Embed Size (px)
DESCRIPTION
Lessons learned in the implementation of strategies in schools: the case of Chile. Marcia Erazo. BMI ( Kg/m2). www.thelancet.com Published online February 4, 2011. School-based strategies. - PowerPoint PPT Presentation
Citation preview

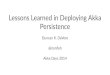
Lessons learned in the implementation of strategies in schools: the case of Chile.
Marcia Erazo

1990 1995 2000 2005 2010 20150
2
4
6
8
10
12
14
16
18
Obesity prevalence
AfricaAsiaLACOceaníaDeveloping countriesDeveloped countriesGlobal
%

3
www.thelancet.com Published online February 4, 2011BMI (KG/M2)

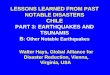
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 20110
5
10
15
20
25
30
School-children obesity rates
Prev
alen
ce ra
tes %

School-based strategies
• Chile, following the guidance of the World Health Organization, in 2007 implemented a series of strategies at schools (1000 schools nationwide).

Main strategies • Healthy kiosks: To reduce the exposure to “junk
food” at school.
• Physical education: To increase the total hours of physical activity
• Health promotion: To introduce health topics on a regular basis at school

Objective
• To analyze the barriers and facilitators to the implementation of strategies in schools.
• Complete reports at:• http://www.minsal.cl/portal/url/page/minsalcl/g_proteccion/
g_alimentos/prot_ego.html

First evaluation (2010)
• Qualitative evaluation, aimed to evaluate the process of implementation at regional and community level.
• Focus group and key stakeholders interviews.

Results
•At regional level:•Horizontal articulation:
• Technical orientations are applied al community level.
• Metropolitan area, there is a lack of coordination.
• There is inter-sectorial work between sports and educational institutions, that work together.

Results
• Vertical integration:
• There is intra-sectorial integration, especially when, at community level, there is a person designated to work the health promotion.
• Monitoring, supervising and accompanying the implementation at community level

Results
• Horizontal articulation at community level:
• There is inter-sectorial work.• Only actions at school level, once a
month.• “The school” sees this activity as an
“extra”.

Second evaluation (2010)
• Quantitave and qualitative methods
• Weight, height• Interviews

Results

Results

Results

Results

Third evaluation (2011)

Facilitators
• Principal’s will, by encouraging healthy habits.
• Possitive assessment of students in more hours of physical activity.

Barriers• Selling unhealthy foods at school.• To give money to children• Lack of continuity of interventions.
• Lack of intra-extra sectorial coordination• Managerial failure
• Lack of “political agreement”

School-based intervention in one community
• Presented in a seminar of successful practices to prevent childhood obesity, organized by PAHO, in Santiago-Chile, January 21-22, 2013.
• Conducted by Municipalidad de Peñalolén• http://www.paho.org/chi/

School-based intervention in one community
• Intervention:• Physical activity:
• 3 hours a week, in different days, specialized teacher, active pauses.
• Healthy eating and nutrition• Anthropometry• Healthy eating education to children, parents
and school community.• Healthy kiosks• Health promotion

Results
Physical activity
2009 2012
Hours 100% <2 a week 100% 3 hrs a wek
Distribution 1 day a week 3 days a week
Professional General teacher Specialized teacher

Active pause

Healthy kiosks
• Change in “terms of reference” to manage to kiosks


Lessons learned• Sustainability of the program is given by:
• Central management• Coordinated Inter-sectorial work• Inclusion of the strategies in the community
health plans and official documents.

Lessons learned
• Successful of the program is given by • The leadership and commitment of the school
principal, • Permanent monitoring of the correct
implementation of strategies, • Fcus on promoting healthy habits to children and
their families, • Reinforcement by regulation within and outside of
the schools of junk food

Thank you!!