Embed Size (px)
DESCRIPTION
emedicine.medscape.com/article/220563-overview
Citation preview

10/28/2015 Leptospirosis Workup: Approach Considerations, Culture, Microscopic Agglutination Testing
http://emedicine.medscape.com/article/220563workup 1/7
Leptospirosis WorkupAuthor: Sandra G Gompf, MD, FACP, FIDSA; Chief Editor: Michael Stuart Bronze, MD more...
Updated: Apr 14, 2015
Approach ConsiderationsLeptospires grow slowly in culture, and recovery rates are low. Serologic tests areavailable only in specialized laboratories, and the sensitivity of acute serologic testsis low. Consequently, those tests should not be the basis on which treatment isinitiated. In a patient with compatible symptoms and a plausible exposure history,empiric therapy should be started.
Laboratory studies are used for two purposes: to confirm the diagnosis and todetermine the extent of organ involvement and severity of complications. Laboratoryconfirmation of leptospirosis can be accomplished through isolation of the pathogenor by serologic testing.
Isolation of the leptospires from human tissue or body fluids is the criterionstandard. Consultation with the local microbiology laboratory is essential, becauseprocessing requires specialized techniques. Urine is the most reliable body fluid tostudy because the urine contains leptospires from the onset of clinical symptomsuntil at least the third week of infection.
Other body fluids contain the organism, but the window of opportunity to isolatethem is shorter. Blood and CSF may produce positive cultures during the first 710days of symptoms.
Tissues (ie, liver, muscle, kidney, skin, eyes) are also sources of identification of theleptospires but are obviously more complicated to acquire. Isolation of leptospirescan be difficult and time consuming, involving reference laboratories and oftentaking several months to complete.
More often, paired acute and convalescent serum specimens are used to confirmthe diagnosis. Again, this is a delayed means of confirmation because the acutesera are collected 12 weeks after onset of symptoms, and the convalescent seraare collected 2 weeks afterward.
Antileptospire antibodies in these samples are detected using the microscopicagglutination test (MAT). The Centers for Disease Control and Prevention (CDC)laboratory in Atlanta, Georgia, performs the MAT using 23 leptospire antigens. A 4fold rise in MAT titer between acute and convalescent sera with any of theseantigens confirms the diagnosis of leptospirosis.
Faster laboratory methods may strongly suggest the diagnosis of leptospirosis, butthey may be no more readily available than the CDC laboratory in Atlanta. A singleMAT titer of 1:800 on any sera or identification of spirochetes on darkfieldmicroscopy, when accompanied by the appropriate clinical scenario, is stronglysuggestive.
In suspected leptospirosis, further laboratory studies should be routinely performedto determine the extent and severity of organ involvement after the acute phase ofillness. A complete blood cell count (CBC) is necessary. Findings on generallaboratory studies are as follows:
In patients with mild disease, elevated erythrocyte sedimentation rates andperipheral leukocytosis (3,00026,000 x 109/L) with a left shift are notedSignificant anemia due to pulmonary and gastrointestinal hemorrhage canoccurThe platelet count may be diminished as a component of disseminatedintravascular coagulation (DIC)levels of blood urea nitrogen and serum creatinine may be profoundlyelevated in the anuric or oliguric phaseSerum creatine kinase levels (MM fraction) are often elevated in patientswith muscular involvement.Coagulation times may be prolonged in patients with hepatic dysfunctionand/or DIC On liver function testing, serum bilirubin levels elevate as part ofthe obstructive disease due to capillaritis in the liver. levels of hepatocellulartransaminases are elevated less often and less significantly (usually < 200U/L). Jaundice and bilirubinemia disproportional to hepatocellular damage iscommon in leptospirosis; alkaline phosphatase levels may be elevated 10fold.
On urinalysis, proteinuria may be present. Leukocytes, erythrocytes, hyaline casts,and granular casts may be present in the urinary sediment.
Analysis of the CSF is useful only in excluding other causes of bacterial meningitis.When the CNS becomes involved in leptospirosis, polymorphonuclear leukocytesinitially predominate and are later replaced by monocytes. CSF protein may benormal or elevated, whereas glucose levels remain normal. CSF pressure is normal,but a lumbar puncture can relieve the headache. Leptospires are routinely isolatedfrom the CSF, but this finding does not change management of the disease.
Imaging studies are useful in determining the extent and severity of organinvolvement. This may include chest radiography to evaluate lung disease andbiliary tract ultrasonography in suspected acalculous cholecystitis.
Electrocardiographic (ECG) abnormalities are common during the leptospiremicphase of Weil syndrome. In severe cases, congestive heart failure and cardiogenic

10/28/2015 Leptospirosis Workup: Approach Considerations, Culture, Microscopic Agglutination Testing
http://emedicine.medscape.com/article/220563workup 2/7
shock may occur.
CultureIsolating the organism by culture allows definitive diagnosis. Leptospires remainviable in anticoagulated blood for as long as 11 days; hence, specimens can bemailed to a reference laboratory for culture. The infecting serovar can be isolatedonly by culture.
Blood cultures may be negative if drawn too early or too late. Leptospires may notbe detected in the blood until 4 days after the onset of symptoms (714 d afterexposure). Once the immune system is activated, blood cultures may again becomenegative. Leptospires may be isolated from the cerebrospinal fluid (CSF) within thefirst 10 days.
Leptospires may be isolated from the urine for several weeks after the initialinfection. In some patients, urine cultures may remain positive for months or yearsafter the onset of illness. Positive urine cultures may take as long as 8 weeks togrow.
Microscopic Agglutination TestingMicroscopic agglutination testing (MAT) uses a battery of antigens taken fromcommon (frequently locally endemic) leptospire serovars. MAT is available only atreference laboratories, such as the Centers for Disease Control and Prevention(CDC).
In a patient with clinical findings consistent with the disease, a single titer exceeding1:200 or serial titers exceeding 1:100 suggest leptospirosis; however, neither isdiagnostic. A 4fold rise in titer between acute and convalescent specimens isconsidered a positive result. The antibody response does not reach detectable levelsuntil the second week of illness, and it can be affected by treatment.
Falsenegative MAT findings may result from testing a single specimen obtainedbefore the immune phase of disease. Test accuracy is also affected by appropriateselection of antigens for the battery, necessitating discussion with the laboratoryabout which serovars are suspected or predominate in the region where the caseoriginated. Falsepositive MAT results may occur with cases of Legionella infection,Lyme disease, and syphilis.
Other TestsScreening tests for leptospirosis, which are easy to perform and provide resultsrelatively rapidly, include the macroscopic slide agglutination test, the Patocslideagglutination test, the microcapsule agglutination test, latex agglutination tests,dipstick tests, and the indirect hemagglutination test. Confirmation of screening testresults (positive or negative) is advisable, however, preferably with MAT.[40]
An immunoglobulin M (IgM) enzymelinked immunoabsorbent assay (ELISA) hasbeen developed. The ELISA uses a broadly reactive antigen and is a standardserologic procedure, as is the MAT.[41] Because it detects IgM, it may be useful fordiagnosis of new infections within 35 days. Positive results should be referred forconfirmatory testing.
Nucleic acid amplification (polymerase chain reaction [PCR])–based techniqueshave been developed to diagnose leptospirosis. PCR can confirm the diagnosisrapidly during the early phase of the disease, when leptospires may be present andbefore antibody titers are detectable, but it requires adequate infrastructure such asappropriate equipment, laboratory space, and skilled personnel. In addition, PCRbased techniques are unable to identify the infecting serovar, which reduce theirepidemiologic and public health value.
Darkfield examination of blood or urine has been used to identify leptospires.However, this technique cannot be recommended, as it frequently leads tomisdiagnosis.
Chest RadiographyThe most common abnormality on chest radiography is bilateral diffuse airspacedisease. Chest radiography may also reveal cardiomegaly and pulmonary edemadue to myocarditis. In patients with alveolar hemorrhage due to pulmonarycapillaritis, the lung parenchyma may contain multiple patchy infiltrates.
Histologic FindingsShortly after inoculation and during the incubation period, leptospires activelyreplicate in the liver. The leptospires then disseminate throughout the body andinfect multiple tissues.
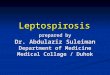
Silver staining and immunofluorescence can identify leptospires in the liver, spleen,kidney, CNS, muscles, and heart. During the acute phase of leptospirosis, histologyreveals these organisms without much inflammatory infiltrate. In addition to thefinding of leptospires during histologic examination, the pathologic effects ofleptospiral toxins are also apparent. See the image below.

10/28/2015 Leptospirosis Workup: Approach Considerations, Culture, Microscopic Agglutination Testing
http://emedicine.medscape.com/article/220563workup 3/7
Silver stain, liver, fatal human leptospirosis. (This image is in the public domain and thus free ofany copyright restrictions. Courtesy of the Centers for Disease Control/Dr. Martin Hicklin)
Leptospirosis may be seen as an infective systemic vasculitis.[18] Leptospiral toxinsbreak down endothelial cell membranes of capillaries. This toxinmediated processallows for extravasation of blood and leptospires from blood vessels into thesupported parenchyma. Secondarily, because the capillaries are no longerfunctional, ischemia and cell death can occur. Later in infection, mononuclear cellspredominate in the areas of this focal cell necrosis.
Leptospires can be identified in immunologically privileged sites, such as renaltubules, CNS, and the anterior chamber of the eyes, for weeks to months after theinitial infection. In nonhuman animals, the intended hosts of infection, theleptospires establish residence in these immunologically privileged sites. Providedthat the animal survives the initial infection, a chronic carrier state is thenestablished, and histology reveals leptospires at these sites for years after initialinfection.
Treatment & Management
Contributor Information and DisclosuresAuthorSandra G Gompf, MD, FACP, FIDSA Associate Professor of Infectious Diseases and International Medicine,University of South Florida College of Medicine; Chief, Infectious Diseases Section, Director, OccupationalHealth and Infection Control Programs, James A Haley Veterans Hospital
Sandra G Gompf, MD, FACP, FIDSA is a member of the following medical societies: American College ofPhysicians, Infectious Diseases Society of America
Disclosure: Nothing to disclose.
Coauthor(s)Judith GreenMcKenzie, MD, MPH, FACP, FACOEM Associate Professor, Director of Clinical Practice,Occupational Medicine Residency Director, University of Pennsylvania School of Medicine
Judith GreenMcKenzie, MD, MPH, FACP, FACOEM is a member of the following medical societies: AmericanCollege of Physicians, American College of Preventive Medicine, National Medical Association, AmericanCollege of Occupational and Environmental Medicine
Disclosure: Nothing to disclose.
Ana Paula Velez, MD Assistant Professor of Medicine, Division of Infectious Disease and InternationalMedicine, University of South Florida College of Medicine and James A Haley Veterans Affairs Medical Center;Attending Physician, Moffitt Cancer Center
Ana Paula Velez, MD is a member of the following medical societies: American College of PhysiciansAmericanSociety of Internal Medicine, American Medical Association, Infectious Diseases Society of America
Disclosure: Nothing to disclose.
Chief EditorMichael Stuart Bronze, MD David Ross Boyd Professor and Chairman, Department of Medicine, Stewart GWolf Endowed Chair in Internal Medicine, Department of Medicine, University of Oklahoma Health ScienceCenter; Master of the American College of Physicians; Fellow, Infectious Diseases Society of America
Michael Stuart Bronze, MD is a member of the following medical societies: Alpha Omega Alpha, AmericanMedical Association, Oklahoma State Medical Association, Southern Society for Clinical Investigation,Association of Professors of Medicine, American College of Physicians, Infectious Diseases Society of America
Disclosure: Nothing to disclose.
AcknowledgementsDenise Demers, MD, FAAP Assistant Professor of Pediatrics, Uniformed Services University of the HealthSciences; Attending Physician, Division of Pediatric Infectious Diseases, Department of Pediatrics, Tripler ArmyMedical Center
Disclosure: Nothing to disclose.
Juan D Diaz, DO Fellow in Infectious Diseases, University of South Florida College of Medicine, Tampa GeneralHospital, and James A Haley Veterans Hospital
Disclosure: Nothing to disclose.
Joseph Domachowske, MD Professor of Pediatrics, Microbiology and Immunology, Department of Pediatrics,Division of Infectious Diseases, State University of New York Upstate Medical University
Joseph Domachowske, MD is a member of the following medical societies: Alpha Omega Alpha, AmericanAcademy of Pediatrics, American Society for Microbiology, Infectious Diseases Society of America, PediatricInfectious Diseases Society, and Phi Beta Kappa

10/28/2015 Leptospirosis Workup: Approach Considerations, Culture, Microscopic Agglutination Testing
http://emedicine.medscape.com/article/220563workup 4/7
Disclosure: Nothing to disclose.
Patrick W Hickey, MD, FAAP Assistant Professor of Pediatrics and Preventive Medicine, Uniformed ServicesUniversity of the Health Sciences; Consulting Staff, Department of Pediatrics, Division of Pediatric InfectiousDisease, Walter Reed Army Medical Center
Patrick W Hickey, MD, FAAP is a member of the following medical societies: Alpha Omega Alpha, AmericanAcademy of Pediatrics, American Society of Tropical Medicine and Hygiene, Infectious Diseases Society ofAmerica, International Society of Travel Medicine, and Pediatric Infectious Diseases Society
Disclosure: Nothing to disclose.
Edmond A Hooker II, MD, DrPH, FAAEM Assistant Professor, Department of Emergency Medicine, Universityof Cincinnati College of Medicine; Associate Professor, Department of Health Services Administration, XavierUniversity
Edmond A Hooker II, MD, DrPH, FAAEM is a member of the following medical societies: American Academy ofEmergency Medicine, American Public Health Association, Society for Academic Emergency Medicine, andSouthern Medical Association
Disclosure: Nothing to disclose.
Matthew R Jezior, MD Fellow, Department of Cardiology, Walter Reed Medical Center
Disclosure: Nothing to disclose.
Maria D Mileno, MD Associate Professor of Medicine, Division of Infectious Diseases, The Warren AlpertMedical School of Brown University
Maria D Mileno, MD is a member of the following medical societies: Alpha Omega Alpha, American College ofPhysicians, American Society of Tropical Medicine and Hygiene, Infectious Diseases Society of America,International Society of Travel Medicine, and Sigma Xi
Disclosure: Nothing to disclose.
Joseph T Morris, MD Chief of Infectious Disease Service, Madigan Army Medical Center; Assistant Professor,Department of Internal Medicine, Uniformed Services University of the Health Sciences
Disclosure: Nothing to disclose.
Gary J Noel, MD Professor, Department of Pediatrics, Weill Cornell Medical College; Attending Pediatrician,New YorkPresbyterian Hospital
Gary J Noel, MD is a member of the following medical societies: Pediatric Infectious Diseases Society
Disclosure: Nothing to disclose.
Cecily K Peterson, MD Program Director, Clinical Faculty, Department of Medicine, Madigan Army MedicalCenter
Disclosure: Nothing to disclose.
Charles V Sanders, MD Edgar Hull Professor and Chairman, Department of Internal Medicine, Professor ofMicrobiology, Immunology and Parasitology, Louisiana State University School of Medicine at New Orleans;Medical Director, Medicine Hospital Center, Charity Hospital and Medical Center of Louisiana at New Orleans;Consulting Staff, Ochsner Medical Center
Charles V Sanders, MD is a member of the following medical societies: Alliance for the Prudent Use ofAntibiotics, Alpha Omega Alpha, American Association for the Advancement of Science, American Associationof University Professors, American Clinical and Climatological Association, American College of PhysicianExecutives, American College of Physicians, American Federation for Medical Research, American Foundationfor AIDS Research, AmericanGeriatricsSociety, American Lung Association, American Medical Association,American Society for Microbiology, American Thoracic Society, American Venereal Disease Association,Association for Professionals in Infection Control and Epidemiology, Association of American Medical Colleges,Association of American Physicians, Association of Professors of Medicine, Infectious Disease Society forObstetrics and Gynecology, InfectiousDiseases Societyof America, Louisiana State Medical Society, OrleansParish Medical Society, Royal Society of Medicine, Sigma Xi, Society of General Internal Medicine,Southeastern Clinical Club, Southern Medical Association, Southern Society for Clinical Investigation, andSouthwestern Association of Clinical Microbiology
Disclosure: Nothing to disclose.
William H Shoff, MD, DTM&H Director, PENN Travel Medicine; Associate Professor, Department of EmergencyMedicine, Hospital of the University of Pennsylvania, University of Pennsylvania School of Medicine
William H Shoff, MD, DTM&H is a member of the following medical societies: American College of Physicians,American Society of Tropical Medicine and Hygiene, International Society of Travel Medicine, Society forAcademic Emergency Medicine, and Wilderness Medical Society
Disclosure: Nothing to disclose.
Russell W Steele, MD Head, Division of Pediatric Infectious Diseases, Ochsner Children's Health Center;Clinical Professor, Department of Pediatrics, Tulane University School of Medicine
Russell W Steele, MD is a member of the following medical societies: American Academy of Pediatrics,American Association of Immunologists, American Pediatric Society, American Society for Microbiology,Infectious Diseases Society of America, Louisiana State Medical Society, Pediatric Infectious Diseases Society,Society for Pediatric Research, and Southern Medical Association
Disclosure: Nothing to disclose.
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center Collegeof Pharmacy; EditorinChief, Medscape Drug Reference
Disclosure: Medscape Salary Employment
Jeter (Jay) Pritchard Taylor III, MD Compliance Officer, Attending Physician, Emergency Medicine Residency,Department of Emergency Medicine, Palmetto Health Richland, University of South Carolina School of Medicine;Medical Director, Department of Emergency Medicine, Palmetto Health Baptist
Jeter (Jay) Pritchard Taylor III, MD is a member of the following medical societies: American Academy of

10/28/2015 Leptospirosis Workup: Approach Considerations, Culture, Microscopic Agglutination Testing
http://emedicine.medscape.com/article/220563workup 5/7
Emergency Medicine, American College of Emergency Physicians, American Medical Association, and Societyfor Academic Emergency Medicine
Disclosure: Nothing to disclose.
Mary L Windle, PharmD Adjunct Associate Professor, University of Nebraska Medical Center College ofPharmacy; EditorinChief, Medscape Drug Reference
Disclosure: Nothing to disclose.
References
1. Palaniappan RU, Ramanujam S, Chang YF. Leptospirosis: pathogenesis, immunity, and diagnosis. CurrOpin Infect Dis. 2007 Jun. 20(3):28492. [Medline].
2. Yang CW. Leptospirosis in Taiwanan underestimated infectious disease. Chang Gung Med J. 2007 MarApr. 30(2):10915. [Medline].
3. Githeko AK, Lindsay SW, Confalonieri UE, Patz JA. Climate change and vectorborne diseases: a regionalanalysis. Bull World Health Organ. 2000. 78(9):113647. [Medline]. [Full Text].
4. National Research Council. Advancing the Science of Climate Change. Washington, DC: The NationalAcademies Press; 2010.
5. CDC. From the Centers for Disease Control and Prevention. Update: outbreak of acute febrile illnessamong athletes participating in EcoChallengeSabah 2000Borneo, Malaysia, 2000. JAMA. 2001 Feb 14.285(6):72830. [Medline].
6. CDC. Update: leptospirosis and unexplained acute febrile illness among athletes participating in triathlonsIllinois and Wisconsin, 1998. MMWR Morb Mortal Wkly Rep. 1998 Aug 21. 47(32):6736. [Medline].
7. CDC. Outbreak of leptospirosis among whitewater raftersCosta Rica, 1996. MMWR Morb Mortal WklyRep. 1997 Jun 27. 46(25):5779. [Medline].
8. Radl C, Müller M, RevillaFernandez S, KarnerZuser S, de Martin A, Schauer U, et al. Outbreak ofleptospirosis among triathlon participants in Langau, Austria, 2010. Wien Klin Wochenschr. 2011 Dec.123(2324):7515. [Medline].
9. CDC. From the Centers for Disease Control and Prevention. Outbreak of acute febrile illness andpulmonary hemorrhageNicaragua, 1995. JAMA. 1995 Dec 6. 274(21):1668. [Medline].
10. Gaynor K, Katz AR, Park SY, Nakata M, Clark TA, Effler PV. Leptospirosis on Oahu: an outbreakassociated with flooding of a university campus. Am J Trop Med Hyg. 2007 May. 76(5):8825. [Medline].
11. Socolovschi C, Angelakis E, Renvoisé A, Fournier PE, Marié JL, Davoust B, et al. Strikes, flooding, rats,and leptospirosis in Marseille, France. Int J Infect Dis. 2011 Oct. 15(10):e7105. [Medline].
12. Levett PN. Leptospirosis. Clin Microbiol Rev. 2001 Apr. 14(2):296326. [Medline]. [Full Text].
13. Inada R, Ido Y, Hoki R. The etiology, mode of infection, and specific therapy of Weil's disease(spirochaetosis icterohaemorrhagica. J Exper Med. 1916. 23:377402.
14. GILLESPIE RW, RYNO J. Epidemiology of leptospirosis. Am J Public Health Nations Health. 1963 Jun.53:9505. [Medline]. [Full Text].
15. Heisey GB, Nimmanitya S, Karnchanachetanee C, Tingpalapong M, Samransamruajkit S, Hansukjariya P,et al. Epidemiology and characterization of leptospirosis at an urban and provincial site in Thailand.Southeast Asian J Trop Med Public Health. 1988 Jun. 19(2):31722. [Medline].
16. SMITH DJ, SELF HR. Observations on the survival of Leptospira australis A in soil and water. J Hyg(Lond). 1955 Dec. 53(4):43644. [Medline]. [Full Text].
17. Cacciapuoti B, Ciceroni L, Maffei C, Di Stanislao F, Strusi P, Calegari L, et al. A waterborne outbreak ofleptospirosis. Am J Epidemiol. 1987 Sep. 126(3):53545. [Medline].
18. Chakurkar G, Vaideeswar P, Pandit SP, Divate SA. Cardiovascular lesions in leptospirosis: an autopsystudy. J Infect. 2008 Mar. 56(3):197203. [Medline].
19. Chierakul W, Tientadakul P, Suputtamongkol Y, Wuthiekanun V, Phimda K, Limpaiboon R, et al.Activation of the coagulation cascade in patients with leptospirosis. Clin Infect Dis. 2008 Jan 15. 46(2):25460. [Medline].
20. Wagenaar JF, Goris MG, Sakundarno MS, Gasem MH, Mairuhu AT, de Kruif MD, et al. What role docoagulation disorders play in the pathogenesis of leptospirosis?. Trop Med Int Health. 2007 Jan. 12(1):11122. [Medline].
21. Smythe L, Adler B, Hartskeerl RA, Galloway RL, Turenne CY, Levett PN. Classification of Leptospiragenomospecies 1, 3, 4 and 5 as Leptospira alstonii sp. nov., Leptospira vanthielii sp. nov., Leptospiraterpstrae sp. nov. and Leptospira yanagawae sp. nov., respectively. Int J Syst Evol Microbiol. 2013 May.63:185962. [Medline].
22. US Department of Health and Human Services. Summary of notifiable diseases, United States 1995.MMWR Morb Mortal Wkly Rep. 1996 Oct 25. 44(53):187. [Medline].
23. Malani J, Pryor J, Lusangulira K. Leptospirosis in Pohnpei (19861995): a case series on the use ofdopamine/steroid for Weil's syndrome. Pacific Health Dialog. 1996. 3:15361.
24. Sasaki DM, Pang L, Minette HP, Wakida CK, Fujimoto WJ, Manea SJ, et al. Active surveillance and riskfactors for leptospirosis in Hawaii. Am J Trop Med Hyg. 1993 Jan. 48(1):3543. [Medline].
25. Katz AR, Buchholz AE, Hinson K, Park SY, Effler PV. Leptospirosis in Hawaii, USA, 19992008. EmergInfect Dis. 2011 Feb. 17(2):2216. [Medline]. [Full Text].
26. Demers RY, Thiermann A, Demers P, Frank R. Exposure to Leptospira icterohaemorrhagiae in innercityand suburban children: a serologic comparison. J Fam Pract. 1983 Dec. 17(6):100711. [Medline].
27. Childs JE, Schwartz BS, Ksiazek TG, Graham RR, LeDuc JW, Glass GE. Risk factors associated withantibodies to leptospires in innercity residents of Baltimore: a protective role for cats. Am J Public Health.1992 Apr. 82(4):5979. [Medline]. [Full Text].

10/28/2015 Leptospirosis Workup: Approach Considerations, Culture, Microscopic Agglutination Testing
http://emedicine.medscape.com/article/220563workup 6/7
28. Trevejo RT, RigauPérez JG, Ashford DA, McClure EM, JarquínGonzález C, Amador JJ, et al. Epidemicleptospirosis associated with pulmonary hemorrhageNicaragua, 1995. J Infect Dis. 1998 Nov. 178(5):145763. [Medline].
29. Jackson LA, Kaufmann AF, Adams WG, Phelps MB, Andreasen C, Langkop CW, et al. Outbreak ofleptospirosis associated with swimming. Pediatr Infect Dis J. 1993 Jan. 12(1):4854. [Medline].
30. Dolhnikoff M, Mauad T, Bethlem EP, Carvalho CR. Pathology and pathophysiology of pulmonarymanifestations in leptospirosis. Braz J Infect Dis. 2007 Feb. 11(1):1428. [Medline].
31. Dall'Antonia M, Sluga G, Whitfield S, Teall A, Wilson P, Krahé D. Leptospirosis pulmonary haemorrhage:a diagnostic challenge. Emerg Med J. 2008 Jan. 25(1):512. [Medline].
32. Shaked Y, Shpilberg O, Samra D, Samra Y. Leptospirosis in pregnancy and its effect on the fetus: casereport and review. Clin Infect Dis. 1993 Aug. 17(2):2413. [Medline].
33. Hawaii Dept of Health. Communicable Disease Surveillance. Hawaii: Communicable Disease Report.Nov/Dec 1999. 15.
34. El Bouazzaoui A, Houari N, Arika A, Belhoucine I, Boukatta B, Sbai H, et al. Facial palsy associated withleptospirosis. Eur Ann Otorhinolaryngol Head Neck Dis. 2011 Nov. 128(5):2757. [Medline].
35. Peter G, Narasimha H. Acalculous cholecystitis: a rare presentation of leptospirosis progressing to Weil'sdisease. Asian Pac J Trop Med. 2011 Dec. 4(12):10078. [Medline].
36. Pappachan JM, Mathew S, Thomas B, Renjini K, Scaria CK, Shukla J. The incidence and clinicalcharacteristics of the immune phase eye disease in treated cases of human leptospirosis. Indian J Med Sci.2007 Aug. 61(8):4417. [Medline].
37. Person DA, Burnett MW. Leptospirosis. Tripler Army Medical Center. Medical Surveillance Monthly Report.1996. 2:78. [Full Text].
38. Person DA. Leptospirosis in the Pacific. : ;:. Tripler Army Medical Center. Medical Surveillance MonthlyReport. 1998. 4:1214. [Full Text].
39. Spichler A, Spichler E, Moock M, Vinetz JM, Leake JA. Acute pancreatitis in fatal anicteric leptospirosis.Am J Trop Med Hyg. 2007 May. 76(5):8867. [Medline].
40. World Health Organization. Human leptospirosis: guidance for diagnosis, surveillance and control. Availableat http://whqlibdoc.who.int/hq/2003/WHO_CDS_CSR_EPH_2002.23.pdf. Accessed: April 24, 2014.
41. Vasconcellos FA, Coutinho ML, da Silva EF, Fernandes CP, Monte LG, Seyffert N, et al. Testing differentantigen capture ELISA formats for detection of Leptospira spp. in human blood serum. Trans R Soc TropMed Hyg. 2010 Apr. 104(4):25964. [Medline].
42. BrettMajor DM, Coldren R. Antibiotics for leptospirosis. Cochrane Database Syst Rev. 2012 Feb 15.2:CD008264. [Medline].
43. Watt G, Padre LP, Tuazon ML, Calubaquib C, Santiago E, Ranoa CP, et al. Placebocontrolled trial ofintravenous penicillin for severe and late leptospirosis. Lancet. 1988 Feb 27. 1(8583):4335. [Medline].
44. Costa E, Lopes AA, Sacramento E, Costa YA, Matos ED, Lopes MB, et al. Penicillin at the late stage ofleptospirosis: a randomized controlled trial. Rev Inst Med Trop Sao Paulo. 2003 MayJun. 45(3):1415.[Medline].
45. Murray CK, Hospenthal DR. Determination of susceptibilities of 26 Leptospira sp. serovars to 24antimicrobial agents by a broth microdilution technique. Antimicrob Agents Chemother. 2004 Oct.48(10):40025. [Medline]. [Full Text].
46. Dursun B, Bostan F, Artac M, Varan HI, Suleymanlar G. Severe pulmonary haemorrhage accompanyinghepatorenal failure in fulminant leptospirosis. Int J Clin Pract. 2007 Jan. 61(1):1647. [Medline].
47. Shenoy VV, Nagar VS, Chowdhury AA, Bhalgat PS, Juvale NI. Pulmonary leptospirosis: an excellentresponse to bolus methylprednisolone. Postgrad Med J. 2006 Sep. 82(971):6026. [Medline]. [Full Text].
48. Meaudre E, Asencio Y, Montcriol A, Martinaud C, Graffin B, Palmier B, et al. [Immunomodulation insevere leptospirosis with multiple organ failure: plasma exchange, intravenous immunoglobulin orcorticosteroids?]. Ann Fr Anesth Reanim. 2008 Feb. 27(2):1726. [Medline].
49. Trivedi SV, Chavda RK, Wadia PZ, Sheth V, Bhagade PN, Trivedi SP, et al. The role of glucocorticoidpulse therapy in pulmonary involvement in leptospirosis. J Assoc Physicians India. 2001 Sep. 49:9013.[Medline].
50. Martins MG, Matos KT, da Silva MV, de Abreu MT. Ocular manifestations in the acute phase ofleptospirosis. Ocul Immunol Inflamm. 1998 Jun. 6(2):759. [Medline].
51. Takafuji ET, Kirkpatrick JW, Miller RN, Karwacki JJ, Kelley PW, Gray MR, et al. An efficacy trial ofdoxycycline chemoprophylaxis against leptospirosis. N Engl J Med. 1984 Feb 23. 310(8):497500.[Medline].
52. [Guideline] Guidugli F, Castro AA, Atallah AN. Antibiotics for preventing leptospirosis. Cochrane DatabaseSyst Rev. 2000. CD001305. [Medline].
53. Agampodi SB, Matthias MA, Moreno AC, Vinetz JM. Utility of quantitative polymerase chain reaction inleptospirosis diagnosis: association of level of leptospiremia and clinical manifestations in Sri Lanka. ClinInfect Dis. 2012 May. 54(9):124955. [Medline]. [Full Text].
54. AREAN VM. The pathologic anatomy and pathogenesis of fatal human leptospirosis (Weil's disease). Am JPathol. 1962 Apr. 40:393423. [Medline]. [Full Text].
55. Barkin RM, Guckian JC, Glosser JW. Infection by leptospira ballum: a laboratoryassociated case. SouthMed J. 1974 Feb. 67(2):155 passim. [Medline].
56. Everard CO, Bennett S, Edwards CN, Nicholson GD, Hassell TA, Carrington DG, et al. An investigation ofsome risk factors for severe leptospirosis on Barbados. J Trop Med Hyg. 1992 Feb. 95(1):1322. [Medline].
57. Gaspari R, Annetta MG, Cavaliere F, Pallavicini F, Grillo R, Conti G, et al. Unusual presentation ofleptospirosis in the late stage of pregnancy. Minerva Anestesiol. 2007 JulAug. 73(78):42932. [Medline].
58. Harris BM, Blatz PJ, Hinkle MK, McCall S, Beckius ML, Mende K, et al. In vitro and in vivo activity of firstgeneration cephalosporins against Leptospira. Am J Trop Med Hyg. 2011 Nov. 85(5):9058. [Medline]. [Full

10/28/2015 Leptospirosis Workup: Approach Considerations, Culture, Microscopic Agglutination Testing
http://emedicine.medscape.com/article/220563workup 7/7
Medscape Reference © 2011 WebMD, LLC
Text].
59. Katz AR, Manea SJ, Sasaki DM. Leptospirosis on Kauai: investigation of a common source waterborneoutbreak. Am J Public Health. 1991 Oct. 81(10):13102. [Medline]. [Full Text].
60. Khositseth S, Sudjaritjan N, Tananchai P, Ongajyuth S, Sitprija V, Thongboonkerd V. Renal magnesiumwasting and tubular dysfunction in leptospirosis. Nephrol Dial Transplant. 2008 Mar. 23(3):9528. [Medline].
61. Khosravi M, Bastani B. Acute renal failure due to leptospirosis in a renal transplant recipient: a brief reviewof the literature. Transplant Proc. 2007 May. 39(4):12636. [Medline].
62. Lettieri C, Moon J, Hickey P, Gray M, Berg B, Hospenthal D. Prevalence of leptospira antibodies in U.S.Army blood bank donors in Hawaii. Mil Med. 2004 Sep. 169(9):68790. [Medline].
63. Musgrave JE, Person DA. Acute renal failure in children due to leptospirosis. Pac Health Dialog. 1996.3:2001.
64. Phimda K, Hoontrakul S, Suttinont C, Chareonwat S, Losuwanaluk K, Chueasuwanchai S, et al.Doxycycline versus azithromycin for treatment of leptospirosis and scrub typhus. Antimicrob AgentsChemother. 2007 Sep. 51(9):325963. [Medline]. [Full Text].
65. Wang Z, Jin L, Wegrzyn A. Leptospirosis vaccines. Microb Cell Fact. 2007 Dec 11. 6:39. [Medline]. [FullText].
66. Watt G, Padre LP, Tuazon M, Calubaquib C. Skeletal and cardiac muscle involvement in severe, lateleptospirosis. J Infect Dis. 1990 Jul. 162(1):2669. [Medline].