Embed Size (px)
Citation preview
T H E D U B L I N J O U R N A L OF
MEDICAL SCIENCE.
MAY 1, 1875.
PART I.
O R I G I N A L COMMUNICATIONS.
.ART. XVII.--Lessons from Surgical Practice. By B. WILLS RICHARDSON, Fellow and Examiner. Royal College of Surgeons, and Surgeon to the Adelaide Hospital, Dublin.
HARE-LIP .
In the Dublin Quarterly Journal of Medical Science for :November, 1871, I described a case of hare-lip, in which very successful results were obtained from the operation known as Langenbeck's modifica- tion of the procedure for preventing notching of the lip, attributed by many English surgeons to Malgaigne.
Langenbeck's method, according to my observation, is more suit- able for the single lateral labial cleft than for the double labial cleft with central labial tubercle, for which form of hare-lip Malgaigne's operation is better adapted.
Although the hare-lip operation by double flap is so generally attributed to Malgalgne, it should be mentioned that S~dillot gives the credit of this mode of operating to a Monsieur Cldmot, but is silent as to the date of Clgmot's description of it, nor does he say where or in what form it was published.
The late Mr. Maurice Collis, on the other hand, gives the in- vention of this double flap operation to a Mr. Samuel Smith, of Leeds, from whom "he recollected" hearing it twenty-one years previous to the date of his communication on the ~esthetic treatment
VOL. L I X . - - N O . 41, T H I R D SERIES. 2 C
378 Lessons from Surgical Practice.
of hare-lip," Mr. Smith having told Mr. Collis that he had devised it "some twenty or thirty years previously." But Mr. Collis could not say whether the description of this operation had ever been published by Mr. Smith. Under these circumstances it is probable that Malgaigne will continue to be credited with the invention of the operation.
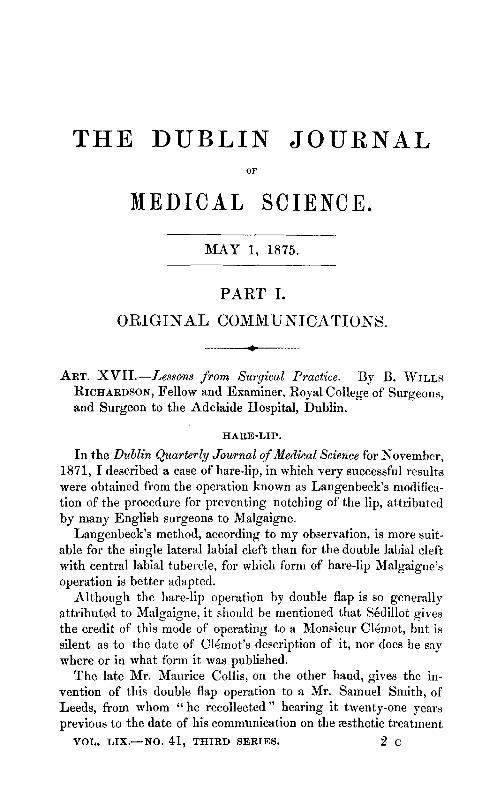
The following description of C14mot's operation shows that it is identical with that of Malgaigne, i.e., by double flap (Figs. 1, 2 and 3).
Fig. 1. Fig. 2. Fig. 3.
Diagrams of Malgaigne's operation for double hare-lip.
Fig. 1.---A B, lines of incision for the formation of the flaps. C, labial tubercle. Fig. 2.--A B, the flaps suspended by their own weight from the free edge of the lip.
C, the refreshed labial tubercle. Fig. 3.--The refreshed edges of each haft of the lip and labial tubercle secured
together--A B, the downward projection formed by the apposition of the shortened gaps. C, labial tubercle. For perspicuity suture holes are only represented.
Cl~mot (S~dillot states) recommended " the refreshing of both sides of the lip by the formation of a thin flap, commenced beyond the superior angle of the fissure, and continued from above down- wards as far as the union of the skin with the mucous rim of the free edge of the lip (Fig. 1, diagram). The two little lateral flaps thus formed fall vertically from above downward (Fig. 2, diagram), by their own weight, beyond the labial edge, their raw surfaces facing one another. They are to be united by a point of suture immediately above the mucous membrane, and their extremities are to be removed a few millimJtres lower. The free edge of the lip then forms a prominent angle (Fig. 3, diagram), the relations of which are to be maintained with threads moistened with collodion, or by means of a very fine pin; and at the end of a little time the prominence of the lip disappears by simple retraction, the result being excellent. I f the prominence is too great, part of it should be removed with scissors. The capital point is to place properly
a Dublin Quarterly Journal of Medical Science. VoL XLV., p. 292. 1868.
By MR. RICHARDSON. 379
in the same horizontal llne the two portions of skin which touch at the mucous margin of the lip. I f this last is wanting or insufficient, we are obliged, in order to prevent the notch, to invert and turn back the skin itself, and after recovery a very regular free labial edge is observed, nevertheless but little agreeable to the eye, because the skin remains white, and the mucous edge which re-appears, and continues it to the right and the left, contrasts with it, owing to its reddish vermilion coloration."
S4dillot gives a caution which should be strictly followed, lest notchlng--for the prevention of which this operation was chiefly devised--should result. "Experience," he says, " confirmed the advantages of C14mot's proceeding, but we recommend not to be too hasty in thinking that the prominence formed by the joined ends of the flaps is exaggerated. Their retraction is very considerable, and it is much better to wait a few months before excising any of them."
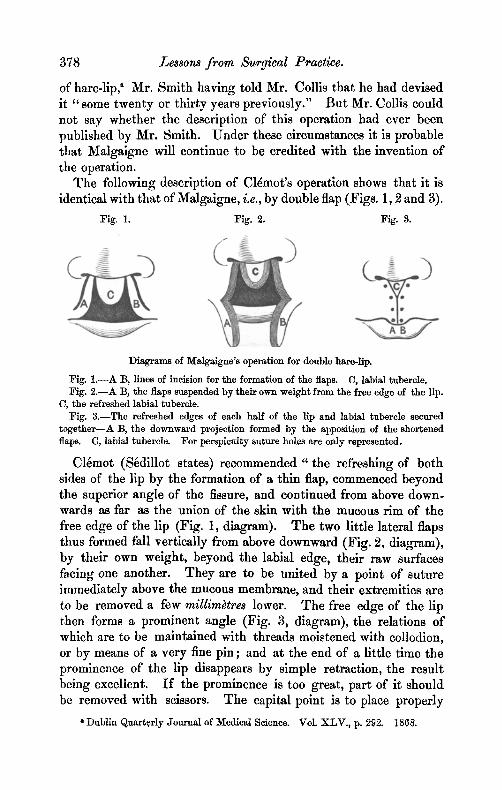
Not only does S6dillot credit Cldmot with this operation, but also he attributes to a Monsieur Mirault an operation almost identical with the modification of it--devised, according to Mr. Spencer Wells, by Langenbeek (Figs. 4, 5, and 6), whose operation I will call it in this communication.
:Fig. 4. Fig. 5. :Fig. 6.
Diagrams of Langenbeck's modification of Malgaigne's operation. Most suitable for single hare-lip.
:Fig. 4 . - -F D, line of incision convex towards the opposite half of the lip. The edge internal to F D should be removed with scissors. E, line of incision for the formation of the flap.
Fig. 5 . - -F D, the refreshed convex margin of the lip. E, the flap suspended from the.free edge of the lip.
:Fig. 6 . - -F D, the refreshed edges secured in apposition. E, the downward pro- jection formed by the end of the shortened flap. :For perspicuity suture holes are only represented.
In these figures it is supposed that the fissure exists at the left side ; but should it be at the right side the different steps of the operation illustrated in them must be reversed.
380 Lessons from Surgical Practice.
Sgdillot, with regard to it, likewise has omitted all mention of the date or the whereabouts of the original description of Mirault's operation.
Mirault, according to S6dillot, "practises on one side refreshing in the ordinary manner (Figs. 4 and 5, diagrams), then he detaches, cleanly and squarely, a small portion of the inferior and horizontal free edge of the lip. He cuts from the other side a flap similar to those of M. C16mot (Figs. 4 and 5, diagrams) adapts it to the wound opposite in order to appreciate its length clearly, and after having cut off the superfluous portion, if necessary, applies it transversely and fixes it underneath the other half of the llp, of which it constitutes the free edge (Fig. 6, diagram). ~
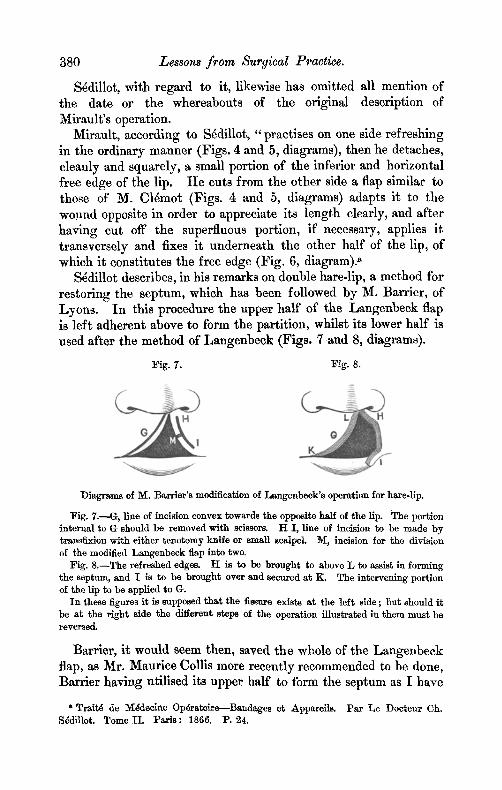
S6dillot describes, in his remarks on double hare-lip, a method for restoring the septum, which has been followed by M. Barrier, of Lyons. In this procedure the upper half of the Langenbeck flap is left adherent above to form the partition, whilst its lower half is used after the method of Langenbeck (Figs. 7 and 8, diagrams).
Fig. 7. Fig. s.
Diagrams of 1~I. Barrler's modification of Langenbeck's operation for hare-lip.
Fig. 7.---G, llne of incision convex towards the opposite half of the lip. The portion internal to G should be removed with scissors. H I, line of incision to be made by transfixion with either tenotomy knife or small sc~Ipel, t~, incision for the division of the modified Langenbeck flap into two.
Fig. 8 . - -The refreshed edges. H is to be brought to above L to assist in forming the septum, and I is to be brought over and secured at K. The intervening portion of the lip to be applied to G.
In these figures it is supposed that the fissure exists at the left side ; l~ut should it be at the right side the different steps of the operation illustrated in them must be reversed.
Barrier, it would seem then, saved the whole of the Langenbeck flap, as Mr. Maurice Collis more recently recommended to be done, Barrier having utilised its upper half to form the septum as I have
�9 Trait4 de M4decine Op4ratoire---Bandages et Apparelis. Pa r Le Doeteur Ch. S~dillot. Tome II. Par is : 1866. P. 24.
By MR. RICHARDSON. 381
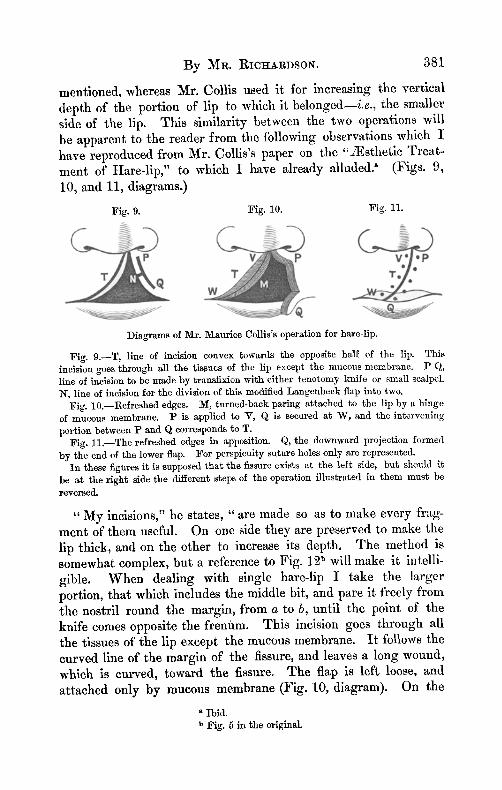
mentioned, whereas Mr. Collis used it for increasing the vertical depth of the portion of lip to which it belonged--i.e., the smaller side of the lip. This similarity between the two operations will be apparent to the reader from the following observations which I have reproduced from Mr. Collis's paper on the "zEsthetie Treat.- ment of Hare-lip," to which I have already alluded2 (Figs. 9, 10, and 11, diagrams.)
Fig. 9. Fig. 10. Fig. 11.
Diagrams of Mr. Maurice Collis's operation for hare-lip.
Fig. 9.--T, line of incision convex towards the opposite half of the lip. This incision goes through all the tissues of the lip except the mucous membrane. P Q, line of incision to be made by transfixion with either tenotomy kifife or small scalpel. N, line of incision for the division of this modified Langenbeck flap into two.
Fig. 10.--Refreshed edges. M, turned-back paring attached to the lip by a hinge of mucous membrane. P is applied to V, Q is secured at W, and the intervening portion between P and Q corresponds to T.
Fig. 11.--The refreshed edges in apposition. Q, the downward projection formed by the end of the lower flap. For perspicuity suture holes only are represented.
In these figures it is supposed that the fissure exists at the left side, but should it be at the right side the different steps of the operation illustrated in them must be reversed.
" M y incisions," he states, "are made so as to make every frag- ment of them useful. On one side they are preserved to make the lip thick, and on the other to increase its depth. The method is somewhat complex, but a reference to Fig. 12 b will make it intelli- gible. When dealing with single hare-lip I take the larger portion, that which includes the middle bit, and pare it freely from the nostril round the margin, from a to b, until the point of the knife comes opposite the frenfim. This incision goes through all the tissues of the lip except the mucous membrane. I t follows the curved line of the margin of the fissure, and leaves a long wound, which is curved, toward the fissure. The flap is left loose, and attached only by mucous membrane (Fig. 10, diagram). On the
Ibid. Fig. 5 in the original.
382 Lessons from Surgical Practice.
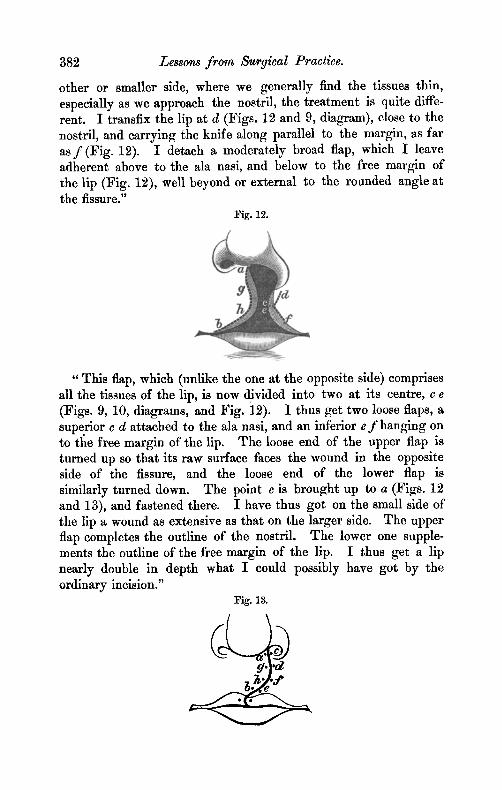
other or smaller side, where we generally find the tissues thin, especially as we approach the nostril, the treatment is quite diffe- rent. I transfix the lip at d (Figs. 12 and 9, diagram), close to the nostril, and carrying the knife along parallel to the margin, as far as f (Fig. 12). I detach a moderately broad flap, which I leave adherent above to the ala nasi, and below to the free margin of the lip (Fig. 12), well beyond or external to the rounded angle at the fissure."
Fig. 12.
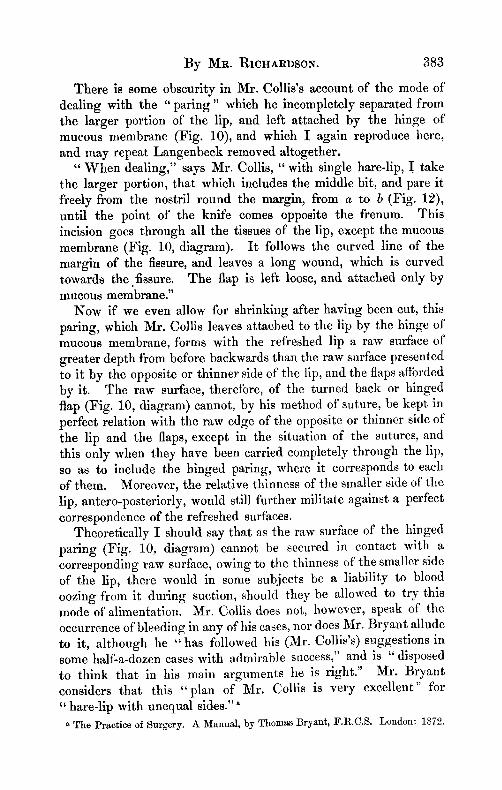
"This flap, which (unlike the one at the opposite side) comprises all the tissues of the lip, is now divided into two at its centre, c e (Figs. 9, 10, diagrams, and Fig. i2). I thus get two loose flaps, a superior c d attached to the ala nasi, and an inferior e f hanging on to the free margin of the lip. The loose end of the upper flap is turned up so that its raw surface faces the wound in the opposite side of the fissure, and the loose end of the lower flap is similarly turned down. The point c is brought up to a (Figs. 12 and 13), and fastened there. I have thus got on the small side of the lip a wound as extensive as that on the larger side. The upper flap completes the outline of the nostril. The lower one supple- ments the outline of the free margin of the lip. I thus get a lip nearly double in depth what I could possibly have got by the ordinary incision."
:Fig. 13.
~r
By MR. RICHARDSON. 383
There is some obscurity in Mr. Collis's account of the mode of dealing with the "paring" which he incompletely separated from the larger portion of the lip, and left attached by the hinge of mucous membrane (Fig. 10), and which I again reproduce here, and may repeat Langenbeck removed altogether.
" When dealing," says Mr. Collis, "with single hare-llp, ! take the larger portion, that which includes the middle bit, and pare it freely from the nostril round the margin, from a to b (Fig. 12), until the point of the knife comes opposite the frenum. This incision goes through all the tissues of the lip, except the mucous membrane (Fig. 10, diagram). I t follows the curved line of the margin of the fissure, and leaves a long wound, which is curved towards the fissure. The flap is left loose, and attached only by mucous membrane."
Now if we even allow for shrinking after having been cut, this paring, which Mr. Collis leaves attached to the lip by the hinge of mucous membrane, forms with the refreshed lip a raw surface of greater depth from before backwards than the raw surface presented to it by the opposite or thinner side of" the lip, and the flaps afforded by it. The raw surface, theretbre, of the turned back or hinged flap (:Fig. 10, diagram) cannot, by his method of suture, be kept. in perfect relation with the raw edge of the opposite or thinner side of the lip and the flaps, except in the situation of the sutures, and this only when they have been carried completely through the lip, so as to include the hinged paring, where it corresponds to each of them. Moreover, the relative thinness of the smaller side of the lip, antero-posteriorly, would still further militate against a perfect correspondence of the refreshed surfaces.
Theoretically I should say that as the raw surface of the hinged paring (Fig. 10, diagram) cannot be secured in contact with a corresponding raw surface, owing to the thinness of the smaller side of the lip, there would in some subjects be a liability to blood oozing from it during suction, should they be allowed to try this mode of alimentation. Mr. Collis does not, however, speak of the occurrence of bleeding in any of his cases, nor does Mr. Bryant allude to it, although he "has followed his (Mr. Collis's)suggestions in some half-a-dozen cases with admirable success," and is "disposed to think that in his main arguments he is right." Mr. Bryant considers that this "plan of Mr. Collis is very excellent" for "hare-lip with unequal sides. ''a
* The Practice of Surgery. A Manual, by Thomas Bryant, F.I~.C.S. London: 1872.
384 Lessons from Surgical Practwe.
Having made these prefatory remarks, chiefly for the information of the student, I will now give the particulars of two cases in which I performed Langenbeck's operation with very favourable results, the downward projection of Cupid's bow being very well supple- mented by the lower end of the flap.
Single Hare-llp, complicated with Cleft of both Palates.
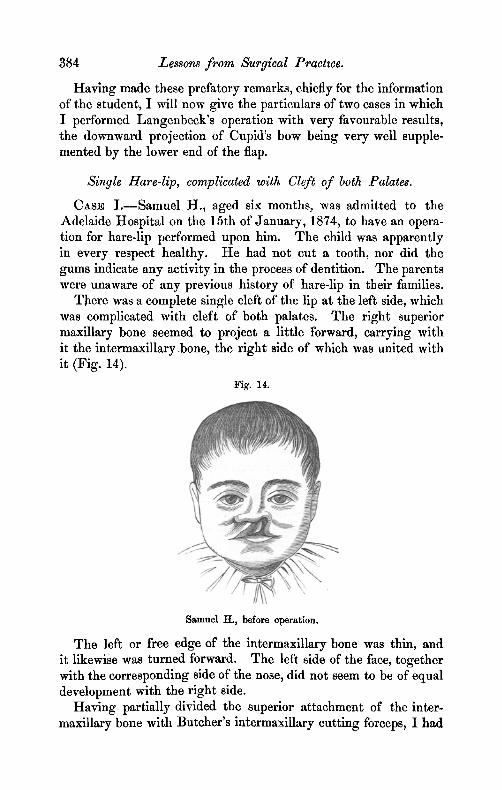
CASE L--Samuel H., aged six months, was admitted to the Adelaide Hospital on the 15th of January, 1874, to have an opera- tion for hare-lip performed upon him. The child was apparently in every respect healthy. He had not cut a tooth, nor did the gums indicate any activity in the process of dentition. The parents were unaware of any previous history of hare-lip in their families.
There was a complete single cleft of the lip at the left side, which was complicated with cleft of both palates. The right superior maxillary bone seemed to project a little forward, carrying with it the intermaxillary ,bone, the right side of which was united with it (Fig. 14).
:Fig. 14.
Samuel H. before operation.
The left or free edge of the intermaxillary bone was thin, and it likewise was turned forward. The left side of the face, together with the corresponding side of the nose, did not seem to be of equal development with the right side.
Having partially divided the superior attachment of the inter- maxillary bone with Butcher's intermaxillary cutting forceps, I had
By MR. RICHARDSON. 385
no difficulty in semi-rotating and at the same time dislocating it backwards into the gap that. existed between its free edge and the left maxilla.
I then dealt with the soft parts after Langenbeck's modification of Malgaigne's operation, the right or larger side of the lip having been refreshed in the manner I have mentioned, and the flap having been formed at the opposite or smaller side of the lip (Figs. 4 and 5). The flap was then allowed to turn down (Fig. 5), and remained suspended by undivided tissues at the free margin of the lip until the pins were inserted. Two very fine hare-lip pins, with twisted suture, were found sufficient to mains the chief portion of the refreshed surfaces or edges in accurate contact. The flap was then shortened by the removal of as much of its free end as would enable the remainder to be accurately adapted to the lowermost portion of the curved raw surface prepared for it, with which, finally, it was secured in contact by means of a couple of very fine silk interrupted sutures (Fig. 6).
Hainsby's truss was next applied, and in a few hours the surface of the lip was painted with thick collodion.
Collis suggests that the collodion should be made very thick, as the " ether in thin collodion acts injuriously on the healing process." This, I believe to be good advice, for thin collodion is apt to in- sinuate itself between the refreshed edges, and may, as he suggests, act injuriously. Indeed, even when of thick consistence, I do not advise its use until the refreshed edges have had time to aggluti- nate with one another. Although non-union after hare-lip opera- tior~s had been observed so long prior to the discovery of collodion, nevertheless it is probable that its insinuation between the refreshed edges might, in a person of low vitality, intercept the healing process.
When placed in bed, the child was given some white wine whey, and afterwards a hydrate of chloral draught, the whey to be given at regular intervals, and the draught to be repeated if necessary for producing sleep.
31st January.---I removed the lower pin, and union appeared firm. The truss was continued, and as the child seemed to suffer from colicky pains, it was given some carminative mixture.
1st February.--I removed the second pin, but left the silk thread in position, being so firmly glued to the lip by means of the collodion ; union appeared perfect; truss continued.
4th February.--The silk thread having partially nnglued was
386 Lessons from Surgical Practice.
removed, as well as the fine silk interrupted sutures which retained the end of the flap in position.
5th March.--The truss was worn up to this date. The anterior portion of the intermaxillary cleft seemed to have completely closed.
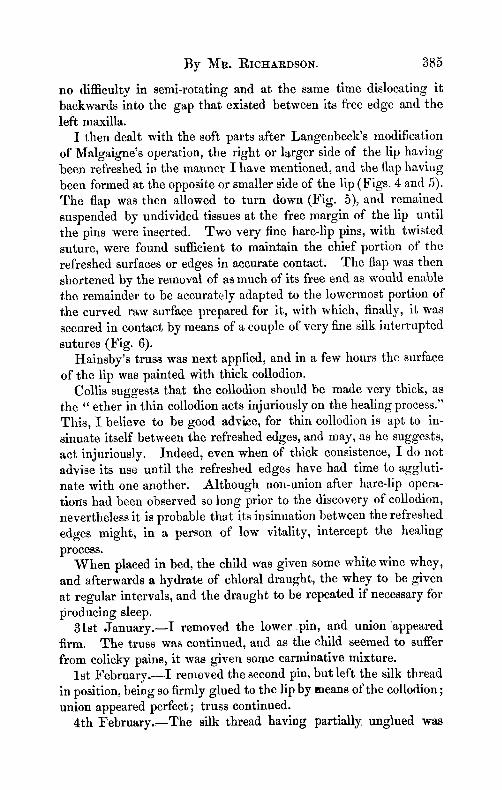
Any further reports of the case are unnecessary, for with the exception of a slight catarrhal attack, all went on well, and I was enabled to allow the child to be brought home on the 27th of March. A day or two previous to this date, our hospital surgeon dentist, Mr. William Pearsall, kindly took an excellent likeness of it in water eolours, from which the following figure (Fig. 15) was engraved. I t accurately represents the appearance of the lip, and shows the central papilla formed by the end of the flap, which was brought over from the smaller side of the lip.
Fig. 15.
Samuel H., after operation.
Single Hare-lip, complicated with Fissures of both Palates. Intra- uterine Union of the Lip with the right side of the Labial Tubercle, the case having beeu originally a Double Hare-lip.
CAs~ I I . - - J . S., aged five months, was brought to me to have the operation for hare-lip per~rmed upon it. There was no history of hare-lip in the family.
To my mind there was sufficlently strong evidence to support the inference that this hare-lip had been double in early foetal life, with both labial and osseous tubercles, the right edges of which had united, during some pgrtion of the child's intra-uterine existence, with those parts with which they should be normally
By MR. RICHARDSON. 387
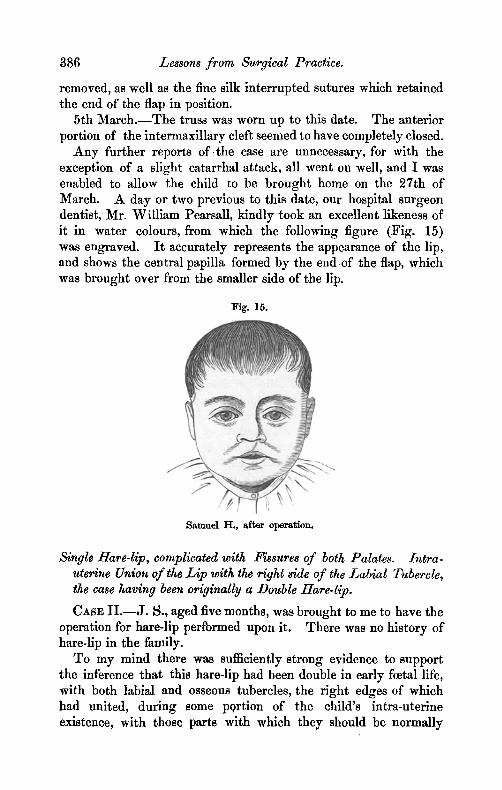
unlted---viz., the right portion of the lip, and the right superior maxilla. I base this opinion upon the following evidence :--The right side or edge of the labial tubercle, or central portion of the lip, furrowed with the filtrum, was united by means of a cicatrieial- looking structure to the corresponding edge of the right or larger portion of the lip. This cicatriclal-looking union was situated at the bottom of a relatively deep groove, which extended from the right naris above to a deep notch inferiorly, where the uniting medium terminated (Fig. 16). In fact, as far as this notch was con- cerned, nature was by no means successful in preventing deformity, for I have seldom seen so deep a notch left after a partially unsuccessful surgical operation for hare-lip.
Fig. 16.
J. S., before operation.
The left edge of the intcrmaxillary bone, which was free, was turned slightly forward, and was separated from the left superior maxilla by the anterior termination of the palatal cleft.
The child being apparently healthy and strong, I performed, on the 6th June, 1874, Langenbeck's operation for hare-lip (Figs. 4, 5, and 6), in the presence of my colleague, Dr. James Little, and of Mr. John Morgan. An anaesthetic was not administered.
The upper attachment of the intermaxillary bone was notched with Butcher's intermaxillary cutting forceps, and the bone was then partially dislocated backwards, so as to occupy the gap that existed between its free edge and the left maxilla. A little of this edge, however, had to be previously removed, the inter- maxillary bone being too wide for the space destined for its
388 .Lessons from Surgical Practice.
reception when dislocated. The right or larger portion of the lip, together with the left edge of the labial tubercle, were pared with scissors, so as to refresh their edges (Figs. 4 and 5), care having been taken to remove the apex of the tubercle, with the view of obliterating the notch which existed between its apex and the margin of the lip (Fig. 16).
The flap was then formed, at the left side of the lip, with a short narrow-bladed knife (Figs. 4 and 5); but this was s(~ badly developed, vertically, that the whole flap was only of sufficient length for complete adaptation to the curved refreshed edge of the right lip, and, therefore, none of it was removed.
The upper three-fourths of the refreshed edges were brought and maintained together with two fine hare-lip pins, the upper pin having been inserted as near the opening of the naris as possible. Inferiorly the free end of the flap was secured in position with two very fine silk interrupted sutures, inserted with curved needles of the smallest calibre made (Fig. 6).
But little blood was lost during the opera~ion. When this was completed, Hainsby's truss was applied, and the baby was ordered a teaspoonful of a hydrate of chloral mixture every hour until sleep supervened. A teaspoonful of a brandy and milk mixture was also to be given occasionally, should it appear exhausted.
7th June.--Only three spoonfuls of the hydrate of chloral mixture had been given when sleep commenced.
8th June . - -The child seemed to suffer from occasional tormina, and was ordered a carminative mixture composed of compound tincture of rhubarb, calcined magnesia, aromatic spirit of ammonia, tincture of opium, with glycerine and water; Hainsby's truss was continued.
9th June . - - I removed the lower pin, and union in the lower half of the lip was found to be perfect; the collodion and Hainsby's truss were continued~
10th June . - - I removed the remaining pin; union in'the upper part of the lip perfect likewise; collodion and Hainsby's truss were continued; the threads of the twisted sutures, being firmly glued to the lip, were not disturbed.
17th June. - -The collodion separated from the llp, and carried the suture silk with it; lip perfectly united, even into the left naris, and inferiorly the extreme end of the Langenbeck flap had united perfectly with the lowermost portion of the refreshed curved edge of the right half of the lip, including the refreshed apex of the
By MR. RICHARDSON. 389
labial tubercle--consequently the whole lip was of equal vertical depth. Some zinc cream was directed to be applied to the lip, and Halnsby's truss to be continued.
18th June.--Removed the fine silk interrupted sutures that secured the end of the Langenbeck flaps in position; use of Hainsby's truss continued.
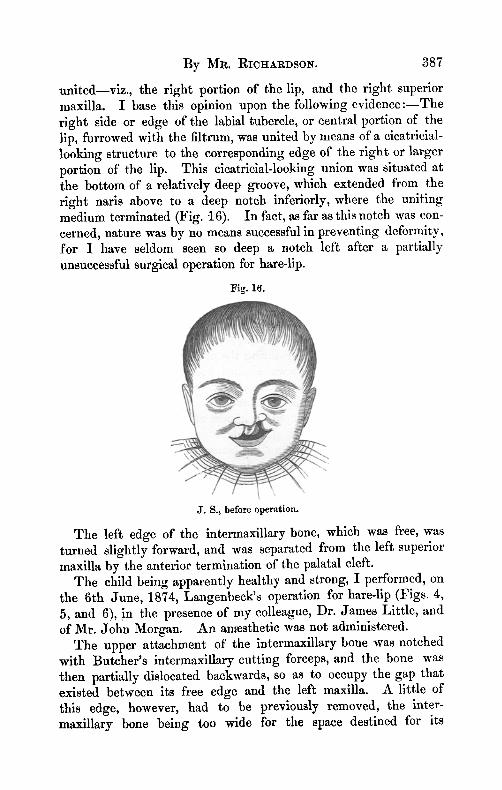
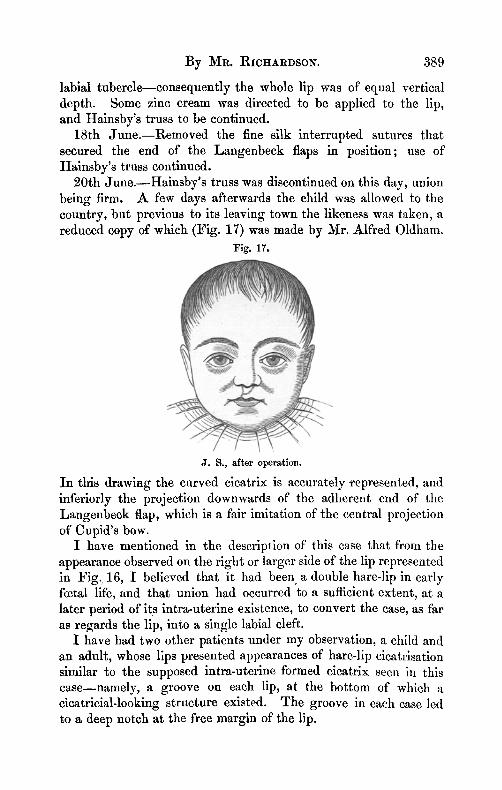
20th June.--Hainsby's truss was discontinued on this day, union being firm. A few days afterwards the child was allowed to the country, but previous to its leaving town the likeness was taken, a reduced copy of which (Fig. 17) was made by Mr. Alfred Oldham.
Fig. 17.
J. S.~ after operation.
In tlris drawing the curved cicatrix is accurately represented, and inferiorly the projection downwards of the adherent end of the Langenbeck flap, which is a fair imitation of the central projection of Cupid's bow.
I have mentioned in the description of this case that from the appearance observed on the right or larger side of the lip represented in Fig. 16, I believed that it had been a double hare-lip in early foetal life, and that union had occurred to a sufficient extent, at a later period of its intra-uterine existence, to convert the case, as far as regards the lip, into a single labial cleft.
I have had two other patients under my observation, a child and an adult, whose lips presented appearances of hare-lip cicatrisation similar to the supposed intra-uterine formed cicatrix seen in this case--namely, a groove on each lip, at the bottom of which a cicatriclal-looking structure existed. The groove in each case led to a deep notch at the free margin of the lip.
390 Lessons from Surgical Practice.
The mother of the child was most positive that u surgical operation had never been performed upon it, and the adult was equally positive that she, also, had never been operated upon for hare-lip. In neither case was there any mark of suture cicatrisation.
When we recollect, however, that there are many people with minds so constituted that they would probably consider it degrading to admit that they themselves or their children had ever been born with cleft-lip, stronger evidence than mere verbal evidence should be required in the endeavour to decide a question of this kind. Such additional proof was afforded by the case represented in Figs. 16 and 17, in which a surgical operation could not have been performed previous to the child coming under my observation, and in which the appearances of a partial intra-uterine union could hardly have been more decisive.
This question is not altogether a new one, for Mr. Spencer Wells, in the article on Hare-lip, in the last edition of " Cooper's Surgical Dictionary," mentions that Wagner had seen two cases in which union of the labial cleft took place within the uterine cavity. Dr. P. Frank, who saw one of these cases, informed Mr. Wells that it was on the left side of the upper lip union had taken place, with a distinct red cicatrix, and, as in my case (Fig. 16), there was a deep indentation of the free margin--which, as Mr. Wells so truly observes, it is our object to avoid in operative proceedures.
The foregoing observations, I needscarcely remind the reader, refer merely to Malgaigne's operation for hare-lip, and to two of its most important modifications. They are to a great extent a reproduction of a lecture I delivered in the Adelaide Hospital during the session of 1873-4, on those operations which I generally practise, having found Malgaigne's and Langenbeck's procedures thoroughly effective in forming a good vertically deep lip, without tendency to notching.
In conclusion, let me observe that I have found the scissors the most handy instrument for forming the convex curved refreshed edge of the larger portion of the lip, and a small nan'ow-bladed scalpel, or a tenotomy knife, the proper instrument for eflttlng the flap in the Langenbeck operation. But in the Malgaigne operation itself, when practised for double hare-lip with labial tubercle, the scissors should be used for refreshing the edges of the latter only.
The scissors in ordinary use for hare-lip operations are unneces- sarily large. A short-bladed and short-handled scissors will be found a much more manageable instrument than it.
The fingers of the operator are sufficient for fixing the larger
Notes on some Diseases of the Skin. 391
portion of the lip in the Langenbeck operation. But a small hook should be used for steadying the portion of lip which supplies the flap in either the Langenbeck or Malgaigne method.
Should the twisted suture be practised for securing the refreshed edges of the lip together, the ingeniously devised needle-guard of Mr. Tyrrell, delineated and described in the number of this Journal for September, 1874 (Vol. LVII I . , p. 223), will be found a useful appliance, and one calculated to afford us some assistance in the management of a hare-lip case, and to spare the patient the additional pain caused by the withdrawing of the broken end of the needle through the flesh, particularly when it has been a little bent by the action of the cutting pliers, which is very common when the needle has not been properly tempered.
ART. X V I I I . - - N o t e s on some Diseases of the Skin--(~t) Favus; (b) Erythema multiforme. ~ By WALTER G. S M I T H , M.D.; Univ. Dubl. ; Fellow and Censor of the King and Queen's College of Physicians ; Assistant Physician to the Adelaide Hospital:
I . FAVUS OF T H E H E A D , TRUNK~ LIMBS, AND NAILS.
I I . F A V U S OF T H E E P I D E R M I S ALONE.
I I I . FAVUS OF T H E E P I D E R M I S ALONE.
IV. E R Y T H E M A M U L T I F O R M E .
I PROPOSE to bring before the Society this evening the notes of a few cases which derive their interest in part from their comparative rarity, but chiefly as exhibiting some features in respect of diagnosis which are of practical consequence. I shall first speak of favus, or, as it is now called, tinea favosa.
A curious point in the natural history o f favus is its very unequal distribution in the limited area of Great Britain and Ireland, as tested by statistics collected in their respective capitals. Thus, in Scotland, Dr. M'Call Anderson met with it 160 times in 11,000 cases--i.e., about 1�89 per cent. In England it is extremely rare, is seldom seen except among the poorest classes, and even at the special hospitals in London not more than two or three cases are observed in a year. Indeed, Dr. Dyce Duckworth, during four years, out of 4,000 or 5,000 cases of skin disease, had met with only four eases of ikvus--/.e., one in 1,000. Among 3,000 private patients, Mr. Erasmus Wilson recognised it twice only. In Dublin I
�9 Read before the Medical Society of the College of Physicians, April 14, 1875. [For the discussion on this paper, see page 455.]