Embed Size (px)
Citation preview

Circulation Journal Vol.82, March 2018
732 NAKABACHI M et al.Circ J 2018; 82: 732 – 738doi: 10.1253/circj.CJ-17-1019
hypertrophic cardiomyopathy (HCM)6 and those with severe LV dysfunction.7 We also have reported that e′ significantly but only weakly correlated with the time constant of LV pressure decay (τ) and that E/e′ modestly correlated with filling pressure in a multicenter study in Japan (strain/strain rate vs. myocardial velocity for assessing left ventricular relaxation and filling pressure: SMAP study).8 Accordingly, we speculated that some characteristics of the subjects in the SMAP study had altered the relation-ships between τ and e′ and between LV filling pressure and E/e′, and we conducted a substudy of SMAP. Because HCM itself has idiosyncratic features associated with LV
T he tissue Doppler-derived early-diastolic mitral annular velocity (e′) and the ratio of early-diastolic left ventricular (LV) inflow velocity (E) to e′ (E/e′)
reflect LV relaxation and filling pressure, respectively.1–3 It is recommended that e′ and E/e′ should not be used for the estimation of LV relaxation and filling pressure in normal subjects, or patients with significant mitral annular calcifi-cation, surgical rings, mitral stenosis, prosthetic mitral valves, moderate to severe primary mitral regurgitation, or constrictive pericarditis.4,5 Some recent reports, however, have noted that E/e′ does not correlate with LV filling pressure even in some clinical settings such as patients with
Received September 22, 2017; revised manuscript received November 16, 2017; accepted December 4, 2017; released online December 29, 2017 Time for primary review: 24 days
Division of Laboratory and Transfusion Medicine, Hokkaido University Hospital, Sapporo (M.N., C.S.); Department of Cardiovascular Medicine, Faculty of Medicine and Graduate School of Medicine (S.Y., H.I., T.H.), Faculty of Health Sciences (K.O., T.M.), Hokkaido University, Sapporo; Department of Cardiovascular Medicine, Tokushima University Hospital, Tokushima (K.K., H.Y.); Department of Cardiology and Nephrology, Mie University Graduate School of Medicine, Tsu (K. Watanabe, K.D.); Cardiovascular Division, Faculty of Medicine, University of Tsukuba, Tsukuba (T.I., Y.S.); Department of Cardio-Renal Medicine and Hypertension, Nagoya City University Graduate School of Medical Sciences, Nagoya (K. Wakami, N.O.), Japan
Mailing address: Satoshi Yamada, MD, PhD, Department of Cardiovascular Medicine, Faculty of Medicine and Graduate School of Medicine, Hokkaido University, Kita-15, Nishi-7, Kita-ku, Sapporo 060-8638, Japan. E-mail: [email protected]
ISSN-1346-9843 All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected]
Left Ventricular Mass Influences Relationship Between Filling Pressure and Early-Diastolic Ratio of Inflow Velocity to
Mitral Annular Velocity (E/e′)
Masahiro Nakabachi, BSc; Satoshi Yamada, MD, PhD; Hiroyuki Iwano, MD, PhD; Taichi Hayashi, MD, PhD; Kazunori Okada, PhD; Kenya Kusunose, MD, PhD;
Kiyotaka Watanabe, MD, PhD; Tomoko Ishizu, MD, PhD; Kazuaki Wakami, MD, PhD; Hirotsugu Yamada, MD, PhD; Kaoru Dohi, MD, PhD; Yoshihiro Seo, MD, PhD; Nobuyuki Ohte, MD, PhD; Chikara Shimizu, MD, PhD; Taisei Mikami, MD, PhD
Background: Early-diastolic mitral annular velocity (e′) and the ratio of early-diastolic left ventricular (LV) inflow velocity (E) to e′ (E/e′) have been widely used as indexes of LV relaxation and filling pressure, respectively. However, many recent studies have demonstrated that they are not reliable in various clinical settings. We thus investigated the factors influencing these echocardiographic parameters in a multicenter study.
Methods and Results: The study group comprised 69 patients, referred for cardiac catheterization, and enrolled in 5 university hospitals. Time constant (τ) and LV mean diastolic pressure (LVMDP) were measured using a micromanometer-tipped catheter. Although e′ only weakly correlated with τ (r=−0.35, P<0.01), E/e′ modestly correlated with LVMDP (r=0.48, P<0.001). Multivariable analysis revealed that hypertension (β=−0.33, P<0.01) and LV ejection fraction (LVEF) (β=0.44, P<0.001) were the independent determinants of e′, and LV mass index (LVMI) (β=0.37, P<0.001) and LVMDP (β=0.47, P<0.001) were those of E/e′. Additionally, E/e′ significantly correlated with LVMDP in patients with normal LVMI (r=0.74, P<0.001) but not in those with increased LVMI.
Conclusions: The coincidence of hypertension and LVEF affected the relationship between LV relaxation and e′, whereas LVMI altered the relationship between LV filling pressure and E/e′. Thus, clinical conditions associated with an increase in LVMI, such as LV hypertrophy and LV dilatation, should be considered when estimating the filling pressure from E/e′.
Key Words: Diastolic function; Echocardiography; Left ventricular filling pressure; Left ventricular hypertrophy; Tissue Doppler
ORIGINAL ARTICLEHeart Failure

Circulation Journal Vol.82, March 2018
733LVH Affects Relationship Between Filling Pressure and E/e′
micromanometer-tipped catheter was tested. Echocardiog-raphy was performed within 3 h of cardiac catheterization. We excluded patients with atrial fibrillation, frequent supraventricular or ventricular premature contraction, moderate to severe aortic or mitral valve disease, significant mitral annular calcification, constrictive pericarditis and inadequate echocardiographic images. Patients who had undergone mitral valve plasty, replacement, or aortic valve replacement, and those who underwent hemodialysis were also excluded. Furthermore, especially in the present study, patients with HCM were excluded from the final population in the SMAP study, and the remaining patients served as the subjects of this subanalysis. The study protocol was approved by the institutional review board of each hospital and all patients gave written informed consent.
LV Pressure MeasurementLV pressures were recorded before coronary angiography. A high-fidelity, 5-Fr (Model SPC-454D, Millar Instruments, Houston, TX, USA) or 6-Fr (Model CA-61000-PLB, CD Leycom, Zoetermeer, The Netherlands) pigtail micro-manometer-tipped catheter was used. LV pressure was acquired at end expiration for 3 consecutive cardiac cycles and digitized with a 1-ms sampling frequency using a data analyzing system (PowerLab and LabChart software version 7.3.4, ADInstruments, New South Wales, Australia). The τ was derived from a monoexponential fit to the LV pressure decay with a zero asymptote.9 LV mean diastolic pressure (LVMDP) was measured as previously described.10 An abnormal LV relaxation was defined as τ ≥48 ms and an elevated LV filling pressure was defined as LVMDP ≥12 mmHg.11 All parameters were averaged over 3 consecu-tive cardiac cycles.
EchocardiographyEchocardiography was performed using 1 of 2 commercially available systems (Aplio Artida SSH-88-CV or Aplio SSA-770A, Toshiba Medical Systems, Tochigi, Japan). LV mass (LVM) was calculated by the following formula from LV linear dimensions and indexed for body surface area (LVM index: LVMI) according to the recent recommendations
diastolic dysfunction and echocardiographic parameters including E/e′ are widely recognized not to be fairly useful for the estimation of LV filling pressure in this particular disease, HCM was excluded from the analysis of this substudy. Thus, the purpose of this study was to determine the factors influencing the echocardiographic estimation of LV relaxation and filling pressure using e′ and E/e′ among clinical information and general parameters of cardiac morphology and function.
MethodsStudy Population and ProtocolThe protocol of the SMAP study was described in the previous report.8 Briefly, the study included 84 patients (suspected of having angina pectoris, prior myocardial infarction, dilated cardiomyopathy, HCM, and hyperten-sive heart disease) who underwent diagnostic cardiac catheterization in 5 institutions in Japan (Hokkaido University Hospital, Nagoya City University Hospital, Mie University Hospital, University of Tsukuba Hospital, and Tokushima University Hospital), and the utility of echocardiographic parameters for the estimation of inva-sively measured LV relaxation and filling pressure using a
Table 1. Study Patients’ Characteristics
Age, years 61±12
Sex, female/male 18/51
BSA, m2 1.67±0.21
Heart rate,* beats/min 67±9 Systolic BP,* mmHg 124±25 Diastolic BP,* mmHg 71±15
NYHA class, n (%)
I 48 (70)
II 17 (25)
III 4 (6)
IV 0 (0)
Heart disease, n (%)
Angina pectoris 20 (29)
Prior MI 15 (22)
Dilated cardiomyopathy 12 (17)
Hypertensive heart disease 8 (12)
None 14 (20)
Multivessel disease, n (%) 15 (22)
Complications, n (%)
Hypertension 41 (59)
Diabetes mellitus 26 (38)
Dyslipidemia 41 (59)
Medications, n (%)
ARBs and/or ACEIs 39 (57)
β-blockers 35 (51)
Calcium-channel blockers 21 (30)
Diuretics 18 (26)
Digitalis 2 (3)
Statins 32 (46)
Antiplatelet drugs 36 (52)
*Measured at the beginning of echocardiographic examination. ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BP, blood pressure; BSA, body surface area; MI, myocardial infarction; NYHA, New York Heart Association.
Table 2. Conventional Echocardiographic Parameters and Hemodynamic Data
LV end-diastolic dimension, mm 51±8 LVMI, g/m2 118±42 LV hypertrophy, n (%) 33 (48)
LA dimension, mm 40±6 LVEF, % 56±17
Reduced LVEF (<50%), n (%) 28 (41)
E/A 0.92±0.60
e´, cm/s 7.5±2.2
E/e´ 9.0±4.3
τ, ms 48±13
Prolonged τ (≥48 ms), n (%) 31 (45)
LVMDP, mmHg 8.0±6.2
Elevated LVMDP (≥12 mmHg), n (%) 15 (22)
E/A, the ratio of left ventricular early-diastolic inflow velocity (E) to atrial systolic velocity (A); e´, early-diastolic mitral annular velocity; E/e´, the ratio of E to e´; EF, ejection fraction; LA, left atrial; LV, left ventricular; MDP, mean diastolic pressure; LVMI, left ventricular mass index; τ, time constant.
Circulation Journal Vol.82, March 2018
734 NAKABACHI M et al.
Moreover, the LV early-diastolic flow propagation velocity (Vp) was measured from the apical color M-mode Doppler image using a previously reported method.14 Finally, the ratio of E to Vp (E/Vp) was calculated.
Data CollectionData collection was the same as previously reported.8 Briefly, the study protocol was written by the investigators from Hokkaido University (S.Y. and H.I.), and reviewed and modified by members of the steering committee (S.Y., H.Y., K.D., Y.S., and N.O.). The data sets were sent to the investigators in Hokkaido University for analysis (T.H., S.Y., H.I., and M.N.).
Statistical AnalysisData are presented as mean ± standard deviation. Liner regression analysis and a Pearson’s product moment correlation coefficients were used to test the correlation between invasive and echocardiographic parameters. Multivariable analysis by using stepwise forward selection method, in which the parameters showing P values <0.10 in the univariable analyses were incorporated as explanatory variables, was used to identify the independent determinants of e′ and E/e′. Additionally, the multivariable regression for determining e′ was tested in the models including the explanatory variables mentioned before except for the
for cardiac chamber quantification by echocardiography in adults12 and those on the use of echocardiography in adult hypertension:13
LVM=0.8 • 1.04 • [(LVDd+IVST+PWT)3−LVDd3]+0.6 [g],
where LVDd is the LV end-diastolic dimension, IVST is the end-diastolic thickness of the interventricular septum, and PWT is the end-diastolic thickness of the LV posterior wall. LV hypertrophy (LVH) was defined as LVMI >95 g/m2 in females and LVMI >115 g/m2 in males according to the same recommendations.12,13 LV ejection fraction (LVEF) was calculated from the apical 4- and 2-chamber views using the biplane method of disks. LV inflow E, deceleration time of the early-diastolic flow (DT), isovolumic relaxation time (IRT), atrial systolic peak velocity (A), and the duration of the atrial systolic flow (Ad) were measured using pulsed-wave Doppler. The ratio of E to A (E/A) was calculated. In the apical 4-chamber view, pulmonary venous flow velocity pattern was recorded using a pulsed-wave Doppler method, and systolic peak velocity (PVS), diastolic peak velocity (PVD), and the duration of the atrial reversal flow (ARd) were measured. The ratio of PVS to PVD (PVS/PVD) and the time difference between ARd and Ad (ARd-Ad) were calculated. In addition, e′ was measured at the septal and lateral sides of the annulus using tissue Doppler imaging and averaged before calculating E/e′.
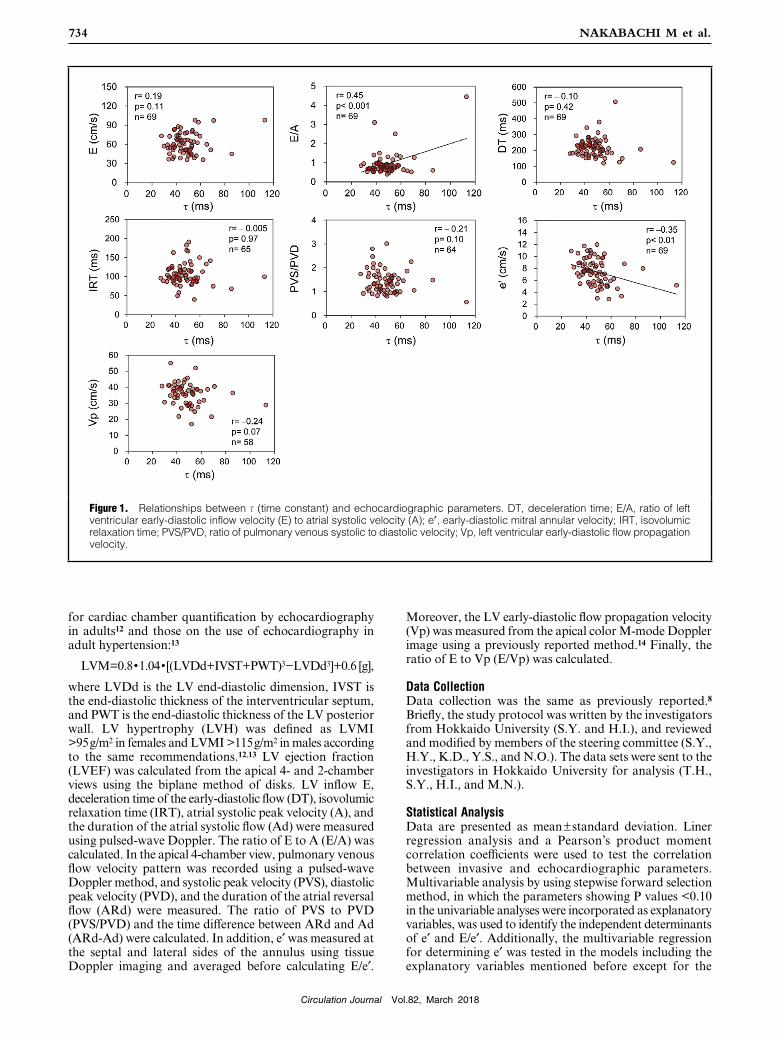
Figure 1. Relationships between τ (time constant) and echocardiographic parameters. DT, deceleration time; E/A, ratio of left ventricular early-diastolic inflow velocity (E) to atrial systolic velocity (A); e′, early-diastolic mitral annular velocity; IRT, isovolumic relaxation time; PVS/PVD, ratio of pulmonary venous systolic to diastolic velocity; Vp, left ventricular early-diastolic flow propagation velocity.

Circulation Journal Vol.82, March 2018
735LVH Affects Relationship Between Filling Pressure and E/e′
myocardial infarction, 12 with dilated cardiomyopathy, 8 with hypertensive heart disease, and 14 normal subjects. Basic echocardiographic parameters and hemodynamic data are shown in Table 2; 33 (48%) of the 69 patients had LVH, and 28 (41%) patients had reduced LVEF (LVEF <50%). Regarding hemodynamics, 31 (45%) patients had abnormal LV relaxation, and 15 (22%) patients had elevated LV filling pressure.
Correlations of Echocardiographic Parameters With τ and LVMDPIn all the patients, E, DT, IRT, PVS/PVD, and Vp did not correlate with τ (Figure 1). Although e′ significantly but only weakly correlated with τ, E/A moderately correlated with τ. DT and PVS/PVD did not correlate with LVMDP (Figure 2). ARd-Ad and E/Vp weakly correlated with LVMDP, whereas E, E/A, and E/e′ moderately correlated with LVMDP. These results confirmed the similar relation-ships of echocardiographic parameters to LV relaxation and filling pressure in all of the patients in the present study to those in the previous SMAP study.
Determinants of e′Univariable analysis showed that hypertension, LV end-diastolic dimension, LVEF, τ, and LVMDP significantly correlated with e′. The multivariable analysis revealed that the presence of hypertension (β=−0.33) and LVEF
presence of hypertension (Table S1, model 1) and except for LVEF (Table S1, model 2) by using the same stepwise method. SPSS (version 19.0, SPSS Inc., Chicago, IL, USA) was used for statistical calculation. The results were considered statistically significant with P<0.05.
ResultsIn the SMAP study, of the 84 patients who were eligible for study enrollment, 1 patient was excluded from the study for the onset of atrial fibrillation during catheterization, 1 patient because the catheter could not be threaded into the left ventricle, 3 patients for moderate mitral regurgitation detected for the first time by the scheduled echocardio-graphic examination, and 2 patients because of inadequate echocardiographic imaging. In the present study, we further excluded 8 patients with HCM as mentioned earlier, and so the remaining 69 patients were analyzed in this substudy.
Patients’ CharacteristicsThe patients’ characteristics are shown in Table 1. Of 34 patients who were suspected of having angina pectoris, 20 were positively diagnosed by coronary angiography. In the remaining 14 patients, coronary angiography and echocar-diography revealed that they did not have coronary artery disease or other cardiac diseases. Finally, the study subjects consisted of 20 patients with angina pectoris, 15 with prior
Figure 2. Relationships between left ventricular mean diastolic pressure (LVMDP) and echocardiographic parameters. ARd-Ad, the difference in duration between pulmonary venous reversal flow and mitral flow during atrial contraction; E/e′, ratio of E to e′; E/Vp, ratio of E to Vp. Other abbreviations as in Figure 1.
Circulation Journal Vol.82, March 2018
736 NAKABACHI M et al.
were the independent determinants of e′, (2) LVMI and LVMDP were the independent determinants of E/e′, and most importantly that (3) E/e′ did not significantly correlate with LVMDP in patients with LVH.
Determinants of e′Tissue Doppler-derived e′ has been considered as a measure of LV relaxation based on experimental studies in which e′ correlated well with invasively measured τ under various loading conditions.15 However, the SMAP study, which we conducted in clinical patients referred for cardiac cathe-terization, showed that e′ significantly but only weakly correlated with τ.8 In the present analysis, we tested the determinants of e′ to clarify the factors other than τ that influence e′ because the characteristics of the studied patients could have altered the relationship between τ and e′. As a result, we found that hypertension as a comorbidity and LVEF, but not τ, were the determinants of e′. To the best of our knowledge, this is the first report to demonstrate that the presence of hypertension and LVEF have an effect on e′.
It has been reported that longitudinally-oriented inner
(β=0.44) were independent determinants of e′ but τ was not (Table 3).
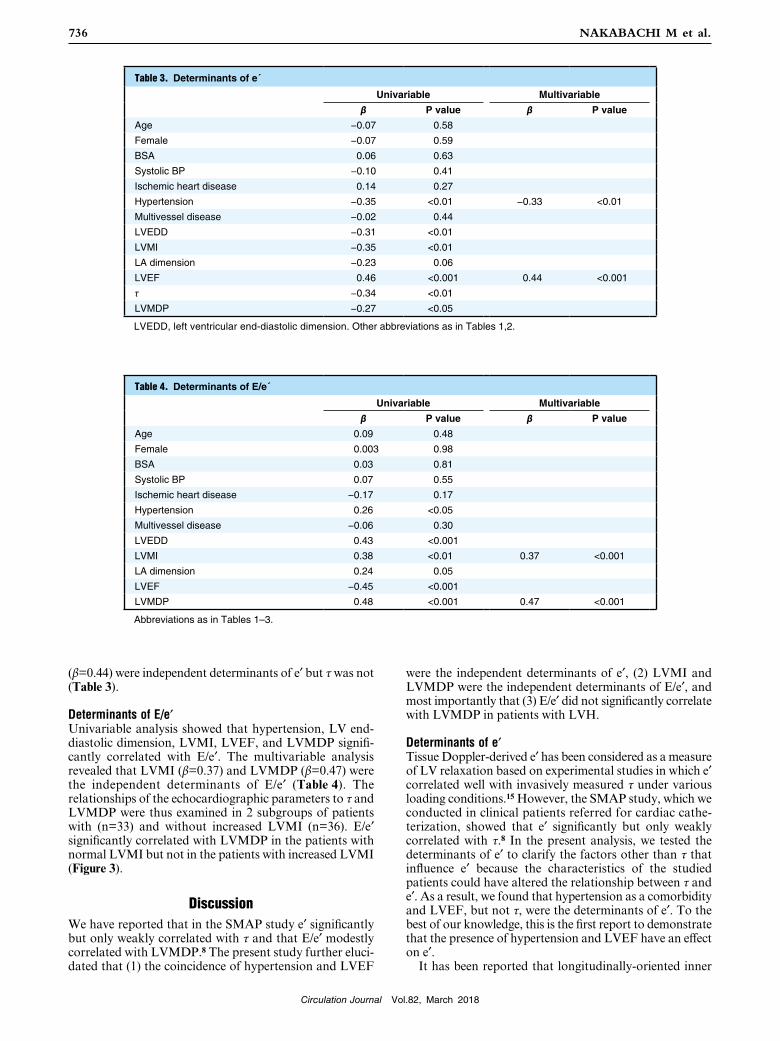
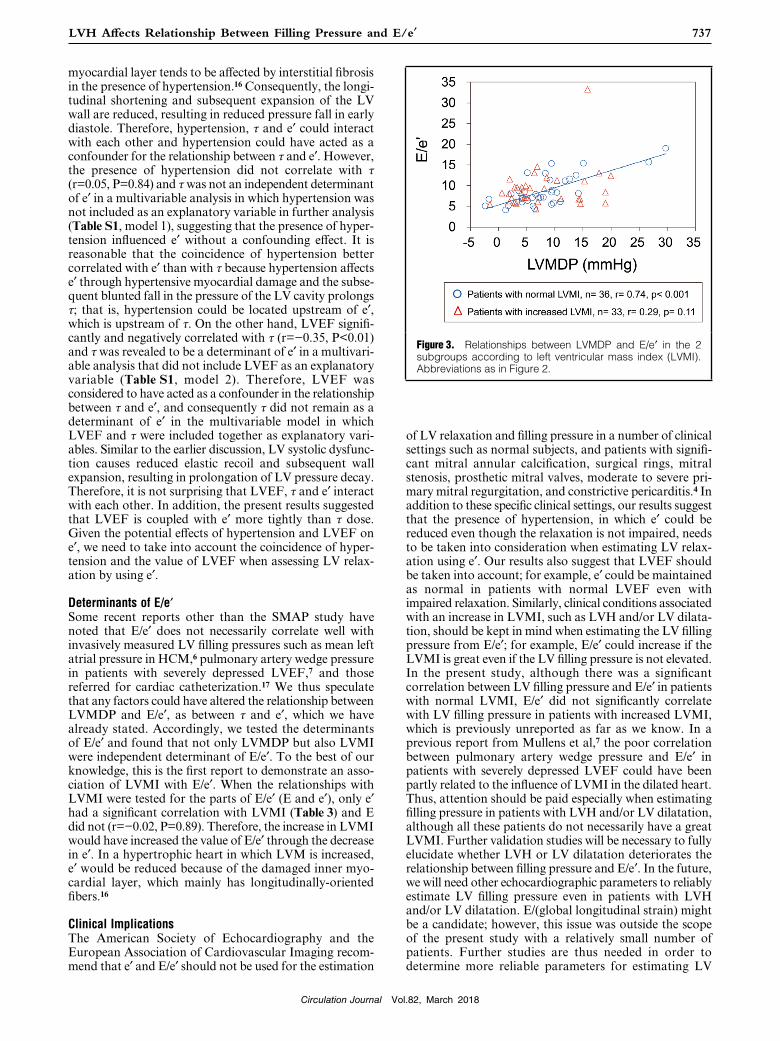
Determinants of E/e′Univariable analysis showed that hypertension, LV end-diastolic dimension, LVMI, LVEF, and LVMDP signifi-cantly correlated with E/e′. The multivariable analysis revealed that LVMI (β=0.37) and LVMDP (β=0.47) were the independent determinants of E/e′ (Table 4). The relationships of the echocardiographic parameters to τ and LVMDP were thus examined in 2 subgroups of patients with (n=33) and without increased LVMI (n=36). E/e′ significantly correlated with LVMDP in the patients with normal LVMI but not in the patients with increased LVMI (Figure 3).
DiscussionWe have reported that in the SMAP study e′ significantly but only weakly correlated with τ and that E/e′ modestly correlated with LVMDP.8 The present study further eluci-dated that (1) the coincidence of hypertension and LVEF
Table 3. Determinants of e´
Univariable Multivariable
β P value β P value
Age −0.07 0.58
Female −0.07 0.59
BSA 0.06 0.63
Systolic BP −0.10 0.41
Ischemic heart disease 0.14 0.27
Hypertension −0.35 <0.01 −0.33 <0.01
Multivessel disease −0.02 0.44
LVEDD −0.31 <0.01 LVMI −0.35 <0.01 LA dimension −0.23 0.06
LVEF 0.46 <0.001 0.44 <0.001
τ −0.34 <0.01 LVMDP −0.27 <0.05
LVEDD, left ventricular end-diastolic dimension. Other abbreviations as in Tables 1,2.
Table 4. Determinants of E/e´
Univariable Multivariable
β P value β P value
Age 0.09 0.48
Female 0.003 0.98
BSA 0.03 0.81
Systolic BP 0.07 0.55
Ischemic heart disease −0.17 0.17
Hypertension 0.26 <0.05 Multivessel disease −0.06 0.30
LVEDD 0.43 <0.001
LVMI 0.38 <0.01 0.37 <0.001
LA dimension 0.24 0.05
LVEF −0.45 <0.001
LVMDP 0.48 <0.001 0.47 <0.001
Abbreviations as in Tables 1–3.
Circulation Journal Vol.82, March 2018
737LVH Affects Relationship Between Filling Pressure and E/e′
of LV relaxation and filling pressure in a number of clinical settings such as normal subjects, and patients with signifi-cant mitral annular calcification, surgical rings, mitral stenosis, prosthetic mitral valves, moderate to severe pri-mary mitral regurgitation, and constrictive pericarditis.4 In addition to these specific clinical settings, our results suggest that the presence of hypertension, in which e′ could be reduced even though the relaxation is not impaired, needs to be taken into consideration when estimating LV relax-ation using e′. Our results also suggest that LVEF should be taken into account; for example, e′ could be maintained as normal in patients with normal LVEF even with impaired relaxation. Similarly, clinical conditions associated with an increase in LVMI, such as LVH and/or LV dilata-tion, should be kept in mind when estimating the LV filling pressure from E/e′; for example, E/e′ could increase if the LVMI is great even if the LV filling pressure is not elevated. In the present study, although there was a significant correlation between LV filling pressure and E/e′ in patients with normal LVMI, E/e′ did not significantly correlate with LV filling pressure in patients with increased LVMI, which is previously unreported as far as we know. In a previous report from Mullens et al,7 the poor correlation between pulmonary artery wedge pressure and E/e′ in patients with severely depressed LVEF could have been partly related to the influence of LVMI in the dilated heart. Thus, attention should be paid especially when estimating filling pressure in patients with LVH and/or LV dilatation, although all these patients do not necessarily have a great LVMI. Further validation studies will be necessary to fully elucidate whether LVH or LV dilatation deteriorates the relationship between filling pressure and E/e′. In the future, we will need other echocardiographic parameters to reliably estimate LV filling pressure even in patients with LVH and/or LV dilatation. E/(global longitudinal strain) might be a candidate; however, this issue was outside the scope of the present study with a relatively small number of patients. Further studies are thus needed in order to determine more reliable parameters for estimating LV
myocardial layer tends to be affected by interstitial fibrosis in the presence of hypertension.16 Consequently, the longi-tudinal shortening and subsequent expansion of the LV wall are reduced, resulting in reduced pressure fall in early diastole. Therefore, hypertension, τ and e′ could interact with each other and hypertension could have acted as a confounder for the relationship between τ and e′. However, the presence of hypertension did not correlate with τ (r=0.05, P=0.84) and τ was not an independent determinant of e′ in a multivariable analysis in which hypertension was not included as an explanatory variable in further analysis (Table S1, model 1), suggesting that the presence of hyper-tension influenced e′ without a confounding effect. It is reasonable that the coincidence of hypertension better correlated with e′ than with τ because hypertension affects e′ through hypertensive myocardial damage and the subse-quent blunted fall in the pressure of the LV cavity prolongs τ; that is, hypertension could be located upstream of e′, which is upstream of τ. On the other hand, LVEF signifi-cantly and negatively correlated with τ (r=−0.35, P<0.01) and τ was revealed to be a determinant of e′ in a multivari-able analysis that did not include LVEF as an explanatory variable (Table S1, model 2). Therefore, LVEF was considered to have acted as a confounder in the relationship between τ and e′, and consequently τ did not remain as a determinant of e′ in the multivariable model in which LVEF and τ were included together as explanatory vari-ables. Similar to the earlier discussion, LV systolic dysfunc-tion causes reduced elastic recoil and subsequent wall expansion, resulting in prolongation of LV pressure decay. Therefore, it is not surprising that LVEF, τ and e′ interact with each other. In addition, the present results suggested that LVEF is coupled with e′ more tightly than τ dose. Given the potential effects of hypertension and LVEF on e′, we need to take into account the coincidence of hyper-tension and the value of LVEF when assessing LV relax-ation by using e′.
Determinants of E/e′Some recent reports other than the SMAP study have noted that E/e′ does not necessarily correlate well with invasively measured LV filling pressures such as mean left atrial pressure in HCM,6 pulmonary artery wedge pressure in patients with severely depressed LVEF,7 and those referred for cardiac catheterization.17 We thus speculate that any factors could have altered the relationship between LVMDP and E/e′, as between τ and e′, which we have already stated. Accordingly, we tested the determinants of E/e′ and found that not only LVMDP but also LVMI were independent determinant of E/e′. To the best of our knowledge, this is the first report to demonstrate an asso-ciation of LVMI with E/e′. When the relationships with LVMI were tested for the parts of E/e′ (E and e′), only e′ had a significant correlation with LVMI (Table 3) and E did not (r=−0.02, P=0.89). Therefore, the increase in LVMI would have increased the value of E/e′ through the decrease in e′. In a hypertrophic heart in which LVM is increased, e′ would be reduced because of the damaged inner myo-cardial layer, which mainly has longitudinally-oriented fibers.16
Clinical ImplicationsThe American Society of Echocardiography and the European Association of Cardiovascular Imaging recom-mend that e′ and E/e′ should not be used for the estimation
Figure 3. Relationships between LVMDP and E/e′ in the 2 subgroups according to left ventricular mass index (LVMI). Abbreviations as in Figure 2.

Circulation Journal Vol.82, March 2018
738 NAKABACHI M et al.
4. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr 2009; 22: 107 – 133.
5. Nagueh SF, Smiseth OA, Appleton CP, Byrd BF 3rd, Dokainish H, Edvardsen T, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2016; 29: 277 – 314.
6. Geske JB, Sorajja P, Nishimura RA, Ommen SR. Evaluation of left ventricular filling pressures by Doppler echocardiography in patients with hypertrophic cardiomyopathy: Correlation with direct left atrial pressure measurement at cardiac catheterization. Circulation 2007; 116: 2702 – 2708.
7. Mullens W, Borowski AG, Curtin RJ, Thomas JD, Tang WH. Tissue Doppler imaging in the estimation of intracardiac filling pressure in decompensated patients with advanced systolic heart failure. Circulation 2009; 119: 62 – 70.
8. Hayashi T, Yamada S, Iwano H, Nakabachi M, Sakakibara M, Okada K, et al. Left ventricular global strain for estimating relaxation and filling pressure: A multicenter study. Circ J 2016; 25: 1163 – 1170.
9. Weiss JL, Frederiksen JW, Weisfeldt ML. Hemodynamic determinants of the time-course of fall in canine left ventricular pressure. J Clin Invest 1976; 58: 751 – 760.
10. Yamamoto K, Nishimura RA, Redfield MM. Assessment of mean left atrial pressure from the left ventricular pressure tracing in patients with cardiomyopathies. Am J Cardiol 1996; 78: 107 – 110.
11. Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM, et al. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: A comparative simultaneous Doppler-catheter-ization study. Circulation 2000; 102: 1788 – 1794.
12. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2015; 28: 1 – 39.
13. Marwick TH, Gillebert TC, Aurigemma G, Chirinos J, Derumeaux G, Galderisi M, et al. Recommendations on the use of echocardiography in adult hypertension: A report from the European Association of Cardiovascular Imaging (EACVI) and the American Society of Echocardiography (ASE). J Am Soc Echocardiogr 2015; 28: 727 – 754.
14. Takatsuji H, Mikami T, Urasawa K, Teranishi J, Onozuka H, Takagi C, et al. A new approach for evaluation of left ventricular diastolic function: Spatial and temporal analysis of left ventricular filling flow propagation by color M-mode Doppler echocardiog-raphy. J Am Coll Cardiol 1996; 27: 365 – 371.
15. Nagueh SF, Sun H, Kopelen HA, Middleton KJ, Khoury DS. Hemodynamic determinants of the mitral annulus diastolic velocities by tissue Doppler. J Am Coll Cardiol 2001; 37: 278 – 285.
16. Ishizu T, Seo Y, Kameda Y, Kawamura R, Kimura T, Shimojo N, et al. Left ventricular strain and transmural distribution of structural remodeling in hypertensive heart disease. Hypertension 2014; 63: 500 – 506.
17. Andersen OS, Smiseth OA, Dokainish H, Abudiab MM, Schutt RC, Kumar A, et al. Estimating left ventricular filling pressure by echocardiography. J Am Coll Cardiol 2017; 69: 1937 – 1948.
Supplementary FilesSupplementary File 1
Table S1. Results of additional multivariable analyses of determi-nants of e′
Please find supplementary file(s);http://dx.doi.org/10.1253/circj.CJ-17-1019
filling pressure regardless of LVMI.
Study LimitationsThere are several limitations to be acknowledged. The number of patients was relatively small, and a larger valida-tion study will be needed in the future. Although particular attention was paid to not changing the intravascular volume and vascular tone during the period between echocardiog-raphy and cardiac catheterization, the examinations were not performed simultaneously, which may have created slight differences in hemodynamic status. Because the study subjects consisted of normal subjects and patients with angina pectoris, prior myocardial infarction, dilated cardio-myopathy, and hypertensive heart disease, the results of the present study are not applicable to all patients with heart failure. After excluding patients with HCM, which itself has idiosyncratic features associated with LV diastolic dysfunction, however, the remaining subjects of the present study might represent appropriate patients for determining the influential factors on echocardiographic estimation of LV relaxation and filling pressure among available clinical information and general parameters of cardiac morphology and function. On the other hand, several specific diseases that may possibly be the cause of heart failure, such as cardiac sarcoidosis and cancer therapeutics-related cardiac dysfunction, should be specifically investigated in the future.
ConclusionsThe present study demonstrated that the coincidence of hypertension and LVEF were independent determinants of e′. Additionally, LVMI and LVMDP were independent determinants of E/e′, and E/e′ did not significantly correlate with LV filling pressure in patients with increased LVMI. Thus, clinical conditions associated with an increase in LVMI, such as LVH and LV dilatation, should be kept in mind when estimating LV filling pressure from E/e′; for example, we should consider that it could overestimate the true LV filling pressure in patients with increased LVMI.
Sources of FundingThis research was supported by Research and Development Committee Program of the Japan Society of Ultrasonics in Medicine.
DisclosuresNone.
References 1. Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quiñones
MA. Doppler tissue imaging: A noninvasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol 1997; 30: 1527 – 1533.
2. Oki T, Tabata T, Yamada H, Wakatsuki T, Shinohara H, Nishikado A, et al. Clinical application of pulsed Doppler tissue imaging for assessing abnormal left ventricular relaxation. Am J Cardiol 1997; 79: 921 – 928.
3. Sohn DW, Chai IH, Lee DJ, Kim HC, Kim HS, Oh BH, et al. Assessment of mitral annulus velocity by Doppler tissue imaging in the evaluation of left ventricular diastolic function. J Am Coll Cardiol 1997; 30: 474 – 480.





























