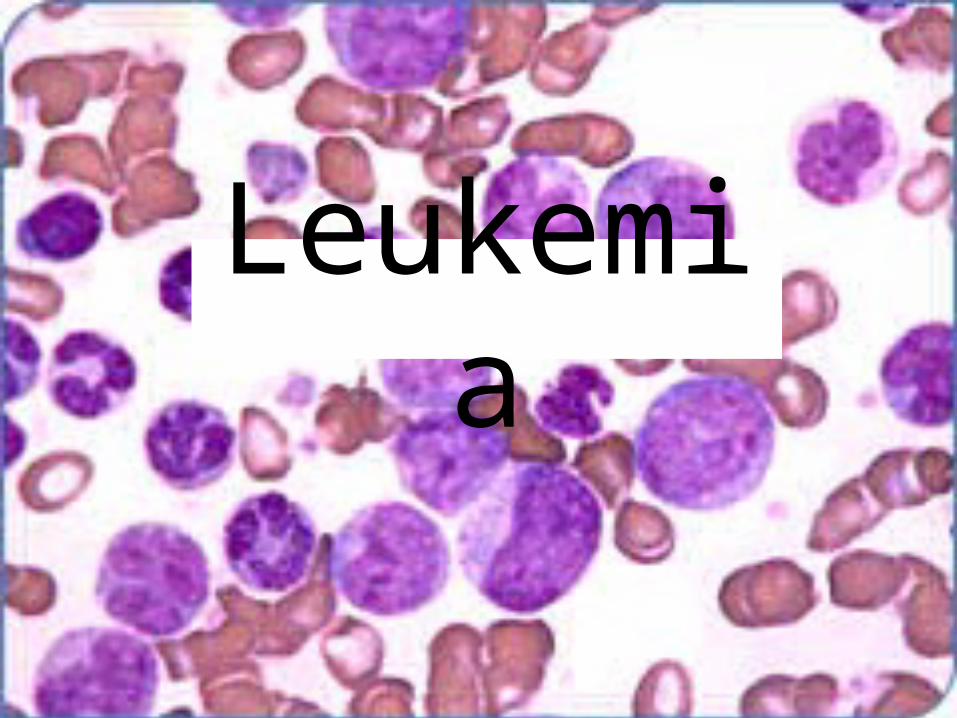
• Is a malignant hematologic disorder characterized by proliferation of abnormal white cells that infiltrate the bone marrow, peripheral blood and organs.
Leukemia
• Acute Leukemias– Blast (precursor) cells– Rapidly fatal if not treated
• Chronic Leukemias– More mature cells– Longer life expectancy
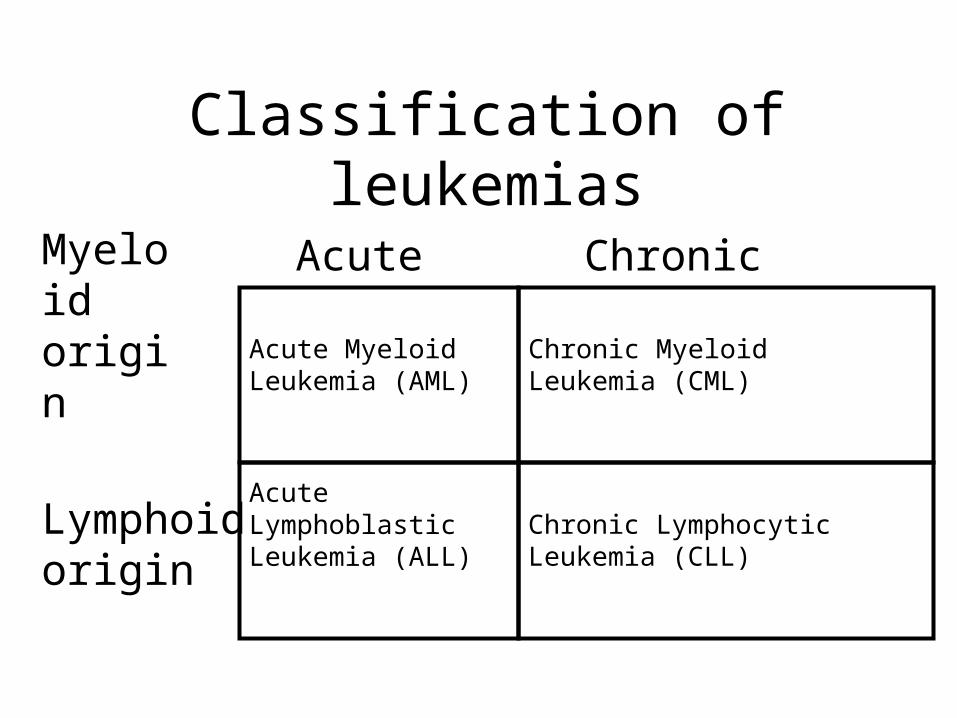
Classification of leukemias
Acute Chronic
Myeloid origin
Lymphoid origin
Acute Myeloid Leukemia (AML)
Acute Lymphoblastic Leukemia (ALL)
Chronic Myeloid Leukemia (CML)
Chronic Lymphocytic Leukemia (CLL)
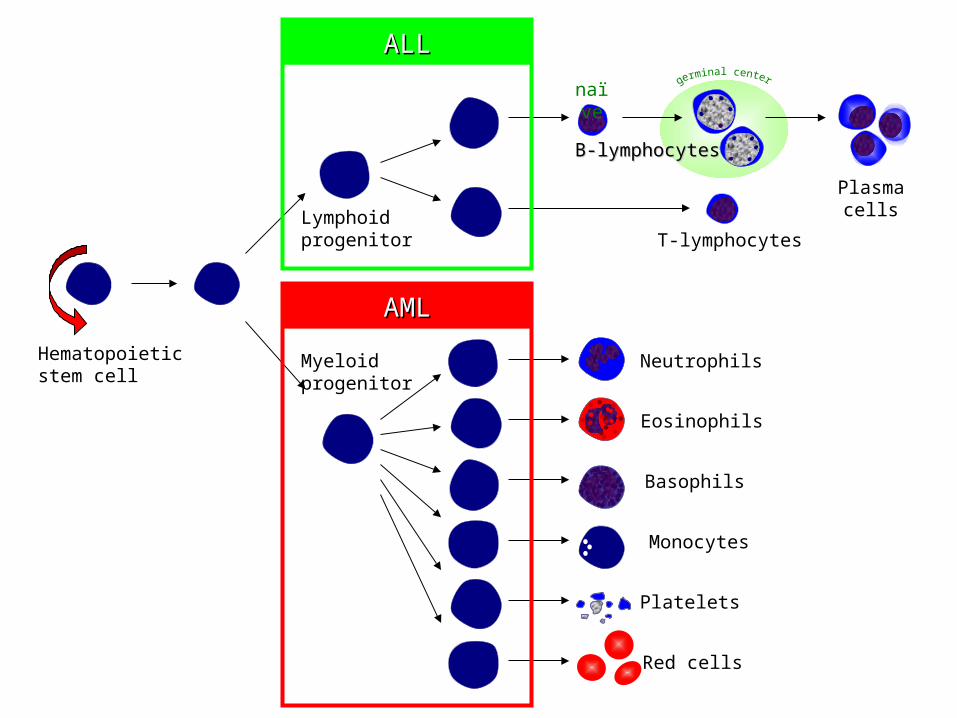
Hematopoieticstem cell
Neutrophils
Eosinophils
Basophils
Monocytes
Platelets
Red cells
Myeloidprogenitor
Lymphoidprogenitor
B-lymphocytesB-lymphocytes
T-lymphocytes
Plasmacells
naïve
ALLALL
AMLAML
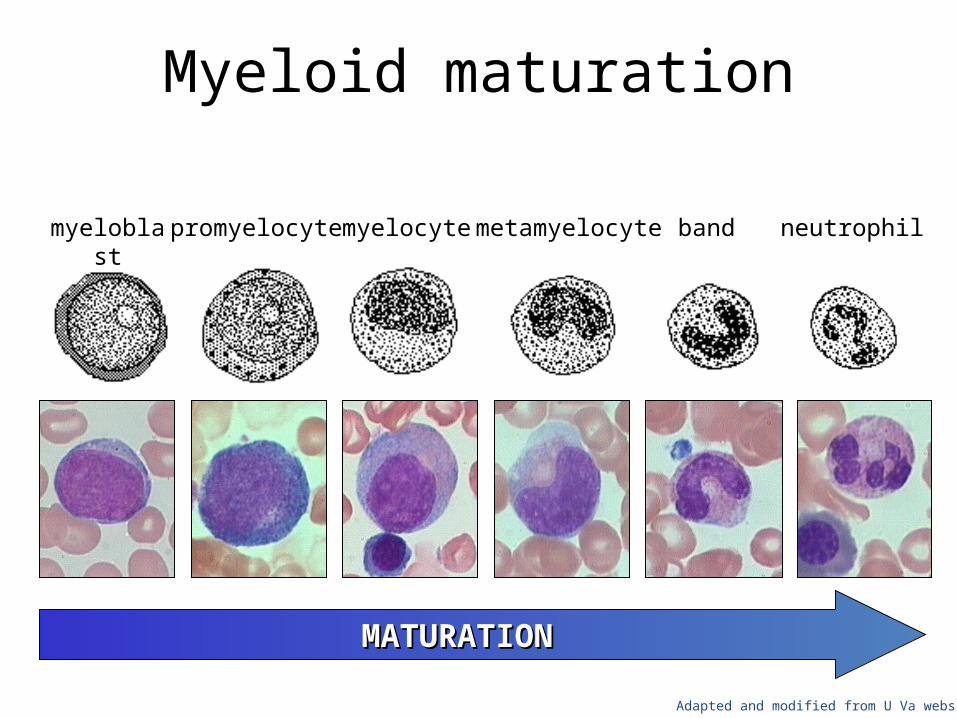
Myeloid maturation
myeloblast promyelocyte myelocyte metamyelocyte band neutrophil
MATURATIONMATURATION
Adapted and modified from U Va website
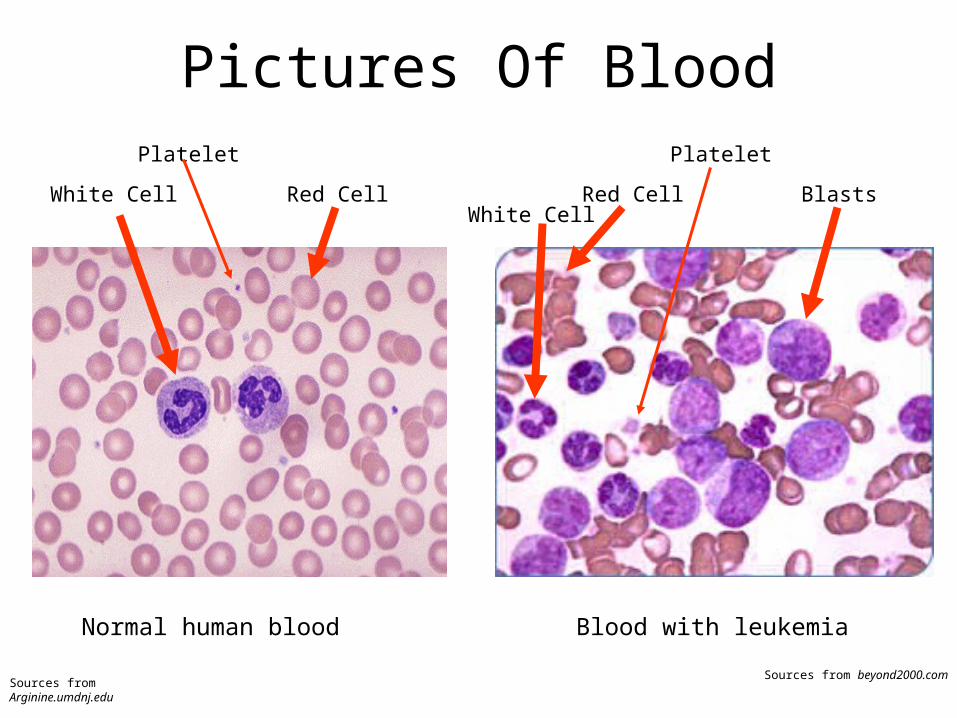
Pictures Of Blood
Normal human blood
White Cell Red Cell
Platelet
Blood with leukemia
BlastsRed Cell
Platelet
White Cell
Sources from Arginine.umdnj.eduSources from beyond2000.com
Acute Lymphoblastic Leukemia
• Proliferation of lymphoblasts– anemia, thrombocytopenia, increased WBC– lymphadenopathy/splenomegaly
• B- or T-cell– flow cytometry
• Most common leukemia of childhood
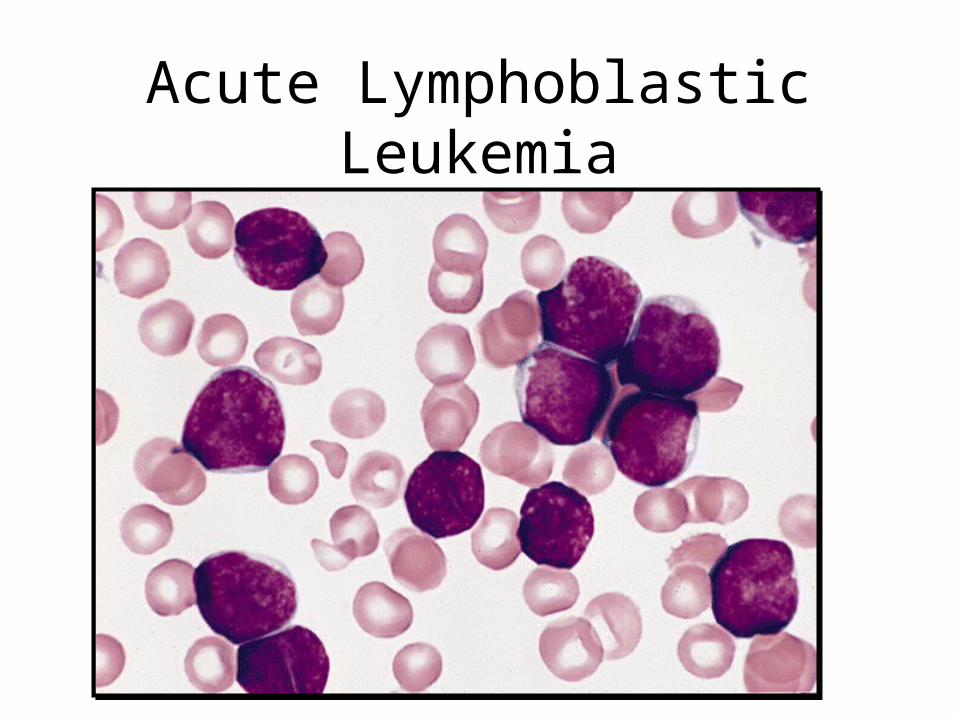
Acute Lymphoblastic Leukemia
Acute Myelogenous Leukemia• Proliferation of myeloblasts
– anemia, thrombocytopenia, increased WBC
• Myeloid, monocytic, RBC, or megakaryocytic– flow cytometry– myeloperoxidase +, TdT-
• Auer rods• Over age of 20
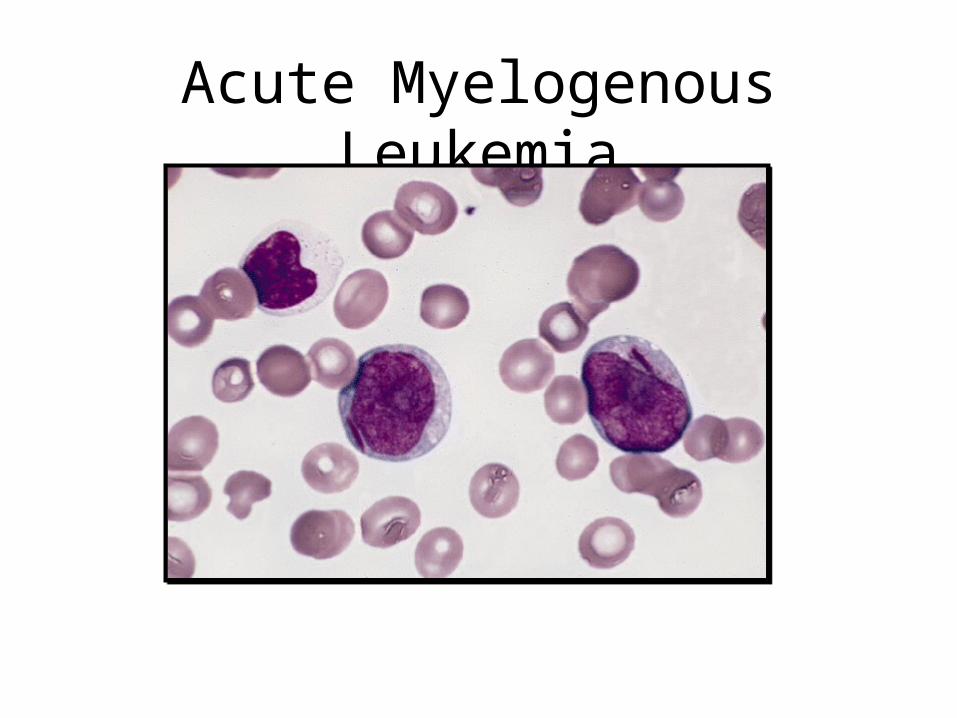
Acute Myelogenous Leukemia
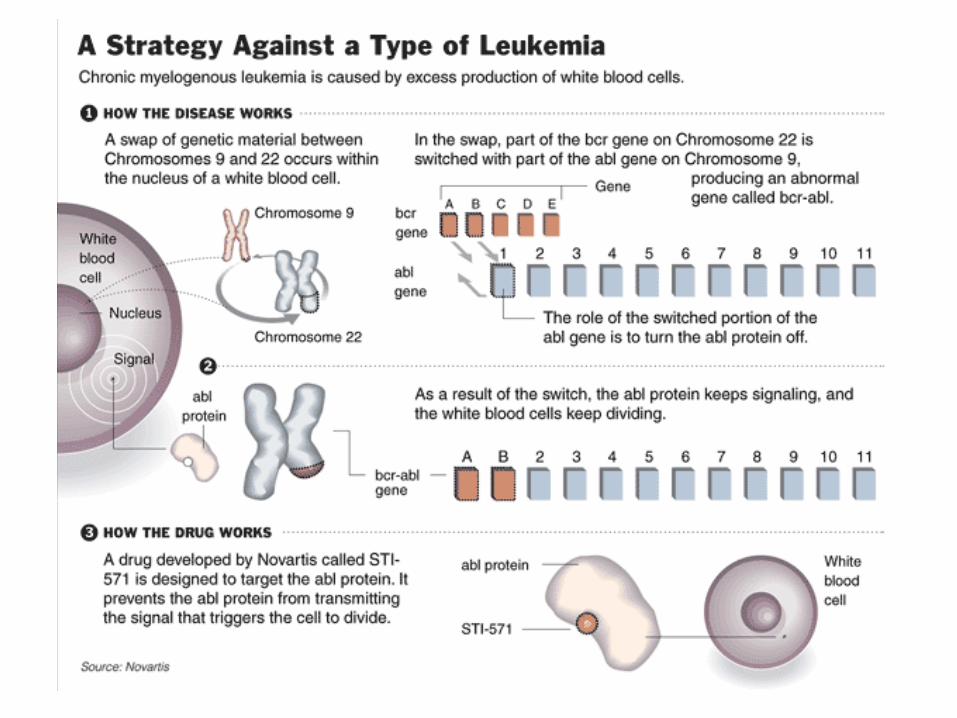
Chronic Myelogenous Leukemia
• One of myeloproliferative diseases (PV, ET)• Proliferation of more mature granulocytes
– normal to increased platelet count– anemia
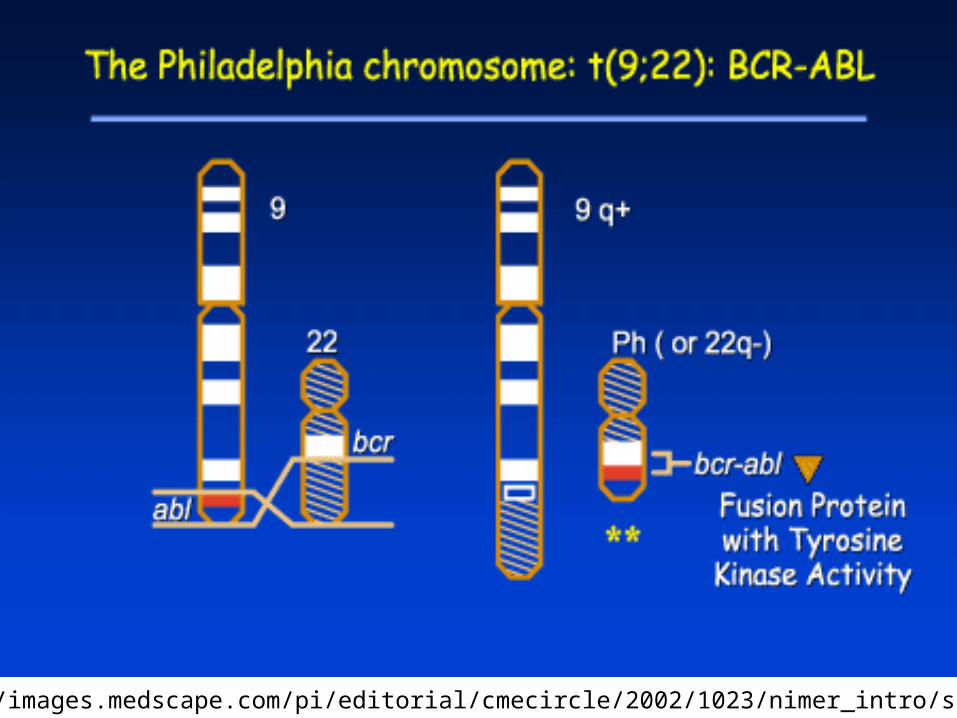
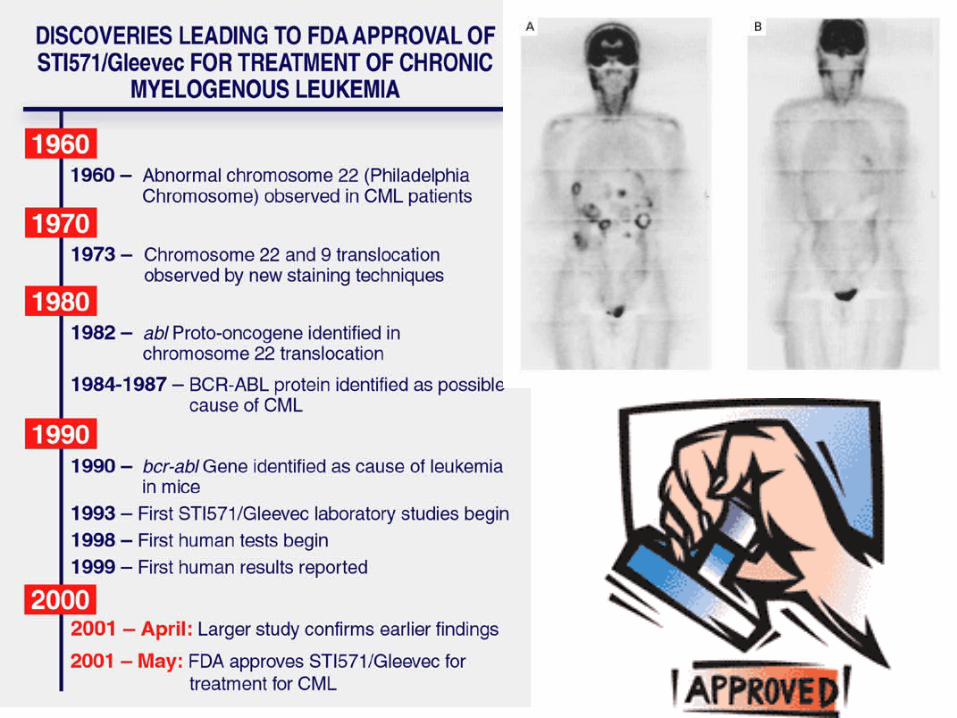
• Splenomegaly• t(9;22) (bcr-abl) (Philadelphia chromosome)
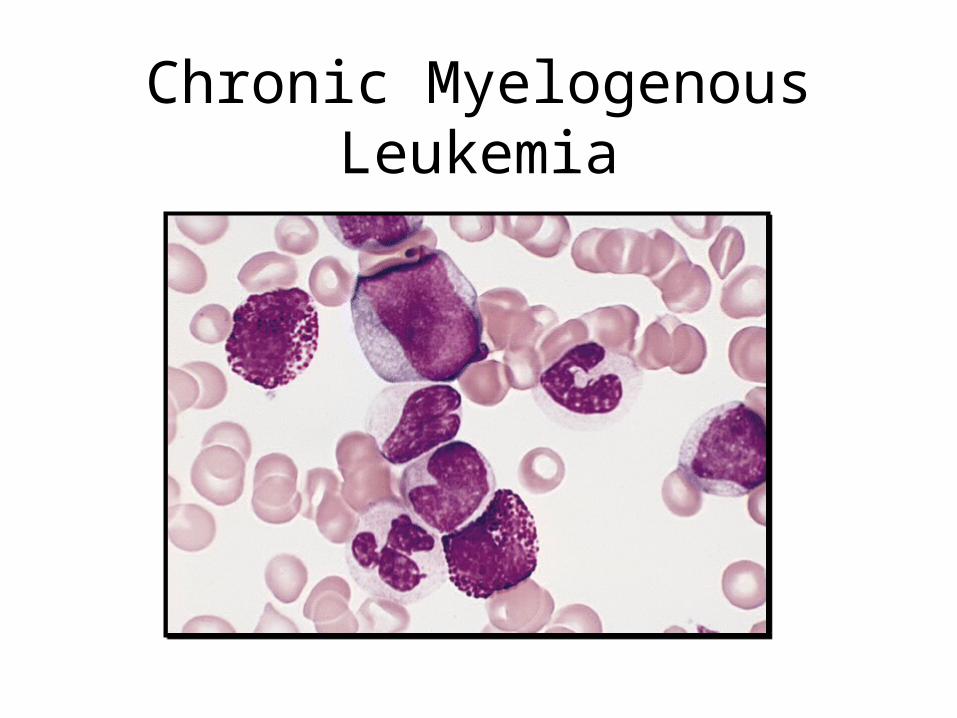
Chronic Myelogenous Leukemia
Chronic Lymphocytic Leukemia
• Proliferation of small mature B-lymphocytes– flow cytometry (monoclonal Kappa or lambda)
• Lymphadenopathy– relationship to small lymphocytic lymphoma
• May have Ab production • 50% 5-year survival
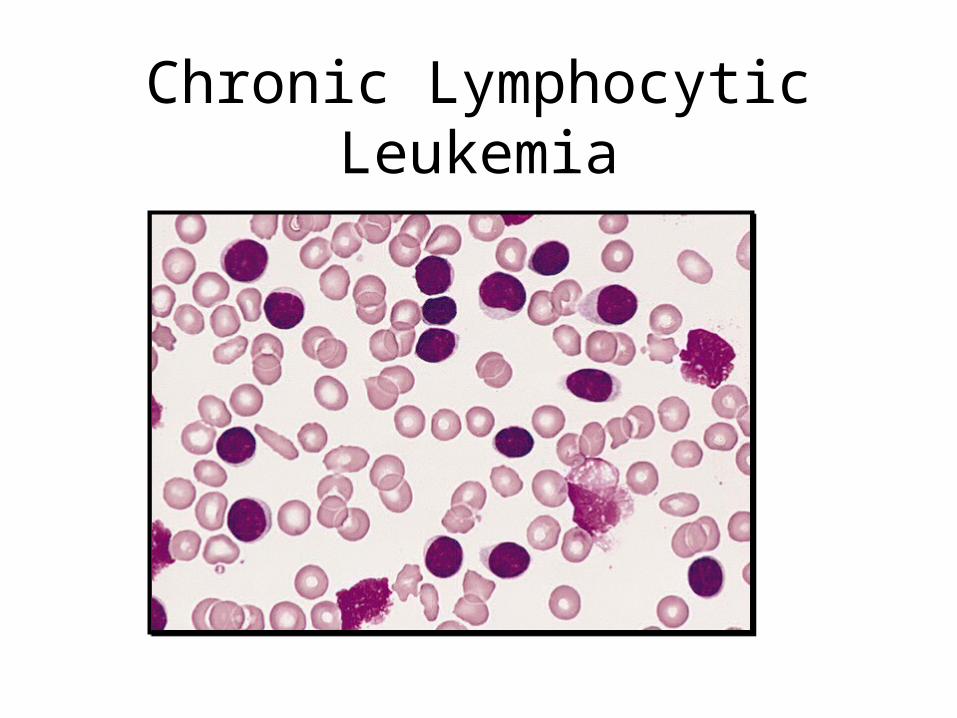
Chronic Lymphocytic Leukemia
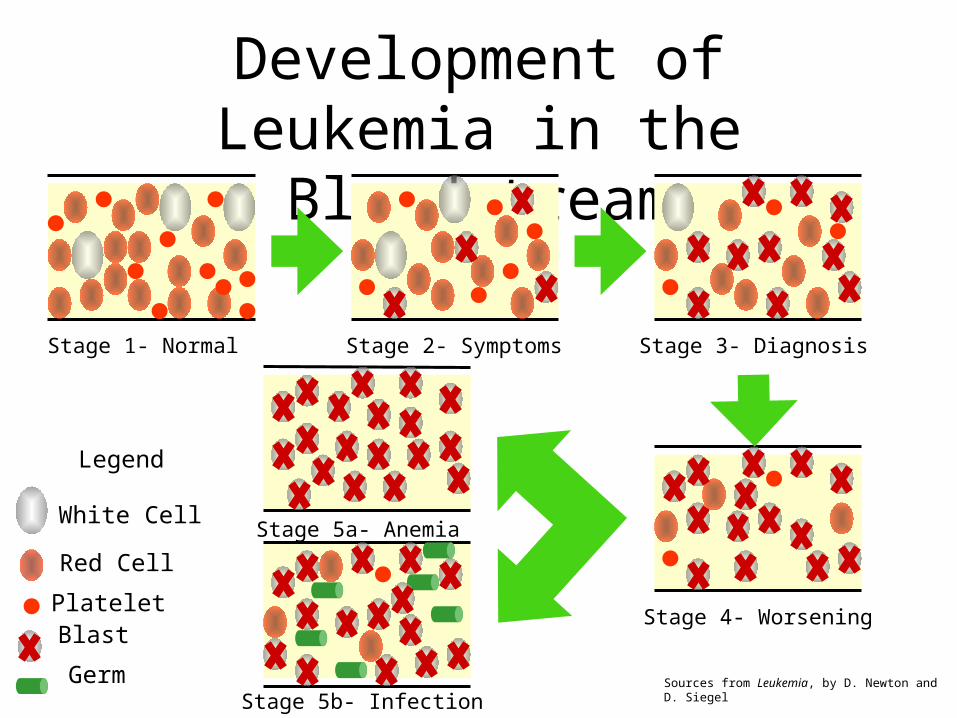
Development of Leukemia in the Bloodstream
Stage 1- Normal Stage 2- Symptoms Stage 3- Diagnosis
Stage 4- Worsening
Stage 5a- Anemia
Stage 5b- Infection
Legend
White Cell
Red Cell
Platelet Blast
Germ Sources from Leukemia, by D. Newton and D. Siegel
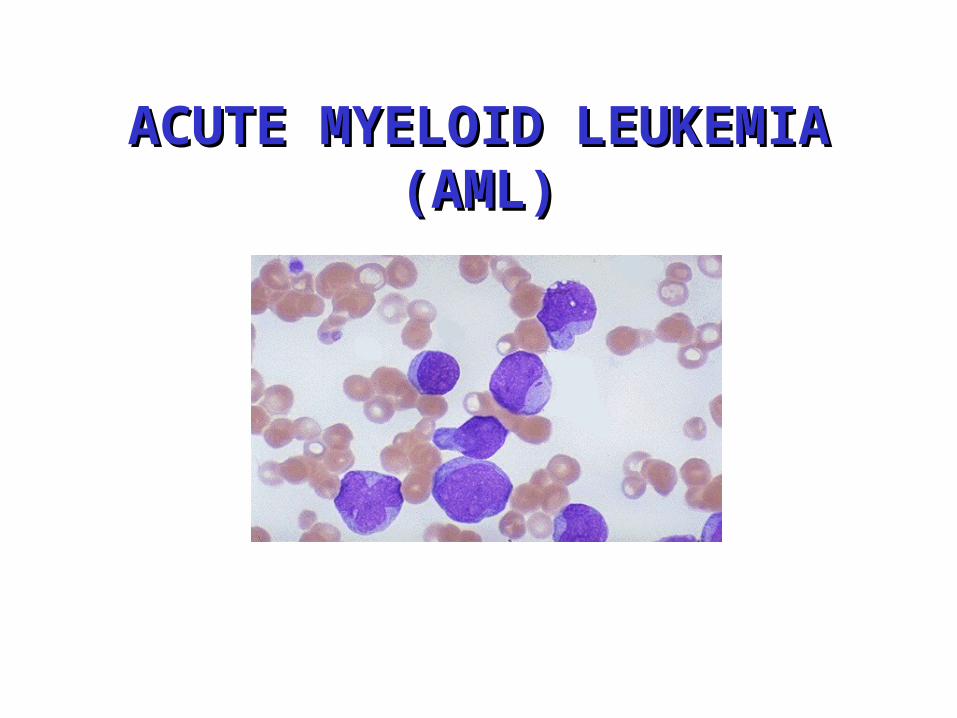
ACUTE MYELOID LEUKEMIA ACUTE MYELOID LEUKEMIA (AML)(AML)
• Acute myeloid leukemia (AML) is one of four types of leukemia.
• AML is cancer of the blood-forming tissue (bone marrow). • Normal bone marrow produces red cells, white cells, and
platelets.• AML causes bone marrow to produce too many immature
white blood cells (blast cells).• Suppresses normal blood cell production.
– Anemia, leucopenia, thrombocytopenia
ACUTE MYELOID LEUKEMIA (AML)Clinical Overview
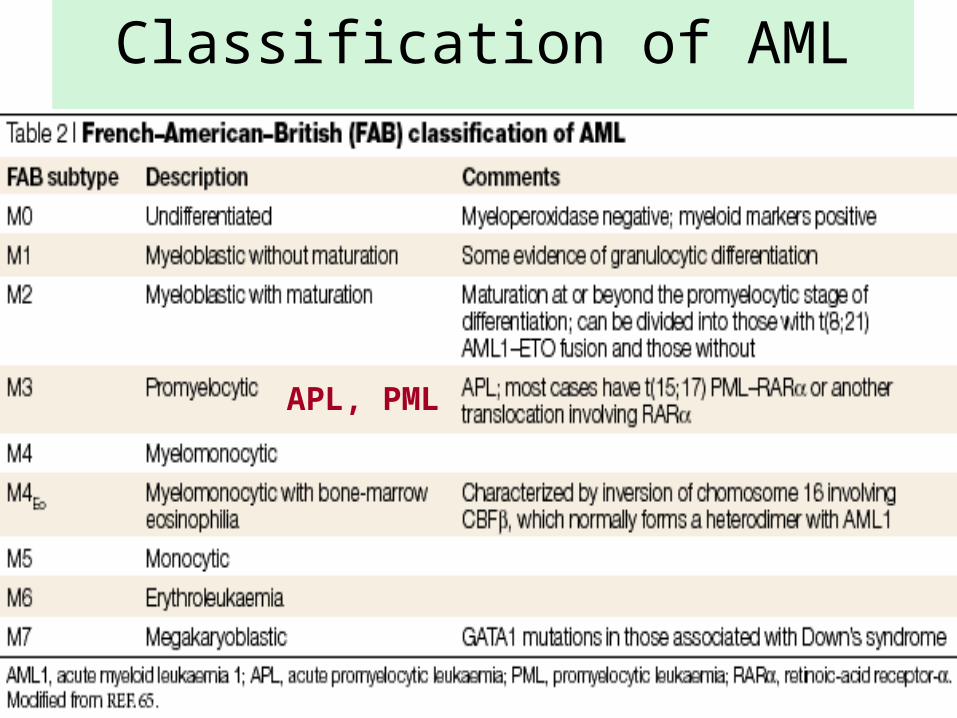
Classification of AML
APL, PML
• Fatigue• Shortness of breath on exertion• Easy bruising• Petechiae• Bleeding in the nose or from the gums• Prolonged bleeding from minor cuts• Recurrent minor infections or poor healing of minor cuts• Loss of appetite or weight loss• Mild fever
Signs and Symptoms
Causation• Genetic changes in AML
• Chromosomal changes lead to activation of oncogenes
• Translocation between chromosomes 8 and 12• Translocation between chromosomes 15 and 17• Deletion of a segment of chromosome 5 or 7
• Genetic factors that predispose an individual to AML• Fanconi’s anemia• Down syndrome• Bloom’s syndrome
Causation• Environmental factors
• Exposure to ionizing radiation• Exposure to benzene• Treatment with alkylating agents or
procarbazine• Treatment with other drugs • Viral oncogenesis (speculative)
• Age• Adults are more likely to develop AML
• Smoking• 20% of AML cases are linked to smoking• Doubles the risk of disease in people older than 60
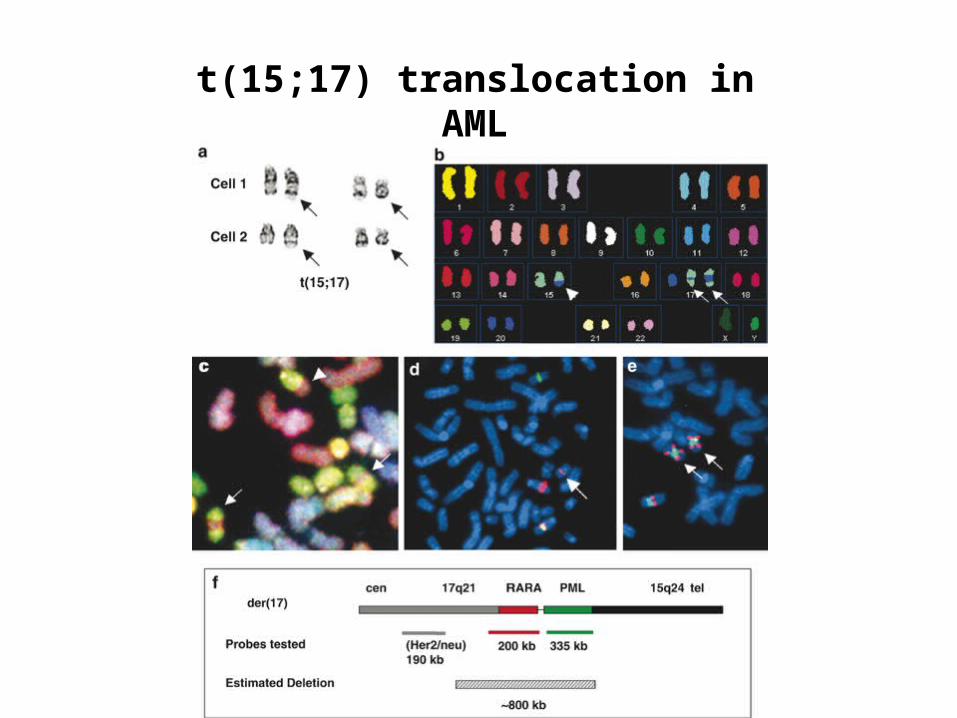
t(15;17) translocation in AML
Clincal manifestations
• symptoms due to:– marrow failure– tissue infiltration– leukostasis– constitutional symptoms– other (DIC)
• usually short duration of symptoms
Marrow failure• neutropenia: infections, sepsis• anemia: fatigue, pallor• thrombocytopenia: bleeding
Infiltration of tissues/organs• enlargement of liver, spleen, lymph nodes• gum hypertrophy• bone pain• other organs: CNS, skin, testis, any organ
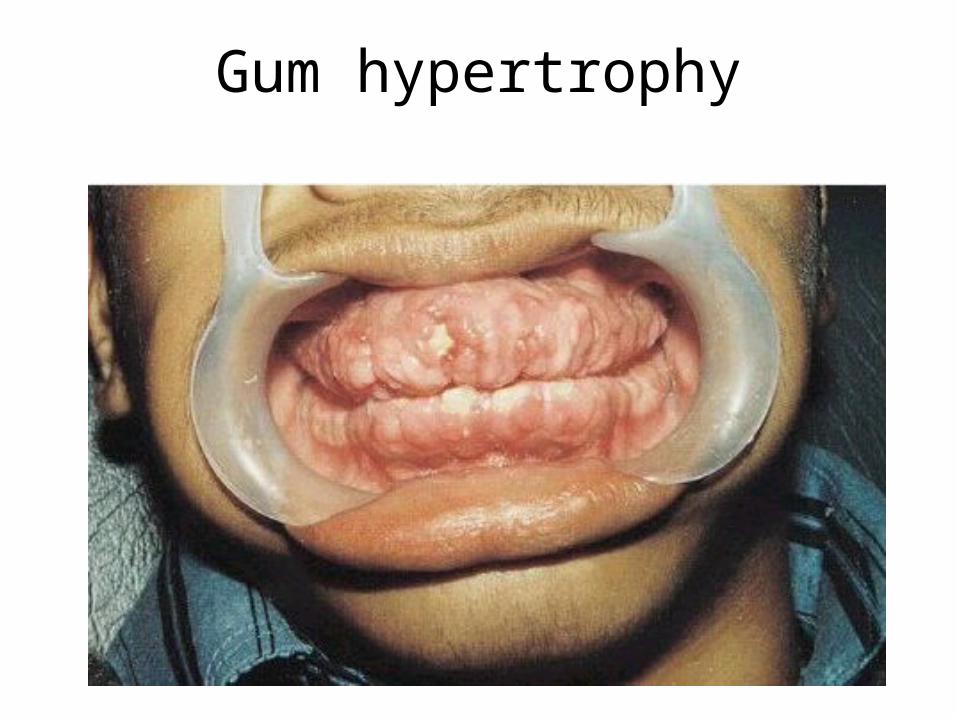
Gum hypertrophy
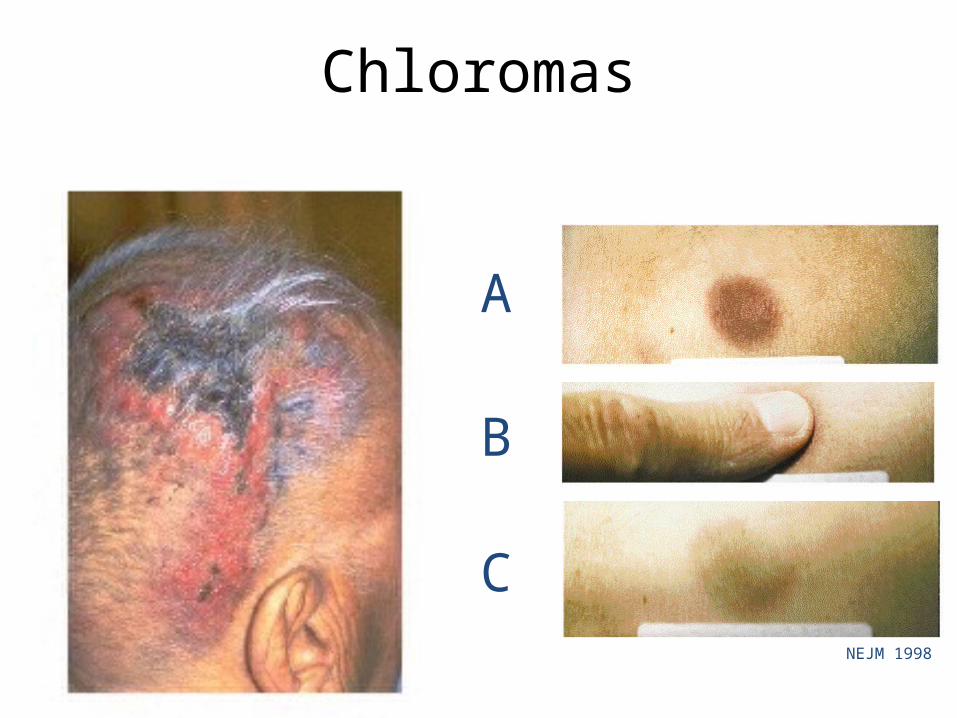
A
B
C
Chloromas
NEJM 1998
Laboratory features
• WBC usually elevated, but can be normal or low
• blasts in peripheral blood• normocytic anemia• thrombocytopenia• neutropenia• DIC
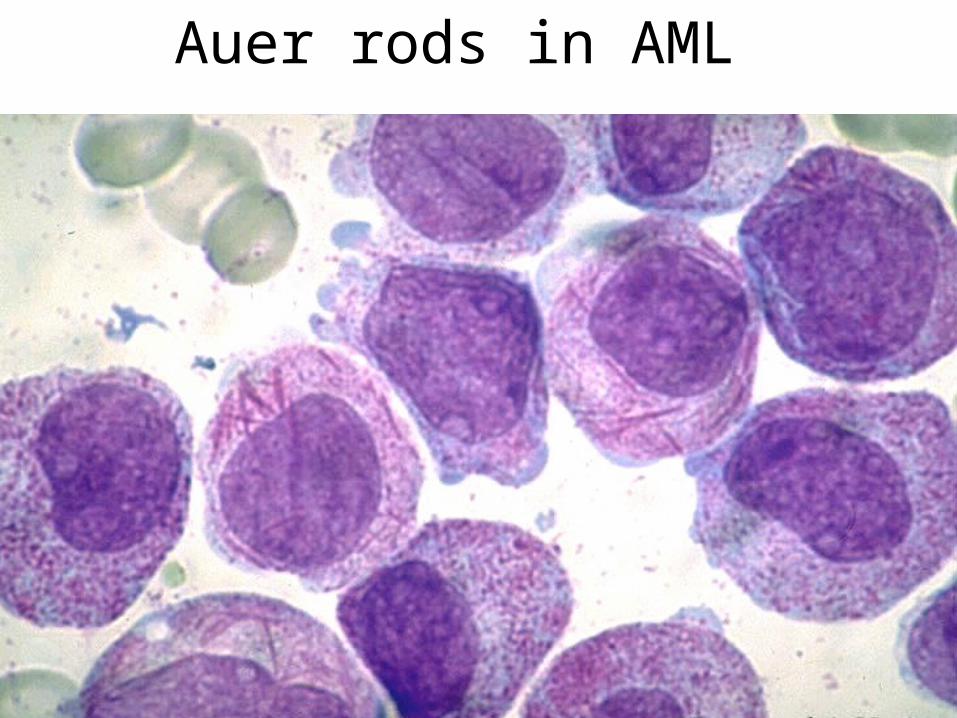
Auer rods in AML
• ChemotherapyPhase One – Remission induction therapyPhase Two – Remission continuation therapy
• Radiation therapy for certain cases• Bone marrow transplantation
Treatments for AML
• Chemotherapy• Induction therapy
• Initial stage of therapy to eradicate systemic and marrow-localized leukemic cells leading to remission
• Combination of an anthrocycline antibiotic and a cytarabine
• Both prevent DNA synthesis thus stopping growth and leading to their death
• If remission is not achieved with the first round of induction therapy, another round is begun
Treatments
• Post-remission therapy • Consolidation therapy
• Goal is to destroy any undetectable leukemic cells • Many different approaches all of which involve
short doses of intensive therapy
• Maintenance therapy• months to years of less intensive therapy to
prevent further recurrence
Treatments
• Bone marrow transplant• Used as a last resort if 3 rounds of induction
therapy have been unsuccessful• Used as or along with post-remission therapy• Two types of transplants are used
• Autologous• Allogeneic
Treatments
• Radiation therapy• Only used in rare cases where leukemic cells
are centralized in one part of the body
Goal of treatment: Remission• Blood cell counts return to normal• Leukemic cells can no longer be found in blood
or marrow
• If at any time after remission is achieved a relapse occurs the initial treatment may be repeated usually with minor changes in protocol
• If after five years of remission there have been no new outbreaks of leukemic cells the patient is considered cured
After remission
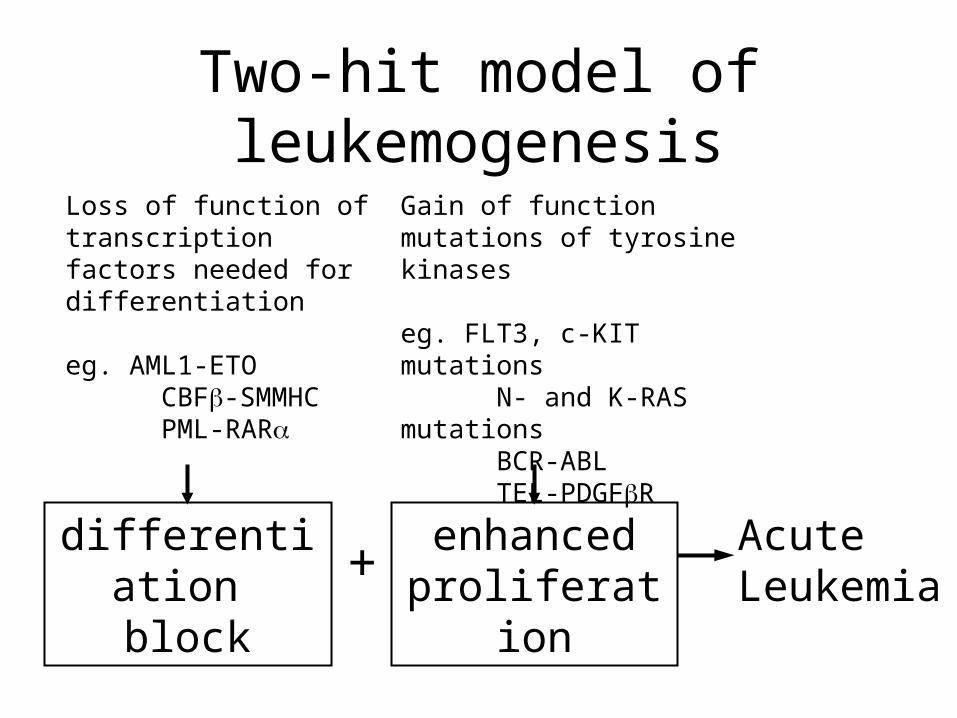
differentiation block
enhancedproliferation
AcuteLeukemia+
Gain of function mutations of tyrosine kinases
eg. FLT3, c-KIT mutations N- and K-RAS mutations BCR-ABL TEL-PDGFR
Loss of function of transcription factors needed for differentiation
eg. AML1-ETO CBF-SMMHC PML-RAR
Two-hit model of leukemogenesis
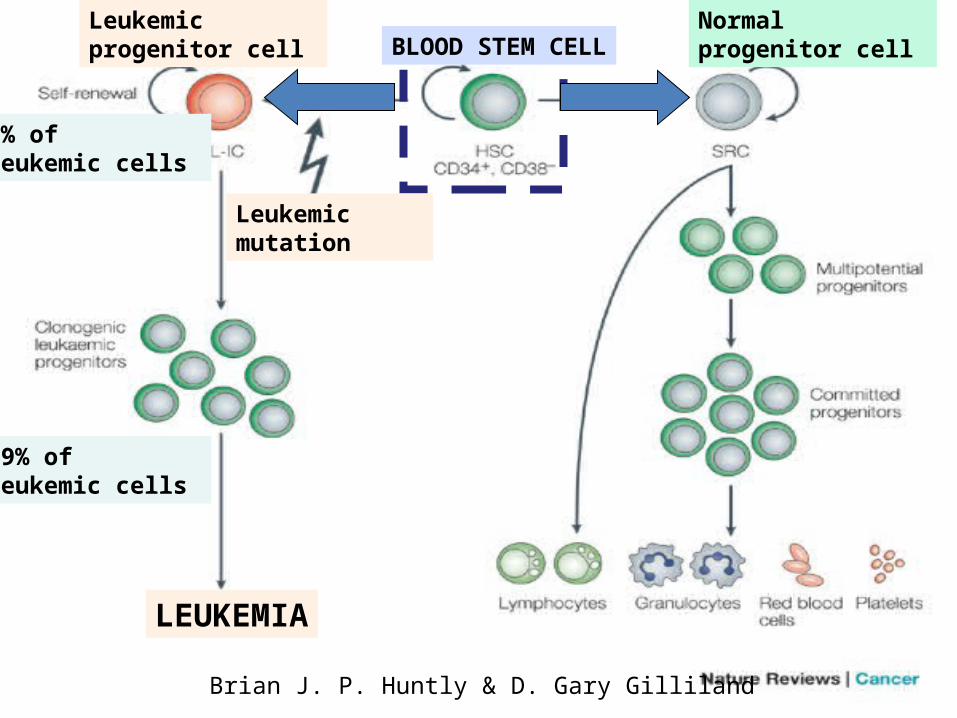
BLOOD STEM CELLNormal progenitor cell
Leukemic progenitor cell
Leukemic mutation
1% of leukemic cells
99% of leukemic cells
LEUKEMIA
Brian J. P. Huntly & D. Gary Gilliland
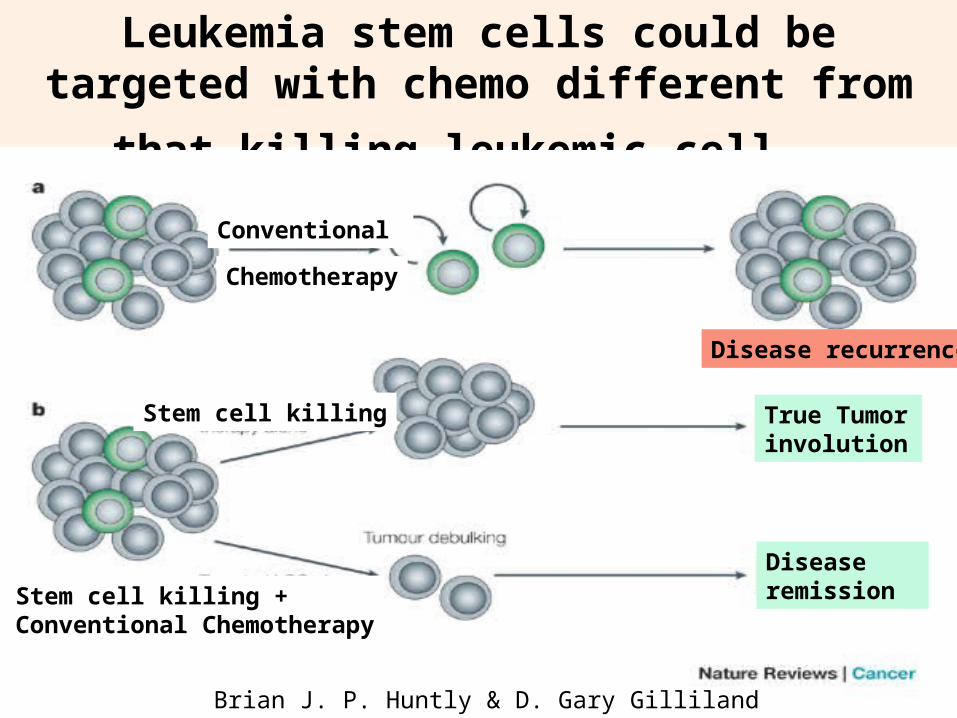
Leukemia stem cells could be targeted with chemo
different from that killing leukemic cell
True Tumor involution
Disease remission
Disease recurrence
Conventional
Chemotherapy
Stem cell killing + Conventional Chemotherapy
Stem cell killing
Brian J. P. Huntly & D. Gary Gilliland
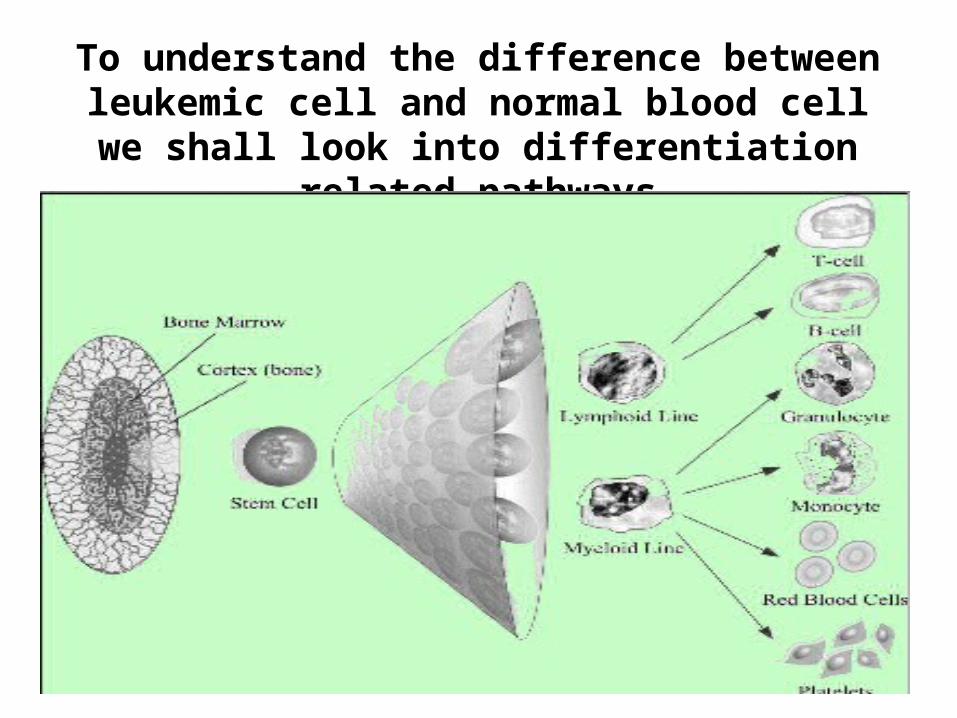
To understand the difference between leukemic cell and normal blood cell we shall look into
differentiation related pathways
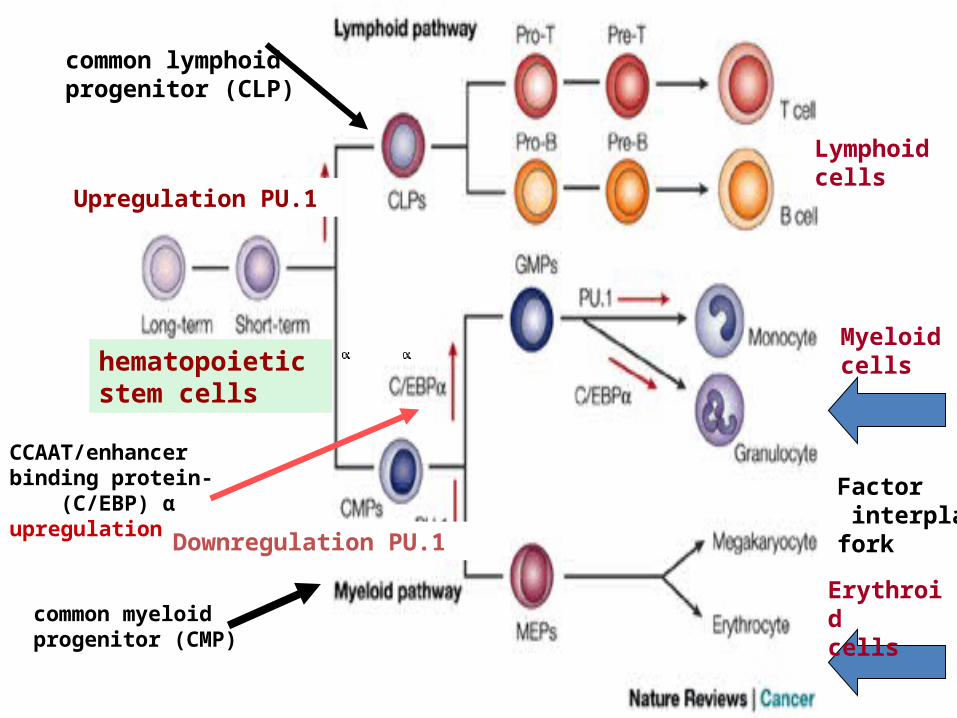
hematopoietic stem cells
Upregulation PU.1
Downregulation PU.1
common lymphoid progenitor (CLP)
CCAAT/enhancer binding protein- (C/EBP) α upregulation
Factor interplay fork
Lymphoidcells
Myeloidcells
Erythroidcellscommon myeloid
progenitor (CMP)
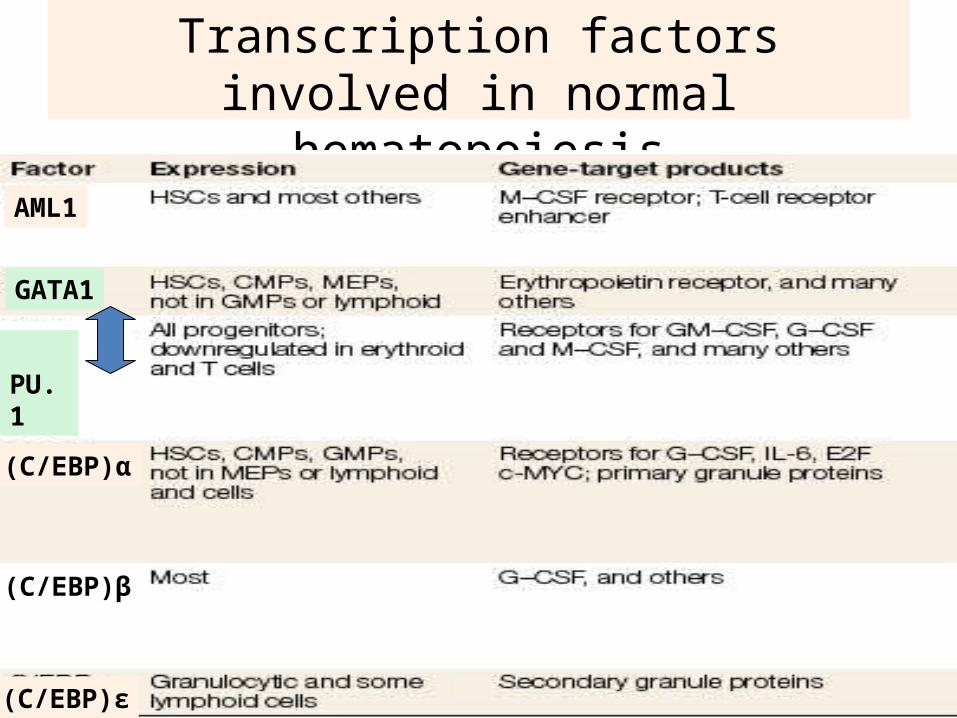
Transcription factors involved in normal hematopoiesis
(C/EBP)α
(C/EBP)β
(C/EBP)ε
AML1
GATA1
PU.1
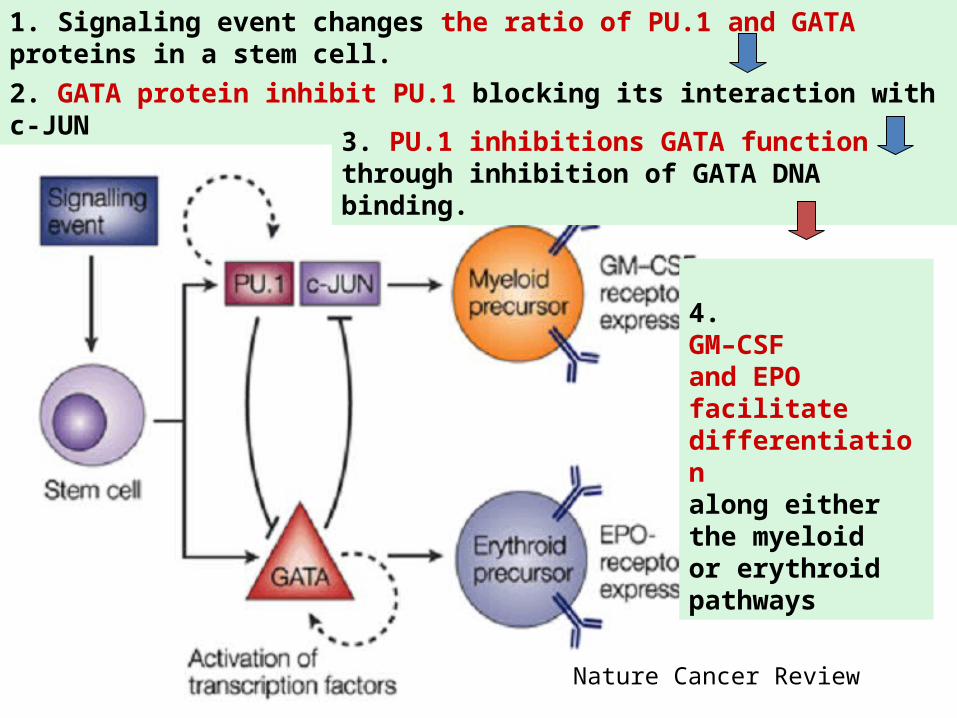
1. Signaling event changes the ratio of PU.1 and GATA proteins in a stem cell.
2. GATA protein inhibit PU.1 blocking its interaction with c-JUN
3. PU.1 inhibitions GATA function through inhibition of GATA DNA binding.
4. GM–CSF and EPO facilitate differentiation along either the myeloidor erythroid pathways
Nature Cancer Review
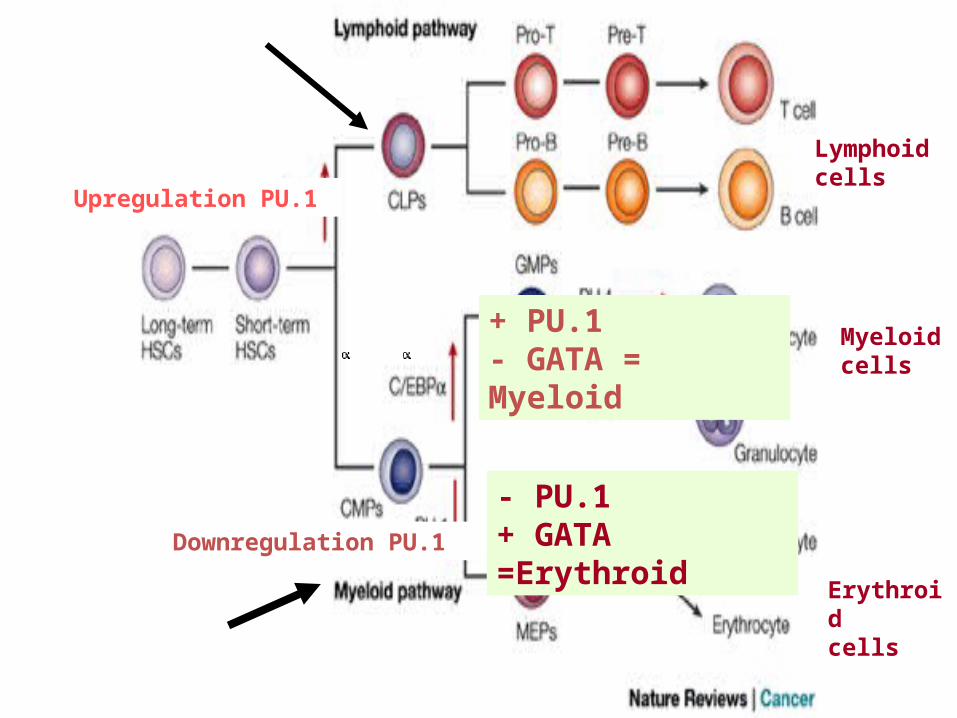
Upregulation PU.1
Downregulation PU.1
Lymphoidcells
Myeloidcells
Erythroidcells
+ PU.1- GATA = Myeloid
- PU.1+ GATA =Erythroid
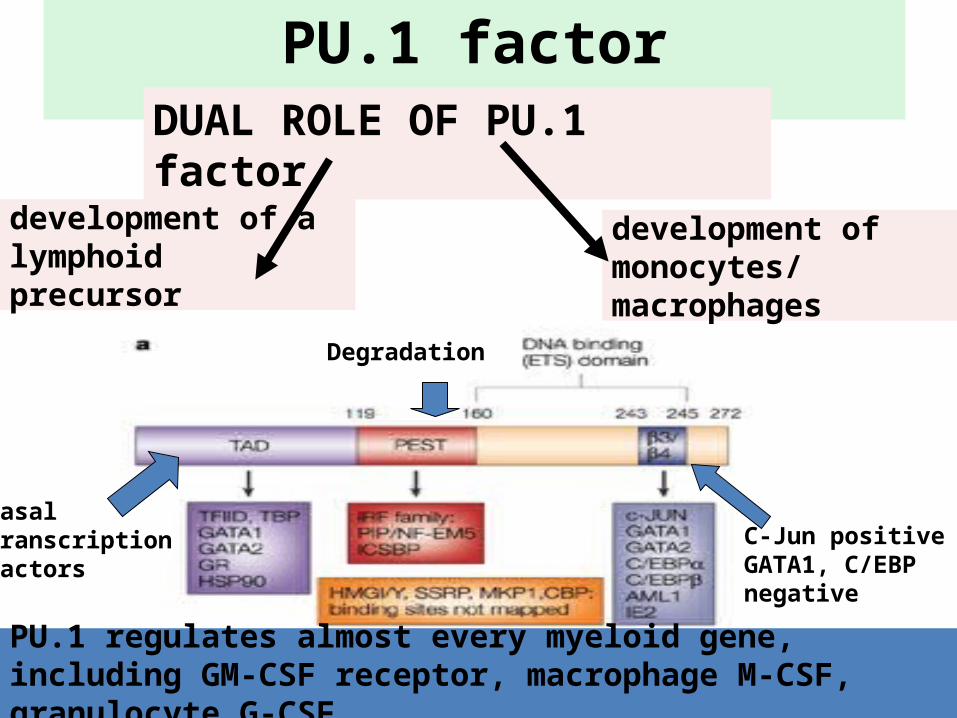
PU.1 factorDUAL ROLE OF PU.1 factor
development of a lymphoidprecursor
development of monocytes/macrophages
PU.1 regulates almost every myeloid gene, including GM-CSF receptor, macrophage M-CSF, granulocyte G-CSF
Basal transcription factors
C-Jun positive GATA1, C/EBPnegative
Degradation
http://images.medscape.com/pi/editorial/cmecircle/2002/1023/nimer_intro/slide03.gif
The Future
• Clinical trials• New drug treatments• Vaccines• Immunotherapy• Leukemia type-specific therapy• Gene therapy
– Block encoding instructions of an oncogene– Target the oncoprotein
• Blood and marrow stem cell transplantation– Bone marrow transplantation provides long-term, disease-free
survival among patients in remission