Embed Size (px)
Citation preview

L’endocrinologia della PCOS
Paolo Moghetti
Endocrinologia, Diabetologia e Malattie del MetabolismoUniversità e Azienda Ospedaliera Universitaria Integrata di Verona

Criteri ESHRE/ASRM per la diagnosi di PCOS- Consensus di Rotterdam -
- Iperandrogenismo (clinico e/o biochimico)
- Oligo-anovulazione cronica
dopo aver escluso altre cause
Hum Reprod & Fertil Steril, 2004
- Ovaie micropolicistiche
La diagnosi richiede almeno due elementi fra:

Fenotipi clinici della PCOS in base ai criteri di Rotterdam
Oligoanovulazione Iperandrogenismo
Morfologia policistica dell’ovaio
Fenotipo classico
Fenotipo ovulatorio
Fenotipo normoandrogenico
Fenotipo completo

1. ….
2. We recommend maintaining the broad, inclusionary diagnostic criteria of Rotterdam while specifically identifying the phenotype.
3. We recommend …to improve the methods and criteria used to assess androgen excess, ovulatory dysfunction, and polycystic ovarian morphology.
4. ….
The NIH Evidence-based Methodology Workshop on PCOS (December 3–5, 2012)
Panel Recommendations

Frequency of PCOS phenotypes in studies
carried out in unselected populations
Lizneva D et al, Fertil Steril 2016
completo classico ovulatorio normoandrogenico

Categoria di BMI
%
41.036.2
22.8
0
10
20
30
40
50
60
70
obesità
sovrappeso
normopeso
42%36%
22%
Fenotipo clinico
%68.1
17.514.4
0
10
20
30
40
50
60
70
classico
ovulatorio
normoandrogenico
15%
68%
17%
Frequenza di fenotipi clinici e categorie di BMI
in 246 donne con PCOS del Verona 3P Study

(Ezeh U et al, JCE&M 2013)
Comparison of PCOS women referred to a tertiary
care clinic vs unselected PCOS and control women identified
at a pre-employment medical screening

Brower MA, Hai Y, et al, Hum Reprod 2019
Bidirectional Mendelian randomization indicates a causal relationship between
increased BMI and PCOS, while the reverse is not the case(750 individuals of European origin with PCOS and 1567 BMI-matched
controls, 92-SNP for BMI with PCOS as the outcome, 16-SNP for PCOS with BMI as the outcome)

Linea guida Endocrine Society sulla PCOS- esclusione di altre patologie -
• Dosaggio sistematico di:– 17OHP
– PRL
– TSH
• Altre ipotesi da considerare, in base alla presentazione clinica:– Gravidanza
– Amenorrea ipotalamica
– Insufficienza ovarica primitiva
– Neoplasie androgeno-secernenti
– S. di Cushing
– AcromegaliaLegro et al, JCE&M 2013

Presenting symptoms in 218 women with
Nonclassic Congenital Adrenal Hyperplasia
Moran C et al, Am J Obstet Gynecol 2000


Androgen levels in androgen-secreting tumors
www.uptodate.com, December 2018
• Virilization of recent onset and rapid progression, a serum total testosterone >150 ng/dL (5.2 nmol/L), or a serum DHEAS >700-800 mcg/dL (18.9-21.7 micromol/L) suggests a neoplastic source of hyperandrogenism.
• Caution must be exercised ... Approximately 20% of ovarian androgen-secreting neoplasms result in testosterone levels under 150 ng/dL,… and small tumors can cause fluctuating androgen levels.
• …there are case reports of adrenal tumors that secrete testosterone directly and exclusively, and some adrenal tumors may cause only a mild elevation in DHEAS.

?
?
Insulin resistance
Increased LH
Androgen excess ?
Hyperinsulinemia
PCOS

T and A4 by LC-MS/MS
DHEAS by CLIA
(≤50yr) (>50yr)
Elhassan YS et al, JCEM 2018
Final diagnosis in 1205 women
investigated for hyperandrogenism at a single tertiary
referral centerin Birmingham
between 2012-2016
CAH: congenital adrenal hyperplasia; ACC: adrenocortical carcinoma; CD: Cushing dis.;
ACA: adrenocortical adenoma; OHT: ovarian hyperthecosis; OvTu: ovarian tumors

Testosterone Androstenedione (DHEA) DHEAS 50%
(DHT)
SURRENE
OVAIO
25%
25% 50%
50%
100%90%
10%
Provenienza degli androgeni circolantinella donna normale

Frequenza di alterazioni degli androgeni circolanti (misurati con LC-MS/MS e dialisi all’equilibrio)
in 254 donne con PCOS della coorte del Verona 3P Study
Considerando insieme
iperandrogenismo clinico e
biochimico, la frazione di soggetti
PCOS iperandrogenici sale a 88%

AUC
PCOS women recognized as hyperandrogenemic by gold standard methods, either without or with FT measurement
Tosi F et al, J Clin Endocrinol Metab 2016

Calcolo con la formula di Vermeulen- ISSAM online calculator -
(http://www.issam.ch/freetesto.htm)
Free androgen index (FAI)Testosterone totale / SHBG x 100
Come stimare il testosterone libero(se non è possibile misurarlo in modo accurato)?
oppure (meglio)

Deming regression of gold
standard vs routine fT assayMisclassification of androgen excess
by routine methods in ~30% of patients
Tosi F et al, J Clin Endocrinol Metab 2016
Impact of inaccuracy in routine androgen assays in the classification of 204 women with PCOS
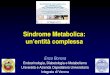
Relationship between serum free testosterone and hirsutism
score in 254 PCOS women of the Verona 3P Study cohort
Fre
e T
esto
ster
on
e (n
g/d
L)
Ferriman-Gallwey score

Rege J et al, J Clin Endocrinol Metab 2018
Pathways of adrenal steroidogenesis (11-oxygenated androgens are highlighted in black)
Dashed arrow denotes minor conversion to product
11KA: 11-ketoandrostenedione; 11OHA: 11b-hydroxyandrostenedione
11KT: 11-ketotestosterone; 11OHT: 11b-hydroxytestosterone

O’Reilly MW et al, JCEM 2017
Classic and 11-oxygenated serum androgens in PCOS women and controls

Rege J et al, J Clin Endocrinol Metab 2018
Serum concentrations of steroids in girls with premature adrenarche
vs age-matched girls (4-7 years)

1/20 vs T
3/4 vs T
Most highly upregulated
genes in cells after treatment
with 100 nM of T or 11KT, as
identified by RNA-Seq.
Rege J et al, J Clin Endocrinol Metab 2018
Androgen-dependent gene regulation in response to C19 steroids in CV1-ARLuc cells
(Selective adrogen-responsive model derived from cells engineered to express androgen receptor and an AR-driven bioluminescence signal)
* P < 0.05 vs basal

Marshall JC and Eagleson CA, Endocrinol Metab Clin North Am 1999
Hormonal changes during an ovulatory menstrual cycle

• The GnRH pulse generator shows an intrinsic firing
frequency of approximately one pulse per hour, which is seen
in isolated hypothalamus, and in vivo after menopause, in
premature ovarian failure, in the physiological late follicular
phase, but also, persistently, in many PCOS women.
• Rapid GnRH pulsatility favours pituitary synthesis of LH
over that of FSH and contributes to the increased LH
concentrations and LH : FSH ratios typical of PCOS.
• Inadequate FSH levels contribute to impaired follicular
development, whereas elevated LH levels augment ovarian
androgen production.
GnRH pulsatility and PCOS
Blank SK, McCartney CR and Marshall JC, Hum Reprod Update 2006

LH pulses
Blank SK, McCartney CR and Marshall JC, Hum Reprod Update 2006
Typical plasma gonadotropin pattern in an amenorrheic PCOS woman

Shaded areas: range of
responses after E2 and
progesterone for 7 days.
Closed circles: findings
when flutamide was
also administered,
before and during E2
and progesterone
treatment.
Eagleson CA et al, J Clin Endocrinol Metab 2000
Absolute change in LH pulses/12 hours following 7 days of estradiol and progesterone, with or without flutamide co-administration,
as a function of mean plasma progesterone on day 7
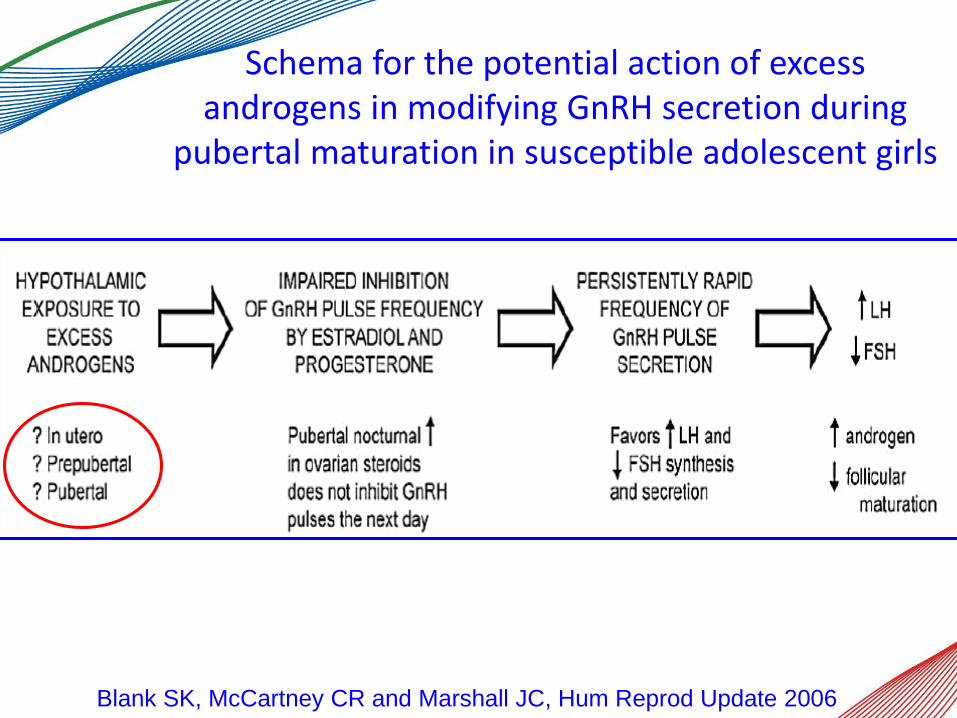
Schema for the potential action of excess androgens in modifying GnRH secretion during
pubertal maturation in susceptible adolescent girls
Blank SK, McCartney CR and Marshall JC, Hum Reprod Update 2006

Model of AMH secretion and action in the ovary
Dewailly D, La Marca A et al Hum Reprod Update 2014

Correlation between follicle count and serum
AMH

(16-19 weeks)
Tata B et al, Nat Med 2018
Serum AMH is increased in pregnant women with PCOS

Peripherally administered AMH in pregnancy reprograms the fetus and induces PCOS in
adulthood in female progenyIn the mother:• Neuroendocrine changes (increased serum LH)• Androgen excess• Impaired fertility (increase in aborted embryos/litter)
In the offspring:• Masculinization of the exposed female fetus (longer ano-genital
distance, neonatal LH and T surge, masculinization of dimorphic brain areas)
• PCOS-like neuroendocrine (persistently hyperactivated GnRH neurons with increased LH and testosterone levels) and reproductive phenotype (disrupted estrous cyclicity and impaired fertility) in adulthood
• No changes in weight
AMH detectable in the maternal brain areas where GnRH terminals are located. However, AMH cannot cross the placental barrier.
AMH effects prevented by co-administration of a GnRH antagonist.Tata B et al, Nat Med 2018

0
10
20
30
40
50
60
70
80
Insulin resistance(clamp, WHO criteria)
% 71
Metabolic syndrome(IDF 2009 criteria)
33
Frequency of insulin resistance and metabolic
syndrome in 137 consecutive PCOS women
(mean age 23 yr, BMI 28.5 kg/m2)
from Moghetti P et al, JCE&M 2013

Muscolo
Insulina
Ipofisi
Ovaio
Surrene
(?)
effetti
metabolici
SHBG
androgeni
LH(?)
modificato da Dunaif A, Endocr Rev 1997

Wild type - lean KO - lean Wild type - obese KO - obese
Fertility rate
0
20
40
60
80
100%
Serum testosterone
0
4
8
12
16
pg/dl
Wu S et al, Diabetes 2014
Obesity induced infertility and hyperandrogenism
are corrected by selective deletion of the insulin
receptor in theca cell

Moghetti P et al, JCE&M 1996
BASAL AND INSULIN-STIMULATED GLUCOSE UPTAKE IN
HYPERANDROGENIC WOMEN BEFORE AND AFTER
ANTIANDROGEN TREATMENT vs HEALTHY CONTROLS
0
15
30
45
60
75
90
Plasma insulin (pmol/l)
0 150 300 450 600 750 900
15
0
30
45
60
75
90
Glu
co
se
up
take
(µ
mo
l/kg
FF
M ·
min
)
p<0.01 vs hyperandrogenic
Controls
Hyperandrogenic before treatment
p<0.01 vs before treatment
Hyperandrogenic after treatment

0
20
40
60
80
100
normal-weight
overweight
obese
Frequency of insulin resistance in PCOS women according to BMI categories
(n= 375, glucose clamp methodology)
Tosi F, Bonora E & Moghetti P, Hum Reprod 2017

Performance dell’indice HOMA nell’identificare
i soggetti insulinoresistenti, definiti dal clamp,
fra le donne con PCOS (n=375)
Tosi F, Bonora E & Moghetti P, Hum Reprod 2017
Potere predittivo positivo: 92.9%
Potere predittivo negativo: 37.6%
R=0.622 p<0.001
0
4
8
12
16
20
0 2 4 6 8 10 12 14 16 18
HOMA-IR
Falsi negativi
Falsi positivi
M-clamp (mg/KgFFM x min-1)

Performance of several surrogate indexes in identifying insulin resistant subjects, as defined
by the hyperinsulinemic euglycemic clamp, in women with PCOS (n=375)
Tosi F, Bonora E & Moghetti P, Hum Reprod 2017

Fraction of subjects, subdivided according to BMI categories or presence/absence of metabolic syndrome, recognized as insulin resistant by the hyperinsulinemic euglycemic clamp and by several surrogate indexes, among women with PCOS
Tosi F, Bonora E & Moghetti P, Hum Reprod 2017

P<0.001 between PCOS phenotypes
“Classic” indicates
hyperandrogenism +
oligoanovulation
with or without PCOm
Divergences in insulin resistance between the PCOS phenotypes derived from
Rotterdam diagnostic criteria
from Moghetti P et al, JCE&M 2013
M-clamp values in PCOS phenotypes and healthy controls

3.52.51.5
-0.2
0.0
0.2
0.4
0.6
0.8
1.0
0
0.2
Baseline After metformin
0.4
0.6
0.8
1.0
responders
(55%)
cycle
s p
er
mo
nth
nonresponders
(45%)
Changes in mestruation ratein individual PCOS women
given metformin
Moghetti P et al, JCE&M 2000

Conclusioni
• La PCOS è una sindrome eterogenea e molto complessa dal punto di vista endocrino.
• L’eccesso di androgeni è l’aspetto più caratterizzante della PCOS, ma nell’accezione attuale non è obbligatorio. L’iperandrogenismo clinico e quello biochimico sono considerati equivalenti ai fini diagnostici, ma sottendono differenze cliniche.
• Le alterazioni neuroendocrine partecipano alla fisiopatologia dell’iperandrogenismo e forse delle alterazioni metaboliche, anche se le influenze reciproche fra questi aspetti rendono difficile stabilire la causa iniziale. L’AMH sembra essere un anello importante in questa catena fisiopatologica.
• L’insulinoresistenza è un altro elemento centrale della sindrome, in termini fisiopatologici e clinici, ma la sua valutazione nella pratica clinica resta problematica.