Embed Size (px)
Citation preview

Getting Collaboration to Work in Wales
Lessons from the NHSand Partners
ReflectionsforPolicy andPractice


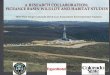
What Makes Effective Partnerships?FlexibilityIt takes time –
invest in relationshipsPublicise successes
Language is importantand common understandingsClarity of purpose
and common goalsBenefits for all over time
Enabling leadership
Top level commitmentEngagement with the workforce
Dedicated resources
COMMUNICATIONStakeholder engagement Collective responsibility
Partnership culture – honesty, openness and trust
Clear project structure andgovernance arrangements
Clarity of outcomesJoint funds to pumpprime projects for early wins
Mainstreaming Personal and organisational learning
Visibility – constantly reinforce and revisit purpose and approach

Getting Collaboration to Work in Wales
2
IntroductionRecent reports commissioned by NLIAH1 suggest that a wide range of factors and influences shape collaborative working. These factors can be categorised as one of three types: contextual factors which are external to the collaboration but have a significant impact on it e.g. financial and legislative frameworks; organisational factors which emphasise the different dimensions of the collaboration itself including ‘hard’ e.g. performance management and ‘soft’ e.g. leadership dimensions; and individual factors which highlight the influence of personal skills and attributes on the collaborative process. Figure 4 illustrates these factors in three concentric rings.
Figure 4: Factors influencing Collaborative Working
This illustration is not intended to provide a conceptual model of collaboration and so there is no attempt to measure the strength of individual factors or to indicate the complexity or direction of the relationships between them, but it is intended to emphasise the point that it is exceedingly difficult to reduce the process of collaborative working to a set of simple lessons to guide policy and practice.
This current research study, involving a detailed assessment of collaborative working in five case studies across Wales, highlights the importance of a number of factors in effective collaborative working, many of which are identified above. These are discussed below and supported by additional reflections from the wider body of literature on collaboration.
1 NLIAH (2007) Working in Collaboration: Learning from Theory and Practice Cardiff: NLIAH
NLIAH (2007) Learning to Collaborate: Lessons for Effective Partnership Working in Health and Social Care Cardiff: NLIAH
History ofCollaboration:Collaborative
Experience and know how
CONTEXTUAL
Social and EconomicDrivers
FinancialFramework
and Incentives
Institutional andStructural
Factors
LegislativeContext
Leadership Culture
Decisionmaking
arrangements
Learning
PublicEngagement
PerformanceManagement
Accountability
FinancialResources
Role andPurpose
INDIVIDUAL
GOVERNANCE
Personal CharacteristicsProfessional Status
Skills and CapabilitiesExperience

Lessons from the NHS and Partners
3
Clarity and Strength of PurposePartnerships are populated by people and organisations from a wide range of sectors, backgrounds, professions and cultures that are charged with different roles and responsibilities, are subjected to different social, economic and financial pressures, and are accountable in different ways to governing bodies and the recipients of their services. Clearly, in this situation, it is no surprise that people and organisations are motivated in different ways to seek collaborative ways to solving complex problems and delivering public services2. In the main, these are:
Having to: because of national government edict and mandate including statutory duties to ‘work in partnership’, general exhortation and the use of financial incentives and flexibilities. Needing to: because of the recognition that organisations are inextricably linked in the design and delivery of many public services, because of the need to avoid duplication and promote better co-ordination, and because of the need to share resources and learning.Wanting to: because it is evident that services should be grounded in the needs of citizens and users and not in the administrative convenience and configuration of service providers i.e. citizen centred/client-focused.
The consequence is that many forms of collaboration consist of people and organisations with multiple and even conflicting motivations, and that these can alter over time as a result of the experiences of collaboration and changes in the external environment3. Moreover, although issues such as trust, reciprocity, autonomy and shared vision are emphasised in much of the literature on effective collaborative working, these are manifest differently in voluntary and mandated expressions of collaboration4.
Linked to motivation, is the importance of clarity and strength of purpose. One clear message to emerge from the case studies was the motivational power of appealing visions – the satisfaction that managers and practitioners derived from working in partnerships that were designed to improve the quality of life of vulnerable people – children with a disability or unemployed workers who suffered from chronic illness. Whenever there were difficult, tense or protracted negotiations and conflicts in the partnership an appeal to the wider purpose of the partnership was often considered to be the glue that ‘kept partners engaged and willing to make compromises’. The members of the Steering Groups in Flintshire CIDS and Neath Port Talbot CCM reported that their purposes provided a clear focus and a common cause. Although there was still potential for difference in interpretation even with a defined client group, it was far less than in partnerships such as those at Wrexham and DIS, which were focussed at a strategic level involving a wide selection of client groups.
2 Gazley, B. (2008) “Intersectoral Collaboration and the Motivation to Collaborate: Toward an Integrated Theory”, in Bingham, L.B. and O’Leary, R. (eds) Big Ideas in Collaborative Public Management New York: M.E.Sharpe
3 Oliver, C. (1990) “Determinants of Interorganizational Relationships: Integration and Future Directions”, Academy of Management Review, Vol. 15 No. 2 pp. 241-265
4 Glasby, J. and Dickinson, H. (2008) Partnership Working in Health and Social Care Bristol: Policy Press

Getting Collaboration to Work in Wales
4
The case studies examined in this research were all engaged in some form of ‘integration’ between health and social care. However, as has been highlighted in the individual studies, there were numerous interpretations and perspectives about the notion of integration. A number of practical guides suggest that there is a continuum along the journey between fragmentation and integration with various positions along the way – co-location and co-ordination5. The design and delivery of services, and the associated management and governance arrangements are different in each of these situations, and it is helpful to establish a consensus about which one is being developed.
However, there is an issue which surfaced in some of the interviews in relation to the question of whether to seek absolute clarity of purpose (and intent) from all parties at the outset of the process, or whether to negotiate sufficient consensus to promote collective action. The issue here was that insistence on clarity may generate paralysis in the partnership if different partners could not reconcile their different values, motivations and views with this clear purpose. Consequently, a certain amount of ambiguity might be helpful in making progress particularly in the early stages of a collaboration – experience may confirm or dismiss initial fear. On the other hand, insufficient clarity at the outset may risk conflict and dissent at a later point when matters of purpose, doing things differently and giving things up become unavoidable.
5 Integrated Care Network (2004) A Practical Guide to Integrated Working Leeds: ICN

Lessons from the NHS and Partners
5
Collaborative Capabilities Many interviewees in the research study believed that the key to making collaborations work was people driven by a common vision and armed with particular skill set. This position finds support in the literature on collaboration which concludes that working and managing in collaborative arenas demands different skills and capabilities from those used when working in single organisations6 and these are summarised in Figure 57.
CapabilitiesforCollaboration
An ability to develop and sustain inter-personal relationships • based on trust and reciprocity
Well developed communication skills including listening•
A tolerance for ambiguity and diversity with an appreciation of • different perspectives and world views
An ability to seek consensus and resolve conflict through • negotiation and diplomacy
An appetite for creativity, innovation and entrepreneurship • coupled with a preparedness to take risks
An ability to understand interdependency and a visualisation • of the organisational roles and responsibilities in a particular health and social care domain
Experience of working in different sectors, different policy • areas and in different types of organisation
Figure 5: Capabilities for Collaboration
These capabilities are very similar to those elaborated by Bingham et al (2008)8 who describe the ‘artful and effective practice’ that is required by the ‘collaborative public manager’ including, designing networks with the necessary players at the table, structuring appropriate governance arrangements, negotiating ethically, facilitation, managing conflict, engaging the public, and designing evaluation systems. In a similar vein, Agranoff’s9 (2004) advice on how to manage in a non-
6 Agranoff, R. and McGuire, M. (2003) Collaborative Public Management: New Strategies for Local Governments Washington: Georgetown University Press
Peck, E. and Dickinson, H. (2008) Managing and Leading in Inter-Agency Settings Bristol: Policy Press
Williams, P. (2002) “The competent boundary spanner”, Public Administration, Vol. 80 pp. 103-124
7 Williams, P.M. (2008) “Competencies for Collaboration”, 2nd Copenhagen Conference on Partnerships
8 Bingham, L.B. Sandfort, J. and O’Leary (2008) “Learning to Do and Doing to Learn: Teaching Managers to Collaborate in Networks, in Bingham, L.B. and O’Leary, R. (eds) Big Ideas in Collaborative Public Management New York: M.E.Sharpe
9 Agranoff, R. (2004) “Leveraging Networks: A Guide for Public Managers Working Across Organizations”, in Kamensky, J.M. and Burlin, T.J. (eds) Collaboration: Using Networks and Partnerships New York: Rowman and Littlefield Publishers Inc.

Getting Collaboration to Work in Wales
6
hierarchical, self-organising network includes:
Being a representative of both your organisation and the network by balancing • the dualism of agency and collective concerns
Taking a share of the administrative burden because of the often lack of co-• ordinating capacity
Recognising shared expertise-based authority – valuing the contribution of • people at different levels both formally and informally and promoting dispersed leadership
Staying within the decision bounds of the network and avoiding unnecessary • interference in the roles and responsibilities of formal organisations
Accommodating and adjusting while maintaining purpose•
Being as creative as possible•
Being patient and using interpersonal skills•
Recruiting members constantly to expand the involvement base and promote • inclusivity
Emphasising incentives to people to participate in networks particularly • enhanced information and knowledge and the opportunity to devise collaborative solutions to common problems
Suitable training, development and other opportunities are necessary to help ensure that partners have the requisite competencies. It is not sufficient to assume that because a particular professional or manager can manage in his/her own organisation, they can perform equally well in a collaboration setting.
Dedicated OfficersThe case studies examined in this research suggested an important role for dedicated officers to support, co-ordinate and service collaborative processes. However, one problem identified was how such people were resourced and sustained. The Joint Working Special Grant had been critical in a number of instances across Wales including the Flintshire CIDS project – but the continuity of this type of pump-priming resource was uncertain. On some occasions, a number of partner agencies contributed to the funding of a dedicated officer, in others there were seconded arrangements, and in others, support was found in a rather ad hoc manner from within general management and administrative arrangements. Clearly, a dedicated officer could help to raise the profile of collaborative ventures as opposed to those that relied on the goodwill of mainstream staff who were attempting to fit collaboration within their existing heavy workloads.

Lessons from the NHS and Partners
7
The message from the DIS project was that a dedicated officer was essential to provide a range of support, servicing, monitoring, communication and co-ordination activities. Basic administrative and secretarial support was needed as a minimum to support the partnership processes, but in some cases, dedicated officers were able to provide a more technical and professional role and assist with policy development and delivery.
Some interesting literature relating to private sector collaborations identifies a range of sources of collaborative capability in addition to dedicated officers, together with examples of some particular techniques that can be used. Four key roles are associated with what is termed successful ‘alliance management’10 – improved knowledge management particularly by acting as the focal point for learning and leveraging lessons and feedback from other alliances; increased external visibility; providing internal co-ordination especially mobilising internal resources to support strategic initiatives; and, facilitating intervention and accountability especially alliance metrics and evaluation.
CollaborativeCapabilityMechanisms
Mechanism Techniques
Training Tool handbook; best practice; competency framework; in/house training; cultural programme
Partnership Function
partnership department/manager; intranet; alliance database
Partnering Tool joint business planning; partner portal
Development Support
rewards; bonuses; management development programme
Experts consultants; mediators; legal/financial experts
Evaluation Tool joint evaluation; alliance metrics; cross-alliance evaluation
Figure 6: Collaborative Capability MechanismsAdapted from: Ard-Pieter de Man (2005) “Alliance Capability: A Comparison of the Alliance Strength of European and American Companies”, European Management Journal, Vol. 23, pp. 315-323
Figure 6 indicates that there are six main mechanisms for facilitating effective collaborative management between organisations – training tools such as best practice documents, collaborative competency frameworks setting out skills, abilities and capabilities for collaborative management and training programmes to encourage collaborative working; dedicated partnership functions in the form of
10 Dyer, J.H. Kale, P. and Singh, H. (2001) “How to Make Strategic Alliances Work”, Sloan Management Review, Vol. 42. No.4. pp. 37-43

Getting Collaboration to Work in Wales
8
departments and people supported by appropriate communications systems and databases; specific tools to encourage collaborative activity such as joint business planning; clear support to acknowledge the value of collaboration in the shape of incentives and rewards and links to individual appraisal systems and management development opportunities (it is likely that financial recognition is not the only way to achieve enhanced collaborative performance11 mainly because collaboration is not an individual endeavour and that people can be motivated by a different set of presumptions); the use of outside experts and consultants to provide special assistance in relation to process or knowledge; and finally, the use of evaluation tools to measure the impact of a collaboration.
Leadership for CollaborationThere is a considerable literature promoting the view that collaborative arenas require different leadership approaches and practices to those traditionally deployed in single organisations12. The context demands a style and approach which stands in sharp contrast to the often directive, command and control frameworks that characterise many bureaucratic public agencies. Figure 7 summarises the key characteristics of collaborative arenas.
Firstly, collaborative settings are characterised by a raft of policy problems that exhibit varying degrees of ‘wickedness’13. These have a propensity to cross many types of boundary – organisational, professional, sectoral and generational; cannot be contained within conventional jurisdictional or professional cages; are ‘wicked’ because of the difficulty of achieving consensus amongst a diverse set of stakeholders and interests promoting different constructions of problem definition, cause and solution14 and are intractable and not easily tamed. As a consequence, they are not easily resolved by single agencies acting autonomously and demand collaborative solutions.
11 Ingraham, P.W. and Getha-Taylor, H. (2008) “Incentivizing Collaborative Performance”, in Bingham, L.B. and O’Leary, R. (eds) Big Ideas in Collaborative Public Management New York: M.E.Sharpe
12 Chrislip, D.D. and Larson, C.E. (1994) Collaborative Leadership San Francisco: Jossey Bass
Crosby, B.C. and Bryson, J.M. (2005a) Leadership for the Common Good: Tackling Public Problems in a Shared-Power World San Francisco: Jossey Bass
Lipman-Blumen, J. (1996) The Connective Edge: Leading in an Interdependent World San Francisco: Jossey Bass
Luke, J.S. (1998) Catalytic Leadership: Strategies for an Interconnected World San Francisco: Jossey Bass
Alexander, J.A. Comfort, M.E. Weiner, B.J. and Bogue, R. (2001) “Leadership in Collaborative Community Health Partnerships”, Nonprofit Management and Leadership, Vol. 12 No. 2 pp. 159-175
13 Rittel, H. and Webber, M. (1974) Dilemmas in a general theory of planning, Policy Sciences, 4, pp.55-169
14 Benford, R.D. and Snow, D.A. (2000) ‘Framing Processes and Social Movements: An Overview and Assessment’, Annual Review of Sociology, Vol 26, 611-639
Gray, B. (2003) ‘Framing of Environmental Disputes’, in Lewicki, R.J. Gray, B. and Elliott, M, Making Sense of Intractable Environmental Conflicts Washington: Island Press.

Lessons from the NHS and Partners
9
TheNatureandCharacteristicsofCollaborativeArenas
Wicked issues: cross boundary; socially constructed; no • optimal solutions; incapable of resolution by one agency acting autonomously
Interdependency and diversity resulting in heightened • complexity and incongruence
Confused by multi-level and tempoal imperatives•
No-one-in-charge: diffuse and contested power relationships•
Multiple and divergent motivations, objectives, value systems•
Diverse cultures, professions, operating systems, legal and • financial frameworks and accountabilities
Figure 7: The Nature and Characteristics of Collaborative Arenas
Secondly, collaboration involves high degrees of interdependency between organisations in terms of their ability to tackle difficult problems efficiently and effectively – the consequent processes, structures and governance arrangements are complex and sometimes difficult to reconcile as a result of diversity. Thirdly, collaborative settings are often made more complex because of the multi-level nature of governance – local, regional, national and European – and the multiple formal and informal relationships between public and private organisations within each level. Also, further confusion is often involved with planning and action over different timescales – immediate to inter-generational. Fourthly, power relationships are not single and hierarchical but dispersed and contested – Crosby and Bryson15 refer to a situation of ‘no-one-in-charge, shared power world’. Fifthly, as has been discussed above, people and organisations involved in collaboration often have different motivations and objectives and their fundamental value systems and ways of working can be different. Lastly, different partner organisations inevitably collide as a result of having different cultures and accountability arrangements, are subject to different statutory duties and performance management frameworks and are influenced by the nature of the professionals that work within them.
In collaborative arenas, leadership needs to be based on 6 key principles outlined in Figure 8. Principle 1 involves building and sustaining effective inter-personal relationships between a diverse set of people and organisations based on trust, reciprocity, respect, valuing difference and diplomacy. This is important at individual, group and network levels. Principle 2 concerns having an understanding of the web of relationships, connections and multiple forms of independencies between organisations – strategically, operationally, spatially and functionally. Principle 3 reflects an ability to both appreciate and understand the different perspectives, cultures and ambitions of a range of partner organisations, and to
15 Crosby, B.C. and Bryson, J.M. (2005) Leadership for the Common Good: Tackling Public Problems in a Shared-Power World San Francisco: Jossey Bass

Getting Collaboration to Work in Wales
10
provide a conducive environment in which to facilitate a process to allow them to realise common purposes.
LeadershipforCollaboration
INTER-PERSONALSKILLS• to build and sustain relationships between diverse stakeholders, and to promote inclusive processes particularly in groups and networks
Appreciation of • STRATEGICINTERDEPENDENCIES and systems – spatial, temporal and funtional – to deal with complexity and connectivity
An ability to perform as a • TRANSLATOR by understanding the diverse meanings and aspirations of disparate constituencies: agencies, professions, cultures and sectors
CREATIVEABILITY• with a propensity for innovation, experimentation and cross fertilisation of ideas/practices
An ability to construct a • LEARNINGENVIRONMENTto reflect the emergent and complex nature of the prevailing environment, and to promote reflection, conceptualisation and thinking
Commitment to • DISPERSED forms of leadership through empowerment strategies and decision making processes that encourage accountability and responsibility
Figure 8: Principles of Leadership for Collaboration
Principle 4 focuses on the need to promote new ways of tackling intractable issues through innovation and experimentation, risk taking, and a sharing of ideas, approaches and practices. Principle 5 values individual and organisational learning and the importance of devising effective formal and informal mechanisms for promoting thinking, reflection and knowledge transfer. Lastly, Principle 6 acknowledges the inappropriateness of models of leadership that are based on controlling, commanding, directive, authoritarian and hierarchical approaches in favour of ones that are more dispersed, empowering and facilitative.
Both the DIS Project and the CCM Programme provide examples of some of the principles for leadership for collaboration articulated by a selection of respondents involved in both partnerships and illustrated in Figure 9.

Lessons from the NHS and Partners
11
LeadershipforCollaborationinWales
1 “Leadership needs to be more facilitative – to be more persuasive,influencing and helping – rather than ‘you will’
2 “he was ideal for the job, not dictatorial; facilitative but task-orientated; provided clarityofexpectation; and stuck with the Project”
3 “she is task-orientated; keeps us on track; is inclusive; very skilful and task-orientated; she has a facilitative style and is wellconnected with senior people in other organisations”
4 “it is critically important to articulate a cleardirection – to constantly talk about solutions and to engage people collaboratively in the realisation of these – communication cannot be over-emphasised”
5 “you can’ttell people what to do – you must find out what people’s views are – you have to exploreandunderstandother people’s perspectives and have confidence in each other – to work with others and nottrytoimposeverticallinesofmanagementinanetworktypearrangement”
6 ‘connectedleadership’ – a form of leadership that required one to understandotherorganisations and putting yourself in their places; to be facilitativeandenabling; to look for win/winsolutions and benefits for all participants; of managing risk differently and to devise accountabilities that straddled different organisations’
Figure 9: Examples of Leadership for Collaboration from the Case Studies

Getting Collaboration to Work in Wales
12
ResourcesDifferent forms of collaboration need access to different kinds of financial resources. In the case studies examined in this research study, reference was made to the need for finance for following purposes:
To support and service the process•
To fund or pump prime pilots or projects•
To mainstream collaborative initiatives within core budgets •
To fund new ways of working in the mainstream (this is different from • mainstreaming pilot projects, but suggests that the collaboration is trying to redesign the mainstream through its operations)
In the case of the CCM, resources of the first two types were very helpful in enabling the project to be designed and delivered. Funding covered the cost of a Programme Manager and a range of other appointments to deliver the CCM programme – this was ‘new’ money, extended when the Project was exceeding its targets. However, the issue of what to do when project funding ceases remained. The Joint Special Working Grant has been used in a number of projects to support dedicated staff without which, in the opinion of local stakeholders, the partnerships would not have been sustainable. Here too the question is what will happen at the termination of the grant. In the absence of such support, where organisations had to struggle to find administrative and secretarial staff from within their own organisations to support partnership processes, this was often considered to limit their overall potential.
Although it was reported by some respondents that some professionals and managers faced with demanding posts were reluctant to devote time to partnership matters, in general, working in collaboration was an acknowledged part of mainstream activity and sometimes formally recognised as such in job descriptions and annual performance review processes as was the case with a number of senior managers in the case studies. In others, jointly funded posts between local authorities and local health boards using S.33 flexibilities were considered to be very helpful. These posts often focus on specific groups of users and one authority for instance has a Director of Integrated Care. However, as was reported by a number of interviewees, jointly funded posts are not without their problems particularly in terms of continuity of funding, tensions around accountability and day to day management.
The DIS Project and the Wrexham Locality work have taken place within a predominantly resource-neutral context, and although the aim is to demonstrate greater efficiencies (and/or effectiveness?) through better co-ordination and integration of services, this has been difficult to demonstrate. Also, the lack of pump priming resources has inhibited the potential for pilots and other interventions.

Lessons from the NHS and Partners
13
Although there are very significant differences between different forms of collaboration, the availability of financial resources is clearly an important factor in servicing and co-ordinating the collaborative process and enabling new projects and programmes to be developed.

Getting Collaboration to Work in Wales
14
Governance ArrangementsGood governance in partnerships is: “about continuing to ensure some form of openly enacted accountability at a local level for public services designed and/or delivered by a disparate range of organisations which are choosing or obliged to collaborate”16. Collaborative working is manifested in different forms and different governance arrangements are necessary to exercise control – to provide a clear focus and purpose for the collaboration, to regulate the behaviour of the actors, and to secure good performance17. Transparent decision making arrangements and clear lines of accountability are especially important factors in collaborative arenas but these may be difficult to secure as partner organisations will also be driven by the governance arrangements of their host organisation which may have different rules and requirements to those of the collaboration.
Clearly, the role and purpose of the Wrexham and DIS Projects are different to those concerned with managing specific initiatives such as the CCM or Flintshire CIDS. However, what is important in all cases is that representation of relevant interests and stakeholders is inclusive and appropriate, and that decision making arrangements, accountability structures and performance management systems are carefully designed to match each type of collaboration. Also, collaborative working is a dynamic process and the role of governing bodies may change over time particularly to reflect the progression between policy formulation and delivery.
ElementsofCollaborativeGovernance
FORMAL INFORMAL
1 Legal Form2 Financial3 Property Rights4 Scope and Exclusivity5 Goals, planning and control
6 Conflict resolution and sanctions7 Decision making and hierarchy8 Communications9 Leadership
10 Reputation11 Personal Relationships13 Norms/Values14 Trust15 Culture
Figure 10: Elements of Collaborative Governance
16 Integrated Care Network (2006) We have to stop meeting like this: the governance of inter-agency partnerships Leeds: ICN
17 Sullivan, H. Barnes, M. and Matka, E. (2007) “ Building Collaborative Capacity for Collaborative Control: Health Action Zones in England”, in Gossling, T. Oerlemans, L. and Jansen, R. (eds) Inside Networks: A Process View on Multi-Organisational Partnerships, Alliances and Networks Cheltenham: Edward Elgar

Lessons from the NHS and Partners
15
Figure 10 suggests that collaborative governance consists of a number of key elements, and the importance of each one varies depending upon the extent of formality or informality intended. So, personal relationships, shared norms and values, trust and compatible cultures may be particularly important within collaborations that rely on informal arrangements, whereas legal and financial matters are particularly crucial in more formal structures. However, the value of this illustration rests essentially in its identification of a checklist of factors that need to be addressed in devising governance arrangements that are fit for purpose for individual initiatives. A Governance Assessment Tool is also available to help guide new partnerships or assess the effectiveness of existing arrangements18.
The issue of accountability is often a source of confusion in collaboratives particularly in relation to performance. The type of problems encountered often include lack of agreement amongst partners on which results to measure; fear of losing control over results they are asked to achieve; overly narrow focus on implementation efforts at the expense of broader policy goals; and the need to clarify “who should be accountable to whom and for what results – both between the collaborative partners themselves, and between the collaborative and its external overseers and stakeholders”19. One framework for distinguishing between the four types of accountability relationships that characterise collaboratives – legal, hierarchical, political and professional – and of linking these to performance is provided by Page (2003) through his notion of platforms of accountability – external authorisation, internal inclusion, results measurement and managing for results (Figure 11).
18 INLOGOV (2003) Governance Assessment Tool www.inlogov.bham.ac.uk/research/esrcpartnership.htm.
Skelcher, C. Mathur, N. and Smith, M. (2004) Effective partnership and good governance: lessons for policy and practice INLOGOV: University of Birmingham
19 Page, S. (2004) “Measuring Accountability for Results in Interagency Collaboratives”, Public Administration, Vol. 64 No. 5 pp. 591-606

Getting Collaboration to Work in Wales
16
PlatformsforAccountabilityofResults: MeasuresforInteragencyCollaboratives
Platform Measures
ExternalAuthorisationThe capacity to manage expectations and to respond to the demands of political stakeholders
Increases in collaborative discretion, flexibilities, and resources; removal of rules; new legislation
InternalInclusionThe capacity to manage expectations and to respond to the demands of professional colleagues and collaborative partners
Increase in diverse stakeholders; enhanced social capital and stronger working relationships; use of participatory decision making
ResultsManagementThe capacity to identify the collaborative’s mission, goals and indicators of progress, and to track data that document changes in progress over time
Methods to track data about progress over time to mission and goals; use of indicators; performance management systems
ManagingforResultsThe capacity to use data about results strategically to assess progress and to improve policies and operations in the future
Ability to adjust policies and programmes in the light of performance data; structure and enforcement of rewards and sanctions for results achieved
Figure 11: Platforms for Accountability of Results (adapted from Page (2004))
Page refers to legal accountability relationships as those entailing a high degree of control that is external to the organisation such as laws and statutory duties; hierarchical relationships with a high degree of internal control such as those provided by rules and bureaucracy; political relationships in the form of pressures from outside stakeholders; and professional relationships through peer expectations and professional bodies. It is likely that each collaborative will have a particular mix of these accountability relationships, although some will be more apparent or relevant than others.

Lessons from the NHS and Partners
17
Integrated Design and DeliveryImplementation is a significant challenge for collaborations as the cases studies demonstrate. Considerable time is required to co-produce effective solutions. A key principle must be to ensure that the process of design and delivery (and evaluation) is integrated – that the processes and structures that are constructed do not impose barriers between them, for example by separating policy makers from implementers.
Delivering integrated solutions in cases such as Monnow Vale and Flintshire CIDS has been difficult and time consuming and there remains disagreement between partners about the best way to make the kinds of changes needed. For example, in the case of Monnow Vale, the merits of the decision to co-locate health and social care services as a prelude to integrated management arrangements were disputed – others argued that it might have been better to get all the organisational change over in one go. The value of formalising delivery through S.33 Flexibility arrangements was also contested – do you ground integration in trust and reciprocity between agencies or do you seek the contractual security of a legally binging agreement that spells out in great detail what the roles, responsibilities and financial requirements are for each partner? Arguably, you can achieve the same purpose with either but the formal route gives a clear indication of exactly how far organisations are prepared to collaborate. On balance, although the journey to integration is problematic, clarity of purpose is likely to encourage a more effective process between design and delivery.

Getting Collaboration to Work in Wales
18
Strategic Management ApproachThe public sector is dominated by a rational, planned and prescriptive approach to strategy making20. This involves a top-down, sequential and ordered approach setting out a course of action into the future. It is often guided by fixed mission statements and accompanied by a number of goals and objectives. There is a presumed rationality between means and ends and the result is often a grand plan or design that is internally consistent and comprehensive21.
Too often this type of approach has proved to be highly inflexible and inappropriate to managing in a fast changing and turbulent world22. Problems such as difficulty in forecasting the future with any degree of accuracy and of a separation between the design and delivery stages of the process have called into question the value of this approach, although it is still in widespread use23.
The evidence of the case studies examined in this research demonstrates that a more emergent approach to strategy is more realistic approach – where thinking and action become more integrated, and reflection and learning are more pronounced (Figure 12). The notion of strategy being ‘crafted’ (Mintzberg, 1987) is helpful – this acknowledges ambiguity and lack of closure as opposed to being prescriptive and explicit. This approach is sensitive to the involvement of a diverse set of stakeholders in the process – both at strategic and operational levels – it encourages processes that are negotiative and interactive, acknowledges that power relationships are dispersed rather than sovereign, and accommodates bargaining and political manoeuvring within and between dominant coalitions of interests. It invites an emphasis on creativity and innovation – exploratory, creative and entrepreneurial efforts that are being promoted in the Wrexham Locality work.
20 Flynn, N. and Talbot, C. (1996) “Strategy and strategists in UK local government”, Journal of Management Development, Vol. 15. No. 2 pp. 24-37
Boyne, G. (2001) “Planning, Performance and Public Services”, Public Administration, Vol. 79 No. 1 pp. 73-98
21 Mintzberg, H. (1994) The Rise and Fall of Strategic Planning New York: Prentice Hall
22 Stacey, R.D. (1990) Dynamic Strategic Management for the 1990s London: Kogan Page
23 Sullivan, H. and Williams, P. (2009) “The Limits of Co-ordination: Community Strategies as Multi-Purpose Vehicles in Wales”, Local Government Studies (forthcoming)

Lessons from the NHS and Partners
19
TheEmergentProcessofStrategyMaking
Emergent strategy implies learning what works – taking one action at • a time in search for a viable pattern or consistency
This does not mean chaos but is unintended order•
Whereas deliberate strategies focus on direction and control, emergent • strategies open up the potential for ‘strategic learning’
Management is not out of control in emergent strategies – it is open, • flexible and responsive
This approach is especially important when an environment is too • unstable or complex to comprehend or too imposing to defy
An emergent strategy allows management to act before everything is • fully understood – to respond to an evolving reality rather than having to focus on a stable fantasy
Whereas more deliberate strategies emphasise central direction and • hierarchy, emergent ones open the way for collective action and convergent behaviour
High complexity and fast rates of change require emergent strategies, • whereas a top-down strategy-making process is more suitable for relatively stable situations characterised by low complexity. In turbulent environment (high uncertainty), the process of defining a strategy becomes a messy and experimental process driven from the bottom up.
Strategy formulation is a political process involving various groups • and individuals pursuing their interests using power and influence and various tactics to devise actions
Emergent strategies are ‘crafted’ with a fusing of formulation and • implementation
Sources Carter, C. Clegg, S.R. and Kornberger, M. (2008) A Very Short, Fairly Interesting and Reasonably Cheap Book about Studying Strategy London: SageMintzberg, H. and Waters, J. (1998) “Of strategies, deliberate and emergent”, in Segal-Horn, S. (ed) The Strategy Reader Oxford: Blackwell
Figure 12: The Emergent Process of Strategy Making

Getting Collaboration to Work in Wales
20
Individual and Organisational LearningOne of the reasons that individuals and organisations work in collaboration is to acquire, share and generate learning and knowledge to apply to the resolution of complex policy problems. An emergent approach to strategy making discussed above is consistent with this motivation. As an outcome in its own right, individual and organisational learning can be highly significant not just for a current collaborative venture but for future initiatives. An important issue is the extent to which learning is pursued in an explicit fashion or whether it is a natural by-product of people from different organisations, cultures, professions and sectors joining together to deliberate on matters of common interest.
Apart from formal partnership meetings, the DIS Project for instance, embarked upon a programme of ‘organisational raids’ and presentations to enhance learning and awareness of best practice; the CCM Project had a representative from another similar project in Wales on its Steering Committee to help share common experiences; and one member of the Monnow Vale Steering Group was a member of the UK Integrated Care Network. The strategy of using pilots and experimental projects as the basis for precipitating whole-system change is very much predicated on risk taking and continuous learning. The approach in Monnow Vale of incremental change based on taking actions and learning from their effectiveness in practice emphasised learning from ‘what works’ and reflective practice.
The critical issue is what, if any, attempts are made to capture, disseminate, embed and formalise learning. Is the learning generated at partnership events transmitted through partner organisations or does it remain with a relatively small cadre of people who are actively engaged in partnership activities? In particular, how is tacit knowledge especially about partnership processes and management converted into an explicit form?24 The evidence from the case studies for the above is limited, and a number of interviewees were acutely aware of the difficulties presented by key partnership personnel leaving collaborative projects and programmes. Finding suitable replacements was not always easy, personal and group dynamics were often affected, and they often took with them ‘learning’ which could not otherwise be acquired.
Formal learning is enabled through policies, systems and procedures that are integrated rather than fragmented25. The case studies of Monnow Vale and Flintshire CIDS highlights the difficulties faced by separate systems and incompatible IT frameworks, but tools such as unified assessments have the potential for promoting a more unified and comprehensive approach to service design and delivery.
24 Salk, J.E. and Simonin, B.L. (2005) “Beyond Alliances: Towards a Meta-Theory of Collaborative Learning”, in Easterby –Smith, M. and Lyles, M.A. (eds) Handbook of Organizational Learning and Knowledge Management Oxford: Blackwell
25 Vera, D. and Crossan, M. (2005) “Organizational Learning and Knowledge Management: Toward an Integrative Framework”, in Easterby –Smith, M. and Lyles, M.A. (eds) Handbook of Organizational Learning and Knowledge Management Oxford: Blackwell

Lessons from the NHS and Partners
21
Outcome Focused EvaluationThe case studies confirm the view that ‘evaluation’ is the ‘cinderella’ of the policy process. Undoubtedly, measuring the success and outcomes of collaboration are difficult and complex – conceptually, methodologically and practically26 – but there is a general reluctance to invest in this element of the process compared to the others. Naturally, policy development, and particularly the vicissitudes of the implementation challenge, is more than sufficient to occupy the working lives of managers and practitioners. However, in the context of a public policy environment which increasingly values transparency, accountability, cost-effectiveness and results, ignoring evaluation is not an option. A culture that demands ‘evidence-based’ policy must acknowledge the contribution of evaluation if key questions are to be answered, for example, how do we know that integration between health and social care is an improvement on a previously fragmented and unco-ordinated approach? Does it deliver a better quality of life for service users? Is it more effective in the use of scarce resources? Does the process of collaboration itself generate social capital, personal networks and inter-organisational learning that can be released to best effect on future co-operative actions?
Evaluation needs to be part of an integrated approach to policy design and delivery – it needs to be considered at the outset of the process and is helped by clarity of purpose which is capable of being converted into key outcomes.
It may be that these outcomes vary between different stakeholders – nevertheless, it is important to articulate these so that a judgment can be made as to whether they have been realised. This ’stakeholder’ approach to evaluation may be particularly appropriate for multi-party collaborations27. Interestingly, in a number of the case studies, reference was made to the need to include service users in the process of evaluation – for instance, the CCM Programme successfully used ‘stories’ from users to evidence the change that had been brought about in their lives as a result of participating in the programme. There is a natural tendency to concentrate on measuring outputs, partly because they are easier to measure and often partly to demonstrate that progress is being made in a partnership. This cannot be a substitute for outcome-focused frameworks that are designed to measure the impact of collaborative action. Recent developments in ‘theory-based’ evaluation in the US and the UK have made important contributions here by emphasising the particularity of collaboration and the implications for evaluation, demonstrating how evaluation and evaluators can help in the design of complex interventions
26 Barnes, Barnes, M Bauld, L Benzeval, M Judge, K Mackenzie, M and H Sullivan (2005) Building capacity for health equity, London, Routledge
27 Barnes, Barnes, M Bauld, L Benzeval, M Judge, K Mackenzie, M and H Sullivan (2005) Building capacity for health equity, London, Routledge

Getting Collaboration to Work in Wales
22
and by bringing ‘professional evaluators’ and practitioners more closely together.28 Nonetheless significant problems still need to be resolved in developing outcome focused evaluation including tackling issues of attribution and measuring synergy.
FrameworkfortheEffectsofCollaboration
First-OrderEffects Social capital: trust, relationships•
Intellectual capital: mutual • understanding, shared problem frames, agreed-upon data
Political capital: ability to work • together for agreed ends
High quality agreements•
Innovative strategies•
Second-OrderEffects New partnerships•
Co-ordination and joint action•
Joint learning extends into the • community
Implementation of agreements•
Changes in practices•
Changes in perceptions•
Third-OrderEffects New collaborations•
More co-evolution, less destructive • conflict
Results on the ground•
New institutions•
New norms and heuristics•
New discourses•
Source: Innes, J. and Booher, D. (1999) “Consensus Building and Complex Adaptive Systems: A Framework for Evaluating Collaborative Planning”, Journal of the American Planning Association, Vol 65 No. 4 pp.412-23Figure 13: Framework for the Effects of Collaboration
28 Sullivan, H and Stewart, M (2006) ‘Who owns Bauld, L Judge, K Barnes, M Benzeval, M MacKenzie, M and Sullivan, H (2005) ‘Promoting Social Change: The experience of Health Action Zones in England’, Journal of Social Policy, Vol. 34, No. 3, pp 427-445
Sullivan, H. Judge, K and Sewell, K (2004) ‘In the eye of the beholder’: Perceptions of local impact in English Health Action Zones’, Social Science and Medicine, Vol. 59, pp1603-1612
the Theory of Change?’, Evaluation, The International Journal for Theory and Practice, Vol. 12, No. 2, pp179-199
Connell, J.P. Kubisch, A.C. Schorr, L.B and C. H. Weiss eds., (1995) New Approaches to Community Initiatives: Volume 1 - Contexts, Methods and Contexts, Washington DC, Aspen Institute
Coote A., Allen J., and Woodhead D. (2004) Finding Out What Works: Building knowledge about complex community based initiatives, London, The King’s Fund.

Lessons from the NHS and Partners
23
Innes and Booher (1999)29 offer a useful framework for identifying the effects of collaboration which could be used as the basis for evaluation (Figure 13). It is unlikely that all these dimensions can be explored in every collaboration and some may be more appropriate than others. However, it does highlight the potential contribution that collaboration can make particularly if sustained over time. First order effects refer to the benefits of the collaborative process in terms of building social capital and enhanced potential for joint working, whereas third order effects focus on the longer term prospect of whole-systems change resulting in institutional reform and the co-evolution of solutions between organisations working in an integrated fashion.
It is clear that existing performance management arrangements, which are different for health and social care, are not always helpful in encouraging the development of attempts to measure the impact of integration. There is a challenge for projects such as Monnow Vale and the Flintshire CIDS Project to develop measures that reflect integrated and collaborative approaches to the problems they face and the services they provide, rather than account for individual contributions and report back to parent organisations.
The CCM Programme stands out as an example of a project conceived and developed within an evidence-based culture. This was partly a product of it being part of a national project and subject to formal evaluations, but also because it had limited funding and needed to demonstrate its effectiveness as a means of securing future resources. In other case studies where a programme of ‘pilots’ or innovative interventions were being sponsored, the need for evaluation was particularly important if the project was to be mainstreamed.
29 Source: Innes, J. and Booher, D. (1999) “Consensus Building and Complex Adaptive Systems: A Framework for Evaluating Collaborative Planning”, Journal of the American Planning Association, Vol. 65 No. 4 pp. 412-23

Getting Collaboration to Work in Wales
24
ConclusionCollaborative working has taken a firm root in most policy areas. However, although it continues to prosper, the evidence of its impact and success is often unconvincing. The potential benefits of this form of working - more effective use of scarce resources and better outcomes for service users – fuel the rhetoric, but in practice, these can be outweighed by the costs associated with collaborative working including, higher transaction costs, failure to reach consensus on purpose and priorities, and problems of converting policy intention into real action.
Many of the interviewees who took part in this research study point to the complexities and problematic nature of collaborative working. They acknowledged the need to build greater collaborative capacities and capabilities to enable people and organisations to work more effectively, and the need to reflect on the considerable body of learning that already exists on policy and practice in this area.
This research study is intended to make a contribution to this learning, primarily through the experiences of collaboration in action in the form of the five case studies in Wales, but also as a result of lessons from the wider literature. Whilst it is unrealistic to be overly prescriptive in terms of ‘what works’ because of the ‘specificity’ inherent within individual forms of collaboration, the potential for achieving successful interventions will be enhanced through a greater appreciation of the factors, determinants and issues discussed above, and which all collaborations are likely to confront.