Embed Size (px)
Citation preview
FSMoCaHB‡DBHMoAHRM�SAHRMMMa
Journal of the American College of Cardiology Vol. 56, No. 19, 2010© 2010 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00P
IMAGES IN CARDIOLOGY
Left Ventricular ThrombosisRefractory to Medical TherapyEric Russell, MD,* Victor Chien, MD,* Zain Khalpey, MD,†� Marc Bonaca, MD,‡Jayashri Aragam, MD,‡§ Miguel Haime, MD,†� Michael Crittenden, MD†�
Boston, Massachusetts
rom the *Boston Universitychool of Medicine, Boston,assachusetts; †Department
f Surgery, Division ofardiac Surgery, Brigham
nd Women’s Hospital,arvard Medical School,oston, Massachusetts;Cardiovascular Division,epartment of Medicine,righam and Women’sospital, Boston,assachusetts; §Department
f Cardiology, Veteran’sdministration Bostonealthcare System, Westoxbury Division, Boston,assachusetts; and the
Surgical Service, Cardiacurgery Section, Veteran’sdministration Bostonealthcare System, Westoxbury Division, Boston,assachusetts.anuscript receiveday 19, 2009;
ccepted May 31, 2009.
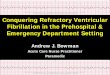
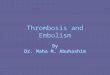
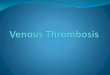
A65-year-old man with a history of pulmonary emboli, atrial fibrillation, nonischemicdilated cardiomyopathy, and significant polysubstance abuse was admitted with dys-pnea, new onset left-hand weakness, and a left-sided facial droop. An echocardiogram
showed an estimated ejection fraction of 20% and an echogenic pedunculated mass in the leftventricle (LV) apex with minimal mobility consistent with an organized LV mural thrombus(A, Online Video 1). Low molecular weight heparin (LMWH) and warfarin were initiated;however, the patient developed a visual field deficit 9 days later. A second trial of anticoagula-tion therapy was attempted, and regular heparin was begun. An echocardiogram 3 days latershowed a significant increase in the size and mobility of the thrombus (B, Online Videos 2and 3). So as to avoid a potentially catastrophic embolic event, the patient underwent a throm-bectomy via left ventriculotomy without complication (C).
ublished by Elsevier Inc. doi:10.1016/j.jacc.2009.05.084