Embed Size (px)
Citation preview
194 CLINICAL IMAGING 1992;16:194-197
LEIOMYOBLASTOMA: VARIED CT APPEARANCE
MARILYN E. LERNER, MD, JACK FARMAN, MB, ChB, MMed, KAY CHO, MD, IRA TYLER, MD, AND DAVID MULLEN, MD
Leiomvoblastoma is an uncommon tumor of the stomach. Usually exogastric in site, the tumor may grow to a significant size before it becomes symp- tomatic.
Various appearances of the tumor include cystic and solid forms as well as a combination of both. Tumor hypervascularity may be identified on com- puted tomography (CT). The development of calcifi- cation in this tumor is rare. Late recurrence of the tumor may occur.
The differential diagnosis should include leiomy- sarcoma, leiomyoma, pancreatic psudocyst, and cys- tadenoma.
KEY WORDS:
Gastric tumor; Large, solid, cystic; Calcification; Late recurrence; Leiomyoblastoma.
INTRODUCTION
Gastric leiomyoblastomas are relatively unusual tu- mors. They often present as intramural lesions and can be well demonstrated on barium examination (1). Some 10%15% are exogastric, these tumors can grow to a large size and cause difficulty in diagnosis (l-4). For these reasons the tumors have at times been misdiagnosed as hepatic masses and pseudocysts of the pancreas (4, 6).
Although cystic leiomyoblastoma is the common
From the Department of Radiology, Columbia-Presbyterian Medical Center. New York. NY [M.E.L.. I.F.l: The Denartment of Radiology, Albert Einstein College of Mgdicine, Bronx, NY (KC., LT.); and The Department of Radiology, Greenwich Hospital, Greenwich, CT (D.M.).
Address reprint requests to: Jack Farman, M.B., Ch.B., M.Med. Columbia-Presbyterian Medical Center, Department of Radiol- ogy-M3-204,177 Ft. Washington Avenue, New York, NY 10032- 3204.
Received February 1992; accepted February 1992. 0 1992 by Elsevier Science Publishing Co., Inc. 655 Avenue of the Americas, New York, NY 10010 0899-7071/92/$5,00
form of presentation on computed axial tomography (CT) (4-8), we encountered one patient whose tumor was totally solid and a second patient whose tumor exhibited calcifications in addition to solid and cystic components. Three other patients presented with the more usually described cystic mass.
CASE REPORTS
Case 1
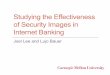
CF., a 70-year-old woman presented with a 5 month history of early satiety, nausea, vomiting, and weight loss. Abdominal ultrasound revealed a large left- upper-quadrant mass with cystic and solid areas. Echogenic foci with shadowing representing calcifi- cations were present as well. The mass extended from the posterior wall of the stomach to involve the spleen and tail of pancreas. Collateral vessels were evident surrounding the mass. Multiple hypoechoic liver lesions were identified and felt to be consistent with metastatic disease. CT revealed a 14 cm x 12 cm x 25 cm mass arising from the posterior wall of the stomach, which involved the pancreas and spleen (Figure 1). Calcification and central necrosis were identified. Collateral vessels were evident along the lateral aspect of the mass, as were multiple low-atten- uation lesions within the liver. An omental implant was identified anteriorly. Angiography disclosed a large hypervascular mass that was supplied from the splenic artery, and from a markedly enlarged gastro- epiploic artery. There was encasement of the splenic artery and occlusion of the splenic vein and coronary vein collaterals.
Ultrasound-guided percutaneous biopsy was per- formed and the presence of malignant leiomyoblas- toma established. At surgery a 12 cm x 25 cm mass was identified arising from the posterior wall of the stomach. A nodular liver was confirmed as well as the omental mass. Multiple lymph nodes were biopsied. Pathologic examination of tissue from multiple biop-
IULY-SEPTEMBER 1992 LEIOMYOBLASTOMA: VARIED CT APPEARANCE 195
FIGURE 1. (A) CT scan of the abdomen. A calcified mass arises from the fundus and greater curvature of the stomach. (B) There is extension of the mass into the left midabdomen.
sies of lymph nodes, liver, and omentum confirmed the presence of metastatic tumor.
Case 2
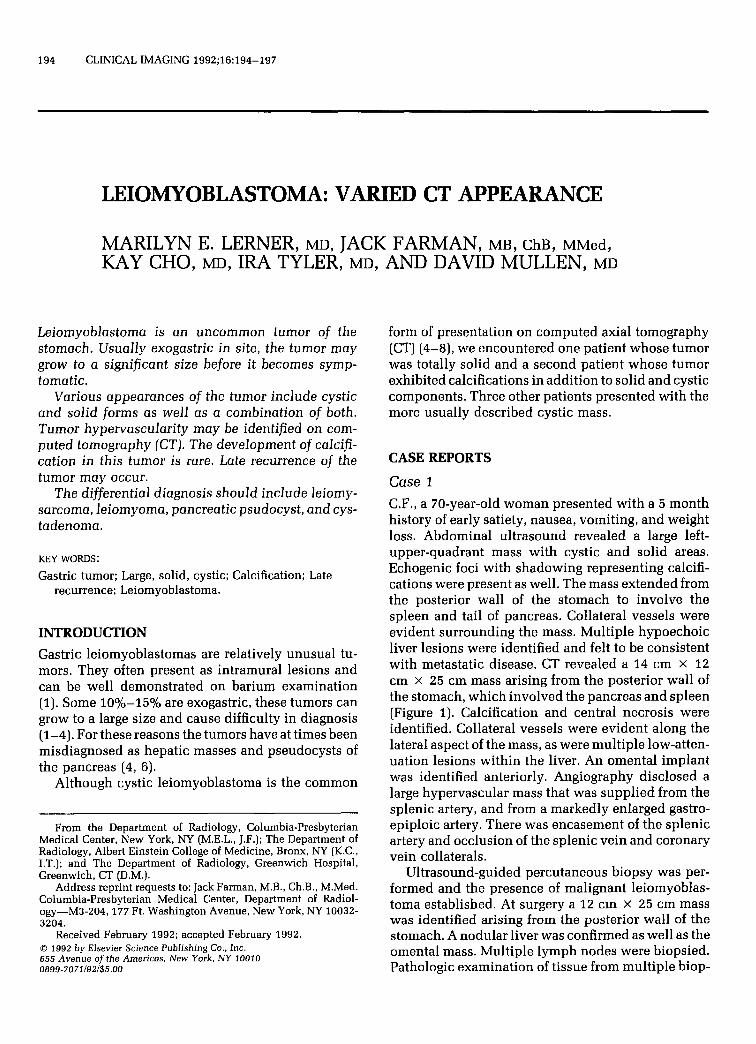
I.J., a 4%year-old black man presented with early satiety and abdominal discomfort. On CT scan a 30 cm exogastric cystic mass was present arising from the lesser curve of the stomach and filled the entire midabdomen (Figure 2). Irregular tumor tissue occu- pied the left lateral wall of the mass. This mass con- tained several fluid levels on ultrasound, and was avascular on angiography. At surgery the huge mass contained 8 L of murky brown fluid with debris. There was a small soft-tissue attachment to the lesser curve of the stomach. On pathologic examination the
FIGURE 2. (A) Abdominal CT scan. A large cystic and solid mass is seen arising from the body of the stomach. (B) The tumor extends inferiorly to distend the whole girth of the abdomen.
mass was identified as a nonmalignant leiomyoblas- toma. The cystic component consisted of hemor- rhagic necrotic debris.
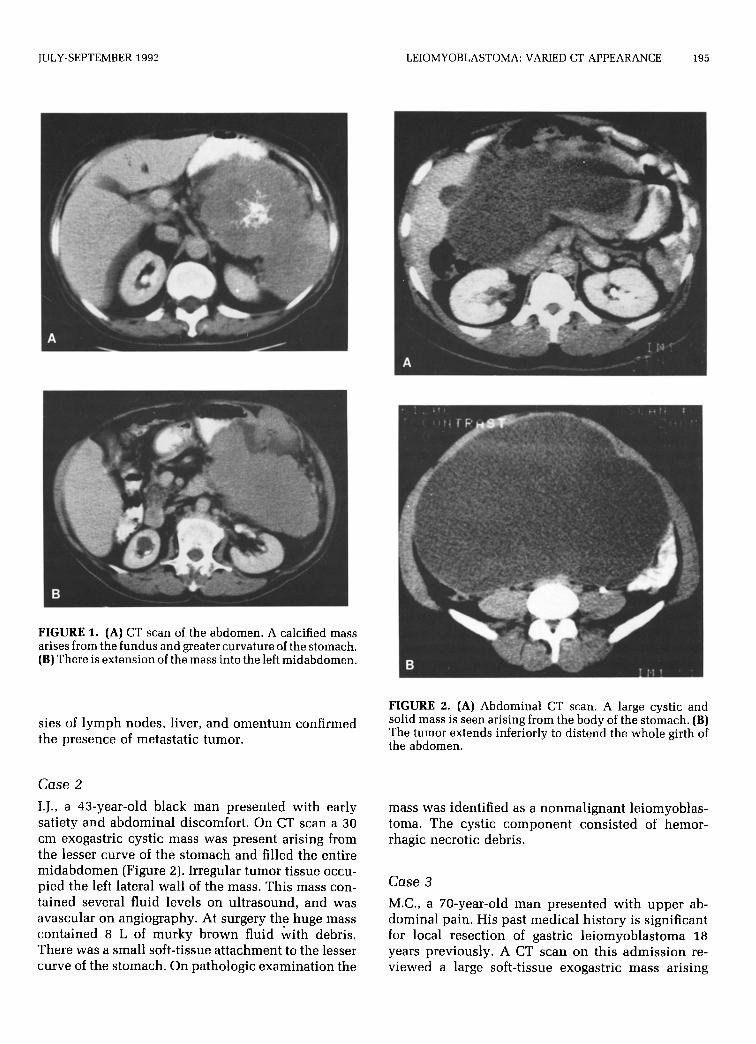
Case 3 M.C., a 70-year-old man presented with upper ab- dominal pain. His past medical history is significant for local resection of gastric leiomyoblastoma 18 years previously. A CT scan on this admission re- viewed a large soft-tissue exogastric mass arising
196 LERNER ET AL. CLINICAL IMAGING VOL. 16. NO. 3
FIGURE 3. CT scan demonstrates a soft-tissue mass arising from the posterior wall of the stomach.
from the posterior wall of the stomach (Figure 3). CT- guided biopsy confirmed the tumor to be a leiomy- oblastoma identical histologically with the original tumor resected 18 years earlier.
Case 4
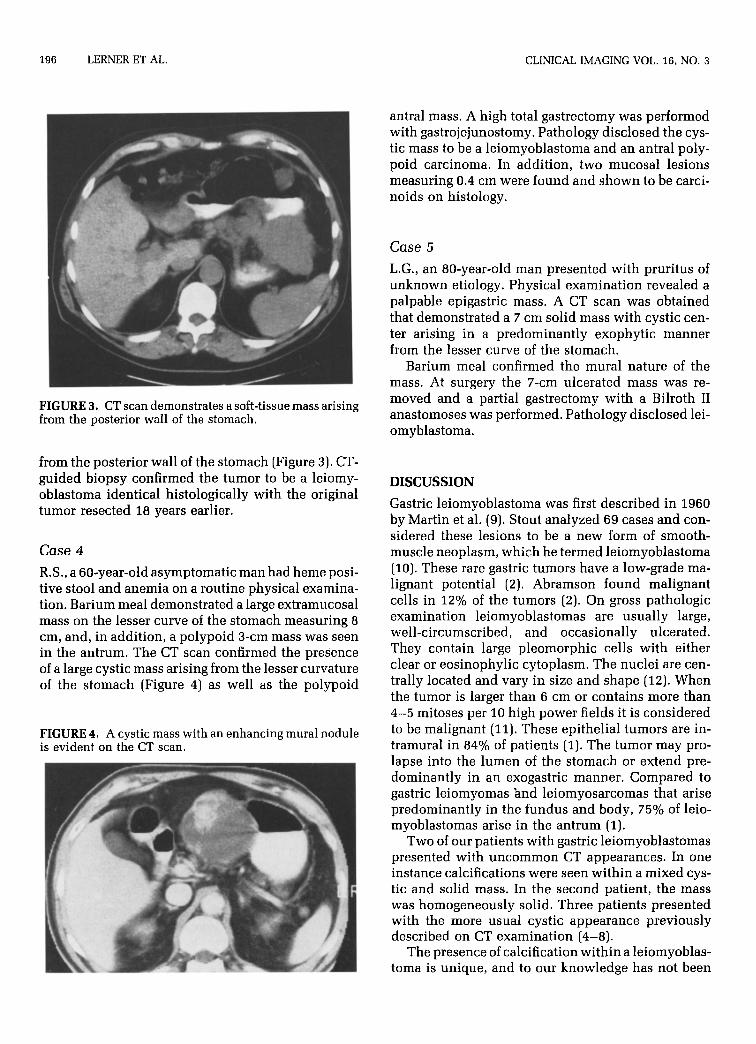
R.S., a 60-year-old asymptomatic man had heme posi- tive stool and anemia on a routine physical examina- tion. Barium meal demonstrated a large extramucosal mass on the lesser curve of the stomach measuring 8 cm, and, in addition, a polypoid 3-cm mass was seen in the antrum. The CT scan confirmed the presence of a large cystic mass arising from the lesser curvature of the stomach (Figure 4) as well as the polypoid
FIGURE 4. A cystic mass with an enhancing mural nodule is evident on the CT scan.
antral mass. A high total gastrectomy was performed with gastrojejunostomy. Pathology disclosed the cys- tic mass to be a leiomyoblastoma and an antral poly- poid carcinoma. In addition, two mucosal lesions measuring 0.4 cm were found and shown to be carci- noids on histology.
Case 5
L.G., an 80-year-old man presented with pruritus of unknown etiology. Physical examination revealed a palpable epigastric mass. A CT scan was obtained that demonstrated a 7 cm solid mass with cystic cen- ter arising in a predominantly exophytic manner from the lesser curve of the stomach.
Barium meal confirmed the mural nature of the mass. At surgery the i’-cm ulcerated mass was re- moved and a partial gastrectomy with a Bilroth II anastomoses was performed. Pathology disclosed lei- omyblastoma.
DISCUSSION
Gastric leiomyoblastoma was first described in 1960 by Martin et al. (9). Stout analyzed 69 cases and con- sidered these lesions to be a new form of smooth- muscle neoplasm, which he termed leiomyoblastoma (10). These rare gastric tumors have a low-grade ma- lignant potential (2). Abramson found malignant cells in 12% of the tumors (2). On gross pathologic examination leiomyoblastomas are usually large, well-circumscribed, and occasionally ulcerated. They contain large pleomorphic cells with either clear or eosinophylic cytoplasm. The nuclei are cen- trally located and vary in size and shape (12). When the tumor is larger than 6 cm or contains more than 4-5 mitoses per 10 high power fields it is considered to be malignant (11). These epithelial tumors are in- tramural in 84% of patients (1). The tumor may pro- lapse into the lumen of the stomach or extend pre- dominantly in an exogastric manner. Compared to gastric leiomyomas and leiomyosarcomas that arise predominantly in the fundus and body, 75% of leio- myoblastomas arise in the antrum (1).
Two of our patients with gastric leiomyoblastomas presented with uncommon CT appearances. In one instance calcifications were seen within a mixed cys- tic and solid mass. In the second patient, the mass was homogeneously solid. Three patients presented with the more usual cystic appearance previously described on CT examination (4-8).
The presence of calcification within a leiomyoblas- toma is unique, and to our knowledge has not been

JULY-SEPTEMBER 1992 LEIOMYOBLASTOMA: VARIED CT APPEARANCE 197
previously described. Metastatic disease to liver, omentum, and lymph nodes though rare may occur.
The angiographic features of these tumors range from being totally avascular to having marked hyper- vascularity. The findings in our patients would ap- pear to coincide with the extent of cystic degenera- tion present within the mass.
Exogastric leiomyoblastoma should be considered in the differential diagnosis of large left-upper-quad- rant masses together with leiomyomas and leiomyo- sarcomas. Other degenerating sarcomatous tumors, such as neuroembryosarcomas, as well as lymphoma, and rarely carcinoma, may present with this appear- ance. Contiguous pancreatic pseudocysts and cysta- denocarcinomas also enter into the differential diag- nosis.
REFERENCES
1. Faegenburg D, Farman J, Dallemand S, et al. Leiomyoblastoma of the stomach. Radiology 1975;117:297-300.
2. Abramson DJ. Leiomyoblastoma of the stomach. Surg Gynecol Obstet 1973;136:118-125.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
Lavin P, Hadgu SI, Foote Jr FW. Gastric and extragastric leio- myoblastomas. Cancer 1972;29:305-311. Stanley JH, Ravenel D, Parker TH, et al. Exogastric leiomy- oblastoma: rare gastric neoplasm mimicking left hepatic mass on computed tomography. Comput Tomogr 1986;10:187-190. Slasky BS, Denese L, Skolnick ML. Exogastric leiomyoblas- toma: diagnosis by CT and ultrasonography. South Med J 1982;75:1275-1277. Malhotia R, Evans R, Bhawan J, et al. A malignant gastric leiomyoblastoma presenting as an infected pseudocyst of the pancreas. Am J Gastroenterol 1988;83:452-456.
Choi BI, Ok ID, Im JG, et al. Exogastric cystic gastric leiomy- oblastoma with unusual CT appearance. Gastrointest Radio1 1988;13:109-111. Postona CT, Gerlag PGG. Leiomyoblastoma of the stomach. Neth J Med 1986;29:126-128. Martin JF, Bazin P, Feroldi J, et al. Tumorous myoides intra- murales de l’estomas; considerations microscopiques a props de 6 cas. Ann Anat Path01 1960;5:484-497. Stout AP. Bizarre smooth muscle tumors of the stomach. Can- cer 1962;15:400-409, Appelman HD, Helurg EB. Gastric epithelial leiomyoma and leiomyosarcoma (leiomyoblastoma). Cancer 1976;38:708- 728. Cotion R, Kumar V, Robbins S. Robbins Pathologic Basis of Disease, 4th ed. Philadelphia: WB Saunders, 1989, pp. 859-860.