Embed Size (px)
Citation preview

2013
http://informahealthcare.com/bijISSN: 0269-9052 (print), 1362-301X (electronic)
Brain Inj, Early Online: 1–10! 2013 Informa UK Ltd. DOI: 10.3109/02699052.2013.775484
Let the games begin: A preliminary study using Attention ProcessTraining-3 and Lumosity� brain games to remediate attention deficitsfollowing traumatic brain injury
Samantha Zickefoose1, Karen Hux1, Jessica Brown1, & Katrina Wulf2
1Barkley Memorial Center, University of Nebraska–Lincoln, Lincoln, NE, USA, and 2Quality Living, Omaha, NE, USA
Abstract
Primary objective: Computer-based treatments for attention problems have become increas-ingly popular and available. The researchers sought to determine whether improvedperformance by survivors of severe traumatic brain injury (TBI) on two computer-basedtreatments generalized to improvements on comparable, untrained tasks and ecologically-plausible attention tasks comprising a standardized assessment.Research design: The researchers used an -A-B-A-C-A treatment design repeated across fouradult survivors of severe TBI.Methods and procedures: Participants engaged in 8 weeks of intervention using both AttentionProcess Training-3 (APT-3) and Lumosity� (2010) Brain Games. Two participants received APT-3treatment first, while the other two received Lumosity� treatment first. All participants receivedboth treatments throughout the course of two, 1-month intervention phases.Main outcomes and results: Individual growth curve analyses showed participants madesignificant improvements in progressing through both interventions. However, limitedgeneralization occurred: one participant demonstrated significantly improved performanceon one of five probe measures and one other participant showed improved performance onsome sub-tests of the Test of Everyday Attention; no other significant generalization resultsemerged. These findings call into question the assumption that intervention using either APT-3or Lumosity� will prompt generalization beyond the actual tasks performed during treatment.
Keywords
Acquired brain injury remediation, APT,APT-3, attention deficits, attention deficitsfollowing traumatic brain injury, AttentionProcess Training, attention treatment,brain games, computer-based brain injurytreatment, Lumosity
History
Received 22 March 2012Revised 28 November 2012Accepted 6 February 2013Published online 5 April 2013
Introduction
Computer-based interventions provide an alternative to trad-
itional therapy approaches for remediating some of the
persistent cognitive challenges experienced by people with
traumatic brain injuries (TBIs) [1]. Such interventions have
several potential advantages such as increasing service
availability to survivors in remote areas, supplementing
traditional therapy with access to unlimited independent
practice and reducing costs by decreasing the amount of time
professionals must devote to service provision [2]. However,
despite these potential advantages—as well as the popularity
and increasing availability of such programmes—their effi-
cacy remains largely unexplored [3], especially with regard to
interventions that are hierarchical in nature and present
increasingly complex challenges as a person demonstrates
mastery of more basic skills [4].
One hierarchically-based programme targeting various
aspects of attention and designed specifically for survivors
of brain injury is Attention Process Training-3 (APT-3) [5].
The APT-3 is a computer-based version of the earlier APT-1
[6] and APT-2 [7] programmes developed by the same
authors. It incorporates specific principles assumed to be
important for attention remediation including: (a) hierarchical
organization to stimulate basic attention skills while increas-
ing the complexity of attention targets, (b) intensive repetition
of exercises and targets to facilitate the establishment of
neural connections and (c) graphic representation of progress
[8]. Because several research groups (e.g. [9–11]) have
documented through pre-/post-intervention comparisons of
participant scores on standardized attention measures that the
APT-1 is effective in improving the attention skills of
survivors of TBI, a logical assumption is that the APT-3
will be comparable in its effectiveness. Questions persist,
however, regarding the functionality of these improvements
given that positive changes following APT-1 intervention
appear primarily at the impairment level of the World Health
Organization’s Model of Disability [12] rather than the
activity and participation levels—that is, the levels most
reflective of skill generalization [13].
Computer-based alternatives to APT-3 are activities avail-
able via the Internet designed to help people maintain or
improve a variety of cognitive functions. Some of these
offerings claim to slow cognitive decline associated with
Correspondence: Karen Hux, PhD, 351 Barkley Memorial Center,University of Nebraska–Lincoln, Lincoln, NE 68583-0738, USA. Tel:402-472-8249. Fax: 402-472-7697. E-mail: [email protected]
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.

normal ageing or the beginning stage of Alzheimer’s disease
or other forms of dementia [14–17]; others purport to improve
memory, attention and/or processing skills in individuals who
have brain damage from acquired or traumatic insults or who
demonstrate impaired functioning related to learning dis-
abilities or attention deficit disorders [18]; still others claim to
help individuals without histories of neurological or cognitive
impairments hone specific skills [19]. Although companies
touting such programmes state that scientific theory and
research support their claims, uncertainty exists about
whether engaging in brain games actually enhances cognitive
functioning [3, 15, 20].
One Web-based program—Lumosity: Reclaim Your
Brain� [21]—purports to help people both with and without
neurological impairments bolster their cognitive performance
by regular engagement in various games and mental exercises.
Initial investigations of the efficacy of using Lumosity� Brain
Games to remediate cognitive challenges secondary to TBI
have been positive. For example, Kesler et al. [22] adminis-
tered Lumosity� Brain Games to children with cancer-related
brain injury and reported significant improvements in
participants’ processing speeds, mental flexibility, memory
and pre-frontal cortex activation following intervention.
Despite these positive findings, researchers and TBI profes-
sionals know little about the generalization of improved
functions to untrained activities or situations occurring
outside of structured therapy sessions.
Programmes such as APT-3 and Lumosity� Brain Games
offer new avenues for structuring attention intervention for
survivors of TBI. The purpose of the research reported herein
was to investigate whether improved performance by adult
survivors of severe TBI on APT-3 and/or Lumosity� activities
generalized to improved performance on comparable,
untrained but similarly-structured attention tasks as well as
to ecologically-plausible attention tasks included as part of a
standardized assessment tool.
Method
Participants
Four adult males with severe TBI served as study participants.
The participants ranged in age from 36–50 years. All had
sustained severe TBIs as indicated by a period of coma
exceeding 1 day or a period of post-traumatic amnesia
exceeding 1 week [23, 24], were a minimum of 3 years post-
injury, spoke English as a primary language, had normal or
corrected-to-normal hearing and vision and did not have any
history of learning disabilities or neurological damage other
than that associated with TBI. None of the participants had
aphasia based on attainment of an Aphasia Quotient score of
93.8 or greater on the Western Aphasia Battery–Revised
(WAB-R) [25]. Participants passed a motor screening and a
mathematical computation screening to ensure adequate skills
to perform the experimental tasks. Demographic, injury-
related and screening test information about each participant
appears in Table I.
Design
The study used a single-subject A-B-A-C-A (i.e. pre-testing,
intervention phase 1, post-testing 1, intervention phase 2,
post-testing 2) treatment design repeated across participants.
Two participants received APT-3 treatment during interven-
tion phase 1, while the other two participants received
Lumosity� treatment; all participants engaged in the alternate
treatment programme during intervention phase 2. Thus, each
participant received both treatments throughout the course of
the two, 1-month intervention phases.
Materials
Formal and informal measures of attention
The researchers used the Test of Everyday Attention (TEA)
[26] and a researcher-generated, repeatable probe to measure
each participant’s attention performance. The TEA is a
standardized measure that targets everyday attention demands
in ecologically-plausible scenarios to assess visual selective
attention/speed (i.e. map search and telephone search without
distraction sub-tests), attentional switching (i.e. visual eleva-
tor sub-test), sustained attention (i.e. lottery and telephone
search while counting sub-tests) and auditory-verbal working
memory (i.e. elevator counting with reversal and elevator
counting with distraction sub-tests). It was administered at
pre-testing, post-testing 1 and post-testing 2. The researcher-
generated probe measures were adapted from the
Neurological Assessment Battery (NAB) Numbers and
Letters Test Parts B, C and D [27]. They were administered
at the same times as the TEA as well as on a weekly basis
during intervention phases 1 and 2. The researchers designed
the probe tasks to emulate the attention targets of the APT-3
and Lumosity� programmes (e.g. sustained attention, select-
ive attention, divided attention). The probes included four
sub-tests: (a) marking the X’s in eight rows of numbers and
letters as quickly as possible; (b) counting the number of X’s
in eight rows of numbers and letters as quickly as possible and
writing down the sum for each line; (c) adding the sum of
numbers in eight rows of letters and numbers from left to
right and writing down the sum of each line; and (d) marking
each X in eight rows of numbers and letters while simultan-
eously adding and then writing down the sum of the numbers
in the row. The researchers developed 10 versions of
comparable mathematical equations and letter combinations
Table I. Participants’ background and aphasia quotient information.
Participant Age (years) Time post-injury (years) Cause of injury Length of coma (days) Length of PTA (months) WAB-R Aphasia quotient
OE 36 3 Penetrating blow 2 40.25 99.6NG 50 35 Fall 115 43.50 98.0KX 36 9 Car accident 84 42.80 97.6KS 49 23 Car accident unknown 41.00 99.6
2 S. Zickefoose et al. Brain Inj, Early Online: 1–10
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.

as those listed in the NAB to prevent specific-task learning.
They measured participant performance based on the accur-
acy of responses.
Perceptual rating scales
The researchers designed a measure to allow participants to
inform them about their perceptions regarding the two
intervention programmes used over the course of treatment.
Specifically, the researchers asked participants the following
two questions at the end of each intervention phase: (a) ‘How
much are you enjoying these activities?’ and (b) ‘Would you
complete these activities on your own?’ Participants
responded by pointing to a number between 1–5 presented
on a Likert-type scale, with higher numbers corresponding
with more positive responses than lower numbers.
Intervention materials
Each individual participated in two intervention programmes
over the course of the research project: the APT-3 and the
Lumosity� Brain Games. The researchers acquired a proto-
type version of the APT-3 from one of the programme authors
for use in this research project (Sohlberg, personal commu-
nication, 17 May 2010). To access Lumosity�, the researchers
purchased a subscription.
The APT-3 programme defines five domains of attention:
(a) sustained attention, (b) selective attention, (c) working
attention, (d) suppression and (e) alternating attention. The
researchers grouped each variation of APT-3 tasks within each
attention domain into a hierarchy of complexity based on the
skills required to complete the tasks, the level of distraction
and the rate of presentation. They used this hierarchy to
determine the sequence of tasks to present to participants as
they progressed through the intervention programme. The
sustained attention domain included a total of 20 levels; the
selective attention domain included 114 levels; the working
memory domain included 13 levels; and the suppression and
alternating attention domain included 16 levels.
Lumosity� is available via an Internet website (i.e. http://
www.lumosity.com) that provides access to brain games
designed to improve cognitive processing speed, flexibility,
attention, memory and problem-solving skills. Game com-
plexity increases and decreases systematically based on an
individual’s performance data. Multiple forms of each game
level are available to prevent task learning with continued
practice.
The researchers selected five attention-oriented
Lumosity� games—Birdwatching, Monster Garden, Playing
Koi, Rotation Matrix and Top Chimp—for use in this research.
Each selected game followed three principles in that they
provided: (a) repeated opportunities for diverse practice, (b)
hierarchical organization of experimental stimuli with grad-
able levels of difficulty and (c) human–computer interactions
through multi-media.
Procedures
The researchers alternately assigned participants to begin
either with the APT-3 or Lumosity� Brain Games interven-
tion and then performed pre-testing to establish each
participant’s baseline level of attention functioning.
Following this, participants engaged in 20 treatment sessions
within a 1-month period, with each session lasting �30
minutes; some daily variation occurred in session length
depending on how quickly a participant performed the tasks
selected for that day. When using APT-3, the participants
performed four tasks during each session—one corresponding
with sustained attention, one with selective attention, one with
working attention and one either with suppression or
alternating attention. When using Lumosity�, the researchers
systematically alternated tasks so that a participant performed
each of the five selected games a minimum of two times per
four sessions. After completing the first month of intervention
(i.e. intervention phase 1), participants performed post-testing
1 and the perceptual rating form for the appropriate
intervention programme; they then proceeded through inter-
vention phase 2 with the alternate intervention programme,
followed by completion of post-testing 2 and the appropriate
perceptual rating form.
Four trained research assistants alternately administered
the daily intervention sessions. The researchers trained the
assistants by demonstrating the data collection procedures
both for the APT-3 and the Lumosity� programmes. In
addition, the research assistants had written step-by-step
programme instructions to guide them through the interven-
tion sessions.
Data analysis
Procedural integrity and inter-judge reliability
The researchers ensured procedural integrity by performing
the following procedures with each research assistant involved
in data collection: (a) providing one-on-one training to
familiarize the assistant with each intervention programme
and explain the set-up and data collection procedures, (b)
demonstrating the set-up and data collection procedures for
both intervention programmes, (c) observing the assistant
performing all set-up and data collection procedures and (d)
providing a written checklist of steps to be performed prior to,
during and following each intervention session.
All scoring of response accuracy for the Lumosity�intervention sessions was handled through the Web-based
program; hence, research assistants only were responsible for
copying scores displayed on the computer monitor. In
contrast, inter-judge reliability was an issue when participants
performed the APT-3 intervention, because the prototype
APT-3 programme did not accurately score participants’
responses within activities. To determine inter-judge reliabil-
ity, the primary researcher and a research assistant independ-
ently collected data during an APT-3 intervention session with
one of the four study participants. Point-to-point reliability for
each APT-3 activity was computed using the following
formula:
number of agreements
number of agreementsþ disagreements� 100:
Inter-judge reliability ranged from 80–100% across the
four administered activities, with the overall reliability
equalling 93%.
DOI: 10.3109/02699052.2013.775484 Remediating attention deficits 3
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.

Dependent variables
The researchers monitored participants’ session-to-session
performance on each APT-3 and Lumosity� task. Graphic
displays and individual growth curve modelling procedures
provided a means of visualizing and quantifying an individ-
ual’s progression through the two intervention phases of the
research. The researchers also monitored participants’ per-
ceived enjoyment of the intervention activities and the
likelihood that they would continue performing similar
activities independently if the option were available to
them. This monitoring was done through responses to
Likert-type questions.
Participants’ scores on probe measures and scaled scores or
adjusted scaled scores, as appropriate, on the pre-testing,
post-testing 1 and post-testing 2 administrations of the TEA
were dependent variables used for analysis of generalization
effects. Graphic displays, computation of trend lines and
comparison of trend line slopes with a slope of 0 provided a
means of judging generalization of improved attention
performance based on the probe measures. The researchers
used graphic displays of TEA scaled score changes to further
evaluate generalization of improved attending behaviour.
Results
The research results appear in three sections. The first section
presents data about each participant’s progression through the
APT-3 and Lumosity� programmes. Included with this are
data about the participants’ perceptions of their enjoyment
and willingness to continue performing the activities beyond
the conclusion of the research project. The second section
includes data about participants’ performances on the probe
measures administered throughout the course of the interven-
tion programmes. Section three includes the pre-testing, post-
testing 1 and post-testing 2 data from the standardized
measure of attention functioning—that is, the TEA.
Progression through intervention programmes
APT-3
Participants progressed at their own speed through multiple
levels of the APT-3 hierarchy of activities within the sustained
attention, selective attention, working attention and suppres-
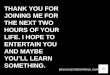
sion and alternating attention domains. Figure 1 displays each
participant’s progression within each domain. Note that
abrupt changes in hierarchy level within the selective
attention domain occurred for participants at various points
during the course of intervention; these were due to
researcher-determined readjustments needed in the difficulty
level of the presented tasks.
The researchers computed trend lines associated with each
participants’ progression through the APT-3 programme
(Table II). Statistical analysis confirmed that the slopes of
the trend lines differed significantly from a line with a slope of
0.00 for all four attention domains across all four participants,
thus suggesting that participants progressed to more challen-
ging levels throughout the course of the intervention.
Participants not desiring to continue with the programme
0
2
4
6
8
10
12
14
16
18
20
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Leve
l
Session
Sustained attention
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
2
0
4
6
8
10
12
Leve
l
Session
Working attention
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 200
2
4
6
8
10
12
14
16
Leve
l
Session
Suppression & alternating attention
OE
NG
KX
KS
OE
NG
KX
KS
0
20
40
60
80
100
Leve
l
Session
Selective attention
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Figure 1. Participants’ progressions through increasing levels of difficulty on APT-3 tasks within each attention domain.
4 S. Zickefoose et al. Brain Inj, Early Online: 1–10
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.

reported that they perceived the tasks as not being functional in
nature and lacking representation of real-life situations.
Participants responded to Likert-type questions at the end
on the APT-3 intervention phase to convey their enjoyment of
and willingness to continue performing APT-3 activities
beyond the conclusion of the research study (Table III). Likert
scores reflected strong enjoyment and interest in continuing
APT-3 by two of the four participants and equally strong
rejection of APT-3 by the other two participants.
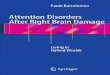
Lumosity�
Figure 2 displays each participant’s progression through the
five selected Lumosity� games. As with the APT-3 data, the
researchers computed trend lines associated with each
participants’ progression through the Lumosity� activities
(Table IV). Statistical analysis confirmed that the trend line
slopes differed significantly from a line with a slope of 0.00
for four of the five game activities across all four participants,
thus suggesting that participants progressed to more challen-
ging levels throughout the course of the intervention. For one
Lumosity� game (i.e. Rotation Matrix), only OE progressed
in a manner in which his trend line differed significantly from
a line with a slope of 0.00.
Table III contains participants’ self-reported perceptions
about their enjoyment of performing Lumosity� activities
and willingness to continue performing the games independ-
ently. All four participants indicated that they enjoyed the
Lumosity� games. However, only two of the four expressed a
strong desire to perform the games outside the realm of the
research; the other two provided neutral Likert responses to
this question. Again, the participants’ verbal comments about
continuing to perform the Lumosity� activities reflected
skepticism about the applicability of the activities to improv-
ing attention skills in real-life situations.
Probe measures
Participants performed a total of nine probes over the course
of the research project: one during pre-testing, three during
intervention phase 1, one during post-testing 1, three during
intervention phase 2 and one during post-testing 2. Each
probe included four tasks: (a) cancellation of X’s appearing in
rows, (b) counting the number of X’s appearing in rows, (c)
summing of digits appearing in rows and (d) simultaneous
cancellation of X’s and summing of digits appearing in rows.
The third and fourth probe tasks were of particular import-
ance because participants had to perform more challenging
activities than they did for the first and second tasks; in
addition, the fourth task required divided attention. Because
individual changes over time were of interest rather than
comparisons across participants, the researchers analysed data
from each participant separately.
Participant OE performed the four probe tasks at a level at
or near ceiling at the time of pre-testing. He then maintained
high accuracy throughout all subsequent probe administra-
tions, with accuracy mean scores exceeding 85% in all
instances (i.e. task 1: M¼ 97.22%, SD¼ 5.51; task 2:
M¼ 93.06%, SD¼ 9.08; task 3: M¼ 94.44%, SD¼ 9.08;
task 4 cancellation: M¼ 87.50%, SD¼ 12.50; task 4 summa-
tion: M¼ 94.44%, SD¼ 9.08). Because of his consistency and
high initial accuracy, comparison of trend line slopes
associated with accuracy improvements on probe tasks
across administrations to a line with a slope of 0.00 yielded
no significant results. Still, the slope of his accuracy score
trend line for the summation portion of probe task 4
approached significance when compared with a line with a
slope of 0.00 (t¼ 2.198; p¼ 0.0639), thus suggesting a trend
towards improvement in this aspect of the divided attention
probe task despite the small margin available for improve-
ment. OE’s improved probe task accuracy occurred primarily
Table II. Participants’ trend line, t-value and p-value data for attention domains targeted in APT-3.
Sustained attention Selective attention Working attentionSuppression &
alternating attention
OETrend line y¼ 0.76xþ 3.04 y¼ 4.83x� 2.53 y¼ 0.07xþ 4.36 y¼ 0.06xþ 3.04t-value t¼ 10.778 t¼ 13.042 t¼ 2.931 t¼ 3.571p-value p50.0001 p50.0001 p50.0089 p¼ 0.0022
NGTrend line y¼ 0.88xþ 2.53 y¼ 7.29x� 6.21 y¼ 0.09xþ 3.56 y¼ 0.09xþ 2.29t-value t¼ 18.010 t¼ 8.295 t¼ 7.758 t¼ 2.995p-value p50.0001 p50.0001 p50.0001 p¼ 0.0078
KXTrend line y¼ 0.85xþ 4.79 y¼ 4.94xþ 16.14 y¼ 0.14xþ 4.09 y¼ 0.09xþ 2.67t-value t¼ 15.031 t¼ 17.689 t¼ 5.327 t¼ 3.915p-value p50.0001 p5.0001 p50.0001 p¼ 0.0010
KSTrend line y¼ 0.76xþ 3.04 y¼ 4.83x� 2.53 y¼ 0.07xþ 4.36 y¼ 0.06xþ 3.04t-value t¼ 10.778 t¼ 13.042 t¼ 2.931 t¼ 3.571p-value p50.0001 p50.0001 p50.0089 p¼ 0.0022
Table III. Likert scale ratings of participants’ enjoyment of andwillingness to continue performing APT-3 and Lumosity� tasksindependently.
APT-3 Lumosity�
Participant EnjoymentWillingnessto continue Enjoyment
Willingnessto continue
OE 5 4 5 5NG 1 1 4 3KX 5 5 4 3KS 1 1 5 5
DOI: 10.3109/02699052.2013.775484 Remediating attention deficits 5
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.

during the first intervention phase when he was using the
APT-3 programme.
Participant NG demonstrated considerably greater accur-
acy variability than OE in performing the probe tasks across
the course of the research. Across administrations, NG
performed probe task 1 with greater accuracy (M¼ 90.28%,
SD¼ 15.02) than any of the other probe tasks (task 2:
M¼ 61.11%, SD¼ 24.56; task 3: M¼ 75.00%, SD¼ 13.98;
task 4 cancellation: M¼ 66.67%, SD¼ 17.68; task 4 summa-
tion: M¼ 75.00%; SD¼ 13.98). No progression of improved
accuracy occurred over the course of the project, as
demonstrated by the finding of no significant differences
0
1
2
3
4
5
6
7
8
9
10
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
Leve
l
Session
Birdwatching0
1
2
3
4
5
6
Leve
l
Session
Monster Garden
0
1
2
3
4
5
Leve
l
Session
Playing Koi0
1
2
3
4
5
6
7
Leve
lSession
Top Chimp
OE
NG
KX
KS
OE
NG
KX
KS
OE
NG
KX
KS
0
2
4
6
8
10
12
Level
Session
Rotation Matrix
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
Figure 2. Participants’ progressions through increasing levels of difficulty on Lumosity� Brain Game activities.
Table IV. Participants’ trend line, t-value and p-value data for Lumosity� Brain Game activities.
Birdwatching Monster Garden Playing Koi Rotation Matrix Top Chimp
OETrend line y¼ 0.30xþ 2.03 y¼ 0.09xþ 1.8 y¼ 0.15xþ 1.90 y¼ 0.02xþ 7.08 y¼ 0.35xþ 1.22t-value t¼ 13.543 t¼ 5.464 t¼ 7.288 t¼ 0.514 t¼ 12.725p-value p50.0001 p50.0001 p50.0001 p¼ 0.6147 p50.0001
NGTrend line y¼ 0.18xþ 1.14 y¼ 0.04xþ 1.59 y¼ 0.18xþ 0.76 y¼ 0.01xþ 6.19 y¼ 0.20xþ 2.40t-value t¼ 13.045 t¼ 2.611 t¼ 8.047 t¼ 0.292 t¼ 5.292p-value p50.0001 p¼ 0.0197 p50.0001 p¼ 0.7749 p¼ 0.0001
KXTrend line y¼ 0.12xþ 1.13 y¼ 0.04xþ 1.49 y¼ 0.14xþ 1.47 y¼ 0.06xþ 6.29 y¼ 0.19xþ 1.91t-value t¼ 9.335 t¼ 3.346 t¼ 7.885 t¼ 2.214 t¼ 5.456p-value p50.0001 p¼ 0.0036 p50.0001 p¼ 0.0439 p50.0001
KSTrend line y¼ 0.20xþ 0.76 y¼ 0.04xþ 1.49 y¼ 0.07xþ 2.12 y¼ 0.02xþ 6.10 y¼ 0.16xþ 2.21t-value t¼ 10.808 t¼ 3.346 t¼ 3.878 t¼ 0.449 t¼ 5.758p-value p50.0001 p¼ 0.0036 p¼ 0.0012 p¼ 0.6599 p50.0001
6 S. Zickefoose et al. Brain Inj, Early Online: 1–10
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.

between the slopes of trend lines associated with each probe
task and a line with a slope of 0.00.
Participant KX also displayed variability in his perform-
ance accuracy on the four probe tasks across the course of the
research project. In contrast to participants OE and NG, KX’s
greatest accuracy and least variability occurred when per-
forming the summation portion of task 4 (M¼ 87.50%,
SD¼ 10.83) rather than when performing the other three
probe tasks (task 1: M¼ 79.17%, SD¼ 21.65; task 2:
M¼ 83.33%, SD¼ 15.31; task 3: M¼ 68.06%, SD¼ 14.13;
task 4 cancellation: M¼ 70.83%, SD¼ 17.68). Comparison of
a line with a slope of 0.00 to the slopes of KX’s performance
accuracy trend lines on each probe task across administrations
yielded a significant difference for task 2 only (t¼ 2.393;
p¼ 0.0479). Improvement in performing task 2 occurred
primarily during the first intervention phase when KX was
using the APT-3 programme.
Participant KS’s accuracy in performing all probe tasks
ranged either from 50–100% or 62.5–100% across the
multiple administrations. His greatest variability in perform-
ance occurred on tasks 1 (M¼ 87.50%, SD¼ 15.31) and 3
(M¼ 80.56%, SD¼ 16.67). These were also the tasks for
which KS received his highest mean accuracy scores; mean
accuracy for task 2 and for the cancellation and summation
aspects of task 4 ranged from a low of 73.61% (task 4
summation) to a high of 77.78% (task 2). KS demonstrated
upward trends in his performance accuracy for tasks 1 and 4
across the course of the research project. Comparison of the
slope of his trend lines associated with these progressions
with a line with a slope of 0.00 approached but did not reach
significance for task 1 (t¼ 2.167; p¼ 0.0670) and for the
cancellation portion of task 4 (t¼ –2.200; p¼ 0.0637). The
trends toward improved performance on the probe tasks
occurred primarily during the first intervention phase when
KS was using the Lumosity� programme.
TEA scores
Participants performed the TEA on three occasions: (a) before
the start of the first intervention, (b) after completing the first
intervention and before initiating the second intervention and
(c) after completing the second intervention. Because of
repeated exposure to the test, practice effects may have
occurred. As such, the researchers used the adjusted scaled
score equivalents to obtained raw scores provided in the TEA
manual to evaluate participants’ performances on the second
and third test administrations. Adjusted scaled score equiva-
lents guard against possible practice effects and allow for
interpretation of performance data when attempting to
identify real improvement among multiple TEA administra-
tions. Computation involves comparing the change in a
person’s score between second and third testing to the mean
practice effect for a given sub-test reported in the TEA
manual. If the change is larger than the mean, improvement
has occurred; however, if the change is smaller than the mean,
deterioration has occurred. The raw scores and scaled or
adjusted scaled scores, as appropriate, for each participant
appear in Table V. The mean scaled or adjusted scaled score
equivalent on each of the TEA sub-tests is 10 with a standard
deviation of 3. As with the probe measures, individual
changes over time were of interest rather than comparisons
across participants; hence, the researchers analysed data from
each participant separately.
OE’s scaled score equivalents on the TEA sub-tests at the
time of pre-testing ranged from 0–4. This corresponded with
performance �2 SD below the mean on all sub-tests. OE’s
adjusted scaled scores improved on six of the nine sub-tests
post-APT-3 intervention and his scores either remained the
same or further improved on four sub-tests post-Lumosity�training. Overall, OE’s adjusted scaled scores improved from
his pre-testing performance on seven of the nine sub-tests over
the combined APT-3 and Lumosity� intervention periods. At
the time of the second post-testing, adjusted scaled scores for
six of the nine sub-tests remained �2 SD below the mean; two
adjusted scaled scores were between 1–2 SD below the mean;
and one adjusted scaled score was within 1 SD above the mean.
NG’s pre-testing scaled score equivalents did not exceed 6
on any of the TEA sub-tests and he received a scaled score of
0 on four of the nine sub-tests. This corresponded with per-
formance between 1–2 SD below the mean on three sub-tests,
Table V. Participants’ scaled or adjusted scaled score results on TEA sub-tests.
Participant Visual selective attention/speed Sustained attention Attentional switching Auditory-verbal working memory
OEPre-testa 4 0 1 0 1 4 4 2Post-APT-3b 5þ 0 7þ 2þ 4þ 13þ 4 2Post-Lumosity�b 6þ 0 6þ 2þ 1 13þ 4 3þ
NGPre-testa 0 0 0 2 6 4 6 5Post- Lumosity�b 5þ 0 0 0� 5� 5þ 5� 7þ
Post -APT-3b 5þ 0 0 0� 3� 7þ 4� 2�
KXPre-testa 4 4 3 6 8 11 10 8Post-APT-3b 5þ 0� 0� 3� 11þ 9� 11þ 7�
Post-Lumosity�b 3� 0� 2� 3� 3� 4� 7� 7�
KSPre-testa 3 2 2 2 5 5 6 7Post- Lumosity�b 3 0� 0� 4þ 6þ 7þ 4� 10þ
Post- APT-3b 3 0� 0� 3þ 2� 9þ 4� 8þ
ascaled score: M¼ 10 (SD¼ 3); badjusted scaled score: M¼ 10 (SD¼ 3).þ indicates increase from baseline performance; � indicates decrease from baseline performance.
DOI: 10.3109/02699052.2013.775484 Remediating attention deficits 7
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.

between 2–3 SD below the mean on two sub-tests and53 SD
below the mean on four sub-tests. After completing the
Lumosity� intervention, NG’s adjusted scaled scores
increased on three of the nine subtests, remained consistent
on three other sub-tests and decreased on the three remaining
sub-tests. After the APT-3 intervention, his adjusted scaled
scores remained consistent on one and improved further on
another of the sub-tests on which he had demonstrated earlier
improvement; his adjusted scaled score performance
decreased or remained at 0 on all remaining sub-tests.
Overall, NG’s adjusted scaled scores improved on two of the
nine sub-tests over the combined Lumosity� and APT-3
intervention periods. At the time of post-testing 2, four of the
nine adjusted scaled scores were at 0 (i.e. 53 SD below
mean), three remained at or less than 2 SD below the mean
and two were between 1–2 SD below the mean.
Four of KX’s scaled score equivalents on TEA sub-tests
corresponded with performance52 SD below the mean at the
time of pre-testing; one scaled score equivalent was between
1–2 SD below the mean; and four were between 1 SD below
and 1 SD above the mean. KX’s adjusted scaled scores
improved on three of the nine sub-tests following completion
of the APT-3 intervention, but his scores decreased on the
remaining six sub-tests. Following the Lumosity� interven-
tion, all but one of KX’s adjusted standard scores decreased or
remained the same as they were following the APT-3
intervention; all scores were lower than at pre-testing.
KS’s scaled score equivalents on TEA sub-tests ranged
from 0–7 at the time of pre-testing. This corresponded with
scores ranging from 1 to53 SD below the mean. Following
intervention with the Lumosity� programme, KS’s adjusted
scaled scores improved on four of the nine TEA sub-tests;
however, his adjusted standard scores on three other sub-tests
decreased. Following completion of the APT-3 intervention,
KS’s adjusted scaled score for one sub-test increased again,
but this gain was offset by his decreased score on another sub-
test. Overall, KS’s adjusted scaled scores improved on three
of the nine sub-tests and declined on four of the nine sub-tests
over the combined Lumosity� and APT-3 interventions. At
the time of the second post-testing, three of the nine adjusted
scaled scores were 0 (i.e. 53 SD below the mean), four
remained52 SD below the mean and two were within 1 SD
below the mean.
Results summary across participants
All four participants demonstrated statistically significant
progress in reaching new levels of difficulty on intervention
tasks over the course of the APT-3 and Lumosity� interven-
tion phases. Specifically, participant KX improved signifi-
cantly on all APT-3 and Lumosity� activities and the other
three participants improved significantly on all but the
Rotation Matrix game of Lumosity�. Likert rating scale
data regarding participants’ perceived enjoyment of the
intervention programmes indicated that all four enjoyed
engaging in the Lumosity� Brain Games, whereas only two
of the four enjoyed engaging in the APT-3 tasks. Similarly, all
four were either neutral or positive about continuing further
with the Lumosity� activities, but only two of the four felt
this way about the APT-3 activities.
Generalization of improved attention evidenced through
probe measure performance changes across participants
appeared predominantly during the first intervention period,
regardless of which intervention programme a given partici-
pant received during that phase. Specifically, early general-
ization was evident for one aspect of the probe measure for
participant KX; the performances of two other participants
(i.e. OE and KS) approached significance either for one or
two aspects of the probe task. OE’s high performance
accuracy at the time of pre-testing suggests that the probe
task may have been inadequate for measuring generalization
of improvement in his attention functioning. Generalization of
improved attention based on repeated performances of the
TEA yielded mixed findings. Participant OE appeared to
generalize his improved attending behaviour attained over the
course of both intervention programmes to several TEA sub-
tests; the TEA sub-test scores of the remaining three
participants were too inconsistent to warrant any such claim
associated with the separate or combined intervention
programmes.
Discussion
Variability across participants
Participation in computer-based intervention programmes is
an attractive alternative to traditional treatment approaches
for many individuals with TBI because of features such as low
cost, wide-spread availability, provision of immediate and
unbiased feedback and built-in entertainment [1, 2].
Application of two such programmes in the study reported
herein resulted in two of four adults with severe TBI
demonstrating improved attending behaviour as measured
either through a researcher-generated probe or through a
standardized attention assessment tool. This is encouraging
given that the individuals had severe attention deficits and
were multiple years post-injury. People with less severe initial
injuries, less persistent attention challenges and in more acute
stages of recovery may benefit more. At the same time,
cautious interpretation of findings is necessary, because the
observed gains in participants’ probe scores early in the
intervention process may have reflected practice effects rather
than actual improvement in attention functioning. In particu-
lar, probe repetition may have provided a means of improving
participants’ understanding of the task directions and/or
awareness of task requirements. Furthermore, the results are
discouraging in that participation in the programmes showed
only limited generalization for the two best-performing
participants and no apparent generalized benefits for the
other two participants. These findings call into question the
claims of some researchers and manufacturers of computer-
based cognitive intervention programmes who purport that
the products are helpful to virtually all people engaging in the
activities on a consistent basis [4, 19]. The results also
confirm the suspicions of many researchers who have noted
the ease of demonstrating improvement on specific interven-
tion tasks but the challenge of converting those gains to
everyday functioning [3, 20, 28].
Each participant in the current study demonstrated a unique
pattern of performance in progressing through the intervention
activities and performing the generalization tasks.
8 S. Zickefoose et al. Brain Inj, Early Online: 1–10
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.

Several factors reflecting the heterogeneity of the TBI
population may have contributed to the observed variability
including individual differences in the extent of neurological
damage, the length of time post-injury and the severity of
attention deficits at the initiation of treatment [8]. In particular,
the participant who appeared to benefit most from the
intervention (i.e. OE) differed from the other participants in
that he was relatively young, had sustained his injury only 3
years prior to study initiation, experienced trauma from the
penetration of a high-pressure pipe through his skull rather
than from a closed head injury and had higher pre-intervention
scores on the TEA and probe measures than the other
participants. In all likelihood, a combination of these factors
contributed to his success in improving his attention and
generalizing those improvements to other tasks. The wide
range across participants post-injury is a limitation of this
study. Additional investigations with homogeneous participant
groups regarding time post-injury are warranted to evaluate the
effects of computer-based intervention programmes during
specific stages of recovery.
Other factors contributing to the obtained results concern
the day-to-day variability of many TBI survivors and the
motivation of individual participants to perform well on the
generalization tasks. In particular, the declining scores
obtained by participant KX on repeated TEA administrations
are difficult to explain in terms other than personal incon-
sistency. No reason exists to assume that participation in the
intervention activities would result in a decline in his
attending skills and no medication, lifestyle or psychological
changes were noted during the course of the research that
would account for his deterioration. As such, frustration with
the difficulty of certain tasks, limited motivation to perform
the testing activities or extreme day-to-day variability warrant
consideration as possible factors influencing his performance.
Factors relating to aspects of the chosen intervention
programmes may also have contributed to the variability
observed across participants and the limited generalization of
improvements. In particular, the researchers determined the
hierarchy for presenting APT-3 tasks and selected the games
for inclusion in the Lumosity� intervention. These decisions
were based on clinical judgement and logical assumptions
about task difficulty and complexity; as such, they are
certainly subject to question. Inclusion of different tasks or a
different sequence of tasks might have yielded better results.
Finally, factors relating to the length and intensity of
treatment may have contributed to the lack of generalization
noted. Specifically, the 30-minute sessions, 5 days per week,
for 4 weeks with each intervention programme may not have
been optimal. Longer or more intense treatment or sessions
distributed over a longer period of time may have fostered
better generalization of improved attending behaviour to
novel activities. In particular, KS and OE’s performances
approaching but not reaching significance on the
probe measures suggest that, had they been given the
opportunity to continue longer, their gains might have
shown greater generalization. This notion is supported by
the reported improvements noted by other researchers [11,
29], who have administered APT interventions with longer
sessions and over longer time periods than was done in the
current study.
The fact that current study participants demonstrated
greater improvement on TEA sub-tests following the first
intervention phase than the second, regardless of the order of
programme presentation, calls into question the idea that
additional intervention time would be of value regarding
generalization to non-experimental tasks, however. The
benefits gained from programme participation appeared
early rather than late in the intervention process. Hence,
assuming that additional treatment time and/or intensity
would facilitate greater generalization of functional changes
in attending behaviour might be erroneous. Indeed, some
researchers (e.g. [9]) have documented no improvement in
brain injury survivors’ attention scores following an extended
period of APT intervention. Ultimately, researchers need to
investigate further the appropriate intensity and duration of
various attention intervention programmes to maximize
positive outcomes for individual survivors.
Preferences for APT-3 vs Lumosity�
Commitment to engaging in attention training activities on a
routine basis is critical to the success of any individual. As
such, having access to a programme with appealing graphics,
animations and sound tracks and that presents activities in a
format bolstering interest and enjoyment can be important. In
the current study, the presence or absence of these types of
features appeared to influence participants’ attitudes toward
the Lumosity� and APT-3 programmes and their desires
regarding continued engagement as reflected through their
Likert-scale ratings. However, the fact that study participants
were not unanimous in their preferences for one programme
over the other confirms the need to consider individual
differences regarding activity difficulty, formatting and pres-
entation options. Important considerations include determin-
ing whether an individual prefers: (a) competing with a
computerized opponent or working independently, (b) parti-
cipating in a game or a drill-and-practice format, (c) having
multiple levels beyond their current ability or being successful
in mastering the highest level available, (d) engaging in
activities of short or long duration, (e) receiving computer-
provided or clinician-provided feedback, (f) having adjust-
ments in difficulty level occur within or between activities
and (g) having considerable or minimal redundancy and
repetition within tasks. Of note, all participants complained
that the intervention activities of both programmes did not
reflect real-life tasks to a satisfactory degree. They appeared
more willing to overlook this lack of functional application—
or at least better tolerate it—when engaged in Lumosity�than APT-3. Perhaps this was because of their perception that
the former activities were mental games with entertainment
value, but the latter were therapy tasks.
Conclusions
The use of tools such as Lumosity� Brain Games and APT-3
to remediate the attention deficits of individuals with TBI is
an area of research requiring further investigation. Indeed,
exploration of the clinical value of brain fitness programmes
is in its infancy regarding the types of individuals most likely
to benefit, the optimum activities for inclusion, and the best
methods of presenting programmes and evaluating outcomes.
DOI: 10.3109/02699052.2013.775484 Remediating attention deficits 9
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.

Although the results presented herein raise questions regard-
ing the efficacy of programmes such as these, further research
is needed to determine the factors that influence whether
particular individuals will or will not benefit. Certainly,
engagement in brain training and brain fitness programmes is
unlikely to have negative ramifications regarding cognitive
outcomes and may provide enjoyable alternatives to other
leisure activities. Still, consumers and professionals should be
wary of poorly-substantiated, universal claims that such
programmes provide a means of boosting the cognitive
functioning of survivors of TBI.
Declaration of interest
The authors report no conflicts of interest. The authors alone
are responsible for the content and writing of the paper.
References
1. Sullivan K, Goudy L, Prauka M, Quinn J, French L, Teixeira K.Computer-based brain-fitness programs for traumatic brain injuryrehabilitation. Poster presented at the annual convention of theAmerican Speech-Language-Hearing Association, San Diego, CA.November 2011.
2. Pierce SM, Mayer NH, Whyte J. Computer-assisted exercisesystems in traumatic brain injury: Cases and commentary. Journalof Head Trauma Rehabilitation 2001;16:406–413.
3. Owen AM, Hampshire A, Grahn JA, Stenton R, Dajani S, BurnsAS, Howard RJ, Ballard CG. Putting brain training to the test.Nature 2010;465:775–778.
4. Gontkovsky ST, McDonald MB, Clark PG, Ruwe WD. Currentdirections in computer-assisted cognitive rehabilitation.NeuroRehabilitation 2002;17:195–199.
5. Sohlberg MM, Mateer C. Attention Process Training APT-3: Adirect attention training program for persons with acquired braininjury. Youngsville, NC: Lash & Associates Publishing/TrainingInc.; 2011.
6. Sohlberg MM, Mateer CA. Attention Process Training (APT).Puyallup, WA: Association for Neuropsychological Research andDevelopment; 1986.
7. Sohlberg MM, Johnson L, Paule L, Raskin SA, Mateer CA.Attention Process Training II: a program to address attentionaldeficits for persons with mild cognitive dysfunction [rehabilitationmaterials]. Puyallup, WA: Association for NeuropsychologicalResearch & Development; 1994.
8. Sohlberg MM, Mateer CA. Cognitive rehabilitation: an integrativeneuropsychological approach. New York: The Guilford Press; 2001.
9. Park N, Proulx GB, Towers WM. Evaluation of the attentionprocess training programme. Neuropsychological Rehabilitation1999;9:117–130.
10. Sohlberg MM, Mateer CA. Effectiveness of Attention-TrainingProgram. Journal of Clinical and Experimental Neuropsychology1987;9:117–130.
11. Sohlberg MM, McLaughlin KA, Pavese A, Heidrich A, Posner MI.Evaluation of Attention Process Training and brain injury education
in persons with acquired brain injury. Journal of Clinical andExperimental Neuropsychology 2000;22:656–676.
12. World Health Organization (WHO). International classificationof functioning, disability and health. Geneva: World HealthOrganization; 2001.
13. Boman I-L, Lindstedt M, Hemmingsson H, Bartfai A. Cognitivetraining in home environment. Brain Injury 2004;18:985–995.
14. Dakim, Inc. Dakim� Brain Fitness: clinically demonstrated toimprove memory. Santa Monica, CA: Lumos Labs, Inc.; 2010.Available online at: http://www.dakim.com/why-it-works/clinical-trials/, accessed 1 January 2012.
15. Fuyuno I. Brain craze. Nature 2007;447:18–20.16. Kawashima R, Okita K, Yamazaki R, Tajima N, Yoshida H, Taira
M, Iwata K, Sasaki T, Maeyama K, Usui N, et al. Reading aloudand arithmetic calculation improve frontal function of people withdementia. Journals of Gerontology, Series A, Biological Sciencesand Medical Sciences 2005;60:380–384.
17. Smith GE, Housen P, Yaffe K, Ruff R, Kennison RF, Mahncke HW,Zelinski EM. A cognitive training program based on principles ofbrain plasticity: Results from the Improvement in Memory withPlasticity-based Adaptive Cognitive Training (IMPACT) Study.Journal of the American Geriatric Society 2009;57:594–603.
18. Klingberg T, Fernell E, Olesen PJ, Johnson M, Gustafsson P,Dahlstrom K, Gillberg CG, Forssberg H, Westerberg H.Computerized training of working memory in children withADHS—a randomized, controlled trial. Journal of the AmericanAcademy of Child and Adolescent Psychiatry 2005;44:177–186.
19. Hardy J, Scanlon M. The science behind Lumosity. San Francisco,CA: Lumos Labs; 2009.
20. George DR, Whitehouse PJ. Marketplace of memory: what thebrain fitness technology industry says about us and how we can dobetter. The Gerontologist 2011;55:590–596.
21. Lumos Labs. Lumosity: Reclaim Your Brain�. San Francisco, CA:Dakim, Inc.; 2010. Available online at: http://www.lumosity.com,accessed April 3, 2010.
22. Kesler SR, Lacayo NJ, Jo B. A pilot study of an online cognitiverehabilitation program for executive function skills in children withcancer-related brain injury. Brain Injury 2010;25:101–112.
23. Fortuny LA, Briggs M, Newcombe F, Ratcliff G, Thomas C.Measuring the duration of post traumatic amnesia. Journal ofNeurology, Neurosurgery and Psychiatry 1980;43:377–379.
24. Russell WR, Smith A. Post-traumatic amnesia in closed headinjury. Archives of Neurology 1961;5:16–29.
25. Kertesz A. The Western Aphasia Battery – Revised [WAB-R]. SanAntonio, TX: Harcourt Assessment, Inc.; 2006.
26. Robertson IH, Ward T, Ridgway V, Nimmo-Smith I. The Test ofEveryday Attention. Bury St. Edmunds: Thames Valley TestCompany; 1994.
27. Stern RA, White T. Neuropsychological Assessment Battery. Lutz,FL: Psychological Assessment Resources, Inc.; 2003.
28. Papp KV, Walsh SJ, Snyder PJ. Immediate and delayed effects ofcognitive interventions in healthy elderly: A review of currentliterature and future directions. Alzheimer’s and Dementia 2009;5:50–60.
29. Palmese CA, Raskin SA. The rehabilitation of attention individualswith mild traumatic brain injury, using the APT-II programme.Brain Injury 2000;14:535–548.
10 S. Zickefoose et al. Brain Inj, Early Online: 1–10
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ibra
ry o
f H
ealth
Sci
-Uni
v of
Il o
n 05
/01/
13Fo
r pe
rson
al u
se o
nly.