Embed Size (px)
Citation preview
CID Management Utilization Review Policy and Procedures 1
CID m a n a g e m e n t
Destie Overpeck February 25, 2013 Division of Workers’ Compensation 1515 Clay Street, 17th Floor Oakland, CA 94612 Re: Submission of Utilization Review Policy and Procedures Dear Ms. Overpeck, At Comprehensive Industrial Disability Management (CID) we strive to ensure our clients’ employees receive best-practice clinical care through our utilization review program: the “RITE Solution”. Our solution is a web-based program that allows our clinical peer reviewers to effectively and efficiently review submitted requests for authorization while focusing on quality of care. The CID UR program follows the HIPAA Privacy Rules, URAC WCUM Standards as well as all California labor code and regulations. Our utilization management solution is designed around a core set of customizable technologies and processes that allow the integration of utilization review procedures into claims management. Consequently, the UR information is immediately available to the claims personnel. In CID’s effort to comply with California Labor Code and Regulations we respectfully submit the following Utilization Review Policy & Procedures on behalf of our organization as well as our contracted clients. Respectfully Submitted by,
Todd Andrew Director of Clinical Operations CID Management P.O. Box 4379 Westlake Village, California 91359 866.301.6568 extension 712 e-mail: [email protected]

CID Management Utilization Review Policy and Procedures 2
CID’s Mission Statement
Providing Intelligent UR Solutions
That Ensure Best Clinical Practice
While Managing Cost of Care

CID Management Utilization Review Policy and Procedures 3
Table of Contents: Part 1. Required Elements & Description of the Utilization Review Process Page
A. Medical Director - 9792.7 (a)(1) 4
B. Utilization Management Process Description – 9792.7 (a)(2) 5
C. Utilization Management Process Description for Expedited Reviews – 9792.7 (a)(2)
13
D. Specific Criteria Utilized in the Decision Making Process – 9792.7 (a)(3) 14
B. Qualifications and Functions of Personnel Involved in the Development and Maintenance of the Utilization Review Plan – 9792.7 (a)(4)
15
C. Qualifications and Functions of Personnel Involved in the Implementation of the Utilization Review Plan – 9792.7 (a)(4)
17
D. Description of Claims Administrator’s Process – 9792.7 (a)(5) 20
I. Prior Authorization Process & Claims Administrator Process By Client 21 Part 2. CID Policies and Procedures.
A. Reference List for Specific Policies Addressing CA Labor Code and Regulations
45
B. CID Policies and Procedures 47
Part 3. Sample Letters 397
Upon reques t by the pub l i c , CID sha l l make ava i lab l e th i s comple t e u t i l iza t ion r ev i ew p lan , cons i s t ing o f the po l i c i e s and proc edures , and des c r ip t ion o f the ut i l iza t ion r ev i ew proce s s .

CID Management Utilization Review Policy and Procedures 4
PART 1. Required Elements & Description of the Utilization Review Process A. Medical Director - 9792.7 (a)(1) CID’s Medical Director is Jonathan S. Rutchik, MD, MPH
• California Medical License: # G85804 • Address: P.O. Box 4379 Westlake Village, CA 91359 • Telephone: 866-301-6568
Dr. Rutchik's focus is neurological illness, workplace injuries and environmental exposure. He is in private practice in the San Francisco Bay area and holds a position as an Assistant Clinical Professor in the Division of Occupational Medicine, in the Department of Internal Medicine at the University of California at San Francisco. Dr. Rutchik completed an Internship through the Department of Labor, OSHA, Washington DC: Office of Occupational Medicine. He is a Board Certified Diplomate of the American Board of Preventative Medicine (Occupational and Environmental Medicine) and Board Certified Diplomate of the American Board of Psychiatry and Neurology. In addition, he is a California Qualified Medical Examiner.

CID Management Utilization Review Policy and Procedures 5
B. Utilization Management Process Description – 9792.7 (a)(2) The following is an abbreviated description of the utilization management process followed by CID. Each section references the associated CID Policy so that the reader may refer to the appropriate policy for further details. Toll Free Telephone & Toll Free Fax Access for Submission of Requests
CID shall maintain toll free telephone and toll free fax access from 9:00 AM to 5:30 PM, in all time zones in which they do business, on normal business days for providers to request authorization for medical services and appeals considerations. For purposes of this section, CID defines normal business days as defined in LC 4600.4 and in section 9 of the Civil Code. CID shall maintain toll free telephone with voice mail, and toll free fax access, during all non- business hours for providers to request authorization for medical services and appeals considerations. CID employees and contractors shall return all mail inquiries, voice mail messages, email messages, or fax messages within 1 business day of receipt. Please see CID Policies 5000, 5005, 5010, 5020, and 5030 for more details.
Date of Receipt
Written requests for authorization shall be deemed to have been received by facsimile on the date the request was received if the receiving facsimile electronically date stamps the transmission. If there is no electronically stamped date recorded, then the date of receipt shall be deemed to be the date the request was transmitted. A request for authorization transmitted by facsimile after 5:30 P.M. Pacific Time shall be deemed to have been received by the claims administrator on the following business day as defined in Labor Code section 4600.4 and in section 9 of the civil Code. Where the request for authorization is received by mail and a proof of service by mail exists, the request shall be deemed to have been received five (5) days after the deposit in the mail at a facility regularly maintained by the United States Postal Service. Where the request is delivered via certified mail, return receipt mail, the request shall be deemed to have been received on the receipt date entered on the return receipt. In the absence of a proof of service by mail or a dated return receipt, the request shall be deemed to have been received on the date stamped on the document by the recipient.
Electronic Review File Creation
Upon receipt of a request for authorization or appeals consideration, the client or CID non-clinical administrative staff shall create an electronic review file. The review file shall contain all elements associated with the review including, but not limited to: stakeholders, activity log, relevant dates pertaining to the review, documents received, generated correspondences, past reviews, etc. Please see attached CID Policy 3010 for more details.

CID Management Utilization Review Policy and Procedures 6
Pre-Review Screening
Should any necessary elements be missing from the review as it is being created, CID non-clinical administrative staff may perform pre-review screening. If so, they shall ensure that pre-review screening occurs within 2 business days of receiving the request for authorization or appeals consideration. The CID staff shall record all information gathered in pre-review screening in the CID utilization management electronic review file. CID defines pre-review screening as including any of the following:
▪ Collection of structured clinical data defined as clinical information that is precise and permits exact matching against explicit medical terms, diagnoses or procedure codes, or other explicit choices, without the need for interpretation
▪ Asking scripted clinical questions; ▪ Accepting responses to scripted clinical questions ▪ Taking specific action, including amendment of items contained in the
electronic review file as explicitly linked to each of the possible responses
Pre-review screening shall not include any of the following: ▪ Applying clinical judgment or interpretation; ▪ Accepting unstructured clinical information; ▪ Deviating from script; ▪ Engaging in unscripted clinical dialogue; ▪ Asking clinical follow up questions; ▪ Issuing determinations of any kind
A copy of the Pre-Review Screening Script may be found on page 3100-4 For dates of injury 1/1/2013 or later; and for all requests for authorization received 7/1/2013 or later; if CID non-clinical staff determine that the DWC Form RFA is not completed as defined in section 9792.6.1(t), they may either treat the form as complete and initiate review for compliance with the timeframes for decision set forth in 8CCR9792.9.1(c)(2); or return it to the requesting physician marked “not complete” no later than five (5) business days from receipt. Please see CID Policy 3100 for more details.
Determination of need for new review following denial
Consistent with 8CCR9792.9(o) and 8CCR9792.9.1(h), review of a request for authorization is not required if there has been a denial of the same request from the same provider within 12 months; unless the new request “is supported by a documented change in the facts material to the basis of the utilization review decision.” CID may elect to take no action on a request for authorization if:
The same treatment was denied within the past 12 months; and The denial arose from a request for authorization from the same physician; and There is no documented change in the facts material to the basis of the original denial.
Regarding the question of whether there has been a change in the facts material to the basis of the original denial, there shall be an operating assumption that such change exists and a new review is required; unless there is a finding by a licensed health care provider that there

CID Management Utilization Review Policy and Procedures 7
has been no such change. Such finding requires that there be consideration of whether there has been:
Relevant supportive change in patient presentation; and/or Relevant supportive findings from new diagnostic studies or imaging; and/or Relevant support change in interval clinical history.
Disputes of Liability
Consistent with 8CCR9792.9(b)(1) and 8CCR9792.9.1(b)(1), utilization review of a treatment request may be deferred if the claims administrator disputes liability for either the occupational injury for which the treatment is recommended or the recommended treatment itself on grounds other than medical necessity. If CID disputes liability under this subdivision, it may, no later than five (5) business days from receipt of the DWC Form RFA, issue a written decision deferring utilization review of the requested treatment. The written decision must be sent to the requesting physician, the injured worker, and if the injured worker is represented by counsel, the injured worker's attorney. The written decision shall only contain the following information specific to the request:
1) The date on which the request for authorization was first received. 2) A description of the specific course of proposed medical treatment for which
authorization was requested. 3) A clear, concise, and appropriate explanation of the reason for the claims
administrator’s dispute of liability for either the injury, claimed body part or parts, or the recommended treatment.
4) A plain language statement advising the injured employee that any dispute under this subdivision shall be resolved either by agreement of the parties or through the dispute resolution process of the Workers’ Compensation Appeals Board.
5) The following mandatory language advising the injured employee: “You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me (insert claims adjuster’s name in parentheses) at (insert telephone number). However, if you are represented by an attorney, please contact your attorney instead of me. and “For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-free 1-800-736-7401.”
Initial Clinical Review
Initial Clinical Reviewers perform first level review on requests for authorization. They review the clinical documentation and apply clinical review criteria, approved by the Medical Director and Clinical Review Committee, to the request for authorization. Initial Clinical Reviewers may issue certifications if the request for authorization matches the clinical review criteria and is medically necessary. Initial Clinical Reviewers may not process non-certifications but rather shall forward all reviews for which they are not recommending certification, to a Clinical Peer Reviewer.
CID Management Utilization Review Policy and Procedures 8
Initial Clinical Reviewers may request additional clinical information, which they deem reasonable and necessary to complete utilization management, from the provider via fax, phone, mail or email. Initial clinical reviewers may make a determination that no review is required, consistent with 8CCR9792.9(o) amd 8CCR9792.9.1(h), as described above. Initial clinical reviewers may issue a dispute of liability notice, consistent with 8CCR9792.9(b) and 8CCR9792.9.1(b), as described above. Please see CID Policies 2200-6 and 3200 for more details.
Clinical Peer Review
Clinical Peer Reviewers perform second or third level review on requests for authorization, reconsiderations or appeals consideration. They review the clinical documentation and apply clinical review criteria, approved by the Medical Director and Clinical Review Committee, to the request for authorization. Clinical Peer Reviewers issue determinations of medical necessity. Clinical Peer Reviewers may request additional clinical information, which they deem reasonable and necessary to complete utilization management, from the provider via fax, phone, mail or email.
In the case of concurrent review, medical care shall not be discontinued until the requesting physician has been notified of the decision and a care plan has been agreed upon by the requesting physician that is appropriate for the medical needs of the injured worker. Clinical peer reviewers may make a determination that no review is required, consistent with 8CCR9792.9(o) amd 8CCR9792.9.1(h), as described above. Clinical peer reviewers may issue a dispute of liability notice, consistent with 8CCR9792.9(b) and 8CCR9792.9.1(b), as described above. Please see CID Policy 2200-6, 3300 and 3600 for more details.
Quality Assurance Quality Control Reviewers
Prior to releasing the UR determination to stakeholders, reviews completed by CID initial clinical reviewers and clinical peer reviewers shall be reviewed by QAQC reviewers. QAQC reviewers shall perform day to day quality assurance and quality control monitoring of:
a. Reviewing internal consistency within the review to ensure that the review does not contradict itself.
b. Reviewing completeness of the review to ensure that it addresses all elements of care requested by the requesting physician.
c. Reviewing guidelines applied for relevance to the requested care. d. Reviewing guidelines for appropriate referencing. e. Reviewing the determination for grammar, punctuation, and spelling.
If the QAQC Reviewer notes non-material changes, such as spelling, grammar, or punctuation, they shall make the non-material changes to the review and shall release the review to
CID Management Utilization Review Policy and Procedures 9
stakeholders. However, if the QAQC reviewer notes material changes, such as incomplete reviews or incorrect guidelines, they shall re-assign the review to the initial clinical reviewer or clinical peer reviewer for correction. The QAQC reviewers shall note any common errors of specific initial clinical reviewers or clinical peer reviewers and shall communicate this to the Clinical Director.
Please see Policy 4000 for more details.
Clinical Review Criteria
CID utilizes clinical review criteria recommended by the CID Clinical Review Criteria Committee and approved by the CID Medical Director. The current clinical review criteria utilized are:
a. State of California Medical Treatment Utilization Schedule b. American College of Occupational and Environmental Medicine’s Occupational
Medicine Practice Guidelines, Second Edition (ACOEM) c. The Official Disability Guidelines (ODG) d. The National Guidelines Clearinghouse e. Department of Industrial Accidents Health Care Services Board Treatment
Guidelines, Commonwealth of Massachusetts f. Colorado Department of Labor and Employment Medical Treatment Guidelines g. Delaware Health Care Services Guidelines h. Minnesota Department of Labor and Industry i. Washington State Department of Labor and Industries Medical Treatment
Guidelines j. Wyoming Workers’ Safety and Compensation Division Treatment k. The National Institute of Health’s PubMed scientific literature database. l. CID Internal Guideline #1: Medical Goods and Services for which No Acceptable
Scientific Evidence Exists Please see CID Policy 1100 for more details.
Requests for Additional Information
During the utilization management process, non-clinical administrative staff, initial clinical review staff or clinical peer reviewers may determine that additional information must be requested from the provider in order to make a determination of medical necessity. In this case, the request for additional information shall be sent within 2 business days of receiving the request for authorization from either the claims administrator or the provider, or sooner if required to comply with regulatory timeframes. The CID System shall generate the appropriate correspondences which shall be delivered to the required stakeholders in a manner and a timeframe consistent with the requirements in 8CCR 9792.9 and 8CCR9792.9.1. CID will document all attempts to obtain additional information. If the client has indicated that they do not want CID to distribute correspondences to a party via a method specified by law, the client shall assume the responsibility of distributing these correspondences themselves.
Please see CID Policy 3700 for more details.

CID Management Utilization Review Policy and Procedures 10
Determination Letters Upon conclusion of the review, the CID system shall generate the determination letters. All determination correspondences shall contain the following elements:
a. The date on which a decision is made b. A description of the specific course of proposed medical treatment for which
authorization was requested c. A specific description of the medical treatment services certified, if any. If for a
hospital stay, this shall include the number of days or units of service certified, if any, the next anticipated review point, if any, the new total number of days or services approved, if any, and the date of admission or onset of services, if any.
d. The name of the initial clinical review staff and/or clinical peer reviewer that made the determination
e. For all reviews with an adverse determination, the determination correspondence shall also include:
i. A clinical rationale which shall include: 1. A clear and concise explanation of the reason for the decision. If a
utilization review decision to modify, deny or delay a medical service is due to incomplete or insufficient information, the decision shall specify the reason for the decision and specify the information that is needed.
2. The principle reason regarding medical necessity ii. A description of the medical criteria or guidelines used iii. A written copy of the relevant portion of the criteria or guidelines used iv. Details about the claims administrator’s internal utilization review appeals
process, if any, and a clear statement that the appeal process is on a voluntary basis
v. The specialty of the reviewer, if any vi. The CID contact telephone number vii. The CID hours of availability viii. For California claims, the following elements will be added:
1. A clear statement that any dispute shall be resolved in accordance with the provisions of Labor Code section 4062, and that an objection to the utilization review decision must be communicated by the injured worker or the injured worker's attorney on behalf of the injured worker to the claims administrator in writing within 20 days of receipt of the decision. It shall further state that the 20-day time limit may be extended for good cause or by mutual agreement of the parties. The letter shall further state that the injured worker may file an Application for Adjudication of Claim and a Declaration of Readiness to Proceed (expedited trial) and an expedited hearing.
2. The following mandatory language: “You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me (insert claims adjuster’s name in parentheses) at (insert telephone number). However, if you are represented by an attorney, please contact your attorney instead of me.”
3. The following mandatory language “For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’
CID Management Utilization Review Policy and Procedures 11
Compensation. For recorded information and a list of offices, call toll-free 1-800-736-7401."
4. For dates of injury before 1/1/2013; and notices sent before 7/1/2013, the following mandatory language “"If you disagree with the utilization review decision and wish to dispute it, you must send written notice of your objection to the claims administrator within 20 days of receipt of the utilization review decision in accordance with Labor Code section 4062. You must meet this deadline even if you are participating in the claims administrator’s internal utilization review appeals process.”
5. For dates of injury 1/1/2013 and later; and dates of injury before 1/1/2013 with notices sent 7/1/2013 or after; a clear statement advising the injured employee that any dispute shall be resolved in accordance with the independent medical review provisions of Labor Code section 4610.5 and 4610.6, and that an objection to the utilization review decision must be communicated by the injured worker, the injured worker’s representative, or the injured worker's attorney on behalf of the injured worker on the enclosed Application for Independent Medical Review, DWC Form IMR-1, within 30 calendar days of receipt of the decision.
6. For dates of injury 1/1/2013 and later; and dates of injury before 1/1/2013 with notices sent 7/1/2013 or after; notice of adverse determination shall also include the Application for Independent Medical Review, DWC Form IMR-1, with all fields completed, except for the signature of the employee,; and an addressed envelope for mailing to the Administrative Director or his or her designee.
7. The date of receipt of additional information requested pursuant to 8CCR9792.9.1(f)(1)(A), (B) or (C), if applicable.
8. The following statement: “In the event that you would like to discuss this decision with the reviewer, please call 866-301-6568 x 790 so that a convenient time may be arranged for this discussion. All reviewers are available for at least four hours per week during normal business days from 9:00 a.m. to 5:30 p.m. PST per regulations 9792.9(k).”
On all correspondences to non-physician providers of goods or service, the clinical rationales and guidelines shall be removed consistent with CA Labor Code and Regulations
The CID System shall generate the appropriate correspondences which shall be delivered to the required stakeholders in a manner and a timeframe consistent with 8CCR 9792.9. If the client has indicated that they do not want CID to distribute correspondences to a party via a method specified by law, the client shall assume the responsibility of distributing these correspondences themselves. In such instance, CID shall inform the client of regulatory requirements regarding timelines and parties to be served communications. Copies of generic determination letters have been included following the Policies and Procedures section of this plan. Please note that each client may require customization to the overall content and format of the letters; however CID ensures that all customized letters are compliant with the labor code and regulations.

CID Management Utilization Review Policy and Procedures 12
Please see CID Policy 3800 for more details. Timeframes
The CID RITE software is designed to ensure that reviews are completed within the regulatory timeframes. The system automatically calculates the due date based on type of review (prospective, concurrent, retrospective), date of receipt of request, presence or absence of notification of extension of due date, and the date of receipt of all necessary information reasonably required to make the determination. The Director of Production, Senior Utilization Management Supervisors and QAQC reviewers monitor the timeframes of all reviews to ensure that they are completed timely. In California, timeframes are monitored for compliance with 8CCR 9792.9 and review due dates are set to ensure completion in a timely fashion. 1.0 Prospective decisions shall be made in a timely fashion that is appropriate for the nature
of the injured workers’ condition, not to exceed five (5) business days from the date of receipt of the written request for authorization.
1.1 If appropriate information, which is necessary to render a decision, is not
provided with the original request for authorization, such information may be requested by a reviewer or non-physician reviewer within five (5) business days from the date of receipt of the written request for authorization.
1.2 If the reasonable information is received prior to the fourteenth (14th) calendar
day following the date of receipt of the written request for authorization, the reviewer shall make a decision within five (5) business days of the receipt of the information. . In no event shall the determination be made more than 14 days from the date of receipt of the original request for authorization by the health care provider.
1.3 If the reasonable information requested is not received within 14 calendar days
of the date of the original request for authorization, a reviewer may deny the request with the stated condition that the request will be reconsidered upon receipt of the information requested.
1.4 In no event shall the determination be made more than 14 calendar days from
the date of receipt of the original request for authorization from the health care provider.
1.5 If the review is expedited, the decision shall be made in a timely fashion
appropriate to the injured worker’s condition, not to exceed 72 hours after the receipt of the written information reasonably necessary to make the determination.
2.0 Concurrent decisions shall be made in a timely fashion that is appropriate for the nature
of the injured workers’ condition, not to exceed five (5) business days from the date of receipt of the written request for authorization.
CID Management Utilization Review Policy and Procedures 13
2.1 If appropriate information, which is necessary to render a decision, is not provided with the original request for authorization, such information may be requested by a reviewer or non-physician reviewer within five (5) business days from the date of receipt of the written request for authorization.
2.2 If the reasonable information is received prior to the fourteenth (14th) calendar
day following the date of receipt of the written request for authorization, the reviewer shall make a decision within five (5) business days of the receipt of the information. . In no event shall the determination be made more than 14 days from the date of receipt of the original request for authorization by the health care provider.
2.3 If the reasonable information requested is not received within 14 calendar days
of the date of the original request for authorization, a reviewer may deny the request with the stated condition that the request will be reconsidered upon receipt of the information requested.
2.4 In no event shall the determination be made more than 14 calendar days from
the date of receipt of the original request for authorization from the health care provider.
2.5 If the review is expedited, the decision shall be made in a timely fashion
appropriate to the injured worker’s condition, not to exceed 72 hours after the receipt of the written information reasonably necessary to make the determination.
3.0 For retrospective reviews, decisions shall be communicated to the requesting physician
within 30 days of receipt of the medical information that is reasonably necessary to make this determination.
3.1 If appropriate information, which is necessary to render a decision, is not
provided with the original request for authorization, such information may be requested by a reviewer or non-physician reviewer within thirty (30) calendar days from the date of receipt of the written request for authorization.
3.2 If the reasonable information is received prior to the thirtieth (30th) calendar day
following the date of receipt of the written request for authorization, the reviewer shall make a decision within thirty (30) calendar days of the receipt of the information.
3.3 If the reasonable information requested is not received within 30 calendar days
of the date of the original request for authorization, the reviewer may deny the request with the stated condition that the request will be reconsidered upon receipt of the information requested.
4.0 Consistent with 8CCR9792.10.1(d); for dates of injury 1/1/2013 or after; and for any UR decision communicated to the physician on 7/1/2013 or after; any appeal review must be completed within 15 days of the date of the UR decision. Please see CID Policy 3900 for more details.
CID Management Utilization Review Policy and Procedures 14
Independent Medical Review (IMR) Consistent with 8CCR9792.10.3(c), CID will respond to any request for additional information from the Administrative Director regarding IMR eligibility within 15 days of receipt of request for information. Consistent with 8CCR9792.10.4(d) and (e), documentation required for IMR as described in 8CCR9792.10.5 must be delivered to the independent review organization within:
24 hours of receipt of notification of IMR, for expedited review; otherwise; 15 calendar days of the date designated on notification if transmitted via mail; or 12 calendar days of the date designated on notification if transmitted electronically.
Such documentation shall include, at minimum:
1) A copy of all reports of the employee’s treating physician relevant to the employee’s current medical condition produced within one year prior to the date of the request for authorization, including those that are specifically identified in the request for authorization or in the utilization review determination.
2) A copy of the adverse determination notifying the employee and the employee’s treating physician that the disputed medical treatment was denied, delayed or modified.
3) A copy of all information, including correspondence, provided to the employee concerning the utilization review decision regarding the disputed treatment.
4) A copy of any materials the employee or the employee’s provider submitted in support of the request for the disputed medical treatment.
5) A copy of any other relevant documents or information used in determining whether the disputed treatment should have been provided, and any statements by the claims administrator explaining the reasons for the decision to deny, modify, or delay the recommended treatment on the basis of medical necessity.
6) Response, if any, to any additional issues raised in the employee’s application for independent medical review.
At the same time that documentation is provided to the IMR organization (IMRO), a notification that lists all documents sent to the IMRO shall be sent to the employee or the employee’s representative. Such notice shall also be accompanied by a copy of all documents not previously provided to the employee or the employee’s representative. Thereafter, if CID becomes aware of any newly developed or discovered relevant medical records in its possession, CID shall forward such materials to the IMRO immediately. At the same time, CID shall also provide a copy of such records to the employee, or the employee’s representative, or the employee’s treating physician, unless the offer of medical records is declined or otherwise prohibited by law. Following submission of documentation to the IMRO, the IMRO may request additional information related to medical necessity. Should such request be received by CID, CID shall provide any available information requested within 1 calendar day for expedited review; and within 5 business days for all other reviews.
CID Management Utilization Review Policy and Procedures 15
Utilization Management Process Description for Expedited Reviews – 9792.7 (a)(2) CID shall complete prospective or concurrent utilization management of expedited reviews, either request for authorization or appeals considerations, in a timely fashion appropriate to the injured worker’s condition, not to exceed 72 hours after the receipt of the written information reasonably necessary to make the determination. For the purposes of this section, decisions related to expedited review refer to the following situations:
a. When the injured worker’s condition is such that the injured worker faces an imminent and serious threat to his or her health, including, but not limited to, the potential loss of life, limb, or other major bodily function, or;
b. The normal timeframe for the decision-making process would be detrimental to the injured worker’s life or health or could jeopardize the injured worker’s permanent ability to regain maximum function.
Please note that the provider must indicate the need for an expedited review upon submission of the request.
In emergency situations posing an immediate threat to the health and safety of patients, CID shall inform the party that failure to obtain prior authorization for emergency health care services is not an acceptable basis for refusal to cover medical services provided to treat and stabilize an injured worker, and that emergency health care services may be subject to retrospective utilization review. If the party requires that prospective utilization review be performed in situations where the health or safety of a patient is under immediate threat, the call shall be transferred directly to the Clinical Director, in his/her absence, to the Director of Production/Senior Utilization Management Supervisor. The Clinical Director, Director of Production, or a Senior Utilization Management Supervisor, shall assign the initial clinical reviewer, clinical peer reviewer, and QAQC reviewer that are immediately available for reviews. The availability of each reviewer shall be confirmed by the Clinical Director, Director or Production, or Senior Utilization Management Supervisor by telephone. Until the review is completed, the Clinical Director, Director of Production, or Senior Utilization Management Supervisor, shall evaluate the progress of the review by checking its status at intervals not to exceed 30 minutes. Immediately upon reaching a determination, the CID system shall generate a determination letter that shall be immediately faxed to the provider. The Clinical Director, Director of Production, or Senior Utilization Management Supervisor, shall further contact the requesting provider via telephone to verify the receipt of the determination to ensure its arrival. Please see CID Policy 3900 for more details.

CID Management Utilization Review Policy and Procedures 16
Specific Criteria Utilized in the Decision Making Process – 9792.7 (a)(3) CID utilizes clinical review criteria recommended by the Clinical Review Criteria Committee and approved by the CID Medical Director. Clinical review criteria used by CID reviewers on California reviews are consistent with the Medical Treatment Utilization Schedule. The current clinical review criteria utilized are:
a. State of California Medical Treatment Utilization Schedule b. American College of Occupational and Environmental Medicine’s Occupational Medicine
Practice Guidelines, Second Edition (ACOEM) c. The Official Disability Guidelines (ODG) d. The National Guidelines Clearinghouse e. Department of Industrial Accidents Health Care Services Board Treatment Guidelines,
Commonwealth of Massachusetts f. Colorado Department of Labor and Employment Medical Treatment Guidelines g. Delaware Health Care Services Guidelines h. Minnesota Department of Labor and Industry i. Washington State Department of Labor and Industries Medical Treatment Guidelines j. Wyoming Workers’ Safety and Compensation Division Treatment k. The National Institute of Health’s PubMed scientific literature database.
Materials from NIH PubMed are not to be used as clinical review criteria unless they rise to the level of evidence described in 8CCR9792.2(c)(1)(A); and unless there are no other sources of scientific evidence available (e.g., source of last resort)
Please see CID Policy 1100 for more details.
CID Management Utilization Review Policy and Procedures 17
B. Qualifications and Functions of Personnel Involved in the Development and Maintenance of the Utilization Review Plan – 9792.7 (a)(4) CID’s Utilization Review Plan was developed, and is maintained and updated, by the CID Medical Director in conjunction with the CID Policy and Procedures Committee. Medical Director
Qualifications: Jonathan S. Rutchik, MD, MPH. California Medical License: # G85804 Dr. Rutchik's focus is neurological illness, workplace injuries and environmental exposure. He is in private practice in the San Francisco Bay area and holds a position as an Assistant Clinical Professor in the Division of Occupational Medicine, in the Department of Internal Medicine at the University of California at San Francisco. Dr. Rutchik completed an Internship through the Department of Labor, OSHA, Washington DC: Office of Occupational Medicine. He is a Board Certified Diplomate of the American Board of Preventative Medicine (Occupational and Environmental Medicine) and Board Certified Diplomate of the American Board of Psychiatry and Neurology. In addition, he is a California Qualified Medical Examiner. Functions: Through oversight of the CID Polices and Procedures committee, the CID Medical Director ensures that the utilization management plan remains compliant with the CA Labor Code and Regulations. The Medical Director is responsible for all decisions made in the utilization review process.
CID Policy and Procedures Committee Members
Director of Clinical Operations Qualifications: Todd Andrew, DC. California Chiropractic License: # DC26334. Dr. Andrew's focus is the overall operations of the CID medical cost containment programs. He oversees CID’s national network of physicians and operations staff to provide customized technology and process driven solutions for the workers' compensation industry. Dr. Andrew graduated with his Doctor of Chiropractic degree (summa cum laude) from PCCW as well as an undergraduate degree from the University of Calgary. He has maintained private practice in San Francisco, CA, and has distinguished himself as an Assistant Professor at Palmer College where he taught in the departments of Diagnosis, Technique and Practice. Dr. Andrew previously served as a Qualified Medical Examiner and holds certifications as an Industrial Disability Examiner, Injury Prevention Specialist and Ergonomic Consultant. Functions: Dr. Andrew is a member of the CID Policy and Procedures Committee. Clinical Director Qualifications: Robert Ward, DC. California Chiropractic License: # DC24025. Dr. Ward's focus is the day to day operations and quality management of the CID UR program. His secondary focus is the appropriate integration and delivery of complementary

CID Management Utilization Review Policy and Procedures 18
and alternative medicine within workers' compensation. He has recently served as a Professor at the Southern California University of Health Sciences where he taught in the departments of Diagnosis and Anatomy. Dr. Ward has served as a Qualified Medical Examiner, as the past editor of The Journal of Chiropractic Education, and as a Clinical Peer Reviewer at CID. Functions: The Clinical Director serves as Chair of the CID Policy and Procedures Committee and reports to the Medical Director. The Clinical Director ensures that the CID Policy and Procedures Committee meets as needed to review the CID policies and procedures of the utilization management program. The Clinical Director conveys the recommendations of the committee to the Medical Director for final approval and adoption. Director of Production: Qualifications: Vaghar Haghiri. Mr. Haghiri is a Director of Production at CID. In that role, he helped develop and maintain processes to manage 250,000+ patient reviews, scheduling and work flow for 75+ physicians, and client accounts from both public and private sectors. Mr. Haghiri carries over 10 years experience in customer service and management support and 5 years experience in utilization management. Functions: Mr. Haghiri is a member of the CID Policy and Procedures Committee.
CID Management Utilization Review Policy and Procedures 19
C. Qualifications and Functions of Personnel Involved in the Implementation of the Utilization Review Plan – 9792.7 (a)(4) Medical Director.
Qualifications: Jonathan S. Rutchik, MD, MPH. California Medical License: # G85804 Dr. Rutchik's focus is neurological illness, workplace injuries and environmental exposure. He is in private practice in the San Francisco Bay area and holds a position as an Assistant Clinical Professor in the Division of Occupational Medicine, in the Department of Internal Medicine at the University of California at San Francisco. Dr. Rutchik completed an Internship through the Department of Labor, OSHA, Washington DC: Office of Occupational Medicine. He is a Board Certified Diplomate of the American Board of Preventative Medicine (Occupational and Environmental Medicine) and Board Certified Diplomate of the American Board of Psychiatry and Neurology. In addition, he is a California Qualified Medical Examiner. Functions: The Medical Director is responsible for credentialing of the clinical staff, clinical oversight and quality management of CID’s utilization management program. Consistent with 8CCR 9792.6, the Medical Director is responsible for all decisions made in the utilization review process. CID’s Medical Director fulfills this responsibility by monitoring the clinical staff as well as by ensuring that the policies and procedures utilized within the utilization management process are compliant with the CA Labor Code and Regulations. Through administration and oversight of the Quality Assurance program and all CID utilization management committees, the CID Medical Director ensures that all CID staff and contractors adhere to the utilization management plan through all clinical and non-clinical facets.
Director of Clinical Operations
Qualifications: Todd Andrew, DC. California Chiropractic License: # DC26334. Dr. Andrew's focus is the overall operations of the CID medical cost containment programs. He oversees CID’s national network of physicians and operations staff to provide customized technology and process driven solutions for the workers' compensation industry. Dr. Andrew graduated with his Doctor of Chiropractic degree (summa cum laude) from PCCW as well as an undergraduate degree from the University of Calgary. He has maintained private practice in San Francisco, CA, and has distinguished himself as an Assistant Professor at Palmer College where he taught in the departments of Diagnosis, Technique and Practice. Dr. Andrew previously served as a Qualified Medical Examiner and holds certifications as an Industrial Disability Examiner, Injury Prevention Specialist and Ergonomic Consultant. Functions: The Director of Clinical Operations oversees the general administration of the Utilization Management program. The Director of Clinical Operations facilitates the integration of the utilization management process, the utilization management technology and the utilization management policies and procedures in the CID utilization management system.

CID Management Utilization Review Policy and Procedures 20
Clinical Director
Qualifications: Robert Ward, DC. California Chiropractic License: # DC24025. Dr. Ward's focus is the day-to-day operations and quality management of the CID UR program. His secondary focus is the appropriate integration and delivery of complementary and alternative medicine within workers' compensation. He has recently served as a Professor at the Southern California University of Health Sciences where he taught in the departments of Diagnosis and Anatomy. Dr. Ward has served as a Qualified Medical Examiner, as the past editor of The Journal of Chiropractic Education, and as a Clinical Peer Reviewer at CID.
Functions: The Clinical Director facilitates the day-to-day operations of the Utilization Management program. Acting as the Medical Director’s senior staff member in the Utilization Management program, the Clinical Director assists in supervising all staff and contractors and serves on all committees.
Associate Clinical Directors
Qualifications: The general qualifications of Initial Clinical Reviewers includes: a health profession degree such as, but not limited to, MD, DO, DC, DPM, LAc, PhD, RN; a current license or certification to practice a health profession; and two years professional experience preferred. Associate Clinical Directors must be licensed by a State or by the District of Columbia. Functions: Associate Clinical Directors assist the Clinical Director in facilitating the day-to-day operations and the general administration of the Utilization Management program.
Initial Clinical Reviewers
Qualifications: The general qualifications of Initial Clinical Reviewers includes: a health profession degree such as, but not limited to, MD, DO, DC, DPM, LAc, PhD, RN; a current license or certification to practice a health profession; and two years professional experience preferred. Initial Clinical Reviewers must be licensed by a State or by the District of Columbia. Functions: Initial Clinical Reviewers perform first level review on requests for authorization. They review the clinical documentation and apply clinical review criteria, approved by the Medical Director and Clinical Review Committee, to the request for authorization. Initial Clinical Reviewers may issue certifications if the request for authorization matches the clinical review criteria and is medically necessary. Initial Clinical Reviewers may not process non-certifications but rather shall forward all reviews for which they are not recommending certification, to a Clinical Peer Reviewer. Initial Clinical Reviewers may request additional clinical information, which they deem reasonable and necessary to complete utilization management, from the provider via fax, phone, mail or email.
Clinical Peer Reviewers
CID Management Utilization Review Policy and Procedures 21
Qualifications: The general qualifications of Clinical Peer Reviewers includes: a health profession degree such as, but not limited to, MD, DO, DC, DPM, LAc, PhD; a current license or certification to practice a health profession; five years professional experience preferred; board certification, preferred where applicable, for appeals consideration. Clinical Peer Reviewers must be licensed by a State or by the District of Columbia. Functions: Clinical Peer Reviewers perform second or third level review on requests for authorization, reconsiderations or appeals consideration. They review the clinical documentation and apply clinical review criteria, approved by the Medical Director and Clinical Review Committee, to the request for authorization. Clinical Peer Reviewers issue determinations of medical necessity.
Clinical Peer Reviewers may request additional clinical information, which they deem reasonable and necessary to complete utilization management, from the provider via fax, phone, mail or email.
Quality Assurance Quality Control Reviewers
Qualifications: The general qualifications of QAQC Reviewers includes: a health profession degree such as, but not limited to, MD, DO, DC, DPM, LAc, PhD, RN; a current license or certification to practice a health profession; and two years professional experience preferred. Functions: QAQC Reviewers perform quality assurance review on reviews at any stage of the utilization management process. If the QAQC Reviewer identifies a review with quality assurance issues, they shall return the review to the Initial Clinical Reviewer or Clinical Peer Reviewer for revision. QAQC Reviewers are required to notify the Clinical Director of common quality assurance quality control issues.
Director of Production / Senior Utilization Management Supervisors
Qualifications: The general qualifications of the Director of Production and Senior Utilization Management Supervisors includes a Bachelor’s degree, one year of experience in administrative or customer service, or an equivalent combination of education and experience. Functions: The Director of Production and Senior Utilization Management Supervisors are responsible for providing administrative support services and supervision of non-clinical staff. These individuals oversee the Utilization Management administrative department including: management of all aspects of non-clinical staff personnel including hiring, training, supervision and performance evaluation; performance of QAQC on administrative utilization management procedures including timeframe adherence; oversight of customer satisfaction and customer relations; and communication and consultation with the Medical Director and Clinical Director in regard to performance of daily tasks.
Non-Clinical Administrative Staff
Qualifications: The general qualifications of the Non-Clinical Administrative Staff includes a Bachelor’s degree, one year of experience in administrative or customer service, or an equivalent combination of education and experience. Functions: The Non-Clinical Administrative Staff are responsible for providing administrative support for processes within utilization management and for performing customer service for the various stakeholders in the utilization management process.
CID Management Utilization Review Policy and Procedures 22
D. Description of Claims Administrator’s Process – (Including 9792.7 (a)(5)) A percentage of CID clients choose to outsource their entire Utilization Management process to CID, whereas others choose to perform initial utilization management functions, such as certifying some requests for authorization, in house. For those clients who outsource their entire Utilization Management process to CID, the claims administrators are responsible for notifying all parties how to contact CID for utilization management functions. For inquiries outside of business hours, the claims administrators shall record a message on their voice mail providing CID’s contact information including phone and fax numbers. Further, the client shall maintain a 24 hour voice mail system and incoming fax line to receive requests for authorization during and after business hours. For these clients, as soon as the claims administrator receives a request for authorization, they shall immediately forward it to CID for completion. For those clients who choose to perform initial utilization management functions in-house, said clients must determine if they require CID’s Medical Director, or a Medical Director of their own, to oversee their in-house utilization management process. If the client wishes to have CID’s Medical Director oversee their in-house utilization management process, they must comply with CID Policy 9000 which was developed by CID’s Medical Director. CID Policy 9000, which is attached to this plan, outlines the procedures the clients must follow in the utilization management process. Please refer to CID Policy 9000 for a complete description of the claims administrator’s procedures. If the client wishes to have a non-CID Medical Director oversee their in-house utilization management process, the client must separately file a letter with the Administrative Director which shall include a copy of the policies and procedures they will follow in the performance of utilization management. These policies and procedures must be developed and approved by their own Medical Director. This letter shall further identify CID as their Utilization Review Organization for all requests which are forwarded for peer review. For these clients, CID’s Medical Director shall only be responsible for requests forwarded to CID for review. CID’s Medical Director shall not be responsible for any portion of the utilization management process performed prior to the review being submitted to CID and shall not be responsible for any determinations rendered by the client. Further details about each client’s specific claims administrator’s processes have been included in the pages that follow.
CID Management Utilization Review Policy and Procedures 23
Client – City of Glendale Client letter on file with AD– Yes PMMC letter on file with AD - Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process The City of Glendale utilizes a prior authorization process as follows:
Prior Authorization The following services and/or procedures shall be considered pre-authorized by the City of Glendale. The provider shall not be required to submit requests through utilization review for these services. For all services and/or procedures not addressed on this list, please submit requests for authorization directly to the claims administrator. Physical Therapy • Up to 9 physical therapy visits per claim • Up to 9 occupational therapy sessions per claim Chiropractic Therapy • Up to 6 chiropractic therapy sessions per claim Medications • Over the counter medications • Ibuprofen and NSAIDs • Up to one month prescription of non-narcotic pain medication administered in first month of injury. • Up to one month prescription of muscle relaxants administered in first month of injury where the patient has acute muscle spasm on clinical exam. Diagnostic Testing • Initial x-ray study of a body part if any red-flags listed below are present.
Red Flags: * Direct trauma to body part(s) * Suspected fracture or dislocation
All Specialty Consultations • For accepted body parts/conditions immediately following injury, for the following: • requests for orthopaedics, neurology, surgical intervention, and PM&R Claims Administrator Approvals The City of Glendale claims administrators may issue approvals on requests for authorization that are not addressed by the prior authorization process. The steps that they follow to issue these approvals are outlined in CID’s filing with the Administrative Director’s office and can be found in CID Policy 9000. The approvals issued by the claims administrators, in compliance with CID Policy 9000, are supervised by CID’s medical director. Diagnostic Testing for Fire Fighters Only (does not includes Firefighter Management personnel):
• MRI
CID Management Utilization Review Policy and Procedures 24
• CT scans • EMG/NCS • EKG
Upon request of the treating physician the claims examiners, with the approval of the HR Director, will be allowed to approve EKGs, CT Scans, MRIs, and EMG/NCS, (excluding surface EMGs (SEMGs)), when said diagnostic examinations can reasonably reduce lost time and overtime expenditures, approval will be granted expeditiously. Utilization Review Organization All requests received by the City of Glendale which the adjustors feel may require physician review are forwarded to Preferred Medical Management Consultants. PMMC reviews the requests following steps outlined in PMMC’s and CID’s filings with the AD. The approvals issued by PMMC, in compliance with CID Policy 9000, are supervised by CID’s medical director. All requests received by PMMC which are determined to require physician review are forwarded to CID.
CID Management Utilization Review Policy and Procedures 25
Client – City of Los Angeles Client letter on file with AD– Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process The City of Los Angeles uses a prior authorization process as follows: On July 1, 2010 the City of Los Angeles will implement a Prior Authorization Program. The Prior Authorization Program allows providers in the City’s First Care Panel to provide routine medical procedures on accepted and delayed claims without Utilization Review based on their adherence to the Medical Treatment Utilization Schedule (MTUS) and evidence-based medicine. All treatment must follow the Title 8 CCR § 9792.20-9792.22 MTUS criteria. The Prior Authorization Program will include the following procedures or ancillary services: PLEASE NOTE: All of the following procedures and ancillary services must be provided by the City of Los Angeles’ Contracted Managed Care Providers on the attached list. For MRI or CT Scan Civilian and Fire Claims: Med Focus Police Claims: One Call Medical For Physical Therapy, Occupational Therapy, or Chiropractic Visits Align Networks For Medication and Durable Medical Equipment Cypress Care
Physical Medicine Up to 24 Physical Therapy, Occupational Therapy, or Chiropractic Sessions Up to 18 Acupuncture Sessions
Psychology Up to 12 Psychological Visits for an accepted non-trauma-related pscyh claim Up to 24 Psychological Visits for an accepted trauma-related pscyh claim
Office Visits & Specialty Referrals Routine Office Visit and Follow Ups Specialty Referral
Imaging and Diagnostics Initial MRI or CT Scan EMG/NCS Plain View X-Rays
Medications 1-year of prescription drugs per Pharmacy Benefit Management (PBM) formulary 1-year of Vicodin and/or Flexeril 1 time 60-day authorization of non-formulary prescription drugs, except Class III/IV narcotics Pain pump refills when pain pump implant was previously approved.

CID Management Utilization Review Policy and Procedures 26
Durable Medical Equipment Basic DME: Splits, Crutches, Braces, cane, walker, standard wheelchair rental, off the shelf braces, walking boots, slings, hot and cold packs.
Surgery Surgery for removal of non-spine related hardware. Routine surgeries of the upper extremity Surgical services: In the event that a surgical procedure has been authorized, the associated services listed below are considered to be subject to prior authorization, and do not require separate authorization:
Surgery of any body part
Complete blood count (CBC) Urinalysis (UA) Pre-operative clearance performed by the surgeon (not by any other provider) Up to 18 sessions of post-operative physical medicine (PT, OT, or chiropractic)
Surgery of the foot or ankle
Inpatient stay of up to 2 days Ankle foot orthosis (AFO) Cam walker Cold packs Walking aid (cane, crutches, brace or walker)
Surgery of the knee or leg
Inpatient stay of up to 4 days Bathing seat Cold pack Continuous passive motion (CPM) during inpatient stay Continuous flow cryotherapy (up to 7 days) Walking aid (cane, crutches, brace or walker)
Surgery of the hip/pelvis
Inpatient stay of up to 5 days Assistant surgeon Cold pack Continuous flow cryotherapy (up to 7 days) Walking aid (cane, crutches, brace or walker)
Surgery of the hand/wrist
Cold pack Surgery of the elbow/forearm
Cold pack Surgery of the shoulder
Inpatient stay of up to 2 days Surgery of the lumbar spine
Assistant surgeon Inpatient stay of up to 4 days

CID Management Utilization Review Policy and Procedures 27
Surgery of the cervical spine Assistant surgeon Inpatient stay of up to 2 days Cold pack
No provider notification letters will be sent by the City claims administrators or designated Utilization Review Organization for the procedures or services that fall under this Program. Claims Administrator Approvals The City of Los Angeles in-house claims administrators, and the claims administrators working on the City of Los Angeles account at the designated third party administrator, may issue approvals on requests for authorization. The steps that they follow to issue these approvals are outlined in CID’s filing with the Administrative Director’s office and can be found in CID Policy 9000. The approvals issued by the claims administrators, in compliance with CID Policy 9000, are supervised by CID’s medical director. Utilization Review Organization All requests received by the City of Los Angeles which they determine to require physician review are forwarded to CID.
CID Management Utilization Review Policy and Procedures 28
Client - City of Santa Monica Client letter on file with AD– Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process The City of Santa Monica does not utilize a prior authorization process. Claims Administrator Approvals The City of Santa Monica has not made known to CID the processes they follow in issuing claims administrator approvals, nor the name of the medical director they are utilizing to supervise the approvals*. Please contact the City of Santa Monica if this information is required. * The administrative approvals issued by the City of Santa Monica staff are not supervised by the CID medical director. Consequently, we are not a party to any administrative approvals issued. Utilization Review Organization All requests received by the City of Santa Monica which they determine to require physician review are forwarded to CID.
CID Management Utilization Review Policy and Procedures 29
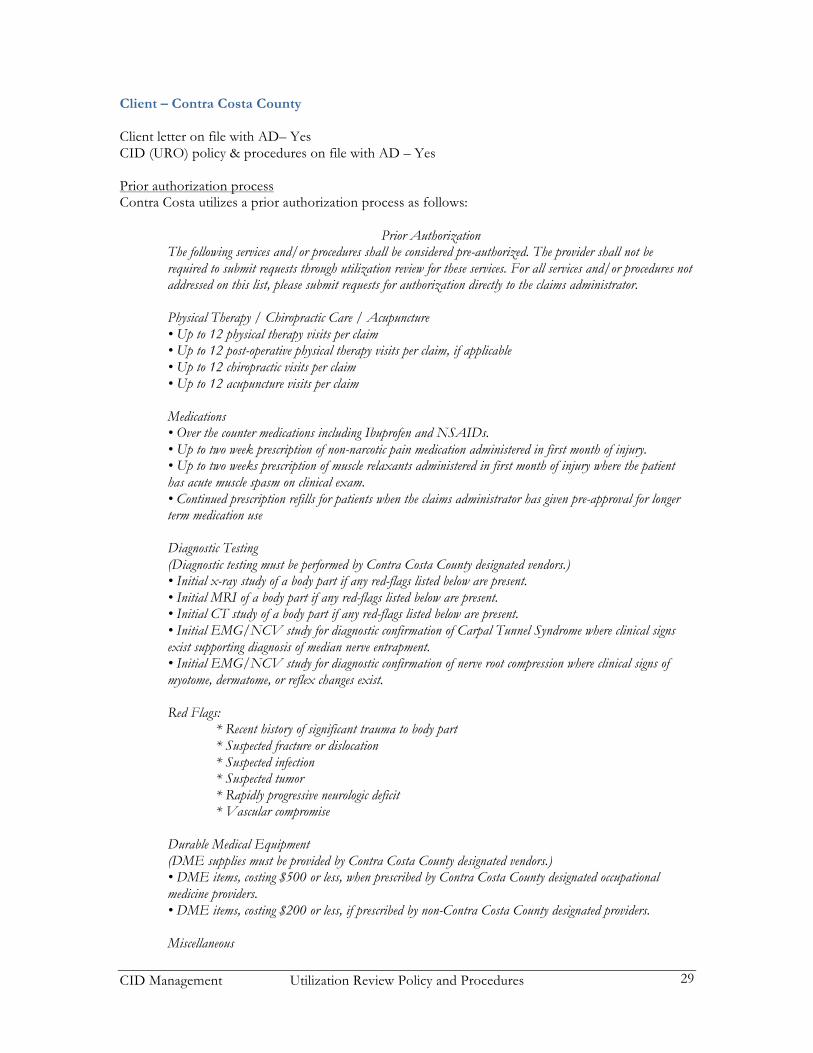
Client – Contra Costa County Client letter on file with AD– Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process Contra Costa utilizes a prior authorization process as follows:
Prior Authorization The following services and/or procedures shall be considered pre-authorized. The provider shall not be required to submit requests through utilization review for these services. For all services and/or procedures not addressed on this list, please submit requests for authorization directly to the claims administrator. Physical Therapy / Chiropractic Care / Acupuncture • Up to 12 physical therapy visits per claim • Up to 12 post-operative physical therapy visits per claim, if applicable • Up to 12 chiropractic visits per claim • Up to 12 acupuncture visits per claim Medications • Over the counter medications including Ibuprofen and NSAIDs. • Up to two week prescription of non-narcotic pain medication administered in first month of injury. • Up to two weeks prescription of muscle relaxants administered in first month of injury where the patient has acute muscle spasm on clinical exam. • Continued prescription refills for patients when the claims administrator has given pre-approval for longer term medication use Diagnostic Testing (Diagnostic testing must be performed by Contra Costa County designated vendors.) • Initial x-ray study of a body part if any red-flags listed below are present. • Initial MRI of a body part if any red-flags listed below are present. • Initial CT study of a body part if any red-flags listed below are present. • Initial EMG/NCV study for diagnostic confirmation of Carpal Tunnel Syndrome where clinical signs exist supporting diagnosis of median nerve entrapment. • Initial EMG/NCV study for diagnostic confirmation of nerve root compression where clinical signs of myotome, dermatome, or reflex changes exist. Red Flags:
* Recent history of significant trauma to body part * Suspected fracture or dislocation * Suspected infection * Suspected tumor * Rapidly progressive neurologic deficit * Vascular compromise
Durable Medical Equipment (DME supplies must be provided by Contra Costa County designated vendors.) • DME items, costing $500 or less, when prescribed by Contra Costa County designated occupational medicine providers. • DME items, costing $200 or less, if prescribed by non-Contra Costa County designated providers. Miscellaneous

CID Management Utilization Review Policy and Procedures 30
• Care consistent with stipulated award • Care consistent with AME/PQME report recommendations • Care consistent with second opinion consultations approved and authorized by Contra Costa County
Claims Administrator Approvals Contra Costa County claims administrators may issue approvals on requests for authorization that are not addressed by the prior authorization process. The steps that they follow to issue these approvals are outlined in CID’s filing with the Administrative Director’s office and can be found in CID Policy 9000. The approvals issued by the claims administrators, in compliance with CID Policy 9000, are supervised by CID’s medical director. Utilization Review Organization All requests received by Contra Costa County which require physician review are forwarded to CID.
CID Management Utilization Review Policy and Procedures 31
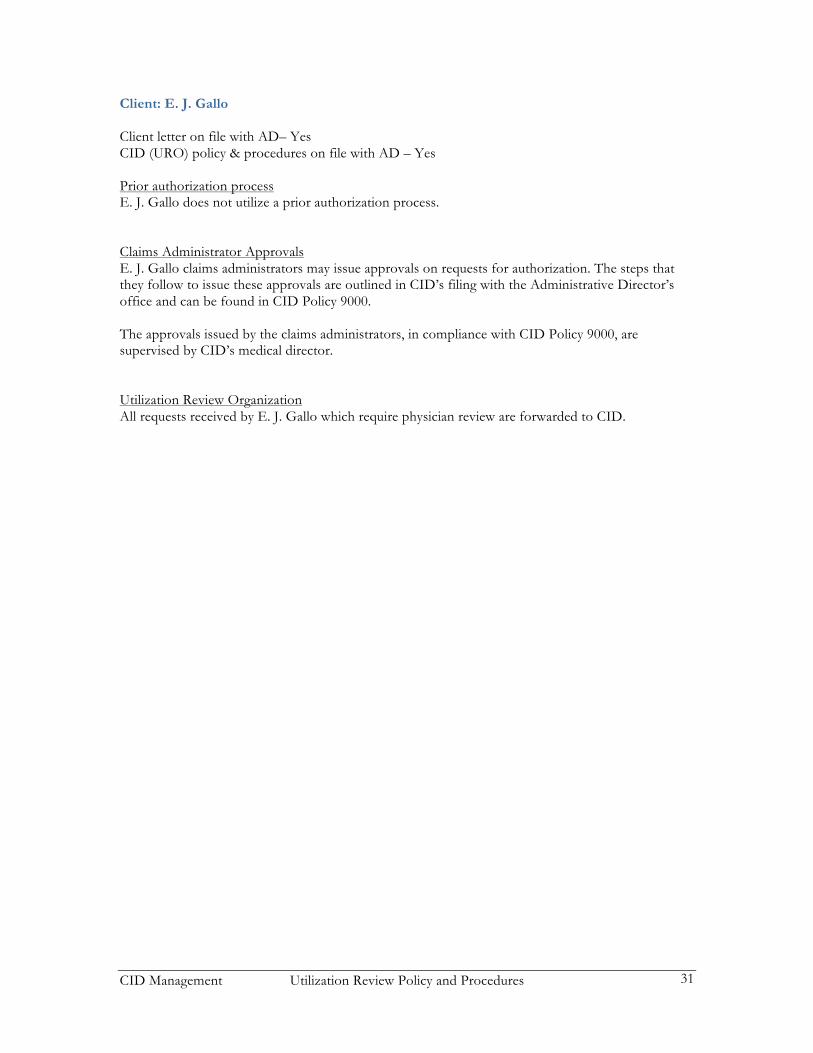
Client: E. J. Gallo Client letter on file with AD– Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process E. J. Gallo does not utilize a prior authorization process. Claims Administrator Approvals E. J. Gallo claims administrators may issue approvals on requests for authorization. The steps that they follow to issue these approvals are outlined in CID’s filing with the Administrative Director’s office and can be found in CID Policy 9000. The approvals issued by the claims administrators, in compliance with CID Policy 9000, are supervised by CID’s medical director. Utilization Review Organization All requests received by E. J. Gallo which require physician review are forwarded to CID.

CID Management Utilization Review Policy and Procedures 32
Client – Fontana Unified School District Client letter on file with AD– Yes PMMC letter on file with AD - Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process Fontana Unified School District (FUSD) utilizes a prior authorization process as follows:
Prior Authorization Per CA Department of Industrial Relations, Title 8, Section 5.5.1, Utilization Review Standards, Section 9792.7(a)(5). The following services and/or procedures shall be considered authorized. The provider shall not be required to submit requests through utilization review for these services. For all services and/or procedures not addressed on this list, please submit requests for authorization directly to the claims administrator. Physical Therapy/Occupational Therapy • First 8 physical therapy visits for the neck and spine • First 6 physical therapy visits for all other body parts to include the knees, ankle, etc. Any request in
excess of 8 visits for the spine and neck, or 6 visits for all other body parts, should be forwarded to Fontana Unified School District.
• First 8 Occupational Therapy visits for the hand and foot only.
Post-Operative Physical Therapy/Occupational Therapy • First 10 physical therapy/occupational therapy sessions post-operatively Medications • Over the counter medications including Ibuprofen and NSAIDs. • Up to two week prescription of non-narcotic pain mediation administered in the first two months of
injury Diagnostic Testing (Diagnostic testing must be performed by FUSD designated vendors.) • X-ray study of a body part if any red-flags listed below are present. • Initial MRI of a body part if any red-flags listed below are present. • Initial CT study of a body part if any red-flags listed below are present. • Initial EMG/NCV study for diagnostic confirmation of Carpal Tunnel Syndrome where clinical signs exist supporting diagnosis of median nerve entrapment. • Initial EMG/NCV study for diagnostic confirmation of nerve root compression where clinical signs of myotome, dermatome, or reflex changes exist. Red Flags:
* Recent history of significant trauma to body part * Suspected fracture or dislocation * Suspected infection * Suspected tumor * Rapidly progressive neurologic deficit * Vascular compromise
Durable Medical Equipment (DME supplies must be provided by FUSD designated vendors)

CID Management Utilization Review Policy and Procedures 33
• DME items costing $100 or less. As a reminder, FUSD has its own durable medical equipment provider. Please send us your prescription in writing and we will process the request for you.
All Specialty Consultations: For accepted body parts/conditions immediately following injury, for the following: * Request for orthopaedics, neurology, surgical intervention, and PM&R AME/QME: Requests for med-legal evaluations/diagnostics
Claims Administrator Approvals FUSD claims administrators may issue approvals on requests for authorization that are not addressed by the prior authorization process. The steps that they follow to issue these approvals are outlined in CID’s filing with the Administrative Director’s office and can be found in CID Policy 9000. The approvals issued by the claims administrators, in compliance with CID Policy 9000, are supervised by CID’s medical director. Utilization Review Organization All requests received by FUSD which the adjustors feel may require physician review are forwarded to peer review. The approvals issued by PMMC, in compliance with CID Policy 9000, are supervised by CID’s medical director. All requests received by PMMC which are determined to require physician review are forwarded to CID.
CID Management Utilization Review Policy and Procedures 34
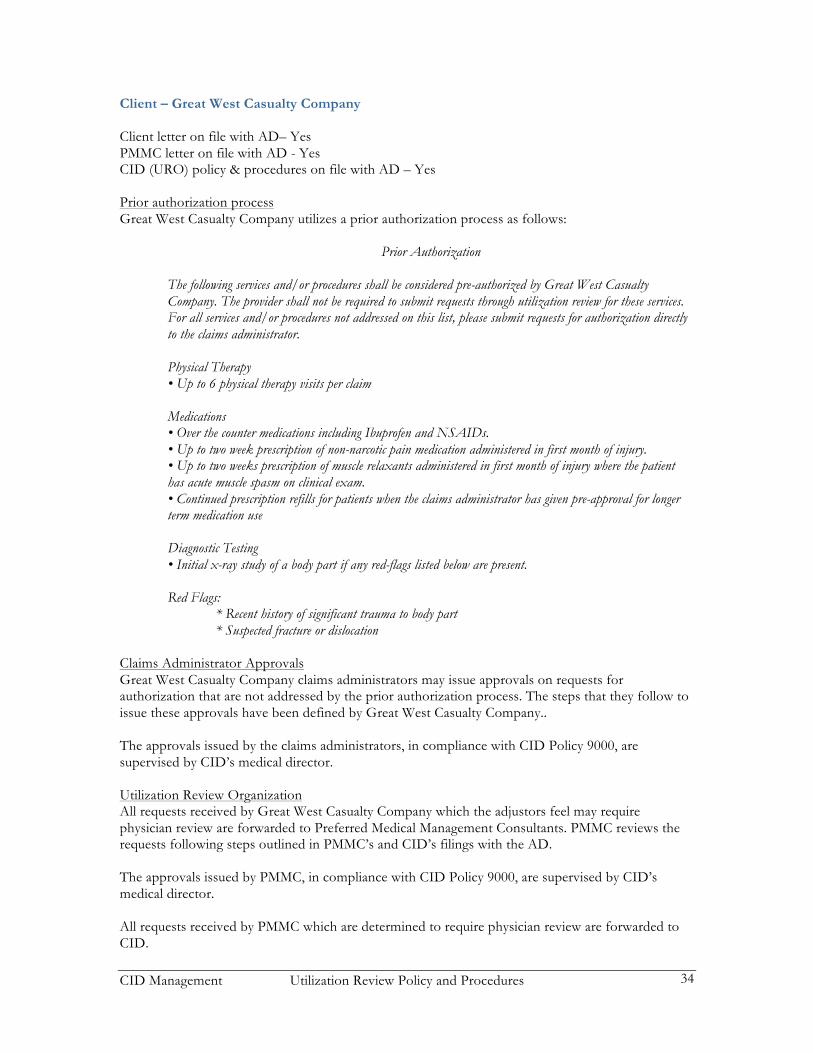
Client – Great West Casualty Company Client letter on file with AD– Yes PMMC letter on file with AD - Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process Great West Casualty Company utilizes a prior authorization process as follows:
Prior Authorization The following services and/or procedures shall be considered pre-authorized by Great West Casualty Company. The provider shall not be required to submit requests through utilization review for these services. For all services and/or procedures not addressed on this list, please submit requests for authorization directly to the claims administrator. Physical Therapy • Up to 6 physical therapy visits per claim Medications • Over the counter medications including Ibuprofen and NSAIDs. • Up to two week prescription of non-narcotic pain medication administered in first month of injury. • Up to two weeks prescription of muscle relaxants administered in first month of injury where the patient has acute muscle spasm on clinical exam. • Continued prescription refills for patients when the claims administrator has given pre-approval for longer term medication use Diagnostic Testing • Initial x-ray study of a body part if any red-flags listed below are present. Red Flags:
* Recent history of significant trauma to body part * Suspected fracture or dislocation
Claims Administrator Approvals Great West Casualty Company claims administrators may issue approvals on requests for authorization that are not addressed by the prior authorization process. The steps that they follow to issue these approvals have been defined by Great West Casualty Company.. The approvals issued by the claims administrators, in compliance with CID Policy 9000, are supervised by CID’s medical director. Utilization Review Organization All requests received by Great West Casualty Company which the adjustors feel may require physician review are forwarded to Preferred Medical Management Consultants. PMMC reviews the requests following steps outlined in PMMC’s and CID’s filings with the AD. The approvals issued by PMMC, in compliance with CID Policy 9000, are supervised by CID’s medical director. All requests received by PMMC which are determined to require physician review are forwarded to CID.
CID Management Utilization Review Policy and Procedures 35
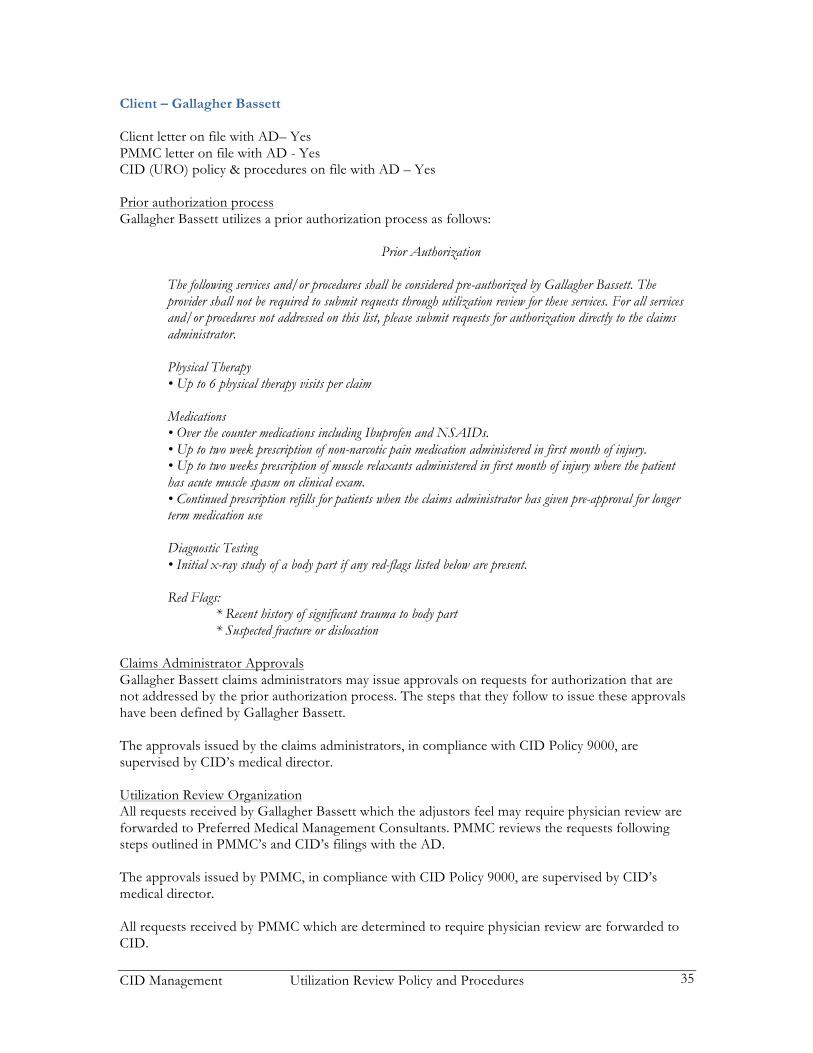
Client – Gallagher Bassett Client letter on file with AD– Yes PMMC letter on file with AD - Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process Gallagher Bassett utilizes a prior authorization process as follows:
Prior Authorization The following services and/or procedures shall be considered pre-authorized by Gallagher Bassett. The provider shall not be required to submit requests through utilization review for these services. For all services and/or procedures not addressed on this list, please submit requests for authorization directly to the claims administrator. Physical Therapy • Up to 6 physical therapy visits per claim Medications • Over the counter medications including Ibuprofen and NSAIDs. • Up to two week prescription of non-narcotic pain medication administered in first month of injury. • Up to two weeks prescription of muscle relaxants administered in first month of injury where the patient has acute muscle spasm on clinical exam. • Continued prescription refills for patients when the claims administrator has given pre-approval for longer term medication use Diagnostic Testing • Initial x-ray study of a body part if any red-flags listed below are present. Red Flags:
* Recent history of significant trauma to body part * Suspected fracture or dislocation
Claims Administrator Approvals Gallagher Bassett claims administrators may issue approvals on requests for authorization that are not addressed by the prior authorization process. The steps that they follow to issue these approvals have been defined by Gallagher Bassett. The approvals issued by the claims administrators, in compliance with CID Policy 9000, are supervised by CID’s medical director. Utilization Review Organization All requests received by Gallagher Bassett which the adjustors feel may require physician review are forwarded to Preferred Medical Management Consultants. PMMC reviews the requests following steps outlined in PMMC’s and CID’s filings with the AD. The approvals issued by PMMC, in compliance with CID Policy 9000, are supervised by CID’s medical director. All requests received by PMMC which are determined to require physician review are forwarded to CID.

CID Management Utilization Review Policy and Procedures 36
Client – Los Angeles Municipal Transportation Authority Client letter on file with AD– Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process Los Angeles Municipal Transportation Authority does not utilize a prior authorization process. Claims Administrator Approvals Los Angeles Municipal Transportation claims administrators may issue approvals on requests for authorization that are not addressed by a prior authorization process. The steps that they follow to issue these approvals have been defined by Los Angeles Municipal Transportation. Any approvals issued by the claims administrators, in compliance with CID Policy 9000, are supervised by CID’s medical director. Utilization Review Organization All requests received by Los Angeles Municipal Transportation which they determine to require physician review are forwarded to CID.
CID Management Utilization Review Policy and Procedures 37
Client – Mainstay Business Solutions / Blue Lake Insurance Services Client letter on file with AD– Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process Mainstay Business Solutions / Blue Lake does not utilize a prior authorization process. Claims Administrator Approvals The claims administrators on the Mainstay Business Solutions / Blue Lake claims send all requests for authorization through Intercare’s utilization review process. A nurse case manager and a nurse assistant, working under the direction of Intermed’s Medical Director, review the requests and approve them if consistent with guidelines. Utilization Review Organization All requests received by Mainstay Business Solutions / Blue Lake which they determine to require physician review are forwarded to CID.

CID Management Utilization Review Policy and Procedures 38
Client – State Farm Insurance Client letter on file with AD– Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process State Farm does not utilize a prior authorization process. Claims Administrator Approvals State Farm claims administrators may issue approvals on requests for authorization. The steps that they follow to issue these approvals are outlined in CID’s filing with the Administrative Director’s office and can be found in CID Policy 9000. The approvals issued by the claims administrators, in compliance with CID Policy 9000, are supervised by CID’s medical director. Utilization Review Organization All requests received by State Farm which require physician review are forwarded to CID.
CID Management Utilization Review Policy and Procedures 39
Client – State Fund Client letter on file with AD– Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process State Fund uses a prior authorization process as follows: “State Fund provides some MPN physicians the authority to perform routine medical procedures without utilization review. Passport participants shall provide treatment consistent with the MTUS found in Title 8 CCR §9792.20 – 9792.22. All Physicians participating in the UR Passport Program are part of the following industrial medical groups: Kaiser Permanente, US Heath Works and Concentra. The program may be expanded to include additional physicians at a later date. Eligible doctors may proceed with the majority of treatments without need for utilization review.
Prior Authorization With the exceptions noted below, treatment provided by physicians eligible for the State Fund UR Passport Program, and that is consistent with the MTUS found in Title 8 CCR §9792.20 – 9792.22 shall be considered pre-authorized. The following services and/or procedures shall not be considered pre-authorized. The provider shall be required to submit requests through utilization review for these services. For all services and/or procedure on this list, please submit requests for authorization directly to the claims administrator.
• All spinal surgeries • Spine Procedures (IDET, discogram, facet injections) • Spinal cord stimulators and implantable pain pumps • Epidural injections (more than 3 pre year to a region) • Open (non-scope) surgeries to knees/shoulders (No UR is required for arthroscopies, foreign body removal,
and “incision and drainage”) • Long term opiate use (more than 90 days) • High dose opiates (more than 120mg of morphine equivalent per day or more than 40 mg methadone per
day) • Home health care and attendant care • Compound medications and medical foods • In-patient pain management program • Weight loss clinics (other than Weight Watchers and in-house weight loss programs) food products not
covered • The following DME: dynamic splinting, lymphedema, H-wave, Interferential units, power mobility
devices/beds/spas [unless rental] No provider notification letters will be sent by the State Fund claims administrators or designated Utilization Review Organization for the procedures or services that fall under this Program.” Claims Administrator Approvals The State Fund in-house staff may issue approvals on requests for authorization. The approvals issued by the State Fund staff are supervised by State Fund’s medical director. Utilization Review Organization

CID Management Utilization Review Policy and Procedures 40
Requests received by State Fund which they determine to require physician review are forwarded to CID, or to another URO contracted with State Fund.

CID Management Utilization Review Policy and Procedures 41
Client - Teichert Client letter on file with AD– Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process Teichert does not utilize a prior authorization process. Claims Administrator Approvals Teichert has not made known to CID the processes they follow in issuing claims administrator approvals, nor the name of the medical director they are utilizing to supervise the approvals*. Please contact Teichert if this information is required. * The administrative approvals issued by the Teichert staff are not supervised by the CID medical director. Consequently, we are not a party to any administrative approvals issued. Utilization Review Organization All requests received by Teichert which they determine to require physician review are forwarded to CID.

CID Management Utilization Review Policy and Procedures 42
Client – The Reny Company Client letter on file with AD– Yes PMMC letter on file with AD - Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process The Reny Company does not utilize a prior authorization process. Claims Administrator Approvals The Reny Company performs bill review and other cost containment services on behalf of their contracted clients. One component of these cost containment solutions is the performance of utilization review. The Reny Company staff do not issue approvals on requests for authorization received from providers, but rather forward all requests to PMMC for review. Utilization Review Organization All requests received by The Reny Company are forwarded to Preferred Medical Management Consultants. PMMC reviews the requests following steps outlined in PMMC’s and CID’s filings with the AD. The approvals issued by PMMC, in compliance with CID Policy 9000, are supervised by CID’s medical director. All requests received by PMMC which are determined to require physician review are forwarded to CID.

CID Management Utilization Review Policy and Procedures 43
Client – Ensign Facility Services, including: Summerfield Healthcare Center Rose Villa Care Center Park View Gardens Brookfield Healthcare Center Sonoma Healthcare Center Victoria Healthcare Center Cloverdale Healthcare Center Palomar Healthcare Center Northbrook Healthcare Center Brookside Healthcare Center Ukiah Convalescent Hospital Sea Cliff Healthcare Center Southland (SNF) and Southland Living (ALF) Claremont Care Center Royal Crt Healthcare Center (Berryman) Arroyo Vista Nursing Center Whittier Hills Healthcare Center Vista Knoll Spec Care Facility Panorama Gardens (Beverly Manor) SNF Glenwood Care Center Arbor Glen Care Center Victoria Care Center Premier Care and Rehabilitation Center Palm Terrace Healthcare Center Atlantic Memorial Healthcare Center Upland Rehabilitation Center Shoreline Healthcare Center Lemon Grove Care and Rehabilitation Center Client letter on file with AD– Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process Ensign Facility Services does not utilize a prior authorization process. Claims Administrator Approvals Ensign Facility Services’ claims administrators may issue approvals on requests for authorization that are not addressed by the prior authorization process. They may choose to process these approvals as outlined in CID’s Policy 9000 on file with the Administrative Director’s office. The approvals issued by the claims administrators, in compliance with CID Policy 9000, are supervised by CID’s medical director. Utilization Review Organization All requests received by Ensign Facility Services which they determine to require physician review are forwarded to CID or another peer review vendor.

CID Management Utilization Review Policy and Procedures 44
Client – City of Simi Valley Client letter on file with AD– Yes PMMC letter on file with AD - Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process The City of Simi Valley utilizes a prior authorization process as follows:
Prior Authorization The following services and/or procedures shall be considered pre-authorized by the City of Simi Valley. The provider shall not be required to submit requests through utilization review for these services. For all services and/or procedures not addressed on this list, please submit requests for authorization directly to the claims administrator. Physical Therapy/Occupational Therapy • Up to 6 physical/occupational therapy visits per claim Post Operative Physical Therapy/Occupational Therapy • Up to 12 physical/occupational therapy visits per claim Chiropractic Care • Up to 12 chiropractic sessions Medications • Over the counter medications including Ibuprofen and NSAIDs. • Up to two week prescription of non-narcotic pain medication administered in first month of injury. • Up to two weeks prescription of muscle relaxants administered in first month of injury • Continued prescription refills up to 90 days for patients when the claims administrator has given pre-approval for longer term medication use Diagnostic Testing (Diagnostic tests must be performed by a City of Simi Valley designated vendor) • Initial x-ray study of a body part if any red-flags exist
Specialist Appointments • Orthopedic Consultations shall be approved as long as it is to examine an injury or illness accepted in the Workers’ Compensation claim Durable Medical Equipment (DME supplies must be provide by the City of Simi Valley’s designated vendors) • Post surgical DME Corticosteroid injections (in non-diabetic patients): • Elbow: single injection in cases of severe pain from epicondylitis • Knee: three injections or less if the patient has osteoarthritis • Shoulder: three injections or less if the patient has rotator cuff disease
CID Management Utilization Review Policy and Procedures 45
Claims Administrator Approvals The City of Simi Valley claims administrators may issue approvals on requests for authorization that are not addressed by the prior authorization process. The steps that they follow to issue these approvals are outlined in CID’s filing with the Administrative Director’s office and can be found in CID Policy 9000. The approvals issued by the claims administrators, in compliance with CID Policy 9000, are supervised by CID’s medical director. Utilization Review Organization All requests received by the City of Simi Valley which the adjustors feel may require physician review are forwarded to reviewer level. For those reviews forwarded to Preferred Medical Management Consultants and CID, the requests will be processes following steps outlined in PMMC’s and CID’s filings with the AD. The approvals issued by PMMC, in compliance with CID Policy 9000, are supervised by CID’s medical director. All requests received by PMMC which are determined to require physician review are forwarded to CID.

CID Management Utilization Review Policy and Procedures 46
Client – Uninsured Employers’ Benefits Trust Fund (UEBTF) Client letter on file with AD– Yes CID (URO) policy & procedures on file with AD – Yes Prior authorization process The City of UEBTF does not utilize a prior authorization process. Claims Administrator Approvals The UEBTF has not made known to CID the processes they follow in issuing claims administrator approvals, nor the name of the medical director they are utilizing to supervise the approvals*. Please contact the UEBTF if this information is required. * The administrative approvals issued by the UEBTF staff are not supervised by the CID medical director. Consequently, we are not a party to any administrative approvals issued. Utilization Review Organization All requests received by the UEBTF which they determine to require physician review are forwarded to CID.

CID Management Utilization Review Policy and Procedures 47
Reference List for Specific Policies Addressing CA Labor Code and Regulations. LC 4604.5. (a) CID Policy 1100
(b) CID Policy 1100 (c) CID Policy 1100 (d) Administrative. No CID policy required.
(1) Administrative. No CID policy required (2) Administrative. No CID policy required
(e) CID Policy 1100 LC 4610. (a) Administrative. No CID policy required
(b) Administrative. No CID policy required (c) CID’s utilization review process is governed by the attached policies and procedures. This letter is on file the Administrative Director and shall be disclosed, if requested by the employer to employees, physicians and the public upon request. CID Policy 1100 addresses the clinical review criteria. (d) CID Policy 3700 addresses requests for information. The Medical Director, and his role in the utilization management process is addressed in this letter. (e) CID Policy 3300. (f) CID Policy 1100.
(1) CID Policy 1100. (2) CID Policy 1100. (3) CID Policy 1100. (4) CID Policy 3800. (5) CID Policy 3800.
(g) Administrative. No CID policy required. (1) CID Policy 3800; CID Policy 3900. (2) CID Policy 3800; CID Policy 3900. (3) Administrative. No CID policy required.
(A) CID Policy 3800. (B) CID Policy 3800.
(4) CID Policy 3800. (5) CID Policy 3700; CID Policy 3800; CID Policy 3900.
(h) CID Policy 5005; CID Policy 5020. (i) Administrative. No CID policy required.
8 CCR: § 9792.6. Administrative. No CID policy required. § 9792.7. (a) Administrative. No CID policy required.
(1) Addressed in this letter. (2) Addressed in this letter. CID Policies 1000 – 7000. (3) Addressed in this letter. CID Policy 1100 (4) Addressed in this letter. CID Policies 1000 – 7000. (5) Addressed in this letter. CID Policy 9000 as specified in this letter.
(b) Administrative. No CID policy required. (1) Addressed in this letter. CID Policy 4000.
(2) CID Policy 3300. (3) CID Policies 3100, 3200, 3700, 3900, 9000.
(c) Addressed in this letter.
CID Management Utilization Review Policy and Procedures 48
(d) Utilization review plan is posted on-line or is available upon request. (1) Utilization review plan is posted on-line or is available upon request.
§ 9792.8. (a) Administrative. No CID policy required.
(1) CID Policy 1100. (2) CID Policy 1100. (3) CID Policy 3800. (4) CID Policy 3300.
§ 9792.9. (a) CID Policies 3000, 3010.
(1) CID Policy 3900. (2) CID Policy 3900.
(b) Administrative. No CID policy required. (1) CID Policy 3900. (2) CID Policies 3700 and 3900. (A) CID Policy 3700. (3) CID Policy 3800. (4) CID Policy 3800. (5) Administrative. No CID policy required.
(c) CID Policy 3800. (d) Administrative. No CID policy required. (e) CID Policies 3000 and 3900.
(1) Administrative. No CID policy required. (2) CID Policy 3900.
(f) CID Policy 3300. (g) Administrative. No CID policy required.
(1) Administrative. No CID policy required. (A) CID Policy 3700.
(B) CID Policy 3700. (C) CID Policy 3700.
(2) CID Policy 3700. (3) CID Policies 3700, 3800, 3900. (4) CID Policies 3700, 3800, 3900.
(h) CID Policies 5000, 5005, 5010, 5020, 5030. (i) CID Policy 3800. (j) CID Policy 3800.
(1) CID Policy 3800. (2) CID Policy 3800. (3) CID Policy 3800. (4) CID Policy 3800. (5) CID Policy 3800. (6) CID Policy 3800. (7) CID Policy 3800. (8) CID Policy 3800. (9) CID Policy 3800.
(k) CID Policy 3800. (l) CID Policy 3700.
§ 9792.10. Administrative. No CID policy required.
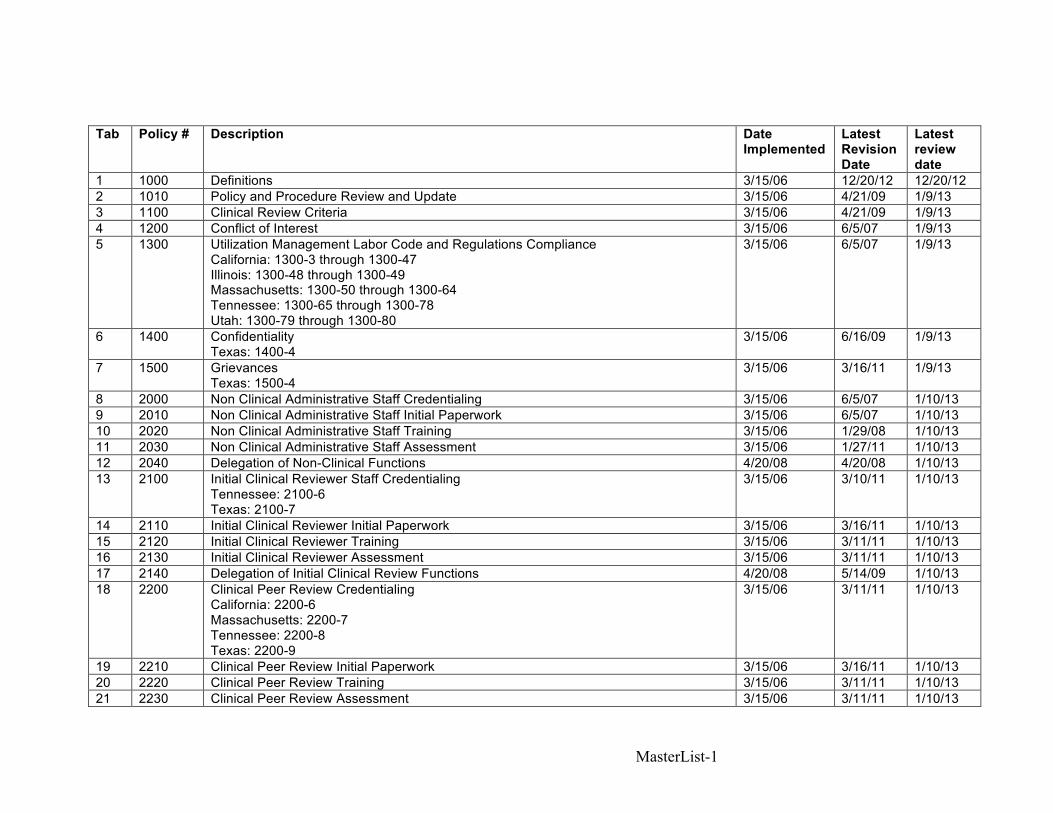
MasterList-1
Tab Policy # Description Date Implemented
Latest Revision Date
Latest review date
1 1000 Definitions 3/15/06 12/20/12 12/20/12 2 1010 Policy and Procedure Review and Update 3/15/06 4/21/09 1/9/13 3 1100 Clinical Review Criteria 3/15/06 4/21/09 1/9/13 4 1200 Conflict of Interest 3/15/06 6/5/07 1/9/13 5 1300 Utilization Management Labor Code and Regulations Compliance
California: 1300-3 through 1300-47 Illinois: 1300-48 through 1300-49 Massachusetts: 1300-50 through 1300-64 Tennessee: 1300-65 through 1300-78 Utah: 1300-79 through 1300-80
3/15/06 6/5/07 1/9/13
6 1400 Confidentiality Texas: 1400-4
3/15/06 6/16/09 1/9/13
7 1500 Grievances Texas: 1500-4
3/15/06 3/16/11 1/9/13
8 2000 Non Clinical Administrative Staff Credentialing 3/15/06 6/5/07 1/10/13 9 2010 Non Clinical Administrative Staff Initial Paperwork 3/15/06 6/5/07 1/10/13 10 2020 Non Clinical Administrative Staff Training 3/15/06 1/29/08 1/10/13 11 2030 Non Clinical Administrative Staff Assessment 3/15/06 1/27/11 1/10/13 12 2040 Delegation of Non-Clinical Functions 4/20/08 4/20/08 1/10/13 13 2100 Initial Clinical Reviewer Staff Credentialing
Tennessee: 2100-6 Texas: 2100-7
3/15/06 3/10/11 1/10/13
14 2110 Initial Clinical Reviewer Initial Paperwork 3/15/06 3/16/11 1/10/13 15 2120 Initial Clinical Reviewer Training 3/15/06 3/11/11 1/10/13 16 2130 Initial Clinical Reviewer Assessment 3/15/06 3/11/11 1/10/13 17 2140 Delegation of Initial Clinical Review Functions 4/20/08 5/14/09 1/10/13 18 2200 Clinical Peer Review Credentialing
California: 2200-6 Massachusetts: 2200-7 Tennessee: 2200-8 Texas: 2200-9
3/15/06 3/11/11 1/10/13
19 2210 Clinical Peer Review Initial Paperwork 3/15/06 3/16/11 1/10/13 20 2220 Clinical Peer Review Training 3/15/06 3/11/11 1/10/13 21 2230 Clinical Peer Review Assessment 3/15/06 3/11/11 1/10/13

MasterList-2
22 2240 Delegation of Clinical Peer Review Functions Massachusetts: 2240-5 Tennessee: 2240-6 Texas: 2240-7
4/20/08 5/14/09 1/10/13
23 2300 QAQC Review Staff Credentialing 3/15/06 3/11/11 1/10/13 24 2310 QAQC Reviewer Initial Paperwork 3/15/06 3/16/11 1/10/13 25 2320 QAQC Reviewer Training 3/15/06 1/29/08 1/10/13 26 2330 QAQC Reviewer Assessment 3/15/06 3/11/11 1/10/13 27 2340 Delegation of QAQC Review Functions 4/20/08 4/20/08 1/10/13 28 3000 Receipt of Request for Utilization Management Services
California: 3000-4 Massachusetts: 3000-5
3/15/06 3/11/11 1/9/13
29 3005 Telephonic Inquiry Regarding Utilization Management Services 3/15/06 6/5/07 1/17/13 30 3010 Utilization Management Electronic Review File 3/15/06 6/5/07 1/17/13 21 3100 Pre-Review Screening
California: 3100-6 3/15/06 4/11/11 1/9/13
32 3200 Initial Clinical Review California: 3200-4 Massachusetts: 3200-5 Tennessee: 3200-6 Texas: 3200-7
3/15/06 7/14/09 01/17/13
33 3300 Clinical Peer Review California: 3300-4 to 3400-5 Massachusetts: 3300-6 Tennessee: 3300-7 Texas: 3300-8
3/15/06 6/17/09 1/9/13
34 3400 Appeals Consideration California: 3400-5 through 3400-6 Massachusetts: 3400-7 Tennessee: 3400-8 Texas: 3400-9 through 3400-12 Utah: 3400-13
3/15/06 6/8/2010 1/10/13
35 3450 Reconsiderations of Determinations at the Request of Claims Administrators 5/13/09 5/13/09 1/10/13 36 3500 Re Considerations
Tennessee: 3500-5 3/15/06 1/29/08 1/17/13
37 3600 Telephonic Peer to Peer Consultations 3/15/06 6/5/07 1/17/13 38 3700 Notifications of Extension of Review Due Date 3/15/06 4/25/12 1/17/13 39 3750 Reimbursement for Duplication of Records 3/15/06 6/5/07 1/17/13 40 3800 Utilization Management Correspondence 3/15/06 3/12/09 1/10/13
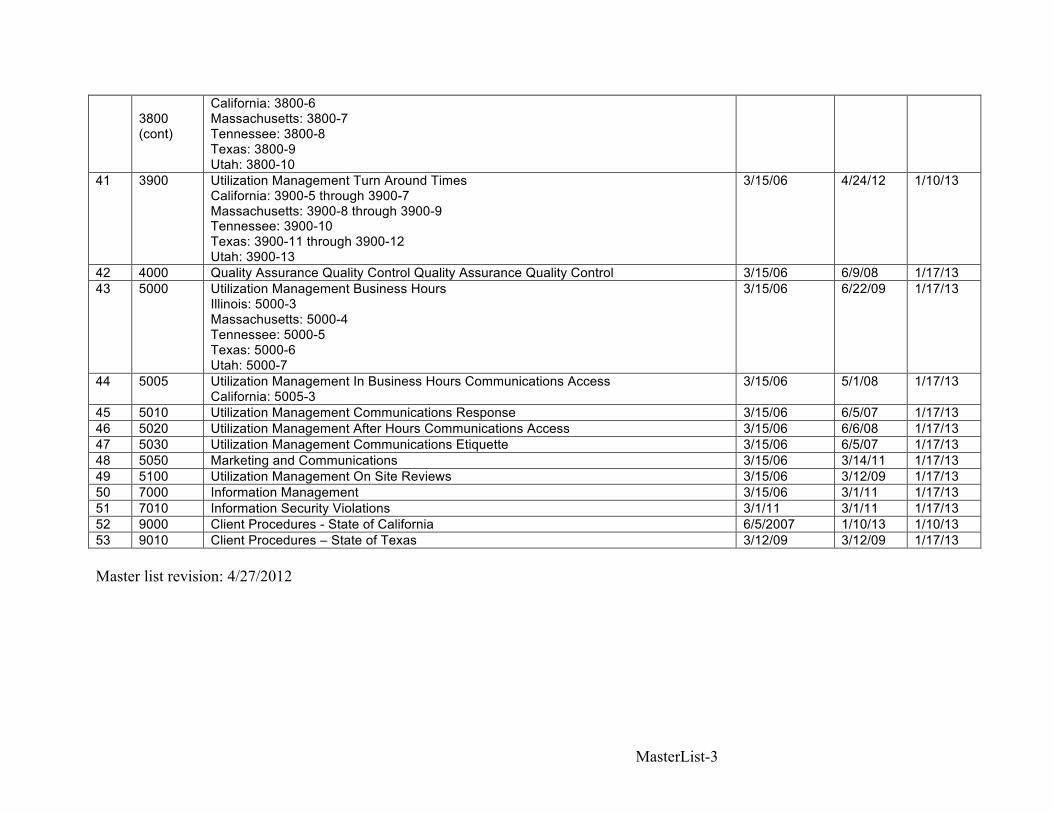
MasterList-3
3800 (cont)
California: 3800-6 Massachusetts: 3800-7 Tennessee: 3800-8 Texas: 3800-9 Utah: 3800-10
41 3900 Utilization Management Turn Around Times California: 3900-5 through 3900-7 Massachusetts: 3900-8 through 3900-9 Tennessee: 3900-10 Texas: 3900-11 through 3900-12 Utah: 3900-13
3/15/06 4/24/12 1/10/13
42 4000 Quality Assurance Quality Control Quality Assurance Quality Control 3/15/06 6/9/08 1/17/13 43 5000 Utilization Management Business Hours
Illinois: 5000-3 Massachusetts: 5000-4 Tennessee: 5000-5 Texas: 5000-6 Utah: 5000-7
3/15/06 6/22/09 1/17/13
44 5005 Utilization Management In Business Hours Communications Access California: 5005-3
3/15/06 5/1/08 1/17/13
45 5010 Utilization Management Communications Response 3/15/06 6/5/07 1/17/13 46 5020 Utilization Management After Hours Communications Access 3/15/06 6/6/08 1/17/13 47 5030 Utilization Management Communications Etiquette 3/15/06 6/5/07 1/17/13 48 5050 Marketing and Communications 3/15/06 3/14/11 1/17/13 49 5100 Utilization Management On Site Reviews 3/15/06 3/12/09 1/17/13 50 7000 Information Management 3/15/06 3/1/11 1/17/13 51 7010 Information Security Violations 3/1/11 3/1/11 1/17/13 52 9000 Client Procedures - State of California 6/5/2007 1/10/13 1/10/13 53 9010 Client Procedures – State of Texas 3/12/09 3/12/09 1/17/13 Master list revision: 4/27/2012

1000-1
CID Management
Definitions
Policy No. 1000 Revision: 4.4 Revision Date:12/20/2012 Page 1 of 9
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes the definitions for general terminology used with utilization review at CID. This policy shall serve as the official reference for terms used within CID policies, documents, and communications.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 4.0 01/29/2008 Revised Revision 4.1 05/01/2008 Revised Revision 4.2 03/12/2009 Revised Revision 4.3 06/16/2009 Revised Revision 4.3 06/08/2010 Reviewed Revision 4.3 02/01/2011 Reviewed Revision 4.4 12/22/2011 Revised Revision 4.4 04/25/2012 Revised Revision 4.4 12/20/2012 Revised
3.0 Persons Affected This policy affects all employees and independent contractors who participate in performing utilization review at CID.
4.0 Policy The policy of CID Management is to require the use of appropriate terminology, on the part of the staff and independent contractors, during the performance of duties and responsibilities at CID. It is further the policy of CID management to ensure that the use of the following terms in any official CID documentation reflects the definitions of those terms as outlined in this policy. This policy is not intended to represent the vocabulary or terms of art of any specific state or jurisdiction.

1000-2
5.0 Definitions
5.1 ACOEM Practice Guidelines: American College of Occupational and Environmental Medicine’s Occupational Medicine Practice Guidelines, Second Edition.
5.2 Adverse Determination: The denial or modification of coverage for a treatment plan,
including diagnosis or therapy. Texas: a determination, made through utilization review or retrospective review, that the health care services furnished or proposed to be furnished to an employee are not medically necessary or appropriate.
5.3 Appeal: Formal request for review or reconsideration of a CID determination 5.4 Appeals Consideration: Clinical review completed by appropriate clinical peer
reviewers who were not involved in the original peer clinical review in which a decision not to certify a requested admission, procedure, or service has been appealed.
5.5 Approval: See certification
California: “Approval” means a decision that the requested treatment or service is medically appropriate to cure or relieve.
5.6 Attending Physician: The physician with primary responsibility for the care provided
to a patient in a hospital or other health care facility 5.7 Authorization: See certification.
California: “Authorization” means assurance that appropriate reimbursement will be made for an approved specific course of proposed medical treatment to cure or relieve the effects of the industrial injury pursuant to section 4600 of the Labor Code, subject to the provisions of section 5402 of the Labor Code, based on a completed “Request for Authorization for Medical Treatment,” DWC Form RFA, as contained in California Code of Regulations, title 8, section 9785.5, that has been transmitted by the treating physician to the claims administrator. Authorization shall be given pursuant to the timeframe, procedure, and notice requirements of California Code of Regulations, title 8, section 9792.9.1, and may be provided by utilizing the indicated response section of the “Request for Authorization for Medical Treatment,” DWC Form RFA.
5.8 Board Certified: A certification approved by the American Board of Medical
Specialties, the American Osteopathic Association, or other organization as accepted by URAC, that a physician has expertise in a particular specialty or field.
5.9 Case Involving Urgent Care: Any request for a utilization management determination
with respect to which the application of the time periods for making non-urgent care determinations a) could seriously jeopardize the life or health of the consumer or the ability of the consumer to regain maximum function, or b) in the opinion of a
1000-3
physician with knowledge of the consumer’s medical condition, would subject the consumer to severe pain that cannot be adequately managed without the care or treatment that is the subject of the case.
5.10 Case Management: A collaborative process which assesses, plans, implements,
coordinates, monitors, and evaluates options and services to meet an individual’s health needs using communication and available resources to promote quality cost-effective outcomes.
5.11 Certification: A determination by an organization that an admission, extension of
stay, or other health care service has been reviewed and, based on the information provided, meets the clinical requirements for medical necessity, appropriateness, level of care, or effectiveness under the auspices of the applicable health benefit plan.
5.12 Channeling: Directing care into a Preferred Provider Organization (PPO) or
specialty network.
5.13 CID: Comprehensive Industrial Disability, Inc.
5.14 Claims Administrator: A self-administered workers' compensation insurer, a self-administered self-insured employer, a self-administered legally uninsured employer, a self-administered joint powers authority, or a third-party claims administrator for an insurer, a self-insured employer, a legally uninsured employer or a joint powers authority. The claims administrator may utilize an agent to fulfill its utilization review responsibilities. California: "Claims Administrator" is a self-administered workers' compensation insurer of an insured employer, a self-administered self-insured employer, a self-administered legally uninsured employer, a self-administered joint powers authority, a third-party claims administrator or other entity subject to Labor Code section 4610, the California Insurance Guarantee Association, and the director of the Department of Industrial Relations as administrator for the Uninsured Employers Benefits Trust Fund (UEBTF). “Claims Administrator” includes any utilization review organization under contract to provide or conduct the claims administrator’s utilization review responsibilities. Unless otherwise indicated by context, “claims administrator” also means the employer.
5.15 Client: A business or individual that purchases services from CID
5.16 Clinical Decision Support Tools: Protocols, guidelines, or algorithms that assist in
the clinical decision-making process.
5.17 Clinical Director: A health professional who: (1) is duly licensed or certified; (2) is an employee of, or party to a contract with, an organization; and (3) who is responsible for clinical oversight of the utilization management program, including the credentialing of professional staff and quality assessment and improvement functions.

1000-4
5.18 Clinical Peer: A physician or other health professional who holds an unrestricted
license and is in the same or similar specialty as typically manages the medical condition, procedures, or treatment under review. Generally, as a peer in a similar specialty, the individual must be in the same profession, i.e., the same licensure category as the ordering provider.
5.19 Clinical Rationale: A statement that provides additional clarification of the
clinical basis for a determination. The clinical rationale should relate the determination to the patient’s condition or treatment plan, and should supply a sufficient basis for a decision to pursue an appeal if appropriate.
5.20 Clinical Review Criteria: The written screens, decision rules, medical protocols,
or guidelines used by the organization as an element in the evaluation of medical necessity and appropriateness of requested admissions, procedures, and services under the auspices of the applicable health benefit plan.
5.21 Complainant:
Texas: A person who files a complaint, as defined below. This could be an employee; an employer; a health care provider; or another person designated to act on behalf of an employee.
5.22 Complaint:
Texas: any dissatisfaction expressed orally or in writing by a complainant to a network regarding any aspect of the network's operation. The term includes dissatisfaction relating to medical fee disputes and the network's administration and the manner in which a service is provided. The term does not include a misunderstanding or a problem of misinformation that is resolved promptly by clearing up the misunderstanding or supplying the appropriate information to the satisfaction of the complainant; or an oral or written expression of dissatisfaction or disagreement with an adverse determination.
5.23 Concurrent Review: The meaning of this term is subject to jurisdictional variance.
California: "Concurrent review" means utilization review conducted during an inpatient stay. Massachusetts: A continuation of previously provided services, without a change in provider or diagnosis. Texas: During the course of treatment, including inpatient hospital stay; a review of on-going health care to determine if an extension of previously preauthorized health care is medically necessary.
5.24 Conditional non-certification: Administrative denial arising from lack of response
to a written request for information; and following a determination by a clinical peer reviewer that the requested information was necessary to arrive at a determination of medical necessity.
1000-5
5.25 Course of treatment: The set of medical goods or services included in a single request for authorization. California: "Course of treatment" means the course of medical treatment set forth in the treatment plan contained on the "Doctor's First Report of Occupational Injury or Illness," Form DLSR 5021, or on the "Primary Treating Physician's Progress Report," DWC Form PR-2, as contained in section 9785.2 or in narrative form containing the same information required in the DWC Form PR-2.
5.26 Delay: An extension of due dates as permitted by review process and
jurisdictional requirements; usually after a request for information. California: “Delay” means a decision by a reviewer that no determination based on medical necessity may be made within the 14-day time limit for the reasons listed in 9792.9.1(f).
5.27 Denied; denial: See non-certification
California: “Denial” means a decision by a physician reviewer that the requested treatment or service is not medically necessary.
5.28 Emergency Health Care Services: Health care services for a medical condition
manifesting itself by acute symptoms of sufficient severity such that the absence of immediate medical attention could reasonably be expected to place the patient's health in serious jeopardy.
5.29 Expedited Appeal: An appeal of an adverse determination in a case involving
urgent care or emergency health care.
5.30 Expedited Review: Prospective or concurrent review of emergency health care services. California: "Expedited review" means utilization review conducted when the injured worker's condition is such that the injured worker faces an imminent and serious threat to his or her health, including, but not limited to, the potential loss of life, limb, or other major bodily function, or the normal timeframe for the decision-making process would be detrimental to the injured worker's life or health or could jeopardize the injured worker's permanent ability to regain maximum function.
5.31 Expert Reviewer:
California: A physician, competent to evaluate the specific clinical issues involved in the medical treatment services and where these services are within the scope of the physician’s practice, who has been consulted by the reviewing physician or utilization review medical director or utilization review clinical director to provide specialized review of medical information.
5.32 Facility Rendering Service: The institution or organization in or by which the
requested admission, procedure, or service is provided. Such facilities may include, but are not limited to: hospitals; outpatient surgical facilities; individual practitioner offices; rehabilitation centers; residential treatment centers; skilled nursing facilities;

1000-6
laboratories; imaging centers; and other organizational providers of direct services to patients
5.33 First Level Review: See initial clinical review
5.34 Health Care Provider:
California: A provider of medical services, as well as related services or goods, including but not limited to an individual provider or facility, a health care service plan, a health care organization, a member of a preferred provider organization or medical provider network as provided in Labor Code section 4616.
5.35 Health Professional: An individual who: (1) has undergone formal training in a
health care field; (2) holds an associate or higher degree in a health care field, or holds a state license or state certificate in a health care field; and (3) has professional experience in providing direct patient care.
5.36 Immediately:
California: "Immediately" means within 24 hours after learning the circumstances that would require an extension of the timeframe for decisions specified, in subdivision (c) and (f)(1) of section 9792.9.1
5.37 Injured worker: an employee reporting information to an employer regarding an
injury or illness occurring in relation to their employment
5.38 Initial Clinical Review: Clinical review conducted by appropriate licensed or certified health professionals. Initial clinical review staff may certify requests for admissions, procedures, and services that meet clinical review criteria, but must refer requests that do not meet clinical review criteria to peer clinical review for certification or non-certification.
5.39 License: A license or permit (or equivalent) to practice medicine or a health
profession that is 1) issued by any state or jurisdiction in the United States; and 2) required for the performance of job functions.
5.40 Life-threatening: A disease or condition from which the likelihood of death is
probable unless the course of the disease or condition is interrupted.
5.41 Medical Director: A doctor of medicine or doctor of osteopathic medicine who is duly licensed to practice medicine and who is an employee of, or party to a contract with, an organization, and who has responsibility for clinical oversight of the organization’s utilization management, credentialing, quality management, and other clinical functions. Note: Specific jurisdictions may have additional requirements for Medical Director. California: "Medical Director" is the physician and surgeon licensed by the Medical Board of California or the Osteopathic Board of California who holds an unrestricted
1000-7
license to practice medicine in the State of California. The Medical Director is responsible for all decisions made in the utilization review process.
5.42 Medical Services: Services provided by a licensed health care professional.
California: those goods and services provided pursuant to Article 2 (commencing with Labor Code section 4600) of Chapter 2 of Part 2 of Division 4 of the Labor Code.
5.43 Modified: A utilization management determination by which some services are
certified and others are non-certified. California: “Modification” means a decision by a physician reviewer that part of the requested treatment or service is not medically necessary.
5.44 Non-Certification: A determination by an organization that an admission,
extension of stay, or other health care service has been reviewed and, based on the information provided, does not meet the clinical requirements for medical necessity, appropriateness, level of care, or effectiveness under the auspices of the applicable health benefit plan.
5.45 Non-Clinical Administrative Staff: Staff who do not meet the definition of health
professional.
5.46 Normal Turn Around Time: See Standard Turn Around Time.
5.47 Ordering Provider: The physician or other provider who specifically prescribes the health care service being reviewed.
5.48 Peer Clinical Review: Clinical review conducted by appropriate health
professionals when a request for an admission, procedure, or service was not certified during initial clinical review.
5.49 Peer-to-Peer Conversation: A conversation conducted by telephone between a
requesting provider and a peer reviewer. May be conducted prior to completion of determination, or subsequent to the rendering of a determination. If conducted subsequent to the rendering of a determination, such conversation shall not be considered a component of an appeal or reconsideration procedure and may not result in alteration or reversal of the original determination.
5.50 Physician Reviewer: See Clinical Peer 5.51 Pre-authorization:
Texas: the process required to request approval from the insurance carrier or the network to provide a specific treatment or service before the treatment or service is provided.
5.52 Pre-Certification Review: See prospective review

1000-8
5.53 Pre-Review Screening: Automated or semi-automated screening of requests for
authorization that may include: (1) collection of structured clinical data (including diagnosis, diagnosis codes,
procedures, procedure codes); (2) asking scripted clinical questions; (3) accepting responses to scripted clinical questions; and (4) taking specific action (certification and assignment of length of stay explicitly
linked to each of the possible responses). It excludes: (1) applying clinical judgment or interpretation; (2) accepting unstructured clinical information; (3) deviating from script; (4) engaging in unscripted clinical dialogue; (5) asking clinical follow-up questions; and (6) issuing non-certifications.
5.54 Principal Reason(s): A clinical or non-clinical statement describing the general
reason(s) for the non-certification determination 5.55 Prior Authorization: See prospective review
California: Any prior authorization process, including but not limited to, where authorization is provided without the submission of the request for authorization. (8CCR9792.7(a)(5))
5.56 Prospective Review: Utilization management conducted prior to a patient’s
admission, stay, or other service or course of treatment (including outpatient procedures and services). California: "Prospective review" means any utilization review conducted, except for utilization review conducted during an inpatient stay, prior to the delivery of the requested medical services Massachusetts: Utilization management conducted prior to a patient’s admission, stay, or other service or course of treatment (including outpatient procedures and services), provided that the services under consideration have never previously been provided for the industrial injury. Texas: See Pre-authorization.
5.57 Provider: A licensed health care facility, program, agency, or health professional
that delivers health care services.
5.58 Quality improvement project: An organization-wide initiative to measure and improve the service and/or care provided by the organization.
5.59 Quality Management (QM) program: A systematic data-driven effort to measure
and improve consumer and client services and/or health care services.

1000-9
5.60 Re-considerations: Clinical review completed by appropriate clinical peer
reviewer who completed an original peer clinical review in which a decision was made not to certify a requested admission, procedure, or service due to a lack of information from the provider. Texas: See Appeals Consideration.
5.61 Request For Authorization: A written request for a specific course of proposed
medical treatment. California: "Request for authorization" means a written request for a specific course of proposed medical treatment. A request for authorization must be set forth on a “Request for Authorization for Medical Treatment (DWC Form RFA),” completed by a treating physician, as contained in California Code of Regulations, title 8, section 9785.5. “Completed,” for the purpose of this section and for purposes of investigations and penalties, means that information specific to the request has been provided by the requesting treating physician for all mandatory fields indicated on the DWC Form RFA. The form must be signed by the physician and may be mailed, faxed or e-mailed.
5.62 Requesting Physician: The physician who has submitted the request for
authorization.
5.63 Retrospective Review: Review conducted after services (including outpatient procedures and services) have been provided to the patient and for which services approval has not already been given. Retrospective review does not include subsequent review of services for which prospective or concurrent reviews for medical necessity and appropriateness were previously conducted. Texas: the process of reviewing the medical necessity and reasonableness of health care that has been provided to an injured employee.
5.64 Review of Service Request: Review of information submitted to the organization
for health care services that do not need medical necessity certification nor result in a non-certification decision.
5.65 Reviewer:
California: "Reviewer" means a medical doctor, doctor of osteopathy, psychologist, acupuncturist, optometrist, dentist, podiatrist, or chiropractic practitioner licensed by any state or the District of Columbia, competent to evaluate the specific clinical issues involved in medical treatment services, where these services are within the scope of the reviewer's practice.
5.66 Rush: A request by the client to complete the utilization management process and
reach a determination by midnight the following business day.
5.67 School: A grouping of practitioners as defined by their professional degree.
1000-10
5.68 Second Level Review: See peer clinical review
5.69 Second Opinion: Requirement of some health plans to obtain an opinion about the medical necessity and appropriateness of specified proposed services by a practitioner other than the one originally making the recommendation.
5.70 Staff: The Organization’s employees, including full-time employees, part-time
employees, and consultants.
5.71 Standard Appeal: An appeal of a non-certification that is not an expedited appeal. In most cases, standard appeals will not relate to cases involving urgent care. However, standard appeals may also include secondary appeals of expedited appeals.
5.72 Standard Turn Around Time: A request to complete the utilization management
process and reach a determination within 2 business days following the receipt of all necessary medical information.
5.73 Stat: A request by the client to complete the utilization management process and
reach a determination by midnight the same business day.
5.74 Structured Clinical Data: Clinical information that is precise and permits exact matching against explicit medical terms, diagnoses or procedure codes, or other explicit choices, without the need for interpretation.
5.75 Third Level Review: See appeals consideration
5.76 Utilization Management (UM): Evaluation of the medical necessity,
appropriateness, and efficiency of the use of health care services, procedures, and facilities under the provisions of the applicable health benefit plan.
5.77 Utilization Review Plan:
California: the written plan filed with the Administrative Director pursuant to Labor Code section 4610, setting forth the policies and procedures, and a description of the utilization process. Texas: the screening criteria and utilization review procedures of an insurance carrier, a workers' compensation health care network, or a utilization review agent.
5.78 Utilization Review Process:
California: "Utilization review process" means utilization management functions that prospectively, retrospectively, or concurrently review and approve, modify, delay, or deny, based in whole or in part on medical necessity to cure or relieve, treatment recommendations by physicians, as defined in Labor Code section 3209.3, prior to, retrospectively, or concurrent with the provision of medical treatment services pursuant to Labor Code section 4600. Utilization review does not include determinations of the work-relatedness of injury or disease, or bill review for the

1000-11
purpose of determining whether the medical services were accurately billed. The utilization review process begins when the completed DWC Form RFA is first received by the claims administrator, or in the case of prior authorization, when the treating physician satisfies the conditions described in the utilization review plan for prior authorization. [Texas] A system for prospective or concurrent review of the medical necessity and appropriateness of health care services being provided or proposed to be provided to an individual in the state of Texas. The term does not include a review in response to an elective request for clarification of coverage or prepayment guarantee.
5.79 Worker: An ill or injured individual who is eligible for workers’ compensation
benefits and who files for, or for whom a workers’ compensation claim has been filed.
5.80 Written Notification: Includes a facsimile as well as communications in paper
form. California: "Written" includes a communication transmitted by facsimile or in paper form. Electronic mail may be used by agreement of the parties.
6.0 Procedures
Not applicable.

CID Management
Policy and Procedure Review and Update
Policy No. 1010 Revision: 3.1 Revision Date: 4/21/2009 Page 1 of 2
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which the CID Policies and Procedures manual is reviewed and revised no less than annually.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.1 04/21/2009 Revised Revision 3.1 06/08/2010 Reviewed Revision 3.1 01/26/2011 Reviewed Revision 3.1 04/22/2012 Reviewed Revision 3.1 01/09/2013 Reviewed
3.0 Persons Affected
This policy affects the senior management and department heads at CID responsible with policy review, revision, and approval duties. Additionally, this policy affects all staff whose jobs are impacted by revisions to the Policies and Procedures.
4.0 Policy
4.1 The policy of CID Management is to ensure that the corporation’s policies and procedures are up-to-date and reflect best practices. As such, CID reviews all policies and procedures no less than annually and during impromptu meetings held as necessary when issues arise.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures

6.1 The Utilization Review Policies and Procedures Committee shall meet not less than
annually to review, and revise as necessary, the Policies and Procedures manual. A scheduled yearly meeting for this purpose is held in mid-April.
6.2 Impromptu meetings of the Utilization Review Policies and Procedures Committee
will be held as necessary when issues arise (e.g. changes in state laws, requests for change by clients, etc).
6.3 The Polices and Procedures manual will be reviewed by the Utilization Review
Policies and Procedures Committee. This committee is comprised of the Medical Director; all Medical Directors associated with state-specific programs; the Clinical Director; the Director of Clinical Operations; the Director of Production; and a clinical reviewer. The UR Policies and Procedures Committee is charged with the following:
6.3.1 Reviewing the existing CID utilization review policies and procedures for
adherence with state and federal law. 6.3.2 Reviewing the existing CID utilization review policies and procedures for
best practice performance. 6.3.3 Reviewing the existing CID corporation-wide policies and procedures for
best practice performance, incorporating QI project recommendations when available.
6.3.4 To purpose, discuss, adopt, and implement changes to any and all existing
CID utilization review policies and procedures as necessary.
6.4 All health care providers on the UR Policies and Procedures Committee are expected to provide substantive input. All content of the Policies and Procedures must be approved by the Medical Director. All Policies and Procedures that are components of a state-specific utilization review plan must also be approved by any state-specific Medical Director.
6.5 Changes, additions, and deletions, as well as newly drafted policies and procedures
are posted to the CID intranet as well as announced via email memo to all affected personnel.

1100-1
CID Management
Clinical Review Criteria
Policy No. 1100 Revision: 4.2 Revision Date: 4/21/2009 Page 1 of 21
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which the Clinical Review Criteria Committee shall select the clinical review criteria that shall be used in the performance of utilization management at CID.
This policy establishes guidelines by which the clinical review criteria shall be communicated to the health professionals, including initial clinical reviewers, expert reviewers, and clinical peers, who perform functions within the scope of utilization management in the employment of, on contracting with, CID. This policy establishes guidelines by which the QAQC Committee shall monitor the application of the clinical review criteria in the performance of utilization management operations.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy and Addenda/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 4.0 01/29/2008 Revised Revision 4.1 04/21/2009 Revised Revision 4.2 06/08/2010 Reviewed Revision 4.2 02/01/2011 Reviewed Revision 4.2 12/22/2011 Reviewed Revision 4.2 04/22/2012 Reviewed Revision 4.2 01/09/2013 Reviewed
3.0 Persons Affected This policy affects all health professionals, including initial clinical reviewers, expert reviewers, and clinical peers, performing functions within the scope of utilization management in the employment of, or contracting with, CID.

1100-2
4.0 Policy The policy of CID Management is to ensure that the clinical review criteria used within utilization management operations at CID be evidence-based and reflect best-practice care. The clinical review criteria shall be evaluated no less than once per year by the Clinical Review Criteria Committee and shall be modified, updated or replaced as deemed necessary and appropriate by said committee. The application of the clinical review criteria by the health professionals, including initial clinical reviewers, expert reviewers, and clinical peers, performing functions within the scope of utilization management in the employment of, or contracting with, CID, shall be monitored by the QAQC Committee.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
6.1 Membership of the Clinical Review Criteria Committee shall include, at minimum, the Medical Director; the Medical Director of any state-specific utilization review program; the Clinical Director; the Clinical Operations Director; an initial clinical reviewer; a clinical peer reviewer; and a QAQC reviewer.
6.2 The Clinical Review Criteria Committee shall meet not less than annually to review
the clinical review criteria currently used in CID’s utilization management operations. 6.3 The Clinical Review Criteria Committee shall meet not less than annually to discuss
the addition, deletion, or modification of clinical review criteria used in CID’s utilization management operations.
6.4 The Clinical Review Criteria Committee shall ensure that the clinical review criteria
approved for use within CID’s utilization management operations meet the following standards:
6.4.1 The clinical review criteria are evidence based 6.4.2 The clinical review criteria were developed with input from providers
involved in full time medical practice. 6.4.3 The clinical review criteria are nationally recognized and are based on
scientific medical evidence.
6.5 The Clinical Review Criteria Committee shall charge the Clinical Director with communicating the selected clinical review criteria to all health professionals, including initial clinical reviewers, expert reviewers, and clinical peers, who perform functions within the scope of utilization management in the employment of, on contracting with, CID.

1100-3
6.6 The Clinical Review Criteria Committee shall charge the Clinical Director with
ensuring that all the health professionals, including initial clinical reviewers, expert reviewers, clinical peers, and quality assurance/quality control reviewers, who perform functions within the scope of utilization management in the employment of, on contracting with, CID, have access to the selected clinical review criteria.
6.7 The QAQC Committee shall monitor the utilization review determinations of all
health professionals, including initial clinical reviewers, expert reviewers, and clinical peers, who perform functions within the scope of utilization management in the employment of, on contracting with, CID, to ensure adherence to the clinical review criteria.
6.8 The QAQC Committee shall impose corrective action for all health professionals,
including initial clinical reviewers, expert reviewers, and clinical peers, who perform functions within the scope of utilization management in the employment of, on contracting with, CID, and who have not adhered to the clinical review criteria.
6.9 The CID clinical review criteria currently in place for utilization management
includes:
6.9.1 American College of Occupational and Environmental Medicine’s Occupational Medicine Practice Guidelines, 2nd ed published by OEM Press, Beverly Farms, MA. www.acoemguidelines.com .
6.9.2 The Official Disability Guidelines published by Work Loss Data Institute,
Encinitas, CA. www.odg-twc.com
6.9.3 The National Guidelines Clearinghouse, an initiative of the Agency of Health Care Research and Quality, U.S. Department of Health and Human Services. www.guidelines.gov This source is not a guideline per se, but a collection of guidelines that have been evaluated and summarized by the U.S. DHHS. When used as review criteria, reviewers will cite the original source guideline.
6.9.4 National Institute of Health’s PubMed scientific literature database.
www.ncbi.nlm.nih.gov/entrez/ This source is not a guideline per se, but a library of peer-reviewed health sciences publications. When used as review criteria, reviewers will cite the original source publication. Articles cited must be the most recent and/or best-quality research on the medical service under review; and must be a randomized clinical trial or better. This source should not be used by reviewers unless there are no other applicable review criteria available.

1100-4
6.9.5 The State of California 8 CCR 9792.21 Medical Treatment Utilization Schedule. http://www.dir.state.ca.us/dwc/DWCPropRegs/MedicalTreatmentUtilizationSchedule/MTUS_FinalRegulations.pdf
6.9.6 Department of Industrial Accidents Health Care Services Board Treatment
Guidelines, Commonwealth of Massachusetts. www.mass.gov/dia/hcsb/treatguides.htm
6.9.7 Colorado Department of Labor and Employment Medical Treatment
Guidelines. http://www.coworkforce.com/dwc/Medical_Treatment.asp
6.9.8 CID Internal Guideline #1: Medical Goods and Services for which No Acceptable Scientific Evidence Exists This criteria may only be used for authorization; and only with prior approval of CID senior clinical staff.
6.9.9 Delaware Health Care Services Guidelines
http://regulations.delaware.gov/AdminCode/title19/1000/1300/1340/
6.9.10 Minnesota Department of Labor and Industry http://www.doli.state.mn.us/WC/TpToc.asp
6.9.11 Washington State Department of Labor and Industries, Medical Treatment
Guidelines http://www.lni.wa.gov/ClaimsIns/Providers/Treatment/TreatGuide/
6.9.12 Wyoming Workers’ Safety and Compensation Division Treatment
Guidelines http://doe.wyo.gov/serviceproviders/Pages/default.aspx
1100-5
CID Management
Clinical Review Criteria Description – ACOEM Guidelines American College of Occupational and Environmental Medicine’s Occupational Medicine Practice Guidelines, published by OEM Press, Beverly Farms, MA. www.acoemguidelines.com . Description: ACOEM guidelines are a set of treatment guidelines applicable to acute musculoskeletal injuries; injuries of the eye; chronic pain; and stress related conditions. How were the criteria developed: According to ACEOM, as the American College of Occupational and Environmental Medicine (ACOEM) prepared to begin the process of review and revision of the first edition material, medical societies representing virtually all specialties involved in occupational medicine were invited to appoint one or more of their members to assist ACOEM in updating the guidelines. Consequently, the guidelines in this volume represent the current, collective voice of health care professionals across the spectrum of specialists who treat work-related injuries and occupational diseases. The individual representatives of the various specialty societies and the independent reviewers involved in the process of updating this edition are listed in the Acknowledgments. Who was involved in the development of the criteria: According to ACOEM, the following people were involved in the development of the criteria: Gunnar B. J. Andersson, MD, PhD Gerald M. Aronoff, MD, DABPM Robert J. Barth, PhD Roger M. Belcourt, MD, MPH, FACOEM Patrick J. Beecher, MD, MPH, MBA, FACOEM Jeremy J. Biggs, MD, MSPH Bernard R. Blais, MD, FACOEM, FAAO, FACS Daniel Bruns, PsyD Kevin Byrne, MD, MPH, FACOEM, FAAFP Eugene Carragee, MD Garson M. Caruso, MD, MPH, FACOEM, FAADEP, CIME Jennifer Christian, MD, MPH Jeffrey L. Cole, MD Penney Cowan David B. Coward, MD Rajiv Das, MD, MPH, MS Ronald Donelson, MD, MS Jed Downs, MD, MPH Mark Easley, MD Hannah Edwards, MD, MPH Marjorie Eskay-Auerbach, MD, JD Steven D. Feinberg, MD, MPH Corey D. Fox, PhD, ABPP M. Felix Freshwater, MD

1100-6
Jill Galper, PT, MEd Elizabeth Genovese, MD, MBA, FACOEM Lee S. Glass, MD, JD Michael Goertz, MD, MPH William W. Greaves, MD, MSPH, FACOEM, FACPM Nelson S. Haas, MD, MPH, MA, FACOEM (Panel Member) Scott Haldeman, MD, DC, PhD, FRCP(C), FAAN, FCCS Jeffrey S. Harris, MD, MPH, MBA, FACOEM Kurt T. Hegmann, MD, MPH, FACOEM, FACP Harold E. Hoffman, MD, FACOEM, FRCPC John P. Holland, MD, MPH Edward B. Holmes, MD, MPH Paul D. Hooper, DC, MPH, MS Stephen Miller Howell, MD Clark Iorio, DO Joshua J. Jacobs, MD Allison L. Jones, MD, MS Julia E. Klees, MD, MPH Wilhelmina C. Korevaar, MD, MMM James E. Lessenger, MD, FACOEM Gideon Letz, MD, MPH Ethan Lichtblau, MD David S. Logerstedt, PT, MPT, MA, SCS Steven Mandel, MD, FACOEM RobRoy Martin, PhD Tom Mayer, MD Joseph C. McCarthy, MD Brian J. McGrory, MD, MS Judith Green McKenzie, MD, MPH, FACOEM J. Mark Melhorn, MD, FACOEM, FAAOS, FAADEP, FACS, FASSH, FAAHS Lori A. Michener, PhD, PT, ATC Debra Milek, MD, MPH Kathryn L. Mueller, MD, MPH, FACOEM Donald R. Murphy, DC, DACAN Frederic G. Nicola, MD, MS Albert J. Osbahr, III, MD, MSCM, FACOEM Charles P. Prezzia, MD, MPH, MMM, FACOEM Arthur Rabenhorst, MD, MS, MPH Deborah M. Ratliff, MD, MPH Lora Regan, MD, MPH, FACOEM David M. Rempel, MD, MPH, FACOEM, FACP Jack Richman, MD, CCBOM, FACOEM, FAADEP, CIME Arlen J. Rollins, DO, MSc, FACOEM, FACPM Kaochoy Saechao, MD, MPH Marc Safran, MD Richard E. Sall, MD
1100-7
Patricia Sinnott, PT, PhD, MPH June Spector, MD, MPH Jamie Stark, MS, PhD Christopher H. Stewart-Patterson, MD James B. Talmage, MD, FACOEM William G. Tellin, DC, DABCO Private Practice, Doctor of Chiropractic James L. Thomas, DPM, FACFAS Russell Travis, MD Charles Turkelson, PhD April Hazard Vallerand, PhD, RN, FAAN Pamela A. Warren, PhD Robert W. Watson, Jr., MD, MPH Janet S. Weiss, MD Lyn D. Weiss, MD Michael S. Weiss, MD, MPH, FACOEM, FAAPMR, FAANEM Robert A. Werner, MD, MS, FAAPMR Thomas Winters, MD, FACOEM Eric M. Wood, MD, MPH Phillip Zinni III, DO, FAOASM, MS, ATC Ronald Zipper, DO, FAOAO, FAADEP, CEDIR, CIME How often will they be updated by developing group: Not addressed within the guidelines.

1100-8
CID Management
Clinical Review Criteria Description – Official Disability Guidelines The Official Disability Guidelines published by Work Loss Data Institute, Encinitas, CA. www.odg-twc.com Description: The ODG is a comprehensive set of treatment guidelines for both acute and chronic conditions. How were the criteria developed: According to the ODG preface, the Official Disability Guidelines (ODG) links together four U.S. government databases to provide length-of-disability experience data that can be used to manage employee productivity. These four databases are the following:
ICD-9-CM — The International Classification of Diseases, 9th Revision, Clinical Modification. This is the principle coding system used worldwide for the diagnosis of any medical condition. The main section of ODG includes verbatim the complete "Volume 1, Diseases: Tabular List" of the current Official ICD-9-CM publication. CDC NCHS NHIS — The National Health Interview Survey (NHIS) is conducted annually by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention (CDC). ODG uses data from every year beginning in 1987 until the most current. OSHA BLS OII — The Bureau of Labor Statistics (BLS) reports annually on Occupational Injuries and Illnesses (OII) from forms submitted by employers to the Occupational Safety and Health Administration (OSHA). ODG uses data from the latest available year. HCUP — The Healthcare Cost and Utilization Project (HCUP) is a family of health care databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ) to create a national information resource of patient-level health care data. HCUP includes the largest collection of longitudinal medical care data in the United States. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to health care programs, and outcomes of treatments at the national, State, and local market levels. The latest available year is included in ODG.
From the beginning, the first edition of Official Disability Guidelines (ODG) in 1996 provided lost time guidelines using actual experience data from these federal government databases, specifically OSHA BLS (Occupational Safety and Health Administration – Bureau of Labor Statistics) and CDC NCHS NHIS (Centers for Disease Control and Prevention, National Center for Health Statistics, National Health Interview Survey). The raw data is presented graphically so users can compare it directly with their own experience, and it is designed to enhance a timely and appropriate return-to-work for workers suffering from illness or injury. From the beginning, ODG was based on actual experience, not “expert” opinion. This made ODG fair to employees and defensible by employers. With changes to the Federal Rules of Evidence, the ODG

1100-9
guidelines also became the most likely to stand up in court. As a result of recent U.S. Supreme Court decisions, the Federal Rules of Evidence were recently amended in December 2000. The new rules state that statistical studies will be admissible under the Federal Rules of Evidence, and that such methods generally satisfy important aspects of the “scientific knowledge” requirement articulated in the Daubert Decision. Furthermore, it states that “courts have described surveys as the most direct form of evidence that can be offered, and several courts have drawn negative inferences from the absence of a survey.” Who was involved in the development of the criteria: The ODG editorial advisory board includes: Philip L. Denniston, Jr. Charles W. Kennedy, Jr., MD Kyle Babick, Ph.D. Robert J. Barth, Ph.D. Melissa Bean, DO, MBA, MPH Douglas Benner, MD Faiyaz A. Bhojani, MD, DrPH, FACP Timothy Bialecki, DC Stanley J. Bigos, MD Susan G. Blitz, MD, MPH Daniel V. Bodin, MD, MBA Shannon Boyer, PhD David H. Brill, MD, MA, MPH Pieter Coetzer, MBChB MSc FAADEP CIME Richard Cohen, MD, MPH Alan Colledge, MD, FAADEP, CIME Alberto M. Colombi, MD Steve Demeter, MD, MPH Bill Defoyd, DC Deborah V. DiBenedetto, MBA RN COHN-S/CM ABDA Dennis DiGiorgi, DC, CHCQM, CCIC Dennis G. Egnatz, MD Michael Erdil, MD, FACOEM Marjorie Eskay-Auerbach, MD, JD Ronald Farabaugh, D.C. Steven Feinberg, MD Marc L. Fleming, MS, Registered Pharmacist Joseph A. Fortuna, MD Matt Foster, PharmD, BCPS Gary C. Freeman, MD, JD, MLA Bob Gant, PhD Diane Green, Annette B. Haag, MA, RN, COHN-S/CM Gary Ierna, D.C. Fikry W. Isaac, MD, MPH David Iskowe,
1100-10
Stephen G. Jacobson, MD Gregory Jewell, MD, MS Pamella D. Johnston-Thomas, MD, MPH Christine M. Kalina, MBA MS RN FAAOHN COHN-S/CM Ralph Kendall, PharmD Charles W. Kennedy, Jr., MD Marvin A. Kohn, M.D. Barry Korn, DO, DPM Elizabeth J. Kuschner, R.Ph., Pharm.D. Clement Leech, MB FFOM RCPI FAADEP Douglas W. Martin, MD FAADEP FACOEM FAAFP Edward G. Mauceri, MD Tom Mayer, MD David K. McKenas, MD, MPH J. Mark Melhorn, MD FAAOS FAADEP FACS Wade Meyer, PT, DPT, CSCS Laurence A. Miller, MD Steve Miller, M.S. Pharm. Dana B. Mirkin, MD DABPM Leticia R. Moczygemba, PharmD, PhD Joseph Monkofsky, Jr., MD, MPH Richard H. Nachtigall, MD William Nemeth, MD Trang Nguyen, MD, PhD Chet Nierenberg, MD Suzanne Novak, MD, Phd Esmond Nwokeji, PhD Janet E. O'Brien, MD, MSPH Mike O'Kelley, DC Kathleen O’Lenic, Pharm.D. Mark C. Olesen, MD, MPH, MBA Phillip Osborne, MD Graves T Owen, MD Scott Phillips, Pharm.D. Stuart H. Platt, MSPT, PT Troy Prevot, PA-C MBA Charles Prezzia, MD, MPH Dave Randolph, MD, MPH, FAADEP Julia Rieve, RN, CCM, BSHCM, CPHQ, FNAHQ Chip Robison, Pharm.D. James K. Ross, MD, MBA Lester Sacks, MD, PhD Jason Schliesser, DC, MPH Frank Schneider, DC, MHA Sanford M. Silverman, MD Howard Smith, MD, JD
1100-11
Ralph Smith, MD, MBA Marc T. Taylor, MD, FAADEP David Teuscher, MD Melissa Tonn, MD MBA MPH Russell Travis, MD Eugene A. Truchelut, MD Nick Tsourmas, MD William C. Watters III, MD Clark Watts, MD, JD Ronald Zipper, DO How often will they be updated by developing group: Updates are done as necessary to the website, which may be as frequent as monthly, but will occur no less than 1 time per year.
1100-12
CID Management
Clinical Review Criteria Description – National Guidelines Clearinghouse The National Guidelines Clearinghouse, an initiative of the Agency of Health Care Research and Quality, U.S. Department of Health and Human Services. www.guidelines.gov Description: The National Guideline Clearinghouse™ (NGC) is a comprehensive database of evidence-based clinical practice guidelines and related documents. NGC is an initiative of the Agency for Healthcare Research and Quality (AHRQ), U.S. Department of Health and Human Services. NGC was originally created by AHRQ in partnership with the American Medical Association and the American Association of Health Plans (now America's Health Insurance Plans [AHIP]).
The NGC mission is to provide physicians, nurses, and other health professionals, health care providers, health plans, integrated delivery systems, purchasers and others an accessible mechanism for obtaining objective, detailed information on clinical practice guidelines and to further their dissemination, implementation and use.
Key components of NGC include:
• Structured abstracts (summaries) about the guideline and its development • Links to full-text guidelines, where available, and/or ordering information for print copies • Palm-based PDA Downloads of the Complete NGC Summary for all guidelines
represented in the database. • A Guideline Comparison utility that gives users the ability to generate side-by-side
comparisons for any combination of two or more guidelines • Unique guideline comparisons called Guideline Syntheses prepared by NGC staff,
compare guidelines covering similar topics, highlighting areas of similarity and difference. NGC Guideline Syntheses often provide a comparison of guidelines developed in different countries, providing insight into commonalities and differences in international health practices.
• An electronic forum, NGC-L for exchanging information on clinical practice guidelines, their development, implementation and use
• An Annotated Bibliography database where users can search for citations for publications and resources about guidelines, including guideline development and methodology, structure, evaluation, and implementation
Other user-friendly features include the following:
• What's New enables users to see what guidelines have been added each week and includes an index of all guidelines in NGC.
• NGC Update Service is a weekly electronic mailing of new and updated guidelines posted to the NGC Web site.
• Detailed Search enables users to create very specific search queries based on the various attributes found in the NGC Classification Scheme.
1100-13
• NGC Browse permits users to scan for guidelines available on the NGC site by disease/condition, treatment/intervention, or developing organization.
• PDA/Palm List provides users with information regarding the availability of full-text guidelines and/or companion documents available through the guideline developer, that can be downloaded for the handheld computer (Personal Digital Assistant [PDA], Palm, etc.).
• AHRQ Evidence Reports/Technical Assessments list provides users with links to the Summaries and Full-Text Reports for evidence reports and technology assessments produced under the Agency for Healthcare Research and Quality (AHRQ) Evidence-based Practice Center (EPC) Program. Access the list of EPC Reports, with links to summaries and/or full-text publications.
• Glossary provides definitions of terms used in the standardized abstracts (summaries). How were the criteria developed: The guidelines may be developed by any agency or organization. The NCG determines which guidelines meet their criteria before posting them to the site. Who was involved in the development of the criteria: The guidelines may be developed by any agency or organization. Each guideline must be evaluated on it’s own. How often will they be updated by developing group: Each guideline developer determines how often the guidelines will be updated.

1100-14
CID Management
Clinical Review Criteria Description – NIH PubMed National Institute of Health’s PubMed scientific literature database. www.ncbi.nlm.nih.gov/entrez/ Description: PubMed, available via the NCBI Entrez retrieval system, was developed by the National Center for Biotechnology Information (NCBI) at the National Library of Medicine (NLM), located at the National Institutes of Health (NIH). Entrez is the text-based search and retrieval system used at NCBI for services including PubMed, Nucleotide and Protein Sequences, Protein Structures, Complete Genomes, Taxonomy, OMIM, and many others. PubMed was designed to provide access to citations from biomedical literature. LinkOut provides access to full-text articles at journal Web sites and other related Web resources. PubMed also provides access and links to the other Entrez molecular biology resources. Publishers participating in PubMed electronically submit their citations to NCBI prior to or at the time of publication. If the publisher has a web site that offers full-text of its journals, PubMed provides links to that site as well as biological resources, consumer health information, research tools, and more. There may be a charge to access the text or information. In addition, PubMed provides a Batch Citation Matcher , which allows users to match their citations to PubMed citations using bibliographic information such as journal, volume, issue, page number, and year. PubMed Coverage - PubMed provides access to bibliographic information that includes MEDLINE, OLDMEDLINE, as well as:
o The out-of-scope citations (e.g., articles on plate tectonics or astrophysics) from certain MEDLINE journals, primarily general science and chemistry journals, for which the life sciences articles are indexed for MEDLINE.
o Citations that precede the date that a journal was selected for MEDLINE indexing.
o Some additional life science journals that submit full text to PubMedCentral and receive a qualitative review by NLM.
How were the criteria developed: Criteria are developed through scientific process. Prior to publication, each is subject to peer review. Who was involved in the development of the criteria: Each criteria is developed by a separate entity or provider. How often will they be updated by developing group: Normally these are not updated as they are results of research processes.

1100-15
CID Management
Clinical Review Criteria Description – State of California 8CCR 9792.21 Medical Treatment Utilization Schedule
The State of California 8 CCR 9792.21 Medical Treatment Utilization Schedule. http://www.dir.ca.gov/t8/ch4_5sb1a5_5_2.html Description: The Administrative Director of the Division of Workers’ Compensation, pursuant to the authority granted by Labor Code sections 59, 133, 4603.5, and 5307.3, has adopted Article 5.5.2 of Chapter 4.5, Subchapter 1, Division 1, of Title 8, California Code of Regulations, Section 9792.21 Medical Treatment Utilization Schedule. How were the criteria developed: CA Labor Code 5307.27 states: On or before December 1, 2004, the administrative director, in consultation with the Commission on Health and Safety and Workers' Compensation, shall adopt, after public hearings, a medical treatment utilization schedule, that shall incorporate the evidence-based, peer-reviewed, nationally recognized standards of care recommended by the commission pursuant to Section 77.5, and that shall address, at a minimum, the frequency, duration, intensity, and appropriateness of all treatment procedures and modalities commonly performed in workers' compensation cases. CA Labor Code 4604.5 (b) states: (b) The recommended guidelines set forth in the schedule adopted pursuant to subdivision (a) shall reflect practices that are evidence and scientifically based, nationally recognized, and peer-reviewed. The guidelines shall be designed to assist providers by offering an analytical framework for the evaluation and treatment of injured workers, and shall constitute care in accordance with Section 4600 for all injured workers diagnosed with industrial conditions. CA Labor Code 4610(f) states: The criteria or guidelines used in the utilization review process to determine whether to approve, modify, delay, or deny medical treatment services shall be all of the following:
(1) Developed with involvement from actively practicing physicians. (2) Consistent with the schedule for medical treatment utilization adopted pursuant to Section 5307.27. Prior to adoption of the schedule, these policies and procedures shall be consistent with the recommended standards set forth in the American College of Occupational and Environmental Medicine Occupational Medical PracticeGuidelines.
Who was involved in the development of the criteria: The State of California has not published a list of the contributors. How often will they be updated by developing group: CA Labor Code 4610 (f) requires criteria to be evaluated at least annually and updated as necessary.

1100-16
CID Management
Clinical Review Criteria Description – Commonwealth of Massachusetts HCSB Treatment Guidelines.
Department of Industrial Accidents Health Care Services Board Treatment Guidelines, Commonwealth of Massachusetts. www.mass.gov/dia/hcsb/treatguides.htm Description: Treatment guidelines or practice algorithms are part of a new direction in health care policy and are considered optimal strategies for patient management around which practice patterns should converge. These treatment guidelines are meant to cover the majority of tests and treatments for each condition for which they apply. The original guidelines were derived from multiple sources including, but not limited to, the American Academy of Orthopedic Surgeons, the state of Washington, Department of Labor and Industries and multi-disciplinary committees of the Health Care Services Board. How were the criteria developed: In 1991, MA Governor William Weld promulgated major Workers' Compensation reform legislation. The legislation provided a new direction for Workers' Compensation health care in Massachusetts's. Central to the reform was the Department of Industrial Accidents' (DIA) implementation of a utilization review and quality assessment program to monitor the appropriateness of medical services, as well as the necessity and the effectiveness of treatment for injured/ill employees. Further, the statute reconvened and enhanced the responsibilities of the Health Care Services Board (HCSB). Composed of 13 voluntary members, one of the responsibilities the Board was charged with was the development of treatment guidelines for the appropriate and necessary treatment of Massachusetts's injured/ill workers. These treatment guidelines were accepted and per statute M.G.L. c. 152 promulgated on July 1, 1993, to be used for all health care services rendered on or after October 1, 1993. Who was involved in the development of the criteria: According to the MA State website, the committee who developed the criteria consisted of 13 voluntary members. The names of the members were not noted. How often will they be updated by developing group: M.G.L. c. 152 requires annual review of the guidelines currently in existence.
1100-17
CID Management
Clinical Review Criteria Description – Colorado Medical Treatment Guidelines
Colorado Department of Labor and Employment Medical Treatment Guidelines. http://www.coworkforce.com/dwc/Medical_Treatment.asp Description: According to the Colorado Division of Workers’ Compensation, in an effort to comply with its legislative charge to assure appropriate medical care at a reasonable cost, the director of the Division has promulgated these "Medical Treatment Guidelines." This rule provides a system of evaluation and treatment guidelines for high cost or high frequency categories of occupational injury or disease to assure appropriate medical care at a reasonable cost. How were the criteria developed: The Colorado Department of Labor and Employment has not published the process by which the criteria were developed. Who was involved in the development of the criteria: The Colorado Department of Labor and Employment has not published a list of the contributors. How often will they be updated by developing group: Pursuant to section 8-42-101(3)(a)(I), C.R.S., prior to July 1 of each year the Division Director shall review all medical treatment guidelines. Written comments which have been submitted by the public to the director or the Division's medical director will be considered during such reviews.

1100-18
CID Management
Clinical Review Criteria Description – Delaware Health Care Practices Guidelines Delaware Health Care Practices Guidelines http://regulations.delaware.gov/AdminCode/title19/1000/1300/1340/ Description: Pursuant to 19 Del.C. §2322C, health care practice guidelines have been adopted and recommended by the Health Care Advisory Panel to guide utilization of health care treatments in workers' compensation including, but not limited to, care provided for the treatment of employees by or under the supervision of a licensed health care provider, prescription drug utilization, inpatient hospitalization and length of stay, diagnostic testing, physical therapy, chiropractic care and palliative care. How were the criteria developed: The Delaware Department of Labor has not published the process by which the criteria were developed. Who was involved in the development of the criteria: Bruce Rudin, M.D. Chair George B. Heckler, Esquire, Vice-Chair Marcia Dewitt Walter Power, M.D. Glenn Brown Josette Covington, M.D. James Downing, M.D. Barry Bakst, D.O. Richard Heffron Wayne Collison Douglas Briggs, D.C How often will they be updated by developing group: The Delaware Department of Labor has not published a schedule of review or revision.

1100-19
CID Management
Clinical Review Criteria Description –
Minnesota Department of Labor and Industry Minnesota Department of Labor and Industry http://regulations.delaware.gov/AdminCode/title19/1000/1300/1340/ Description: Guidelines developed by the Minnesota Department of Labor and Industry in the form of regulatory language, in an attempt to define what is medically necessary. How were the criteria developed: The Minnesota Department of Labor and Industry has not published the process by which the criteria were developed. Who was involved in the development of the criteria: Philip Bachman, M.D. Beth Baker, M.D., MSRB chairperson Barbara Baum, M.S., P.T. Jeffrey Bonsell, D.C. Michael Goertz, M.D. Andrea Trimble Hart, CPCU Kathi Henrickson, R.N. Gregory J. Hynan, D.C. John Kipp, M.D., J.D. Reed Pollack Andrew Schmidt, M.D. Elizabeth Shogren, R.N. Jon Talsness, M.D. How often will they be updated by developing group: The Minnesota Department of Labor and Industry has not published a schedule of review or revision.
1100-20
CID Management
Clinical Review Criteria Description –
Washington State Department of Labor and Industries, Medical Treatment Guidelines
Washington State Department of Labor and Industries, Medical Treatment Guidelines http://www.lni.wa.gov/ClaimsIns/Providers/Treatment/TreatGuide/ Description: How were the criteria developed: The Washington State Department of Labor and Industries, Medical Treatment Guidelines have been “developed by the Office of the Medical Director in collaboration with practicing physicians and advisors”. This is believed to be the Industrial Insurance Medical Advisory Committee. Who was involved in the development of the criteria: Ruth M. Bishop, DO Gregory T. Carter, MD Dianna Chamblin, MD (Vice-chair) G. A. DeAndrea, MD, MBA Jordan Firestone, MD, PhD, MPH Andrew Friedman, MD Kirk T. Harmon, MD Walter F. Krengel III, MD Robert G. R. Lang, MD (Chair) Janet E. Ploss, MD Mark Sullivan, MD, PhD David J. Tauben, MD G. Robert Waring, MD Gerald N. Yorioka, MD How often will they be updated by developing group: The Washington State Department of Labor and Industries has not published a schedule of review or revision.

1100-21
CID Management
Clinical Review Criteria Description – Wyoming Workers’ Safety and
Compensation Division Treatment Guidelines Wyoming Workers’ Safety and Compensation Division Treatment Guidelines http://doe.wyo.gov/serviceproviders/Pages/default.aspx Description: None provided by jurisdictional authority How were the criteria developed: Consensus development will take place between the Medical Commission members and active practicing community-based Heath Care Providers who are clinical experts in the topic(s) to be addressed. Newly developed treatment guidelines may be quite liberally contructed, however, subsequent tightening of the treatment guidelines would occur as national guidelines are set, or other scientific evidence becomes available. Who was involved in the development of the criteria: Unknown How often will they be updated by developing group: The Wyoming Workers’ Safety and Compensation Division has not published a schedule of review or revision.

1200-1
CID Management
Conflict of Interest
Policy No. 1200 Revision: 3.0 Revision Date: 6/5/2007 Page 1 of 2
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines addressing conflicts of interest that may arise in the performance of utilization management.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 05/14/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 01/27/2011 Reviewed Revision 3.0 04/22/2012 Reviewed Revision 3.0 01/09/2013 Reviewed
3.0 Persons Affected This policy affects all CID employees and contractors who participate in any utilization management operations.
4.0 Policy The policy of CID Management is to avoid any conflicts of interest which may arise in the performance of utilization management operations. Conflicts of interest may include, but are not limited to:
4.1 an ownership interest of greater than 5% between affected parties 4.2 a material professional or business relationship 4.3 a direct or indirect financial incentive for a particular determination 4.4 incentives to promote the use of a certain product or service
1200-2
4.5 a known familial relationship 4.6 any prior involvement in the specific case under review
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 Each CID employee and contractor shall sign a contract stating that they shall not
perform utilization management services in situations where a conflict of interest exists.
6.2 Each CID employee and contractor shall be trained on recognizing conflict of interest
situations. 6.3 If, in the performance of utilization management duties, any CID non-clinical
administrative staff member discovers that they have a conflict of interest, they shall immediately cease activity and notify their direct supervisor.
6.4 The supervisor shall then re-assign the work duties to an alternate CID non-clinical
administrative staff member for whom no conflict of interest exists. 6.5 The supervisor shall record the conflict of interest, and the re-assignment of work
duties, within the CID system. 6.6 If, in the performance of utilization management duties, any initial clinical reviewer
or clinical peer reviewer contracted with CID discovers that they have a conflict of interest, they shall immediately recuse themselves from the review using the CID system.
6.7 The CID system shall re-assign the work duties to an alternate initial clinical reviewer
or clinical peer reviewer for whom no conflict of interest has been identified. 6.8 The CID system shall record the conflict of interest, and the re-assignment of work
duties, as an activity within the CID system.
6.9 To avoid conflict of interest situations, CID specifically does not have a system for reimbursement, bonuses, or incentives to staff based directly or indirectly on consumer utilization of health care services.

1300-1
CID Management
Utilization Management Labor Code and Regulations Compliance
Policy No. 1300 Revision: 3.0 Revision Date: 6/5/07 Page 1 of 58
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which CID ensures that it remains compliant with labor code and regulations, including URAC Standards, addressing the performance of utilization management operations.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy and Addenda/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 05/14/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 01/26/2011 Reviewed Revision 3.0 12/22/2011 Reviewed Revision 3.0 04/22/2012 Reviewed Revision 3.0 01/09/2013 Reviewed
3.0 Persons Affected This policy affects the Medical Director, Clinical Director and any parties or committees that may be required to convene as a result of changes to the labor code or regulations.
4.0 Policy The policy of CID Management is to monitor the labor code and regulations, including URAC Standards, addressing utilization management on an ongoing basis to ensure the CID utilization management policies and procedures remain in compliance.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
1300-2
6.1 On an ongoing basis, the Medical Director and Clinical Director shall monitor the utilization management labor codes and regulations in each state in which CID performs utilization management functions.
6.2 On an ongoing basis, the Clinical Director shall monitor for changes in URAC
Standards for current compliance. Additionally, the Clinical Director will check with URAC for updates to the Standards by contacting URAC by phone at (202) 216-9010 and check on the www.urac.com website under the link “News Room” and sub-link “Latest News Releases” for updates or revision to the URAC Standards.
6.3 If an update is made to either labor codes or regulations surrounding utilization
management, the Medical Director and Clinical Director shall notify any CID parties and/or committees that must be convened to address the new labor code and/or regulations.
6.4 The CID parties and/or committees shall review the current policies and procedures
and make any necessary modifications to ensure CID’s continued compliance with labor code and regulations.
6.5 The CID parties and/or committees shall report their actions to the Medical Director
and Clinical Director. 6.6 The Medical Director shall review the final modifications to the CID policies and/or
procedures and ensure that CID remains in compliance with labor code and regulations surrounding utilization management.
1300-3
Addenda
California Labor Code and Regulations
4604.5. (a) The recommended guidelines set forth in the medical treatment utilization schedule adopted by the administrative director pursuant to Section 5307.27 shall be presumptively correct on the issue of extent and scope of medical treatment. The presumption is rebuttable and may be controverted by a preponderance of the scientific medical evidence establishing that a variance from the guidelines reasonably is required to cure or relieve the injured worker from the effects of his or her injury. The presumption created is one affecting the burden of proof. (b) The recommended guidelines set forth in the schedule adopted pursuant to subdivision (a) shall reflect practices that are evidence and scientifically based, nationally recognized, and peer reviewed. The guidelines shall be designed to assist providers by offering an analytical framework for the evaluation and treatment of injured workers, and shall constitute care in accordance with Section 4600 for all injured workers diagnosed with industrial conditions. (c) (1) Notwithstanding the medical treatment utilization schedule, for injuries occurring on
and after January 1, 2004, an employee shall be entitled to no more than 24 chiropractic, 24 occupational therapy, and 24 physical therapy visits per industrial injury.
(2) (A) Paragraph (1) shall not apply when an employer authorizes, in writing, additional visits to a health care practitioner for physical medicine services. Payment or authorization for treatment beyond the limits set forth in paragraph (1) shall not be deemed a waiver of the limits set forth by paragraph (1) with respect to future requests for authorization.
(B) The Legislature finds and declares that the amendments made to subparagraph (A) by the act adding this subparagraph are declaratory of existing law.
(3) Paragraph (1) shall not apply to visits for postsurgical physical medicine and postsurgical rehabilitation services provided in compliance with a postsurgical treatment utilization schedule established by the administrative director pursuant to Section 5307.27.
(d) For all injuries not covered by the official utilization schedule adopted pursuant to Section 5307.27, authorized treatment shall be in accordance with other evidence-based medical treatment guidelines that are recognized generally by the national medical community and scientifically based. 4610. (a) For purposes of this section, "utilization review" means utilization review or utilization management functions that prospectively, retrospectively, or concurrently review and approve, modify, delay, or deny, based in whole or in part on medical necessity to cure and relieve, treatment recommendations by physicians, as defined in Section 3209.3, prior to, retrospectively, or concurrent with the provision of medical treatment services pursuant to Section 4600.

1300-4
(b) Every employer shall establish a utilization review process in compliance with this section, either directly or through its insurer or an entity with which an employer or insurer contracts for these services. (c) Each utilization review process shall be governed by written policies and procedures. These policies and procedures shall ensure that decisions based on the medical necessity to cure and relieve of proposed medical treatment services are consistent with the schedule for medical treatment utilization adopted pursuant to Section 5307.27. These policies and procedures, and a description of the utilization process, shall be filed with the administrative director and shall be disclosed by the employer to employees, physicians, and the public upon request. (d) If an employer, insurer, or other entity subject to this section requests medical information from a physician in order to determine whether to approve, modify, delay, or deny requests for authorization, the employer shall request only the information reasonably necessary to make the determination. The employer, insurer, or other entity shall employ or designate a medical director who holds an unrestricted license to practice medicine in this state issued pursuant to Section 2050 or Section 2450 of the Business and Professions Code. The medical director shall ensure that the process by which the employer or other entity reviews and approves, modifies, delays, or denies requests by physicians prior to, retrospectively, or concurrent with the provision of medical treatment services, complies with the requirements of this section. Nothing in this section shall be construed as restricting the existing authority of the Medical Board of California. (e) No person other than a licensed physician who is competent to evaluate the specific clinical issues involved in the medical treatment services, and where these services are within the scope of the physician's practice, requested by the physician may modify, delay, or deny requests for authorization of medical treatment for reasons of medical necessity to cure and relieve. (f) The criteria or guidelines used in the utilization review process to determine whether to approve, modify, delay, or deny medical treatment services shall be all of the following:
(1) Developed with involvement from actively practicing physicians. (2) Consistent with the schedule for medical treatment utilization adopted pursuant to
Section 5307.27. (3) Evaluated at least annually, and updated if necessary. (4) Disclosed to the physician and the employee, if used as the basis of a decision to
modify, delay, or deny services in a specified case under review. (5) Available to the public upon request. An employer shall only be required to disclose
the criteria or guidelines for the specific procedures or conditions requested. An employer may charge members of the public reasonable copying and postage expenses related to disclosing criteria or guidelines pursuant to this paragraph. Criteria or guidelines may also be made available through electronic means. No charge shall be required for an employee whose physician's request for medical treatment services is under review.
(g) In determining whether to approve, modify, delay, or deny requests by physicians prior to, retrospectively, or concurrent with the provisions of medical treatment services to employees all of the following requirements shall be met:

1300-5
(1) Prospective or concurrent decisions shall be made in a timely fashion that is appropriate for the nature of the employee's condition, not to exceed five working days from the receipt of the information reasonably necessary to make the determination, but in no event more than 14 days from the date of the medical treatment recommendation by the physician. In cases where the review is retrospective, a decision resulting in denial of all or part of the medical treatment service shall be communicated to the individual who received services, or to the individual's designee, within 30 days of receipt of information that is reasonably necessary to make this determination. If payment for a medical treatment service is made within the time prescribed by Section 4603.2, a retrospective decision to approve the service need not otherwise be communicated.
(2) When the employee's condition is such that the employee faces an imminent and serious threat to his or her health, including, but not limited to, the potential loss of life, limb, or other major bodily function, or the normal timeframe for the decisionmaking process, as described in paragraph (1), would be detrimental to the employee's life or health or could jeopardize the employee's ability to regain maximum function, decisions to approve, modify, delay, or deny requests by physicians prior to, or concurrent with, the provision of medical treatment services to employees shall be made in a timely fashion that is appropriate for the nature of the employee's condition, but not to exceed 72 hours after the receipt of the information reasonably necessary to make the determination.
(3) (A) Decisions to approve, modify, delay, or deny requests by physicians for authorization prior to, or concurrent with, the provision of medical treatment services to employees shall be communicated to the requesting physician within 24 hours of the decision. Decisions resulting in modification, delay, or denial of all or part of the requested health care service shall be communicated to physicians initially by telephone or facsimile, and to the physician and employee in writing within 24 hours for concurrent review, or within two business days of the decision for prospective review, as prescribed by the administrative director. If the request is not approved in full, disputes shall be resolved in accordance with Section 4610.5, if applicable, or otherwise in accordance with Section 4062.
(B) In the case of concurrent review, medical care shall not be discontinued until the employee's physician has been notified of the decision and a care plan has been agreed upon by the physician that is appropriate for the medical needs of the employee. Medical care provided during a concurrent review shall be care that is medically necessary to cure and relieve, and an insurer or self-insured employer shall only be liable for those services determined medically necessary to cure and relieve. If the insurer or self-insured employer disputes whether or not one or more services offered concurrently with a utilization review were medically necessary to cure and relieve, the dispute shall be resolved pursuant to Section 4610.5, if applicable, or otherwise pursuant to Section 4062. Any compromise between the parties that an insurer or self-insured employer believes may result in payment for services that were not medically necessary to cure and relieve shall be reported by the insurer or the self-insured employer to the licensing board of the provider or providers who received the payments, in a manner set forth by the respective board and in such a way as to minimize reporting costs both to the

1300-6
board and to the insurer or self-insured employer, for evaluation as to possible violations of the statutes governing appropriate professional practices. No fees shall be levied upon insurers or self-insured employers making reports required by this section.
(4) Communications regarding decisions to approve requests by physicians shall specify the specific medical treatment service approved. Responses regarding decisions to modify, delay, or deny medical treatment services requested by physicians shall include a clear and concise explanation of the reasons for the employer's decision, a description of the criteria or guidelines used, and the clinical reasons for the decisions regarding medical necessity. If a utilization review decision to deny or delay a medical service is due to incomplete or insufficient information, the decision shall specify the reason for the decision and specify the information that is needed.
(5) If the employer, insurer, or other entity cannot make a decision within the timeframes specified in paragraph (1) or (2) because the employer or other entity is not in receipt of all of the information reasonably necessary and requested, because the employer requires consultation by an expert reviewer, or because the employer has asked that an additional examination or test be performed upon the employee that is reasonable and consistent with good medical practice, the employer shall immediately notify the physician and the employee, in writing, that the employer cannot make a decision within the required timeframe, and specify the information requested but not received, the expert reviewer to be consulted, or the additional examinations or tests required. The employer shall also notify the physician and employee of the anticipated date on which a decision may be rendered. Upon receipt of all information reasonably necessary and requested by the employer, the employer shall approve, modify, or deny the request for authorization within the timeframes specified in paragraph (1) or (2).
(6) A utilization review decision to modify, delay, or deny a treatment recommendation shall remain effective for 12 months from the date of the decision without further action by the employer with regard to any further recommendation by the same physician for the same treatment unless the further recommendation is supported by adocumented change in the facts material to the basis of the utilization review decision.
(7) Utilization review of a treatment recommendation shall not be required while the employer is disputing liability for injury or treatment of the condition for which treatment is recommended pursuant to Section 4062.
(8) If utilization review is deferred pursuant to paragraph (7), and it is finally determined that the employer is liable for treatment of the condition for which treatment is recommended, the time for the employer to conduct retrospective utilization review in accordance with paragraph (1) shall begin on the date the determination of the employer's liability becomes final, and the time for the employer to conduct prospective utilization review shall commence from the date of the employer's receipt of a treatment recommendation after the determination of the employer's liability.
(h) Every employer, insurer, or other entity subject to this section shall maintain telephone access for physicians to request authorization for health care services.
1300-7
(i) If the administrative director determines that the employer, insurer, or other entity subject to this section has failed to meet any of the timeframes in this section, or has failed to meet any other requirement of this section, the administrative director may assess, by order, administrative penalties for each failure. A proceeding for the issuance of an order assessing administrative penalties shall be subject to appropriate notice to, and an opportunity for a hearing with regard to, the person affected. The administrative penalties shall not be deemed to be an exclusive remedy for the administrative director. These penalties shall be deposited in the Workers' Compensation Administration Revolving Fund. 4610.5. (a) This section applies to the following disputes:
(1) Any dispute over a utilization review decision regarding treatment for an injury occurring on or after January 1, 2013.
(2) Any dispute over a utilization review decision if the decision is communicated to the requesting physician on or after July 1, 2013, regardless of the date of injury.
(b) A dispute described in subdivision (a) shall be resolved only in accordance with this section. (c) For purposes of this section and Section 4610.6, the following definitions apply:
(1) "Disputed medical treatment" means medical treatment that has been modified, delayed, or denied by a utilization review decision.
(2) "Medically necessary" and "medical necessity" mean medical treatment that is reasonably required to cure or relieve the injured employee of the effects of his or her injury and based on the following standards, which shall be applied in the order listed, allowing reliance on a lower ranked standard only if every higher ranked standard is inapplicable to the employee's medical condition: (A) The guidelines adopted by the administrative director pursuant to Section
5307.27. (B) Peer-reviewed scientific and medical evidence regarding the effectiveness of the
disputed service. (C) Nationally recognized professional standards. (D) Expert opinion. (E) Generally accepted standards of medical practice. (F) Treatments that are likely to provide a benefit to a patient for conditions for which
other treatments are not clinically efficacious. (3) "Utilization review decision" means a decision pursuant to Section 4610 to modify,
delay, or deny, based in whole or in part on medical necessity to cure or relieve, a treatment recommendation or recommendations by a physician prior to, retrospectively, or concurrent with the provision of medical treatment services pursuant to Section 4600 or subdivision (c) of Section 5402.
(4) Unless otherwise indicated by context, "employer" means the employer, the insurer of an insured employer, a claims administrator, or a utilization review organization, or other entity acting on behalf of any of them.
(d) If a utilization review decision denies, modifies, or delays a treatment recommendation, the employee may request an independent medical review as provided by this section.

1300-8
(e) A utilization review decision may be reviewed or appealed only by independent medical review pursuant to this section. Neither the employee nor the employer shall have any liability for medical treatment furnished without the authorization of the employer if the treatment is delayed, modified, or denied by a utilization review decision unless the utilization review decision is overturned by independent medical review in accordance with this section. (f) As part of its notification to the employee regarding an initial utilization review decision that denies, modifies, or delays a treatment recommendation, the employer shall provide the employee with a one-page form prescribed by the administrative director, and an addressed envelope, which the employee may return to the administrative director or the administrative director's designee to initiate an independent medical review. The employer shall include on the form any information required by the administrative director to facilitate the completion of the independent medical review. The form shall also include all of the following:
(1) Notice that the utilization review decision is final unless the employee requests independent medical review.
(2) A statement indicating the employee's consent to obtain any necessary medical records from the employer or insurer and from any medical provider the employee may have consulted on the matter, to be signed by the employee.
(3) Notice of the employee's right to provide information or documentation, either directly or through the employee's physician, regarding the following: (A) The treating physician's recommendation indicating that the disputed medical
treatment is medically necessary for the employee's medical condition. (B) Medical information or justification that a disputed medical treatment, on an
urgent care or emergency basis, was medically necessary for the employee's medical condition.
(C) Reasonable information supporting the employee's position that the disputed medical treatment is or was medically necessary for the employee's medical condition, including all information provided to the employee by the employer or by the treating physician, still in the employee's possession, concerning the employer's or the physician' s decision regarding the disputed medical treatment, as well as any additional material that the employee believes is relevant.
(g) The independent medical review process may be terminated at any time upon the employer's written authorization of the disputed medical treatment. (h) (1) The employee may submit a request for independent medical review to the division no later than 30 days after the service of the utilization review decision to the employee.
(2) If at the time of a utilization review decision the employer is also disputing liability for the treatment for any reason besides medical necessity, the time for the employee to submit a request for independent medical review to the administrative director or administrative director's designee is extended to 30 days after service of a notice to the employee showing that the other dispute of liability has been resolved.
(3) If the employer fails to comply with subdivision (e) at the time of notification of its utilization review decision, the time limitations for the employee to submit a request

1300-9
for independent medical review shall not begin to run until the employer provides the required notice to the employee.
(4) A provider of emergency medical treatment when the employee faced an imminent and serious threat to his or her health, including, but not limited to, the potential loss of life, limb, or other major bodily function, may submit a request for independent medical review on its own behalf. A request submitted by a provider pursuant to this paragraph shall be submitted to the administrative director or administrative director's designee within the time limitations applicable for an employee to submit a request for independent medical review.
(i) An employer shall not engage in any conduct that has the effect of delaying the independent review process. Engaging in that conduct or failure of the plan to promptly comply with this section is a violation of this section and, in addition to any other fines, penalties, and other remedies available to the administrative director, the employer shall be subject to an administrative penalty in an amount determined pursuant to regulations to be adopted by the administrative director, not to exceed five thousand dollars ($5,000) for each day that proper notification to the employee is delayed. The administrative penalties shall be paid to the Workers' Compensation Administration Revolving Fund. (j) For purposes of this section, an employee may designate a parent, guardian, conservator, relative, or other designee of the employee as an agent to act on his or her behalf. A designation of an agent executed prior to the utilization review decision shall not be valid. The requesting physician may join with or otherwise assist the employee in seeking an independent medical review, and may advocate on behalf of the employee. (k) The administrative director or his or her designee shall expeditiously review requests and immediately notify the employee and the employer in writing as to whether the request for an independent medical review has been approved, in whole or in part, and, if not approved, the reasons therefor. If there appears to be any medical necessity issue, the dispute shall be resolved pursuant to an independent medical review, except that, unless the employer agrees that the case is eligible for independent medical review, a request for independent medical review shall be deferred if at the time of a utilization review decision the employer is also disputing liability for the treatment for any reason besides medical necessity. (l) Upon notice from the administrative director that an independent review organization has been assigned, the employer shall provide to the independent medical review organization all of the following documents within 10 days of notice of assignment:
(1) A copy of all of the employee's medical records in the possession of the employer or under the control of the employer relevant to each of the following: (A) The employee's current medical condition. (B) The medical treatment being provided by the employer. (C) The disputed medical treatment requested by the employee.
(2) A copy of all information provided to the employee by the employer concerning employer and provider decisions regarding the disputed treatment.
(3) A copy of any materials the employee or the employee's provider submitted to the employer in support of the employee's request for the disputed treatment.
1300-10
(4) A copy of any other relevant documents or information used by the employer or its utilization review organization in determining whether the disputed treatment should have been provided, and any statements by the employer or its utilization review organization explaining the reasons for the decision to deny, modify, or delay the recommended treatment on the basis of medical necessity. The employer shall concurrently provide a copy of the documents required by this paragraph to the employee and the requesting physician, except that documents previously provided to the employee or physician need not be provided again if a list of those documents is provided.
(m) Any newly developed or discovered relevant medical records in the possession of the employer after the initial documents are provided to the independent medical review organization shall be forwarded immediately to the independent medical review organization. The employer shall concurrently provide a copy of medical records required by this subdivision to the employee or the employee's treating physician, unless the offer of medical records is declined or otherwise prohibited by law. The confidentiality of medical records shall be maintained pursuant to applicable state and federal laws. (n) If there is an imminent and serious threat to the health of the employee, as specified in subdivision (c) of Section 1374.33 of the Health and Safety Code, all necessary information and documents required by subdivision (l) shall be delivered to the independent medical review organization within 24 hours of approval of the request for review. (o) The employer shall promptly issue a notification to the employee, after submitting all of the required material to the independent medical review organization, that lists documents submitted and includes copies of material not previously provided to the employee or the employee's designee.
1300-11
4610.6. (a) Upon receipt of a case pursuant to Section 4610.5, an independent medical review organization shall conduct the review in accordance with this article and any regulations or orders of the administrative director. The organization's review shall be limited to an examination of the medical necessity of the disputed medical treatment. (b) Upon receipt of information and documents related to a case, the medical reviewer or reviewers selected to conduct the review by the independent medical review organization shall promptly review all pertinent medical records of the employee, provider reports, and any other information submitted to the organization or requested from any of the parties to the dispute by the reviewers. If the reviewers request information from any of the parties, a copy of the request and the response shall be provided to all of the parties. The reviewer or reviewers shall also review relevant information related to the criteria set forth in subdivision (c). (c) Following its review, the reviewer or reviewers shall determine whether the disputed health care service was medically necessary based on the specific medical needs of the employee and the standards of medical necessity as defined in subdivision (c) of Section 4610.5. (d) The organization shall complete its review and make its determination in writing, and in layperson's terms to the maximum extent practicable, within 30 days of the receipt of the request for review and supporting documentation, or within less time as prescribed by the administrative director. If the disputed medical treatment has not been provided and the employee's provider or the administrative director certifies in writing that an imminent and serious threat to the health of the employee may exist, including, but not limited to, serious pain, the potential loss of life, limb, or major bodily function, or the immediate and serious deterioration of the health of the employee, the analyses and determinations of the reviewers shall be expedited and rendered within three days of the receipt of the information. Subject to the approval of the administrative director, the deadlines for analyses and determinations involving both regular and expedited reviews may be extended for up to three days in extraordinary circumstances or for good cause. (e) The medical professionals' analyses and determinations shall state whether the disputed health care service is medically necessary. Each analysis shall cite the employee's medical condition, the relevant documents in the record, and the relevant findings associated with the provisions of subdivision (c) to support the determination. If more than one medical professional reviews the case, the recommendation of the majority shall prevail. If the medical professionals reviewing the case are evenly split as to whether the disputed health care service should be provided, the decision shall be in favor of providing the service. (f) The independent medical review organization shall provide the administrative director, the employer, the employee, and the employee's provider with the analyses and determinations of the medical professionals reviewing the case, and a description of the qualifications of the medical professionals. The independent medical review organization shall keep the names of the reviewers confidential in all communications with entities or individuals outside the independent medical review organization. If more than one medical professional reviewed the case and the result was differing determinations, the independent medical review organization shall provide each of the separate reviewer's analyses and determinations.

1300-12
(g) The determination of the independent medical review organization shall be deemed to be the determination of the administrative director and shall be binding on all parties. (h) A determination of the administrative director pursuant to this section may be reviewed only by a verified appeal from the medical review determination of the administrative director, filed with the appeals board for hearing pursuant to Chapter 3 (commencing with Section 5500) of Part 4 and served on all interested parties within 30 days of the date of mailing of the determination to the aggrieved employee or the aggrieved employer. The determination of the administrative director shall be presumed to be correct and shall be set aside only upon proof by clear and convincing evidence of one or more of the following grounds for appeal:
(1) The administrative director acted without or in excess of the administrative director's powers.
(2) The determination of the administrative director was procured by fraud. (3) The independent medical reviewer was subject to a material conflict of interest that is
in violation of Section 139.5. (4) The determination was the result of bias on the basis of race, national origin, ethnic
group identification, religion, age, sex, sexual orientation, color, or disability. (5) The determination was the result of a plainly erroneous express or implied finding of
fact, provided that the mistake of fact is a matter of ordinary knowledge based on the information submitted for review pursuant to Section 4610.5 and not a matter that is subject to expert opinion.
(i) If the determination of the administrative director is reversed, the dispute shall be remanded to the administrative director to submit the dispute to independent medical review by a different independent review organization. In the event that a different independent medical review organization is not available after remand, the administrative director shall submit the dispute to the original medical review organization for review by a different reviewer in the organization. In no event shall a workers' compensation administrative law judge, the appeals board, or any higher court make a determination of medical necessity contrary to the determination of the independent medical review organization. (j) Upon receiving the determination of the administrative director that a disputed health care service is medically necessary, the employer shall promptly implement the decision as provided by this section unless the employer has also disputed liability for any reason besides medical necessity. In the case of reimbursement for services already rendered, the employer shall reimburse the provider or employee, whichever applies, within 20 days, subject to resolution of any remaining issue of the amount of payment pursuant to Sections 4603.2 to 4603.6, inclusive. In the case of services not yet rendered, the employer shall authorize the services within five working days of receipt of the written determination from the independent medical review organization, or sooner if appropriate for the nature of the employee's medical condition, and shall inform the employee and provider of the authorization. (k) Failure to pay for services already provided or to authorize services not yet rendered within the time prescribed by subdivision (l) is a violation of this section and, in addition to any other fines, penalties, and other remedies available to the administrative director, the employer shall be subject to an administrative penalty in an amount determined pursuant to regulations to be
1300-13
adopted by the administrative director, not to exceed five thousand dollars ($5,000) for each day the decision is not implemented. The administrative penalties shall be paid to the Workers' Compensation Administration Revolving Fund. (l) The costs of independent medical review and the administration of the independent medical review system shall be borne by employers through a fee system established by the administrative director. After considering any relevant information on program costs, the administrative director shall establish a reasonable, per-case reimbursement schedule to pay the costs of independent medical review organization reviews and the cost of administering the independent medical review system, which may vary depending on the type of medical condition under review and on other relevant factors. (m) The administrative director may publish the results of independent medical review determinations after removing individually identifiable information. (n) If any provision of this section, or the application thereof to any person or circumstances, is held invalid, the remainder of the section, and the application of its provisions to other persons or circumstances, shall not be affected thereby.
1300-14
§ 9792.6. Utilization Review Standards—Definitions - For Utilization Review Decisions Issued Prior to July 1, 2013 for Injuries Occurring Prior to January 1, 2013. The following definitions apply to any request for authorization of medical treatment, made under Article 5.5.1 of this Subchapter, for an occupational injury or illness occurring prior to January 1, 2013 if the decision on the request is communicated to the requesting physician prior to July 1, 2013. (a) “ACOEM Practice Guidelines” means the American College of Occupational and Environmental Medicine's Occupational Medicine Practice Guidelines, Second Edition. (b) “Authorization” means assurance that appropriate reimbursement will be made for an approved specific course of proposed medical treatment to cure or relieve the effects of the industrial injury pursuant to section 4600 of the Labor Code, subject to the provisions of section 5402 of the Labor Code, based on the Doctor's First Report of Occupational Injury or Illness,” Form DLSR 5021, or on the “Primary Treating Physician's Progress Report,” DWC Form PR-2, as contained in section 9785.2, or in narrative form containing the same information required in the DWC Form PR-2. (c) “Claims Administrator” is a self-administered workers' compensation insurer, an insured employer, a self-administered self-insured employer, a self-administered legally uninsured employer, a self-administered joint powers authority, a third-party claims administrator or other entity subject to Labor Code section 4610. The claims administrator may utilize an entity contracted to conduct its utilization review responsibilities. (d) “Concurrent review” means utilization review conducted during an inpatient stay. (e) “Course of treatment” means the course of medical treatment set forth in the treatment plan contained on the “Doctor's First Report of Occupational Injury or Illness,” Form DLSR 5021, or on the “Primary Treating Physician's Progress Report,” DWC Form PR-2, as contained in section 9785.2 or in narrative form containing the same information required in the DWC Form PR-2. (f) “Emergency health care services” means health care services for a medical condition manifesting itself by acute symptoms of sufficient severity such that the absence of immediate medical attention could reasonably be expected to place the patient's health in serious jeopardy. (g) “Expedited review” means utilization review conducted when the injured worker's condition is such that the injured worker faces an imminent and serious threat to his or her health, including, but not limited to, the potential loss of life, limb, or other major bodily function, or the normal timeframe for the decision-making process would be detrimental to the injured worker's life or health or could jeopardize the injured worker's permanent ability to regain maximum function. (h) “Expert reviewer” means a medical doctor, doctor of osteopathy, psychologist, acupuncturist, optometrist, dentist, podiatrist, or chiropractic practitioner licensed by any state or the District of Columbia, competent to evaluate the specific clinical issues involved in the medical treatment

1300-15
services and where these services are within the individual's scope of practice, who has been consulted by the reviewer or the utilization review medical director to provide specialized review of medical information. (i) “Health care provider” means a provider of medical services, as well as related services or goods, including but not limited to an individual provider or facility, a health care service plan, a health care organization, a member of a preferred provider organization or medical provider network as provided in Labor Code section 4616. (j) “Immediately” means within 24 hours after learning the circumstances that would require an extension of the timeframe for decisions specified in subdivisions (b)(1), (b)(2) or (c) and (g)(1) of section 9792.9. (k) “Material modification” is when the claims administrator changes utilization review vendor or makes a change to the utilization review standards as specified in section 9792.7. (l) “Medical Director” is the physician and surgeon licensed by the Medical Board of California or the Osteopathic Board of California who holds an unrestricted license to practice medicine in the State of California. The Medical Director is responsible for all decisions made in the utilization review process. (m) “Medical services” means those goods and services provided pursuant to Article 2 (commencing with Labor Code section 4600) of Chapter 2 of Part 2 of Division 4 of the Labor Code. (n) “Prospective review” means any utilization review conducted, except for utilization review conducted during an inpatient stay, prior to the delivery of the requested medical services. (o) “Request for authorization” means a written confirmation of an oral request for a specific course of proposed medical treatment pursuant to Labor Code section 4610(h) or a written request for a specific course of proposed medical treatment. An oral request for authorization must be followed by a written confirmation of the request within seventy-two (72) hours. Both the written confirmation of an oral request and the written request must be set forth on the “Doctor's First Report of Occupational Injury or Illness,” Form DLSR 5021, section 14006, or on the Primary Treating Physician Progress Report, DWC Form PR-2, as contained in section 9785.2, or in narrative form containing the same information required in the PR-2 form. If a narrative format is used, the document shall be clearly marked at the top that it is a request for authorization. (p) “Retrospective review” means utilization review conducted after medical services have been provided and for which approval has not already been given. (q) “Reviewer” means a medical doctor, doctor of osteopathy, psychologist, acupuncturist, optometrist, dentist, podiatrist, or chiropractic practitioner licensed by any state or the District of Columbia, competent to evaluate the specific clinical issues involved in medical treatment services, where these services are within the scope of the reviewer's practice.

1300-16
(r) “Utilization review plan” means the written plan filed with the Administrative Director pursuant to Labor Code section 4610, setting forth the policies and procedures, and a description of the utilization review process. (s) “Utilization review process” means utilization management functions that prospectively, retrospectively, or concurrently review and approve, modify, delay, or deny, based in whole or in part on medical necessity to cure or relieve, treatment recommendations by physicians, as defined in Labor Code section 3209.3, prior to, retrospectively, or concurrent with the provision of medical treatment services pursuant to Labor Code section 4600. Utilization review does not include determinations of the work-relatedness of injury or disease, or bill review for the purpose of determining whether the medical services were accurately billed. (t) “Written” includes a facsimile as well as communications in paper form. Authority cited: Sections 133, 4603.5, and 5307.3, Labor Code. Reference: Sections 3209.3, 4062, 4600, 4600.4, 4604.5, and 4610, and 4610.5, Labor Code.

1300-17
§ 9792.6.1. Utilization Review Standards—Definitions – On or After January 1, 2013. The following definitions apply to any request for authorization of medical treatment, made under Article 5.5.1 of this Subchapter, for either: (1) an occupational injury or illness occurring on or after January 1, 2013; or (2) where the decision on the request is communicated to the requesting physician on or after July 1, 2013, regardless of the date of injury. (a) “Approval” means a decision that the requested treatment or service is medically appropriate to cure or relieve. (b) “Authorization” means assurance that appropriate reimbursement will be made for an approved specific course of proposed medical treatment to cure or relieve the effects of the industrial injury pursuant to section 4600 of the Labor Code, subject to the provisions of section 5402 of the Labor Code, based on a completed “Request for Authorization for Medical Treatment,” DWC Form RFA, as contained in California Code of Regulations, title 8, section 9785.5, that has been transmitted by the treating physician to the claims administrator. Authorization shall be given pursuant to the timeframe, procedure, and notice requirements of California Code of Regulations, title 8, section 9792.9.1, and may be provided by utilizing the indicated response section of the “Request for Authorization for Medical Treatment,” DWC Form RFA. (c) (1) "Claims Administrator" is a self-administered workers' compensation insurer of an insured employer, a self-administered self-insured employer, a self-administered legally uninsured employer, a self-administered joint powers authority, a third-party claims administrator or other entity subject to Labor Code section 4610, the California Insurance Guarantee Association, and the director of the Department of Industrial Relations as administrator for the Uninsured Employers Benefits Trust Fund (UEBTF). “Claims Administrator” includes any utilization review organization under contract to provide or conduct the claims administrator’s utilization review responsibilities. Unless otherwise indicated by context, “claims administrator” also means the employer. (d) "Concurrent review" means utilization review conducted during an inpatient stay. (e) "Course of treatment" means the course of medical treatment set forth in the treatment plan contained on the "Doctor's First Report of Occupational Injury or Illness," Form DLSR 5021, found at California Code of Regulations, title 8, section 14006, or on the "Primary Treating Physician's Progress Report," DWC Form PR-2, as contained in section 9785.2 or in narrative form containing the same information required in the DWC Form PR-2. (f) “Delay” means a decision by a reviewer that no determination based on medical necessity may be made within the 14-day time limit for the reasons listed in 9792.9.1(f). (g) “Denial” means a decision by a physician reviewer that the requested treatment or service is not medically necessary.

1300-18
(h) “Dispute liability” means an assertion by the claims administrator that a factual or legal basis exists that precludes compensability on the part of the claims administrator for an occupational injury, a claimed injury to any part or parts of the body, or a requested medical treatment. (i) "Emergency health care services" means health care services for a medical condition manifesting itself by acute symptoms of sufficient severity such that the absence of immediate medical attention could reasonably be expected to place the patient's health in serious jeopardy. (j) "Expedited review" means utilization review conducted when the injured worker's condition is such that the injured worker faces an imminent and serious threat to his or her health, including, but not limited to, the potential loss of life, limb, or other major bodily function, or the normal timeframe for the decision-making process would be detrimental to the injured worker's life or health or could jeopardize the injured worker's permanent ability to regain maximum function. (k)"Expert reviewer" means a medical doctor, doctor of osteopathy, psychologist, acupuncturist, optometrist, dentist, podiatrist, or chiropractic practitioner licensed by any state or the District of Columbia, competent to evaluate the specific clinical issues involved in the medical treatment services and where these services are within the individual's scope of practice, who has been consulted by the reviewer or the utilization review medical director to provide specialized review of medical information. (l) "Health care provider" means a provider of medical services, as well as related services or goods, including but not limited to an individual provider or facility, a health care service plan, a health care organization, a member of a preferred provider organization or medical provider network as provided in Labor Code section 4616. (m) "Immediately" means within 24 hours after learning the circumstances that would require an extension of the timeframe for decisions specified, in subdivision (c) and (f)(1) of section 9792.9.1 (n) "Material modification" is when the claims administrator changes utilization review vendor or makes a change to the utilization review standards as specified in section 9792.7. (o) "Medical Director" is the physician and surgeon licensed by the Medical Board of California or the Osteopathic Board of California who holds an unrestricted license to practice medicine in the State of California. The Medical Director is responsible for all decisions made in the utilization review process. (p) "Medical services" means those goods and services provided pursuant to Article 2 (commencing with Labor Code section 4600) of Chapter 2 of Part 2 of Division 4 of the Labor Code. (q) “Medical Treatment Utilization Schedule” means the standards of care adopted by the Administrative Director pursuant to Labor Code section 5307.27 and set forth in Article 5.5.2 of this Subchapter, beginning with section 9792.20.
1300-19
(r) “Modification” means a decision by a physician reviewer that part of the requested treatment or service is not medically necessary. (s) "Prospective review" means any utilization review conducted, except for utilization review conducted during an inpatient stay, prior to the delivery of the requested medical services (t) "Request for authorization" means a written request for a specific course of proposed medical treatment. A request for authorization must be set forth on a “Request for Authorization for Medical Treatment (DWC Form RFA),” completed by a treating physician, as contained in California Code of Regulations, title 8, section 9785.5. “Completed,” for the purpose of this section and for purposes of investigations and penalties, means that information specific to the request has been provided by the requesting treating physician for all fields indicated on the DWC Form RFA. The form must be signed by the physician and may be mailed, faxed or e-mailed. (u) "Retrospective review" means utilization review conducted after medical services have been provided and for which approval has not already been given. (w) "Reviewer" means a medical doctor, doctor of osteopathy, psychologist, acupuncturist, optometrist, dentist, podiatrist, or chiropractic practitioner licensed by any state or the District of Columbia, competent to evaluate the specific clinical issues involved in medical treatment services, where these services are within the scope of the reviewer's practice. (x) "Utilization review plan" means the written plan filed with the Administrative Director pursuant to Labor Code section 4610, setting forth the policies and procedures, and a description of the utilization review process. (y) "Utilization review process" means utilization management functions that prospectively, retrospectively, or concurrently review and approve, modify, delay, or deny, based in whole or in part on medical necessity to cure or relieve, treatment recommendations by physicians, as defined in Labor Code section 3209.3, prior to, retrospectively, or concurrent with the provision of medical treatment services pursuant to Labor Code section 4600. Utilization review does not include determinations of the work-relatedness of injury or disease, or bill review for the purpose of determining whether the medical services were accurately billed. The utilization review process begins when the completed DWC Form RFA is first received by the claims administrator, or in the case of prior authorization, when the treating physician satisfies the conditions described in the utilization review plan for prior authorization. (z) "Written" includes a communication transmitted by facsimile or in paper form. Electronic mail may be used by agreement of the parties. Authority cited: Sections 133, 4603.5, and 5307.3, Labor Code. Reference: Sections 3209.3, 4062, 4600, 4600.4, 4604.5, 4610, and 4610.5, Labor Code.

1300-20
§ 9792.7. Utilization Review Standards—Applicability (a) Effective January 1, 2004, every claims administrator shall establish and maintain a utilization review process for treatment rendered on or after January 1, 2004, regardless of date of injury, in compliance with Labor Code section 4610. Each utilization review process shall be set forth in a utilization review plan which shall contain:
(1) The name, address, phone number, and medical license number of the employed or designated medical director, who holds an unrestricted license to practice medicine in the state of California issued pursuant to section 2050 or section 2450 of the Business and Professions Code.
(2) A description of the process whereby requests for authorization are reviewed, and decisions on such requests are made, and a description of the process for handling expedited reviews.
(3) A description of the specific criteria utilized routinely in the review and throughout the decision-making process, including treatment protocols or standards used in the process. A description of the personnel and other sources used in the development and review of the criteria, and methods for updating the criteria. Prior to and until the Administrative Director adopts a medical treatment utilization schedule pursuant to Labor Code section 5307.27, the written policies and procedures governing the utilization review process shall be consistent with the recommended standards set forth in the American College of Occupational and Environmental Medicine’s Occupational Medicine Practice Guidelines, Second Edition. The Administrative Director incorporates by reference the American College of Occupational and Environmental Medicine’s Occupational Medicine Practice Guidelines (ACOEM), Second Edition (2004), published by OEM Press. A copy may be obtained from OEM Press, 8 West Street, Beverly Farms, Massachusetts 01915 (www.oempress.com). After the Administrative Director adopts a medical treatment utilization schedule pursuant to Labor Code section 5307.27, the written policies and procedures governing the utilization review process shall be consistent with the recommended standards set forth in that schedule.
(4) A description of the qualifications and functions of the personnel involved in decision-making and implementation of the utilization review plan.
(5) A description of the claims administrator’s practice, if applicable, of any prior authorization process, including but not limited to, where authorization is provided without the submission of the request for authorization.
(b) (1) The medical director shall ensure that the process by which the claims administrator
reviews and approves, modifies, delays, or denies requests by physicians prior to, retrospectively, or concurrent with the provision of medical services, complies with Labor Code section 4610 and these implementing regulations.
(2) A reviewer who is competent to evaluate the specific clinical issues involved in the medical treatment services, and where these services are within the reviewer’s scope of practice, may, except as indicated below, delay, modify or deny, requests for authorization of medical treatment for reasons of medical necessity to cure or relieve the effects of the industrial injury.
1300-21
(3) A non-physician reviewer may be used to initially apply specified criteria to requests for authorization for medical services. A non-physician reviewer may approve requests for authorization of medical services. A non-physician reviewer may discuss applicable criteria with the requesting physician, should the treatment for which authorization is sought appear to be inconsistent with the criteria. In such instances, the requesting physician may voluntarily withdraw a portion or all of the treatment in question and submit an amended request for treatment authorization, and the non-physician reviewer may approve the amended request for treatment authorization. Additionally, a non-physician reviewer may reasonably request appropriate additional information that is necessary to render a decision but in no event shall this exceed the time limitations imposed in section 9792.9 subdivisions (b)(1), (b)(2) or (c). Any time beyond the time specified in these paragraphs is subject to the provisions of subdivision (g)(1)(A) through (g)(1)(C) of section 9792.9.
(c) The complete utilization review plan, consisting of the policies and procedures, and a description of the utilization review process, shall be filed by the claims administrator, or by the external utilization review organization contracted by the claims administrator to perform the utilization review, with the Administrative Director. In lieu of filing the utilization review plan, the claims administrator may submit a letter identifying the external utilization review organization which has been contracted to perform the utilization review functions, provided that the utilization review organization has filed a complete utilization review plan with the Administrative Director. A modified utilization review plan shall be filed with the Administrative Director within 30 calendar days after the claims administrator makes a material modification to the plan. (d) Upon request by the public, the claims administrator shall make available the complete utilization review plan, consisting of the policies and procedures, and a description of the utilization review process.
(1) The claims administrator may make available the complete utilization review plan, consisting of the policies and procedures and a description of the utilization review process, through electronic means. If a member of the public requests a hard copy of the utilization review plan, the claims administrator may charge reasonable copying and postage expenses related to disclosing the complete utilization review plan. Such charge shall not exceed $0.25 per page plus actual postage costs.
Authority: Sections 133, 4603.5, and 5307.3, Labor Code. Reference: Sections 4062, 4600, 4600.4, 4604.5, and 4610, Labor Code.
1300-22
§ 9792.8. Utilization Review Standards—Medically-Based Criteria (a) (1) The criteria shall be consistent with the schedule for medical treatment utilization
adopted pursuant to Labor Code section 5307.27. Prior to adoption of the schedule, the criteria or guidelines used in the utilization review process shall be consistent with the American College of Occupational and Environmental Medicine’s (ACOEM) Practice Guidelines, Second Edition. The guidelines set forth in the ACOEM Practice Guidelines shall be presumptively correct on the issue of extent and scope of medical treatment until the effective date of the utilization schedule adopted pursuant to Labor Code section 5307.27. The presumption is rebuttable and may be controverted by a preponderance of the scientific medical evidence establishing that a variance from the guidelines is reasonably required to cure or relieve the injured worker from the effects of his or her injury.
(2) For all conditions or injuries not addressed by the ACOEM Practice Guidelines or by the official utilization schedule after adoption pursuant to Labor Code section 5307.27, authorized treatment shall be in accordance with other evidence-based medical treatment guidelines that are generally recognized by the national medical community and are scientifically based. Treatment may not be denied on the sole basis that the treatment is not addressed by the ACOEM Practice Guidelines until adoption of the medical treatment utilization schedule pursuant to Labor Code section 5307.27. After the Administrative Director adopts a medical treatment utilization schedule pursuant to Labor Code section 5307.27, treatment may not be denied on the sole basis that the treatment is not addressed by that schedule.
(3) The relevant portion of the criteria or guidelines used shall be disclosed in written form to the requesting physician, the injured worker, and if the injured worker is represented by counsel, the injured worker’s attorney, if used as the basis of a decision to modify, delay, or deny services in a specific case under review. The claims administrator may not charge an injured worker, the injured worker’s attorney or the requesting physician for a copy of the relevant portion of the criteria or guidelines used to modify, delay or deny the treatment request.
(4) Nothing in this section precludes authorization of medical treatment not included in the specific criteria under section 9792.8(a)(3).
Authority: Sections 133, 4603.5, and 5307.3, Labor Code. Reference: Sections 4062, 4600, 4600.4, 4604.5, and 4610, Labor Code.

1300-23
§9792.9. Utilization Review Standards--Timeframe, Procedures and Notice Content – For Utilization Review Decisions Issued Prior to July 1, 2013 for Injuries Occurring Prior to January 1, 2013. This section applies to any request for authorization of medical treatment, made under Article 5.5.1 of this Subchapter, for an occupational injury or illness occurring prior to January 1, 2013 if the decision on the request is communicated to the requesting physician prior to July 1, 2013. (a) The request for authorization for a course of treatment as defined in section 9792.6(e) must be in written form.
(1) For purposes of this section, the written request for authorization shall be deemed to have been received by the claims administrator by facsimile on the date the request was received if the receiving facsimile electronically date stamps the transmission. If there is no electronically stamped date recorded, then the date the request was transmitted. A request for authorization transmitted by facsimile after 5:30 PM Pacific Time shall be deemed to have been received by the claims administrator on the following business day as defined in Labor Code section 4600.4 and in section 9 of the Civil Code. The copy of the request for authorization received by a facsimile transmission shall bear a notation of the date, time and place of transmission and the facsimile telephone number to which the request was transmitted or be accompanied by an unsigned copy of the affidavit or certificate of transmission which shall contain the facsimile telephone number to which the request was transmitted. The requesting physician must indicate the need for an expedited review upon submission of the request.
(2) Where the request for authorization is made by mail, and a proof of service by mail exists, the request shall be deemed to have been received by the claims administrator five (5) days after the deposit in the mail at a facility regularly maintained by the United States Postal Service. Where the request for authorization is delivered via certified mail, return receipt mail, the request shall be deemed to have been received by the claims administrator on the receipt date entered on the return receipt. In the absence of a proof of service by mail or a dated return receipt, the request shall be deemed to have been received by the claims administrator on the date stamped as received on the document.
(b) Utilization review of a request for authorization of medical treatment may be deferred if the claims administrator disputes liability for either the occupational injury for which the treatment is recommended or the recommended treatment itself on grounds other than medical necessity.
(1) If the claims administrator disputes its liability for the requested medical treatment under this subdivision, it may, no later than five (5) business days from receipt of the request for authorization, issue a written decision deferring utilization review of the requested treatment. The written decision must be sent to the requesting physician, the injured worker, and if the injured worker is represented by counsel, the injured worker's attorney. The written decision shall only contain the following information specific to the request: (A) The date on which the request for authorization was first received. (B) A description of the specific course of proposed medical treatment for which
authorization was requested.

1300-24
(C) A clear, concise, and appropriate explanation of the reason for the claims administrator’s dispute of liability for either the injury, claimed body part or parts, or the recommended treatment.
(D) A plain language statement advising the injured employee that any dispute under this subdivision shall be resolved either by agreement of the parties or through the dispute resolution process of the Workers’ Compensation Appeals Board.
(E) The following mandatory language advising the injured employee: “You have a right to disagree with decisions affecting your claim. If you have questions
about the information in this notice, please call me (insert claims adjuster’s name in parentheses) at (insert telephone number). However, if you are represented by an attorney, please contact your attorney instead of me.” and “For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-free 1-800-736-7401.”
(2) If utilization review is deferred pursuant to this subdivision, and it is finally determined that the claims administrator is liable for treatment of the condition for which treatment is recommended, the time for the claims administrator to conduct retrospective utilization review in accordance with this section shall begin on the date the determination of the claims administrator’s liability becomes final. The time for the claims administrator to conduct prospective utilization review shall commence from the date of the claims administrator’s receipt of a request for authorization after the final determination of liability.
(c) The utilization review process shall meet the following timeframe requirements:
(1) Prospective or concurrent decisions shall be made in a timely fashion that is appropriate for the nature of the injured worker's condition, not to exceed five (5) working days from the date of receipt of the written request for authorization.
(2) If appropriate information which is necessary to render a decision is not provided with the original request for authorization, such information may be requested by a reviewer or non-physician reviewer within five (5) working days from the date of receipt of the written request for authorization to make the proper determination. In no event shall the determination be made more than 14 days from the date of receipt of the original request for authorization by the health care provider. (A) If the reasonable information requested by the claims administrator is not received
within 14 days of the date of the original written request by the requesting physician, a reviewer may deny the request with the stated condition that the request will be reconsidered upon receipt of the information requested.
(3) Decisions to approve a physician's request for authorization prior to, or concurrent with, the provision of medical services to the injured worker shall be communicated to the requesting physician within 24 hours of the decision. Any decision to approve a request shall be communicated to the requesting physician initially by telephone or facsimile. The communication by telephone shall be followed by written notice to the requesting physician within 24 hours of the decision for concurrent review and within two business days for prospective review.
1300-25
(4) Decisions to modify, delay or deny a physician's request for authorization prior to, or concurrent with the provision of medical services to the injured worker shall be communicated to the requesting physician initially by telephone or facsimile. The communication by telephone shall be followed by written notice to the requesting physician, the injured worker, and if the injured worker is represented by counsel, the injured worker's attorney within 24 hours of the decision for concurrent review and within two business days of the decision for prospective review. In addition, the non-physician provider of goods or services identified in the request for authorization, and for whom contact information has been included, shall be notified in writing of the decision modifying, delaying, or denying a request for authorization that shall not include the rationale, criteria or guidelines used for the decision.
(5) For purposes of this section “normal business day” means a business day as defined in Labor Code section 4600.4 and Civil Code section 9.
(d) When review is retrospective, decisions shall be communicated to the requesting physician who provided the medical services and to the individual who received the medical services, and his or her attorney/designee, if applicable, within 30 days of receipt of the medical information that is reasonably necessary to make this determination. In addition, the non-physician provider of goods or services identified in the request for authorization, and for whom contact information has been included, shall be notified in writing of the decision modifying, delaying, or denying a request for authorization that shall not include the rationale, criteria or guidelines used for the decision. (e) Failure to obtain prior authorization for emergency health care services shall not be an acceptable basis for refusal to cover medical services provided to treat and stabilize an injured worker presenting for emergency health care services. Emergency health care services, however, may be subjected to retrospective review. Documentation for emergency health care services shall be made available to the claims administrator upon request. (f) Prospective or concurrent decisions related to an expedited review shall be made in a timely fashion appropriate to the injured worker's condition, not to exceed 72 hours after the receipt of the written information reasonably necessary to make the determination. The requesting physician must indicate the need for an expedited review upon submission of the request. Decisions related to expedited review refer to the following situations:
(1) When the injured worker's condition is such that the injured worker faces an imminent and serious threat to his or her health, including, but not limited to, the potential loss of life, limb, or other major bodily function, or
(2) The normal timeframe for the decision-making process, as described in subdivision (b), would be detrimental to the injured worker's life or health or could jeopardize the injured worker's permanent ability to regain maximum function.
(g) The review and decision to deny, delay or modify a request for medical treatment must be conducted by a reviewer, who is competent to evaluate the specific clinical issues involved in the medical treatment services, and where these services are within the scope of the individual's practice.

1300-26
(h) (1) The timeframe for decisions specified in subdivisions (b)(1), (b)(2) or (c) may only be extended by the claims administrator under the following circumstances: (A) The claims administrator is not in receipt of all of the necessary medical information
reasonably requested. (B) The reviewer has asked that an additional examination or test be performed upon the
injured worker that is reasonable and consistent with professionally recognized standards of medical practice.
(C) The claims administrator needs a specialized consultation and review of medical information by an expert reviewer.
(2) If subdivisions (A), (B) or (C) above apply, the claims administrator shall immediately notify the requesting physician, the injured worker, and if the injured worker is represented by counsel, the injured worker's attorney in writing, that the claims administrator cannot make a decision within the required timeframe, and specify the information requested but not received, the additional examinations or tests required, or the specialty of the expert reviewer to be consulted. The claims administrator shall also notify the requesting physician, the injured worker, and if the injured worker is represented by counsel, the injured worker's attorney of the anticipated date on which a decision will be rendered. This notice shall include a statement that if the injured worker believes that a bona fide dispute exists relating to his or her entitlement to medical treatment, the injured worker or the injured worker's attorney may file an Application for Adjudication of Claim, Form WCAB 1, and a Declaration of Readiness to Proceed (expedited trial), DWC-CA form 10252.1. In addition, the non-physician provider of goods or services identified in the request for authorization, and for whom contact information has been included, shall be notified in writing of the decision to extend the timeframe and the anticipated date on which the decision will be rendered in accordance with this subdivision. The written notification shall not include the rationale, criteria or guidelines used for the decision.
(3) Upon receipt of information pursuant to subdivisions (A), (B), or (C) above, and (b)(2)(A), the claims administrator shall make the decision to approve, and the reviewer shall make a decision to modify or deny the request for authorization within five (5) working days of receipt of the information for prospective or concurrent review. The decision shall be communicated pursuant to subdivisions (b)(3) or (b)(4).
(4) Upon receipt of information pursuant to subdivisions (A), (B), or (C) above, the claims administrator shall make the decision to approve, and the reviewer shall make a decision to modify or deny the request for authorization within thirty (30) days of receipt of the information for retrospective review.
(i) Every claims administrator shall maintain telephone access from 9:00 AM to 5:30 PM Pacific Time, on normal business days, for health care providers to request authorization for medical services. Every claims administrator shall have a facsimile number available for physicians to request authorization for medical services. Every claims administrator shall maintain a process to receive communications from health care providers requesting authorization for medical services after business hours. For purposes of this section “normal business day” means a business day as defined in Labor Code section 4600.4 and Civil Code section 9. In addition, for purposes of this section the requirement that the claims administrator maintain a process to receive

1300-27
communications from requesting physicians after business hours shall be satisfied by maintaining a voice mail system or a facsimile number for after business hours requests. (j) A written decision approving a request for treatment authorization under this section shall specify the specific medical treatment service approved. (k) A written decision modifying, delaying or denying treatment authorization under this section, sent prior to July 1, 2013, shall be provided to the requesting physician, the injured worker, and if the injured worker is represented by counsel, the injured worker's attorney and shall contain the following information:
(1) The date on which the decision is made. (2) A description of the specific course of proposed medical treatment for which
authorization was requested. (3) A specific description of the medical treatment service approved, if any. (4) A clear and concise explanation of the reasons for the claims administrator's decision. (5) A description of the medical criteria or guidelines used pursuant to section 9792.8,
subdivision (a)(3). (6) The clinical reasons regarding medical necessity. (7) A clear statement that any dispute shall be resolved in accordance with the provisions of
Labor Code section 4062, and that an objection to the utilization review decision must be communicated by the injured worker or the injured worker's attorney on behalf of the injured worker to the claims administrator in writing within 20 days of receipt of the decision. It shall further state that the 20-day time limit may be extended for good cause or by mutual agreement of the parties. The letter shall further state that the injured worker may file an Application for Adjudication of Claim, Form WCAB 1, and a Declaration of Readiness to Proceed (expedited trial), DWC-CA form 10252.1.
(8) (A) Include the following mandatory language: Either “If you want further information, you may contact the local state Information and Assistance office by calling [enter district I & A office telephone number closest to the injured worker] or you may receive recorded information by calling 1-800-736-7401. or “If you want further information, you may contact the local state Information and Assistance office closest to you. Please see attached listing (attach a listing of I&A offices and telephone numbers) or you may receive recorded information by calling 1-800-736-7401.” and “You may also consult an attorney of your choice. Should you decide to be represented by an attorney, you may or may not receive a larger award, but, unless you are determined to be ineligible for an award, the attorney's fee will be deducted from any award you might receive for disability benefits. The decision to be represented by an
1300-28
attorney is yours to make, but it is voluntary and may not be necessary for you to receive your benefits.” (B) Instead of the mandatory language stated in subdivision (k)(8)(A), the following
language may be used: “You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me (insert claims adjuster’s name in parentheses) at (insert telephone number). However, if you are represented by an attorney, please contact your attorney instead of me. and “For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-free 1-800-736-7401.” In addition, the non-physician provider of goods or services identified in the request for authorization, and for whom contact information has been included, shall be notified in writing of the decision modifying, delaying, or denying a request for authorization that shall not include the rationale, criteria or guidelines used for the decision.
(9) Details about the claims administrator's internal utilization review appeals process, if any, and a clear statement that the appeals process is on a voluntary basis, including the following mandatory statement: “If you disagree with the utilization review decision and wish to dispute it, you must send written notice of your objection to the claims administrator within 20 days of receipt of the utilization review decision in accordance with Labor Code section 4062. You must meet this deadline even if you are participating in the claims administrator's internal utilization review appeals process.”
(l) A written decision modifying, delaying or denying treatment authorization under this section, sent on or after July 1, 2013, shall be provided to the requesting physician, the injured worker, and if the injured worker is represented by counsel, the injured worker's attorney and shall contain the following information:
(1) The date on which the decision is made. (2) A description of the specific course of proposed medical treatment for which
authorization was requested. (3) A list of all medical records reviewed. (4) A specific description of the medical treatment service approved, if any. (5) A clear, concise, and appropriate explanation of the reasons for the claims administrator’s
decision, including the clinical reasons regarding medical necessity and a description of the relevant medical criteria or guidelines used to reach the decision pursuant to section 9792.8. If a utilization review decision to modify, deny or delay a medical service is due to incomplete or insufficient information, the decision shall specify the reason for the decision and specify the information that is needed.

1300-29
(6) The Application for Independent Medical Review, DWC Form IMR, with all fields, except for the signature of the employee, to be completed by the claims administrator. The application, set forth at section 9792.10.1, shall include an addressed envelope, which may be postage-paid for mailing to the Administrative Director or his or her designee.
(7) A clear statement advising the injured employee that any dispute shall be resolved in accordance with the independent medical review provisions of Labor Code section 4610.5 and 4610.6, and that an objection to the utilization review decision must be communicated by the injured worker, the injured worker’s representative, or the injured worker's attorney on behalf of the injured worker on the enclosed Application for Independent Medical Review, DWC Form IMR, within 30 calendar days of receipt of the decision.
(8) Include the following mandatory language advising the injured employee: “You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me (insert claims adjuster’s name in parentheses) at (insert telephone number). However, if you are represented by an attorney, please contact your attorney instead of me. and “For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-free 1-800-736-7401.”
(9) Details about the claims administrator's internal utilization review appeals process for the requesting physician, if any, and a clear statement that the internal appeals process is a voluntary process that neither triggers nor bars use of the dispute resolution procedures of Labor Code section 4610.5 and 4610.6, but may be pursued on an optional basis.
(m) The written decision modifying, delaying or denying treatment authorization provided to the requesting physician shall also contain the name and specialty of the reviewer or expert reviewer, and the telephone number in the United States of the reviewer or expert reviewer. The written decision shall also disclose the hours of availability of either the review, the expert reviewer or the medical director for the treating physician to discuss the decision which shall be, at a minimum, four (4) hours per week during normal business hours, 9:00 AM to 5:30 PM., Pacific Time or an agreed upon scheduled time to discuss the decision with the requesting physician. In the event the reviewer is unavailable, the requesting physician may discuss the written decision with another reviewer who is competent to evaluate the specific clinical issues involved in the medical treatment services. (n) Authorization may not be denied on the basis of lack of information without documentation reflecting an attempt to obtain the necessary information from the physician or from the provider of goods or services identified in the request for authorization either by facsimile or mail. (o) A utilization review decision to modify, delay, or deny a request for authorization of medical treatment shall remain effective for 12 months from the date of the decision without further

1300-30
action by the claims administrator with regard to any further recommendation by the same physician for the same treatment unless the further recommendation is supported by a documented change in the facts material to the basis of the utilization review decision. Authority: Sections 133, 4603.5 and 5307.3, Labor Code. Reference: Sections 4062, 4600, 4600.4, 4604.5, 4610, and 4610.5, Labor Code.
1300-31
§9792.9.1. Utilization Review Standards--Timeframe, Procedures and Notice – On or After January 1, 2013. This section applies to any request for authorization of medical treatment, made under Article 5.5.1 of this Subchapter, for either: (1) an occupational injury or illness occurring on or after January 1, 2013; or (2) where the decision on the request is communicated to the requesting physician on or after July 1, 2013, regardless of the date of injury. (a) The request for authorization for a course of treatment as defined in section 9792.6.1(e) must be in written form set forth on the “Request for Authorization for Medical Treatment (DWC Form RFA),” as contained in California Code of Regulations, title 8, section 9785.5.
(1) For purposes of this section, the DWC Form RFA shall be deemed to have been received by the claims administrator or its utilization review organization by facsimile or by electronic mail on the date the form was received if the receiving facsimile or electronic mail address electronically date stamps the transmission when received. If there is no electronically stamped date recorded, then the date the form was transmitted shall be deemed to be the date the form was received by the claims administrator or the claims administrator’s utilization review organization. A DWC Form RFA transmitted by facsimile after 5:30 PM Pacific Time shall be deemed to have been received by the claims administrator on the following business day, except in the case of an expedited or concurrent review. The copy of the DWC Form RFA or the cover sheet accompanying the form transmitted by a facsimile transmission or by electronic mail shall bear a notation of the date, time and place of transmission and the facsimile telephone number or the electronic mail address to which the form was transmitted or the form shall be accompanied by an unsigned copy of the affidavit or certificate of transmission, or by a fax or electronic mail transmission report, which shall display either the facsimile telephone number to which the form was transmitted. The requesting physician must indicate if there is the need for an expedited review on the DWC Form RFA.
(2) (A) Where the DWC Form RFA is sent by mail, the form, absent documentation of receipt, shall be deemed to have been received by the claims administrator five (5) business days after the deposit in the mail at a facility regularly maintained by the United States Postal Service.
(B) Where the DWC Form RFA is delivered via certified mail, with return receipt mail, the form, absent documentation of receipt, shall be deemed to have been received by the claims administrator on the receipt date entered on the return receipt.
(C) In the absence of documentation of receipt, evidence of mailing, or a dated return receipt, the DWC Form RFA shall be deemed to have been received by the claims administrator five days after the latest date the sender wrote on the document.
(3) Every claims administrator shall maintain telephone access and have a representative personally available by telephone from 9:00 AM to 5:30 PM Pacific Time, on business days for health care providers to request authorization for medical services. Every claims administrator shall have a facsimile number available for physicians to request authorization for medical services. Every claims administrator shall maintain a process to receive communications from health care providers requesting authorization for medical services after business hours. For purposes of this section the requirement that the claims administrator maintain a process to receive communications from requesting physicians
1300-32
after business hours shall be satisfied by maintaining a voice mail system or a facsimile number or a designated email address for after business hours requests.
(b) Utilization review of a medical treatment request made on the DWC Form RFA may be deferred if the claims administrator disputes liability for either the occupational injury for which the treatment is recommended or the recommended treatment itself on grounds other than medical necessity.
(1) If the claims administrator disputes liability under this subdivision, it may, no later than five (5) business days from receipt of the DWC Form RFA, issue a written decision deferring utilization review of the requested treatment. The written decision must be sent to the requesting physician, the injured worker, and if the injured worker is represented by counsel, the injured worker's attorney. The written decision shall only contain the following information specific to the request: (A) The date on which the DWC Form RFA was first received. (B) A description of the specific course of proposed medical treatment for which
authorization was requested. (C) A clear, concise, and appropriate explanation of the reason for the claims
administrator’s dispute of liability for either the injury, claimed body part or parts, or the recommended treatment.
(D) A plain language statement advising the injured employee that any dispute under this subdivision shall be resolved either by agreement of the parties or through the dispute resolution process of the Workers’ Compensation Appeals Board.
(E) The following mandatory language advising the injured employee: “You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me (insert claims adjuster’s name in parentheses) at (insert telephone number). However, if you are represented by an attorney, please contact your attorney instead of me. and “For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-free 1-800-736-7401.”
(2) If utilization review is deferred pursuant to this subdivision, and it is finally determined that the claims administrator is liable for treatment of the condition for which treatment is recommended, the time for the claims administrator to conduct retrospective utilization review in accordance with this section shall begin on the date the determination of the claims administrator’s liability becomes final. The time for the claims administrator to conduct prospective utilization review shall commence from the date of the claims administrator’s receipt of a DWC Form RFA after the final determination of liability.
(c) The utilization review process shall meet the following timeframe requirements:
(1) The first day in counting any timeframe requirement is the day after the receipt of the DWC Form RFA, except when the timeline is measured in hours. Whenever the

1300-33
timeframe requirement is stated in hours, the time for compliance is counted in hours from the time of receipt of the DWC Form RFA.
(2) If the DWC Form RFA is not completed as defined in section 9792.6.1(t), a non-physician reviewer or reviewer may either treat the form as complete and comply with the timeframes for decision set forth in this section or return it to the requesting physician marked “not complete” no later than five (5) business days from receipt. The timeframe for a decision on that returned request for authorization shall begin anew upon receipt of a completed DWC Form RFA.
(3) Prospective or concurrent decisions to approve, modify, delay, or deny a request for authorization shall be made in a timely fashion that is appropriate for the nature of the injured worker's condition, not to exceed five (5) business days from the date of receipt of the completed DWC Form RFA, but in no event more than 14 calendar days from initial receipt of the complete DWC Form RFA. (A) Prospective or concurrent decisions to approve, modify, delay, or deny a request for
authorization related to an expedited review shall be made in a timely fashion appropriate to the injured worker's condition, not to exceed 72 hours after the receipt of the written information reasonably necessary to make the determination. The requesting physician must certify the need for an expedited review upon submission of the request.
(B) If appropriate information which is necessary to render a decision is not provided with the original request for authorization, such information may be requested by a reviewer or non-physician reviewer within five (5) business days from the date of receipt of the DWC Form RFA to make the proper determination.
(C) If the reasonable information requested by a reviewer or non-physician reviewer within five (5) business days from the date of receipt of the completed DWC Form RFA is not received within 14 days from receipt of the completed DWC Form RFA, the reviewer may deny the request with the stated condition that the request will be reconsidered upon receipt of the information requested, or the reviewer may issue a decision to delay as provided in subdivision (f)(1)(A).
(4) Retrospective decisions to approve modify, delay, or deny a request for authorization shall be made within 30 days of receipt of the medical information that is reasonably necessary to make this determination.
(d) Decisions to approve a request for authorization.
(1) All decisions to approve a request for authorization set forth in a DWC Form RFA shall specify the specific medical treatment service requested, the specific medical treatment service approved, and the date of the decision.
(2) For prospective, concurrent, or expedited review, approvals shall be communicated to the requesting physician within 24 hours of the decision, and shall be communicated to the requesting physician initially by telephone, facsimile, or electronic mail. The communication by telephone shall be followed by written notice to the requesting physician within 24 hours of the decision for concurrent review and within two (2) business days for prospective review.
(3)(A) For retrospective review, a written decision to approve shall be communicated to the requesting physician who provided the medical services and to the individual who received the medical services, and his or her attorney/designee, if applicable.

1300-34
(B) Payment, or partial payment consistent with the provisions of California Code of Regulations, title 8, section 9792.5, of a medical bill for services requested on the DWC Form RFA, within the 30-day timeframe set forth in subdivision (c)(4), shall be deemed a retrospective approval, even if a portion of the medical bill for the requested services is contested, denied, or considered incomplete. A document indicating that a payment has been made for the requested services, such as an explanation of review, may be provided to the injured employee who received the medical services, and his or her attorney/designee, if applicable, in lieu of a communication expressly acknowledging the retrospective approval.
(e) Decisions to modify, delay, or deny a request for authorization.
(1) The review and decision to deny, delay, or modify a request for medical treatment must be conducted by a reviewer, who is competent to evaluate the specific clinical issues involved in the medical treatment services, and where these services are within the scope of the individual's practice.
(2) Failure to obtain authorization prior to providing emergency health care services shall not be an acceptable basis for refusal to cover medical services provided to treat and stabilize an injured worker presenting for emergency health care services. Emergency health care services may be subjected to retrospective review. Documentation for emergency health care services shall be made available to the claims administrator upon request.
(3) For prospective, concurrent, or expedited review, a decision to modify, delay, or deny shall be communicated to the requesting physician within 24 hours of the decision, and shall be communicated to the requesting physician initially by telephone, facsimile, or electronic mail. The communication by telephone shall be followed by written notice to the requesting physician within 24 hours of the decision for concurrent review and within two (2) business days for prospective review and for expedited review within 72 hours of receipt of the request.
(4) For retrospective review, a written decision to deny part or all of the requested medical treatment shall be communicated to the requesting physician who provided the medical services and to the individual who received the medical services, and his or her attorney/designee, if applicable, within 30 days of receipt of information that is reasonably necessary to make this determination.
(5) The written decision modifying, delaying or denying treatment authorization shall be provided to the requesting physician, the injured worker, the injured worker’s representative, and if the injured worker is represented by counsel, the injured worker's attorney and shall only contain the following information specific to the request: (A) The date on which the DWC Form RFA was first received. (B) The date on which the decision is made. (C) A description of the specific course of proposed medical treatment for which
authorization was requested. (D) A list of all medical records reviewed. (E) A specific description of the medical treatment service approved, if any. (F) A clear, concise, and appropriate explanation of the reasons for the reviewing
physician’s decision, including the clinical reasons regarding medical necessity and a description of the relevant medical criteria or guidelines used to reach the decision pursuant to section 9792.8. If a utilization review decision to modify, deny or delay a
1300-35
medical service is due to incomplete or insufficient information, the decision shall specify the reason for the decision and specify the information that is needed.
(G) The Application for Independent Medical Review, DWC Form IMR, with all fields, except for the signature of the employee, to be completed by the claims administrator. The application, set forth at section 9792.10.1, shall include an addressed envelope, which may be postage-paid for mailing to the Administrative Director or his or her designee.
(H) A clear statement advising the injured employee that any dispute shall be resolved in accordance with the independent medical review provisions of Labor Code section 4610.5 and 4610.6, and that an objection to the utilization review decision must be communicated by the injured worker, the injured worker’s representative, or the injured worker's attorney on behalf of the injured worker on the enclosed Application for Independent Medical Review, DWC Form IMR, within 30 calendar days of receipt of the decision.
(I) Include the following mandatory language advising the injured employee: “You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me (insert claims adjuster’s name in parentheses) at (insert telephone number). However, if you are represented by an attorney, please contact your attorney instead of me. and “For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-free 1-800-736-7401.”
(J) Details about the claims administrator's internal utilization review appeals process for the requesting physician, if any, and a clear statement that the internal appeals process is voluntary process that neither triggers nor bars use of the dispute resolution procedures of Labor Code section 4610.5 and 4610.6, but may be pursued on an optional basis.
(K) The written decision modifying, delaying or denying treatment authorization provided to the requesting physician shall also contain the name and specialty of the reviewer or expert reviewer, and the telephone number in the United States of the reviewer or expert reviewer. The written decision shall also disclose the hours of availability of either the reviewer, the expert reviewer or the medical director for the treating physician to discuss the decision which shall be, at a minimum, four (4) hours per week during normal business hours, 9:00 AM to 5:30 PM., Pacific Time or an agreed upon scheduled time to discuss the decision with the requesting physician. In the event the reviewer is unavailable, the requesting physician may discuss the written decision with another reviewer who is competent to evaluate the specific clinical issues involved in the medical treatment services.
(f)(1) The timeframe for decisions specified in subdivision (c) may only be extended with a
written notice of delay by the reviewer under one or more of the following circumstances:
1300-36
(A) The reviewer is not in receipt of all of the necessary medical information reasonably requested.
(B) The reviewer has asked that an additional examination or test be performed upon the injured worker that is reasonable and consistent with professionally recognized standards of medical practice.
(C) The reviewer needs a specialized consultation and review of medical information by an expert reviewer.
(2) If subdivisions (f)(1)(A), (B) or (C) above apply, the reviewer shall immediately notify the requesting physician, the injured worker, and if the injured worker is represented by counsel, the injured worker's attorney in writing, that the reviewer cannot make a decision within the required timeframe, and specify the information requested but not received, the additional examinations or tests required, or the specialty of the expert reviewer to be consulted. The reviewer shall also notify the requesting physician, the injured worker, and if the injured worker is represented by counsel, the injured worker's attorney of the anticipated date on which a decision will be rendered
(3) Upon receipt of the information requested pursuant to subdivisions (f)(1)(A), (B), or (C), the claims administrator or reviewer, for prospective or concurrent review, shall make the decision to approve, modify, or deny the request for authorization within five (5) business days of receipt of the information. The requesting physician shall be notified by telephone, facsimile or electronic mail within 24 hours of making the decision The written decision shall include the date the information was received and the decision shall be communicated in the manner set out in section 9792.9.1(d) or (e), whichever is applicable.
(4) Upon receipt of the information requested pursuant to subdivisions (f)(1)(A), (B), or (C), the claims administrator or reviewer, for prospective or concurrent decisions related to an expedited review, shall make the decision to approve, modify, or deny the request for authorization within 72 hours of receipt of the information. The requesting physician shall be notified by telephone, facsimile or electronic mail within 24 hours of making the decision. The written notice of decision shall include the date the requested information was received and be communicated pursuant to subdivisions (d)(2) or (e)(3), whichever is applicable.
(5) Upon receipt of the information requested pursuant to subdivisions (f)(1)(A), (B), or (C), the claims administrator or reviewer, for retrospective review, shall make the decision to approve, modify, delay, or deny the request for authorization within thirty (30) calendar days of receipt of the information requested. The decision shall include the date it was made and be communicated pursuant to subdivisions (d)(3) or (e)(4), whichever is applicable.
(g) Whenever a reviewer issues a decision to deny a request for authorization based on the lack of medical information necessary to make a determination, the claims administrator’s file must document the attempt by the claims administrator or reviewer to obtain the necessary medical information from the physician either by facsimile, mail, or e-mail. (h) A utilization review decision to modify, delay, or deny a request for authorization of medical treatment shall remain effective for 12 months from the date of the decision without further action by the claims administrator with regard to any further recommendation by the same

1300-37
physician for the same treatment unless the further recommendation is supported by a documented change in the facts material to the basis of the utilization review decision. Authority: Sections 133, 4603.5 and 5307.3, Labor Code. Reference: Sections 4062, 4600, 4600.4, 4604.5, 4610, and 4610.5, Labor Code.
1300-38
§9792.10. Utilization Review Standards--Dispute Resolution– For Utilization Review Decisions Issued Prior to July 1, 2013 for Injuries Occurring Prior to January 1, 2013. This section applies to any request for authorization of medical treatment, made under Article 5.5.1 of this Subchapter, for an occupational injury or illness occurring prior to January 1, 2013 if the decision on the request is communicated to the requesting physician prior to July 1, 2013. (a)(1) If the request for authorization of medical treatment is not approved, or if the request for
authorization for medical treatment is approved in part, any dispute shall be resolved in accordance with Labor Code section 4062.
(2) An objection to a decision disapproving in whole or in part a request for authorization of medical treatment, must be communicated to the claims administrator by the injured worker or the injured worker's attorney in writing within 20 days of receipt of the utilization review decision. The 20-day time limit may be extended for good cause or by mutual agreement of the parties.
(3) Nothing in this paragraph precludes the parties from participating in an internal utilization review appeal process on a voluntary basis provided the injured worker and if the injured worker is represented by counsel, the injured worker's attorney have been notified of the 20-day time limit to file an objection to the utilization review decision in accordance with Labor Code section 4062.
(4) Additionally, the injured worker or the injured worker's attorney may file an Application for Adjudication of Claim, Form WCAB 1, and a Declaration of Readiness to Proceed (expedited trial), DWC-CA form 10252.1, and request an expedited hearing and decision on his or her entitlement to medical treatment if the request for medical treatment is not authorized within the time limitations set forth in section 9792.9, or when there exists a bona fide dispute as to entitlement to medical treatment.
(b) The following requirements shall be met prior to a concurrent review decision to deny authorization for medical treatment and to resolve disputes:
(1) In the case of concurrent review, medical care shall not be discontinued until the requesting physician has been notified of the decision and a care plan has been agreed upon by the requesting physician that is appropriate for the medical needs of the injured worker. In addition, the non-physician provider of goods or services identified in the request for authorization, and for whom contact information has been included, shall be notified in writing of the decision modifying, delaying, or denying a request for authorization that shall not include the rationale, criteria or guidelines used for the decision.
(2) Medical care provided during a concurrent review shall be medical treatment that is reasonably required to cure or relieve from the effects of the industrial injury.
Authority: Sections 133, 4603.5 and 5307.3, Labor Code. Reference: Sections 4062, 4600, 4600.4, 4604.5, 4610, and 4610.5, Labor Code.

1300-39
§ 9792.10.1. Utilization Review Standards--Dispute Resolution – On or After January 1, 2013. This section applies to any request for authorization of medical treatment, made under Article 5.5.1 of this Subchapter, for either: (1) an occupational injury or illness occurring on or after January 1, 2013; or (2) where the decision on the request is communicated to the requesting physician on or after July 1, 2013, regardless of the date of injury. (a) For the purpose of independent medical review under sections 9792.10.1 through 9792.10.9 of this Article, the following definitions apply:
(1) "Claims Administrator" is a self-administered workers' compensation insurer of an insured employer, a self-administered self-insured employer, a self-administered legally uninsured employer, a self-administered joint powers authority, a third-party claims administrator or other entity subject to Labor Code section 4610, the California Insurance Guarantee Association, and the director of the Department of Industrial Relations as administrator for the Uninsured Employers Benefits Trust Fund (UEBTF). “Claims Administrator” includes any utilization review organization under contract to provide or conduct the claims administrator’s utilization review responsibilities. Unless otherwise indicated by context, “claims administrator” also means the employer.
(2) “Disputed medical treatment” means medical treatment that has been modified, delayed, or denied by a utilization review decision.
(3) “Expedited review” means independent medical review conducted when the employee’s condition is such that the employee faces an imminent and serious threat to his or her health, including, but not limited to, serious pain, the potential loss of life, limb, or other major bodily function, the immediate and serious deterioration of the health of the employee, or the normal timeframe for the decision-making process would be detrimental to the employee’s life or health or could jeopardize the injured worker's permanent ability to regain maximum function.
(4) “Medically necessary” and “medical necessity” mean medical treatment that is reasonably required to cure or relieve the employee of the effects of their injury and based on the following standards, which shall be applied in the order listed, allowing reliance on a lower ranked standard only if every higher ranked standard is inapplicable to the employee’s medical condition: (A) The Medical Treatment Utilization Schedule adopted by the Administrative Director
pursuant to Labor Code section 5307.27 and set forth in Article 5.5.2 of this Subchapter, beginning with section 9792.20.
(B) Peer-reviewed scientific and medical evidence regarding the effectiveness of the disputed service.
(C) Nationally recognized professional standards. (D) Expert opinion. (E) Generally accepted standards of medical practice. (F) Treatments that are likely to provide a benefit to a patient for conditions for which
other treatments are not clinically efficacious. (5) “Utilization review decision” means a decision pursuant to Labor Code section 4610 to
modify, delay, or deny, based in whole or in part on medical necessity to cure or relieve, a treatment recommendation or recommendations by a physician prior to, retrospectively,

1300-40
or concurrent with the provision of medical treatment services pursuant to Labor Code sections 4600 or 5402(c).
(b)(1) If the request for authorization of medical treatment is not approved, or if the request for authorization for medical treatment is approved in part, any dispute shall be resolved in accordance with Labor Code sections 4610.5 and 4610.6. Neither the employee nor the claims administrator shall have any liability for medical treatment furnished without the authorization of the claims administrator if the treatment is delayed, modified, or denied by a utilization review decision unless the utilization review decision is overturned by independent medical review or the Workers’ Compensation Appeals Board under this Article.
(2) A request for independent medical review must be communicated by the employee, the employee’s representative, or the employee’s attorney by mail, facsimile, or electronic transmission to the Administrative Director, or the Administrative Director’s designee, within 30 days of service of the utilization review decision. The request must be made on the Application for Independent Medical Review, DWC Form IMR, and submitted with a copy of the written decision delaying, denying, or modifying the request for authorization of medical treatment. (A) An unrepresented employee may designate a parent, guardian, conservator, relative,
or other designee of the employee as an agent to act on his or her behalf in filing an application for independent medical review under this subdivision. A designation of an agent executed prior to the utilization review decision shall not be valid.
(B) The physician whose request for authorization of medical treatment was delayed, denied, or modified may join with or otherwise assist the employee in seeking an independent medical review. The physician may submit documents on the employee’s behalf pursuant to section 9792.10.5 (b) and may respond to any inquiry by the independent review organization.
(C) A provider of emergency medical treatment when the employee faced an imminent and serious threat to his or her health, including, but not limited to, the potential loss of life, limb, or other major bodily function, may submit an application for independent medical review under subdivision (b)(2) on its own behalf within 30 days of receipt of the utilization review decision that either delays, denies, or modifies the provider’s retrospective request for authorization of the emergency medical treatment.
(3) If expedited review is requested for a decision eligible for independent medical review, the Application for Independent Medical Review, DWC Form IMR, shall include, unless the initial utilization review decision was made on an expedited basis, a certification from the employee’s treating physician indicating that the employee faces an imminent and serious threat to his or her health as described in section 9792.10.1(a)(3).
(c)(1) If at the time of a utilization review decision the claims administrator is also disputing liability for the treatment for any reason besides medical necessity, the time for the employee to submit an application for independent medical review under subdivision (b)(2) is extended to 30 days after service of a notice to the employee showing that the other dispute of liability has been resolved.
(2) If the claims administrator fails to comply with any provision of section 9792.9(l) or section 9792.9.1(e) at the time of notification of its utilization review decision, the time

1300-41
limitations for the employee to submit an application for independent medical review under subdivision (b)(2) shall not begin to run until the claims administrator provides the written decision, with all required elements, to the employee.
(d) Nothing in this section precludes the parties from participating in an internal utilization review appeal process on a voluntary basis provided the employee and, if the employee is represented by counsel, the employee's attorney, have been notified of the 30-day time limit to file an objection to the utilization review decision in accordance with Labor Code sections 4610.5 and 4610.6. Any internal utilization review appeal process conducted under this subdivision must be completed within 15 days of the date of utilization review decision. (e) The following requirements shall be met prior to a concurrent review decision to deny authorization for medical treatment and to resolve disputes:
(1) In the case of concurrent review, medical care shall not be discontinued until the requesting physician has been notified of the decision and a care plan has been agreed upon by the requesting physician that is appropriate for the medical needs of the employee. In addition, the non-physician provider of goods or services identified in the request for authorization, and for whom contact information has been included, shall be notified in writing of the decision modifying, delaying, or denying a request for authorization that shall not include the rationale, criteria or guidelines used for the decision.
(2) Medical care provided during a concurrent review shall be medical treatment that is reasonably required to cure or relieve from the effects of the industrial injury.
Authority: Sections 133, 4603.5 and 5307.3, Labor Code. Reference: Sections 4062, 4600, 4600.4, 4604.5, 4610, and 4610.5, Labor Code.
1300-42
§ 9792.10.5. Independent Medical Review – Medical Records. (a) (1) Within fifteen (15) days following receipt of the mailed notification from the independent
review organization that the disputed medical treatment has been assigned for independent medical review, or within twelve (12) days if the notification was sent electronically, or for expedited review within twenty-four (24) hours following receipt of the notification, the claims administrator shall provide to the independent medical review organization all of the following documents: (A) A copy of all reports of the employee’s treating physician relevant to the employee’s
current medical condition produced within one year prior to the date of the request for authorization, including those that are specifically identified in the request for authorization or in the utilization review determination.
(B) A copy of the adverse determination by the claims administrator notifying the employee and the employee’s treating physician that the disputed medical treatment was denied, delayed or modified.
(C) A copy of all information, including correspondence, provided to the employee by the claims administrator concerning the utilization review decision regarding the disputed treatment.
(D) A copy of any materials the employee or the employee’s provider submitted to the claims administrator in support of the request for the disputed medical treatment.
(E) A copy of any other relevant documents or information used by the claims administrator in determining whether the disputed treatment should have been provided, and any statements by the claims administrator explaining the reasons for the decision to deny, modify, or delay the recommended treatment on the basis of medical necessity.
(F) The claims administrator’s response to any additional issues raised in the employee’s application for independent medical review.
(2) The claims administrator shall, concurrent with the provision of documents under subdivision (a), serve on the employee or the employee’s representative a notification that lists all of the documents submitted to the independent review organization under subdivision (a). The claims administrator shall provide with the notification a copy of all documents that was not previously provided to the employee or the employee’s representative.
(3) Any newly developed or discovered relevant medical records in the possession of the claims administrator after the documents identified in subdivision (a) are provided to the independent review organization shall be forwarded immediately to the independent review organization. The claims administrator shall concurrently provide a copy of medical records required by this subdivision to the employee, or the employee’s representative, or the employee’s treating physician, unless the offer of medical records is declined or otherwise prohibited by law.
(b) (1) Within fifteen (15) days following receipt of the notification from the independent review
organization that the disputed medical treatment has been assigned for independent medical review, or for expedited review, within twenty-four (24) hours following receipt of the notification, the employee, or any party identified in section 9792.10.1(b)(2), may provide to the independent medical review organization any of the following documents:

1300-43
(i) The treating physician’s recommendation indicating that the disputed medical treatment is medically necessary for the employee’s medical condition.
(ii) Medical information or justification that a disputed medical treatment, on an urgent care or emergency basis, was medically necessary for the employee’s medical condition.
(iii) Reasonable information supporting the position that the disputed medical treatment is or was medically necessary, including all information provided by the employee’s treating physician, or any additional material that the employee believes is relevant.
(2) The employee or any party identified in section 9792.10.1(b)(2) shall, concurrent with the provision of documents under subdivision (b), serve the documents provided under subdivision (b) on the claims administrator, except that documents previously provided to the claims administrator need not be provided again if a list of those documents is served.
(3) Any newly developed or discovered relevant medical records in the possession of the employee, or any party identified in section 9792.10.1(b)(2), after the documents identified in subdivision (b) are provided to the independent review organization shall be forwarded immediately to the independent review organization. The employee, or any party identified in section 9792.10.1(b)(2), shall concurrently provide a copy of medical records required by this subdivision to the claims administrator, unless the offer of medical records is declined or otherwise prohibited by law.
(c) At any time following the submission of documents under subdivision (a) and (b), the independent review organization may reasonably request appropriate additional documentation or information necessary to make a determination that the disputed medical treatment is medically necessary. Additional documentation or other information requested under this section shall be sent by the party to whom the request was made, with service on all other parties, within five (5) business days after the request is received in routine cases or one (1) calendar day after the request is received in expedited cases. (d) The confidentiality of medical records shall be maintained pursuant to applicable state and federal laws. Authority: Sections 133, 4603.5 and 5307.3, Labor Code. Reference: Sections 4062, 4600, 4600.4, 4604.5, 4610, and 4610.5, Labor Code.
1300-44
§9785. Reporting Duties of the Primary Treating Physician. (a) For the purposes of this section, the following definitions apply:
(1) The “primary treating physician” is the physician who is primarily responsible for managing the care of an employee, and who has examined the employee at least once for the purpose of rendering or prescribing treatment and has monitored the effect of the treatment thereafter. The primary treating physician is the physician selected by the employer, the employee pursuant to Article 2 (commencing with section 4600) of Chapter 2 of Part 2 of Division 4 of the Labor Code, or under the contract or procedures applicable to a Health Care Organization certified under section 4600.5 of the Labor Code, or in accordance with the physician selection procedures contained in the medical provider network pursuant to Labor Code section 4616.
(2) A “secondary physician” is any physician other than the primary treating physician who examines or provides treatment to the employee, but is not primarily responsible for continuing management of the care of the employee.
(3) “Claims administrator” is a self-administered insurer providing security for the payment of compensation required by Divisions 4 and 4.5 of the Labor Code, a self-administered self-insured employer, or a third-party administrator for a self-insured employer, insurer, legally uninsured employer, or joint powers authority.
(4) “Medical determination” means, for the purpose of this section, a decision made by the primary treating physician regarding any and all medical issues necessary to determine the employee's eligibility for compensation. Such issues include but are not limited to the scope and extent of an employee's continuing medical treatment, the decision whether to release the employee from care, the point in time at which the employee has reached permanent and stationary status, and the necessity for future medical treatment.
(5) “Released from care” means a determination by the primary treating physician that the employee's condition has reached a permanent and stationary status with no need for continuing or future medical treatment.
(6) “Continuing medical treatment” is occurring or presently planned treatment that is reasonably required to cure or relieve the employee from the effects of the injury.
(7) “Future medical treatment” is treatment which is anticipated at some time in the future and is reasonably required to cure or relieve the employee from the effects of the injury.
(8) “Permanent and stationary status” is the point when the employee has reached maximal medical improvement, meaning his or her condition is well stabilized, and unlikely to change substantially in the next year with or without medical treatment.
(b)(1) An employee shall have no more than one primary treating physician at a time.
(2) An employee may designate a new primary treating physician of his or her choice pursuant to Labor Code §§4600 or 4600.3 provided the primary treating physician has determined that there is a need for: (A) continuing medical treatment; or (B) future medical treatment. The employee may designate a new primary treating
physician to render future medical treatment either prior to or at the time such treatment becomes necessary.
(3) If the employee disputes a medical determination made by the primary treating physician, including a determination that the employee should be released from care, the dispute

1300-45
shall be resolved under the applicable procedures set forth at Labor Code sections 4061 and 4062. If the employee objects to a decision made pursuant to Labor Code section 4610 to modify, delay, or deny a treatment recommendation, the dispute shall be resolved pursuant to Labor Code section 4610.5, if applicable, or otherwise pursuant to Labor Code section 4062. No other primary treating physician shall be designated by the employee unless and until the dispute is resolved.
(4) If the claims administrator disputes a medical determination made by the primary treating physician, the dispute shall be resolved under the applicable procedures set forth at Labor Code sections 4610, 4061 and 4062.
(c) The primary treating physician, or a physician designated by the primary treating physician, shall make reports to the claims administrator as required in this section. A primary treating physician has fulfilled his or her reporting duties under this section by sending one copy of a required report to the claims administrator. A claims administrator may designate any person or entity to be the recipient of its copy of the required report. (d) The primary treating physician shall render opinions on all medical issues necessary to determine the employee's eligibility for compensation in the manner prescribed in subdivisions (e), (f) and (g) of this section. The primary treating physician may transmit reports to the claims administrator by mail or FAX or by any other means satisfactory to the claims administrator, including electronic transmission. (e)(1) Within 5 working days following initial examination, a primary treating physician shall
submit a written report to the claims administrator on the form entitled “Doctor's First Report of Occupational Injury or Illness,” Form DLSR 5021. Emergency and urgent care physicians shall also submit a Form DLSR 5021 to the claims administrator following the initial visit to the treatment facility. On line 24 of the Doctor's First Report, or on the reverse side of the form, the physician shall (A) list methods, frequency, and duration of planned treatment(s), (B) specify planned consultations or referrals, surgery or hospitalization and (C) specify the type, frequency and duration of planned physical medicine services (e.g., physical therapy, manipulation, acupuncture).
(2) Each new primary treating physician shall submit a Form DLSR 5021 following the initial examination in accordance with subdivision (e)(1).
(3) Secondary physicians, physical therapists, and other health care providers to whom the employee is referred shall report to the primary treating physician in the manner required by the primary treating physician.
(4) The primary treating physician shall be responsible for obtaining all of the reports of secondary physicians and shall, unless good cause is shown, within 20 days of receipt of each report incorporate, or comment upon, the findings and opinions of the other physicians in the primary treating physician's report and submit all of the reports to the claims administrator.
(f) A primary treating physician shall, unless good cause is shown, within 20 days report to the claims administrator when any one or more of the following occurs:
(1) The employee's condition undergoes a previously unexpected significant change;
1300-46
(2) There is any significant change in the treatment plan reported, including, but not limited to, (A) an extension of duration or frequency of treatment, (B) a new need for hospitalization or surgery, (C) a new need for referral to or consultation by another physician, (D) a change in methods of treatment or in required physical medicine services, or (E) a need for rental or purchase of durable medical equipment or orthotic devices;
(3) The employee's condition permits return to modified or regular work; (4) The employee's condition requires him or her to leave work, or requires changes in work
restrictions or modifications; (5) The employee is released from care; (6) The primary treating physician concludes that the employee's permanent disability
precludes, or is likely to preclude, the employee from engaging in the employee's usual occupation or the occupation in which the employee was engaged at the time of the injury;
(7) The claims administrator reasonably requests appropriate additional information that is necessary to administer the claim. “Necessary” information is that which directly affects the provision of compensation benefits as defined in Labor Code Section 3207.
(8) When continuing medical treatment is provided, a progress report shall be made no later than forty-five days from the last report of any type under this section even if no event described in paragraphs (1) to (7) has occurred. If an examination has occurred, the report shall be signed and transmitted within 20 days of the examination.
Except for a response to a request for information made pursuant to subdivision (f)(7), reports required under this subdivision shall be submitted on the “Primary Treating Physician's Progress Report” form (Form PR-2) contained in Section 9785.2, or in the form of a narrative report. If a narrative report is used, it must be entitled “Primary Treating Physician's Progress Report” in bold-faced type, must indicate clearly the reason the report is being submitted, and must contain the same information using the same subject headings in the same order as Form PR-2. A response to a request for information made pursuant to subdivision (f)(7) may be made in letter format. A narrative report and a letter format response to a request for information must contain the same declaration under penalty of perjury that is set forth in the Form PR-2: “I declare under penalty of perjury that this report is true and correct to the best of my knowledge and that I have not violated Labor Code §139.3.” By mutual agreement between the physician and the claims administrator, the physician may make reports in any manner and form. (g) As applicable in section 9792.9.1, a written request for authorization of medical treatment for a specific course of proposed medical treatment, or a written confirmation of an oral request for a specific course of proposed medical treatment, must be set forth on the “Request for Authorization of Medical Treatment,” DWC Form RFA, contained in section 9785.5. A written confirmation of an oral request shall be clearly marked at the top that it is written confirmation of an oral request. The DWC Form RFA must include as an attachment documentation substantiating the need for the requested treatment.

1300-47
(h) When the primary treating physician determines that the employee's condition is permanent and stationary, the physician shall, unless good cause is shown, report within 20 days from the date of examination any findings concerning the existence and extent of permanent impairment and limitations and any need for continuing and/or future medical care resulting from the injury. The information may be submitted on the “Primary Treating Physician's Permanent and Stationary Report” form (DWC Form PR-3 or DWC Form PR-4) contained in section 9785.3 or section 9785.4, or in such other manner which provides all the information required by Title 8, California Code of Regulations, section 10606. For permanent disability evaluation performed pursuant to the permanent disability evaluation schedule adopted on or after January 1, 2005, the primary treating physician's reports concerning the existence and extent of permanent impairment shall describe the impairment in accordance with the AMA Guides to the Evaluation on Permanent Impairment, 5th Edition (DWC Form PR-4). Qualified Medical Evaluators and Agreed Medical Evaluators may not use DWC Form PR-3 or DWC Form PR-4 to report medical-legal evaluations. (i) The primary treating physician, upon finding that the employee is permanent and stationary as to all conditions and that the injury has resulted in permanent partial disability, shall complete the “Physician’s Return-to-Work & Voucher Report” (DWC-AD 10133.36) and attach the form to the report required under subdivision (h). (j) Any controversies concerning this section shall be resolved pursuant to Labor Code Section 4603 or 4604, whichever is appropriate. (k) Claims administrators shall reimburse primary treating physicians for their reports submitted pursuant to this section as required by the Official Medical Fee Schedule. Authority cited: Sections 133, 4603.5 and 5307.3, Labor Code. Reference: Sections 4061, 4061.5, 4062, 4600, 4600.3, 4603.2, 4604.5, 4610.5, 4658.7, 4660, 4662, 4663 and 4664, Labor Code.
1400-1
CID Management
Confidentiality
Policy No. 1400 Revision: 3.3 Revision Date: 6/16/2009 Page 1 of 3
_______________ ________________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which confidentiality of all information shall be maintained.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.1 08/15/2008 Revised Revision 3.2 03/12/2009 Revised Revision 3.3 06/16/2009 Revised Revision 3.3 06/08/2010 Reviewed Revision 3.3 01/26/2011 Reviewed Revision 3.3 04/22/2012 Reviewed Revision 3.3 01/09/2013 Reviewed
3.0 Persons Affected This policy affects all CID employees and contractors who perform utilization management operations, and all others who serve on committees or boards.
4.0 Policy The policy of CID Management is to handle all information in a manner that that ensures the privacy and security of the records. All information that identifies a specific individual shall be kept confidential and shall not be disclosed to any individual or organization outside of disclosures permitted or required by law. The release or re-release of confidential information to unauthorized persons is strictly prohibited.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.

1400-2
6.0 Procedures 6.1 All CID employees and contractors, who perform utilization management operations,
as well as all committee members and board members, shall sign a CID / Business Associate HIPAA Agreement.
6.2 All CID employees and contractors, who perform utilization management operations,
as well as all committee members and board members, shall review this policy.
6.3 All CID employees and contractors, who respond to communications, shall undergo training regarding this policy, these procedures and their implementation.
6.4 All information that identifies a specific individual shall be kept confidential and shall
not be disclosed to any individual or organization outside of disclosures permitted or required by law.
6.5 To the extent permitted by state and federal law, the release of information on a
specific review is restricted to the following people: 6.5.1 CID employee’s or contractors who require the information to perform
utilization management operations 6.5.2 Patient 6.5.3 Patient’s legal counsel 6.5.4 Claims administrator 6.5.5 Client appointed personnel specified by the client as being involved in the
claim and/or review (e.g. nurse case manager) 6.5.6 Defense attorney 6.5.7 Requesting physician, or their office staff 6.5.8 Attending physician, or their office staff 6.5.9 Secondary physicians, or their office staff 6.5.10 Non-physician provider of goods and/or services
6.6 If a CID employee or contractor receives a request for information regarding a
specific claim or review, they shall verify that the requestor is a party identified in point 6.5 of this policy. If it can not be established that the requestor is a party identified in point 6.5 of this policy, the requestor shall be referred to the claims administrator for further help.
6.7 The release of patient information, such as social security number, date of birth,
contact information that does not specifically bear upon the utilization management determination shall be prohibited. If any person requests this information, the requestor shall be referred to the claim administrator for further help.
6.8 The release of provider information, such as federal tax id number or contact
information, which does not specifically bear upon the utilization management determination, shall only be accessible to the client for purposes of billing and bill review. Any other release of this information shall be prohibited. If any person

1400-3
requests this information, the requestor shall be referred to the claim administrator for further help.
6.9 In the event that CID publishes data, such as quality review studies or performance
tracking, in every instance where such publication includes data which identifies a particular physician or health care provider, the physician or health care provider shall be provided written notice of the publication.

1500-1
CID Management
Grievances
Policy No. 1500 Revision: 3.2 Revision Date: 3/16/2011 Page 1 of 3
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which grievances shall be handled.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.1 06/09/2008 Revised Revision 3.2 03/24/2009 Revised Revision 3.2 06/08/2010 Reviewed Revision 3.2 01/28/2011 Revised Revision 3.2 03/16/2011 Revised Revision 3.2 04/22/2012 Reviewed Revision 3.2 01/09/2013 Reviewed
3.0 Persons Affected This policy affects all CID employees and contractors who perform utilization management operations. This policy further affects all stakeholders on any services rendered by CID utilization management.
4.0 Policy The policy of CID Management is to formally investigate all complaints and grievances filed against any CID employee or contractor who performs utilization management operations, or against the CID utilization management process itself. All clinical-related and determination-related issues shall be addressed by the Appeals Consideration policy. All non-clinical-related and non-determination-related grievance issues shall be addressed by this policy.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.

1500-2
6.0 Procedures 6.1 The Clinical Director shall ensure that the Grievance Process is outlined on all
determination letters. 6.2 The Clinical Director shall ensure that the Grievance Process is posted on the CID
webpage at http://www.cidmcorp.com/support/grievance.htm.
6.3 The Clinical Director shall ensure that all non-clinical administrative staff members who are required to interact with outside parties are trained on, and can answer questions related to, the grievance process, including providing contact information for appropriate regulatory and/or investigational agencies.
6.4 CID encourages all stakeholders to resolve individual inquires and problems without
the initiation of a formal grievance. Any party who has an inquiry or complaint may contact CID at 1-866-301-6568 for verbal resolution.
6.5 In the event that a complaint may not be settled at the informal level and the party is
still dissatisfied, he/she will be advised to file a formal grievance. 6.6 Grievances must be submitted within one year of occurrence and shall be submitted
in writing. The written grievance shall contain the following information: 6.6.1 The individual’s name, address and telephone number 6.6.2 A summary of the grievance, any previous contact made with CID, and a
description of the relief sought 6.6.3 The individuals signature 6.6.4 The date the grievance was signed.
6.7 The written grievance shall be mailed to CID. The mailing address for this purpose shall be provided on the grievance form and on adverse determination letters. The grievance form shall be available to the public via CID’s public web site.
6.8 Upon receipt, the written grievance shall be forwarded to the chair of the Grievance
Committee who shall acknowledge the receipt of the grievance within 5 business days.
6.9 The Grievance Committee shall investigate the grievance and shall notify the party of
the final decision in writing within 30 calendar days.
6.10 Should the Grievance Committee determine that any action is required as a result of the grievance, they shall communicate this determination to the Clinical Director who shall be responsible for ensuring the follow up action occurs.

1500-3
6.11 All complaints and grievances shall be reported by the Clinical Director, at the
quarterly meetings of the QAQC Committee.
2000-1
CID Management
Non-Clinical Administrative Staff Credentialing
Policy No. 2000 Revision: 3.0 Revision Date: 6/5/07 Page 1 of 3
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which non-clinical administrative staff employed by CID to perform utilization management operations are credentialed.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy & Form/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 04/16/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 01/27/2011 Reviewed Revision 3.0 04/22/2012 Reviewed Revision 3.0 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all non-clinical administrative staff members employed by CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to perform credentialing on all non-clinical administrative staff members upon initial hiring. The credentialing may include, but is not limited to, reference checks.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
6.1 Upon interviewing prospective employees or contractors, CID shall require the candidates to list a minimum of two references.
2000-2
6.2 If, following the interview process, CID has determined that the candidate is a viable
choice for the position, prior to making a job offer, a member of the interview team may contact the references listed by the candidate.
6.3 The CID interview team member calling for reference check shall complete the
attached form, ‘Telephone Reference Check – Non-Clinical Administrative Staff’, for each reference contacted.
6.4 The completed ‘Telephone Reference Check – Non-Clinical Administrative Staff’
form shall be added to the employee’s personnel folder if they are hired.

2000-3
CID Management
Telephone Reference Check - Non-Clinical Administrative Staff
Applicant’s Name: Person Contacted: Company Contacted: Title: Phone: My name is _________________ and I work at CID Management. I am calling to perform a reference check for __________________ who has applied for a _________________ position with us. He/She has listed you as a reference. Is this a good time to speak with you?
[if no, offer to call back at a convenient time or provide your number and allow them to call you back] 1. What was your relationship to: 2. What were his/her dates of employment? Start date_________ End Date ___________ 3. What was the nature of his/her job with your organization? 4. What did you think of his/her work? 5. What were his/her strong points? 6. What were his/her weak points? 7. How well did he/she work with co-workers? 8. Please comment on his/her:
a. Attitude b. Dependability c. Quality/Quantity of work d. Degree of supervision needed e. Leadership
9. Why did he/she leave the position? 10. Would you re-employ? If no, why not? 11. Is there anything else you would like to add regarding his/her employment or job
performance? Signature: __________________________________ Date: _________________

2010-1
CID Management
Non-Clinical Administrative Staff Initial Paperwork
Policy No. 2010 Revision: 3.0 Revision Date: 6/5/07 Page 1 of 2
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines for paperwork required to be signed by non-clinical administrative staff prior to being employed with CID to perform utilization management operations.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 04/16/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 02/01/2011 Reviewed Revision 3.0 04/22/2012 Reviewed Revision 3.0 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all non-clinical administrative staff members employed by CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to require the following items to be completed by all non-clinical administrative staff members employed by CID to perform utilization management operations prior to commencement of the employment relationship:
4.1 Employment Application 4.2 Non-clinical administrative staff contract 4.3 Non-disclosure agreement 4.4 CID/business associate HIPAA agreement
2010-2
4.5 Conflict of interest form 4.6 W9 or W2, as applicable
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 Prior to interview, all candidates must complete an employment application form. 6.2 Upon official offer of an employment position, CID shall provide the candidate with a
copy of, and shall review, explain and answer any questions from the candidate regarding the following documents:
6.2.1 Non-clinical administrative staff contract 6.2.2 Non-disclosure agreement 6.2.3 CID/business associate HIPAA agreement
6.2.4 Conflict of interest form 6.2.5 W9
6.3 The candidate shall have all the time they feel they require to review the documents
and ask questions of CID. 6.4 Upon receipt of all completed documents listed in section 6.2, the employee shall
begin employment at CID.
2020-1
CID Management
Non-Clinical Administrative Staff Training
Policy No. 2020 Revision: 5.0 Revision Date: 1/29/2008 Page 1 of 3
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines for training provided to non-clinical administrative staff employed with CID to perform utilization management operations.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 05/24/2006 Addition of training in URAC standards Revision 3.0 08/26/2006 Revised Revision 4.0 06/05/2007 Revised Revision 5.0 01/29/2008 Revised Revision 5.0 04/16/2009 Reviewed Revision 5.0 06/08/2010 Reviewed Revision 5.0 02/01/2011 Reviewed Revision 5.0 04/22/2012 Reviewed Revision 5.0 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all non-clinical administrative staff members employed by CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to provide non-clinical administrative staff, employed by CID to perform utilization management operations, with the following training sessions:
4.1 Introduction to CID 4.2 Introduction to workers’ compensation 4.3 Introduction to utilization management
4.3.1 Overview of utilization management

2020-2
4.3.2 Labor code, regulations, and case law regarding utilization management 4.3.3 CID’s utilization management process
4.3.4 URAC utilization management standards
4.4 Conflict of interest policies and procedures 4.5 Confidentiality policies and procedures
4.6 Job specific training,
4.7 Periodic Training Updates as required including:
4.7.1 Changes to the CID utilization management process 4.7.2 Changes to labor code, regulations, or case law regarding utilization
management 4.8 Training on identification and prevention of fraud and abuse, as appropriate to job
functions
4.9 Re-Training on an annual basis.
5.0 Definitions
Definitions of terms are set forth in Policy 1000. 6.0 Procedures
6.1 Upon hire, the non-clinical administrative staff employee’s supervisor shall schedule
the following training sessions for the new non-clinical administrative staff employee: 6.1.1 Introduction to CID 6.1.2 Introduction to workers’ compensation 6.1.3 Introduction to utilization management
6.1.3.1 Overview of utilization management
6.1.3.2 Labor code, regulations, and case law regarding utilization
management
6.1.3.3 CID’s utilization management process

2020-3
6.1.3.4 URAC utilization management standards
6.1.4 Conflict of interest policies and procedures
6.1.5 Confidentiality policies and procedures
6.1.6 Job specific training
6.1.7 Identification of fraud and abuse
6.2 Completion of each training session in section 6.1 shall be logged into the non-clinical administrative staff employee’s personnel file by the employee’s supervisor.
6.3 As needed, the employee’s supervisor shall schedule periodic training updates for all
non-clinical administrative staff employees. 6.4 Completion of periodic training updates may be logged into the non-clinical
administrative staff employee’s personnel file at the discretion of the employee’s supervisor.
6.5 If the employee’s supervisor notes an area of performance in which the non-clinical
administrative staff employee is not adhering to CID’s policies and procedures, or in which the job duties are being performed in an unacceptable fashion, the supervisor shall schedule re-training. The reason for the re-training shall be logged into the non-clinical administrative staff employee’s personnel file by the employee’s supervisor.
6.6 Completion of each re-training session shall be logged into the non-clinical
administrative staff employee’s personnel file by the employee’s supervisor. 6.7 If QAQC committee notes an area of performance in which the non-clinical
administrative staff employee is not adhering to CID’s policies and procedures, or in which the job duties are being performed in an unacceptable fashion, they shall communicate this to the employee and the employee’s supervisor. The supervisor shall schedule re-training. The reason for the re-training shall be logged into the non-clinical administrative staff employee’s personnel file by the employee’s supervisor.
6.8 Completion of each re-training session shall be logged into the non-clinical
administrative staff employee’s personnel file by the employee’s supervisor.
2030-1
CID Management
Non-Clinical Administrative Staff Assessment
Policy No. 2030 Revision: 3.1 Revision Date: 1/27/2011 Page 1 of 7
__________________ ____________ Jonathan Rutchik, MD Robert W. Ward, DC Medical Director, CID President/Managing Director,
CID 1.0 Purpose
This policy establishes guidelines by which non-clinical administrative staff shall undergo assessment.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy and Forms/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 04/16/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.1 01/27/2011 Revised Revision 3.1 04/22/2012 Reviewed Revision 3.1 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all non-clinical administrative staff employed by, or contracted with, CID Management.
4.0 Policy The policy of CID Management is to perform ongoing assessment of non-clinical administrative staff to identify strengths as well as areas in need of improvement. It is further the policy of CID Management to work with the non-clinical administrative staff member at the time of the assessment to create a personal development plan that the non-clinical administrative staff member shall endeavor to complete prior to the following scheduled assessment.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.

2030-2
6.0 Procedures 6.1 The Director of Production shall schedule periodic assessments for each non-clinical
administrative staff member. The periodic assessments shall occur, at minimum, at the following times:
6.1.1 At the 3 month anniversary with CID 6.1.2 At the 6 month anniversary with CID 6.1.3 At the 1 year anniversary with CID, and yearly thereafter.
6.2 Prior to the scheduled assessment, the Director of Production shall complete the attached assessment form.
6.3 Prior to the scheduled assessment, the Director of Production shall review a minimum
of 5 reviews on which the non-clinical administrative staff member worked using the attached form to grade their performance.
6.4 During the scheduled assessment, the Director of Production shall review the
assessment form with the non-clinical administrative staff member and explain all comments listed therein. The Director of Production shall answer any questions the non-clinical administrative staff member has in regard to the assessment form or comments.
6.5 Following the review of the assessment form, the Director of Production and the non-
clinical administrative staff member shall complete the section on the final page entitled “Action Plan”. This shall constitute the non-clinical administrative staff member’s personal development plan.
6.6 The non-clinical staff member shall then be provided the opportunity to add any
comments to the form and then sign and date the form.
6.7 The Director of Production shall provide one copy of the final form to the non-clinical staff member and shall place a copy of the final form in the non-clinical staff member’s personnel file.
6.8 The President/Managing Director shall schedule periodic assessments for each
Director of Production. The periodic assessments shall occur, at minimum, at the following times:
6.8.1 At the 3 month anniversary with CID 6.8.2 At the 6 month anniversary with CID 6.8.3 At the 1 year anniversary with CID, and yearly thereafter.
2030-3
6.9 Prior to the scheduled assessment, the President/Managing Director shall complete
the attached assessment form. 6.10 Prior to the scheduled assessment, the Director of Production shall review a
minimum of 5 reviews on which the non-clinical administrative staff member worked using the attached form to grade their performance.
6.11 During the scheduled assessment, the President/Managing Director shall review
the assessment form with the Director of Production and explain all comments listed therein. The President/Managing Director shall answer any questions the Director of Production has in regard to the assessment form or comments.
6.12 Following the review of the assessment form, the President/Managing Director
and the Director of Production shall complete the section on the final page entitled “Action Plan”. This shall constitute the Director of Production’s personal development plan.
6.13 The Director of Production shall then be provided the opportunity to add any
comments to the form and then sign and date the form.
6.14 The President/Managing Director shall provide one copy of the final form to the Director of Production and shall place a copy of the final form in the Director of Production’s personnel file.
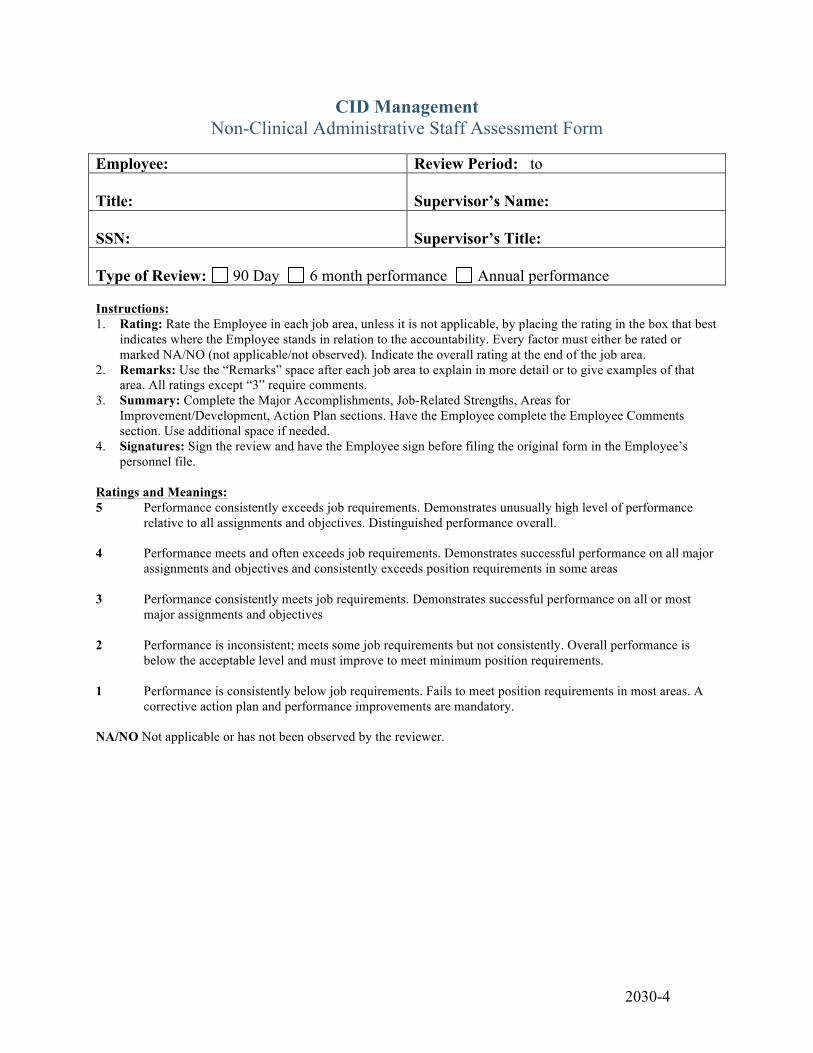
2030-4
CID Management Non-Clinical Administrative Staff Assessment Form
Employee: Review Period: to Title:
Supervisor’s Name:
SSN:
Supervisor’s Title:
Type of Review: 90 Day 6 month performance Annual performance Instructions: 1. Rating: Rate the Employee in each job area, unless it is not applicable, by placing the rating in the box that best
indicates where the Employee stands in relation to the accountability. Every factor must either be rated or marked NA/NO (not applicable/not observed). Indicate the overall rating at the end of the job area.
2. Remarks: Use the “Remarks” space after each job area to explain in more detail or to give examples of that area. All ratings except “3” require comments.
3. Summary: Complete the Major Accomplishments, Job-Related Strengths, Areas for Improvement/Development, Action Plan sections. Have the Employee complete the Employee Comments section. Use additional space if needed.
4. Signatures: Sign the review and have the Employee sign before filing the original form in the Employee’s personnel file.
Ratings and Meanings: 5 Performance consistently exceeds job requirements. Demonstrates unusually high level of performance
relative to all assignments and objectives. Distinguished performance overall.
4 Performance meets and often exceeds job requirements. Demonstrates successful performance on all major assignments and objectives and consistently exceeds position requirements in some areas
3 Performance consistently meets job requirements. Demonstrates successful performance on all or most
major assignments and objectives 2 Performance is inconsistent; meets some job requirements but not consistently. Overall performance is
below the acceptable level and must improve to meet minimum position requirements. 1 Performance is consistently below job requirements. Fails to meet position requirements in most areas. A
corrective action plan and performance improvements are mandatory. NA/NO Not applicable or has not been observed by the reviewer.
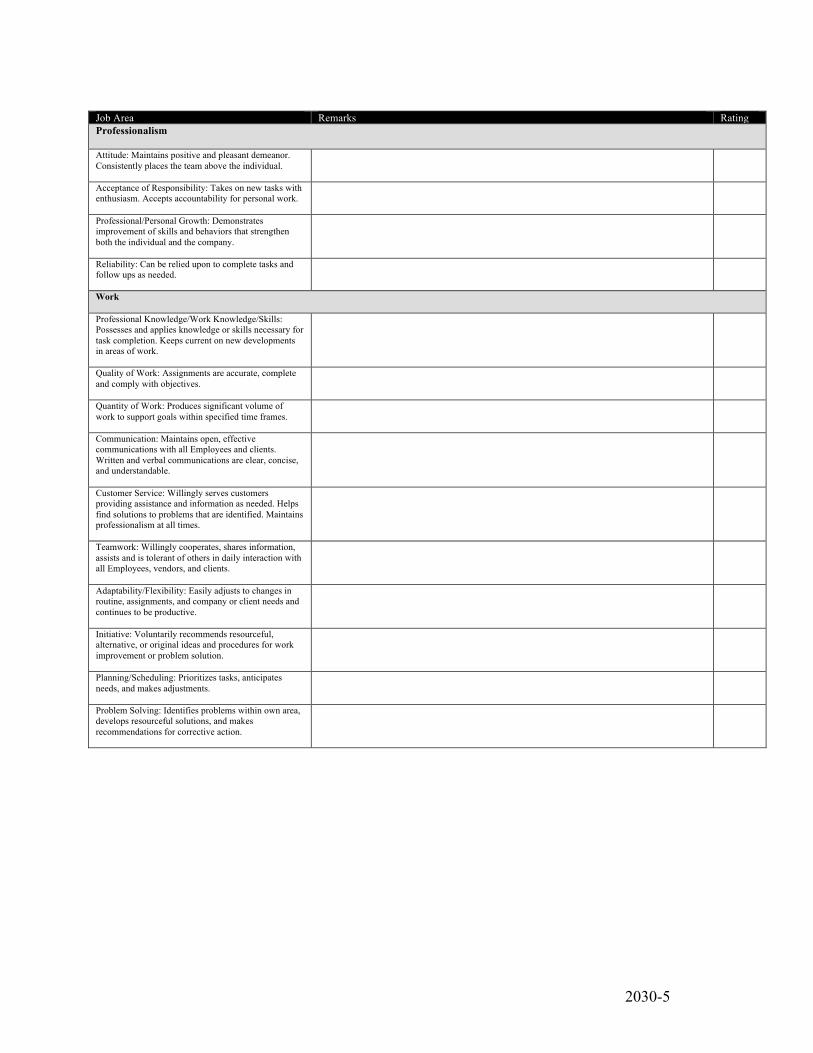
2030-5
Job Area Remarks Rating Professionalism Attitude: Maintains positive and pleasant demeanor. Consistently places the team above the individual.
Acceptance of Responsibility: Takes on new tasks with enthusiasm. Accepts accountability for personal work.
Professional/Personal Growth: Demonstrates improvement of skills and behaviors that strengthen both the individual and the company.
Reliability: Can be relied upon to complete tasks and follow ups as needed.
Work Professional Knowledge/Work Knowledge/Skills: Possesses and applies knowledge or skills necessary for task completion. Keeps current on new developments in areas of work.
Quality of Work: Assignments are accurate, complete and comply with objectives.
Quantity of Work: Produces significant volume of work to support goals within specified time frames.
Communication: Maintains open, effective communications with all Employees and clients. Written and verbal communications are clear, concise, and understandable.
Customer Service: Willingly serves customers providing assistance and information as needed. Helps find solutions to problems that are identified. Maintains professionalism at all times.
Teamwork: Willingly cooperates, shares information, assists and is tolerant of others in daily interaction with all Employees, vendors, and clients.
Adaptability/Flexibility: Easily adjusts to changes in routine, assignments, and company or client needs and continues to be productive.
Initiative: Voluntarily recommends resourceful, alternative, or original ideas and procedures for work improvement or problem solution.
Planning/Scheduling: Prioritizes tasks, anticipates needs, and makes adjustments.
Problem Solving: Identifies problems within own area, develops resourceful solutions, and makes recommendations for corrective action.

2030-6
Summary
Sections 1, 2, 3, and 4 are to be completed by the Supervisor(s). Section 5 is completed by Employee. 1. Major accomplishments since the last review:
2. Job related strengths:
3. Areas for improvement/development:
4. Action plan:
5. Employee’s Comments:
Signatures I acknowledge that this review has been discussed with me. My signature does not imply agreement or disagreement. Employee: ______________________________________________ Date: ____________________ Supervisor:_______________________________________________ Date: ____________________

2030-7
CID Management
Non-Clinical Administrative Staff Review-Specific Assessment
Score: Note: each checkbox that is checked off earns 5%. For a checkbox to be checked it has to be complete and of good quality. A blank checkbox means that area was missing or of poor quality. Client: CID Review #: Non-Clinical Administrative Staff: Date of Review: Claim & Patient Demographics (25%)
Patient and Patient Demographics correct – SSN, DOB, name, etc. Claim stakeholders correctly identified Stakeholder demographics correct Claim demographics correct – claim #, DOI, injured body parts, etc. Correct organization and location.
Review (35%)
Review dates are correct Review stakeholders correctly identified Stakeholder demographics correct Review timeframe correctly identified Reason for review correctly identified Correct number of requested treatments/visits identified Correct date range for requested treatments/visits identified
CID Stakeholders (20%)
Correct administrative user identified Correct initial clinical reviewer identified Correct clinical peer reviewer identified Correct QAQC reviewer identified
Activities and Documents (15%)
All activities are documented Correct documents uploaded Follow up activities set, if applicable
Migration Status is correct (5%)
Overall impression: Notes:
2040-1
CID Management
Delegation of Non-Clinical Functions
Policy No. 2040 Revision: 1.0 Revision Date: 04/20/2008 Page 1 of 4
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines establishing requirements for delegation of functions performed by non-clinical administrative staff employed by CID to a non-CID vendor.
2.0 Revision History
Revision 1.0 04/20/2008 New Policy & Form/Initial Implementation Revision 1.0 04/20/2009 Reviewed Revision 1.0 06/08/2010 Reviewed Revision 1.0 01/26/2011 Reviewed Revision 1.0 04/22/2012 Reviewed Revision 1.0 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all non-clinical administrative staff members employed by vendors under contract with CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to ensure that all non-clinical work performed on behalf of CID by a contracted vendor complies with all requirements and criteria applied to work performed by non-clinical administrative staff employed by CID.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
6.1 Upon identification of a potential vendor for providing functions performed by non-clinical administrative staff, the Clinical Director shall verify that the vendor holds current non-conditional accreditation by URAC for CORE standards.

2040-2
6.2 Prior to contractual agreement for delegation of non-clinical functions, the CID Committee on Policies and Procedures shall review the policies and procedures of the potential vendor. The Committee on Policies and Procedures shall report its findings to all CID Directors, and those findings must at minimum indicate that the vendor is in full compliance with CID polices and procedures, or must specifically identify any areas of potential non-compliance.
6.2.1 Potential vendors must have a policy that prohibits any system for
reimbursement, bonuses, or incentives to staff based directly or indirectly on consumer utilization of health care services.
6.3 The Committee on Policies and Procedures shall obtain and review current policies
and procedures of each vendor contractually performing delegated non-clinical functions at least annually, and shall perform a limited review in the event that the vendor advises CID of a material change in the manner or method of performing delegated functions. The Committee on Policies and Procedures shall report its findings to all CID Directors, and those findings must at minimum indicate that the vendor is in full compliance with CID polices and procedures, or must specifically identify any areas of potential non-compliance.
6.4 Delegated non-clinical functions must be governed by a written contractual
agreement. All such written contracts must conform to the following criteria:
6.4.1 All non-clinical functions which may be delegated to the vendor must be specified.
6.4.2 All non-clinical functions which may not be designated to the vendor must be specified. Non-clinical functions specifically excluded must be consistent with CID Policy 3100 (Pre-Review Screening). Any functions related to domains identified by the Committee on Policies and Procedures as non-compliant with CID policies and procedures must also be specified as excluded.
6.4.3 Contract must specify that vendor must perform all delegated functions in accordance with CID policies and procedures and URAC standards.
6.4.4 Vendor must be required to report any material change in the manner or method of performing delegated functions prior to enacting such change.
6.4.5 Contract must specify that CID may conduct surveys of the vendor as required.
6.4.6 Contract must require that the vendor submit periodic reports to CID regarding the performance of its delegated responsibilities.
6.4.7 Contract must require that in the event of identified problems or non-compliance with either CID policies/procedures or URAC standards, that the vendor will cease performing delegated functions related to the identified problem until correction has been successfully implemented.
6.4.8 Contract must specify that no non-clinical CID functions or work may be further delegated or subcontracted to another party or vendor.
2040-3
6.4.9 Contract must specify that all delegated non-clinical functions or work will be completed via the CID’s proprietary medical management system and database.
6.4.10 Contract must specify that all persons directly involved in performing delegated non-clinical functions must be vetted by the CID Credentialing Committee prior to performing those functions, including provision of a non-disclosure agreement; a HIPAA agreement; and a conflict of interest form.
6.4.11 Contract must specify that all persons directly involved in performing delegated non-clinical functions must be provided with all job-specific training materials available to CID non-clinical staff.
6.5 The Director of Production shall perform periodic assessments for each vendor staff
member performing delegated non-clinical functions. These periodic assessments shall occur, at minimum, at the following times:
6.5.1 After 3 months of performing delegated non-clinical functions for CID 6.5.2 After 6 months of performing delegated non-clinical functions for CID 6.5.3 After 1 year of performing delegated non-clinical functions for CID, and
yearly thereafter.
6.6 The assessment of vendor staff undertaken by the Director of Production shall consist of review of a minimum of 5 reviews on which the vendor staff member worked, using the attached form to grade their performance.
6.7 Periodic assessments of vendor staff are to be forwarded by the Director of Production to the CID Clinical Director.
6.8 The Clinical Director shall incorporate the outcomes of vendor staff assessment into annual reporting to the QAQC Committee.
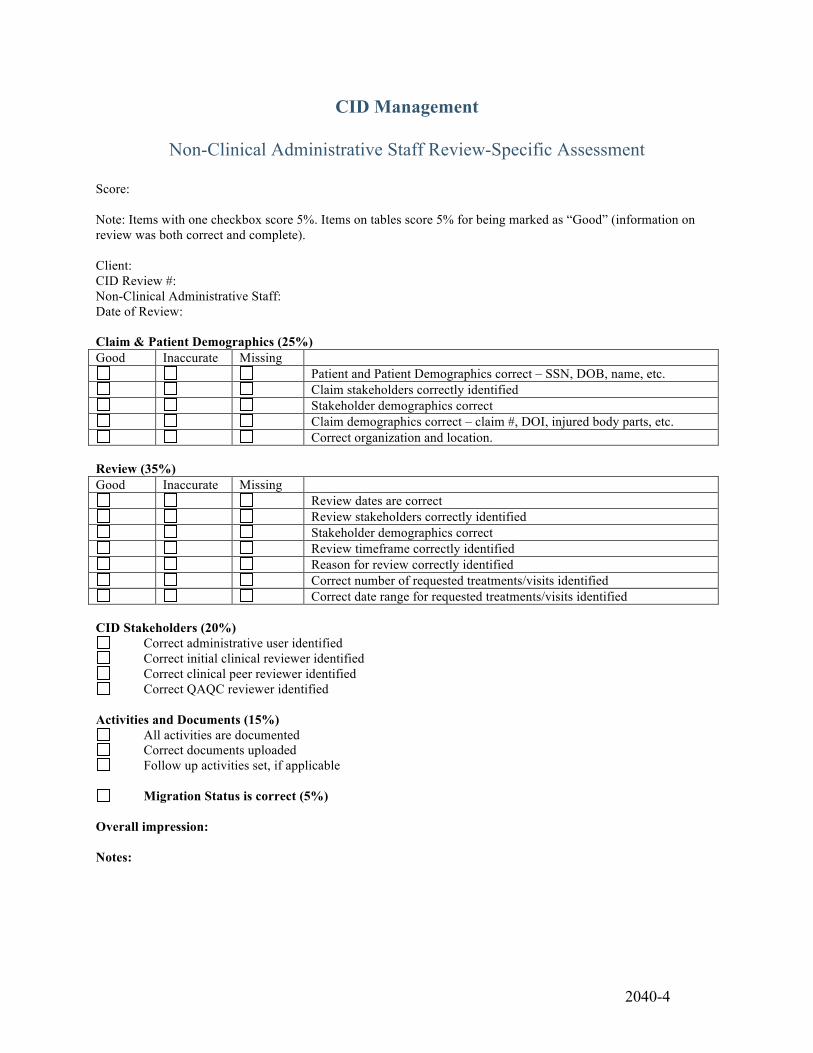
2040-4
CID Management
Non-Clinical Administrative Staff Review-Specific Assessment
Score: Note: Items with one checkbox score 5%. Items on tables score 5% for being marked as “Good” (information on review was both correct and complete). Client: CID Review #: Non-Clinical Administrative Staff: Date of Review: Claim & Patient Demographics (25%) Good Inaccurate Missing
Patient and Patient Demographics correct – SSN, DOB, name, etc. Claim stakeholders correctly identified Stakeholder demographics correct Claim demographics correct – claim #, DOI, injured body parts, etc. Correct organization and location.
Review (35%) Good Inaccurate Missing
Review dates are correct Review stakeholders correctly identified Stakeholder demographics correct Review timeframe correctly identified Reason for review correctly identified Correct number of requested treatments/visits identified Correct date range for requested treatments/visits identified
CID Stakeholders (20%)
Correct administrative user identified Correct initial clinical reviewer identified Correct clinical peer reviewer identified Correct QAQC reviewer identified
Activities and Documents (15%)
All activities are documented Correct documents uploaded Follow up activities set, if applicable
Migration Status is correct (5%)
Overall impression: Notes:
2100-1
CID Management
Initial Clinical Reviewer Credentialing
Policy No. 2100 Revision: 3.3 Revision Date: 3/10/11 Page 1 of 7
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which initial clinical reviewers contracted with CID to perform utilization management operations are credentialed.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.1 04/20/2008 Revised Revision 3.2 06/17/2009 Revised Revision 3.2 06/08/2010 Reviewed Revision 3.3 03/10/2011 Revised Revision 3.3 04/22/2012 Reviewed Revision 3.3 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all initial clinical reviewers contracted with CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to perform credentialing on all initial clinical reviewers upon initial contracting. It is further the policy of CID Management to perform re-credentialing on all initial clinical reviewers on a yearly basis.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
2100-2
6.1 If, following the interview process, CID has determined that the candidate is a viable choice for the position and that a contract offer is desired, prior to making a contract offer the Recruiter of Clinical Personnel shall perform an initial credentialing check.
6.2 The initial credentialing check by the Recruiter of Clinical Personnel shall include
primary source verification as appropriate including any, or all, of the following: 6.2.1 State licensing boards -- validating the practitioner's license to practice
and confirming whether there are any sanctions against the license. 6.2.2 Schools/training programs - validating the practitioner's highest level of
training in his/her specialty and validating board certification status with the American Board of Medical Specialties.
6.2.3 National Technical Information Service (NTIS) -- validating the
practitioner's license to prescribe drugs. The certificates reviewed are the Drug Enforcement Agency (DEA) certificate or Controlled Drug Substance Registration (CDS).
6.2.4 Medicare/Medicaid - determining whether sanctions have been imposed
by the federal government's Office of Inspector General (OIG) or Office of Personnel Management (OPM).
6.2.5 Malpractice history - reviewing claims history.
6.3 The Recruiter of Clinical Personnel shall evaluate to determine if the candidate meets
the following inclusion criteria: 6.3.1 Has undergone formal training in a health care field
6.3.2 Holds an associates degree in a health care field, or holds a state license,
or state certificate in a health care field,
6.3.3 Has professional experience in providing direct patient care,
6.3.4 Holds a current unrestricted license to practice in a health care field
6.3.5 Has an acceptable malpractice history.
6.4 The Recruiter of Clinical Personnel shall also evaluate to determine if the candidate meets the following exclusion criteria:
6.4.1 Has a history of revocation, suspension or limitation to practice their health care discipline,
6.4.2 Has a sanction or disciplinary action within the past five years by their
licensing board,
2100-3
6.4.3 Has an unacceptable malpractice history,
6.4.4 Has a history of felony convictions.
6.5 If, upon initial credentialing, the Recruiter of Clinical Personnel discovers that the
candidate meets all inclusion criteria as outlined in CID Policy 2100, and does not meet any exclusion criteria as outlined in CID Policy 2100, the Recruiter of Clinical Personnel shall forward documentation from primary verification sources to the Director of Clinical Personnel. The Director of Clinical personnel shall also verify that the candidate meets all inclusion criteria from CID Policy 2100 and none of the exclusion from CID Policy 2100 The Director of Clinical Personnel shall conclude that the candidate has passed the credentialing process and shall disclose this information to the Recruiter of Clinical Personnel and Clinical Director.
6.6 If, upon initial credentialing, the Recruiter of Clinical Personnel or the Director of
Clinical Personnel discovers any item that precludes the candidate from meeting all inclusion criteria as outlined in CID Policy 2100, or any item that matches any exclusion criteria as outlined in CID Policy 2100, the Recruiter of Clinical Personnel or the Director of Clinical Personnel shall conclude that the candidate has not passed the credentialing process and shall disclose this information to the Recruiter of Clinical Personnel; the Director of Clinical Personnel; and Clinical Director. The party providing such disclosure shall further indicate the principle reason(s) the candidate did not pass the credentialing process.
6.7 If the candidate successfully passed the credentialing process, the Recruiter of
Clinical Personnel; the Director of Clinical Personnel; or the Clinical Director shall contact the candidate with a contract offer.
6.8 If the candidate has not passed the credentialing process, the Director of Clinical
Personnel or Clinical Director shall contact the candidate to inform him/her that no contract offer will be made and provide the candidate of the principle reason(s) he/she did not pass the credentialing process.
6.9 The candidate shall have the opportunity to respond to the principle reason(s);
however in absence of proving the unsuccessful attempt at credentialing was due to incorrect information, the credentialing decision shall stand.
6.10 The Director of Clinical Personnel shall insure that a re-credentialing of all initial
clinical reviewers is performed by the Director of Clinical Personnel or a Recruiter of Clinical Personnel at regular intervals, not to exceed 1 year and no later than scheduled expiration of licensure/certification. The performance of this credentialing shall include primary source verification as appropriate including any, or all, of the following:
2100-4
6.10.1 State licensing boards -- validating the practitioner's license to practice and confirming whether there are any sanctions against the license.
6.10.2 Validating board certification status with the American Board of Medical
Specialities.
6.10.3 National Technical Information Service (NTIS) -- validating the practitioner's license to prescribe drugs. The certificates reviewed are the Drug Enforcement Agency (DEA) certificate or Controlled Drug Substance Registration (CDS).
6.10.4 Medicare/Medicaid - determining whether sanctions have been imposed
by the federal government's Office of Inspector General (OIG) or Office of Personnel Management (OPM).
6.10.5 Malpractice history - reviewing claims history.
6.11 The periodic re-credentialing evaluation shall determine if the initial clinical
reviewer continues to meet all of the inclusion criteria from CID Policy 2100; and shall determine that the initial clinical reviewer meets none of the exclusion criteria from CID Policy 2100.
6.12 If, upon re-credentialing, the Director of Clinical Personnel or a Recruiter of
Clinical Personnel discovers that the initial clinical reviewer meets all inclusion criteria as outlined in CID Policy 2100, and does not meet any exclusion criteria as outlined in CID Policy 2100, the Director of Clinical Personnel or a Recruiter of Clinical Personnel shall conclude that the initial clinical reviewer has passed the credentialing process and shall document this in the initial clinical reviewer’s personnel file.
6.13 If, upon re-credentialing, the Director of Clinical Personnel or a Recruiter of
Clinical Personnel discovers any item that precludes the initial clinical reviewer from meeting all inclusion criteria as outlined in CID Policy 2100, or any item that matches any exclusion criteria as outlined in CID Policy 2100, the Director of Clinical Personnel or a Recruiter of Clinical Personnel shall conclude that the initial clinical reviewer has not passed the credentialing process and shall disclose this information to the Director of Clinical Personnel and the Clinical Director. Such disclosure shall further include the principle reason(s) the initial clinical reviewer did not pass the re-credentialing process.
6.14 If the initial clinical reviewer has not passed the re-credentialing process, the
Medical Director or Clinical Director shall contact the initial clinical reviewer to inform him/her that his/her contract will be terminated and provide the initial clinical reviewer of the principle reason(s) he/she did not pass the credentialing process.

2100-5
6.15 The initial clinical reviewer shall have the opportunity to respond to the principle reasons, however in absence of proving the unsuccessful attempt at re-credentialing was due to incorrect information, the credentialing decision and contract termination shall stand.
2110-1
CID Management
Initial Clinical Reviewer Initial Paperwork
Policy No. 2110 Revision: 3.1 Revision Date: 3/16/2011 Page 1 of 4
______________ _________________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines for paperwork required to be signed by initial clinical reviewer prior to being contracted with CID to perform utilization management operations.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy and Forms/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 04/16/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.1 03/16/2011 Revised Revision 3.1 04/22/2012 Reviewed Revision 3.1 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all initial clinical reviewer members contracted by CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to require the following items to be completed by all initial clinical reviewer members contracted by CID to perform utilization management operations prior to commencement of the contractor relationship:
4.1 Initial clinical reviewer contract 4.2 Non-disclosure agreement 4.3 CID/business associate HIPAA agreement
4.4 Conflict of interest form
2110-2
4.5 W2 or W9, as applicable It is further the policy of CID Management to require the following items be submitted by all initial clinical reviewers contracted by CID to perform utilization management operations prior to commencement of the contractor relationship:
4.6 Copy of current health care provider licenses
4.7 Listing of all active and inactive health care provider licenses ever held
4.8 Disclosure of all prior disciplinary actions taken by health care licensing boards as
well as any prior malpractice actions.
4.9 Completed Electronic Signature Form.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
6.1 Upon official offer of an contractor position, CID shall request the candidate provide the following documents:
6.1.1 Copy of current curriculum vitae, if available
6.1.2 Copy of current health care provider licenses
6.1.3 Listing of all active and inactive health care provider licenses ever held
6.1.4 Disclosure of all prior disciplinary actions taken by health care licensing
boards as well as any prior malpractice actions.
6.1.5 Completed Electronic Signature Form.
6.2 Upon official offer of an contractor position, CID shall provide the candidate with a copy of, and shall review, explain and answer any questions from the candidate regarding the following documents:
6.2.1 Initial clinical reviewer contract 6.2.2 Non-disclosure agreement 6.2.3 CID/business associate HIPAA agreement
6.2.4 Conflict of interest form

2110-3
6.2.5 W2 or W9, as appropriate
6.3 The candidate shall have all the time they feel they require to review the documents
and ask questions of CID. 6.4 Upon receipt of all documents listed in 6.1 and receipt of all completed documents
listed in section 6.2, the contractor shall begin employment at CID.
2110-4
CID Management
Electronic Signature Form
Your name and electronic signature will be added to all documents that you create within the CID system (e.g. determination letters, requests for additional information). To capture and create your electronic signature, you need to:
1) Sign in each of the boxes below 2) Use black or blue ink 3) Make sure that your signature does not touch or cross any of the box boundaries
Once you have signed each of the boxes, please fax this form to 925-886-4855. Following that, please mail a hardcopy of this page to CID at 2415 San Ramon Valley Blvd #4414, San Ramon, CA 94583. Thank you.
I hereby authorize CID to create an electronic signature for me, using the signatures in the boxes above, and to attach this signature to any documents generated by me within the CID system. Signature: __________________________________ Date: _________________
2120-1
CID Management
Initial Clinical Reviewer Training
Policy No. 2120 Revision: 5.1 Revision Date: 3/11/2011 Page 1 of 3
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines for training provided to initial clinical reviewers contracted with CID to perform utilization management operations.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 05/24/2006 Addition of training in URAC standards Revision 3.0 08/26/2006 Revised Revision 4.0 06/05/2007 Revised Revision 5.0 01/29/2008 Revised Revision 5.0 04/16/2009 Reviewed Revision 5.0 06/08/2010 Reviewed Revision 5.1 03/11/2011 Revised Revision 5.1 04/22/2012 Reviewed Revision 5.1 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all initial clinical reviewers contracted with CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to provide initial clinical reviewers, contracted with CID to perform utilization management operations, with the following training sessions:
4.1 Introduction to CID 4.2 Introduction to workers’ compensation 4.3 Introduction to utilization management
4.3.1 Overview of utilization management

2120-2
4.3.2 Labor code, regulations, and case law regarding utilization management 4.3.3 CID’s utilization management process
4.3.4 URAC utilization management standards
4.4 Conflict of interest policies and procedures 4.5 Confidentiality policies and procedures
4.6 Job specific training
4.7 Periodic Training Updates as required including:
4.7.1 Changes to the CID utilization management process 4.7.2 Changes to labor code, regulations, or case law regarding utilization
management 4.8 Training on identification and prevention of fraud and abuse, as appropriate to job
functions
4.9 Re-Training on an annual basis.
5.0 Definitions
Definitions of terms are set forth in Policy 1000. 6.0 Procedures
6.1 Upon hire, the Clinical Director or Senior Clinical Staff shall schedule the following
training sessions for the new initial clinical reviewer contractor:
6.1.1 Introduction to CID 6.1.2 Introduction to workers’ compensation 6.1.3 Introduction to utilization management
6.1.3.1 Overview of utilization management
6.1.3.2 Labor code, regulations, and case law regarding utilization
management
6.1.3.3 CID’s utilization management process

2120-3
6.1.3.4 URAC utilization management standards
6.1.4 Conflict of interest policies and procedures
6.1.5 Confidentiality policies and procedures
6.1.6 Job specific training
6.1.7 Identification of fraud and abuse
6.2 Completion of each training session in section 6.1 shall be logged into the initial
clinical reviewer’s personnel file by the Clinical Director or Senior Clinical Staff. 6.3 As needed, the Clinical Director or Senior Clinical Staff shall schedule periodic
training updates for all initial clinical reviewers. 6.4 Completion of periodic training updates may be logged into the initial clinical
reviewer’s personnel file at the discretion of the Clinical Director or Senior Clinical Staff.
6.5 If the Clinical Director or Senior Clinical Staff notes an area of performance in which
the initial clinical reviewer is not adhering to CID’s policies and procedures, or in which the job duties are being performed in an unacceptable fashion, the Clinical Director or Senior Clinical Staff shall schedule re-training. The reason for the re-training shall be logged into the initial clinical reviewer’s personnel file by the Clinical Director or Senior Clinical Staff.
6.6 Completion of each re-training session shall be logged into the initial clinical
reviewer’s personnel file by the Clinical Director or Senior Clinical Staff. 6.7 If QAQC committee notes an area of performance in which the initial clinical
reviewer is not adhering to CID’s policies and procedures, or in which the job duties are being performed in an unacceptable fashion, they shall communicate this to the initial clinical reviewer and the Clinical Director or Senior Clinical Staff. The Clinical Director or Senior Clinical Staff shall schedule re-training. The reason for the re-training shall be logged into the initial clinical reviewer’s personnel file by the Clinical Director or Senior Clinical Staff.
6.8 Completion of each re-training session shall be logged into the initial clinical
reviewer’s personnel file by the Clinical Director or Senior Clinical Staff.

2130-1
CID Management
Initial Clinical Reviewer Assessment
Policy No. 2130 Revision: 4.1 Revision Date: 3/11/2011 Page 1 of 3
________________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which initial clinical reviewer shall undergo assessment.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy and Forms/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 4.0 05/14/2009 Revised Revision 4.0 06/08/2010 Reviewed Revision 4.0 01/27/2011 Reviewed Revision 4.1 03/11/2011 Revised Revision 4.1 04/22/2012 Reviewed Revision 4.1 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all initial clinical reviewers employed by, or contracted with, CID Management.
4.0 Policy The policy of CID Management is to perform ongoing assessment of initial clinical reviewers to identify strengths as well as areas in need of improvement. It is further the policy of CID Management to work with the initial clinical reviewers at the time of the assessment to create a personal development plan that the initial clinical reviewers shall endeavor to complete prior to the following scheduled assessment.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
2130-2
6.1 The Clinical Director or Senior Clinical Staff shall conduct periodic assessments for
each initial clinical reviewer. The periodic assessments shall occur with reference to the following intervals:
6.1.1 At the 3 month anniversary with CID 6.1.2 At the 6 month anniversary with CID 6.1.3 At the 1 year anniversary with CID, and yearly thereafter.
6.2 The scheduled assessment will include consideration of reviews on which the initial
reviewer worked, using the attached form to grade their performance. The performance assessment forms will be completed by the Clinical Director or Senior Clinical Staff. Whenever possible, a minimum of 5 reviews on which the initial clinical reviewer worked should be considered during each assessment interval.
6.3 As review assessments are completed, the Clinical Director or Senior Clinical Staff
member who completed the assessment shall provide the assessment form and the draft assessed to the initial clinical reviewer, with explanations of all noted issues. The Clinical Director or Senior Clinical Staff member who completed the assessment shall invite the initial reviewer to discuss any questions or concerns regarding the assessment; and shall be available for such discussion.
6.4 In the event that an initial reviewer is noted to have similar performance issues on a
consistent or repetitive basis, the Clinical Director or Director of Clinical Training and Assessment shall make available appropriate re-training resources.
6.5 The Clinical Director or Director of Clinical Training and Assessment shall place a
copy of each assessment form in the initial clinical reviewer’s personnel file.
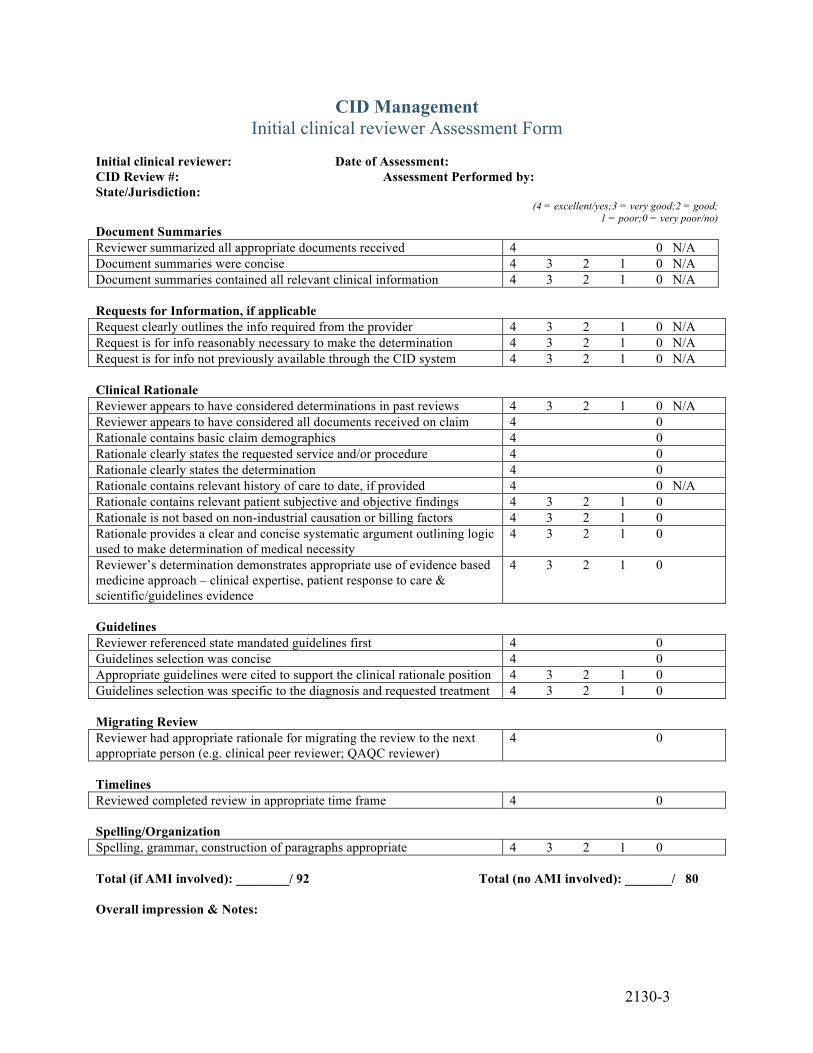
2130-3
CID Management Initial clinical reviewer Assessment Form
Initial clinical reviewer: Date of Assessment: CID Review #: Assessment Performed by: State/Jurisdiction:
(4 = excellent/yes;3 = very good;2 = good; 1 = poor;0 = very poor/no)
Document Summaries Reviewer summarized all appropriate documents received 4 0 N/A Document summaries were concise 4 3 2 1 0 N/A Document summaries contained all relevant clinical information 4 3 2 1 0 N/A Requests for Information, if applicable Request clearly outlines the info required from the provider 4 3 2 1 0 N/A Request is for info reasonably necessary to make the determination 4 3 2 1 0 N/A Request is for info not previously available through the CID system 4 3 2 1 0 N/A Clinical Rationale Reviewer appears to have considered determinations in past reviews 4 3 2 1 0 N/A Reviewer appears to have considered all documents received on claim 4 0 Rationale contains basic claim demographics 4 0 Rationale clearly states the requested service and/or procedure 4 0 Rationale clearly states the determination 4 0 Rationale contains relevant history of care to date, if provided 4 0 N/A Rationale contains relevant patient subjective and objective findings 4 3 2 1 0 Rationale is not based on non-industrial causation or billing factors 4 3 2 1 0 Rationale provides a clear and concise systematic argument outlining logic used to make determination of medical necessity
4 3 2 1 0
Reviewer’s determination demonstrates appropriate use of evidence based medicine approach – clinical expertise, patient response to care & scientific/guidelines evidence
4 3 2 1 0
Guidelines Reviewer referenced state mandated guidelines first 4 0 Guidelines selection was concise 4 0 Appropriate guidelines were cited to support the clinical rationale position 4 3 2 1 0 Guidelines selection was specific to the diagnosis and requested treatment 4 3 2 1 0 Migrating Review Reviewer had appropriate rationale for migrating the review to the next appropriate person (e.g. clinical peer reviewer; QAQC reviewer)
4 0
Timelines Reviewed completed review in appropriate time frame 4 0 Spelling/Organization Spelling, grammar, construction of paragraphs appropriate 4 3 2 1 0 Total (if AMI involved): ________/ 92 Total (no AMI involved): _______/ 80 Overall impression & Notes:
2140-1
CID Management
Delegation of Initial Clinical Review Functions
Policy No. 2140 Revision: 2.0 Revision Date: 5/14/2009 Page 1 of 5
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines establishing requirements for delegation of functions performed by initial clinical reviewers to a non-CID vendor.
2.0 Revision History
Revision 1.0 04/20/2008 New Policy & Form/Initial Implementation Revision 2.0 05/14/2009 Revised Revision 2.0 06/08/2010 Reviewed Revision 2.0 01/26/2011 Reviewed Revision 2.0 04/22/2012 Reviewed Revision 2.0 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all clinical staff employed by vendors under contract with CID to perform functions that are components of an initial clinical review.
4.0 Policy The policy of CID Management is to ensure that all initial clinical review functions performed on behalf of CID by a contracted vendor complies with all requirements and criteria applied to work performed by initial clinical reviewers employed by CID.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 Upon identification of a potential vendor for providing functions performed by initial
clinical reviewers, the Clinical Director shall verify that the vendor holds current non-conditional accreditation by URAC for CORE standards.
2140-2
6.2 Prior to contractual agreement for delegation of initial clinical review functions, the CID Committee on Policies and Procedures shall review the policies and procedures of the potential vendor. The Committee on Policies and Procedures shall report its findings to all CID Directors, and those findings must at minimum indicate that the vendor is in full compliance with CID polices and procedures, or must specifically identify any areas of potential non-compliance.
6.2.1 Potential vendors must have a policy that prohibits any system for
reimbursement, bonuses, or incentives to staff based directly or indirectly on consumer utilization of health care services.
6.3 The Committee on Policies and Procedures shall obtain and review current policies
and procedures of each vendor contractually performing delegated initial clinical review functions at least annually, and shall perform a limited review in the event that the vendor advises CID of a material change in the manner or method of performing delegated functions. The Committee on Policies and Procedures shall report its findings to all CID Directors, and those findings must at minimum indicate that the vendor is in full compliance with CID polices and procedures, or must specifically identify any areas of potential non-compliance.
6.4 Delegated initial clinical review functions must be governed by a written contractual
agreement. All such written contracts must conform to the following criteria:
6.4.1 All initial clinical review functions which may be delegated to the vendor must be specified, and must be consistent with CID Policy 3200 (Initial Clinical Review).
6.4.2 All clinical functions which may not be designated to the vendor must be specified. Clinical functions specifically excluded must be consistent with CID Policy 3200 (Initial Clinical Review). Any functions related to domains identified by the Committee on Policies and Procedures as non-compliant with CID policies and procedures must also be excluded.
6.4.3 Contract must specify that vendor must perform all delegated functions in accordance with CID policies and procedures and URAC standards.
6.4.4 Vendor must be required to report any material change in the manner or method of performing delegated functions prior to enacting such change.
6.4.5 Contract must specify that CID may conduct surveys of the vendor as required.
6.4.6 Contract must require that the vendor submit periodic reports to CID regarding the performance of its delegated responsibilities.
6.4.7 Contract must require that in the event of identified problems or non-compliance with either CID policies/procedures or URAC standards, that the vendor will cease performing delegated functions related to the identified problem until correction has been successfully implemented.
6.4.8 Contract must specify that no initial clinical review CID functions or work may be further delegated or subcontracted to another party or vendor.
2140-3
6.4.9 Contract must specify that all delegated initial clinical review functions or work will be completed via the CID’s proprietary medical management system and database.
6.4.10 Contract must specify that each person directly involved in performing delegated initial clinical review functions must be vetted by the CID Credentialing Committee prior to performing those functions, including provision of a copy of a valid clinical license; documentation of malpractice insurance coverage; a copy of a curriculum vitae, including education and history of providing direct patient care; non-disclosure agreement; a HIPAA agreement; and a conflict of interest form.
6.4.11 Contract must specify that the vendor will provide certification for each person involved in performing delegated initial clinical review functions has no history of revocation, suspension or limitation to practice their health care discipline; no sanction or disciplinary action within the past five years by their licensing board; no history of malpractice claims or convictions; and no history of felony convictions.
6.4.12 Contract must specify that any person deemed by the CID Credentialing Committee to be unqualified or unsuitable as an initial clinical reviewer shall be prohibited from performing any delegated functions of initial clinical review on behalf of CID.
6.4.13 Contract must specify that documentation described in 6.4.11 and 6.4.12 shall be provided to the CID Credentialing Committee at least annually for re-credentialing of each person performing delegated initial clinical review functions.
6.4.14 Contract must specify that all persons directly involved in performing delegated initial clinical review functions must be provided with all job-specific training materials available to CID initial clinical reviewers.
6.4.15 Individuals who conduct initial clinical review have access to consultation with a licensed doctor of medicine or doctor of osteopathic medicine; or licensed health professional in the same licensure category as the ordering provider; or a health professional with the same clinical education as the ordering provider in clinical specialties where licensure is not issued. The contract must specify whether the vendor or CID is to provide this professional support. In the event that the vendor provides this support, person(s) providing the support must be vetted by the CID Credentialing Committee prior to the commencement of delegated initial review functions.
6.5 The Clinical Director shall perform periodic assessments for each vendor staff
member performing delegated initial clinical review functions. These periodic assessments shall occur, at minimum, at the following times:
6.5.1 After 3 months of performing delegated initial clinical review functions
for CID

2140-4
6.5.2 After 6 months of performing delegated initial clinical review functions for CID
6.5.3 After 1 year of performing delegated initial clinical review functions for
CID, and yearly thereafter.
6.6 The assessment of vendor staff undertaken by the Clinical Director shall consist of review of a minimum of 5 reviews on which the vendor staff member worked, using the attached form to grade their performance.
6.7 The Clinical Director shall incorporate the outcomes of vendor staff assessment into annual reporting to the QAQC Committee.
6.8 No initial clinical review functions shall be delegated for emergency, urgent, expedited or concurrent reviews.
6.9 All reviews for which initial clinical reviewer functions have been delegated to a non-CID contracted vendor shall be verified for correctness and accuracy by a CID QA/QC reviewer prior to release of any determination letters.

2140-5
Initial clinical reviewer: Date of Assessment: CID Review #: Assessment Performed by: State/Jurisdiction:
(4 = excellent/yes;3 = very good;2 = good; 1 = poor;0 = very poor/no)
Document Summaries Reviewer summarized all appropriate documents received 4 0 N/A Document summaries were concise 4 3 2 1 0 N/A Document summaries contained all relevant clinical information 4 3 2 1 0 N/A Requests for Information, if applicable Request clearly outlines the info required from the provider 4 3 2 1 0 N/A Request is for info reasonably necessary to make the determination 4 3 2 1 0 N/A Request is for info not previously available through the CID system 4 3 2 1 0 N/A Clinical Rationale Reviewer appears to have considered determinations in past reviews 4 3 2 1 0 N/A Reviewer appears to have considered all documents received on claim 4 0 Rationale contains basic claim demographics 4 0 Rationale clearly states the requested service and/or procedure 4 0 Rationale clearly states the determination 4 0 Rationale contains relevant history of care to date, if provided 4 0 N/A Rationale contains relevant patient subjective and objective findings 4 3 2 1 0 Rationale is not based on non-industrial causation or billing factors 4 3 2 1 0 Rationale provides a clear and concise systematic argument outlining logic used to make determination of medical necessity
4 3 2 1 0
Reviewer’s determination demonstrates appropriate use of evidence based medicine approach – clinical expertise, patient response to care & scientific/guidelines evidence
4 3 2 1 0
Guidelines Reviewer referenced state mandated guidelines first 4 0 Guidelines selection was concise 4 0 Appropriate guidelines were cited to support the clinical rationale position 4 3 2 1 0 Guidelines selection was specific to the diagnosis and requested treatment 4 3 2 1 0 Migrating Review Reviewer had appropriate rationale for migrating the review to the next appropriate person (e.g. clinical peer reviewer; QAQC reviewer)
4 0
Timelines Reviewed completed review in appropriate time frame 4 0 Spelling/Organization Spelling, grammar, construction of paragraphs appropriate 4 3 2 1 0 Total (if AMI involved): ________/ 92 Total (no AMI involved): _______/ 80 Overall impression & Notes:
2200-1
CID Management
Clinical Peer Reviewer Credentialing
Policy No. 2200 Revision: 3.3 Revision Date: 3/11/2011 Page 1 of 9
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which clinical peer reviewers contracted with CID to perform utilization management operations are credentialed.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.1 04/20/2008 Revised Revision 3.2 04/21/2009 Revised Revision 3.2 06/08/2010 Reviewed Revision 3.2 01/27/2011 Reviewed Revision 3.3 03/11/2011 Revised Revision 3.3 12/22/2011 Reviewed Revision 3.3 04/22/2012 Reviewed Revision 3.3 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all clinical peer reviewers contracted with CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to perform credentialing on all clinical peer reviewers upon initial contracting. It is further the policy of CID Management to perform re-credentialing on all clinical peer reviewers on a yearly basis.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures

2200-2
6.1 If, following the interview process, CID has determined that the candidate is a viable
choice for the position and that a contract offer is desired, prior to making a contract offer the Recruiter of Clinical Personnel shall perform an initial credentialing check.
6.2 The initial credentialing check by the Recruiter of Clinical Personnel shall include
primary source verification as appropriate including any, or all, of the following: 6.2.1 State licensing boards -- validating the practitioner's license to practice
and confirming whether there are any sanctions against the license. 6.2.2 Schools/training programs - validating the practitioner's highest level of
training in his/her specialty and validating board certification status with the American Board of Medical Specialities.
6.2.3 National Technical Information Service (NTIS) -- validating the
practitioner's license to prescribe drugs. The certificates reviewed are the Drug Enforcement Agency (DEA) certificate or Controlled Drug Substance Registration (CDS).
6.2.4 Medicare/Medicaid - determining whether sanctions have been imposed
by the federal government's Office of Inspector General (OIG) or Office of Personnel Management (OPM).
6.2.5 Malpractice history - reviewing claims history.
6.3 The Recruiter of Clinical Personnel shall evaluate to determine if the candidate meets
the following inclusion criteria: 6.3.1 Has undergone formal training in a health care field
6.3.2 Holds an associates degree in a health care field, or holds a state license,
or state certificate in a health care field,
6.3.3 Has professional experience in proving direct patient care,
6.3.4 Holds a current unrestricted license to practice in a health care field
6.3.5 Has an acceptable malpractice history.
6.4 The Recruiter of Clinical Personnel shall also evaluate to determine if the candidate meets the following exclusion criteria:
6.4.1 Has a history of revocation, suspension or limitation to practice their health care discipline,

2200-3
6.4.2 Has a sanction or disciplinary action within the past five years by their licensing board,
6.4.3 Has an unacceptable malpractice history,
6.4.4 Has a history of felony convictions.
6.5 If, upon initial credentialing, the Recruiter of Clinical Personnel discovers that the
candidate meets all inclusion criteria as outlined in CID Policy 2200, and does not meet any exclusion criteria as outlined in CID Policy 2200, the Recruiter of Clinical Personnel shall forward documentation from primary verification sources to the Director of Clinical Personnel. The Director of Clinical personnel shall also verify that the candidate meets all inclusion criteria from CID Policy 2200 and none of the exclusion from CID Policy 2200 The Director of Clinical Personnel shall conclude that the candidate has passed the credentialing process and shall disclose this information to the Recruiter of Clinical Personnel and Clinical Director.
6.6 If, upon initial credentialing, the Recruiter of Clinical Personnel or the Director of
Clinical Personnel discovers any item that precludes the candidate from meeting all inclusion criteria as outlined in CID Policy 2200, or any item that matches any exclusion criteria as outlined in CID Policy 2200, the Recruiter of Clinical Personnel or the Director of Clinical Personnel shall conclude that the candidate has not passed the credentialing process and shall disclose this information to the Recruiter of Clinical Personnel; the Director of Clinical Personnel; and Clinical Director. The party providing such disclosure shall further indicate the principle reason(s) the candidate did not pass the credentialing process.
6.7 If the candidate successfully passed the credentialing process, the Recruiter of
Clinical Personnel; the Director of Clinical Personnel; or the Clinical Director shall contact the candidate with a contract offer.
6.8 If the candidate has not passed the credentialing process, the Director of Clinical
Personnel or Clinical Director shall contact the candidate to inform him/her that no contract offer will be made and provide the candidate of the principle reason(s) he/she did not pass the credentialing process.
6.9 The candidate shall have the opportunity to respond to the principle reason(s);
however in absence of proving the unsuccessful attempt at credentialing was due to incorrect information, the credentialing decision shall stand.
6.10 The Director of Clinical Personnel shall insure that a re-credentialing of all initial
clinical reviewers is performed by the Director of Clinical Personnel or a Recruiter of Clinical Personnel at regular intervals, , not to exceed 1 year and no later than scheduled expiration of licensure/certification.. The performance of this credentialing shall include primary source verification as appropriate including any, or all, of the following:
2200-4
6.10.1 State licensing boards -- validating the practitioner's license to practice
and confirming whether there are any sanctions against the license. 6.10.2 Validating board certification status with the American Board of Medical
Specialities.
6.10.3 National Technical Information Service (NTIS) -- validating the practitioner's license to prescribe drugs. The certificates reviewed are the Drug Enforcement Agency (DEA) certificate or Controlled Drug Substance Registration (CDS).
6.10.4 Medicare/Medicaid - determining whether sanctions have been imposed
by the federal government's Office of Inspector General (OIG) or Office of Personnel Management (OPM).
6.10.5 Malpractice history - reviewing claims history.
6.11 The periodic re-credentialing evaluation shall determine if the initial clinical
reviewer continues to meet all of the inclusion criteria from CID Policy 2200; and shall determine that the initial clinical reviewer meets none of the exclusion criteria from CID Policy 2200:
6.12 If, upon re-credentialing, the Director of Clinical Personnel or a Recruiter of
Clinical Personnel discovers that the clinical peer reviewer meets all inclusion criteria as outlined in CID Policy 2200, and does not meet any exclusion criteria as outlined in CID Policy 2200, the Director of Clinical Personnel or a Recruiter of Clinical Personnel shall conclude that the clinical peer reviewer has passed the credentialing process and shall document this in the clinical peer reviewer’s personnel file.
6.13 If, upon re-credentialing, the Director of Clinical Personnel or a Recruiter of
Clinical Personnel discovers any item that precludes the clinical peer reviewer from meeting all inclusion criteria as outlined in CID Policy 2200, or any item that matches any exclusion criteria as outlined in CID Policy 2200, the Director of Clinical Personnel or a Recruiter of Clinical Personnel shall conclude that the clinical peer reviewer has not passed the credentialing process and shall disclose this information to the Director of Clinical Personnel and the Clinical Director. Such disclosure shall further include the principle reason(s) the clinical peer reviewer did not pass the re-credentialing process.
6.14 If the clinical peer reviewer has not passed the re-credentialing process, the
Medical Director or Clinical Director shall contact the clinical peer reviewer to inform him/her that his/her contract will be terminated and provide the clinical peer reviewer of the principle reason(s) he/she did not pass the credentialing process.
2200-5
6.15 The clinical peer reviewer shall have the opportunity to respond to the principle reasons, however in absence of proving the unsuccessful attempt at re-credentialing was due to incorrect information, the credentialing decision and contract termination shall stand.

2200-6
Addendum – State of California 1.0 The clinical peer reviewer may be a:
medical doctor; doctor of osteopathy; psychologist; acupuncturist; optometrist; dentist; podiatrist; or chiropractic practitioner.
2.0 The clinical peer reviewer must be licensed, by any state or the District of Columbia. 3.0 The clinical peer reviewer must be competent to evaluate the specific clinical issues involved
in medical treatment services, where these services are within the scope of the reviewer's practice.
2210-1
CID Management
Clinical Peer Reviewer Initial Paperwork
Policy No. 2210 Revision: 3.0 Revision Date: 3/16/2011 Page 1 of 4
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines for paperwork required to be signed by clinical peer reviewer prior to being contracted with CID to perform utilization management operations.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy and Forms/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 05/14/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 03/16/2011 Revised Revision 3.0 04/22/2012 Reviewed Revision 3.0 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all clinical peer reviewer members contracted by CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to require the following items to be completed by all clinical peer reviewer members contracted by CID to perform utilization management operations prior to commencement of the contractor relationship:
4.1 Clinical peer reviewer contract 4.2 Non-disclosure agreement 4.3 CID/business associate HIPAA agreement
4.4 Conflict of Interest form
2210-2
4.5 W2 or W9, as applicable It is further the policy of CID Management to require the following items be submitted by all clinical peer reviewers contracted by CID to perform utilization management operations prior to commencement of the contractor relationship:
4.6 Copy of current curriculum vitae 4.7 Copy of current health care provider licenses
4.8 Listing of all active and inactive health care provider licenses ever held 4.9 Copy of current malpractice insurance policy coversheet
4.10 Disclosure of all prior disciplinary actions taken by health care licensing boards as
well as any prior malpractice actions.
4.11 Completed Electronic Signature Form.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
6.1 Upon official offer of an contractor position, CID shall request the candidate provide the following documents:
6.1.1 Copy of current curriculum vitae
6.1.2 Copy of current health care provider licenses
6.1.3 Listing of all active and inactive health care provider licenses ever held
6.1.4 Copy of current malpractice insurance policy coversheet
6.1.5 Disclosure of all prior disciplinary actions taken by health care licensing
boards as well as any prior malpractice actions.
6.1.6 Completed Electronic Signature Form.
6.2 Upon official offer of an contractor position, CID shall provide the candidate with a copy of, and shall review, explain and answer any questions from the candidate regarding the following documents:
6.2.1 Clinical peer reviewer contract

2210-3
6.2.2 Non-disclosure agreement 6.2.3 CID/business associate HIPAA agreement
6.2.4 Conflict of interest form 6.2.5 W2 or W9, as applicable
6.3 The candidate shall have all the time they feel they require to review the documents
and ask questions of CID. 6.4 Upon receipt of all documents listed in 6.1 and receipt of all completed documents
listed in section 6.2, the contractor shall begin employment at CID.
2210-4
CID Management
Electronic Signature Form
Your name and electronic signature will be added to all documents that you create within the CID system (e.g. determination letters, requests for additional information). To capture and create your electronic signature, you need to:
1) Sign in each of the boxes below 2) Use black or blue ink 3) Make sure that your signature does not touch or cross any of the box boundaries
Once you have signed each of the boxes, please fax this form to 925-886-4855. Following that, please mail a hardcopy of this page to CID at 2415 San Ramon Valley Blvd #4414, San Ramon, CA 94583. Thank you.
I hereby authorize CID to create an electronic signature for me, using the signatures in the boxes above, and to attach this signature to any documents generated by me within the CID system. Signature: __________________________________ Date: _________________

2220-1
CID Management
Clinical Peer Reviewer Training
Policy No. 2220 Revision: 5.1 Revision Date: 3/11/2011 Page 1 of 3
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines for training provided to clinical peer reviewers contracted with CID to perform utilization management operations.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 05/24/2006 Addition of training in URAC standards Revision 3.0 08/26/2006 Revised Revision 4.0 06/05/2007 Revised Revision 5.0 01/29/2008 Revised Revision 5.0 05/14/2009 Reviewed Revision 5.0 06/08/2010 Reviewed Revision 5.1 03/11/2011 Revised Revision 5.1 04/22/2012 Reviewed Revision 5.1 04/22/2012 Reviewed
3.0 Persons Affected This policy affects all clinical peer reviewers contracted with CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to provide clinical peer reviewers, contracted with CID to perform utilization management operations, with the following training sessions:
4.1 Introduction to CID 4.2 Introduction to workers’ compensation 4.3 Introduction to utilization management
4.3.1 Overview of utilization management
2220-2
4.3.2 Labor code, regulations, and case law regarding utilization management 4.3.3 CID’s utilization management process
4.3.4 URAC utilization management standards
4.4 Conflict of interest policies and procedures 4.5 Confidentiality policies and procedures
4.6 Job specific training 4.7 Periodic Training Updates as required including:
4.7.1 Changes to the CID utilization management process 4.7.2 Changes to labor code, regulations, or case law regarding utilization
management 4.8 Training on identification and prevention of fraud and abuse, as appropriate to job
functions
4.9 Re-Training on an annual basis.
5.0 Definitions
Definitions of terms are set forth in Policy 1000. 6.0 Procedures
6.1 Upon hire, the Clinical Director or Senior Clinical Staff shall schedule the following
training sessions for the new clinical peer reviewer contractor:
6.1.1 Introduction to CID 6.1.2 Introduction to workers’ compensation 6.1.3 Introduction to utilization management
6.1.3.1 Overview of utilization management
6.1.3.2 Labor code, regulations, and case law regarding utilization
management
6.1.3.3 CID’s utilization management process
2220-3
6.1.3.4 URAC utilization management standards
6.1.4 Conflict of interest policies and procedures
6.1.5 Confidentiality policies and procedures
6.1.6 Job specific training
6.1.7 Identification of fraud and abuse
6.2 Completion of each training session in section 6.1 shall be logged into the clinical
peer reviewer’s personnel file by the Clinical Director or Senior Clinical Staff. 6.3 As needed, the Clinical Director or Senior Clinical Staff shall schedule periodic
training updates for all clinical peer reviewers. 6.4 Completion of periodic training updates may be logged into the clinical peer
reviewer’s personnel file at the discretion of the Clinical Director or Senior Clinical Staff.
6.5 If the Clinical Director or Senior Clinical Staff notes an area of performance in which
the clinical peer reviewer is not adhering to CID’s policies and procedures, or in which the job duties are being performed in an unacceptable fashion, the Clinical Director or Senior Clinical Staff shall schedule re-training. The reason for the re-training shall be logged into the clinical peer reviewer’s personnel file by the Clinical Director or Senior Clinical Staff.
6.6 Completion of each re-training session shall be logged into the clinical peer
reviewer’s personnel file by the Clinical Director or Senior Clinical Staff. 6.7 If QAQC committee notes an area of performance in which the clinical peer reviewer
is not adhering to CID’s policies and procedures, or in which the job duties are being performed in an unacceptable fashion, they shall communicate this to the clinical peer reviewer and the Clinical Director or Senior Clinical Staff. The Clinical Director or Senior Clinical Staff shall schedule re-training. The reason for the re-training shall be logged into the clinical peer reviewer’s personnel file by the Clinical Director or Senior Clinical Staff.
6.8 Completion of each re-training session shall be logged into the clinical peer
reviewer’s personnel file by the Clinical Director or Senior Clinical Staff.
2230-1
CID Management
Clinical Peer Reviewer Assessment
Policy No. 2230 Revision: 4.1 Revision Date: 3/11/2011 Page 1 of 3
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which clinical peer reviewers, Medical Director, and Clinical Director shall undergo assessment.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy and Forms/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 4.0 05/14/2009 Revised Revision 4.0 06/08/2010 Reviewed Revision 4.0 01/27/2011 Reviewed Revision 4.1 03/11/2011 Revised Revision 4.1 04/22/2012 Reviewed Revision 4.1 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all clinical peer reviewers, Medical Director, and Clinical Director employed by, or contracted with, CID Management.
4.0 Policy The policy of CID Management is to perform ongoing assessment of clinical peer reviewers including the Medical Director and Clinical Director to identify strengths as well as areas in need of improvement. It is further the policy of CID Management to work with the clinical peer reviewers at the time of the assessment to create a personal development plan that the clinical peer reviewers shall endeavor to complete prior to the following scheduled assessment.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
2230-2
6.0 Procedures 6.1 The Clinical Director or Senior Clinical Staff shall conduct periodic assessments for
each clinical peer reviewer. The periodic assessments shall occur with reference to the following intervals:
6.1.1 At the 3 month anniversary with CID 6.1.2 At the 6 month anniversary with CID 6.1.3 At the 1 year anniversary with CID, and yearly thereafter.
6.2 The scheduled assessment will include consideration of reviews on which the initial reviewer worked, using the attached form to grade their performance. The performance assessment forms will be completed by the Clinical Director or Senior Clinical Staff. Whenever possible, a minimum of 5 reviews on which the clinical peer reviewer worked should be considered during each assessment interval.
6.3 As review assessments are completed, the Clinical Director or Senior Clinical Staff
member who completed the assessment shall provide the assessment form and the draft assessed to the clinical peer reviewer, with explanations of all noted issues. The Clinical Director or Senior Clinical Staff member who completed the assessment shall invite the initial reviewer to discuss any questions or concerns regarding the assessment; and shall be available for such discussion.
6.4 In the event that an initial reviewer is noted to have similar performance issues on a
consistent or repetitive basis, the Clinical Director or Director of Clinical Training and Assessment shall make available appropriate re-training resources.
6.5 The Clinical Director or Director of Clinical Training and Assessment shall place a
copy of each assessment form in the clinical peer reviewer’s personnel file.
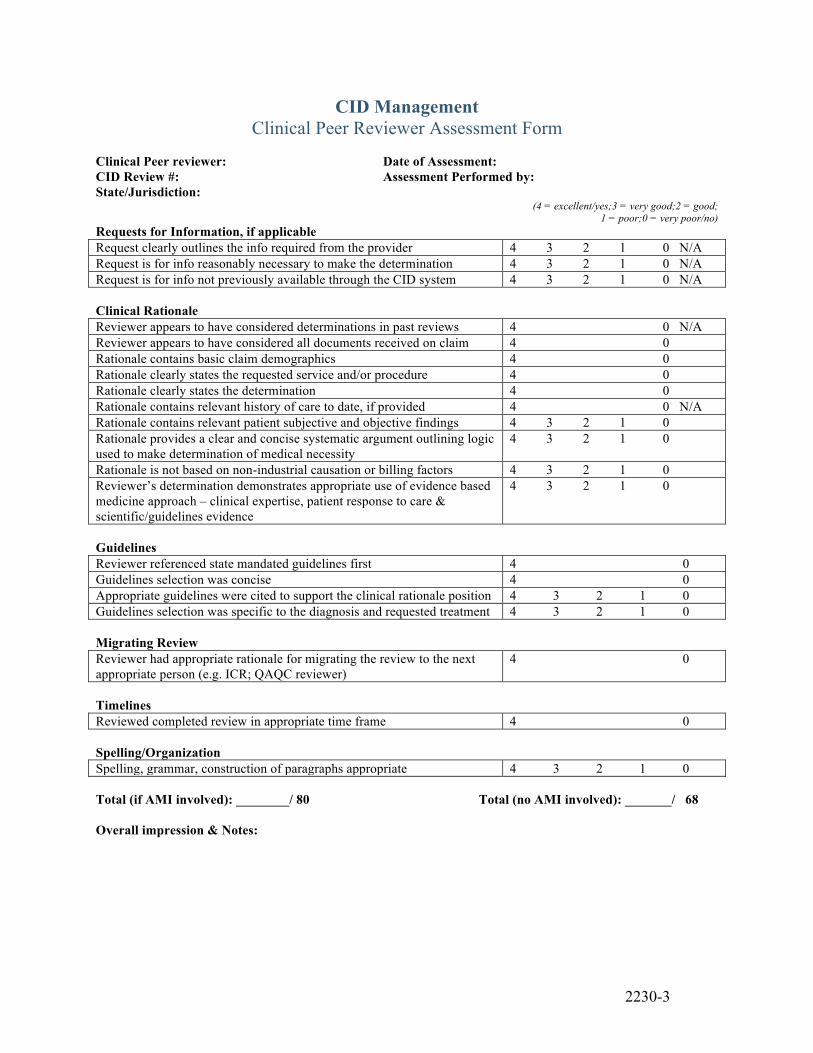
2230-3
CID Management Clinical Peer Reviewer Assessment Form
Clinical Peer reviewer: Date of Assessment: CID Review #: Assessment Performed by: State/Jurisdiction:
(4 = excellent/yes;3 = very good;2 = good; 1 = poor;0 = very poor/no)
Requests for Information, if applicable Request clearly outlines the info required from the provider 4 3 2 1 0 N/A Request is for info reasonably necessary to make the determination 4 3 2 1 0 N/A Request is for info not previously available through the CID system 4 3 2 1 0 N/A Clinical Rationale Reviewer appears to have considered determinations in past reviews 4 0 N/A Reviewer appears to have considered all documents received on claim 4 0 Rationale contains basic claim demographics 4 0 Rationale clearly states the requested service and/or procedure 4 0 Rationale clearly states the determination 4 0 Rationale contains relevant history of care to date, if provided 4 0 N/A Rationale contains relevant patient subjective and objective findings 4 3 2 1 0 Rationale provides a clear and concise systematic argument outlining logic used to make determination of medical necessity
4 3 2 1 0
Rationale is not based on non-industrial causation or billing factors 4 3 2 1 0 Reviewer’s determination demonstrates appropriate use of evidence based medicine approach – clinical expertise, patient response to care & scientific/guidelines evidence
4 3 2 1 0
Guidelines Reviewer referenced state mandated guidelines first 4 0 Guidelines selection was concise 4 0 Appropriate guidelines were cited to support the clinical rationale position 4 3 2 1 0 Guidelines selection was specific to the diagnosis and requested treatment 4 3 2 1 0 Migrating Review Reviewer had appropriate rationale for migrating the review to the next appropriate person (e.g. ICR; QAQC reviewer)
4 0
Timelines Reviewed completed review in appropriate time frame 4 0 Spelling/Organization Spelling, grammar, construction of paragraphs appropriate 4 3 2 1 0 Total (if AMI involved): ________/ 80 Total (no AMI involved): _______/ 68 Overall impression & Notes:

2240-1
CID Management
Delegation of Clinical Peer Review Functions
Policy No. 2240 Revision: 1.0 Revision Date: 5/14/2009 Page 1 of 7
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines establishing requirements for delegation of functions performed by clinical peer reviewers to a non-CID vendor.
2.0 Revision History
Revision 1.0 04/20/2008 New Policy & Form/Initial Implementation Revision 2.0 05/14/2009 Revised Revision 2.0 06/08/2010 Reviewed Revision 2.0 01/26/2011 Reviewed Revision 2.0 04/06/2012 Reviewed Revision 2.0 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all clinical staff employed by vendors under contract with CID to perform functions that are components of a clinical peer review.
4.0 Policy The policy of CID Management is to ensure that all clinical peer review functions performed on behalf of CID by a contracted vendor complies with all requirements and criteria applied to work performed by clinical peer reviewers employed by CID.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
6.1 Upon identification of a potential vendor for providing functions performed by clinical peer reviewers, the Clinical Director shall verify that the vendor holds current non-conditional accreditation by URAC for CORE standards.

2240-2
6.2 Prior to contractual agreement for delegation of clinical peer review functions, the
CID Committee on Policies and Procedures shall review the policies and procedures of the potential vendor. The Committee on Policies and Procedures shall report its findings to all CID Directors, and those findings must at minimum indicate that the vendor is in full compliance with CID polices and procedures, or must specifically identify any areas of potential non-compliance.
6.2.1 Potential vendors must have a policy that prohibits any system for
reimbursement, bonuses, or incentives to staff based directly or indirectly on consumer utilization of health care services.
6.3 The Committee on Policies and Procedures shall obtain and review current policies
and procedures of each vendor contractually performing delegated clinical peer review functions at least annually, and shall perform a limited review in the event that the vendor advises CID of a material change in the manner or method of performing delegated functions. The Committee on Policies and Procedures shall report its findings to all CID Directors, and those findings must at minimum indicate that the vendor is in full compliance with CID polices and procedures, or must specifically identify any areas of potential non-compliance.
6.4 Delegated clinical peer review functions must be governed by a written contractual
agreement. All such written contracts must conform to the following criteria:
6.4.1 All clinical peer review functions which may be delegated to the vendor must be specified, and must be consistent with CID Policy 3300 (Clinical Peer Review).
6.4.2 All clinical functions which may not be designated to the vendor must be specified. Clinical functions specifically excluded must be consistent with CID Policy 3300 (Clinical Peer Review). Any functions related to domains identified by the Committee on Policies and Procedures as non-compliant with CID policies and procedures must also be excluded.
6.4.3 Contract must specify that vendor must perform all delegated functions in accordance with CID policies and procedures and URAC standards.
6.4.4 Vendor must be required to report any material change in the manner or method of performing delegated functions prior to enacting such change.
6.4.5 Contract must specify that CID may conduct surveys of the vendor as required.
6.4.6 Contract must require that the vendor submit periodic reports to CID regarding the performance of its delegated responsibilities.
6.4.7 Contract must require that in the event of identified problems or non-compliance with either CID policies/procedures or URAC standards, that the vendor will cease performing delegated functions related to the identified problem until correction has been successfully implemented.
6.4.8 Contract must specify that no clinical peer review CID functions or work may be further delegated or subcontracted to another party or vendor.

2240-3
6.4.9 Contract must specify that all delegated clinical peer review functions or work will be completed via the CID’s proprietary medical management system and database.
6.4.10 Contract must specify that each person directly involved in performing delegated clinical peer review functions must be vetted by the CID Credentialing Committee prior to performing those functions, including provision of a copy of a valid clinical license; documentation of malpractice insurance coverage; a copy of a curriculum vitae, including education and history of providing direct patient care; non-disclosure agreement; a HIPAA agreement; and a conflict of interest form.
6.4.11 Contract must specify that the vendor will provide certification for each person involved in performing delegated clinical peer review functions has no history of revocation, suspension or limitation to practice their health care discipline; no sanction or disciplinary action within the past five years by their licensing board; no history of malpractice claims or convictions; and no history of felony convictions.
6.4.12 Contract must specify that any person deemed by the CID Credentialing Committee to be unqualified or unsuitable as a clinical peer reviewer shall be prohibited from performing any delegated functions of clinical peer review on behalf of CID.
6.4.13 Contract must specify that documentation described in 6.4.11 and 6.4.12 shall be provided to the CID Credentialing Committee at least annually for re-credentialing of each person performing delegated clinical peer review functions.
6.4.14 Contract must specify that all persons directly involved in performing delegated clinical peer review functions must be provided with all job-specific training materials available to CID clinical peer reviewers.
6.5 The Clinical Director shall perform periodic assessments for each vendor staff
member performing delegated clinical peer review functions. These periodic assessments shall occur, at minimum, at the following times:
6.5.1 After 3 months of performing delegated clinical peer review functions for
CID 6.5.2 After 6 months of performing delegated clinical peer review functions for
CID 6.5.3 After 1 year of performing delegated clinical peer review functions for
CID, and yearly thereafter.
6.6 The assessment of vendor staff undertaken by the Clinical Director shall consist of review of a minimum of 5 reviews on which the vendor staff member worked, using the attached form to grade their performance.

2240-4
6.7 The Clinical Director shall incorporate the outcomes of vendor staff assessment into annual reporting to the QAQC Committee.
6.8 No clinical peer review functions shall be delegated for emergency, urgent, expedited or concurrent reviews.
6.9 All reviews for which clinical peer reviewer functions have been delegated to a non-CID contracted vendor shall be verified for correctness and accuracy by a CID QAQC reviewer prior to release of any determination letters.

2300-1
CID Management
QAQC Reviewer Credentialing
Policy No. 2300 Revision: 3.2 Revision Date: 3/11/2011 Page 1 of 5
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which QAQC reviewers contracted with CID to perform utilization management operations are credentialed.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.1 04/20/2008 Revised Revision 3.1 05/14/2009 Reviewed Revision 3.1 06/08/2010 Reviewed Revision 3.1 01/27/2011 Reviewed Revision 3.2 03/11/2011 Revised Revision 3.2 04/22/2012 Reviewed Revision 3.2 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all QAQC reviewers contracted with CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to perform credentialing on all QAQC reviewers upon initial contracting. It is further the policy of CID Management to perform re-credentialing on all QAQC reviewers on a yearly basis.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
2300-2
6.1 If, following the interview process, CID has determined that the candidate is a viable choice for the position and that a contract offer is desired, prior to making a contract offer the Recruiter of Clinical Personnel shall perform an initial credentialing check.
6.2 The initial credentialing check by the Recruiter of Clinical Personnel shall include
primary source verification as appropriate including any, or all, of the following: 6.2.1 State licensing boards -- validating the practitioner's license to practice
and confirming whether there are any sanctions against the license. 6.2.2 Schools/training programs - validating the practitioner's highest level of
training in his/her specialty and validating board certification status with the American Board of Medical Specialties.
6.2.3 National Technical Information Service (NTIS) -- validating the
practitioner's license to prescribe drugs. The certificates reviewed are the Drug Enforcement Agency (DEA) certificate or Controlled Drug Substance Registration (CDS).
6.2.4 Medicare/Medicaid - determining whether sanctions have been imposed
by the federal government's Office of Inspector General (OIG) or Office of Personnel Management (OPM).
6.2.5 Malpractice history - reviewing claims history.
6.3 The Recruiter of Clinical Personnel shall evaluate to determine if the candidate meets
the following inclusion criteria: 6.3.1 Has undergone formal training in a health care field
6.3.2 Holds an associates degree in a health care field, or holds a state license,
or state certificate in a health care field,
6.3.3 Has professional experience in providing direct patient care,
6.3.4 Holds a current unrestricted license to practice in a health care field
6.3.5 Has an acceptable malpractice history.
6.4 The Recruiter of Clinical Personnel shall also evaluate to determine if the candidate meets the following exclusion criteria:
6.4.1 Has a history of revocation, suspension or limitation to practice their health care discipline,
6.4.2 Has a sanction or disciplinary action within the past five years by their
licensing board,
2300-3
6.4.3 Has an unacceptable malpractice history,
6.4.4 Has a history of felony convictions.
6.5 If, upon initial credentialing, the Recruiter of Clinical Personnel discovers that the
candidate meets all inclusion criteria as outlined in CID Policy 2300, and does not meet any exclusion criteria as outlined in CID Policy 2300, the Recruiter of Clinical Personnel shall forward documentation from primary verification sources to the Director of Clinical Personnel. The Director of Clinical personnel shall also verify that the candidate meets all inclusion criteria from CID Policy 2300 and none of the exclusion from CID Policy 2300 The Director of Clinical Personnel shall conclude that the candidate has passed the credentialing process and shall disclose this information to the Recruiter of Clinical Personnel and Clinical Director.
6.6 If, upon initial credentialing, the Recruiter of Clinical Personnel or the Director of
Clinical Personnel discovers any item that precludes the candidate from meeting all inclusion criteria as outlined in CID Policy 2300, or any item that matches any exclusion criteria as outlined in CID Policy 2300, the Recruiter of Clinical Personnel or the Director of Clinical Personnel shall conclude that the candidate has not passed the credentialing process and shall disclose this information to the Recruiter of Clinical Personnel; the Director of Clinical Personnel; and Clinical Director. The party providing such disclosure shall further indicate the principle reason(s) the candidate did not pass the credentialing process.
6.7 If the candidate successfully passed the credentialing process, the Recruiter of
Clinical Personnel; the Director of Clinical Personnel; or the Clinical Director shall contact the candidate with a contract offer.
6.8 If the candidate has not passed the credentialing process, the Director of Clinical
Personnel or Clinical Director shall contact the candidate to inform him/her that no contract offer will be made and provide the candidate of the principle reason(s) he/she did not pass the credentialing process.
6.9 The candidate shall have the opportunity to respond to the principle reason(s);
however in absence of proving the unsuccessful attempt at credentialing was due to incorrect information, the credentialing decision shall stand.
6.10 The Director of Clinical Personnel shall insure that a re-credentialing of all initial
clinical reviewers is performed by the Director of Clinical Personnel or a Recruiter of Clinical Personnel at regular intervals, not to exceed 1 year and no later than scheduled expiration of licensure/certification. The performance of this credentialing shall include primary source verification as appropriate including any, or all, of the following:
2300-4
6.10.1 State licensing boards -- validating the practitioner's license to practice and confirming whether there are any sanctions against the license.
6.10.2 Validating board certification status with the American Board of Medical
Specialties.
6.10.3 National Technical Information Service (NTIS) -- validating the practitioner's license to prescribe drugs. The certificates reviewed are the Drug Enforcement Agency (DEA) certificate or Controlled Drug Substance Registration (CDS).
6.10.4 Medicare/Medicaid - determining whether sanctions have been imposed
by the federal government's Office of Inspector General (OIG) or Office of Personnel Management (OPM).
6.10.5 Malpractice history - reviewing claims history.
6.11 The periodic re-credentialing evaluation shall determine if the initial clinical
reviewer continues to meet all of the inclusion criteria from CID Policy 2300; and shall determine that the initial clinical reviewer meets none of the exclusion criteria from CID Policy 2300.
6.12 If, upon re-credentialing, the Director of Clinical Personnel or a Recruiter of
Clinical Personnel discovers that the QAQC reviewer meets all inclusion criteria as outlined in CID Policy 2300, and does not meet any exclusion criteria as outlined in CID Policy 2300, the Director of Clinical Personnel or a Recruiter of Clinical Personnel shall conclude that the QAQC reviewer has passed the credentialing process and shall document this in the QAQC reviewer’s personnel file.
6.13 If, upon re-credentialing, the Director of Clinical Personnel or a Recruiter of
Clinical Personnel discovers any item that precludes the QAQC reviewer from meeting all inclusion criteria as outlined in CID Policy 2300, or any item that matches any exclusion criteria as outlined in CID Policy 2300, the Director of Clinical Personnel or a Recruiter of Clinical Personnel shall conclude that the QAQC reviewer has not passed the credentialing process and shall disclose this information to the Director of Clinical Personnel and the Clinical Director. Such disclosure shall further include the principle reason(s) the QAQC reviewer did not pass the re-credentialing process.
6.14 If the QAQC reviewer has not passed the re-credentialing process, the Medical
Director or Clinical Director shall contact the QAQC reviewer to inform him/her that his/her contract will be terminated and provide the QAQC reviewer of the principle reason(s) he/she did not pass the credentialing process.
6.15 The QAQC reviewer shall have the opportunity to respond to the principle
reasons, however in absence of proving the unsuccessful attempt at re-credentialing

2300-5
was due to incorrect information, the credentialing decision and contract termination shall stand.

2310-1
CID Management
QAQC Reviewer Initial Paperwork
Policy No. 2310 Revision: 3.0 Revision Date: 3/16/2011 Page 1 of 3
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines for paperwork required to be signed by QAQC reviewer prior to being contracted with CID to perform utilization management operations.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy and Forms/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 05/14/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 01/27/2011 Reviewed Revision 3.0 03/16/2011 Revised Revision 3.0 04/22/2012 Revised Revision 3.0 01/22/2013 Revised
3.0 Persons Affected This policy affects all QAQC reviewer members contracted by CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to require the following items to be completed by all QAQC reviewer members contracted by CID to perform utilization management operations prior to commencement of the contractor relationship:
4.1 QAQC reviewer contract 4.2 Non-disclosure agreement 4.3 CID/business associate HIPAA agreement
4.4 Conflict of interest form
2310-2
4.5 W9 or W2, as applicable
It is further the policy of CID Management to require the following items be submitted by all QAQC reviewers contracted by CID to perform utilization management operations prior to commencement of the contractor relationship:
4.6 Copy of current health care provider licenses
4.7 Listing of all active and inactive health care provider licenses ever held 4.8 Copy of current malpractice insurance policy coversheet
4.9 Disclosure of all prior disciplinary actions taken by health care licensing boards as
well as any prior malpractice actions.
4.10 Completed Electronic Signature Form.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
6.1 Upon official offer of an contractor position, CID shall request the candidate provide the following documents:
6.1.1 Copy of current curriculum vitae, if available
6.1.2 Copy of current health care provider licenses
6.1.3 Listing of all active and inactive health care provider licenses ever held
6.1.4 Copy of current malpractice insurance policy coversheet
6.1.5 Disclosure of all prior disciplinary actions taken by health care licensing
boards as well as any prior malpractice actions.
6.1.6 Completed Electronic Signature Form.
6.2 Upon official offer of an contractor position, CID shall provide the candidate with a copy of, and shall review, explain and answer any questions from the candidate regarding the following documents:
6.2.1 QAQC reviewer contract
2310-3
6.2.2 Non-disclosure agreement 6.2.3 CID/business associate HIPAA agreement
6.2.4 Conflict of interest form 6.2.5 W9 or W2, as applicable
6.3 The candidate shall have all the time they feel they require to review the documents
and ask questions of CID. 6.4 Upon receipt of all documents listed in 6.1 and receipt of all completed documents
listed in section 6.2, the contractor shall begin employment at CID.
2320-1
CID Management
QAQC Reviewer Training
Policy No. 2320 Revision: 4.0 Revision Date: 1/29/2008 Page 1 of 3
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines for training provided to QAQC reviewers contracted with CID to perform utilization management operations.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 05/24/2006 Addition of training in URAC standards Revision 3.0 08/26/2006 Revised Revision 4.0 06/05/2007 Revised Revision 5.0 01/29/2008 Revised Revision 5.0 05/14/2009 Reviewed Revision 5.0 06/08/2010 Reviewed Revision 5.0 01/27/2011 Reviewed Revision 5.0 04/22/2012 Reviewed Revision 5.0 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all QAQC reviewers contracted with CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to provide QAQC reviewers, contracted with CID to perform utilization management operations, with the following training sessions:
4.1 Introduction to CID 4.2 Introduction to workers’ compensation 4.3 Introduction to utilization management
4.3.1 Overview of utilization management
2320-2
4.3.2 Labor code, regulations, and case law regarding utilization management 4.3.3 CID’s utilization management process
4.3.4 URAC utilization management standards
4.4 Conflict of interest policies and procedures 4.5 Confidentiality policies and procedures
4.6 Job specific training 4.7 Periodic Training Updates as required including:
4.7.1 Changes to the CID utilization management process 4.7.2 Changes to labor code, regulations, or case law regarding utilization
management 4.8 Training on identification and prevention of fraud and abuse, as appropriate to job
functions
4.9 Re-Training on an annual basis.
5.0 Definitions
Definitions of terms are set forth in Policy 1000. 6.0 Procedures
6.1 Upon hire, the Clinical Director or Senior Clinical Staff shall schedule the following
training sessions for the new QAQC reviewer contractor:
6.1.1 Introduction to CID 6.1.2 Introduction to workers’ compensation 6.1.3 Introduction to utilization management
6.1.3.1 Overview of utilization management
6.1.3.2 Labor code, regulations, and case law regarding utilization
management
6.1.3.3 CID’s utilization management process
2320-3
6.1.3.4 URAC utilization management standards
6.1.4 Conflict of interest policies and procedures
6.1.5 Confidentiality policies and procedures
6.1.6 Job specific training
6.1.7 Identification of fraud and abuse
6.2 Completion of each training session in section 6.1 shall be logged into the QAQC
reviewer’s personnel file by the Clinical Director or Senior Clinical Staff. 6.3 As needed, the Clinical Director or Senior Clinical Staff shall schedule periodic
training updates for all QAQC reviewers. 6.4 Completion of periodic training updates may be logged into the QAQC reviewer’s
personnel file at the discretion of the Clinical Director or Senior Clinical Staff. 6.5 If the Clinical Director or Senior Clinical Staff notes an area of performance in which
the QAQC reviewer is not adhering to CID’s policies and procedures, or in which the job duties are being performed in an unacceptable fashion, the Clinical Director or Senior Clinical Staff shall schedule re-training. The reason for the re-training shall be logged into the QAQC reviewer’s personnel file by the Clinical Director or Senior Clinical Staff.
6.6 Completion of each re-training session shall be logged into the QAQC reviewer’s
personnel file by the Clinical Director or Senior Clinical Staff. 6.7 If QAQC committee notes an area of performance in which the QAQC reviewer is
not adhering to CID’s policies and procedures, or in which the job duties are being performed in an unacceptable fashion, they shall communicate this to the QAQC reviewer and the Clinical Director or Senior Clinical Staff. The Clinical Director or Senior Clinical Staff shall schedule re-training. The reason for the re-training shall be logged into the QAQC reviewer’s personnel file by the Clinical Director or Senior Clinical Staff.
6.8 Completion of each re-training session shall be logged into the QAQC reviewer’s
personnel file by the Clinical Director or Senior Clinical Staff.

2330-1
CID Management
QAQC Reviewer Assessment
Policy No. 2330 Revision: 4.1 Revision Date: 3/11/2011 Page 1 of 3
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which QAQC reviewers shall undergo assessment.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy and Forms/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 4.0 05/14/2009 Revised Revision 4.0 06/08/2010 Reviewed Revision 4.0 01/27/2011 Reviewed Revision 4.1 03/11/2011 Revised Revision 4.1 04/22/2012 Revised Revision 4.1 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all QAQC reviewers employed by, or contracted with, CID Management.
4.0 Policy The policy of CID Management is to perform ongoing assessment of QAQC reviewers to identify strengths as well as areas in need of improvement. It is further the policy of CID Management to work with the QAQC reviewers at the time of the assessment to create a personal development plan that the QAQC reviewers shall endeavor to complete prior to the following scheduled assessment.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
2330-2
6.1 The Clinical Director or Senior Clinical Staff shall conduct periodic assessments for each QAQC reviewer. The periodic assessments shall occur with reference to the following intervals:
6.1.1 At the 3 month anniversary with CID 6.1.2 At the 6 month anniversary with CID 6.1.3 At the 1 year anniversary with CID, and yearly thereafter.
6.2 The scheduled assessment will include consideration of reviews on which the initial reviewer worked, using the attached form to grade their performance. The performance assessment forms will be completed by the Clinical Director or Senior Clinical Staff. Whenever possible, a minimum of 5 reviews on which the QAQC reviewer worked should be considered during each assessment interval.
6.3 As review assessments are completed, the Clinical Director or Senior Clinical Staff
member who completed the assessment shall provide the assessment form and the draft assessed to the QAQC reviewer, with explanations of all noted issues. The Clinical Director or Senior Clinical Staff member who completed the assessment shall invite the initial reviewer to discuss any questions or concerns regarding the assessment; and shall be available for such discussion.
6.4 In the event that an initial reviewer is noted to have similar performance issues on a
consistent or repetitive basis, the Clinical Director or Director of Clinical Training and Assessment shall make available appropriate re-training resources.
6.5 The Clinical Director or Director of Clinical Training and Assessment shall place a
copy of each assessment form in the QAQC reviewer’s personnel file.
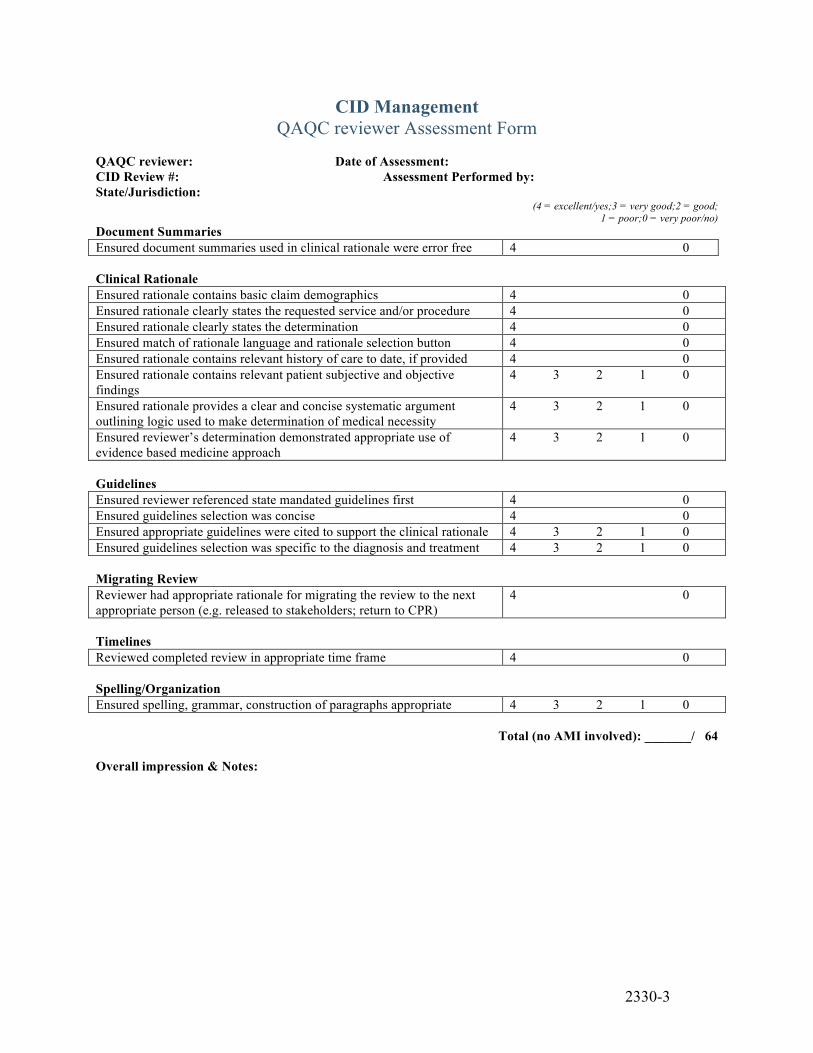
2330-3
CID Management QAQC reviewer Assessment Form
QAQC reviewer: Date of Assessment: CID Review #: Assessment Performed by: State/Jurisdiction:
(4 = excellent/yes;3 = very good;2 = good; 1 = poor;0 = very poor/no)
Document Summaries Ensured document summaries used in clinical rationale were error free 4 0 Clinical Rationale Ensured rationale contains basic claim demographics 4 0 Ensured rationale clearly states the requested service and/or procedure 4 0 Ensured rationale clearly states the determination 4 0 Ensured match of rationale language and rationale selection button 4 0 Ensured rationale contains relevant history of care to date, if provided 4 0 Ensured rationale contains relevant patient subjective and objective findings
4 3 2 1 0
Ensured rationale provides a clear and concise systematic argument outlining logic used to make determination of medical necessity
4 3 2 1 0
Ensured reviewer’s determination demonstrated appropriate use of evidence based medicine approach
4 3 2 1 0
Guidelines Ensured reviewer referenced state mandated guidelines first 4 0 Ensured guidelines selection was concise 4 0 Ensured appropriate guidelines were cited to support the clinical rationale 4 3 2 1 0 Ensured guidelines selection was specific to the diagnosis and treatment 4 3 2 1 0 Migrating Review Reviewer had appropriate rationale for migrating the review to the next appropriate person (e.g. released to stakeholders; return to CPR)
4 0
Timelines Reviewed completed review in appropriate time frame 4 0 Spelling/Organization Ensured spelling, grammar, construction of paragraphs appropriate 4 3 2 1 0
Total (no AMI involved): _______/ 64 Overall impression & Notes:

2340-1
CID Management
Delegation of QA/QC Review Functions
Policy No. 2340 Revision: 1.0 Revision Date: 4/20/2008 Page 1 of 1
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines establishing requirements for delegation of functions performed by QA/QC reviewers to a non-CID vendor.
2.0 Revision History
Revision 1.0 04/202008 New Policy & Form/Initial Implementation Revision 1.0 05/14/2009 Reviewed Revision 1.0 06/08/2010 Reviewed Revision 1.0 01/27/2011 Reviewed Revision 1.0 04/22/2012 Reviewed Revision 1.0 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all QAQC reviewers contracted with CID to perform utilization management operations.
4.0 Policy The policy of CID Management is to ensure that all QA/QC review functions will be performed by QA/QC reviewers employed by CID.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 There shall be no contractual delegation of QA/QC review functions to any vendor.
All such functions shall be provided by QA/QC reviewers employed by CID.

3000-1
CID Management
Receipt of Request For Authorization
Policy No. 3000 Revision: 4.1 Revision Date: 3/11/2011 Page 1 of 5
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which CID may receive requests for authorization.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 4.0 01/29/2008 Revised Revision 4.0 05/14/2009 Reviewed Revision 4.0 06/08/2010 Reviewed Revision 4.1 03/11/2011 Revised Revision 4.1 04/24/2012 Reviewed Revision 4.1 01/09/2013 Reviewed
3.0 Persons Affected This policy affects CID non-clinical administrative staff whose job duties include receipt of requests for utilization management services.
4.0 Policy The policy of CID Management is to allow clients to specify whether requests for authorization may only be processed if received from the claim administrator directly or if they may be processed if received from any other stakeholder which may include, but is not limited to: the requesting physician, the claims adjustor, the facility rendering the service, the provider, or a state regulator. CID reserves the right to edit the client’s list to comply with any applicable state labor code or regulation.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
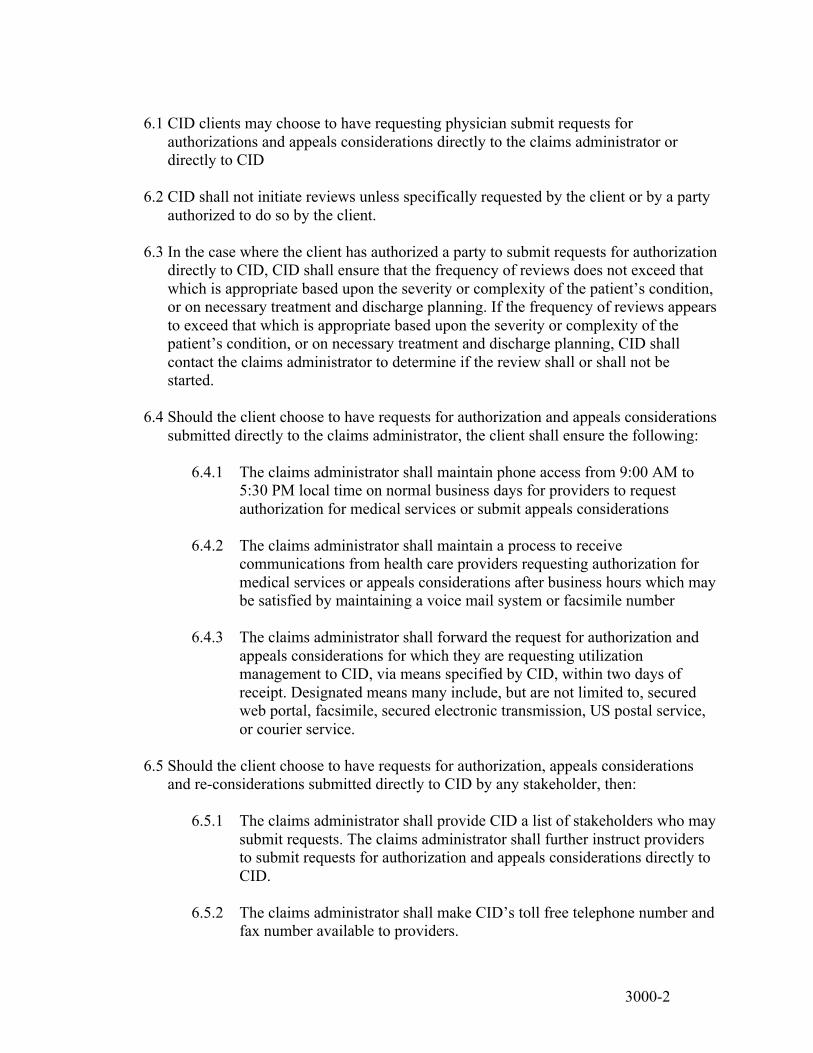
3000-2
6.1 CID clients may choose to have requesting physician submit requests for
authorizations and appeals considerations directly to the claims administrator or directly to CID
6.2 CID shall not initiate reviews unless specifically requested by the client or by a party
authorized to do so by the client. 6.3 In the case where the client has authorized a party to submit requests for authorization
directly to CID, CID shall ensure that the frequency of reviews does not exceed that which is appropriate based upon the severity or complexity of the patient’s condition, or on necessary treatment and discharge planning. If the frequency of reviews appears to exceed that which is appropriate based upon the severity or complexity of the patient’s condition, or on necessary treatment and discharge planning, CID shall contact the claims administrator to determine if the review shall or shall not be started.
6.4 Should the client choose to have requests for authorization and appeals considerations
submitted directly to the claims administrator, the client shall ensure the following: 6.4.1 The claims administrator shall maintain phone access from 9:00 AM to
5:30 PM local time on normal business days for providers to request authorization for medical services or submit appeals considerations
6.4.2 The claims administrator shall maintain a process to receive
communications from health care providers requesting authorization for medical services or appeals considerations after business hours which may be satisfied by maintaining a voice mail system or facsimile number
6.4.3 The claims administrator shall forward the request for authorization and
appeals considerations for which they are requesting utilization management to CID, via means specified by CID, within two days of receipt. Designated means many include, but are not limited to, secured web portal, facsimile, secured electronic transmission, US postal service, or courier service.
6.5 Should the client choose to have requests for authorization, appeals considerations
and re-considerations submitted directly to CID by any stakeholder, then: 6.5.1 The claims administrator shall provide CID a list of stakeholders who may
submit requests. The claims administrator shall further instruct providers to submit requests for authorization and appeals considerations directly to CID.
6.5.2 The claims administrator shall make CID’s toll free telephone number and
fax number available to providers.

3000-3
6.5.3 Each claims administrator shall record a message on their voice mail
message directing parties to submit requests for authorization and appeals considerations directly to CID and provide CID’s toll free telephone number and fax number.
6.5.4 CID shall maintain phone access from 9:00 AM to 5:30 PM in all time
zones in which CID conducts utilization management functions, on normal business days for parties to request authorization for medical services and appeals considerations.
6.5.5 CID shall maintain a process to receive communications from parties
requesting authorization for medical services and appeals considerations after business hours which may be satisfied by maintaining a voice mail system or facsimile number.
6.6 Written requests for authorization shall be deemed to have been received by facsimile
on the date the request was received if the receiving facsimile electronically date stamps the transmission. If there is no electronically stamped date recorded, then the date of receipt shall be deemed to be the date the request was transmitted. A request for authorization transmitted by facsimile after 5:30 P.M. local time shall be deemed to have been received on the following business day.
6.7 Where the request for authorization is received by mail and a proof of service by mail
exists, the request shall be deemed to have been received five (5) days after the deposit in the mail at a facility regularly maintained by the United States Postal Service. Where the request is delivered via certified mail, return receipt mail, the request shall be deemed to have been received on the receipt date entered on the return receipt. In the absence of a proof of service by mail or a dated return receipt, the request shall be deemed to have been received on the date the documentation was uploaded to the CID system (e.g., electronic date stamp).
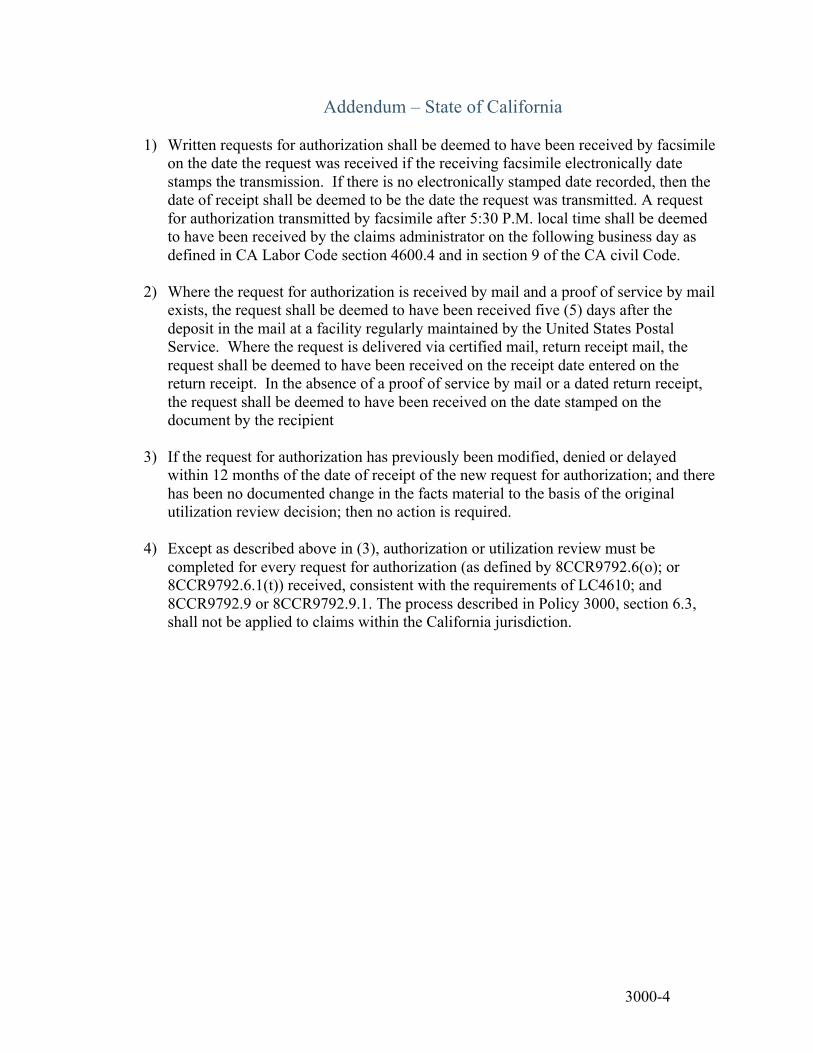
3000-4
Addendum – State of California
1) Written requests for authorization shall be deemed to have been received by facsimile on the date the request was received if the receiving facsimile electronically date stamps the transmission. If there is no electronically stamped date recorded, then the date of receipt shall be deemed to be the date the request was transmitted. A request for authorization transmitted by facsimile after 5:30 P.M. local time shall be deemed to have been received by the claims administrator on the following business day as defined in CA Labor Code section 4600.4 and in section 9 of the CA civil Code.
2) Where the request for authorization is received by mail and a proof of service by mail exists, the request shall be deemed to have been received five (5) days after the deposit in the mail at a facility regularly maintained by the United States Postal Service. Where the request is delivered via certified mail, return receipt mail, the request shall be deemed to have been received on the receipt date entered on the return receipt. In the absence of a proof of service by mail or a dated return receipt, the request shall be deemed to have been received on the date stamped on the document by the recipient
3) If the request for authorization has previously been modified, denied or delayed within 12 months of the date of receipt of the new request for authorization; and there has been no documented change in the facts material to the basis of the original utilization review decision; then no action is required.
4) Except as described above in (3), authorization or utilization review must be completed for every request for authorization (as defined by 8CCR9792.6(o); or 8CCR9792.6.1(t)) received, consistent with the requirements of LC4610; and 8CCR9792.9 or 8CCR9792.9.1. The process described in Policy 3000, section 6.3, shall not be applied to claims within the California jurisdiction.

3005-1
CID Management
Telephonic Inquiry Regarding Utilization Management Services
Policy No. 3005 Revision: 3.0 Revision Date: 6/5/07 Page 1 of 2
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which telephonic inquiries regarding utilization management services shall be addressed.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 05/14/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 03/14/2011 Reviewed Revision 3.0 04/24/2012 Reviewed Revision 3.0 01/17/2013 Reviewed
3.0 Persons Affected This policy affects CID non-clinical administrative staff whose job duties include answering telephone calls and emails which may include inquiries regarding the utilization management process.
4.0 Policy The policy of CID Management is to train the non-clinical administrative staff to respond to non-clinical questions regarding the utilization management process.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 Upon receipt of a non-clinical question regarding the utilization management process,
non-clinical administrative staff shall respond to the inquiry giving as much detail as
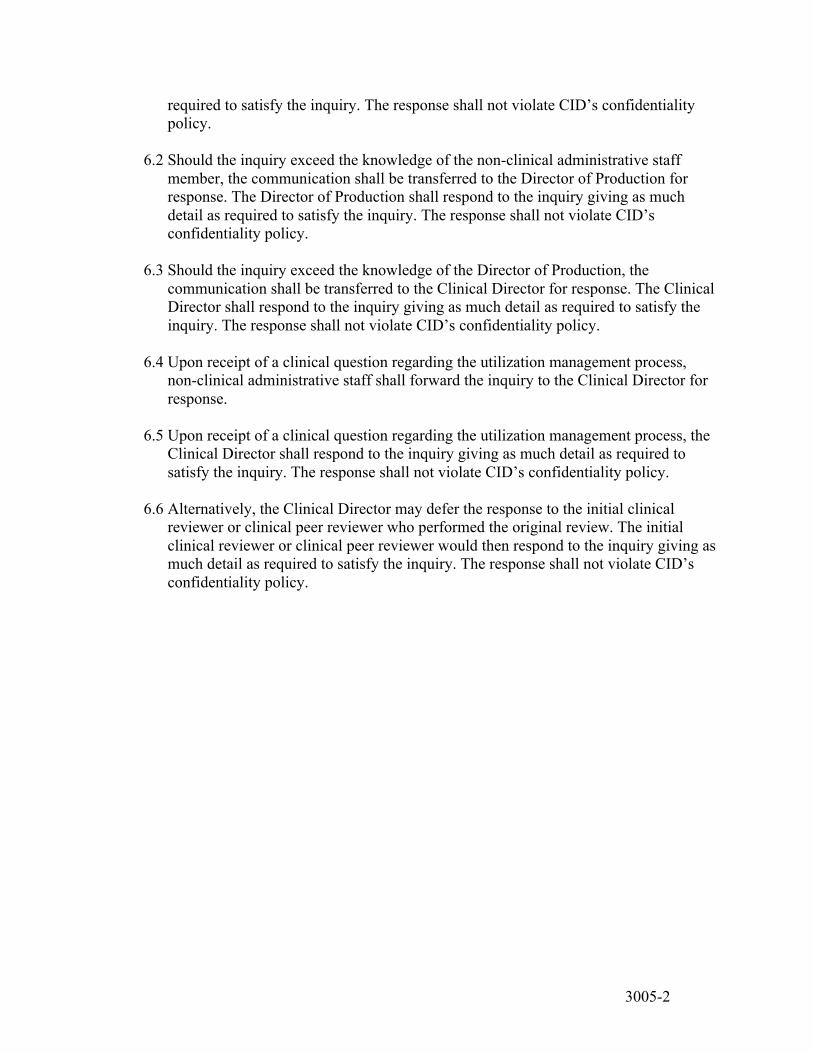
3005-2
required to satisfy the inquiry. The response shall not violate CID’s confidentiality policy.
6.2 Should the inquiry exceed the knowledge of the non-clinical administrative staff
member, the communication shall be transferred to the Director of Production for response. The Director of Production shall respond to the inquiry giving as much detail as required to satisfy the inquiry. The response shall not violate CID’s confidentiality policy.
6.3 Should the inquiry exceed the knowledge of the Director of Production, the
communication shall be transferred to the Clinical Director for response. The Clinical Director shall respond to the inquiry giving as much detail as required to satisfy the inquiry. The response shall not violate CID’s confidentiality policy.
6.4 Upon receipt of a clinical question regarding the utilization management process,
non-clinical administrative staff shall forward the inquiry to the Clinical Director for response.
6.5 Upon receipt of a clinical question regarding the utilization management process, the
Clinical Director shall respond to the inquiry giving as much detail as required to satisfy the inquiry. The response shall not violate CID’s confidentiality policy.
6.6 Alternatively, the Clinical Director may defer the response to the initial clinical
reviewer or clinical peer reviewer who performed the original review. The initial clinical reviewer or clinical peer reviewer would then respond to the inquiry giving as much detail as required to satisfy the inquiry. The response shall not violate CID’s confidentiality policy.

3010-1
CID Management
Utilization Management Electronic Review File
Policy No. 3010 Revision: 3.0 Revision Date: 6/5/07 Page 1 of 6
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines for the electronic review file.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 05/14/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 03/14/2011 Reviewed Revision 3.0 04/24/2012 Reviewed Revision 3.0 01/17/2013 Reviewed
3.0 Persons Affected This policy affects CID non-clinical administrative staff and clinical staff.
4.0 Policy The policy of CID Management is to create an electronic review file for each request for authorization, appeals consideration, or re-consideration received. It is further the policy of CID Management to capture all information and documents relevant to the request for authorization, appeals determination, or re-consideration as a component of the electronic review file. It is further the policy of CID Management to create a link between reviews for a given claim to allow reviewers access to all prior information received on a claim to avoid duplicate requests for information from providers.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures

3010-2
6.1 Once a request for authorization, appeals consideration, or re-consideration has been submitted to CID, the non-clinical administrative staff shall evaluate the submission using the following steps:
6.1.1 If the request for authorization or appeals consideration has been
submitted to CID directly from the claims administrator, the non-clinical administrative staff shall: 6.1.1.1 Review the information submitted to ensure that the claims
administrator has provided the necessary information required to create an electronic review file. The necessary information may include, but is not limited to: 6.1.1.1.1 Compensability of the claim 6.1.1.1.2 Patient demographic information, 6.1.1.1.3 Provider demographic information, 6.1.1.1.4 Applicant attorney demographic information, 6.1.1.1.5 Defense attorney demographic information, 6.1.1.1.6 Workers’ compensation claim demographic
information, 6.1.1.1.7 Pre-review screening information collected by the
client, 6.1.1.1.8 Specific request for authorization or appeals
consideration for which the client is requesting utilization management
6.1.1.2 If the necessary information is not present, the non-clinical
administrative staff shall contact the claim administrator to request the additional information. This communication may occur via phone call, electronic means, or fax, and shall be logged into the CID system. 6.1.1.2.1 If the requested additional information is received, the
non-clinical administrative staff shall proceed to point 6.1.1.3
6.1.1.2.2 If the requested additional information is not received
within 1 business day, the non-clinical administrative staff shall contact the claim administrator again to

3010-3
request the additional information. This communication may occur via phone call, electronic means, or fax, and shall be logged into the CID system. Contacts will be made at a frequency of 1 time per day until the necessary information is received.
6.1.1.3 If the necessary information is present, the non-clinical
administrative staff shall utilize the CID secured web-site and proprietary software to create an electronic review file for the request for authorization, appeals consideration, or re-consideration.
6.1.1.4 Based on the specific medical discipline of the review, the CID
system shall automatically assign the review to the appropriate initial clinical reviewer or to a clinical peer reviewer based upon criteria set forth by the Medical and/or Clinical Directors.
6.1.2 If the request for authorization or appeals consideration has been
submitted to CID directly from any party other than the claims administrator, the non-clinical administrative staff shall: 6.1.2.1 Verify that the party submitting the request is permitted to do so as
per CID policies or the contract with the client, taking into consideration CID’s right to edit this list to comply with state labor code and regulations.
6.1.2.1.1 If the party is permitted to do so, the non-clinical
administrative staff member shall proceed to 6.1.2.2 6.1.2.1.2 If the party is not permitted to do so, then the non-
clinical administrative staff member shall contact the submitting party and inform them that client has not authorized CID to receive requests from that party and that they must contact the claims administrator directly.
6.1.2.2 Log onto the client’s electronic claims management system via
secured link to gather the following information: 6.1.2.2.1 Compensability of claim 6.1.2.2.2 Patient demographic information, 6.1.2.2.3 Provider demographic information, 6.1.2.2.4 Applicant attorney demographic information,
3010-4
6.1.2.2.5 Defense attorney demographic information, 6.1.2.2.6 Workers’ compensation claim demographic
information. 6.1.2.3 Review the information submitted to ensure that the provider has
clearly outlined the specific course of proposed medical treatment for which authorization or appeals consideration was requested
6.1.2.4 If the specific course of proposed medical treatment for which
authorization or appeals consideration was requested is not clear, the non-clinical administrative staff shall utilize the CID secured web-site and proprietary software to create an electronic review file for the request for authorization or appeals consideration. Using the CID software, the non-clinical administrative staff member shall then fax the provider requesting clarification of the specific course of proposed medical treatment for which authorization or appeals consideration was requested
6.1.2.5 If the specific course of proposed medical treatment for which
authorization or appeals consideration was requested is clear, the non-clinical administrative staff shall utilize the CID secured web-site and proprietary software to create an electronic review file for the request for authorization or appeals consideration.
6.1.2.6 Based on the specific medical discipline of the review, the CID
system shall automatically assign the review to the appropriate initial clinical reviewer or to a clinical peer reviewer based upon criteria set forth by the Medical and/or Clinical Directors
6.2 The electronic review file shall contain:
6.2.1 A specific review number 6.2.2 The type and category of the review 6.2.3 The names, contact information, and relationship to the review for each
review stakeholder including, but not limited to: 6.2.3.1 Patient 6.2.3.2 Patient’s legal counsel
6.2.3.3 Claims administrator
6.2.3.4 Client appointed personnel including, but not limited to:
3010-5
6.2.3.4.1 Claims assistants 6.2.3.4.2 Claims supervisor
6.2.3.4.3 Medical management staff
6.2.3.5 Defense legal counsel
6.2.3.6 Requesting physician
6.2.3.7 Attending physician
6.2.3.8 Secondary physicians
6.2.3.9 Non-physician providers of goods and/or services
6.2.3.10 Non-clinical administrative staff member
6.2.3.11 Initial clinical reviewer
6.2.3.12 Clinical peer reviewer
6.2.3.13 QAQC reviewer
6.2.4 All relevant dates for the review including, but not limited to:
6.2.4.1 Date client received request 6.2.4.2 Date claims administrator requested additional information, if
applicable
6.2.4.3 Date claims administrator received additional information, if applicable
6.2.4.4 Date CID received request
6.2.4.5 Date CID requested additional information, if applicable
6.2.4.6 Date CID received additional information, if applicable
6.2.4.7 Date review was placed on hold, if applicable
6.2.4.8 Date review was released from hold, if applicable
6.2.4.9 Dates administrative processing of review began and ended
3010-6
6.2.4.10 Dates initial clinical review began and ended
6.2.4.11 Dates clinical peer review began and ended
6.2.4.12 Dates QAQC review began and ended
6.2.4.13 Date request was released to the client
6.2.4.14 Date request was released to all stakeholders
6.2.4.15 Date request was withdrawn, if applicable.
6.2.5 All documents received for the review 6.2.6 All documents generated for the review by CID 6.2.7 All activities performed on the review including, but not limited to:
6.2.7.1 Creation of review 6.2.7.2 Uploading of any documents 6.2.7.3 Generation of any documents 6.2.7.4 Distribution of any correspondences 6.2.7.5 Receipt of any communications including email, telephone calls,
faxes, or mail 6.2.7.6 Initiation of any emails, telephone calls, faxes or mail 6.2.7.7 Record of discussion with any person via telephone 6.2.7.8 Copy of any email sent or received.
6.2.8 A link to all previous reviews completed on the claim, and a link to all
previous documents received for the claim, to provide the clinical staff access to all previous documents received in order to avoid duplicate requests for information from providers.
3100-1
CID Management
Pre-Review Screening
Policy No. 3100 Revision: 4.0 Revision Date: 4/11/2011 Page 1 of 5
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which pre-review screening may be done.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy and Form/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 05/14/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 03/14/2011 Reviewed Revision 4.0 04/11/2011 Revised Revision 4.0 04/24/2012 Reviewed Revision 4.0 01/09/2013 Reviewed
3.0 Persons Affected This policy affects all CID employees and contractors whose job duties include pre-review screening.
4.0 Policy The policy of CID Management is to allow non-clinical administrative staff to perform pre-review screening provided that that pre-review screening is limited to the collection of non-clinical data or provided that the collection of clinical data occurs following scripts approved by the CID medical director. It is further the policy of CID Management that non-certifications shall not be issued solely on the basis of pre-review screening.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures
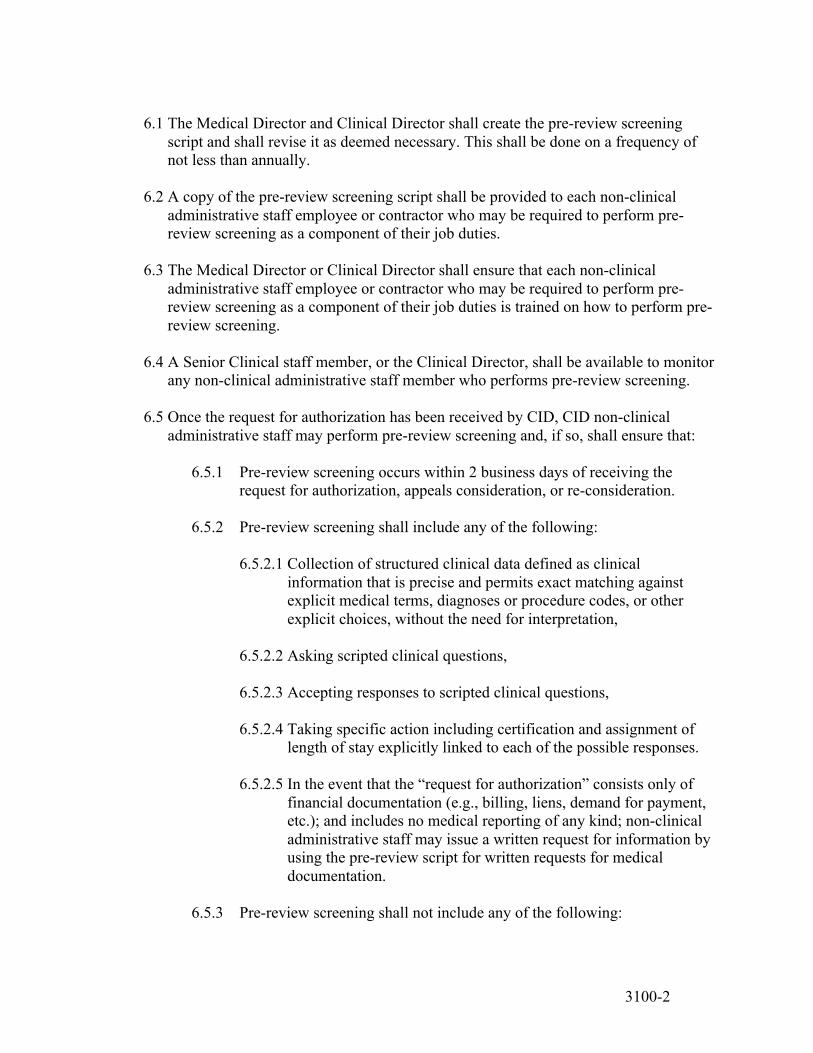
3100-2
6.1 The Medical Director and Clinical Director shall create the pre-review screening
script and shall revise it as deemed necessary. This shall be done on a frequency of not less than annually.
6.2 A copy of the pre-review screening script shall be provided to each non-clinical
administrative staff employee or contractor who may be required to perform pre-review screening as a component of their job duties.
6.3 The Medical Director or Clinical Director shall ensure that each non-clinical
administrative staff employee or contractor who may be required to perform pre-review screening as a component of their job duties is trained on how to perform pre-review screening.
6.4 A Senior Clinical staff member, or the Clinical Director, shall be available to monitor
any non-clinical administrative staff member who performs pre-review screening.
6.5 Once the request for authorization has been received by CID, CID non-clinical administrative staff may perform pre-review screening and, if so, shall ensure that:
6.5.1 Pre-review screening occurs within 2 business days of receiving the request for authorization, appeals consideration, or re-consideration.
6.5.2 Pre-review screening shall include any of the following:
6.5.2.1 Collection of structured clinical data defined as clinical
information that is precise and permits exact matching against explicit medical terms, diagnoses or procedure codes, or other explicit choices, without the need for interpretation,
6.5.2.2 Asking scripted clinical questions,
6.5.2.3 Accepting responses to scripted clinical questions,
6.5.2.4 Taking specific action including certification and assignment of
length of stay explicitly linked to each of the possible responses.
6.5.2.5 In the event that the “request for authorization” consists only of financial documentation (e.g., billing, liens, demand for payment, etc.); and includes no medical reporting of any kind; non-clinical administrative staff may issue a written request for information by using the pre-review script for written requests for medical documentation.
6.5.3 Pre-review screening shall not include any of the following:
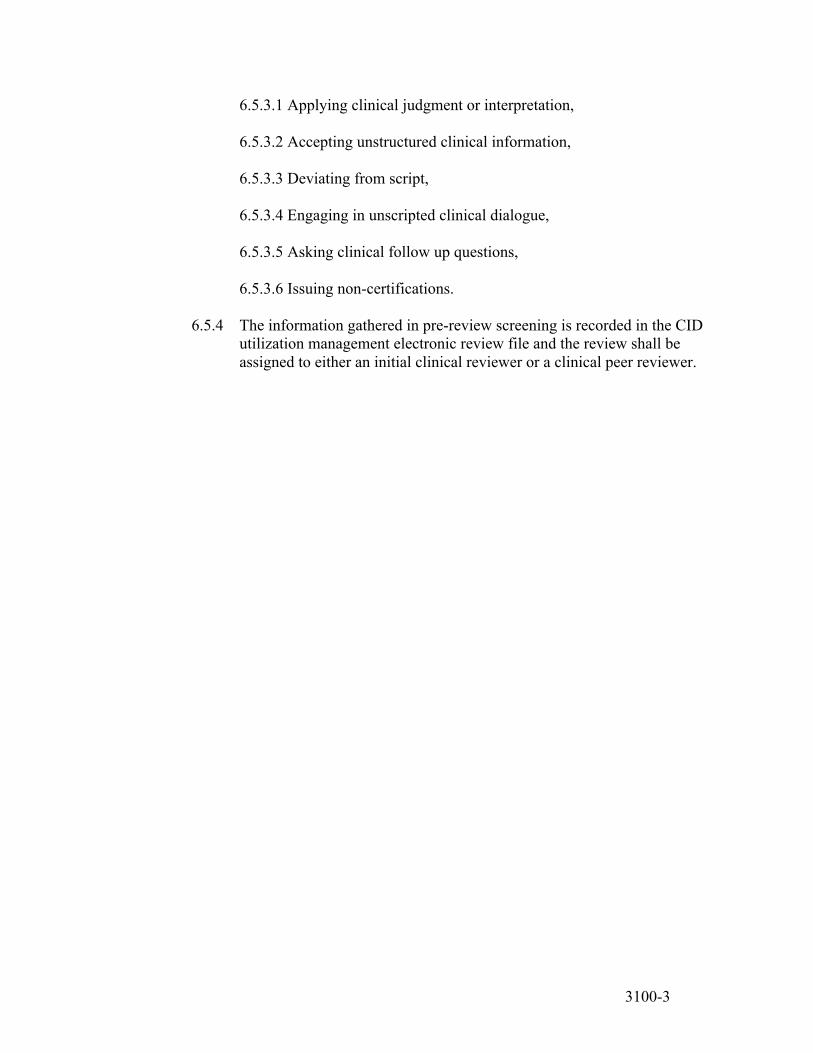
3100-3
6.5.3.1 Applying clinical judgment or interpretation, 6.5.3.2 Accepting unstructured clinical information,
6.5.3.3 Deviating from script,
6.5.3.4 Engaging in unscripted clinical dialogue,
6.5.3.5 Asking clinical follow up questions,
6.5.3.6 Issuing non-certifications.
6.5.4 The information gathered in pre-review screening is recorded in the CID
utilization management electronic review file and the review shall be assigned to either an initial clinical reviewer or a clinical peer reviewer.
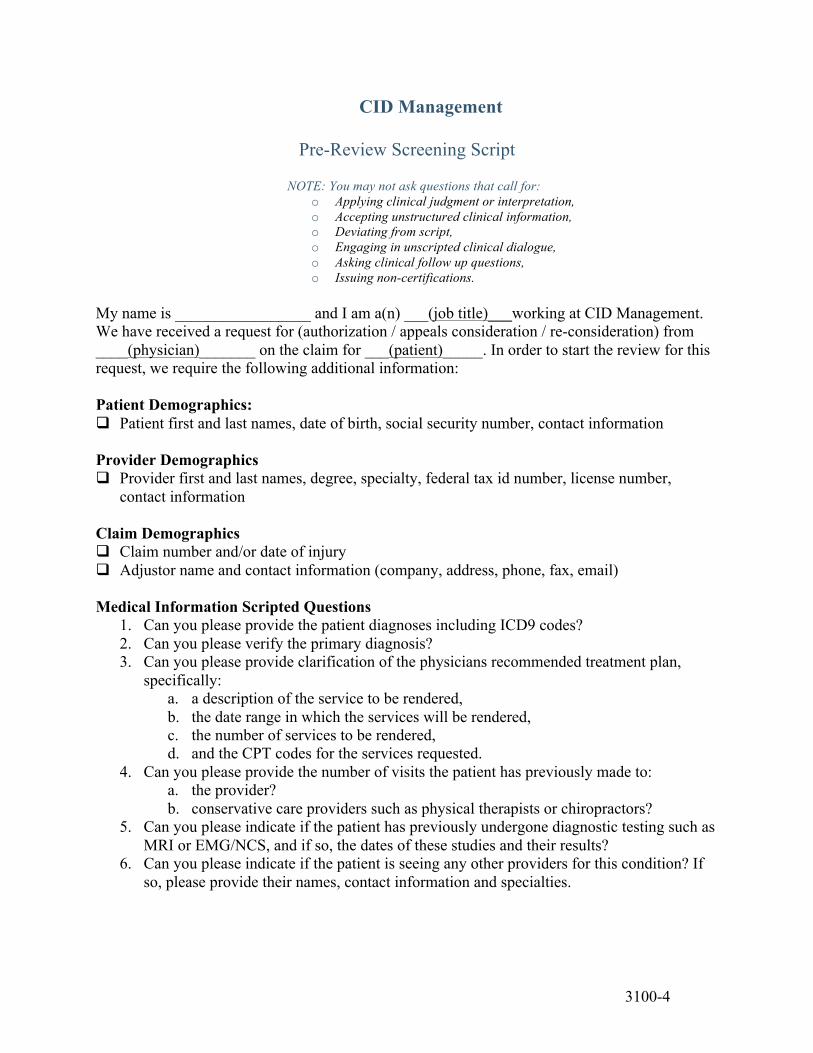
3100-4
CID Management
Pre-Review Screening Script
NOTE: You may not ask questions that call for: o Applying clinical judgment or interpretation, o Accepting unstructured clinical information, o Deviating from script, o Engaging in unscripted clinical dialogue, o Asking clinical follow up questions, o Issuing non-certifications.
My name is _________________ and I am a(n) ___(job title)___working at CID Management. We have received a request for (authorization / appeals consideration / re-consideration) from ____(physician)_______ on the claim for ___(patient)_____. In order to start the review for this request, we require the following additional information: Patient Demographics: Patient first and last names, date of birth, social security number, contact information Provider Demographics Provider first and last names, degree, specialty, federal tax id number, license number,
contact information Claim Demographics Claim number and/or date of injury Adjustor name and contact information (company, address, phone, fax, email) Medical Information Scripted Questions
1. Can you please provide the patient diagnoses including ICD9 codes? 2. Can you please verify the primary diagnosis? 3. Can you please provide clarification of the physicians recommended treatment plan,
specifically: a. a description of the service to be rendered, b. the date range in which the services will be rendered, c. the number of services to be rendered, d. and the CPT codes for the services requested.
4. Can you please provide the number of visits the patient has previously made to: a. the provider? b. conservative care providers such as physical therapists or chiropractors?
5. Can you please indicate if the patient has previously undergone diagnostic testing such as MRI or EMG/NCS, and if so, the dates of these studies and their results?
6. Can you please indicate if the patient is seeing any other providers for this condition? If so, please provide their names, contact information and specialties.

3100-5
CID Management
Pre-Review Script for Written Request for Medical Documentation The request was submitted without clinical information/reporting. Please forward the appropriate clinical reporting/documentation which: 1) displays the provider’s request for the above procedure/service; 2) provides the patient’s subjective and objective status at the time the procedure/service was requested; and 3) contains the provider’s clinical rationale supporting the medical necessity of the request.

3100-6
Addendum – California Claims 1. Consistent with Policy 3100, CID non-clinical administrative staff may not apply clinical
judgment or interpretation. 2. Consequently, non-clinical staff are not permitted to:
2.1. Issue authorizations (certifications) 2.2. Issue denials (non-certifications) 2.3. Issue delays 2.4. Issue any request for information that is inconsistent with the scripted requests for
information contained in Policy 3100.
3200-1
CID Management
Initial Clinical Review
Policy No. 3200 Revision: 4.2 Revision Date: 7/14/2009 Page 1 of 7
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which initial clinical review, also known as first level review, may be conducted at CID.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 4.0 05/1/2008 Revised Revision 4.0 04/21/2009 Reviewed Revision 4.1 06/18/2009 Revised Revision 4.2 07/14/2009 Revised Revision 4.2 06/08/2010 Reviewed Revision 4.2 03/14/2011 Reviewed Revision 4.2 04/24/2012 Reviewed Revision 4.2 01/17/2013 Reviewed
3.0 Persons Affected This policy affects initial clinical reviewers contracted with CID.
4.0 Policy The policy of CID Management is to perform initial clinical review of all requests for authorization to determine if the request for authorization matches the CID clinical review criteria. It is further the policy of CID Management that determinations of modification, non-certification and conditional non-certification shall not be issued by initial clinical reviewers.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.

3200-2
6.0 Procedures 6.1 CID may utilize initial clinical review staff to perform first level review on requests
for authorization submitted by providers. 6.2 Initial clinical reviewers shall have access to consultation with a:
6.2.1 Licensed doctor of medicine or doctor of osteopathic medicine 6.2.2 Licensed health professional in the same licensure category as the
requesting physician, 6.2.3 Health professional with the same clinical education as the requesting
physician in clinical specialties where licensure is not issued. 6.3 For prospective and concurrent reviews, the initial clinical reviewers shall make the
determination based solely upon information obtained by CID at the time of review determination. For retrospective reviews, the initial clinical reviewers shall make the determination based solely upon information available to the requesting physician at the time the medical care was provided.
6.4 Initial clinical review staff shall review the request for authorization and evaluate the
request to determine if it complies fully with the clinical review criteria.
6.4.1 If the request for authorization complies fully with the clinical review criteria and the client contract specifies that reviews may be approved through initial clinical review, then the initial clinical review staff shall add the following items to the electronic review file and use the CID secured web-based system to electronically identify the review as complete: 6.4.1.1 A specific description of the medical treatment service certified 6.4.1.2 A clinical rationale which shall include:
6.4.1.2.1 A clear and concise explanation of the reason for the
decision 6.4.1.2.2 The clinical reason regarding medical necessity
6.4.1.3 A description of the medical criteria or guidelines used
6.4.1.4 A written copy of the relevant portion of the criteria or guidelines
used
3200-3
6.4.2 If the request for authorization does not comply fully with the clinical review criteria, or if the client contract specifies that all reviews must undergo second level review regardless of determination, then the initial clinical review staff shall add the following items to the electronic review file and assign the review to a clinical peer reviewer for second level review. 6.4.2.1 A summary of the documents reviewed 6.4.2.2 A specific description of the medical treatment services consistent
with, and those inconsistent with, the clinical review criteria.
6.4.2.3 A clinical rationale which shall include:
6.4.2.3.1 A clear and concise explanation of the reason for the decision
6.4.2.3.2 The clinical reason regarding medical necessity
6.4.2.4 A description of the medical criteria or guidelines used 6.4.2.5 A written copy of the relevant portion of the criteria or guidelines
used.
6.4.2.6 The initial reviewer’s clinical concerns and/or rationale for forwarding the review to clinical peer review.
3200-4
Addendum – California 1.0 Prior to conducting initial review, the initial clinical reviewer may determine that no
utilization review is necessary, consistent with 8CCR9792.9(o) or 8CCR9792.9.1(h). This requires that all of the following conditions must be met:
1.1 There has been a denial, modification or delay of the same request from the same provider.
1.2 Less than 12 months has elapsed between the prior determination described in 1.1 and the request for authorization under review.
1.3 There has been no documented change in the facts material to the basis of the prior determination described in 1.1 and 1.2. Such change may consist of:
1.3.1 Relevant supportive change in patient presentation; and/or 1.3.2 Relevant supportive findings from new diagnostic studies and/or imaging;
and/or 1.3.3 Relevant supportive change in interval clinical history.
2.0 Consistent with 8CCR9792.9.1(c)(2), if the request for authorization is for a date of injury 1/1/13 or after or the review is being conducted 7/1/13 or after; and if all mandatory fields on the DWC Form RFA have not been completed; the DWC Form RFA may be returned to the requesting provider marked as “not complete”. The review in progress will at that point be completed; and a new review initiated if and when a completed DWC Form RFA is received.
3.0 Consistent with 8CCR9792.9(b) and 8CCR9792.9.1(b), if the initial clinical reviewer believes that there should be a dispute of liability for the requested course of treatment, they may stop review of those portions of the course of treatment so disputed by timely issuance of a notice of dispute of liability. Such notice shall contain:
3.1 The date on which the request for authorization was first received. 3.2 A description of the specific course of proposed medical treatment for which
authorization was requested. 3.3 A clear, concise, and appropriate explanation of the reason that liability is being
disputed for the injury/illness, claimed body part(s) and/or recommended treatment. 3.4 A plain language statement advising the injured employee that any dispute under this
subdivision shall be resolved either by agreement of the parties or through the dispute resolution process of the Workers’ Compensation Appeals Board.
3.5 The following mandatory language: 3.5.1 “You have a right to disagree with decisions affecting your claim. If you
have questions about the information in this notice, please call me (insert claims adjuster’s name in parentheses) at (insert telephone number). However, if you are represented by an attorney, please contact your attorney instead of me.”
3.5.2 “For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-free 1-800-736-7401.”
4.0 If the process in 3.0 (above) is followed, then utilization review or authorization of the requested course of care shall be completed within the time frame described in 8CCR9792.9(b)(2) and 8CCR9792.9.1(b)(2).
3300-1
CID Management
Clinical Peer Review
Policy No. 3300 Revision: 5.2 Revision Date: 6/17/2009 Page 1 of 8
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which clinical peer review, also known as second level review, may be conducted at CID.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 4.0 01/29/2008 Revised Revision 5.0 05/01/2008 Revised Revision 5.1 03/12/2009 Revised Revision 5.2 06/17/2009 Revised Revision 5.2 06/08/2010 Reviewed Revision 5.2 03/14/2011 Reviewed Revision 5.2 04/24/2012 Reviewed Revision 5.2 01/09/2013 Reviewed
3.0 Persons Affected This policy affects clinical peer reviewers contracted with CID.
4.0 Policy The policy of CID Management is to perform clinical peer review of all requests for authorization where it has been determined that the request for authorization does not match the CID clinical review criteria or where requested by the client. It is the policy of CID Management to mandate that all determinations involving modification, non-certification or conditional non-certification be made by a clinical peer reviewer. The clinical peer reviewer shall determine if the clinical information dictates that a variance from the clinical review criteria is appropriate in which case the request for authorization shall be certified, or if the clinical information does not support a variance from the clinical review criteria in which case the request for authorization shall be non-certified. It is further the policy of CID
3300-2
Management that the clinical peer reviewers hold a current and valid license in the same category as the requesting physician, hold a current and valid license in the discipline of the requested service, or as a doctor of medicine or doctor of osteopathic medicine.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 CID utilizes clinical peer reviewer to perform second level review on requests for
authorization, appeals consideration, and re-consideration submitted by providers. 6.2 Clinical peer reviewers shall be assigned to reviews based upon a matrix developed
by the medical director or clinical director such that the reviewers are qualified as determined by the medical director or clinical director to render a clinical opinion about the medical condition, procedures, and treatment under review and hold a current and valid license:
6.2.1 In the same licensure category as the ordering provider, or 6.2.2 In the discipline of the requested service, or 6.2.3 As a doctor of medicine or doctor of osteopathic medicine.
6.3 Clinical peer reviewers shall review the request for authorization and evaluate the
request to determine if it complies fully with the clinical review criteria. If the request for authorization has previously been reviewed by initial clinical review staff, the clinical peer reviewer shall additionally review the notes added to the review by the initial clinical review staff.
6.4 If the request for authorization falls outside the scope of clinical practice of the
clinical peer reviewer, the clinical peer reviewer shall use the CID system to request the review be transferred to an alternate clinical peer reviewer.
6.5 For prospective and concurrent reviews, the clinical peer reviewers shall make the
determination based solely upon information obtained by CID at the time of review determination. For retrospective reviews, the clinical peer reviewers shall make the determination based solely upon information available to the requesting physician at the time the medical care was provided.
6.6 If the request for authorization complies fully with the clinical review criteria, the
peer clinical review staff shall add the following items to the electronic review file and use the CID secured web-based system to electronically identify the review as complete:
3300-3
6.6.1 A specific description of the medical treatment service certified, if any 6.6.2 A clinical rationale which shall include:
6.6.2.1 A clear and concise explanation of the reason for the decision 6.6.2.2 The clinical reason regarding medical necessity
6.6.3 A description of the medical criteria or guidelines used
6.6.4 A written copy of the relevant portion of the criteria or guidelines used
6.7 If the request for authorization does not comply fully with the clinical review criteria,
the clinical peer reviewer shall determine if the clinical information dictates that a variance from the clinical review criteria is appropriate in which case the request for authorization shall be certified, or if the clinical information does not support a variance from the clinical review criteria in which case the request for authorization shall be non-certified. The peer clinical review staff shall then add the following items to the electronic review file and use the CID secured web-based system to electronically identify the review as complete:
6.7.1 A specific description of the medical treatment services certified and non-
certified 6.7.2 A clinical rationale which shall include:
6.7.2.1 A clear and concise explanation of the reason for the decision 6.7.2.2 The clinical reason regarding medical necessity
6.7.3 A description of the medical criteria or guidelines used 6.7.4 A written copy of the relevant portion of the criteria or guidelines used.
6.8 For electronic review files on which initial clinical review staff have completed any of the steps listed above, the peer clinical reviewer shall review that work of the initial clinical review staff and make all necessary modifications and corrections prior to electronically marking the review as complete.
6.9 Once completed, a determination shall not be materially changed. Upon receipt of
additional information, an appeal or re-consideration may be initiated however the original determination shall not be materially changed.
3300-4
Addendum – State of California 1.0 Prior to conducting peer review, the clinical peer reviewer may determine that no utilization
review is necessary, consistent with 8CCR9792.9(o) or 8CCR9792.9.1(h). This requires that all of the following conditions must be met:
1.1 There has been a denial, modification or delay of the same request from the same provider.
1.2 Less than 12 months has elapsed between the prior determination described in 1.1 and the request for authorization under review.
1.3 There has been no documented change in the facts material to the basis of the prior determination described in 1.1 and 1.2. Such change may consist of:
1.3.1 Relevant supportive change in patient presentation; and/or
1.3.2 Relevant supportive findings from new diagnostic studies and/or imaging; and/or
1.3.3 Relevant supportive change in interval clinical history. 2.0 Consistent with 8CCR9792.9.1(c)(2), if the request for authorization is for a date of injury
1/1/13 or after or the review is being conducted 7/1/13 or after; and if all mandatory fields on the DWC Form RFA have not been completed; the DWC Form RFA may be returned to the requesting provider marked as “not complete”. The review in progress will at that point be completed; and a new review initiated if and when a completed DWC Form RFA is received.
3.0 Consistent with 8CCR9792.9(b) and 8CCR9792.9.1(b), if the clinical peer reviewer believes that there should be a dispute of liability for the requested course of treatment, they may stop review of those portions of the course of treatment so disputed by timely issuance of a notice of dispute of liability. Such notice shall contain:
3.1 The date on which the request for authorization was first received.
3.2 A description of the specific course of proposed medical treatment for which authorization was requested.
3.3 A clear, concise, and appropriate explanation of the reason that liability is being disputed for the injury/illness, claimed body part(s) and/or recommended treatment.
3.4 A plain language statement advising the injured employee that any dispute under this subdivision shall be resolved either by agreement of the parties or through the dispute resolution process of the Workers’ Compensation Appeals Board.
3.5 The following mandatory language:
3.5.1 “You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me (insert claims adjuster’s name in parentheses) at (insert telephone number). However, if you are represented by an attorney, please contact your attorney instead of me.”
3.5.2 “For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an
3300-5
information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-free 1-800-736-7401.”
4.0 If the process in 3.0 (above) is followed, then utilization review or authorization of the requested course of care shall be completed within the time frame described in 8CCR9792.9(b)(2) and 8CCR9792.9.1(b)(2).
5.0 Consistent with Labor Code 4610(g)(3)(B), in the case of concurrent review, medical care shall not be discontinued (non-certified, or modified such that a component of care is non-certified). until the requesting physician has been notified of the decision and a care plan has been agreed upon by the requesting physician that is appropriate for the medical needs of the injured worker.
6.0 The preferred method of such notification and subsequent agreement on a care plan is contact by telephone. All such contact and attempted contact, and attempts to agree on a care plan, must be documented by the clinical peer reviewer within the CID database.
7.0 Medical care provided during a concurrent review shall be medical treatment that is reasonably required to cure or relieve from the effects of the industrial injury. In the event that the requesting physician has not agreed to a care plan that the clinical peer reviewer believes is consistent with this standard, the clinical rationale shall provide the basis for this opinion, and shall recommend to the claims administrator that retrospective assessment of the dispute be sought as described in LC4610(g)(3)(B).
3400-1
CID Management
Appeals Consideration
Policy No. 3400 Revision: 4.3 Revision Date: 6/8/2010 Page 1 of 12
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which appeals consideration, also known as third level review, may be conducted at CID.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 4.0 01/29/2008 Revised Revision 4.1 03/24/2009 Revised Revision 4.2 06/18/2009 Revised Revision 4.3 06/08/2010 Revised Revision 4.3 03/14/2011 Reviewed Revision 4.3 04/24/2012 Reviewed Revision 4.3 01/10/2013 Reviewed
3.0 Persons Affected This policy affects initial clinical reviewers and clinical peer reviewers contracted with CID.
4.0 Policy The policy of CID Management is to perform appeals consideration on reviews previously completed by CID clinical reviewers, provided that the appeals consideration meet the appropriate inclusion criteria. It is further the policy of CID Management to ensure that all decisions to modify or non-certify appeals considerations are performed by board certified clinical peer reviewers who did not make the original determination to modify or non-certify the care, nor are the subordinate of such an individual.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
3400-2
6.0 Procedures 6.1 CID non-clinical administrative staff shall ensure that appeals considerations meet the
following inclusion criteria. If the inclusion criteria are not met, the appeals consideration shall not be started and the requestor shall be advised to contact the claims administrator.
6.1.1 The party submitting the appeals consideration is a party authorized to do
so by law. In jurisdictions without explicit designation of parties authorized to submit an appeal, submission of appeals shall be limited to the injured worker and the provider or facility providing services.
6.1.2 The appeals consideration is accompanied by medical information above
and beyond that which was submitted in the initial request for authorization.
6.1.3 The appeals consideration is received within 30 calendar days of the initial
determination date.
6.1.4 For concurrent reviews involving urgent care, there shall be the availability of an expedited review, and in the case of an adverse determination to the expedited appeals consideration, the further availability of a single standard appeals consideration allowed.
6.1.5 For prospective and retrospective reviews, there shall be availability of a
single standard appeals consideration allowed.
6.2 Requests for appeal consideration may be initiated by parties via telephone, however shall not be started until receipt of additional medical information and specific appeal request in writing.
6.3 CID administrative staff shall forward a copy of the appeals consideration, as well as
all additional medical documentation received, to the claims administrator. 6.4 CID may utilize initial clinical review staff to perform initial review on requests for
appeals consideration. 6.5 Initial clinical review staff shall review the request for appeals consideration and
evaluate the request to determine if it complies fully with the clinical review criteria.
6.5.1 The initial clinical review staff shall add the following items to the electronic review file and assign the review to the clinical peer reviewer specified by the CID system. The CID system shall ensure that the clinical peer reviewer chosen is: (a) a clinical peer; (b) holds an active, unrestricted license to practice medicine or a health profession; (c) are board certified in the appropriate discipline, if applicable; (d) are in the same profession and in a similar specialty as typically manages the

3400-3
medical condition, procedure, or treatment as mutually deemed appropriate; and (e) are neither the individual who made the original non-certification, nor the subordinate of such an individual, for third level review. 6.5.1.1 A summary of the documents reviewed 6.5.1.2 A specific description of the medical treatment services certified
and non-certified
6.5.1.3 A clinical rationale which shall include:
6.5.1.3.1 A clear and concise explanation of the reason for the decision
6.5.1.3.2 The clinical reason regarding medical necessity
6.5.1.4 A description of the medical criteria or guidelines used 6.5.1.5 A written copy of the relevant portion of the criteria or guidelines
used.
6.5.1.6 The initial reviewer’s clinical concerns and/or rationale for forwarding the review to clinical peer review.
6.6 Clinical peer reviewers shall review the request for appeals consideration and
evaluate the request to determine if it complies fully with the clinical review criteria. If the appeals consideration has previously been reviewed by initial clinical review staff, the peer clinical reviewer shall additionally review the notes added to the review by the initial clinical review staff.
6.7 If the request for appeals consideration complies fully with the clinical review
criteria, the peer clinical review staff shall add the following items to the electronic review file and use the CID secured web-based system to electronically identify the review as complete:
6.7.1 A specific description of the medical treatment service certified 6.7.2 A clinical rationale which shall include:
6.7.2.1 A clear and concise explanation of the reason for the decision 6.7.2.2 The clinical reason regarding medical necessity
6.7.3 A description of the medical criteria or guidelines used

3400-4
6.7.4 A written copy of the relevant portion of the criteria or guidelines used
6.8 If the request for appeals consideration does not comply fully with the clinical review criteria, the clinical peer reviewer shall determine if the clinical information dictates that a variance from the clinical review criteria is appropriate in which case the request for appeals consideration shall be certified, or if the clinical information does not support a variance from the clinical review criteria in which case the request for appeals consideration shall be non-certified. The peer clinical review staff shall then add the following items to the electronic review file and use the CID secured web-based system to electronically identify the review as complete:
6.8.1 A specific description of the medical treatment services certified and non-
certified 6.8.2 A clinical rationale which shall include:
6.8.2.1 A clear and concise explanation of the reason for the decision 6.8.2.2 The clinical reason regarding medical necessity
6.8.3 A description of the medical criteria or guidelines used 6.8.4 A written copy of the relevant portion of the criteria or guidelines used.
6.9 For electronic review files on which initial clinical review staff have completed any of the steps listed above, the peer clinical reviewer shall review that work of the initial clinical review staff and make all necessary modifications and corrections prior to electronically marking the review as complete.

3400-5
Addendum – State of California
1) Consistent with 8CCR9792.10.1(d); for dates of injury 1/1/2013 or after; and for any UR decision communicated to the physician on 7/1/2013 or after; any appeal review must be completed within 15 days of the date of the UR decision.
2) Consistent with (1) and to allow meaningful completion of appeals; for dates of injury 1/1/2013 or after; and for any UR decision communicated to the physician on 7/1/2013 or after; any appeal request must be received within 10 days of the date of the UR decision.
3450-1
CID Management
Reconsiderations of Determinations at the Request of Claims Administrators
Policy No. 3450 Revision: 1.0 Revision Date: 5/13/2009 Page 1 of 5
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which reconsiderations of determinations, including certifications, may be conducted at CID at the request of the claims administrator.
2.0 Revision History
Revision 1.0 05/13/2009 New Policy/Initial Implementation Revision 1.0 06/08/2010 Reviewed Revision 1.0 03/14/2011 Reviewed Revision 1.0 04/24/2012 Reviewed Revision 1.0 01/10/2013 Reviewed
3.0 Persons Affected This policy affects initial clinical reviewers and clinical peer reviewers contracted with CID.
4.0 Policy The policy of CID Management is to perform reconsideration on reviews previously completed by CID initial and/or clinical reviewers, at the request of the claims administrator, provided that the reconsideration request meets the appropriate inclusion criteria. It is further the policy of CID Management to ensure that reconsiderations are performed by the reviewer who issued the original determination, if available; that any adverse determinations (conditional non-certification, non-certification or modification) arising from such reconsideration must be issued by a clinical peer reviewer; and that in the event of reversal or alteration of a certification, there shall be made available to the patient or provider the opportunity for a standard appeal.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures

3450-2
6.1 CID non-clinical administrative staff shall ensure that reconsiderations at the request of the claims administrator meet the following inclusion criteria. If the inclusion criteria are not met, the reconsideration shall not be started and the claims administrator shall be so advised.
6.1.1 The party submitting the request for reconsideration is a party authorized
to do so by the claims administrator.
6.1.2 The determination for which reconsideration is being requested did not arise from an appeal.
6.1.3 The reconsideration request is provided in writing; includes a written
indication of the basis for disagreement with the original determination; and the request is based on at least one of the following assertions:
6.1.3.1 That the reviewer did not have access to crucial medical
information; 6.1.3.2 That the reviewer failed to consider substantive information
already available; 6.1.3.3 That the reviewer made significant factual errors in interpreting the
available medical documents; and/or 6.1.3.4 That the reviewer substantively misapplied clinical review criteria
(e.g., evidence-based guidelines)
6.1.4 In all instances in which a reconsideration of a certification is requested, the request must be accompanied by medical information above and beyond that which was submitted in the initial request for authorization.
6.1.5 The written request for reconsideration is received within 14 calendar days
of the initial determination date.
6.2 Requests for reconsideration may be initiated by an authorized party via telephone, however shall not be started until receipt of additional written materials as described above in 6.1.2 and 6.1.3.
6.3 CID administrative staff shall forward a copy of the request for reconsideration, as
well as all additional medical documentation received, to the provider of medical goods or services and to the injured worker.
6.4 In the event that client-requested reconsideration is made regarding concurrent
inpatient services not yet provided, the client-requested reconsideration must be completed and determination notice sent prior to the dates of service for the request(s) under review.
6.5 CID may utilize initial clinical review staff to perform initial review on requests for
reconsideration.

3450-3
6.6 Initial clinical review staff shall review the request for reconsideration and evaluate
the request to determine if it complies fully with the clinical review criteria.
6.6.1 The initial clinical review staff shall add the following items to the electronic review file and assign the review to the clinical peer reviewer specified by the CID system. The CID system shall ensure that the clinical peer reviewer chosen is: (a) a clinical peer; (b) holds an active, unrestricted license to practice medicine or a health profession; (c) are board certified in the appropriate discipline, if applicable; (d) are in the same profession and in a similar specialty as typically manages the medical condition, procedure, or treatment as mutually deemed appropriate; and (e) are the individual who made the original determination, if available. 6.6.1.1 A summary of the documents reviewed 6.6.1.2 A specific description of the medical treatment services certified
and non-certified
6.6.1.3 A clinical rationale which shall include:
6.6.1.3.1 A clear and concise explanation of the reason for the original decision
6.6.1.3.2 A clear and concise statement of the reasoning for the reconsideration request
6.6.1.3.3 The clinical reason regarding medical necessity
6.6.1.4 A description of the medical criteria or guidelines used 6.6.1.5 A written copy of the relevant portion of the criteria or guidelines
used.
6.6.1.6 The initial reviewer’s clinical concerns and/or rationale for forwarding the review to clinical peer review.
6.7 Clinical peer reviewers shall review the request for reconsideration and evaluate the
request to determine if it complies fully with the clinical review criteria. If the reconsideration has previously been reviewed by initial clinical review staff, the peer clinical reviewer shall additionally review the notes added to the review by the initial clinical review staff.
6.8 If the request for reconsideration complies fully with the clinical review criteria, the
peer clinical review staff shall add the following items to the electronic review file

3450-4
and use the CID secured web-based system to electronically identify the review as complete:
6.8.1 A specific description of the medical treatment service certified 6.8.2 A clinical rationale which shall include:
6.8.2.1 A clear and concise explanation of the reason for the decision 6.8.2.2 The clinical reason regarding medical necessity
6.8.3 A description of the medical criteria or guidelines used
6.8.4 A written copy of the relevant portion of the criteria or guidelines used
6.9 If the request for reconsideration does not comply fully with the clinical review
criteria, the clinical peer reviewer shall determine if the clinical information dictates that a variance from the clinical review criteria is appropriate in which case the request for reconsideration shall be certified, or if the clinical information does not support a variance from the clinical review criteria in which case the request for appeals consideration shall be non-certified. The peer clinical review staff shall then add the following items to the electronic review file and use the CID secured web-based system to electronically identify the review as complete:
6.9.1 A specific description of the medical treatment services certified and non-
certified 6.9.2 A clinical rationale which shall include:
6.9.2.1 A clear and concise explanation of the reason for the decision 6.9.2.2 The clinical reason regarding medical necessity
6.9.3 A description of the medical criteria or guidelines used 6.9.4 A written copy of the relevant portion of the criteria or guidelines used.
6.10 For electronic review files on which initial clinical review staff have completed any of the steps listed above, the peer clinical reviewer shall review that work of the initial clinical review staff and make all necessary modifications and corrections prior to electronically marking the review as complete.
6.11 In no instance shall conducting a reconsideration review be considered as a substitute for the appeals process afforded to the injured worker/provider under Policy 3400.

3450-5
6.12 In the event that a reconsideration of previously certified medical goods or services results in a reversal of any or all of the certification, the injured worker/provider must be afforded the opportunity for a standard appeal, and must be properly notified of that opportunity and appropriate process.

3500-1
CID Management
Re-Considerations
Policy No. 3500 Revision: 3.0 Revision Date: 1/29/2008 Page 1 of 5
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which re-considerations may be conducted at CID.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 4.0 01/29/2008 Revised Revision 4.0 05/14/2009 Reviewed Revision 4.0 06/08/2010 Reviewed Revision 4.0 03/14/2011 Reviewed Revision 4.0 04/24/2012 Reviewed Revision 4.0 01/17/2013 Reviewed
3.0 Persons Affected This policy affects initial clinical reviewers and clinical peer reviewers contracted with CID.
4.0 Policy The policy of CID Management is to perform re-considerations on reviews previously non-certified by CID clinical peer reviewers due to a lack of information, provided that the re-consideration meets the appropriate inclusion criteria
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 CID non-clinical administrative staff shall ensure that re-considerations meet the
following inclusion criteria. If the inclusion criteria are not met, the appeals consideration shall not be started and the requestor shall be advised to contact the claims administrator.

3500-2
6.1.1 The party submitting the re-consideration is a party authorized to do so by
law. 6.1.2 The re-consideration is accompanied by medical information above and
beyond that which was submitted in the initial request for authorization. 6.1.3 The re-consideration is received within 45 calendar days of the initial
determination date.
6.2 CID administrative staff shall forward a copy of the re-consideration, as well as all additional medical documentation received, to the claims administrator.
6.3 CID may utilize initial clinical review staff to perform initial review on requests for
re-consideration. 6.4 Initial clinical review staff shall review the request for re-consideration and evaluate
the request to determine if it complies fully with the clinical review criteria.
6.4.1 If the request for re-consideration complies fully with the clinical review criteria, the initial clinical review staff shall add the following items to the electronic review file and use the CID secured web-based system to electronically identify the review as complete: 6.4.1.1 A specific description of the medical treatment service certified 6.4.1.2 A clinical rationale which shall include:
6.4.1.2.1 A clear and concise explanation of the reason for the
decision 6.4.1.2.2 The clinical reason regarding medical necessity
6.4.1.3 A description of the medical criteria or guidelines used
6.4.1.4 A written copy of the relevant portion of the criteria or guidelines
used
6.4.2 If the request for re-consideration does not comply fully with the clinical review criteria, the initial clinical review staff shall add the following items to the electronic review file and assign the review to the clinical peer reviewer who reviewed the original request, if available. If the clinical peer reviewer who reviewed the original request is not available, the review shall be assigned to a clinical peer reviewer competent to evaluate the services requested.
3500-3
6.4.2.1 A summary of the documents reviewed 6.4.2.2 A specific description of the medical treatment services certified
and non-certified
6.4.2.3 A clinical rationale which shall include:
6.4.2.3.1 A clear and concise explanation of the reason for the decision
6.4.2.3.2 The clinical reason regarding medical necessity
6.4.2.4 A description of the medical criteria or guidelines used 6.4.2.5 A written copy of the relevant portion of the criteria or guidelines
used.
6.4.2.6 The initial reviewer’s clinical concerns and/or rationale for forwarding the review to clinical peer review.
6.5 Clinical peer reviewers shall review the request for re-consideration and evaluate the request to determine if it complies fully with the clinical review criteria. If the re-consideration has previously been reviewed by initial clinical review staff, the peer clinical reviewer shall additionally review the notes added to the review by the initial clinical review staff.
6.6 If the request for re-consideration complies fully with the clinical review criteria, the
peer clinical review staff shall add the following items to the electronic review file and use the CID secured web-based system to electronically identify the review as complete:
6.6.1 A specific description of the medical treatment service certified 6.6.2 A clinical rationale which shall include:
6.6.2.1 A clear and concise explanation of the reason for the decision 6.6.2.2 The clinical reason regarding medical necessity
6.6.3 A description of the medical criteria or guidelines used
6.6.4 A written copy of the relevant portion of the criteria or guidelines used
6.7 If the request for re-consideration does not comply fully with the clinical review
criteria, the clinical peer reviewer shall determine if the clinical information dictates
3500-4
that a variance from the clinical review criteria is appropriate, in which case the request for re-consideration shall be certified, or if the clinical information does not support a variance from the clinical review criteria in which case the request for re-consideration shall be non-certified. The peer clinical review staff shall then add the following items to the electronic review file and use the CID secured web-based system to electronically identify the review as complete:
6.7.1 A specific description of the medical treatment services certified and non-
certified 6.7.2 A clinical rationale which shall include:
6.7.2.1 A clear and concise explanation of the reason for the decision 6.7.2.2 The clinical reason regarding medical necessity
6.7.3 A description of the medical criteria or guidelines used 6.7.4 A written copy of the relevant portion of the criteria or guidelines used.
6.8 For electronic review files on which initial clinical review staff have completed any of the steps listed above, the peer clinical reviewer shall review that work of the initial clinical review staff and make all necessary modifications and corrections prior to electronically marking the review as complete.
3600-1
CID Management
Telephonic Peer To Peer Consultation
Policy No. 3600 Revision: 3.0 Revision Date: 6/5/07 Page 1 of 2
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which telephonic peer to peer consultations may occur in the performance of utilization management operations.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 05/14/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 03/14/2011 Reviewed Revision 3.0 04/24/2012 Reviewed Revision 3.0 01/17/2013 Reviewed
3.0 Persons Affected This policy affects clinical peer reviewers contracted with CID.
4.0 Policy The policy of CID Management is to perform telephonic peer to peer consultations during utilization management operations when specifically requested by the client or by the requesting physician.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 If requested by a client or requesting physician, CID clinical peer reviewers may
conduct telephonic peer to peer consultations prior to developing a determination for requests for authorization, appeals consideration, or re-considerations.
3600-2
6.2 If a telephonic peer to peer consultation is requested by a client or a requesting
physician, CID clinical peer reviewers shall attempt a phone call to the requesting physician’s office during regular business hours. This process shall be repeated up to 3 times, at a frequency of one call per day, as permitted by the regulatory timeframes associated with the review. The clinical peer reviewer shall leave messages on each attempt indicating their return number and the times that they can be reached.
6.3 If a telephonic peer to peer consultation is requested by a client or a requesting
physician, and if the requesting physician has not responded to the clinical peer reviewer’s attempts to contact them by telephone, then following the third attempt, or a lesser number of attempts if dictated by regulatory timeframes associated with the review, the clinical peer reviewer shall complete utilization management determination without speaking to the requesting physician.
6.4 If a telephonic peer to peer consultation is requested by a client or a requesting
physician, and if the clinical peer reviewer speaks with the requesting physician, the clinical peer reviewer shall document the call in the activities section of the electronic review file and shall reference the telephone call in the clinical rationale section of the review determination.
6.5 If a telephonic peer to peer consultation is requested by a client or a requesting
physician, and if the clinical peer reviewer is not available at a time that the requesting physician is available, the Clinical Director or Director of Production shall assign another clinical peer reviewer who is qualified to review the requested treatment, to make the telephone call within 1 business day at a time when the requesting physician is available.
3700-1
CID Management
Notifications of Extension of Review Due Date
Policy No. 3700 Revision: 3.1 Revision Date: 4/25/2012 Page 1 of 7
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines for sending notifications of extension of review due date to the requesting physician. It establishes the situations and reasons for which notifications of extension of review due date may be sent.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 05/14/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 03/14/2011 Reviewed Revision 3.1 04/25/2012 Revised Revision 3.1 04/25/2012 Reviewed
3.0 Persons Affected This policy affects all CID employees and contractors performing utilization management operations.
4.0 Policy The policy of CID Management is to complete reviews only upon receipt of all reasonably necessary medical information. If the initial clinical reviewer or clinical peer reviewer determines that they are not in possession of all reasonably necessary medical information required to complete the review, they shall notify the stakeholders of the information they require and that the review determination due date will be extended until said information is submitted, or until deadline for providing information is reached. Further, it is the policy of CID Management to ensure that reviews are completed by clinical staff members competent to evaluate the medical services requested. In the event that an expert reviewer is required, CID shall notify the stakeholders that an expert reviewer is being assigned to the review and that the determination due date will be extended pending receipt of the expert reviewer’s determination.
3700-2
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 During the utilization management process, non-clinical administrative staff, initial
clinical review staff or clinical peer reviewers may determine that the review may not be completed in the allowed timeframes and that a notification of extension of review due date must be sent.
6.2 The notification of extension of review due date shall be sent within 48 business
hours of receiving the request for authorization from either the claims administrator or the provider.
6.3 The three situations in which a notification of extension of review due date may be
sent are:
6.3.1 The necessary medical information reasonably needed to make a determination is not present and needs to be requested from the provider by either the initial clinical review staff or the clinical peer reviewer.
6.3.2 The clinical peer reviewer determines that an additional examination or
test, that is reasonable and consistent with professionally recognized standards of medical practice, must be performed upon the injured worker to collect information needed in order to make an appropriate determination.
6.3.3 The non-clinical administrative staff, initial clinical review staff, or
clinical peer reviewer determines that a specialized consultation and review of medical information by an expert reviewer is required in order to make an appropriate determination.
6.4 The notification of extension of review due date shall contain the anticipated date on
which a decision will be rendered and any language required by applicable law or regulations.
6.5 If a notification of extension of review due date is sent to the provider requesting
additional information that the initial clinical review staff or clinical peer reviewer deems is reasonably necessary to make the determination, then:
6.5.1 The information requested shall be limited to information reasonably
necessary to certify the admission, procedure or treatment, length of stay, or frequency or duration of services.
3700-3
6.5.2 The notification of extension of review due date may be delivered to any
party specified by the client including, but not limited to:
6.5.3 Claims administrator 6.5.4 Nurse case manager
6.5.5 Attending physician
6.5.6 Requesting physician
6.5.7 Provider(s) of services or goods other than the attending or
requesting physicians
6.5.8 Patient
6.5.9 Patient’s legal counsel
6.5.10 Client’s legal counsel
6.5.1 If the client indicates that they do not want CID to distribute the notification of extension of review due date to a party that is required law to receive said notifications of extension of review due date, the client shall assume the responsibility of distributing these notifications of extension of review due date themselves.
6.5.2 Notifications of extension of review due date may be delivered to the
appropriate parties via any method specified by the client including, but not limited to secured electronic means, fax, US mail, and courier service.
6.5.3 If the client indicates that they do not want CID to distribute the
notification of extension of review due date to a party via a method specified by law, the client shall assume the responsibility of distributing these notifications of extension of review due date themselves.
6.5.4 The requested information shall be accepted from any reasonably reliable
source.
6.5.5 If the requested information is received within 2 business days, the non clinical administrative staff shall upload the requested information to the electronic review file and shall assign the review to the appropriate initial clinical review staff or clinical peer reviewer for completion.
3700-4
6.5.6 If the requested information is not received within 2 business days, the non clinical administrative staff may send an additional copy of the request for information to the requesting physician.
6.5.7 Steps 6.5.5 and 6.5.6 shall continue until the information is received or
until the day prior to the regulatory due date.
6.5.8 If the requested information is not received by the day prior to the regulatory due date,
6.5.8.1 For states in which conditional denials may be rendered, the CID
system shall add the following language to the review: “In regard to the request for (request), CID faxed the provider requesting additional information. As of this date, the provider has not submitted the requested data. To comply with utilization review timeframes it is recommended that the request be conditionally denied. The request will be reconsidered upon receipt of the information requested.”
6.5.8.2 For states in which conditional denials may not be rendered, the
CID system shall add the following language to the review: “In regard to the request for (request), CID faxed the provider requesting additional information. As of this date, the provider has not submitted the requested data. To comply with utilization review timeframes it is recommended that the request be denied due to lack of medical evidence.”
6.5.8.3 Assign the review to a clinical peer reviewer for completion
6.6 If a notification of extension of review due date is sent requesting an additional
examination or test be completed, that is reasonable and consistent with professionally recognized standards of medical practice, then:
6.6.1 The information requested shall be limited to information reasonably
necessary to certify the admission, procedure or treatment, length of stay, or frequency or duration of services.
6.6.2 The notification of extension of review due date may be delivered to any
party specified by the client including, but not limited to: 6.6.2.1 Claims administrator 6.6.2.2 Nurse case manager
6.6.2.3 Attending physician
3700-5
6.6.2.4 Requesting physician
6.6.2.5 Provider(s) of services or goods other than the attending or requesting physicians
6.6.2.6 Patient
6.6.2.7 Patient’s legal counsel
6.6.2.8 Client’s legal counsel
6.6.3 If the client indicates that they do not want CID to distribute the
notification of extension of review due date to a party that is required law to receive said notifications of extension of review due date, the client shall assume the responsibility of distributing these notifications of extension of review due date themselves.
6.6.4 Notifications of extension of review due date may be delivered to the
appropriate parties via any method specified by the client including, but not limited to secured electronic means, fax, US mail, and courier service.
6.6.5 If the client indicates that they do not want CID to distribute the
notification of extension of review due date to a party via a method specified by law, the client shall assume the responsibility of distributing these notifications of extension of review due date themselves
6.6.6 The requested information shall be accepted from any reasonably reliable
source.
6.6.7 If the requested examination or test result is received within 2 business days, the non clinical administrative staff shall upload the requested information to the electronic review file and shall assign the review to the appropriate initial clinical review staff or clinical peer reviewer for completion.
6.6.8 If the requested examination or test result is not received within 2 business
days, the non clinical administrative staff may send a second copy of the request for information to the requesting physician.
6.6.9 Steps 6.6.7 and 6.6.8 shall continue until the information is received or
until the day prior to the regulatory due date.
6.6.10 If the requested information is not received by the day prior to the regulatory due date,
3700-6
6.6.10.1 For states in which conditional denials may be rendered, the CID system shall add the following language to the review: “In regard to the request for (request), CID faxed the provider requesting additional information. As of this date, the provider has not submitted the requested data. To comply with utilization review timeframes it is recommended that the request be conditionally denied. The request will be reconsidered upon receipt of the information requested.”
6.6.10.2 For states in which conditional denials may not be
rendered, the CID system shall add the following language to the review: “In regard to the request for (request), CID faxed the provider requesting additional information. As of this date, the provider has not submitted the requested data. To comply with utilization review timeframes it is recommended that the request be denied due to lack of medical evidence.”
6.6.10.3 Assign the review to a clinical peer reviewer for
completion
6.7 If a notification of extension of review due date is sent to the provider informing them that a specialized consultation and review of medical information by an expert reviewer is required in order to make an appropriate determination then:
6.7.1 The notification of extension of review due date shall include the specialty of the
expert reviewer consulted 6.7.2 The notification of extension of review due date may be delivered to any party
specified by the client including, but not limited to
6.7.2.1 Claims administrator 6.7.2.2 Nurse case manager
6.7.2.3 Attending physician
6.7.2.4 Requesting physician
6.7.2.5 Provider(s) of services or goods other than the attending or requesting
physicians
6.7.2.6 Patient
6.7.2.7 Patient’s legal counsel
6.7.2.8 Client’s legal counsel
3700-7
6.7.3 If the client indicates that they do not want CID to distribute the notification of
extension of review due date to a party that is required law to receive said notifications of extension of review due date, the client shall assume the responsibility of distributing these notifications of extension of review due date themselves.
6.7.4 Notifications of extension of review due date may be delivered to the appropriate
parties via any method specified by the client including, but not limited to secured electronic means, fax, US mail, and courier service.
6.7.5 If the client indicates that they do not want CID to distribute the notification of
extension of review due date to a party via a method specified by law, the client shall assume the responsibility of distributing these notifications of extension of review due date themselves
6.7.6 The review shall be forwarded to the expert reviewer immediately
6.7.7 Once a determination is received from the expert reviewer, it shall be uploaded to
the system within the same business day and shall be immediately distributed to the stakeholders as per client contract.
3750-1
CID Management
Reimbursement For Duplication Of Records
Policy No. 3750 Revision: 3.0 Revision Date: 6/5/07 Page 1 of 2
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which parties shall be reimbursed in the event that they are required to submit duplicate reports as a result of the utilization management process.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 05/14/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 03/14/2011 Reviewed Revision 3.0 04/24/2012 Reviewed Revision 3.0 01/17/2013 Reviewed
3.0 Persons Affected This policy affects all clients and all stakeholders on reviews completed by CID Management.
4.0 Policy The policy of CID Management is to avoid requiring stakeholders to submit duplicate copies of records as a result of the utilization management process. It is further the policy of CID management to inform all clients and employers, with whom CID is contracted for utilization management services, that it is their responsibility to reimburse providers for duplicate copies of records as required by the labor code and regulations.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.

3750-2
6.0 Procedures 6.1 Upon initiation of a contract with a client, CID shall train the client’s administration,
supervisory staff and general staff on the CID utilization review process. 6.2 As a component of the initial training of the client’s administration, supervisory staff
and general staff, CID shall inform all parties to verify their responsibility to reimburse providers for duplicate records in compliance with labor code and regulations.
6.3 CID shall convey to the client’s administration, supervisory staff and general staff
that they should forward all relevant medical records for review to avoid requiring the provider to submit duplicate records.
6.4 If providers contact CID to request payment for duplication of records via any means
including, but not limited to: telephone, fax, mail, email, or web, CID shall inform them to contact the claims administrator.
6.5 To avoid requesting duplicate copies of records, prior to requesting additional
information from the provider, CID initial clinical reviewers and clinical peer reviewers shall review all documents attached to prior reviews on a claimant’s claim. Only in the event that CID does not have a copy of the document, shall the initial clinical reviewer or clinical peer reviewer contact the provider for a copy.
3800-1
CID Management
Utilization Management Correspondence
Policy No. 3800 Revision: 4.2 Revision Date: 3/12/2009 Page 1 of 11
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines for correspondence generation as a component of the utilization management operation.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 01/15/2007 Revised Revision 4.0 06/05/2007 Revised Revision 4.1 05/01/2008 Revised Revision 4.2 03/12/2009 Revised Revision 4.2 06/08/2010 Reviewed Revision 4.2 03/14/2011 Reviewed Revision 4.2 04/24/2012 Reviewed
3.0 Persons Affected This policy affects all CID employees and contractors who participate in the utilization management operations.
4.0 Policy The policy of CID Management is to provide correspondences at each step of the utilization management process to inform all parties of the status of the review. It is further the policy of CID Management to allow the clients to customize which correspondences are sent, and to which stakeholders they are sent.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures

3800-2
6.1 During the performance of utilization management, the following documents may be created by the CID system:
6.1.1 Request for utilization review received. This correspondence is generated
when the request for authorization, appeals consideration, or re-consideration is first uploaded into the CID system.
6.1.2 Notification of extension of review due date – additional information required. This correspondence is generated when it is determined that additional clinical information is required in order to make an appropriate determination.
6.1.3 Notification of extension of review due date – additional tests/procedures
required. This correspondence is generated when it is determined that additional clinical tests and/or procedures must be performed, and their results forwarded to CID, in order to make an appropriate determination.
6.1.4 Notification of extension of review due date – expert reviewer. This
correspondence is generated when it is determined that an expert clinical reviewer is needed to review the request.
6.1.5 Notification the provider submitted additional information. This
correspondence is generated when the provider submits the additional information, or the additional test and/or procedures findings, requested following a notification of extension of review due date.
6.1.6 Determination letter – Certified. This correspondence is generated when it
is determined that the request for authorization, appeals consideration, or re-consideration is being certified.
6.1.7 Determination letter – Modified. This correspondence is generated when it
is determined that the request for authorization, appeals consideration, or re-consideration is being partially certified.
6.1.8 Determination letter – Non-certified. This correspondence is generated
when it is determined that the request for authorization, appeals consideration, or re-consideration is being non-certified.
6.1.9 Determination letter – Conditionally Non-certified. This correspondence is
generated when there has been a request for additional information, or the clinical findings from additional tests and/or procedures, and the information has not been received by the regulatory due date.

3800-3
6.1.10 Review placed on hold by CID. This correspondence generates when CID places a review on hold pending additional information from the claims administrator that is required to complete the review.
6.1.11 Review placed on hold by client. This correspondence generates when the
client places a review on hold.
6.1.12 Review off of hold, back in progress. This correspondence generates when a review is taken off of CID enforced hold or client enforced hold, and is assigned to either an initial clinical reviewer or a clinical peer reviewer.
6.1.13 Review withdrawn by CID. This correspondence generates when CID
withdraws a review that it began in error.
6.1.14 Review withdrawn by client. This correspondence generates when the client requests that CID cease action on a review and withdraws it from review.
6.2 All correspondences shall include a reference number to the specific review in
question. 6.3 All determination correspondences shall contain the following elements:
6.3.1 The date on which a decision is made 6.3.2 A description of the specific course of proposed medical treatment for
which authorization was requested 6.3.3 A specific description of the medical treatment services certified, if any. If
for a hospital stay, this shall include the number of days or units of service certified, if any, the next anticipated review point, if any, the new total number of days or services approved, if any, and the date of admission or onset of services, if any.
6.3.4 For all reviews with an adverse determination, the determination
correspondence shall also include:
6.3.4.1 A clinical rationale which shall include:
6.3.4.2 A clear and concise explanation of the reason for the decision
6.3.4.3 The principle reason regarding medical necessity
6.3.4.4 A description of the medical criteria or guidelines used
3800-4
6.3.4.5 A written copy of the relevant portion of the criteria or guidelines used
6.3.4.6 Details about the claims administrator’s internal utilization review
appeals process, if any, and a clear statement that the appeal process is on a voluntary basis
6.3.4.7 The name of the initial clinical review staff and/or clinical peer
reviewer that made the determination
6.3.4.8 The specialty of the reviewer, if any
6.3.4.9 The CID contact telephone number
6.3.4.10 The CID hours of availability
6.4 The correspondences shall be delivered to the following parties, as identified on the review, unless not required by law or specifically excluded by the client contract:
6.4.1 Claims administrator 6.4.2 Nurse case manager
6.4.3 Attending physician
6.4.4 Requesting physician
6.4.5 Facility rendering service
6.4.6 Secondary physicians
6.4.7 Provider(s) of services or goods other than the attending or requesting
physicians
6.4.8 Patient
6.4.9 Patient’s legal counsel
6.4.10 Client’s legal counsel
6.5 If the client indicates that they do not want CID to distribute the correspondences to a party that is required by law to receive said correspondences, the client shall assume the responsibility of distributing these correspondences themselves.
6.6 Correspondences shall be delivered to the parties via the following specified method,
unless the client contract specifies otherwise:
3800-5
6.6.1 Claims administrator by email within 24 hours of decision 6.6.2 Nurse case manager by email within 24 hours of decision
6.6.3 Attending physician by fax within 24 hours of decision
6.6.4 Requesting physician by fax within 24 hours of decision
6.6.5 Facility rendering service by fax within 24 hours of decision
6.6.6 Secondary physicians by fax within 24 hours of decision
6.6.7 Provider(s) of services or goods other than the attending or requesting
physicians by fax within 24 hours of decision
6.6.8 Patient by mail, to be mailed within 24 hours of decision for concurrent review and within 1 business day of decision for all other reviews
6.6.9 Patient’s legal counsel by mail, to be mailed within 24 hours of decision
for concurrent review and within 1 business day of decision for all other reviews
6.6.10 Client’s legal counsel by mail, to be mailed within 1 business day of
decision
6.7 If the client indicates that they do not want CID to distribute correspondences to a party via a method specified by law, the client shall assume the responsibility of distributing these correspondences themselves.
6.8 Unless specifically barred by contract with the client, upon request by any authorized
party, CID shall re-issue a copy of the original communication and forward by fax or email. If CID is barred from doing so by contract with client, the party shall be advised to contact the claims administrator for a copy of the communication.

3800-6
Addendum – California Claims 1.0 For California claims, the following additional elements will be added to authorization
letters:
1.1 The date of the decision 2.0 For California claims; for dates of injury on 1/1/2013 or after, and/or for notice of
determination sent on 7/1/2013 or after; the following elements will be added to adverse determination letters:
2.1 The date on which DWC Form RFA was first received 2.2 The date on which the decision is made
2.3 A list of all medical records reviewed 2.4 If a utilization review decision to modify, deny or delay a medical service is due to
incomplete or insufficient information, the decision shall specify the reason for the decision and specify the information that is needed.
2.5 The Application for Independent Medical Review, DWC Form IMR, with all fields, except for the signature of the employee, completed; with an addressed envelope, for mailing to the Administrative Director or his or her designee.
2.6 A clear statement advising the injured employee that any dispute shall be resolved in accordance with the independent medical review provisions of Labor Code section 4610.5 and 4610.6, and that an objection to the utilization review decision must be communicated by the injured worker, the injured worker’s representative, or the injured worker's attorney on behalf of the injured worker on the enclosed Application for Independent Medical Review, DWC Form IMR, within 30 calendar days of receipt of the decision..
2.7 The following mandatory language “You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me (insert claims adjuster’s name in parentheses) at (insert telephone number). However, if you are represented by an attorney, please contact your attorney instead of me.
2.8 The following mandatory language: “For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-free 1-800-736-7401.”
3.0 2.0 For California claims; for dates of injury before 1/1/2013; and for notice of determination sent prior to 7/1/2013; the following elements will be added to adverse determination letters:
3.1 The date on which the decision is made
3.2 A clear statement that any dispute shall be resolved in accordance with the provisions of Labor Code section 4062, and that an objection to the utilization review decision must be communicated by the injured worker or the injured worker's attorney on behalf of the injured worker to the claims administrator in writing within 20 days of
3800-7
receipt of the decision. It shall further state that the 20-day time limit may be extended for good cause or by mutual agreement of the parties. The letter shall further state that the injured worker may file an Application for Adjudication of Claim, Form WCAB 1, and a Declaration of Readiness to Proceed (expedited trial), DWC-CA form 10252.1.
3.3 The following mandatory language: “You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me (insert claims adjuster’s name in parentheses) at (insert telephone number). However, if you are represented by an attorney, please contact your attorney instead of me.”
3.4 The following mandatory language: “For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-free 1-800-736-7401.”
3.5 The following mandatory language: “If you disagree with the utilization review decision and wish to dispute it, you must send written notice of your objection to the claims administrator within 20 days of receipt of the utilization review decision in accordance with Labor Code section 4062. You must meet this deadline even if you are participating in the claims administrator's internal utilization review appeals process.”
4.0 On all correspondences to non-physician providers of goods or service, the clinical rationales and guidelines shall be removed consistent with CA Labor Code and Regulations.

3900-1
CID Management
Utilization Management Turn Around Times
Policy No. 3900 Revision: 6.1 Revision Date: 4/24/2012 Page 1 of 10
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines for review timeframes. It addresses the following time frames: standard, expedited, rush, and stat which shall apply to requests for authorization, appeals consideration or re-considerations. It also details the mechanism used to respond on an urgent basis to situations that pose an immediate threat to the health and safety of patients.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 05/24/2006 Revised Revision 3.0 08/26/2006 Revised Revision 4.0 01/15/2007 Revised Revision 5.0 06/05/2007 Revised Revision 5.1 05/01/2008 Revised Revision 5.2 03/12/2009 Revised Revision 5.2 06/08/2010 Reviewed Revision 6.0 01/28/2011 Revised Revision 6.1 06/14/2011 Revised Revision 6.1 04/24/2012 Revised Revision 6.1 04/24/2012 Revised Revision 6.1 01/10/2013 Reviewed
3.0 Persons Affected This policy affects all CID employees and contractors who participate in the utilization management operations.
4.0 Policy The policy of CID Management is to perform reviews in a timely fashion remaining compliant with all required laws and regulations. It is further the policy of CID Management to perform reviews in a timely fashion with consideration given to the medical condition of the patient. These timeframes apply to requests for authorization, appeals consideration, and re-consideration.

3900-2
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 CID defines its timeframes for utilization management for all reviews (prospective,
concurrent and retrospective) as: 6.1.1 Standard goal – It is CID’s intention to complete all reviews within 2
business days of receipt of all necessary information; even if requirements below in 6.1.2 through 6.1.7 are less stringent. This standard is a goal for timeliness, and is not a process requirement. Deadlines indicated below in 6.1.2 through 6.1.7 are mandatory, and must be complied with.
6.1.2 Expedited (Urgent or Emergent situation posing threat to health or life of patient) - within 4-6 hours of receipt, as possible. Process described below in Section 6.6.
6.1.3 Rush – by midnight next business day 6.1.4 Stat – by midnight same business day 6.1.5 Prospective – within 15 calendar days of receipt of request
6.1.6 Retrospective – within 30 days of receipt of request
6.1.7 Concurrent (continuation of inpatient services)– within 2 business days of
receipt of request
6.1.8 Timeframe extension for request for information – In the event that there
is insufficient information to complete a determination, and a written request for information has been sent to the health care provider and the patient, the deadline for completing the review will be extended by 45 calendar days. In the event that the requested information is provided prior to the extended deadline, the review shall be completed within 2 business days of receipt of additional information. Such time frame extensions shall not be permitted for Expedited or Concurrent review.
6.1.9 Timeframe extension for reasons other than request for information – There shall be no extension of review timeframe for any cause other than a request for information.

3900-3
6.2 Requesting physicians and/or clients shall be required to indicate the requested turn
around time (standard, expedited, rush, stat) for review of a request for authorization, appeals consideration or re-consideration. If no timeframe is indicated, it shall be concluded that a standard turn around time is requested.
6.3 Upon receipt of a request for authorization, appeals consideration, or re-
consideration, the CID staff shall review the following if applicable: if the request is prospective/concurrent/retrospective, the date the request was received by the client, the date the client sent a notification of extension of review due date, the date the client received additional information, the date the request was received by CID. Based on this information, and in full consideration to the prevailing utilization management laws and regulations, the appropriate due date shall be determined for the review
6.4 The CID staff shall then review the submitted documents to determine if the
submitter has requested a standard, expedited, rush, or stat request. If the requested response date is earlier than the due date calculated in 6.3, then the due date shall be updated accordingly. If not, the due date calculated in 6.3 shall be retained.
6.5 The Senior Utilization Review Manager shall oversee reviews in progress to ensure
their completion by the due date.
6.6 Urgent Situations Posing an Immediate Threat to the Health and Safety of Patients (a.k.a. emergency health care services”)
6.6.1 If a situation presents where a party communicates to CID that the health
or safety of a patient is under immediate threat, the call shall be transferred directly to the Clinical Director, in his/her absence, to the Director of Production.
6.6.2 The Clinical Director, or Director of Production, shall immediately inform
the requesting party that future denial of payment for emergency care may never be based on lack of prior authorization, and that emergency services provided may be reviewed retrospectively based on medical necessity at the time the services were provided. In the event that the requesting party desires prior authorization, utilization review shall proceed as described in 6.6.3 through 6.6.6.
6.6.3 The Clinical Director, or Director of Production, assign the initial clinical
reviewer, clinical peer reviewer, and QAQC reviewer that are immediately available for reviews. The availability of each reviewer shall be confirmed by the Clinical Director or Director of Production by telephone.
3900-4
6.6.4 The Clinical Director, or Director of Production, shall evaluate the progress of the review by checking its status at intervals not to exceed 30 minutes.
6.6.5 Immediately upon reaching a determination, the CID system shall generate
a determination letter that shall be immediately faxed to the provider.
6.6.6 Immediately upon noting a determination has been reached, the Clinical Director, or Director of Production, shall contact the requesting provider via telephone to verify the receipt of the determination to ensure its arrival.
3900-5
Addendum – California Claims 1.0 Prospective reviews shall be made in a timely fashion that is appropriate for the nature of the
injured workers’ condition, not to exceed five (5) business days from the date of receipt of the written request for authorization.
1.1 If appropriate information, which is necessary to render a decision, is not provided
with the original request for authorization, such information may be requested by a reviewer or non-physician reviewer within five (5) business days from the date of receipt of the written request for authorization.
1.2 If the reasonable information is received prior to the fourteenth (14th) calendar day
following the date of receipt of the written request for authorization, the reviewer shall make a decision within five (5) business days of the receipt of the information. . In no event shall the determination be made more than 14 days from the date of receipt of the original request for authorization by the health care provider.
1.3 If the reasonable information requested is not received within 14 calendar days of the
date of the original request for authorization, a reviewer may deny the request with the stated condition that the request will be reconsidered upon receipt of the information requested.
1.4 In no event shall the determination be made more than 14 calendar days from the date
of receipt of the original request for authorization from the health care provider.
1.5 If the review is expedited, the decision shall be made in a timely fashion appropriate to the injured worker’s condition, not to exceed 72 hours after the receipt of the written information reasonably necessary to make the determination.
2.0 Concurrent reviews shall be made in a timely fashion that is appropriate for the nature of the
injured workers’ condition, not to exceed five (5) business days from the date of receipt of the written request for authorization.
2.1 If appropriate information, which is necessary to render a decision, is not provided
with the original request for authorization, such information may be requested by a reviewer or non-physician reviewer within five (5) business days from the date of receipt of the written request for authorization.
2.2 If the reasonable information is received prior to the fourteenth (14th) calendar day
following the date of receipt of the written request for authorization, the reviewer shall make a decision within five (5) business days of the receipt of the information. . In no event shall the determination be made more than 14 days from the date of receipt of the original request for authorization by the health care provider.
2.3 If the reasonable information requested is not received within 14 calendar days of the
date of the original request for authorization, a reviewer may deny the request with

3900-6
the stated condition that the request will be reconsidered upon receipt of the information requested.
2.4 In no event shall the determination be made more than 14 calendar days from the date
of receipt of the original request for authorization from the health care provider.
2.5 If the review is expedited, the decision shall be made in a timely fashion appropriate to the injured worker’s condition, not to exceed 72 hours after the receipt of the written information reasonably necessary to make the determination.
3.0 For retrospective reviews, decisions shall be communicated to the requesting physician
within 30 days of receipt of the medical information that is reasonably necessary to make this determination.
3.1 If appropriate information, which is necessary to render a decision, is not provided
with the original request for authorization, such information may be requested by a reviewer or non-physician reviewer within thirty (30) calendar days from the date of receipt of the written request for authorization.
3.2 If the reasonable information is received prior to the thirtieth (30th) calendar day
following the date of receipt of the written request for authorization, the reviewer shall make a decision within thirty (30) calendar days of the receipt of the information.
3.3 If the reasonable information requested is not received within 30 calendar days of the
date of the original request for authorization, the reviewer may deny the request with the stated condition that the request will be reconsidered upon receipt of the information requested.
4.0 Consistent with 8CCR9792.10.1(d); for dates of injury 1/1/2013 or after; and for any UR
decision communicated to the physician on 7/1/2013 or after; any appeal review must be completed within 15 days of the date of the UR decision.

4000-1
CID Management
Quality Assurance Quality Control
Policy No. 4000 Revision: 4.1 Revision Date: 6/9/2008 Page 1 of 5
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which quality assurance and quality control shall happen in the utilization management process at CID. It also details the structure and responsibilities of the Quality Assurance / Quality Control (QAQC) Committee.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 4.0 01/29/2008 Revised Revision 4.1 06/09/2008 Revised Revision 4.1 05/14/2009 Reviewed Revision 4.1 06/08/2010 Reviewed Revision 4.1 01/26/2011 Reviewed Revision 4.1 04/24/2012 Reviewed Revision 4.1 01/17/2013 Reviewed
3.0 Persons Affected This policy affects all employees and independent contractors who participate in performing utilization review at CID.
4.0 Policy The policy of CID Management is to ensure that reviews are completed with the highest quality by creating a QAQC program to monitor CID processes, provide feedback to the employees and contractors as necessary, and continually improve CID utilization management operations. It is further the policy of CID Management that a high quality product shall be the goal of every employee and contractor affiliated with our organization.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.

4000-2
6.0 Procedures
6.1 Quality Assurance / Quality Control Committee
6.1.1 The QAQC Committee has been granted the authority for quality
management by the CID Executive Committee, including both Managing Directors and the Clinical Director.
6.1.2 On a quarterly basis, the QAQC Committee shall meet.
6.1.3 Each meeting of the QAQC Committee will be maintained in approved
meeting minutes.
6.1.4 The QAQC Committee shall be comprised of the Clinical Director (Ex Officio) who serves as the committee’s chair, the Director of Clinical Operations (Ex Officio), a rotating (1 year term) Director of Production, a rotating (1 year term) clinical staff member, and a rotating (1 year term) Non-CID representative. The clinical staff member may be an initial clinical reviewer, a clinical peer reviewer, or a QAQC reviewer. The Non-CID representative shall meet the professional requirements of a clinical peer reviewer.
6.1.5 The scope and objective of the QAQC Committee is to continually strive
to improve the overall quality and accuracy of all reviews produced by CID.
6.1.6 The QAQC Committee will develop, monitor progress of, and update as
necessary, quality improvement goals. These goals will be used as benchmarks, along with the QAQC project status reports, to evaluate the effectiveness of the QAQC program. The program’s effectiveness will be reported in a QAQC Program Evaluation presented to the Executive Committee each year in the month of December.
6.1.7 The QAQC Committee shall review policies, regulations, and procedures
concerning quality assurance and quality control in the utilization management operations.
6.1.8 The QAQC Committee shall provide guidance to staff on quality
management projects, their scope, progress, and outcome, as well as the implementations of revised policies and procedures, as necessary. Following the completion of QAQC projects CID staff will be briefed on the results from the project via email summary or in-office meeting.
6.1.9 The QAQC Committee shall develop and approve projects to monitor
quality of utilization management operations.
4000-3
6.1.10 The Quality Assurance / Quality Control Committee shall review any
QAQC projects currently in progress and shall utilize any information found within these projects to develop recommendations to modify existing Policies or Procedures to fine-tune the utilization management operations.
6.1.11 The Quality Assurance Quality Control Committee shall pass these
recommendations to the Utilization Management Policies and Procedures Committee as well as to the Medical Director and Clinical Director.
6.1.12 The Utilization Management Policies and Procedures Committee shall
review the recommendations and shall develop any changes to existing Policies and Procedures as deemed necessary. These changes shall be forwarded to the Medical Director and Clinical Director for final review and edit prior to being implemented.
6.1.13 CID will administer the CID Management Confidential Survey each year
to all clients by mail. The QAQC Committee will be given the summary report of the CID Management Confidential Survey results each year upon compilation. The Committee will review this summary and recommend and develop QAQC projects for improvement of client satisfaction scores if a deficit in client satisfaction is noted.
6.1.13.1 In addition to other aspects of the survey summary report,
the summary specifically notes details regarding the ability of consumers/clients to access services (Question #1 and 9 on the survey). If clients are unsatisfied with access to services an investigation by the Clinical Director or Director of Clinical Operations will be conducted. If needed, a quality improvement project (QIP) will be initiated with specific goals and statistically valid measurements. The results of such a QIP are to be reported to the QAQC Committee and the Executive Committee upon its completion.
6.1.14 Annually, during the month of December, the results of the daily QAQC
program and the quarterly QAQC program will be reported to the Executive Committee by the Director of Clinical Operations (a standing member of the Executive Committee). Any comments, concerns, or directives will be reported back to the QAQC and Utilization Management Policy and Procedure Committees. Reports will be presented to the Executive Committee by the Director of Clinical Operations during the course of the year if QAQC issues arise that are unresolved at the second- and third-level committee level.
4000-4
6.2 Daily Quality Assurance/Quality Control Program. The objective of the daily QAQC program is to provide the resources and staff to review the critical aspects of all outbound reviews. By performing this QAQC check CID decreases errors, omissions, internal inconsistencies, inappropriate guideline referencing, etc.
6.2.1 Following completion of reviews, initial clinical reviewers and clinical
peer reviewers shall mark their reviews as “Released to QAQC”. 6.2.2 The CID system shall migrate these reviews to the assigned QAQC
Reviewer’s in-box.
6.2.3 QAQC Reviewers shall perform day to day quality assurance and quality
control monitoring of all reviews in their in-box. This monitoring shall include: 6.2.3.1 Reviewing internal consistency within the review to ensure that the
review does not contradict itself. In the event that there is an inconsistency between determination language and the reviewer’s button selection of determination type, if the language clearly indicates the reviewer’s intent then the inconsistency shall be resolved according to procedure 6.2.4. If the intent of the clinical reviewer is not clearly reflected in the determination language, then the conflict inconsistency shall be resolved according to procedure 6.2.5.
6.2.3.2 Reviewing completeness of the review to ensure that it addresses
all elements of care requested by the requesting physician. 6.2.3.3 Reviewing guidelines applied for relevance to the requested care. 6.2.3.4 Reviewing guidelines for appropriate referencing. 6.2.3.5 Reviewing completion criteria and savings estimate for accuracy. 6.2.3.6 Reviewing the grammar, punctuation, and spelling.
6.2.4 If the QAQC Reviewer notes non-material changes, such as spelling,
grammar, or punctuation, they shall make the non-material changes to the review and shall release the review to the client.
6.2.5 If the QAQC Reviewer notes material changes, such as incomplete
reviews or incorrect guidelines, they shall re-assign the review to the initial clinical reviewer or clinical peer reviewer for correction.
4000-5
6.2.6 The QAQC Reviewers shall note any common errors of specific initial clinical reviewers or clinical peer reviewers and shall communicate this to the Clinical Director.
6.2.7 If the QAQC Reviewers shall note any common errors of specific initial
clinical reviewers or clinical peer reviewers, the Clinical Director shall contact the specific initial clinical reviewer or clinical peer reviewer to address and resolve these issues.
6.3 Quarterly Quality Assurance/Quality Control Program
6.3.1 On a quarterly basis, the Quality Assurance/Quality Control Committee
shall meet. Details of the meeting’s agenda, charter, participants, goals, etc is noted above it section 6.1.
6.3.2 A standing agenda item at the quarterly meetings will be an analysis of all
complaints, grievances, and appeals. For each complaint or grievance all materials will be presented and the course of action, outcome, and resolution will be discussed. The total number of reviews requested as well as the number and percentages of reviews certified, conditionally non-certified, non-certified, appeals certified, appeals conditionally non-certified, and appeals non-certified will be presented and discussed. Reference and comparison to past review percentages will be conducted for tracking of rates and trends.
6.4 Annually, during the month of December, the results of the daily QAQC program and
the quarterly QAQC Committee meeting minutes will be presented to the Executive Committee by the Director of Clinical Operations (a standing member of the Executive Committee) in the form of a QAQC Program Evaluation. Any comments, concerns, or directives will be reported back to the QAQC and Utilization Management Policy and Procedure Committees in writing.
6.5 The Executive Committee can request reports, meeting minutes, or other materials from the QAQC Committee at any time to ensure accountability.
6.6 Reports will be presented to the Executive Committee by the Director of Clinical
Operations during the course of the year if QAQC issues arise that are unresolved at the second- and third-level committee level.

5000-1
CID Management
Utilization Management Business Hours
Policy No. 5000 Revision: 3.2 Revision Date: 6/22/2009 Page 1 of 7
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines outlining CID Management’s business hours for utilization management operations.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.1 06/06/2008 Revised Revision 3.1 03/19/2009 Reviewed Revision 3.2 06/22/2009 Revised Revision 3.2 06/08/2010 Reviewed Revision 3.2 01/27/2011 Reviewed Revision 3.2 04/24/2012 Reviewed Revision 3.2 01/17/2013 Reviewed
3.0 Persons Affected This policy affects all CID employees and contractors who perform utilization management operations.
4.0 Policy The policy of CID Management is to maintain business hours between 9:00 a.m. and 5:30 p.m. on all business days in all time zones in which CID conducts business. For the purpose of this policy, business days are defined as any day not defined as a holiday, or optional bank holiday, within the CA Civil Code which states:
4.1 Civil Code 7. Holidays within the meaning of this code are every Sunday and such
other days as are specified or provided for as holidays in the Government Code of the State of California.

5000-2
4.2 Civil Code 7.1. Optional bank holidays within the meaning of Section 9 are: o Any closing of a bank because of an extraordinary situation, as that term is
defined in the Bank Extraordinary Situation Closing Act (Chapter 20 (commencing with Section 3600) of Division 1 of the Financial Code).
o Every Saturday o Every Sunday o January 1st o The third Monday in January, known as “Dr. Martin Luther King, Jr. Day” o February 12, known as “Lincoln Day” o The third Monday in February o The last Monday in May o July 4th o The first Monday in September o September 9th, known as “Admission Day” o The second Monday in October, known as “Columbus Day” o November 11th, known as “Veteran’s Day” o December 25th o Good Friday from 12 noon until closing o The Thursday in November appointed as “Thanksgiving Day” o Any Monday following any Sunday on which January 1st, February 12th, July
4th, September 9th, November 11th, or December 25th falls. o Any Friday preceding any Saturday on which July 4th, September 9th, or
December 25th falls.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 The CID Clinical Director and Senior Utilization Review Managers shall meet in
December to set the following year’s business day schedule. 6.2 The Senior Utilization Review Manager shall schedule utilization review non-clinical
administrative staff to ensure the office is staffed for business operations between 8:30 a.m. and 5:30 p.m. local time in all time zones in which CID maintains business operations.
6.2.1 The Senior Utilization Review Manager shall report to the Clinical
Director and Director of Clinical Operations on a quarterly basis any instances in which no staff were available during business hours, as well as the cause of any such lapse in staffing.
6.3 The Clinical Director shall schedule initial clinical reviewers and clinical peer
reviewers to ensure utilization management functions may be performed every business day of the year.

5005-1
CID Management
Utilization Management In-Business Hours Communications Access
Policy No. 5005 Revision: 3.1 Revision Date: 5/1/2008 Page 1 of 3
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which CID shall make itself available for communications from clients and stakeholders
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.1 05/01/2008 Revised Revision 3.1 05/14/2009 Reviewed Revision 3.1 06/08/2010 Reviewed Revision 3.1 01/27/2011 Reviewed Revision 3.1 04/24/2012 Reviewed Revision 3.1 01/17/2013 Reviewed
3.0 Persons Affected This policy affects all CID employees and contractors who perform utilization management operations.
4.0 Policy
The policy of CID Management is to provide access to the utilization management department during normal business hours, by a toll free phone number, toll free fax number, and US postal address.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures

5005-2
6.1 The Director of Production shall ensure that CID maintains a toll free phone number for use in utilization review operations.
6.2 The Director of Production shall ensure that CID maintains a toll free fax number for
use in utilization review operations. 6.3 The Clinical Director shall ensure that the toll free phone number, toll free fax
number and US postal address are printed on all forms and all written communications generated by CID.
6.4 The Director of Customer Relations shall ensure that all clients have a copy of CID’s
toll free number, toll free fax number and US postal address for distribution as they deem appropriate.
6.5 The Clinical Director shall ensure that the complete Policies and Procedures will be
made available to the public on request.

5005-3
Addendum – California 1.0 The Clinical Director shall ensure that the current Utilization Review Plan, as filed with the
Administrative Director, will be made available to the public on request.

5010-1
CID Management
Utilization Management Communications Response
Policy No. 5010 Revision: 3.0 Revision Date: 6/5/07 Page 1 of 2
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which CID employees or contractors respond to mail, voice mail, fax, or email messages.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 05/14/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 01/27/2011 Reviewed Revision 3.0 04/24/2012 Reviewed Revision 3.0 01/17/2013 Reviewed
3.0 Persons Affected This policy affects all CID employees and contractors who perform utilization management operations.
4.0 Policy
The policy of CID Management is to return mail inquiries, voice mail messages, email messages, or fax messages within 1 business day of receipt.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 The Director of Production shall schedule non-clinical administrative staff to check
the mailbox once per business day after standard US post delivery time.
5010-2
6.2 The Director of Production shall schedule non-clinical administrative staff to check the general voice mail message box four times per business day including: immediately upon arrival in the office; mid-morning; mid afternoon; end of business day.
6.3 The Director of Production shall schedule non-clinical administrative staff to check
the general email in-box four times per business day including: immediately upon arrival in the office; mid-morning; mid afternoon; end of business day.
6.4 Each non-clinical administrative staff member shall check their personal voice mail
message box four times per business day including: immediately upon arrival in the office; mid-morning; mid afternoon; end of business day.
6.5 Each non-clinical administrative staff member shall check their email in-box four
times per business day including: immediately upon arrival in the office; mid-morning; mid afternoon; end of business day.
6.6 Each clinical contractor or staff member, including but not limited to, initial clinical
reviewer and clinical peer reviewer, shall check their email in-box once per business day.
6.7 All CID employees and contractors shall reply to mail, voice mail, email, or fax
messages within 1 business day of receipt.
6.8 All CID employees and contractors shall reply to mail, voice mail, email or fax messages during reasonable and normal business hours unless otherwise mutually agreed to by the party to be contacted.
6.9 All CID employees and contractors shall log the date and content of received mail,
voice mail, email or fax message within the CID system, if the communication directly referenced a review or claim in the CID system.
6.10 All CID employees and contractors shall log the date and content of their
response to the mail, voice mail, email or fax message within the CID system, if the communication directly referenced a review or claim in the CID system.
5020-1
CID Management
Utilization Management After Hours Communications
Policy No. 5020 Revision: 3.1 Revision Date: 6/6/08 Page 1 of 2
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which after hours communications shall be handled.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.1 06/06/2008 Revised Revision 3.1 03/19/2009 Reviewed Revision 3.1 06/08/2010 Reviewed Revision 3.1 01/27/2011 Reviewed Revision 3.1 04/24/2012 Reviewed Revision 3.1 01/17/2013 Reviewed
3.0 Persons Affected This policy affects all CID employees and contractors who perform utilization management operations.
4.0 Policy The policy of CID Management is to maintain 24-hour access to secure electronic submission, fax machines and voice mail systems for providers or clients to submit requests for authorization, appeals consideration or re-considerations outside of regular business hours as defined in CID Policy 5000. It is further the policy of CID to maintain a 24-hour find-me-follow-me access line for clients to contact the Clinical Director or Senior Utilization Review Staff in case of emergency.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.

5020-2
6.0 Procedures 6.1 The Director of Production shall ensure that CID maintains a 24-hour voice mail
service that allows clients and review stakeholders to leave messages after regular business hours.
6.2 The Director of Production shall ensure that CID maintains a 24-hour fax service that
allows clients and review stakeholders to fax requests for authorization, appeals consideration or re-consideration after regular business hours.
6.3 The Director of Production shall ensure that CID maintains a 24-hour secured
electronic submission service that allows clients and review stakeholders to submit requests for authorization, appeals consideration, or re-consideration after regular business hours.
6.4 The Director of Production shall report on a quarterly basis to the Clinical Director
and Director of Clinical Operations all known instances of outages of service on the voice mail, fax and electronic access services described above in sections 6.1, 6.2 and 6.3, and all known instances of complaints regarding lack of access to these services.
6.5 The Clinical Director shall ensure that CID maintains a 24-hour find-me-follow-me
access line for clients to contact the Clinical Director or Senior Utilization Review Staff in case of emergency.
6.6 The Clinical Director shall ensure that all clients have access and training on how to
utilize the 24-hour find-me-follow-me access line in cases of emergency.
5030-1
CID Management
Utilization Management Communications Etiquette
Policy No. 5030 Revision: 3.0 Revision Date: 6/5/07 Page 1 of 2
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which CID employees and contractors shall conduct themselves in communications with any party.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.0 05/14/2009 Reviewed Revision 3.0 06/08/2010 Reviewed Revision 3.0 01/27/2011 Reviewed Revision 3.0 04/24/2012 Reviewed Revision 3.0 01/17/2013 Reviewed
3.0 Persons Affected This policy affects all CID employees and contractors who perform utilization management operations.
4.0 Policy
The policy of CID Management is to provide professional and courteous communications to all parties.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 All CID employees and contractors shall maintain the highest levels of
professionalism in all communications which shall include: 6.1.1 Answering communications promptly and courteously
5030-2
6.1.2 Providing proper identification, including own name (full or partial), job title, and company name with placing and answering communications
6.1.3 Showing respect and courtesy by using the customer’s full name, title or rank, except where the circumstances are such that the use of the callers first name would be more appropriate
6.1.4 Ensuring that transferred calls are answered before disconnecting from the customer
6.1.5 Handing customer communications in a thoughtful, considerate, patient and helpful manner.
5050-1
CID Management
Marketing and Communications
Policy No. 5050 Revision: 6.0 Revision Date: 3/14/2011 Page 1 of 3
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which all marketing and communications materials will be produced.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 05/24/2006 Revised 6.3 Revision 3.0 08/26/2006 Revised Revision 4.0 06/05/2007 Revised Revision 5.0 01/29/2008 Revised Revision 5.1 06/06/2008 Revised Revision 5.1 05/14/2009 Reviewed Revision 5.1 06/08/2010 Reviewed Revision 5.1 01/26/2011 Reviewed Revision 6.0 03/14/2011 Revised Revision 6.0 04/24/2012 Reviewed Revision 6.0 01/17/2013 Reviewed
3.0 Persons Affected This policy affects all CID employees and contractors who are involved in the production of marketing and communications materials. This includes, but is not limited to, the Managing Directors, the Clinical Director, Operations Director, and any marketing subcontractors. The public and potential clients are also affected. These clients include requesting physicians, nurse case managers, claim’s administrators, and health insurance companies.
4.0 Policy The policy of CID Management is to clearly and accurately communicate information about our services to clients.
5.0 Definitions

5050-2
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 CID does direct marketing through individual mailings, emailings, e-newsletters,
print collateral, Google adwords, website postings, and attendance/representation at conventions.
6.2 CID sometimes partners with companies who are similarly positioned in the worker’s
compensation market, such as CompIQ and Interplan, to help market our product along with their own at conventions, sales calls, etc.
6.3 CID utilizes two independent review groups prior to approval and production of any
marketing materials. Only upon separate approval by these two review bodies (at least one person from each group) are marketing materials produced and distributed. These two independent review bodies are:
6.3.1 Clinical Group, consisting of member who have clinical experience and
are licensed health care providers. This group shall review all marketing materials for accuracy and intent from a clinical perspective, and shall ensure that: 6.3.1.1 The information presented clearly and accurately communicates
information regarding CID’s services 6.3.1.2 The information does not misrepresent the organization’s services.
6.3.2 Business Group. This shall review all marketing materials for accuracy,
lucidity, and intent, from a business perspective, and shall ensure that: 6.3.2.1 The information presented clearly and accurately communicates
information regarding CID’s services 6.3.2.2 The information does not misrepresent the organization’s services.
6.4 All marketing materials to be used on a continuing basis are to be reviewed as
described above on at least an annual basis.
6.5 New marketing materials shall not be distributed until both review groups agree that there are no errors in content. Established materials that are found to have errors on periodic re-review are to be corrected as rapidly as possible or withdrawn from use.
6.6 Any complaints or grievances related to marketing or misrepresentation are handled through the grievance process (see Policy 1500) and are maintained for future reference.

5050-3
Addenda to Policy 5050: Group Rosters as of 4/24/2012 Clinical Group: Todd Andrew Lisa Shaw O’Connor Jason Vanderford Robert Ward Business Group Steven Cardinale Rick Leinwohl

5100-1
CID Management
Utilization Management On Site Reviews
Policy No. 5100 Revision: 3.1 Revision Date: 3/12/2009 Page 1 of 3
_______________ ______________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which CID employees and contractors function when performing on-site reviews.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 3.1 03/12/2009 Revised Revision 3.1 06/08/2010 Reviewed Revision 3.1 03/14/2011 Reviewed Revision 3.1 04/24/2012 Reviewed Revision 3.1 01/17/2013 Reviewed
3.0 Persons Affected This policy affects all CID employees or contractors who perform utilization management operations on-site.
4.0 Policy The policy of CID Management is to represent a professional and respectful presence when performing reviews onsite.
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 Prior to scheduling employees or contractors to work on-site, the Clinical Director or
Director of Production shall contact the client to determine any facility or organization requirements that may exist.

5100-2
6.2 The Clinical Director or Director of Production shall write up specific procedures
CID employees or contractors must follow for each specific organization or facility.
6.3 A copy of the written procedures shall be forwarded to the organization or facility for review, comment and update as necessary.
6.4 The Clinical Director or Director of Production shall review the written procedures
with all CID employees and contractors who will be on-site at that organization or facility. A hard copy of these procedures will be provided to the CID employees and contractors for reference.
6.5 When performing utilization management functions on-site, CID employees and
contractors shall provide the organization or facility in which they will be working at least one business day notice of their arrival unless otherwise agreed.
6.6 When performing utilization management functions on-site, CID employees and
contractors shall check in with designated staff or personnel upon their arrival and shall check out with designated staff or personnel upon their departure.
6.7 When performing utilization management functions on-site, CID employees and
contractors shall conduct themselves in a professional manner obeying any and all rules and regulations of the organization or facility in which they are working.
6.8 When performing utilization management functions on-site, CID employees and
contractors shall carry their CID picture ID identifying their position with CID. The picture ID shall be worn in a conspicuous location. When performing utilization management functions on-site in Texas, the CID picture ID shall also include CID’s Texas Department of Insurance identification number.
6.9 When performing utilization management functions on-site, CID employees and
contractors shall wear appropriate facility-supplied identification tags in a conspicuous location, if so requested.
6.10 CID staff shall not observe, participate in, record or otherwise be present during an
injured employee’s examination, treatment, procedure or therapy unless approved by the injured employee and the treating physician or modified by contract.
6.11 CID staff will not require as a condition of treatment approval or for any other
reason, the observation of a psychotherapy session or the submission or review of a mental health therapist’s process or progress notes.
6.12 CID staff, if so requested, will agree that the medical records remain available in the
designated area during the onsite review and that reasonable hospital administrative procedures shall be followed so as not to disrupt hospital operations or patient care.
5100-3
CID Management
On-site Picture ID
7000-1
CID Management
Information Management
Policy No. 7000 Revision: 5.0 Revision Date: 3/1/2011 Page 1 of 6
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC Medical Director, CID Clinical Director, CID
1.0 Purpose
This policy establishes guidelines by which data and information is managed, maintained, secured, destroyed, and remains confidential. Disaster recovery plans are outlined. Hardware, software, processes, and subcontracting towards the above objectives are also delineated.
2.0 Revision History
Revision 1.0 03/15/2006 New Policy/Initial Implementation Revision 2.0 08/26/2006 Revised Revision 3.0 06/05/2007 Revised Revision 4.0 01/29/2008 Revised Revision 4.1 05/15/2009 Revised Revision 4.1 06/08/2010 Reviewed Revision 5.0 03/01/2011 Revised Revision 5.0 04/24/2012 Revised Revision 5.0 01/17/2013 Revised
3.0 Persons Affected This policy affects all employees and independent contractors who participate in performing utilization review at CID.
4.0 Policy The policy of CID Management is to ensure the integrity, security, and confidentiality of all data records handled by CID in the course of operations. Additionally, systems are utilized to efficiently manage all data and provide for redundancies in storage, back-up, and accessibility equipment and processes. CID continuously monitors updates in software, hardware, firmware, and subcontractor options to improve system stability, security, and accessibility. CID strives to maximize convenience for our clients while ensuring compliance with all state and industry regulations as we maximize effectiveness brought about by technological solutions.
5.0 Definitions
7000-2
5.1 Definitions of terms are set forth in Policy 1000.
6.0 Procedures
6.1 Data / Information System Overview
6.1.1 CID has structured our internal Utilization Review architecture around an atomic object oriented software methodology. This allows us to quickly create interfaces to virtually any system. The system is delivered via the web and uses Microsoft’s software development foundation to deliver both the web interface and any EDI bridges necessary.
6.1.2 As a consequence of our OO/.NET infrastructure and our relational and
XML based data warehouse we can craft custom EDI interfaces as well as standard interfaces. With past and current clients we have successfully implemented an interface that can deliver not only billing information but real-time utilization review activities, decisions, and supporting activity documentation. EDI files can be transmitted via email, or FTP. Information is also compliant with OLE, DB//ODBC - making it possible to work with any database engine and provide daily integration data, decision and treatment data, and other data organized in any format appropriate to the customer’s system. Data can be arranged by date/time and delivered based upon action/task, decision type, savings type, savings amount, document type, charges, etc.
6.1.3 CID’s technology is completely web-based. The entire UR system is based
around transactional technology which ensures data integrity. All related documents are uploaded into our technology system. These images reside on a system fault tolerant server and are backed-up via an incremental redundancy system. All images are available to authorized users via CID’s web system using a standard web browser and Adobe Acrobat Reader version 6.0 or greater.
6.2 CID uses our proprietary medical management system to manage and track reviews.
Reviews can be submitted in several different formats including:
6.2.1 Email: We have the ability to receive reviews via both encrypted and unencrypted email. Each client is assigned specific review email addresses (such as [email protected]) which allows us to track usage and delivery times. Encryption is accomplished using Verisign public key encryption mechanisms with public and private keys exchanged between CID and the client. Additionally we can offer both public and private email addresses (such as [email protected]) so that not only can client
7000-3
employees submit email reviews, but providers can submit additional documentation via email.
6.2.2 Fax: We have implemented fax systems using Fax.com and MetroFax as our primary service providers. Fax.com and MetroFax telecommunication companies that provides HIPAA compliant fax servers. Fax.com and MetroFax maintains several thousand fax servers. Faxes are automatically converted to electronic documents and submitted into CID internal system.
6.2.3 Web: Clients receive access to CID’s client portal to submit UR requests
and to track their progress. This portal sits behind a full secure web application using Microsoft’s .NET framework. This encrypted portal allows client employees to view requests and upload information and documentation directly to the CID online application.
6.2.4 US Postal Mail: We use a single physical location for all reviews. This
location provides a secure staffed facility to receive all documentation. All correspondence are retrieved on a daily basis and scanned into our system at our local premises.
6.2.5 FTP: We offer many different alternatives to electronic submission
including: FTP, XML, EDI. These are typically customized for each client. We can support interfaces directly to claims systems (such as Valley Oaks) where requests can be easily generated from the claims system directly, to FTP servers where groups of requests as PDF files are batched on a daily basis. This can be done via secure FTP (e.g. via SSL) if requested to allow for secure delivery of documents.
6.3 CID uses the same methods for delivery of information and decisions as we use for
request submission:
6.3.1 Email: Decisions can be emailed to any party using either standard or secure email. Additionally, several stakeholders can be notified at the same time that a decision has been completed (e.g. examiner and supervisor). Decision documents are delivered via PDF files so that documents cannot be altered.
6.3.2 Detailed decision information is included not only in the attached PDF files, but as text within the body of the email if requested. This allows users to copy and paste the decision information into other systems as well as have a PDF version of the documentation which includes physician signatures.
6.3.3 Fax: We use Fax.com and MetroFax as our primary fax delivery providers. Within 15 minutes, these services attempt to deliver the fax at least 3 times. These services log notifications of successful or
7000-4
unsuccessful delivery and any unsuccessful faxes are submitted to our customer service team for hand processing.
6.3.4 Web: Our client portal not only allows for request submission but also for
monitoring status and downloading documentation upon completion. When a decision has been reached the documents are available for immediate download from our secure server
6.3.5 US Postal Mail: Some documentation is required to be distributed via the
US Postal Service (such as patient notification of denials). Our internal system automatically prints these notifications for hand processing and mailing by our administrative staff.
6.3.6 FTP: The same electronic mechanisms provided for document submission
are available for review decisions: FTP, XML, EDI. All communications can be customized from automatic insertion into claim management systems (such as dropping decisions directly into Valley Oaks), to secure FTP transmissions on a batch or push basis. Typically this is customized on a client-by-client basis.
6.4 Document Formats used in CID Processes
6.4.1 For document submission we accept any Microsoft Office document type
(e.g. Word, Excel, etc), plus Adobe PDF documents, ASCII text files and standard image files (GIF, JPG, TIF). Additionally we can accept electronic file types including: CSV, XML, ASC, TXT.
6.4.2 Internally documents are created and handled as PDF and/or text files.
6.4.3 Decisions are submitted to stakeholders via PDF files and as plain text
within emails.
6.5 Backup and Storage System Technologies
6.5.1 CID’s entire system is has been developed using a secure web delivery methodology. Our technology is based upon the .NET framework from Microsoft and is hosted in HIPAA compliant data centers. Currently our data servers are located at RackSpace (www.rackspace.com) The RackSpace solution incorporates the following critical components:
o Secured Space with superior data center infrastructure; o High Speed Internet Access; o Server and Application Monitoring; o Daily and Weekly Data Backups; o Shared and dedicated firewalls; o Managed intrusion detection;

7000-5
o Vulnerability scanning; o Systems and database administration; o Remote hands & hardware support; o 24/7 first, second, and third level engineering support
6.5.2 CID data and file servers are backed up on a daily schedule, with complete backups done weekly.
6.5.3 CID has separated out our DNS routing capabilities to a third party,
UltraDNS, to provide redundancy in our routing, reducing downtime in the event of a network crash. CID contracts with RackSpace which allows for a seamless recovery from a system crash.
6.6 Data/Document Destruction
6.6.1 CID maintains a strict confidentiality plan which includes:
6.6.1.1 Shredding of all paperwork received or generated by our
operations.
6.6.1.2 It is CID’s policy to never delete any electronic data or records from the CID server. “Deleted” information on the network / website only appears to be deleted. It is removed from the current view but is accessible by administrators as data linked to the appropriate review. All data, included “deleted” data is stored on the server and back-up servers.
6.6.2 CID uses a version control system to maintain copies of all templates that
are transmitted to stakeholders.
6.7 Monitoring Data for Accuracy / Data Integrity
6.7.1 Each piece of data imported or created in the CID system, as well as every activity, is assigned a unique identifier. This unique identifier allows tracing and retrieval of any data ever handled on the CID system. The unique identifier combined with CID’s policy of never deleting any electronic data means that any data that has even been on CID’s system is retrievable.
6.7.2 The CID proprietary medical management system software keeps track of
each action along the UR process by recording it under the “Claims Activities” tab associated with each claim. The information recorded includes the user’s name, action performed, and date/time stamp. Additionally, a more detailed log of activities, transmittals, communications, etc are recorded under the “Review Activities” tab which
7000-6
is automatically or manually (for different operations/processes) inputted with the user’s name, description of task/process, and a date/time stamp.
6.7.2.1 These logs of activities with user information, date/time stamp, and
detail of activity allow managerial and QA/QC personnel to go through random samples of reviews checking for accuracy, compliance with required time frames, etc. This allows trending data and a record of personnel performance which is used as part of routine personnel assessments.
6.7.3 Data integrity errors, especially patient demographic information and
duplicate entries are reduced by built-in safeguards in the CID proprietary software. When entering a new patient, the CID system requires the data entry personnel to first search in the database for that patient’s name and social security number. Only upon failure to find a match in the CID database is the employee allowed by the software to enter the new patient’s demographics, claim details, and clinical information.
6.8 Security and Confidentiality Measures
6.8.1 CID Employees and contractors are to secure their workstations each time
they leave their proximity while working on CID related materials.
6.8.2 CID Employees are prohibited from saving data, documents, or any other review related materials to any external networks or portable media devices.
6.8.3 CID provides an encrypted secured website.
6.8.4 CID direct employees are required to have a unique assigned user ID and password to access the CID website and network.
6.8.5 CID has a Role / Task-based security configuration. Tasks are specific
actions which require access to pre-determined levels or review pages. Roles can be assigned to do a certain number of tasks depending on security level and level of interaction (data entry, supervisor, or observational only).
6.8.5.1 Granting of Role / Task-based security access is handled by CID
administrators.
6.8.5.2 Each client assigns their own roles which encompass specific tasks performed by their personnel. These role assignments are provided to CID administrators who personalize the Role / Task security system for each client.

7000-7
7000-1
CID Management
Information Security Violations
Policy No. 7010 Revision: 1.0 Revision Date: 3/1/2011 Page 1 of 6
_______________ _______________ Jonathan Rutchik, MD Robert W. Ward, DC Medical Director, CID Clinical Director, CID
1.0 Purpose
This policy defines the circumstances under which CID shall provide notice regarding a breach in security of confidential information.
2.0 Revision History
Revision 1.0 03/01/2011 New Policy/Initial Implementation Revision 1.0 04/24/2012 Reviewed Revision 1.0 01/17/2013 Reviewed
3.0 Persons Affected This policy affects all employees and independent contractors who participate in performing utilization review at CID. This policy further affects all clients contracted with CID.
4.0 Policy This policy applies to information safeguarded both by CID and/or by third-party vendors and contractors working with CID. Suspected or confirmed information security breaches must be reported immediately to the Security Officer. A breach is defined as unauthorized access of CID information. The Security Officer will investigate all reports of security breaches of confidential information. Based on the results of the investigation, internal and/or external parties may be notified, as necessary and appropriate.
5.0 Definitions
5.1 Definitions of terms are set forth in Policy 1000.
6.0 Procedures
6.1 Upon notification of a suspected information security breach, the Security Officer will:

7000-2
6.1.1 Report the breach to the appropriate officials
6.1.2 Block, mitigate, or de-escalate the breach, if possible.
6.1.3 Implement processes and procedures to prevent similar breaches from
occurring in the future.
6.2 Internal Notification
6.2.1 The Security Officer shall report all suspected cases of significant information breaches to the President, and will work with him/her to establish an appropriate response strategy. If the Security Officer's investigation determines that criminal activity has taken place, the Security Officer will further report this to the President. The Executive Committee will be notified of the results of the initial investigation.
6.3 External Notification
6.3.1 The Security Officer in consultation with the President will determine if
external notification will be required in the event of an information breach. External notification is required if any of the following conditions are met:
6.3.1.1 Has access been gained to unencrypted confidential information?
6.3.1.2 Has a physical device that contains unencrypted confidential
information been lost or stolen?
6.3.1.3 Is there evidence that unencrypted confidential information has been copied or removed?
6.3.1.4 Is there evidence that the intrusion was intended to acquire unencrypted confidential information?
6.3.1.5 Do local, state, or federal laws or company policy require notification in this instance?
6.3.2 Parties to be notified may include:
6.3.2.1 Anyone affected by the breach, or whose data may have been compromised.
6.3.2.2 Government officials as required by law.

7000-3
Addendum Current Security Officer: Aaron Mayerson, Senior Development Engineer.
9000-1
CID Management
California Based Clients Policy & Procedures
Policy No. 9000 Revision: 2.2 Revision Date: 01/10/2013 Page 1 of 22
_______________ ________________ Jonathan Rutchik, MD Robert W. Ward, DC
Medical Director, CID Clinical Director, CID 1.0 Purpose
This policy establishes guidelines by which California based clients shall operate if they are contracting with CID as their Utilization Management vendor for purposes of peer review, and who want their complete Utilization Management program to be under the supervision of CID Medical Director.
2.0 Revision History
Revision 1.0 06/05/2007 New Policy/Initial Implementation Revision 2.0 08/22/2007 Revised Revision 2.1 05/01/2008 Revised Revision 2.1 05/14/2009 Reviewed Revision 2.1 06/08/2010 Reviewed Revision 2.1 03/14/2011 Reviewed Revision 2.1 04/24/2012 Reviewed Revision 2.2 01/10/2013 Revised
3.0 Persons Affected This policy affects all CID clients who are contracting with CID as their Utilization Management vendor for purposes of peer review, and who want their complete Utilization Management program to be under the supervision of CID Medical Director. Client’s who contract with CID for peer review purposes only, and who do not wish to have their entire Utilization Management program to be under the supervision of the CID Medical Director, are not governed by this policy.
4.0 Policy The policy of CID Management is to ensure that clients, who contract with CID as their Utilization Management vendor for purposes of peer review, and who want their complete Utilization Management program to be under the supervision of CID Medical Director, operate their Utilization Management process in a manner compliant with the CA Labor Code and Regulations.
9000-2
5.0 Definitions
Definitions of terms are set forth in Policy 1000.
6.0 Procedures 6.1 Utilization Management Business Hours
6.1.1 The client shall ensure their office is staffed for utilization review
operations between 9:00 a.m. and 5:30 p.m. local time on all business days in all time zones in which the client maintains business operations.
6.1.2 Business days shall not include the following holidays:
6.1.2.1 Civil Code 7. Holidays within the meaning of this code are every Sunday and such other days as are specified or provided for as holidays in the Government Code of the State of California.
6.1.2.2 Civil Code 7.1. Optional bank holidays within the meaning of
Section 9 are: • Any closing of a bank because of an extraordinary situation, as
that term is defined in the Bank Extraordinary Situation Closing Act (Chapter 20 (commencing with Section 3600) of Division 1 of the Financial Code).
• Every Saturday • Every Sunday • January 1st • The third Monday in January, known as “Dr. Martin Luther
King, Jr. Day” • February 12, known as “Lincoln Day” • The third Monday in February • The last Monday in May • July 4th • The first Monday in September • September 9th, known as “Admission Day” • The second Monday in October, known as “Columbus Day” • November 11th, known as “Veteran’s Day” • December 25th • Good Friday from 12 noon until closing • The Thursday in November appointed as “Thanksgiving Day” • Any Monday following any Sunday on which January 1st,
February 12th, July 4th, September 9th, November 11th, or December 25th falls.
9000-3
• Any Friday preceding any Saturday on which July 4th, September 9th, or December 25th falls.
6.2 Utilization Management In Business Hours Communications Access
6.2.1 The client shall ensure that they maintain a telephone number for use in
utilization management operations. This telephone number need not be dedicated for utilization management operations alone.
6.2.2 The client shall ensure that they maintain a fax number for use in utilization management operations. This fax number need not be dedicated for utilization management operations alone.
6.2.3 The client shall ensure that the client’s phone number, fax number, and US
postal address, or CID’s phone number, fax number, and US postal address, are printed on all utilization management forms and on all generated utilization management correspondences.
6.2.4 The client shall distribute the phone number, fax number, and US postal
address to all parties as they deem appropriate.
6.3 Utilization Management After Hours Communications Access 6.3.1 The client shall ensure that they maintain a 24-hour voice mail service that
allows review stakeholders to leave messages after regular business hours. 6.3.2 The client shall ensure that they maintain a 24-hour fax service that allows
clients and review stakeholders to fax requests for authorization, appeals consideration or re-consideration after regular business hours.
6.3.3 The client shall ensure that instructions are left on a voice mail recording
instructing review stakeholders how to contact the client in case of emergency.
6.4 Utilization Management Communications Response
6.4.1 The client shall check their US Post mailbox once per business day after
standard US post delivery time. 6.4.2 The client shall check voice mail messages a minimum of four times per
business day. 6.4.3 The client shall check emails in-boxes a minimum of four times per
business day. 6.4.4 The client shall reply to mail, voice mail, email, or fax messages within 1
business day of receipt.

9000-4
6.4.5 The client shall reply to mail, voice mail, email or fax messages during
reasonable and normal business hours unless otherwise mutually agreed to by the party to be contacted.
6.4.6 The client shall log the date and content of received mail, voice mail,
email or fax message within the CID system, if the communication directly referenced a review or claim in the CID system.
6.4.7 The client shall log the date and content of their response to the mail,
voice mail, email or fax message within the CID system, if the communication directly referenced a review or claim in the CID system.
6.5 Utilization Management Communications Etiquette
6.5.1 The client shall maintain the highest levels of professionalism in all
communications associated with utilization management which shall include: 6.5.1.1 Answering communications promptly and courteously 6.5.1.2 Providing proper identification, including own name (full or
partial), job title, and company name when placing and answering communications
6.5.1.3 Showing respect and courtesy by using the stakeholder’s full name,
title or rank, except where the circumstances are such that the use of the callers first name would be more appropriate
6.5.1.4 Ensuring that transferred calls are answered before disconnecting
from the stakeholder 6.5.1.5 Handing stakeholder communications in a thoughtful, considerate,
patient and helpful manner.
6.6 Telephonic Inquiry Regarding Utilization Management Services 6.6.1 Upon receipt of a non-clinical question regarding the utilization
management process, the client shall respond to the inquiry giving as much detail as required to satisfy the inquiry. The response shall not violate CID’s confidentiality policy.
6.6.2 Should the inquiry exceed the knowledge of the client, the communication
shall be transferred to CID for response.
6.7 Utilization Management Electronic Review File

9000-5
6.7.1 Once a request for authorization is submitted; if there has been a
utilization review decision to modify, deny or delay the same requested goods or services; from the same provider; within the past 12 months; then no further action is required unless the further recommendation is supported by a documented change in the facts material to the basis of the utilization review decision.
6.7.2 Once a request for authorization, appeals consideration, or re-consideration has been submitted, the client shall utilize the CID secured web-site and proprietary software to create an electronic review file for the request for authorization, appeals consideration, or re-consideration.
6.7.3 The client shall ensure that the electronic review file contain all elements
outlined in Policy 3010 if applicable to the claim and review.
6.8 Conflict of Interest
6.8.1 Each client staff member involved in the utilization management process shall sign a letter stating that they shall not perform utilization management services in situations where a conflict of interest exists.
6.8.2 Each client staff member shall be trained on recognizing conflict of
interest situations.
6.8.3 If, in the performance of utilization management duties, a client staff member discovers that they have a conflict of interest, they shall use the CID system to recuse themselves from the review and have it re-assigned to an alternate staff member.
6.8.4 The CID system shall record the conflict of interest, and the re-assignment
of work duties, as an activity within the CID system.
6.8.5 To avoid conflict of interest situations, the client specifically does not have a system for reimbursement, bonuses, or incentives to staff based directly or indirectly on consumer utilization of health care services.
6.9 Confidentiality
6.9.1 The client shall ensure that all information that identifies a specific
individual shall be kept confidential and shall not be disclosed to any individual or organization outside of disclosures permitted or required by law.
6.10 Pre-review Screening

9000-6
6.10.1 The Medical Director and Clinical Director shall create the pre-review screening script and shall revise it as deemed necessary. This shall be done on a frequency of not less than annually.
6.10.2 A copy of the pre-review screening script shall be provided to the client in
case they choose to perform pre-review screening. 6.10.3 The Medical Director or Clinical Director shall ensure that the client is
trained on how to perform pre-review screening. 6.10.4 The Clinical Director or Senior Clinical Member, shall be available by
phone at CID to assist the client with any questions regarding pre-review screening.
6.10.5 The client shall ensure that:
6.10.5.1 Pre-review screening occurs within 2 business days of
receiving the request for authorization, appeals consideration, or re-consideration, or occurs the day of receipt for expedited reviews.
6.10.5.2 Pre-review screening shall include any of the following:
6.10.5.2.1 Collection of structured clinical data defined as clinical
information that is precise and permits exact matching against explicit medical terms, diagnoses or procedure codes, or other explicit choices, without the need for interpretation,
6.10.5.2.2 Asking scripted clinical questions, 6.10.5.2.3 Accepting responses to scripted clinical questions, 6.10.5.2.4 Taking specific action including certification and
assignment of length of stay explicitly linked to each of the possible responses.
6.10.5.3 Pre-review screening shall not include any of the following:
6.10.5.3.1 Applying clinical judgment or interpretation,
6.10.5.3.2 Accepting unstructured clinical information,
6.10.5.3.3 Deviating from script,
6.10.5.3.4 Engaging in unscripted clinical dialogue,
9000-7
6.10.5.3.5 Asking clinical follow up questions,
6.10.5.3.6 Issuing non-certifications.
6.10.5.4 As a component of pre-review screening, the client shall be
able to ask the provider if an amended treatment plan would be acceptable. If the provider agrees, and submits a written statement that he/she is withdrawing the original request and submitted an amended request, then the client shall be able to certify the request if the requested service/procedure does not match the Peer Review Triggers outlined by the Medical Director. If the written amended is not received within 24 hours, the client shall process the review as normal.
6.11 Notification of Dispute of Liability
6.11.1 If the claims administrator disputes its liability for the requested medical
treatment under this subdivision, it may, no later than five (5) business days from receipt of the request for authorization, issue a written decision deferring utilization review of the requested treatment. The written decision must be sent to the requesting physician, the injured worker, and if the injured worker is represented by counsel, the injured worker's attorney. The written decision shall only contain the following information specific to the request: 6.11.1.1 The date on which the request for authorization was first
received.
6.11.1.2 A description of the specific course of proposed medical treatment for which authorization was requested.
6.11.1.3 A clear, concise, and appropriate explanation of the reason for the claims administrator’s dispute of liability for either the injury, claimed body part or parts, or the recommended treatment.
6.11.1.4 A plain language statement advising the injured employee that any dispute under this subdivision shall be resolved either by agreement of the parties or through the dispute resolution process of the Workers’ Compensation Appeals Board.
6.11.1.5 The following mandatory language: “You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me (insert claims adjuster’s name in parentheses) at (insert telephone number). However, if you are represented by an

9000-8
attorney, please contact your attorney instead of me.”
6.11.1.6 The following mandatory language: “For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-free 1-800-736-7401.”
6.12 Notification of Extension of review due date 6.12.1 During the utilization management process, the client may determine that
the review may not be completed in the allowed timeframes and that a notification of extension of review due date must be sent.
6.12.2 The client shall send the notification of extension of review due date
within 2 business days of receiving the request for authorization or on the day of receipt for expedited reviews.
6.12.3 The situations in which a notification of extension of review due date may
be sent are:
6.12.3.1 The necessary medical information reasonably needed to make a determination is not present and needs to be requested from the provider
6.12.3.2 The client determines that a specialized consultation and
review of medical information by an expert reviewer is required in order to make an appropriate determination.
6.12.4 The notification of extension of review due date shall contain the
anticipated date on which a decision will be rendered and for California based claims shall include the following statement: “If the injured worker believes that a bona fide dispute exists relating to his or her entitlement to medical treatment, the injured worker or the inured worker’s attorney may file an Application for Adjudication of Claim and Request for Expedited Hearing, DWC Form 4, in accordance with sections 10136(b)(1), 10400, and 10408.”
6.12.5 If a notification of extension of review due date is sent to the provider
requesting additional information that the client deems is reasonably necessary to make the determination, then:
6.12.5.1 The information requested shall be limited to information
reasonably necessary to certify the admission, procedure or treatment, length of stay, or frequency or duration of services.
Robert Ward � 1/10/13 2:25 PMComment [1]: New policy section based on SB863.
9000-9
6.12.5.2 The notification of extension of review due date may be
delivered to any party specified by the client including, but not limited to: 6.12.5.2.1 Claims administrator 6.12.5.2.2 Nurse case manager
6.12.5.2.3 Attending physician
6.12.5.2.4 Requesting physician
6.12.5.2.5 Provider(s) of services or goods other than the attending
or requesting physicians
6.12.5.2.6 Patient
6.12.5.2.7 Patient’s legal counsel
6.12.5.2.8 Client’s legal counsel
6.12.5.3 If the client indicates that they do not want CID to distribute the notification of extension of review due date to a party that is required law to receive said notifications of extension of review due date, the client shall assume the responsibility of distributing these notifications of extension of review due date themselves.
6.12.5.4 Notifications of extension of review due date may be delivered
to the appropriate parties via any method specified by the client including, but not limited to secured electronic means, fax, US mail, and courier service.
6.12.5.5 If the client indicates that they do not want CID to distribute
the notification of extension of review due date to a party via a method specified by law, the client shall assume the responsibility of distributing these notifications of extension of review due date themselves.
6.12.5.6 The requested information shall be accepted from any
reasonably reliable source.
6.12.5.7 If the requested information is received within 2 business days, the client shall upload the requested information to the electronic review file and shall assign the review for completion.
9000-10
6.12.5.8 If the requested information is not received within 2 business days, the CID system shall send an additional copy of the request for information to the requesting physician.
6.12.5.9 Steps 6.11.5.7 and 6.11.5.8 shall continue until the information
is received or until the 14th calendar day following the receipt of the request for authorization, whichever occurs first.
6.12.5.10 If the requested information is not received by the 14th calendar
day after the receipt of the request for authorization, the CID system shall:
6.12.5.10.1Add the following language to the review for California
based reviews: “CID faxed the provider on (dates) in order to request the following information: (requested information here). The CID clinical staff deemed that this additional information was reasonably necessary to make the determination of appropriateness of care. As of this date, the provider has not submitted the requested data. To comply with timeframes for utilization review established in LC 4610, authorization is hereby denied in accordance with CCR 9792.9(c)(2)(A); or CCR 9792.9.1(c)(3)(A). The request will be reconsidered upon receipt of the information requested.”
6.12.5.10.2Assign the review to a clinical peer reviewer for
completion
6.12.6 If a notification of extension of review due date is sent to the provider informing them that a specialized consultation and review of medical information by an expert reviewer is required in order to make an appropriate determination then: 6.12.6.1 The notification of extension of review due date shall
include the specialty of the expert reviewer consulted 6.12.6.2 The notification of extension of review due date may be
delivered to any party specified by the client including, but not limited to:
6.12.6.2.1 Claims administrator 6.12.6.2.2 Nurse case manager
6.12.6.2.3 Attending physician
Robert Ward � 1/10/13 2:17 PMComment [2]: Amended to match new reg numbers; may not match system language.

9000-11
6.12.6.2.4 Requesting physician
6.12.6.2.5 Provider(s) of services or goods other than the attending
or requesting physicians
6.12.6.2.6 Patient
6.12.6.2.7 Patient’s legal counsel
6.12.6.2.8 Client’s legal counsel
6.12.6.3 If the client indicates that they do not want CID to distribute the notification of extension of review due date to a party that is required law to receive said notifications of extension of review due date, the client shall assume the responsibility of distributing these notifications of extension of review due date themselves.
6.12.6.4 Notifications of extension of review due date may be
delivered to the appropriate parties via any method specified by the client including, but not limited to secured electronic means, fax, US mail, and courier service.
6.12.6.5 If the client indicates that they do not want CID to
distribute the notification of extension of review due date to a party via a method specified by law, the client shall assume the responsibility of distributing these notifications of extension of review due date themselves
6.12.6.6 The review shall be forwarded to the expert reviewer
immediately
6.12.6.7 Once a determination is received from the expert reviewer, it shall be uploaded to the system within the same business day and shall be immediately distributed to the stakeholders as per client contract.
6.13 Peer Review Triggers
6.13.1 Each client has developed their unique list of Peer Review Triggers. If the
request for authorization is consistent with the triggers, the client shall ensure that the review is forwarded to CID for peer review.
6.14 Forwarding Requests for Authorization to Peer Review
9000-12
6.14.1 The client shall ensure that requests for authorization are forwarded to Peer Review no later than the third day after receipt unless: 6.14.1.1 The client has sent a notification of extension of review due
date requesting additional information in which case the request for authorization shall be forwarded to Peer Review no later than the third day following receipt of the requested information, or the twelfth day after receipt of the original request, whichever occurs first, or
6.14.1.2 The client has sent notification of expert review in which
case the request for authorization shall be forwarded to Peer Review immediately after the notification of expert review has been sent.
6.15 Reimbursement for Duplication of Records
6.15.1 To avoid requesting duplicate copies of records, prior to requesting
additional information from the provider, the client shall review all documents received on a claim. Only in the event that the client does not have a copy of the document, shall the client contact the provider for a copy.
6.15.2 If the client requests a duplicate copy of a previously submitted record,
then the client shall reimburse providers for duplicate records in compliance with labor code and regulations.
6.15.3 The client shall attach all relevant medical records to the review to avoid
requiring the provider to submit duplicate records and to allow all parties to see the documents considered when the decision was made.
6.15.4 If providers contact CID to request payment for duplication of records via
any means including, but not limited to: telephone, fax, mail, email, or web, CID shall inform them to contact the claims administrator.
6.16 Utilization Management Correspondence
6.16.1 During the performance of utilization management, the following documents may be created by the CID system:
6.16.1.1 Notice of Dispute of Liability. This correspondence is
generated when the request for authorization is deemed to non-industrial.
6.16.1.2 Request for utilization review received. This correspondence is generated when the request for authorization,
Robert Ward � 1/10/13 2:28 PMComment [3]: New. This template does not yet exist; nor have we decided on the process for sending it. We do need it.
9000-13
appeals consideration, or re-consideration is first uploaded into the CID system.
6.16.1.3 Notification of extension of review due date – additional information required. This correspondence is generated when it is determined that additional clinical information is required in order to make an appropriate determination.
6.16.1.4 Notification of extension of review due date – additional
tests/procedures required. This correspondence is generated when it is determined that additional clinical tests and/or procedures must be performed, and their results forwarded to CID, in order to make an appropriate determination.
6.16.1.5 Notification of extension of review due date – expert
reviewer. This correspondence is generated when it is determined that an expert clinical reviewer is needed to review the request.
6.16.1.6 Notification the provider submitted additional information.
This correspondence is generated when the provider submits the additional information, or the additional test and/or procedures findings, requested following a notification of extension of review due date.
6.16.1.7 Determination letter – Certified. This correspondence is
generated when it is determined that the request for authorization, appeals consideration, or re-consideration is being certified.
6.16.1.8 Determination letter – Modified. This correspondence is
generated when it is determined that the request for authorization, appeals consideration, or re-consideration is being partially certified.
6.16.1.9 Determination letter – Non-certified. This correspondence
is generated when it is determined that the request for authorization, appeals consideration, or re-consideration is being non-certified.
6.16.1.10 Determination letter – Conditionally Non-certified. This
correspondence is generated when there has been a request for additional information, or the clinical findings from additional tests and/or procedures, and the information has not been received by the 14th day following original receipt of the request for authorization, appeals consideration, or re-consideration.

9000-14
6.16.1.11 Review placed on hold by CID. This correspondence generates when CID places a review on hold pending additional information from the claims administrator that is required to complete the review.
6.16.1.12 Review placed on hold by client. This correspondence
generates when the client places a review on hold.
6.16.1.13 Review off of hold, back in progress. This correspondence generates when a review is taken off of CID enforced hold or client enforced hold, and is assigned to either an initial clinical reviewer or a clinical peer reviewer.
6.16.1.14 Review withdrawn by CID. This correspondence generates
when CID withdraws a review that it began in error.
6.16.1.15 Review withdrawn by client. This correspondence generates when the client requests that CID cease action on a review and withdraws it from review.
6.16.2 All correspondences shall include a reference number to the specific
review in question.
6.16.3 All determination correspondences shall contain the following elements as indicated in Policy 3800 (Utilization Management Correspondence).
6.16.4 The correspondences shall be delivered to the following parties, as
identified on the review, unless specifically excluded by the client contract:
6.16.4.1 Claims administrator
6.16.4.2 Nurse case manager
6.16.4.3 Attending physician
6.16.4.4 Requesting physician
6.16.4.5 Facility rendering service
6.16.4.6 Secondary physicians
6.16.4.7 Provider(s) of services or goods other than the attending or
requesting physicians
6.16.4.8 Patient
Robert Ward � 1/10/13 2:20 PMComment [4]: This section originally contained all of the required letter elements for CA, including the mandatory language. Since this policy is describing letters being generated through the CID portal (rather than informing clients what they must do), it makes sense to refer back to the relevant policy; rather than trying to keep multiple sections compliant with changing regulatory requirements.

9000-15
6.16.4.9 Patient’s legal counsel
6.16.4.10 Client’s legal counsel
6.16.5 If the client indicates that they do not want CID to distribute the
correspondences to a party that is required by law to receive said correspondences, the client shall assume the responsibility of distributing these correspondences themselves.
6.16.6 Correspondences shall be delivered to the parties via the following
specified method, unless the client contract specifies otherwise:
6.16.6.1 Claims administrator by email within 24 hours of decision
6.16.6.2 Nurse case manager by email within 24 hours of decision
6.16.6.3 Attending physician by fax within 24 hours of decision
6.16.6.4 Requesting physician by fax within 24 hours of decision
6.16.6.5 Facility rendering service by fax within 24 hours of decision
6.16.6.6 Secondary physicians by fax within 24 hours of decision
6.16.6.7 Provider(s) of services or goods other than the attending or
requesting physicians by fax within 24 hours of decision
6.16.6.8 Patient by mail, to be mailed within 24 hours of decision for concurrent review and within 1 business day of decision for all other reviews
6.16.6.9 Patient’s legal counsel by mail, within 24 hours of decision for concurrent review and within 1 business day of decision for all other reviews
6.16.6.10 Client’s legal counsel by mail, to be mailed within 1
business day of decision
6.16.7 If the client indicates that they do not want CID to distribute correspondences to a party via a method specified by law, the client shall assume the responsibility of distributing these correspondences themselves.

9000-16
6.16.8 Unless specifically barred by contract with the client, upon request by any authorized party, CID shall re-issue a copy of the original communication and forward by fax or mail. If CID is barred from doing so by contract with client, the party shall be advised to contact the claims administrator for a copy of the communication.
6.17 Utilization Management Turn Around Times:
CID defines its timeframes for utilization management for all reviews (prospective, concurrent and retrospective) as described in Policy 3900 (Utilization Management Turn Around Times)
6.17.1 Requesting physicians and/or clients shall be required to indicate the
requested turn around time (standard, expedited, rush, stat) for review of a request for authorization, appeals consideration or re-consideration. If no timeframe is indicated, it shall be concluded that a standard turn around time is requested.
6.17.2 Upon receipt of a request for authorization, appeals consideration, or re-
consideration, the CID system shall review the following if applicable: if the request is prospective/concurrent/retrospective, the date the request was received by the client, the date the client sent a notification of extension of review due date, the date the client received additional information, the date the request was received by CID. Based on this information, the CID system shall determine the appropriate due date for the review giving consideration to the utilization management laws and regulations.
6.17.3 The entering party shall then review the submitted documents to determine
if the submitter has requested a standard, expedited, rush, or stat request. If the requested response date is earlier than the due date calculated in accordance with Policy 3900, California addendum, then the CID system shall update the due date accordingly. If not, the CID system shall retain the due date calculated in accordance with Policy 3900, California addendum.
6.17.4 The client shall oversee reviews in progress, if they have not been
submitted to CID for peer review, to ensure their completion by the due date.
6.17.5 Urgent Situations Posing an Immediate Threat to the Health and Safety of
Patients (a.k.a. expedited review or “emergency health care services”)
6.17.5.1 If a situation presents where a party communicates to the client that the health or safety of a patient is under immediate threat, the call shall be transferred directly to the Clinical Director or, in his/her absence, to the Director of Production.
Robert Ward � 1/10/13 2:21 PMComment [5]: This section originally contained a very detailed description of CA timelines.
Robert Ward � 1/10/13 2:22 PMComment [6]: This section originally referred to the detailed description of timelines that has been removed form this policy.
Robert Ward � 1/10/13 2:24 PMComment [7]: Perhaps we should revise this process to be a call to a shared number that rings for me, the Assoc Clin Dirs; and possibly the Dir of Prod.

9000-17
6.17.5.2 The Clinical Director, or Director of Production, shall
assign the initial clinical reviewer, clinical peer reviewer, and QAQC reviewer that are immediately available for reviews. The availability of each reviewer shall be confirmed by the Clinical Director or Director of Production by telephone.
6.17.5.3 The Clinical Director, or Director of Production, shall
evaluate the progress of the review by checking its status at intervals not to exceed 30 minutes.
6.17.5.4 Immediately upon reaching a determination, the CID
system shall generate a determination letter that shall be immediately faxed to the provider.
6.17.5.5 Immediately upon noting a determination has been reached,
the Clinical Director, or Director of Production, shall contact the requesting provider via telephone to verify the receipt of the determination to ensure its arrival.
6.18 Quality Assurance Quality Control
6.18.1 On a quarterly basis, the Quality Assurance/Quality Control Committee
shall meet. 6.18.2 On quarterly basis, the Clinical Director shall present statistics compiled
from reviews performed by the client for review by the Quality Assurance/Quality Control Committee.
6.18.3 The Quality Assurance/Quality Control Committee shall determine if any
changes, retraining, or updates are required. If so, they shall task the Clinical Director with enacting the changes, retraining, or updates.
6.19 Grievances
6.19.1 The Clinical Director shall ensure that the Grievance Process is outlined on all determination letters.
6.19.2 The Clinical Director shall ensure that the Grievance Process is posted on
the CID webpage at http://www.cidmcorp.com/support/grievance.htm.
6.19.3 The Clinical Director shall ensure that the client is trained on, and can answer questions related to, the grievance process
6.19.4 CID encourages all stakeholders to resolve individual inquires and
problems without the initiation of a formal grievance. Any party who has
9000-18
an inquiry or complaint may contact CID at 1-866-301-6568 for verbal resolution.
6.19.5 In the event that a complaint may not be settled at the informal level and
the party is still dissatisfied, he/she will be advised to file a formal grievance.
6.19.6 Grievances must be submitted within one year of occurrence and shall be
submitted in writing. The written grievance shall contain the following information:
6.19.6.1 The individual’s name, address and telephone number 6.19.6.2 A summary of the grievance, any previous contact made
with CID, and a description of the relief sought 6.19.6.3 The individuals signature 6.19.6.4 The date the grievance was signed.
6.19.7 The written grievance shall be mailed to P.O. Box 4379, Westlake Village,
CA 91359. 6.19.8 Upon receipt, the written grievance shall be forwarded to the chair of the
Grievance Committee who shall acknowledge the receipt of the grievance within 5 business days.
6.19.9 The Grievance Committee shall investigate the grievance and shall notify
the party of the final decision in writing within 30 calendar days. 6.19.10Should the Grievance Committee determine that any action is required as
a result of the grievance, they shall communicate this determination to the Clinical Director who shall be responsible for ensuring the follow up action occurs.

9000-19
CID Management Pre-Review Screening Script
NOTE: You may not ask questions that call for:
o Applying clinical judgment or interpretation, o Accepting unstructured clinical information, o Deviating from script, o Engaging in unscripted clinical dialogue, o Asking clinical follow up questions, o Issuing non-certifications.
My name is _________________ and I am a(n) ___(job title)___working at ___(company)____. We have received a request for (authorization / appeals consideration / re-consideration) from ____(physician)_______ on the claim for ___(patient)_____. In order to start the review for this request, we require the following additional information: Patient Demographics: Patient first and last names, date of birth and/or social security number, contact information Provider Demographics Provider first and last names, degree and/or specialty, federal tax id number and /or license
number, contact information (address, phone, fax, email) Claim Demographics Claim number and/or date of injury Adjustor name and contact information (company, address, phone, fax, email) Medical Information Scripted Questions
1. Can you please provide the patient diagnoses including ICD9 codes? 2. Can you please provide clarification of the physicians recommended treatment plan,
specifically: a. a description of the service to be rendered, b. the date range in which the services will be rendered, c. the number of services to be rendered, d. and the CPT codes for the services requested.
3. Can you please provide the number of visits the patient has previously made to: a. the provider? b. conservative care providers such as physical therapists or chiropractors?
4. Can you please indicate if the patient has previously undergone diagnostic testing such as MRI or EMG/NCV, and if so, the dates of these studies and their results?
5. Can you please indicate if the patient is seeing any other providers for this condition? If so, please provide their names, contact information and specialties.
6. You have submitted a request for: ___________________. Would you consider amending the request to: ____________________? If so, please submit a written note that states that you are withdrawing your original request and submitted the amended request in its place.

9000-20
CID Management
Pre-Review Script for Written Request for Medical Documentation The request was submitted without clinical information/reporting. Please forward the appropriate clinical reporting/documentation which: 1) displays the provider’s request for the above procedure/service; 2) provides the patient’s subjective and objective status at the time the procedure/service was requested; and 3) contains the provider’s clinical rationale supporting the medical necessity of the request.
Robert Ward � 1/10/13 2:30 PMComment [8]: This has been in our pre-screening policy (3100) for some time. It is new to Policy 9000.
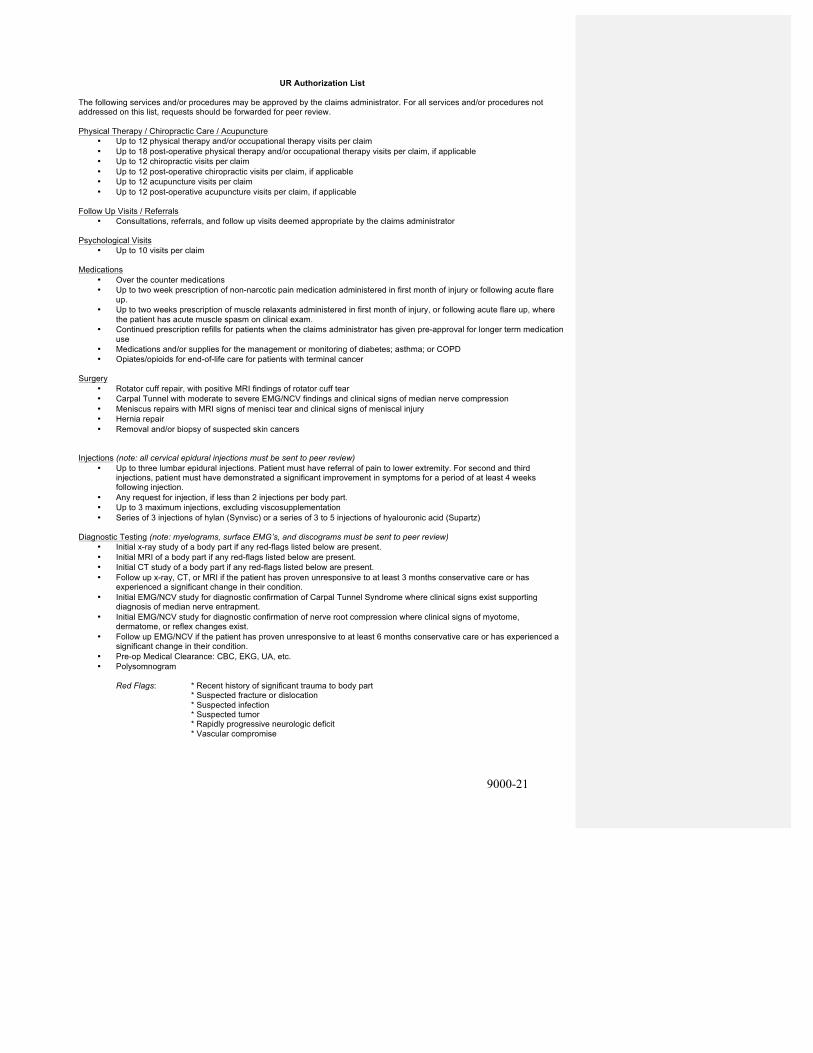
9000-21
UR Authorization List The following services and/or procedures may be approved by the claims administrator. For all services and/or procedures not addressed on this list, requests should be forwarded for peer review. Physical Therapy / Chiropractic Care / Acupuncture
• Up to 12 physical therapy and/or occupational therapy visits per claim • Up to 18 post-operative physical therapy and/or occupational therapy visits per claim, if applicable • Up to 12 chiropractic visits per claim • Up to 12 post-operative chiropractic visits per claim, if applicable • Up to 12 acupuncture visits per claim • Up to 12 post-operative acupuncture visits per claim, if applicable
Follow Up Visits / Referrals
• Consultations, referrals, and follow up visits deemed appropriate by the claims administrator
Psychological Visits • Up to 10 visits per claim
Medications • Over the counter medications • Up to two week prescription of non-narcotic pain medication administered in first month of injury or following acute flare
up. • Up to two weeks prescription of muscle relaxants administered in first month of injury, or following acute flare up, where
the patient has acute muscle spasm on clinical exam. • Continued prescription refills for patients when the claims administrator has given pre-approval for longer term medication
use • Medications and/or supplies for the management or monitoring of diabetes; asthma; or COPD • Opiates/opioids for end-of-life care for patients with terminal cancer
Surgery
• Rotator cuff repair, with positive MRI findings of rotator cuff tear • Carpal Tunnel with moderate to severe EMG/NCV findings and clinical signs of median nerve compression • Meniscus repairs with MRI signs of menisci tear and clinical signs of meniscal injury • Hernia repair • Removal and/or biopsy of suspected skin cancers
Injections (note: all cervical epidural injections must be sent to peer review)
• Up to three lumbar epidural injections. Patient must have referral of pain to lower extremity. For second and third injections, patient must have demonstrated a significant improvement in symptoms for a period of at least 4 weeks following injection.
• Any request for injection, if less than 2 injections per body part. • Up to 3 maximum injections, excluding viscosupplementation • Series of 3 injections of hylan (Synvisc) or a series of 3 to 5 injections of hyalouronic acid (Supartz)
Diagnostic Testing (note: myelograms, surface EMG’s, and discograms must be sent to peer review)
• Initial x-ray study of a body part if any red-flags listed below are present. • Initial MRI of a body part if any red-flags listed below are present. • Initial CT study of a body part if any red-flags listed below are present. • Follow up x-ray, CT, or MRI if the patient has proven unresponsive to at least 3 months conservative care or has
experienced a significant change in their condition. • Initial EMG/NCV study for diagnostic confirmation of Carpal Tunnel Syndrome where clinical signs exist supporting
diagnosis of median nerve entrapment. • Initial EMG/NCV study for diagnostic confirmation of nerve root compression where clinical signs of myotome,
dermatome, or reflex changes exist. • Follow up EMG/NCV if the patient has proven unresponsive to at least 6 months conservative care or has experienced a
significant change in their condition. • Pre-op Medical Clearance: CBC, EKG, UA, etc. • Polysomnogram
Red Flags: * Recent history of significant trauma to body part
* Suspected fracture or dislocation * Suspected infection * Suspected tumor * Rapidly progressive neurologic deficit * Vascular compromise

9000-22
Durable Medical Equipment • DME items, costing $500 or less • Prosthetic devices (limbs, hearing aids, glass eyes, etc.) • CPAP or BiPAP and supplies in cases of diagnosed sleep apnea
Miscellaneous
• Care consistent with stipulated award • Care consistent with AME/PQME report recommendations • Care consistent with second opinion consults formally approved by the client • Up to 1 week of Home Health Care/transfer to Skilled Nursing Facility/Convalescent/Residential Facility • Non-invasive/remote checks of function of implanted devices (pacemakers, pumps, etc.)
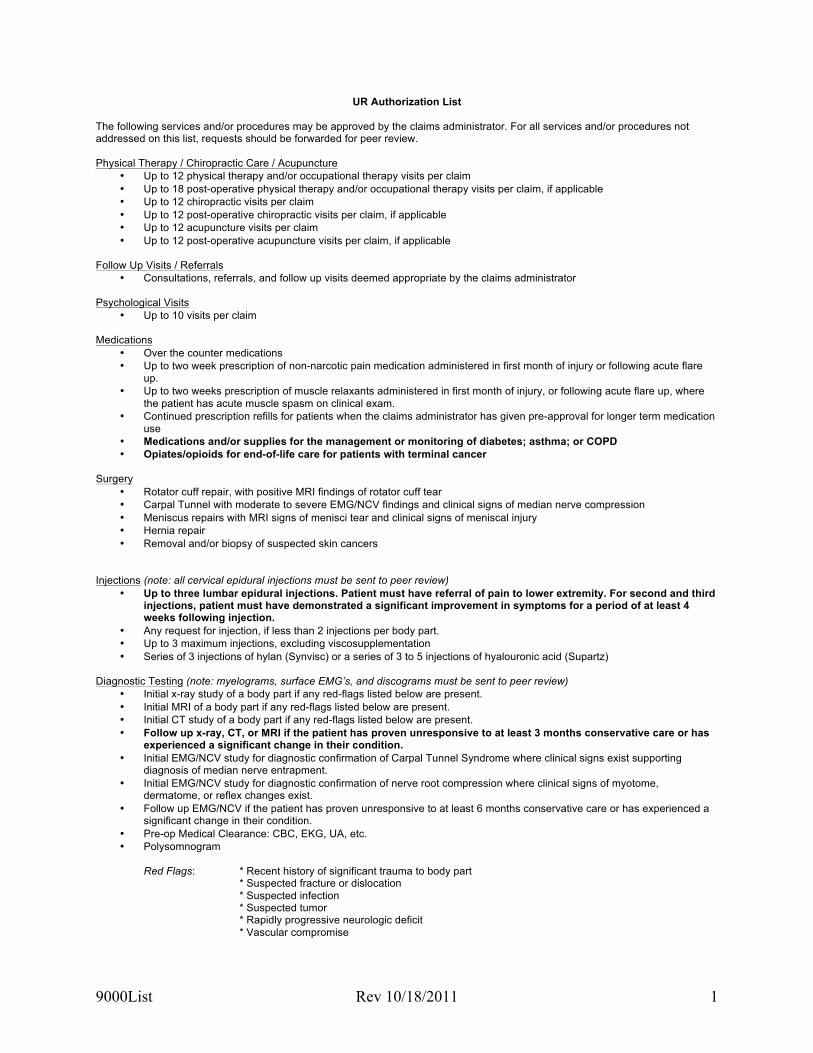
9000List Rev 10/18/2011 1
UR Authorization List The following services and/or procedures may be approved by the claims administrator. For all services and/or procedures not addressed on this list, requests should be forwarded for peer review. Physical Therapy / Chiropractic Care / Acupuncture
• Up to 12 physical therapy and/or occupational therapy visits per claim • Up to 18 post-operative physical therapy and/or occupational therapy visits per claim, if applicable • Up to 12 chiropractic visits per claim • Up to 12 post-operative chiropractic visits per claim, if applicable • Up to 12 acupuncture visits per claim • Up to 12 post-operative acupuncture visits per claim, if applicable
Follow Up Visits / Referrals
• Consultations, referrals, and follow up visits deemed appropriate by the claims administrator
Psychological Visits • Up to 10 visits per claim
Medications • Over the counter medications • Up to two week prescription of non-narcotic pain medication administered in first month of injury or following acute flare
up. • Up to two weeks prescription of muscle relaxants administered in first month of injury, or following acute flare up, where
the patient has acute muscle spasm on clinical exam. • Continued prescription refills for patients when the claims administrator has given pre-approval for longer term medication
use • Medications and/or supplies for the management or monitoring of diabetes; asthma; or COPD • Opiates/opioids for end-of-life care for patients with terminal cancer
Surgery
• Rotator cuff repair, with positive MRI findings of rotator cuff tear • Carpal Tunnel with moderate to severe EMG/NCV findings and clinical signs of median nerve compression • Meniscus repairs with MRI signs of menisci tear and clinical signs of meniscal injury • Hernia repair • Removal and/or biopsy of suspected skin cancers
Injections (note: all cervical epidural injections must be sent to peer review)
• Up to three lumbar epidural injections. Patient must have referral of pain to lower extremity. For second and third injections, patient must have demonstrated a significant improvement in symptoms for a period of at least 4 weeks following injection.
• Any request for injection, if less than 2 injections per body part. • Up to 3 maximum injections, excluding viscosupplementation • Series of 3 injections of hylan (Synvisc) or a series of 3 to 5 injections of hyalouronic acid (Supartz)
Diagnostic Testing (note: myelograms, surface EMG’s, and discograms must be sent to peer review)
• Initial x-ray study of a body part if any red-flags listed below are present. • Initial MRI of a body part if any red-flags listed below are present. • Initial CT study of a body part if any red-flags listed below are present. • Follow up x-ray, CT, or MRI if the patient has proven unresponsive to at least 3 months conservative care or has
experienced a significant change in their condition. • Initial EMG/NCV study for diagnostic confirmation of Carpal Tunnel Syndrome where clinical signs exist supporting
diagnosis of median nerve entrapment. • Initial EMG/NCV study for diagnostic confirmation of nerve root compression where clinical signs of myotome,
dermatome, or reflex changes exist. • Follow up EMG/NCV if the patient has proven unresponsive to at least 6 months conservative care or has experienced a
significant change in their condition. • Pre-op Medical Clearance: CBC, EKG, UA, etc. • Polysomnogram
Red Flags: * Recent history of significant trauma to body part
* Suspected fracture or dislocation * Suspected infection * Suspected tumor * Rapidly progressive neurologic deficit * Vascular compromise

9000List Rev 10/18/2011 2
Durable Medical Equipment • DME items, costing $500 or less • Prosthetic devices (limbs, hearing aids, glass eyes, etc.) • CPAP or BiPAP and supplies in cases of diagnosed sleep apnea
Miscellaneous
• Care consistent with stipulated award • Care consistent with AME/PQME report recommendations • Care consistent with second opinion consults formally approved by the client • Up to 1 week of Home Health Care/transfer to Skilled Nursing Facility/Convalescent/Residential Facility • Non-invasive/remote checks of function of implanted devices (pacemakers, pumps, etc.)

Determination letter templates Dates of injury prior to 1/1/2013 and review before 7/1/2013

Review #«Id»
«project.doc_address» «project.doc_city», «project.doc_state» «project.doc_zip» «project.doc_phone» (p) «project.doc_fax» (fax)
«CurrentDate»
«FullName» «address.street1» «address.street2» «address.city» «address.state» «address.postalcode»
Request for Additional Information RE: Patient: «claim.patient.FullName»
Claim: «claim.claimnumber» Date request received by «organization.client_name»: «receivedbyclienttimestamp_string» Date request received by CID: «DateReceivedByUR_string»
Dear «FullName», We have been requested by «organization.client_name», to perform utilization review to determine if the requested health care services are medically necessary and appropriate. This letter is to notify you that the reviewer has determined that additional information is required to make a determination of medical necessity. We are requesting that the requesting provider submit the following information in order to allow us to complete this review: Physician requesting authorization: «physician.FullName» Specific Treatment Plan Requested: «requestedtreatmentplan_without_dates» Information Being Requested: «MostRecentRequestForMoreInfo.moreinforeq» This information may be faxed to CID at «project.doc_fax» or mailed to «project.doc_address» «project.doc_city», «project.doc_state» «project.doc_zip». Please feel free to contact us with any questions. Respectfully, CID Management «cc»
Utilization Review strictly analyzes the medical necessity of treatment requests.
Review #«Id»
«project.doc_address» «project.doc_city», «project.doc_state» «project.doc_zip» «project.doc_phone» (p) «project.doc_fax» (fax)
CID Management does not affirm the acceptance of this workers compensation claim.

Review #«Id»
«project.doc_address» «project.doc_city», «project.doc_state» «project.doc_zip» «project.doc_phone» (p) «project.doc_fax» (fax)
«CurrentDate»
«FullName» «address.street1» «address.street2» «address.city» «address.state» «address.postalcode»
Recommendation: CERTIFY RE: Patient: «claim.patient.FullName»
Claim: «claim.claimnumber» Date request received by «organization.client_name»: «receivedbyclienttimestamp_string» Date request received by CID: «DateReceivedByUR_string» Decision date: «decisionrendereddate_string»
Dear «FullName», We have been requested by «organization.client_name», to perform utilization review to determine if the requested health care services are medically necessary and appropriate. This letter is to notify you that the following health care services are certified as medically necessary: Specific Treatment Plan Requested «requestedtreatmentplan_without_dates» UR Determination «authorizedtreatmentplan» Clinical Rationale «clinical_rationale» Criteria/Guidelines Applied «guidelines» Please feel free to contact us should you have any additional questions regarding this claim or if medical necessity substantiates further treatment. Respectfully, «signoff_user.FullQualifiedPathOfSignatur» «signoff_user.FullName» «signoff_user.StateLicensesDisplayString» «signoff_user.BoardCertificationDisplaySt»

«cc»
Utilization Review strictly analyzes the medical necessity of treatment requests. CID Management does not affirm the acceptance of this workers compensation claim.
Review #«Id»
«project.doc_address» «project.doc_city», «project.doc_state» «project.doc_zip» «project.doc_phone» (p) «project.doc_fax» (fax)
«CurrentDate»
«FullName» «address.street1» «address.street2» «address.city» «address.state» «address.postalcode» RE: Patient: «claim.patient.FullName»
Claim: «claim.claimnumber» Date request received by «organization.client_name»: «receivedbyclienttimestamp_string» Date request received by CID: «DateReceivedByUR_string» Decision date: «decisionrendereddate_string»
Dear «FullName», We have been requested by «organization.client_name», to perform utilization review to determine if the requested health care services are medically necessary and appropriate for this claim. This letter is to notify you of our determination regarding medical necessity: Specific Treatment Plan Requested «requestedtreatmentplan_without_dates» UR Determination «authorizedtreatmentplan» Clinical Rationale «clinical_rationale» Criteria/Guidelines Applied «guidelines» Information regarding our optional internal appeals and reconsiderations processes is attached to this determination letter. If the requesting physician would like to discuss this determination with the reviewer, the requesting physician may contact CID at «project.doc_phone» so that a convenient time may be arranged for this discussion. All reviewers are available for at least four hours per week during normal business days from 9:00 a.m. to 5:30 p.m. PST. Please feel free to contact us should you have any additional questions regarding this claim. Respectfully,

«signoff_user.FullQualifiedPathOfSignatur» «signoff_user.FullName» «signoff_user.StateLicensesDisplayString» «signoff_user.BoardCertificationDisplaySt» «cc»
Utilization Review strictly analyzes the medical necessity of treatment requests. CID Management does not affirm the acceptance of this workers compensation claim.
CID Reconsiderations Process
For any treatment request which was conditionally denied, the treatment request will be reconsidered upon receipt of the requested information.
CID Optional Internal UR Appeals Process If the provider has not previously submitted an appeal for any treatment request which was modified or denied in this review, the patient or requesting provider has the option of submitting a request for appeal on a voluntary basis. The request for appeal must:
1. Be in writing; and 2. Be received by CID within thirty (30) days of the date of the original determination; and 3. Indicate if the appeal warrants an expedited review*; and 4. Contain either:
a. Additional information supporting the request; or b. The basis or rationale for disagreement with the denial.
Appeal requests which do not match the above requirements will not be considered. Appeals and/or Reconsiderations may be faxed to «project.doc_fax» or may be submitted via mail to «project.doc_address», «project.doc_city», «project.doc_state» «project.doc_zip». * Expedited appeals shall only be granted if:
1. the timeline for making a determination could seriously jeopardize the life or health of the patient or the ability of the patient to regain maximum function; or
2. the patient would be in severe pain that could not be adequately managed without the care or treatment under review.
If you disagree with the utilization review decision and wish to dispute it, you must send written notice of your objection to the claims administrator within 20 days of receipt of the utilization review decision in accordance with Labor Code section 4062. You must meet this deadline even if you are participating in the claims administrator’s internal utilization review appeals process. This 20-‐day time limit may be extended for good cause or by mutual agreement of the parties.
Additional Language required by California Labor Code and Regulations:
You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me «claim.examiner.FullName» at «claim.examiner.telephone». However, if you are represented by an attorney, please contact your attorney instead of me. For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-‐free 1-‐800-‐736-‐7401. The injured worker may file an Application for Adjudication of Claim and a Declaration of Readiness to Proceed (expedited trial) and request for an expedited hearing.
Review #«Id»
«project.doc_address» «project.doc_city», «project.doc_state» «project.doc_zip» «project.doc_phone» (p) «project.doc_fax» (fax)
«CurrentDate»
«FullName» «address.street1» «address.street2» «address.city» «address.state» «address.postalcode»
Recommendation: NON-‐CERTIFY
RE: Patient: «claim.patient.FullName» Claim: «claim.claimnumber» Date request received by «organization.client_name»: «receivedbyclienttimestamp_string» Date request received by CID: «DateReceivedByUR_string» Decision date: «decisionrendereddate_string»
Dear «FullName», We have been requested by «organization.client_name», to perform utilization review to determine if the requested health care services are medically necessary and appropriate for this claim. This letter is to notify you that the following health care serviced did not meet the established criteria for medical necessity: Specific Treatment Plan Requested «requestedtreatmentplan_without_dates» UR Determination «authorizedtreatmentplan» Clinical Rationale «clinical_rationale» Criteria/Guidelines Applied «guidelines» Information regarding our optional internal appeals process is attached to this determination letter. If the requesting physician would like to discuss this determination with the reviewer, the requesting physician may contact CID at «project.doc_phone» so that a convenient time may be arranged for this discussion. All reviewers are available for at least four hours per week during normal business days from 9:00 a.m. to 5:30 p.m. PST. Please feel free to contact us should you have any additional questions regarding this claim.

Respectfully, «signoff_user.FullQualifiedPathOfSignatur» «signoff_user.FullName» «signoff_user.StateLicensesDisplayString» «signoff_user.BoardCertificationDisplaySt» «cc»
Utilization Review strictly analyzes the medical necessity of treatment requests. CID Management does not affirm the acceptance of this workers compensation claim.

CID Optional Internal UR Appeals Process
If the provider has not previously submitted an appeal for any treatment request which was modified or denied in this review, the patient or requesting provider has the option of submitting a request for appeal on a voluntary basis. The request for appeal must:
1. Be in writing; and 2. Be received by CID within thirty (30) days of the date of the original determination; and 3. Indicate if the appeal warrants an expedited review*; and 4. Contain either:
a. Additional information supporting the request; or b. The basis or rationale for disagreement with the denial.
Appeal requests which do not match the above requirements will not be considered. Appeals and information may be faxed to «project.doc_fax» or may be submitted via mail to «project.doc_address», «project.doc_city», «project.doc_state» «project.doc_zip». * Expedited appeals shall only be granted if:
1. the timeline for making a determination could seriously jeopardize the life or health of the patient or the ability of the patient to regain maximum function; or
2. the patient would be in severe pain that could not be adequately managed without the care or treatment under review.
If you disagree with the utilization review decision and wish to dispute it, you must send written notice of your objection to the claims administrator within 20 days of receipt of the utilization review decision in accordance with Labor Code section 4062. You must meet this deadline even if you are participating in the claims administrator’s internal utilization review appeals process. This 20-‐day time limit may be extended for good cause or by mutual agreement of the parties.
Additional Language required by California Labor Code and Regulations: You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me «claim.examiner.FullName» at «claim.examiner.telephone». However, if you are represented by an attorney, please contact your attorney instead of me. For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-‐free 1-‐800-‐736-‐7401. The injured worker may file an Application for Adjudication of Claim and a Declaration of Readiness to Proceed (expedited trial) and request for an expedited hearing.

Determination letter templates Dates of injury 1/1/13 and after; and all dates of injury for utilization review 7/1/2013 and after.

Review #«Id»
«project.doc_address» «project.doc_city», «project.doc_state» «project.doc_zip» «project.doc_phone» (p) «project.doc_fax» (fax)
«CurrentDate»
«FullName» «address.street1» «address.street2» «address.city» «address.state» «address.postalcode»
Request for Additional Information RE: Patient: «claim.patient.FullName»
Claim: «claim.claimnumber» Date request received by «organization.client_name»: «receivedbyclienttimestamp_string» Date request received by CID: «DateReceivedByUR_string»
Dear «FullName», We have been requested by «organization.client_name», to perform utilization review to determine if the requested health care services are medically necessary and appropriate. This letter is to notify you that the reviewer has determined that additional information is required to make a determination of medical necessity. We are requesting that the requesting provider submit the following information in order to allow us to complete this review: Physician requesting authorization: «physician.FullName» Specific Treatment Plan Requested: «requestedtreatmentplan_without_dates» Information Being Requested: «MostRecentRequestForMoreInfo.moreinforeq» This information may be faxed to CID at «project.doc_fax» or mailed to «project.doc_address» «project.doc_city», «project.doc_state» «project.doc_zip». Please feel free to contact us with any questions. Respectfully, CID Management «cc»
Utilization Review strictly analyzes the medical necessity of treatment requests.

Review #«Id»
«project.doc_address» «project.doc_city», «project.doc_state» «project.doc_zip» «project.doc_phone» (p) «project.doc_fax» (fax)
CID Management does not affirm the acceptance of this workers compensation claim.

Review #«Id»
«project.doc_address» «project.doc_city», «project.doc_state» «project.doc_zip» «project.doc_phone» (p) «project.doc_fax» (fax)
«CurrentDate»
«FullName» «address.street1» «address.street2» «address.city» «address.state» «address.postalcode»
Recommendation: CERTIFY RE: Patient: «claim.patient.FullName»
Claim: «claim.claimnumber» Date request received by «organization.client_name»: «receivedbyclienttimestamp_string» Date request received by CID: «DateReceivedByUR_string» Date additional information received, if applicable: Decision date: «decisionrendereddate_string»
Dear «FullName», We have been requested by «organization.client_name», to perform utilization review to determine if the requested health care services are medically necessary and appropriate. This letter is to notify you that the following health care services are certified as medically necessary: Specific Treatment Plan Requested «requestedtreatmentplan_without_dates» UR Determination «authorizedtreatmentplan» Clinical Rationale «clinical_rationale» Criteria/Guidelines Applied «guidelines» Please feel free to contact us should you have any additional questions regarding this claim or if medical necessity substantiates further treatment. Respectfully, «signoff_user.FullQualifiedPathOfSignatur» «signoff_user.FullName» «signoff_user.StateLicensesDisplayString»

«signoff_user.BoardCertificationDisplaySt» «cc»
Utilization Review strictly analyzes the medical necessity of treatment requests. CID Management does not affirm the acceptance of this workers compensation claim.
Review #«Id»
«project.doc_address» «project.doc_city», «project.doc_state» «project.doc_zip» «project.doc_phone» (p) «project.doc_fax» (fax)
«CurrentDate»
«FullName» «address.street1» «address.street2» «address.city» «address.state» «address.postalcode» RE: Patient: «claim.patient.FullName»
Claim: «claim.claimnumber» Date request received by «organization.client_name»: «receivedbyclienttimestamp_string» Date request received by CID: «DateReceivedByUR_string» Date additional information received, if applicable: Decision date: «decisionrendereddate_string»
Dear «FullName», We have been requested by «organization.client_name», to perform utilization review to determine if the requested health care services are medically necessary and appropriate for this claim. This letter is to notify you of our determination regarding medical necessity: Specific Treatment Plan Requested «requestedtreatmentplan» UR Determination «authorizedtreatmentplan» Clinical Rationale «clinical_rationale» Criteria/Guidelines Applied «guidelines» Information regarding our optional internal appeals and reconsiderations processes is attached to this determination letter. If the requesting physician would like to discuss this determination with the reviewer, the requesting physician may contact CID at «project.doc_phone» so that a convenient time may be arranged for this discussion. All reviewers are available for at least four hours per week during normal business days from 9:00 a.m. to 5:30 p.m. PST. Please feel free to contact us should you have any additional questions regarding this claim.

Respectfully, «signoff_user.FullQualifiedPathOfSignatur» «signoff_user.FullName» «signoff_user.StateLicensesDisplayString» «signoff_user.BoardCertificationDisplaySt» «cc»
Utilization Review strictly analyzes the medical necessity of treatment requests. CID Management does not affirm the acceptance of this workers compensation claim.

CID Reconsiderations Process For any treatment request which was conditionally denied, the treatment request will be reconsidered upon receipt of the requested information.
CID Optional Internal UR Appeals Process
If the provider has not previously submitted an appeal for any treatment request which was modified or denied in this review, the patient or requesting provider has the option of submitting a request for appeal on a voluntary basis. . Participation in this optional appeals process neither triggers nor bars the use of the dispute resolution procedures of Labor Code 4610.5 and 4610.6. The request for the optional internal appeal must:
1. Be in writing; and 2. Be received by CID within 10 days of the date of the original determination; and 3. Indicate if the appeal warrants an expedited review*; and 4. Contain either:
a. Additional information supporting the request; or b. The basis or rationale for disagreement with the denial.
Appeal requests which do not match the above requirements will not be considered. Appeals and/or Reconsiderations may be faxed to «project.doc_fax» or may be submitted via mail to «project.doc_address», «project.doc_city», «project.doc_state» «project.doc_zip». * Expedited appeals shall only be granted if:
1. the timeline for making a determination could seriously jeopardize the life or health of the patient or the ability of the patient to regain maximum function; or
2. the patient would be in severe pain that could not be adequately managed without the care or treatment under review.
Additional Language required by California Labor Code and Regulations:
You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me «claim.examiner.FullName» at «claim.examiner.telephone». However, if you are represented by an attorney, please contact your attorney instead of me. For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-‐free 1-‐800-‐736-‐7401. The injured worker may file an Application for Adjudication of Claim and a Declaration of Readiness to Proceed (expedited trial) and request for an expedited hearing. If you disagree with the utilization review decision and wish to dispute it, the injured worker, the injured worker's representative, or the injured worker's attorney must communicate this dispute on the enclosed Application for Independent Medical Review, DWC Form IMR-‐1, within 30 calendar days of receipt of the decision. Disputes will be resolved in accordance with the independent medical review provisions of Labor Code section 4610.5 and 4610.6.

Medical Records Reviewed The following is a list of documents reviewed: «DocumentsReviewed»

State of California Department of Industrial Relations Division of Workers’ Compensation
Application for Independent Medical Review (All fields must be completed by the Claims Administrator)
«claim.claimnumber» «claim.dateofinjury» «decisionrendereddate_string» «claim.wcabnumber» Type of Review (Required)
Claims Number Date of Injury Date of UR WCIS Claim
Number
EAMS No (if applicable)
X Regular
(Required) (Required) Decision (Required) (Required) Expedited Injured worker Information (completion of this section is required) «project.doc_state» «project.doc_state» Injured Worker First Name
MI Injured Worker Last Name
«claim.patient.address.street1» «claim.patient.address.city» «claim.patient.address.state» «claim.patient.address.zip» Injured Worker Street Address/PO Box Injured Worker City State Zip Code Medical provider information (Completion of this section is required) «project.doc_state» «project.doc_state» Provider First Name Provider Last Name Employer and Claims Administrator Information (Completion of this section is required) «claim.Employer» Employer Name (Please leave blank spaces between number, names or words) «project.doc_state» Claims Administrator Company Name (Please leave blank spaces between numbers, names or words) «claim.examiner.FullName» Claims Examiner Name «claim.examiner.address.street1» Claims Administrator Street Address/PO Box (Please leave blank spaces between numbers, names or words) «claim.examiner.address.city» «claim.examiner.address.state» «claim.examiner.address.zip» Claims Administrator City
State Zip Code
«primary_icd9_code.description» Please reference the URO determination previously provided. Primary Diagnosis (Use ICD Code where practical)
Indicate the treatment requested, attach additional pages if necessary
Is the claims administrator disputing liability for the requested medical treatment besides the question of medical necessity? Yes X No If yes, indicate why liability is being disputed ___________________________________________________________________________________ Consent to obtain medical records I am asking for an independent medical review (IMR) to make a decision about the requested medical treatment that was delayed, denied, or modified by my claims administrator. I allow my health care providers and claims administrator to furnish medical records and information relevant for review of the disputed treatment to the independent review organization designated by the Administrative Director of the Division of Workers' Compensation. These records may include medical, diagnostic imaging reports, and other records related to my case. These records may also include non-medical records and any other information related to my case. I allow the independent review organization designated by the Administrative Director of the Division of Workers' Compensation to review these records and information sent by my claims administrators and treating physicians. My permission will end one year from the date below, except as allowed by law. I can end my permission sooner if I wish. Date: _______________________ ___________________________________________ MM/DD/YYYY Employee’s Signature File this Application by mail by sending the form to: DWC-IMR, c/o MAXIMUM Federal Services, Inc 625 Collidge Drive, Suite 100, Folsom, CA 95630 You may also file this form by faxing the document to: Fax (916) 364-8134 DWC form IMR (1/1/2013)

IMR Application Instructions
Instructions for the Employee If your claims administrator denies, delays, or modifies your treating physician's request for medical services or treatment, you can request an Independent Medical Review (IMR) by a physician who is not connected to your claims administrator. The specialty of the reviewing physician will be matched to the specialty of your treating physician or the specialty most knowledgeable about the disputed medical services or treatment. The request must be made on this form. If the IMR is decided in your favor, your claims administrator must give you the service or treatment your physician requested. You pay no costs for an IMR. Please be aware that if you decide not to participate in the IMR process, you may be giving up your rights to pursue legal action against your claims administrator regarding the service or treatment you are requesting.
How to Apply
All of the information on the form, except for your signature, should already be filled in by your claims administrator when you receive the form. Review the form to make sure that all the information provided by your claims administrator is correct. If you believe that any of the information on the form is incorrect, please submit a separate sheet that provides the correct information. Review the consent to obtain medical records, then sign and date the form where indicated at the bottom. If you are seeking an expedited review, the form must be submitted with the physician's certification that you are facing an imminent and serious threat to your health. If you have designated a parent, guardian, conservator, relative, or other designee to act on your behalf in filing this application, they may sign for you. An application for IMR must be filed within thirty (30) days from the day you receive the utilization review decision letter informing you that the medical services or treatment requested by your treating physician was denied, delayed, or modified.
Employee Right to Provide Information
You have the right to submit, either directly or through your treating physician, information and documentation to support the requested medical treatment. Such information and documentation may include:
Your treating physician's recommendation that the requested medical treatment is medically necessary for your medical condition.
Medical information or justification that the requested medical treatment, on an urgent care or emergency basis, was medically necessary for your medical condition Reasonable information supporting the position that the disputed medical treatment is or was medically necessary including all information provided by the employee's treating physician or any additional material that the employee believes is relevant. Evidence that the medical guidelines relied upon to deny or modify your physician's requested medical treatment is inapplicable or scientifically incorrect.
Determining Your Eligibility for IMR
The Application will be initially screened to determine if it is eligible for IMR. If the Application is found eligible, you will be sent written notification of the contact information of the Independent Medical Review Organization (IMRO). You must then send, as instructed, the relevant medical records as defined by California Code of Regulations, title 8, section 9792.10.5 to the IMRO. Please review California Code of Regulations, title 8, sections 9792.10.1, et seq. for additional requirements regarding the IMR process. Note that claims administrators are responsible for the costs of IMR. If the IMRO requests medical records from your treating physician, it is important that your treating physician provides the records promptly. The IMRO designated by the Division of Workers' Compensation will review your application and send you a letter telling you that you qualify for an IMR. The letter will include instructions as to how to submit your information and records. If your application for a regular, non-expedited review is determined to be eligible for IMR, the IMRO is required to reach a decision on your application within thirty (30) days from the date they receive all necessary documents and information.
Do Not File this page with your request for IMR
DWC form IMR (1/1/2013)
Review #«Id»
«project.doc_address» «project.doc_city», «project.doc_state» «project.doc_zip» «project.doc_phone» (p) «project.doc_fax» (fax)
«CurrentDate»
«FullName» «address.street1» «address.street2» «address.city» «address.state» «address.postalcode»
Recommendation: NON-‐CERTIFY
RE: Patient: «claim.patient.FullName» Claim: «claim.claimnumber» Date request received by «organization.client_name»: «receivedbyclienttimestamp_string» Date request received by CID: «DateReceivedByUR_string» Date additional information received, if applicable: Decision date: «decisionrendereddate_string»
Dear «FullName», We have been requested by «organization.client_name», to perform utilization review to determine if the requested health care services are medically necessary and appropriate for this claim. This letter is to notify you that the following health care serviced did not meet the established criteria for medical necessity: Specific Treatment Plan Requested «requestedtreatmentplan» UR Determination «authorizedtreatmentplan» Clinical Rationale «clinical_rationale» Criteria/Guidelines Applied «guidelines» Information regarding our optional internal appeals process is attached to this determination letter. If the requesting physician would like to discuss this determination with the reviewer, the requesting physician may contact CID at «project.doc_phone» so that a convenient time may be arranged for this discussion. . All reviewers are available for at least four hours per week during normal business days from 9:00 a.m. to 5:30 p.m. PST. Additionally, please feel free to contact us should you have any additional questions regarding this claim.

Respectfully, «signoff_user.FullQualifiedPathOfSignatur» «signoff_user.FullName» «signoff_user.StateLicensesDisplayString» «signoff_user.BoardCertificationDisplaySt» «cc»
Utilization Review strictly analyzes the medical necessity of treatment requests. CID Management does not affirm the acceptance of this workers compensation claim.

CID Optional Internal UR Appeals Process
For any treatment request which was modified or denied, the patient or requesting provider has the option of submitting a request for appeal on a voluntary basis. Participation in this optional appeals process neither triggers nor bars the use of the dispute resolution procedures of Labor Code 4610.5 and 4610.6. The request for the optional internal appeal must:
1. Be in writing; and 2. Be received by CID within 10 days of the date of the original determination; and 3. Indicate if the appeal warrants an expedited review*; and 4. Contain either:
a. Additional information supporting the request; or b. The basis or rationale for disagreement with the denial.
Appeal requests which do not match the above requirements will not be considered. Appeals and information may be faxed to «project.doc_fax» or may be submitted via mail to «project.doc_address», «project.doc_city», «project.doc_state» «project.doc_zip». * Expedited appeals shall only be granted if:
1. the timeline for making a determination could seriously jeopardize the life or health of the patient or the ability of the patient to regain maximum function; or
2. the patient would be in severe pain that could not be adequately managed without the care or treatment under review.
Additional Language required by California Labor Code and Regulations: You have a right to disagree with decisions affecting your claim. If you have questions about the information in this notice, please call me «claim.examiner.FullName» at «claim.examiner.telephone». However, if you are represented by an attorney, please contact your attorney instead of me. For information about the workers’ compensation claims process and your rights and obligations, go to www.dwc.ca.gov or contact an information and assistance (I&A) officer of the state Division of Workers’ Compensation. For recorded information and a list of offices, call toll-‐free 1-‐800-‐736-‐7401. The injured worker may file an Application for Adjudication of Claim and a Declaration of Readiness to Proceed (expedited trial) and request for an expedited hearing. If you disagree with the utilization review decision and wish to dispute it, the injured worker, the injured worker's representative, or the injured worker's attorney must communicate this dispute on the enclosed Application for Independent Medical Review, DWC Form IMR-‐1, within 30 calendar days of receipt of the decision. Disputes will be resolved in accordance with the independent medical review provisions of Labor Code section 4610.5 and 4610.6.

Medical Records Reviewed
The following is a list of «DocumentsReviewed»
State of California Department of Industrial Relations Division of Workers’ Compensation
Application for Independent Medical Review (All fields must be completed by the Claims Administrator)
«claim.claimnumber» «claim.dateofinjury» «decisionrendereddate_string» «claim.wcabnumber» Type of Review (Required)
Claims Number Date of Injury Date of UR WCIS Claim
Number
EAMS No (if applicable)
X Regular
(Required) (Required) Decision (Required) (Required) Expedited Injured worker Information (completion of this section is required) «project.doc_state» «project.doc_state» Injured Worker First Name
MI Injured Worker Last Name
«claim.patient.address.street1» «claim.patient.address.city» «claim.patient.address.state» «claim.patient.address.zip» Injured Worker Street Address/PO Box Injured Worker City State Zip Code Medical provider information (Completion of this section is required) «project.doc_state» «project.doc_state» Provider First Name Provider Last Name Employer and Claims Administrator Information (Completion of this section is required) «claim.Employer» Employer Name (Please leave blank spaces between number, names or words) «project.doc_state» Claims Administrator Company Name (Please leave blank spaces between numbers, names or words) «claim.examiner.FullName» Claims Examiner Name «claim.examiner.address.street1» Claims Administrator Street Address/PO Box (Please leave blank spaces between numbers, names or words) «claim.examiner.address.city» «claim.examiner.address.state» «claim.examiner.address.zip» Claims Administrator City
State Zip Code
«primary_icd9_code.description» Please reference the URO determination previously provided. Primary Diagnosis (Use ICD Code where practical)
Indicate the treatment requested, attach additional pages if necessary
Is the claims administrator disputing liability for the requested medical treatment besides the question of medical necessity? Yes X No If yes, indicate why liability is being disputed ___________________________________________________________________________________ Consent to obtain medical records I am asking for an independent medical review (IMR) to make a decision about the requested medical treatment that was delayed, denied, or modified by my claims administrator. I allow my health care providers and claims administrator to furnish medical records and information relevant for review of the disputed treatment to the independent review organization designated by the Administrative Director of the Division of Workers' Compensation. These records may include medical, diagnostic imaging reports, and other records related to my case. These records may also include non-medical records and any other information related to my case. I allow the independent review organization designated by the Administrative Director of the Division of Workers' Compensation to review these records and information sent by my claims administrators and treating physicians. My permission will end one year from the date below, except as allowed by law. I can end my permission sooner if I wish. Date: _______________________ ___________________________________________ MM/DD/YYYY Employee’s Signature File this Application by mail by sending the form to: DWC-IMR, c/o MAXIMUM Federal Services, Inc 625 Collidge Drive, Suite 100, Folsom, CA 95630 You may also file this form by faxing the document to: Fax (916) 364-8134 DWC form IMR (1/1/2013)

IMR Application Instructions
Instructions for the Employee If your claims administrator denies, delays, or modifies your treating physician's request for medical services or treatment, you can request an Independent Medical Review (IMR) by a physician who is not connected to your claims administrator. The specialty of the reviewing physician will be matched to the specialty of your treating physician or the specialty most knowledgeable about the disputed medical services or treatment. The request must be made on this form. If the IMR is decided in your favor, your claims administrator must give you the service or treatment your physician requested. You pay no costs for an IMR. Please be aware that if you decide not to participate in the IMR process, you may be giving up your rights to pursue legal action against your claims administrator regarding the service or treatment you are requesting.
How to Apply
All of the information on the form, except for your signature, should already be filled in by your claims administrator when you receive the form. Review the form to make sure that all the information provided by your claims administrator is correct. If you believe that any of the information on the form is incorrect, please submit a separate sheet that provides the correct information. Review the consent to obtain medical records, then sign and date the form where indicated at the bottom. If you are seeking an expedited review, the form must be submitted with the physician's certification that you are facing an imminent and serious threat to your health. If you have designated a parent, guardian, conservator, relative, or other designee to act on your behalf in filing this application, they may sign for you. An application for IMR must be filed within thirty (30) days from the day you receive the utilization review decision letter informing you that the medical services or treatment requested by your treating physician was denied, delayed, or modified.
Employee Right to Provide Information
You have the right to submit, either directly or through your treating physician, information and documentation to support the requested medical treatment. Such information and documentation may include:
Your treating physician's recommendation that the requested medical treatment is medically necessary for your medical condition.
Medical information or justification that the requested medical treatment, on an urgent care or emergency basis, was medically necessary for your medical condition Reasonable information supporting the position that the disputed medical treatment is or was medically necessary including all information provided by the employee's treating physician or any additional material that the employee believes is relevant. Evidence that the medical guidelines relied upon to deny or modify your physician's requested medical treatment is inapplicable or scientifically incorrect.
Determining Your Eligibility for IMR
The Application will be initially screened to determine if it is eligible for IMR. If the Application is found eligible, you will be sent written notification of the contact information of the Independent Medical Review Organization (IMRO). You must then send, as instructed, the relevant medical records as defined by California Code of Regulations, title 8, section 9792.10.5 to the IMRO. Please review California Code of Regulations, title 8, sections 9792.10.1, et seq. for additional requirements regarding the IMR process. Note that claims administrators are responsible for the costs of IMR. If the IMRO requests medical records from your treating physician, it is important that your treating physician provides the records promptly. The IMRO designated by the Division of Workers' Compensation will review your application and send you a letter telling you that you qualify for an IMR. The letter will include instructions as to how to submit your information and records. If your application for a regular, non-expedited review is determined to be eligible for IMR, the IMRO is required to reach a decision on your application within thirty (30) days from the date they receive all necessary documents and information.
Do Not File this page with your request for IMR
DWC form IMR (1/1/2013)

















![130225 - Apresentação 4Q12 - eng - SD [Somente leitura]](https://img.pdfslide.us/doc/110x75/6200ae2dbee82b194554a037/130225-apresentao-4q12-eng-sd-somente-leitura.jpg)