Embed Size (px)
Citation preview

2929
Left Ventricular Diastolic Chamber Stiffnessand Intramyocardial Coronary Capacitance
in Isolated Dog HeartsJun Watanabe, MD, PhD; Marc J. Levine, MD; Fabio Bellotto, MD;
Robert G. Johnson, MD; William Grossman, MD
Background. Because the myocardium is perfused primarily during diastole, changes in diastolicproperties of the left ventricle (LV) should influence the intramyocardial circulation.Methods and Results. We examined the influence of LV diastolic properties on the magnitude and
localization of intramyocardial coronary capacitance by analyzing the coronary pressure-venous flowrelation in isolated, isovolumic dog heart preparations. After sudden occlusion of the left coronary arteryduring a long diastole, we measured precapacitance and postcapacitance resistances (RPRE and RposT) andcalculated intramyocardial coronary capacitance (CNM) from RosT and the time constant of the coronaryvenous flow decay. Using this method, we characterized the effects of coronary vasodilation, LV diastolicvolume, and LV diastolic chamber stiffness on the coronary circulation. The magnitude of CIM increasedfrom 0.09±0.01 to 0.24±0.20 mL * mm Hg- * 100 g` (P<.01) after adenosine-induced vasodilation,whereas both Rpos and RPRE decreased significantly. The ratio of Rpos to RPRE+RPOST decreased from035±0.02 to 0.23±0.02 (P<.01), suggesting redistribution of CIM to the distal portion of the coronaryvascular tree. An increase in LV volume and wall stress was imposed to increase LV diastolic pressurefrom 2±0.1 to 25±1 mm Hg this increased Rpos significantly but not RpRE and decreased the magnitudeof COM. The resistance ratio did not change significantly. Increased LV diastolic chamber stiffness inducedby hypoxic perfusion (isovolumic LV diastolic pressure increased from 11±1 to 28±1 mm Hg) raised RposTand decreased the magnitude of CnM from 032±0.12 to 0.17±0.04 mL' mm Hg-". 100 g` (P<.05). Theresistance ratio increased significantly from 0.21±0.05 to 033±0.05 with increased LV diastolic chamberstiffness. Adjustment ofLV diastolic volume to lower diastolic pressure to 10±1 mm Hg did not alter thesechanges significantly, suggesting that an intrinsic increase in myocardial stiffness played a major role inthese changes.
Conclusions. Extravascular compression by raised LV diastolic volume and/or increased LV diastolicchamber stiffness acted mainly on coronary vessels that determine intramyocardial capacitance andpostcapacitance resistance. (Circulation. 1993;88:2929-2940.)KEY WORDs * diastole * flow * myocardium * left ventricle
M yocardium, especially the subendocardium, isconsidered to be perfused during diastole.Therefore, much attention has been paid to
diastolic coronary hemodynamics. Most studies haveused diastolic coronary vascular resistance as an indica-tor of coronary vascular tone. However, some findingshave suggested that it is difficult to calculate diastoliccoronary resistance in the beating heart. Thus, in dias-tole, coronary venous flow (CVF) is quite small despitehigh coronary arterial flow.1'2 In the dynamic situation,diastolic coronary flow is not uniform throughout thecoronary bed (from the coronary ostium to the coronaryvenous outlets). Accordingly, we may not apply a simple
Received May 3, 1993; revision accepted August 24, 1993.From the Charles A. Dana Research Institute and Harvard-
Thorndike Laboratory of Beth Israel Hospital, Departments ofMedicine (J.W., M.J.L., W.G.) (Cardiovascular Division) andSurgery (F.B., R.G.J.), Beth Israel Hospital and Harvard MedicalSchool, Boston.Correspondence to Dr William Grossman, Cardiovascular Divi-
sion, Beth Israel Hospital, 330 Brookline Ave, Boston, MA 02215.
Ohm's law concept to calculate diastolic coronary vas-cular resistance in the beating heart.Most of the blood entering the coronary circulation
during diastole is observed to be stored in coronarycapacitance vessels and squeezed out during systole.3These capacitance vessels may function as a reservoirduring diastole and may determine the effective coro-nary back pressure.3 Thus, coronary capacitance mightbe quite important in determining diastolic coronaryflow as well as coronary vascular resistance. Recentreports have indicated that small intramyocardial ves-sels rather than large epicardial arteries have enoughcapacitive function to store most of diastolic inflow.3-5The tone of these small arteries may be affected byseveral factors, including myogenic, metabolic, neuro-humoral, and endothelial factors,6'7 and the capacityof maximum dilation may be limited by extravascularcompression due to ventricular hypertrophy.68 Also,increased left ventricular (LV) diastolic wall stressand/or impaired LV diastolic relaxation may be ex-pected to limit the capacity of maximum dilation.9-13The present study was designed to assess the magni-
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

2930 Circulation Vol 88, No 6 December 1993
Coronary OcclusIon PCRPRE RPO8T
PIN POUT
PDIS IMc,
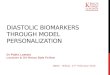
FIG 1. Schematic representation of the coronary circu-lation with intramyocardial coronary capacitance (CIM)and both pre-CiM and post-CiM resistance (RPRE andRPOST). PIN is coronary input pressure and POUT is coronaryoutflow pressure. PDIS is coronary pressure distal tocoronary occlusion. (See text for detail.)
tude and localization of intramyocardial coronarycapacitance and the influence of changes in vasomotortone, intravascular pressure, increases in LV diastolicpressure and wall stress, and decreased LV diastolicchamber stiffness on these parameters of intramyocar-dial coronary capacitance.
MethodsTheoretical Considerations
Fig 1 shows a schematic linear model of the coronarycirculation that includes precapacitance resistance(RPRE), postcapacitance resistance (RPOST), and intra-myocardial capacitance (CIM). CIM is capacitive function(compliance) of intramyocardial coronary vessels and isusually estimated by a volume change (dV) as a result ofa pressure change (dP).3 As proposed originally bySpaan et al,3 the distribution of resistance between RpREand RPOST defines functionally the localization of CIM. Tocalculate these parameters, a transient response of theoutflow is examined after a sudden cessation of theinflow. Thus, the inflow is abruptly occluded during thesteady state of a long diastole, maintaining outputpressure (POUT) constant. After the occlusion, we canexpect that CVF will persist for several seconds6 as theresult of a discharge from coronary capacitance vessels.CVF is determined by (Pc-Pou-)/RposT, where Pc is thepressure at CIM. Therefore, RPOST is determined by(Pc-Pou)ICVF. Because POU is known, we can calcu-late RPOST if we can measure Pc. In this model, we mayassume that coronary pressure distal to the coronaryocclusion (PDIs) reflects Pc since there is no flow throughthe precapacitance resistance (RPRE). Practically, thecoronary perfusion line is occluded suddenly during along diastole. The coronary pressure distal to the occlu-sion will correspond to PDIS of this model. We may beable to anticipate that the relation between PDIS andCVF is linear, and its slope indicates postcapacitanceresistance. Because total resistance (RPRE+RPOST) canbe easily calculated from the steady-state flow anddriving pressure (PIN-POUT), we can calculate a ratio ofRPOST/(RPRE+RPOST) that indicates distribution of RPREand RPOST, defining the functional localization of CIM inthe model mentioned above. The magnitude of CIM canbe calculated from postcapacitance resistance (RpOST)and from the time constant of CVF decay after cessa-tion of coronary inflow since the time constant (Tc)might be determined by the multiplication of CIM andRPOST (TC=CIMm RPOST). This simplification was usedprimarily to assess CIM. Based on this concept, we
Pressure
VentricularPressure
CoronaryVenousFlow
CoronaryVenousFlow
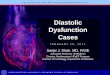
FIG 2. Illustration of the experimental preparation. (Seetext for detail.)
performed experiments designed to obtain the requiredmeasurements in an isolated dog heart preparation.
Animal PreparationExperiments were performed in isolated dog hearts
(body weight, 23 to 29 kg) perfused by arterial blood ofa support dog (body weight, 25 to 36 kg) anesthetizedintravenously with a mixture of a-chloralose (50 mg/kg)and urethane (500 mg/kg). Details of the isolated heartmodel have been described elsewhere.10 Fig 2 shows theexperimental layout in which a thin-wall Latex balloonwas secured in the left ventricle through the mitralannulus with a small drain inserted into the left ventri-cle from the apex to prevent blood accumulation be-tween the balloon and the ventricular wall. The pericar-dium was removed in this study.A Gregg-type cannula was secured in the left main
coronary artery. The left coronary arteries were per-fused at constant pressure (around 70 mm Hg) from apressurized arterial blood reservoir. Another thin-wallcannula with a flow probe was inserted to the greatcardiac vein (GCV) through the coronary sinus and awide incision in the right atrium. The other end of thisGCV cannula was open to air. The atrioventricularnode was destroyed by formalin injection,14 and ventric-ular pacing was performed. A long diastole was inducedby sudden cessation of pacing.15 We used lidocaine (0.5-to 1.0-mg bolus) to suppress ventricular escape beats, ifrequired. Arterial blood was sampled repeatedly tocontrol pH, Pco2, and Po2 within the physiologicalrange.LV pressure and coronary arterial perfusion pressure
(CPP) were recorded with a catheter-tip micromanom-eter (Millar Instruments, Houston, Tex) and pressuretransducer (Statham P23D), respectively. Phasic flow ofthe left coronary artery and GCV were measured withthe flowthrough-type Doppler probes (5 mm internaldiameter for left coronary flow and 3 mm for GCV flow[GCVF]; Titronics Medical Instrument, Iowa City) anda Doppler unit (model 545C-A, University of Iowa).Calibration of flow measurement was performed in eachexperiment by the timed collection method.
Fig 3 shows schematic tracings of CPP, left coronaryarterial flow (LCAF), and GCVF. During a long dias-tole, after confirmation of the plateau of diastoliccoronary inflow and outflow, the arterial perfusion lineis occluded suddenly just proximal to the measurement
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

Watanabe et al Intramyocardial Coronary Capacitance 2931
B
QCVF| /
*1/Slp... CPP
PpO89(RpRE +Rpo0=-(1I8lope)I(CPPIGCVF)CaIm uTc/R PwOT (GCV area)Normalized Ciip-CI (LCAF/GCVF)I(LV Weiht)
FIG 3. A, Schematic tracings of coronary pressure distalto the occlusion (CPP), left coronary arterial flow (LCAF),and great cardiac vein flow (GCVF) in the present study.Tc is the time constant of GCVF decay. B, Schematiccoronary pressure-GCVF relation. RPOST is the reciprocalvalue of the slope of this relation. The equations showhow to calculate the ratio of RPOST to total resistance andhow to normalize the magnitude of intramyocardial ca-pacitance (CiM). (See text for detail.)
point of CPP. This produces the expected rapid de-crease in LCAF and a relatively slow decrease in CPPand GCVF (Fig 3A). Based on the concept describedunder "Theoretical Considerations," the relation be-tween coronary pressure distal to the occlusion andGCVF may be analyzed on a pressure-flow plane (Fig3B). The slope of this relation is obtained by a least-squares method, and its reciprocal value used to assessthe functional resistance, which is located distal tointramyocardial capacitance (RPOST; Figs 1 and 3B). Themagnitude of intramyocardial capacitance is obtainedby RPOST and the time constant (Tc) of the GCVF decayafter coronary occlusion (Fig 3A), which is calculated bya standard exponential fit. This exponential fitting wasperformed in the range where the coronary pressure-venous flow relation was linear, and the values ofcorrelation coefficient of the fitted line were more than.85. It is clear that GCVF does not indicate the total leftcoronary outflow; however, it is impossible to measuretotal coronary venous flow because of the many differ-ent venous drainage pathways in the dog heart. We haveperformed GCVF measurement to avoid a large capac-itance of coronary sinus, assuming that the pattern ofthe other venous outflow is identical to GCVF pattern.Although the absolute measurements relate only to thearea of myocardium from which the GCV drains venousblood, we may normalize the value by LV weight asshown in the bottom of Fig 3.
Vasodilation StudyIn eight hearts, the magnitude and localization of
intramyocardial coronary capacitance were assessed bythe same method mentioned, before and after coronaryvasodilation caused by adenosine infusion (250 ,ug/min).Maximum vasodilation was confirmed by the absence ofreactive hyperemia after 15 seconds of coronary occlu-sion. Perfusion pressure was maintained constant(around 70 mm Hg) throughout the intervention in eachdog. To minimize vasoconstriction during the long dias-
tole before vasodilation, heart rate and LV developedpressure were maintained as low as possible to reducemyocardial oxygen requirement before the longdiastole.
Perfusion Pressure StudyIn additional experiments (n=4), we examined the
effect of perfusion pressure before the time of coronaryocclusion on the magnitude and the localization ofintramyocardial coronary capacitance. Coronary vesselswere vasodilated by adenosine infusion (250 1£g/min).CPP was reduced from approximately 100 to 40 mm Hg.
Left Ventricular Diastolic Volume StudyIn eight hearts, the measurements were performed at
different LV balloon volumes. LV balloon volume wasincreased so that LV end-diastolic pressure would beincreased from 1 mm Hg to approximately 25 mm Hg.Adenosine was infused (250 jig/min) for maximumvasodilation. CPP was maintained constant at approxi-mately 70 mm Hg.
Left Ventricular Diastolic Chamber Stiffness StudyIn six of eight hearts, the effect of a change in LV
diastolic chamber stiffness on intramyocardial coronarycapacitance was examined. Two hearts were excludedfrom data analysis because an increase in LV diastolicpressure was clearly lower than target value (25 mm Hg)after 45 minutes of hypoxic perfusion. LV diastolicchamber stiffness was changed by hypoxic blood perfu-sion. Hypoxic blood consisted of methemoglobin-con-taining red blood cells resuspended in plasma. Thepreparation of this methemoglobin-containing redblood cell solution has been described elsewhere.10Adenosine infusion (250 gg/min) was continued tomaintain coronary vasodilation constant. Initial LVend-diastolic pressure was adjusted to around 10mm Hg. In the early stage of hypoxic blood perfusion (in2 minutes), the magnitude and localization of intramyo-cardial coronary capacitance were assessed as the con-trol values before any change in LV diastolic pressure.An increase in LV diastolic chamber stiffness wasmonitored by a change in LV diastolic pressure, keepingLV balloon volume constant. When LV diastolic pres-sure increased to approximately 25 mm Hg after 25 to40 minutes of hypoxic perfusion, an experimental mea-surement was performed. To assess the effect of LVdiastolic pressure per se, measurements were againrepeated when LV diastolic pressure was decreasedfrom around 25 to 10 mm Hg (control value) by reduc-ing LV balloon volume while hypoxic perfusion wascontinued. Coronary flow probes were calibrated withthe hypoxic blood in each experiment. CPP was main-tained at approximately 70 mm Hg.
Data AnalysisAll data were recorded on an eight-channel electro-
static recorder (Gould ES 1000) at a paper speed of 50mm/s. GCVF and coronary pressure data were digi-talized for further analysis by a personal computersystem (IBM-PC AT with a digitizer). Data were ex-pressed as mean±SEM. Two-way ANOVA with re-peated measurements was used for statistical analysis.
A Cornary
cpP ae............
LOAF
.,,.CVF
T'cTC '-
0 a
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

2932 Circulation Vol 88, No 6 December 1993
A200 r
LCAF
LV0
CPP
0t
l sec
LCAF-v
GCVFM = l; ~o
CPP
a
.c
IL
100 V
50
00 25 50 75
Coronary Pressure mm Hg
FIG 4. A, Simultaneous recordings of left coronary arterial flow (LCAF), great cardiac vein flow (GCVF), coronaryperfusion pressure (CPP), and left ventricular pressure (LVP) in a long diastole. After LACF and GCVF reached a plateau,LCAF was suddenly interrupted by occluding the perfusion line. Note that GCVF persisted for several seconds aftercoronary occlusion while CPP showed a bimodal decay. B, Coronary pressure-venous flow relation from data of Fig 4A.The relation had a horizontal portion and a second linear decline portion. The former corresponds to the rapid decreasein CPP and persistent GCVF immediately after coronary occlusion, and the latter corresponds to an exponential decreasein both CPP and GCVF (Fig 4A).
ResultsFig 4A shows representative tracings during a long
diastole. After confirming the plateau of LCAF andGCVF, the coronary perfusion line was occluded sud-denly. Note that CVF persisted and decreased graduallyover several seconds, as expected from Fig 3A. Usually,the duration of diastole was not sufficient for GCVF tocease in these experiments. Coronary pressure, mea-sured distal to the occlusion, showed an early rapiddecrease followed by a gradual exponential decay. Fig4B shows the relation between coronary pressure distalto the occlusion and CVF (GCVF), plotted from Fig 4A.This relation exhibited a horizontal portion and asecond linear decline of both pressure and flow. Thissecond decline phase is consistent with the expectationfrom our model (Figs 1 and 3) in which the dischargingflow from CIM is determined by a postcapacitance resis-tance (RpOST). To calculate RPOST, we fitted a regressionline to this decline portion by a least-squares method.The reciprocal value of the slope in this case (Fig 4) was0.12 mm Hg . mL` * min' and represents an estimateof RPOST (postcapacitance resistance; Fig 1) for the areaof myocardium drained by the GCV. The total coronaryvascular resistance (RPRE+RPOST) of this area was 0.65mm Hg * mL` * mink (coronary driving pressure di-vided by GCVF measured just before the occlusion; see
Fig 3). Thus, 81% of total coronary resistance wasfunctionally distributed proximal to CIM, and 19% ofcoronary resistance was distal to CIM. In the caseillustrated in Fig 4, the time constant of the CVF decaywas 1.47 seconds, and the capacitance value was 0.20mL/mm Hg. When normalized as described in Fig 3, thiscapacitance value was 0.23 mL * mm Hg-1* 100 g`.
Effects of Vasodilation on Coronary CapacitanceTable 1 summarizes basic coronary hemodynamic
data before and after adenosine infusion for all exper-iments. CPP was maintained nearly constant. LCAF andGCVF increased significantly after adenosine infusion.Before adenosine infusion, coronary vasoconstrictionmight occur during a long diastole'5 because of adecrease in oxygen demand. We attempted to minimizethis vasoconstriction by reducing heart rate and LVdeveloped pressure (low LV balloon volume) before thelong diastole, and we confirm that a change in coronaryflow was only 1.8% per second during long diastoles andwas considered small enough to be ignored.
Fig 5A shows the coronary pressure-venous flowrelations before and after adenosine infusion. Afteradenosine, the curve shifted upward, and the seconddecline portion became steeper. The reciprocal slopevalues of the fitted lines to these portions were 0.36
ECG
1
a
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

Watanabe et al Intramyocardial Coronary Capacitance 2933
TABLE 1. Coronary Perfusion Pressure, Total LeftCoronary Flow, and Great Cardiac Vein Flow During thePlateau Phase of a Long Diastole
Before AfterAdenosine Adenosine P
Coronary perfusionpressure, mm Hg 71±3 68±3 NS
Left coronary flow,mL/min 113±12 207±11 <.001
Left coronary flow,mL. min .100 g-1 98±7 189±8 <.001Great cardiac veinflow, mL/min 58±6 128±11 <.001
All measurements were performed just before the coronaryocclusion.
(before adenosine) and 0.07 mm Hg * min~1. mLU' (af-ter adenosine). Fig 5B shows superimposed tracings ofGCVF versus time after coronary occlusion. The timeconstant of these curves decreased after adenosinevasodilation from 2.02 to 1.25 seconds. From thesevalues, the calculated magnitude of CIM was 0.08 beforeadenosine and 0.20 mL. mm Hg-' * 100 g` after aden-osine. The ratio of RPOST to RPRE+RPOST was 0.35 beforeadenosine and 0.25 after adenosine. Table 2 summa-rizes data from eight hearts. After adenosine, the timeconstant of GCVF decreased significantly. The resis-tance distal to CIM (RposT) and the total resistance(RPRE+RPOST) decreased significantly. The ratio of RPOSTto RPRE+RPOST decreased from 0.35±0.02 to 0.23±0.02(P<.01), indicating that the relative location of CIMshifted distally after adenosine. The magnitude of CIMincreased significantly from 0.09±0.01 to 0.24±0.2mL mm Hg`* 100 g`.
A250
200
c
c-
ILWIto
150
100
50
25 50 75Coronary Pressure mm Hg
TABLE 2. Effects of Adenosine-induced Vasodliation onthe Localization and the Magnitude of IntramyocardialCoronary Capacitance
Before AfterAdenosine Adenosine P
RPOST,mm Hg . min- . mLV1 0.42±0.09 0.1 1+0.01 <.01
RPRE,mm Hg . min1 . mL-1 0.73±0.08 0.37+0.04 <.01
RPRE+ RPOST,mm Hg* min- . mL-1 1.15+0.17 0.48+0.06 <.01
RposT/(RPRE+RposT) 0.35±0.02 0.23+0.02 <.01Tc, s 1.66+0.06 1.43±0.05 <.05
CIM-GCV, mL/mm Hg 0.06+0.01 0.19+0.02 <.001
CIM-LV, mL.mm Hg-1 * 100 g-' 0.09+0.01 0.24±0.02 <.001
RPOST and RPRE indicate the precapacitance and postcapaci-tance coronary resistance, defining the localization of the intra-myocardial capacitance by the ratio of RPOST/(RPRE+RPOST); Tc,time constant of the decay of the great cardiac vein flow;CIM-GCV, magnitude of the intramyocardial capacitance calcu-lated from Tc and Rposr; and CIM-LV is the capacitance normal-ized by the total left ventricular mass.
Perfusion Pressure StudyFig 6A shows the effects of perfusion pressure on
coronary pressure-venous flow relations. Perfusionpressure before the occlusion varied from approxi-mately 100 to 40 mm Hg. Vasodilation was induced byadenosine infusion (250 jig/min). The horizontal por-tion shifted downward with decreased perfusion pres-sure; however, the slope of the second decline portionsremained unchanged, indicating that RPOST did notchange. Fig 6B shows superimposed tracings of GCVF
B
100
250
200
150
100
50
0 _c
lsec
FIG 5. A, Coronary pressure-venous flow relations before and after adenosine vasodilation determined from coronaryartery in-flow occlusion experiments as illustrated in Fig 4. After vasodilation, the slope of the linear decline portionincreases substantially. B, Superimposed great cardiac vein flow (GCVF) recording after coronary occlusion. (See text fordetail.)
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

2934 Circulation Vol 88, No 6 December 1993
A
300 ,
250c
P4a
&LU3
200 h
150 I
100
50
0 0
a
-4-4a
I'
2L
20 40 so so 10oCORONARY PRESSURE m He
350
300
250
200
150
100
50
0
lsec
FIG 6. A, Coronary pressure-venous flow relations when the preceding coronary perfusion pressure was changed fromapproximately 100 to 40 mm Hg. Coronary vessels were maximally vasodilated by adenosine infusion. Note that theslopes of the second decline portion are not altered by these changes in perfusion pressure. B, Superimposed tracingsof great cardiac vein flow (GCVF) versus time. (See text for detail.)
decay. The tracings of the gradual decline portion werenearly parallel, and the time constant appeared to beidentical. Table 3 summarizes data from four heartswhen CPP was varied from 96±6 to 60±1 mm Hg. Themagnitude of CIM was 0.19±0.01 (high perfusion pres-sure) and 0.17±0.01 (low perfusion pressure). The ratioof RPOST to RPRE+RPOST was not changed, indicating noshift of the localization of CIM.
Left Ventricular Diastolic Volume StudyFig 7A shows the coronary pressure-venous flow rela-
tions at the different LV diastolic pressures produced by
TABLE 3. Effects of Coronary Perfusion Pressure onthe Localization and the Magnitude of IntramyocardialCoronary Capacitance
Coronary PerfuslonPressure, mm Hg
High (96±6) Low (60±11) p
RPOST,mm Hg * min-' . mL-1 0.11±0.02 0.13±0.02 NS
RPRE .mm Hg. min-1 - mL-1 0.29±0.04 0.31±0.04 NS
RPRE+ RPOST,mm Hg. min-1 . mL~1 0.40±0.07 0.44±0.09 NS
RposT/(RPRE+RposT) 0.28±0.01 0.29±0.03 NS
Tc, s 1.50±0.10 1.42±0.07 NSCIM-GCV, mL/mm Hg 0.15±0.02 0.12±0.05 NSCIM-LVmL- mm Hg-1 * 100 g~' 0.19±0.01 0.17±0.04 NS
RPOST and RPRE indicate the precapacitance and postcapaci-tance coronary resistance, defining the localization of the intra-myocardial capacitance by the ratio of RPOST/(RPRE+RPOST); Tc,time constant of the decay of the great cardiac vein flow;CiM-GCV, magnitude of the intramyocardial capacitance calcu-lated from Tc and RPOST; and CIM-LV is the capacitance normal-ized by the total left ventricular mass.
changing LV balloon volume. In this example, LV dia-stolic pressure was increased from 1 to 24 mm Hg. Thereciprocal slope of the second decline portion (RPOST)increased from 0.10 to 0.16 mm Hg . min' * mL` at thehigher preload. Fig 7B shows the superimposed tracings ofGCVF after the occlusion. The two tracings were nearlyidentical in the gradual decrease portion. Table 4 summa-rizes data from eight hearts when LV balloon volume wasincreased to raise diastolic pressure during long diastolesfrom 2±0.1 to 25±1 mm Hg. The coronary resistancedistal to the capacitance (RPOST) increased significantlyfrom 0.11±0.01 to 0.16±0.02 mmHg .min- mL-'. Onthe other hand, coronary resistance proximal to the ca-pacitance (RPRE) did not change. The magnitude of CIMdecreased significantly from 0.24±0.03 to 0.18±0.03mL* mm Hg-1 * 100 g`. The ratio of RPOST to RpRE+RposTwas not increased significantly.
Left Ventricular Diastolic Chamber Stiffness StudyDiastolic hemodynamic data of this protocol are
summarized in Table 5 (n=6). During hypoxic coronaryperfusion for 25 to 40 minutes, LV diastolic pressureincreased from 11±1 to 28±1 mm Hg (P<.01) despiteconstant LV balloon volume. Fig 8 shows the relationbetween end-diastolic pressure and LV balloon volumein a representative case. After 30 minutes of hypoxiccoronary perfusion, the LV diastolic pressure-volumerelation shifted upward and its slope became steeper,indicating that an increase in diastolic myocardial stiff-ness raised the isovolumic LV diastolic pressure. Then,LV diastolic pressure was adjusted back to 10±1mm Hg (Table 5) by reducing LV balloon volumeduring continued hypoxic perfusion to isolate an effectof increased LV diastolic pressure per se.
Fig 9A shows the coronary pressure-venous flowrelations under the three conditions of this protocol.Tracing I is the control and was obtained immediatelyafter the initiation of hypoxic coronary perfusion, be-fore isovolumic LV diastolic pressure had changed.
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

Watanabe et al Intramyocardial Coronary Capacitance
300
250
2001-
1501
100 f
25
50
W0 75
a300
250
200
100
50
100 lsecCORONARY PRESSURE m Hg
FIG 7. A, Coronary pressure-venous flow relations when left ventricular balloon volume was increased sufficiently toproduce a rise in left ventricular diastolic pressure (LVDP) from 1 to 24 mm Hg. The relation shifted to the right, and theslope of the second decline portion decreased. B, Superimposed tracings of great cardiac vein flow (GCVF) for the sameexperiment.
Tracing II was obtained during hypoxic perfusion whenLV diastolic pressure had increased to 25 mm Hg, duepresumably to an increase in myocardial stiffness. Trac-ing III was obtained after LV diastolic pressure wasadjusted to 10 mm Hg (control level) by decreasing LVballoon volume. The reciprocal slope of the seconddecline portion (RposT) changed from 0.11 (tracing I,control) to 0.32 (tracing II, increased stiffness) and 0.25mm Hg* mink rmL-1 (tracing III, adjusted LV diastolic
TABLE 4. Effects of Altered Left Ventricular DiastolicVolume on the Localization and the Magnitude of theIntramyocardial Coronary Capacitance
Left Ventricular DiastolicVolume, mm Hg
Low (2±0.1) High (25±11) PRPOST,mm Hg . min1 . mLU1 0.11±0.01 0.16±0.02 <.05
RPRE,mm Hg. min-1 * mL-1 0.38±0.04 0.39±0.05 NS
RPRE+ RPOST,mm Hg . min-1 - mL-1 0.49±0.06 0.55±0.06 NS
RposT/(RPRE+ Rposr) 0.24±0.04 0.29±0.03 NS
Tc, s 1.44±0.08 1.49±0.09 NS
CIM-GCV, mL/mm Hg 0.19±0.02 0.12±0.03 <.05
CIM-LV,mL. mm Hg-' . 100 g-' 0.24±0.03 0.18±0.03 <.05
RposT and RPRE indicate the precapacitance and postcapaci-tance coronary resistance, defining the localization of the intra-myocardial capacitance by the ratio of RPOsT/(RPRE+RPOST); Tc,time constant of the decay of the great cardiac vein flow;CIM-GCV, magnitude of the intramyocardial capacitance calcu-lated from Tc and RPOST; and CIM-LV is the capacitance normal-ized by the total left ventricular mass. Left ventricular balloonvolume was increased to raise left ventricular diastolic pressurefrom 2±0.1 to 25±1 mm Hg.
pressure). Fig 9B shows the superimposed tracings ofGCVF versus time after the coronary occlusion. Thetime constant of these tracings appeared unchanged.Table 6 summarizes the capacitance and resistance dataof this protocol. The magnitude of CIM was decreasedfrom 0.32±0.12 (control) to 0.17±0.04 (increased stiff-ness) and 0.16±0.03 mL- mm Hg-l * 100 g` (adjustedLV diastolic pressure). RPOST increased significantlyfrom 0.10±0.02 to 0.25+±0.04 (increased stiffness) and0.21±0.03 mm Hg* min' mL-1 (adjusted LV diastolicpressure). The change in RPRE was not significant. Theratio of RPOST to RPRE+RPOST increased from 0.21±0.05(control) to 0.36+0.06 (increased stiffness) and0.33+±0.05 (adjusted LV diastolic pressure). A decreasein LV diastolic pressure to the control level (adjustedLV diastolic pressure) appeared to reduce the totalcoronary resistance (RPRE+RPOST) slightly (not statisti-cally significant) and had no effect on the other param-eters we measured.
DiscussionWe examined the localization and magnitude of ca-
pacitive function of the intramyocardial coronary ves-
sels (intramyocardial coronary capacitance, CIM), at-tempting to characterize effects of coronary vasculartone and extravascular compression. Coronary vasodi-lation increased the magnitude of CIM and shifted therelative localization of CIM to the distal portion in thecoronary vascular tree. In contrast, changes in CPP hadlittle effect on the magnitude and localization of CIM.Increased LV diastolic volume decreased the magnitudeof CIM without affecting the relative localization of CIM,whereas increased LV diastolic chamber stiffness in-duced by hypoxic perfusion decreased the magnitude ofCIM and shifted the localization of CIM to the proximalportion of the coronary vascular tree.
A
c-4
a
Ua
IL
U
Low LVDP
High LVDP
. a -A-
2935
1
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

2936 Circulation Vol 88, No 6 December 1993
TABLE 5. Diastolic Hemodynamic Data With Increased Left Ventricular DiastolicChamber Stiffness Caused by Hypoxic Perfusion
Control Hypoxic Perfusion P* Adjusted LVDP P* PtLVDP, mm Hg 11±1 28±1 <.01 10±1 NS <.01Perfusion pressure, mm Hg 67±2 74±3 <.05 73±4 NS NSLeft coronary flow, mUmin 231±40 184±33 <.01 195±36 <.01 NSGCVflow, mL/min 114±14 83±13 <.05 88±14 <.05 NSLVDP indicates left ventricular diastolic pressure; and GCV, great cardiac vein.*P difference from control; tP difference from increased LVDP study. (See text for detail.)
Methodological ConsiderationsIn the present study, we calculated intramyocardial
coronary capacitance assuming a particular lumped RCmodel (Fig 1). The localization of CIM was defined bythe ratio between precapacitance and postcapacitancecoronary resistance.3,'6-'8 However, transmural pressureacross the LV wall most likely produces a gradient oftissue pressure from the endocardium to the epicar-dium.19,20 This gradient may cause a different effect oncoronary vessels, depending on their depth.2' In thisregard, the lumped model may not be adequate for aquantitative analysis. Therefore, LV diastolic pressurewas set at a low level to minimize transmitted intramyo-cardial pressure'9 in the vasodilation and CPP studies.In the LV diastolic volume and chamber stiffness stud-ies, LV diastolic pressure increased significantly. Thus,we need to interpret carefully the results from theseprotocols, although a qualitative interpretation mightstill be possible. We calculated the magnitude andlocalization of CIM using a lumped model in diastole;however, one may not use the lumped model to simulatethe systolic behavior of CIM because of substantialheterogeneity of coronary volume change through themyocardial layers in systole.22,23The assumption that PC=PDIS may be acceptable
when there is no significant pressure discontinuity (wa-terfall) between Pc and PDIS. Although this possibility isundeniable, myocardial microcirculatory studies havenever observed actual vessel collapse at the zero-flowpoint. In previous studies concerning coronary capaci-tance, this potential discontinuity was not used. Thus,Spaan et a13 assessed a decay curve of PDIS after
LVEDP mmHg
70
LV Volume ml
FIG 8. The relation between left ventricular (LV) end-di-astolic pressure and LV balloon volume during hypoxicperfusion. The LV diastolic pressure-volume relation dur-ing hypoxia is steeper than the control, indicating thatmyocardial stiffness is increased in this protocol.
coronary occlusion to estimate precapacitance coronaryresistance, and Lee et al16 used a kind of diode distal toRPOST. The location of waterfalls is another controversythat remains to be clarified.That the coronary pressure-venous flow relation ap-
peared to be linear in its decline portion may not provethat there is a single linear process at work. Hanley eta124 reported significant dependency of coronary resis-tance on both inflow and outflow pressure. This prob-lem may be a general problem when we assess coronarycirculation in terms of coronary resistance based onOhm's law. In the present study, the pressure changewhere the pressure-flow relation was analyzed was lessthan 15 mm Hg (Hanley et a124 used a driving pressureof 10 to 30 mm Hg for calculating coronary resistance).We believe that this should minimize a change incoronary resistance caused by an alteration of coronarypressure.Another assumption of this study is that the profile of
the venous flow pattern during a long diastole is uniformin all the coronary outflow veins. This assumption hasbeen used by others in the studies of coronary capaci-tance67 using coronary venous flow analysis, since it isimpossible to measure phasic total coronary venous flowbecause of the multiplicity of venous pathways in thedog.25The calculated magnitude of CIM in this study was
0.09+0.01 before vasodilation with adenosine and0.24±0.2 mL mm Hg-' 100 g' after vasodilation.These values are nearly identical to values reported byothers; that is, 0.07 mL * mm Hg'* 100 g` before vaso-dilation,3 0.091 mL* mm Hg1. 100 g` before vasodila-tion,3 and 0.07±0.05 and 0.22±0.03 mL. mm Hg`. 100g-1 before and after vasodilation,4 respectively. Al-though some investigators1626 have reported substan-tially lower values, these values were calculated bycoronary inflow (ie, arterial) pressure and flow analysisand might reflect mostly epicardial coronary arterialcapacitance.3'17An advantage of the present method is that postcapac-
itance coronary resistance could be calculated directlyfrom data obtained in a single diastole. Therefore, we canassess the localization of CIM (the distribution of preca-pacitance and postcapacitance coronary resistance) undervarious conditions of coronary tone and extravascularcompressive factors. This localization of CIM may indicatewhich part of the coronary bed plays a functionally dom-inant role in total coronary capacitance.
Effect of Vasodilation on Magnitude andLocalization of CIMThe magnitude of CIM increased from 0.09±0.01 to
0.24±0.2 mL * mm Hg1* 100 g` after vasodilation with
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

Watanabe et al Intramyocardial Coronary Capacitance
75 100
B100
I
50 E
0 L _i
lsec
FIG 9. A, Coronary pressure-venous flow relations with altered left ventricular (LV)-diastolic chamber stiffness producedby hypoxic perfusion. Relation is control (LV diastolic pressure, 10 mm Hg). Relation 11 was obtained during hypoxicblood perfusion after LV diastolic pressure at constant volume had risen to 25 mm Hg. Relation Ill was obtained byreducing LV balloon volume to return LV diastolic pressure to 10 mm Hg during continued hypoxic perfusion. The slopeof the relation decreased from I to 11. B, Superimposed tracings of great cardiac vein flow (GCVF).
adenosine. These values imply that intramyocardialvessels could store 1.8 to 4.8 mL. 100 g per beat of thecoronary inflow blood, even if the transmural pressure
of the coronary capacitance vessels changed by only 20mm Hg between systole and diastole. Thus, this largeintramyocardial coronary capacitance supports the in-tramyocardial pump action concept.3 Epicardial coro-
nary arterial capacitance (0.0022 mL * mm Hg`* 100g-1)3 cannot store blood in diastole because this capac-
itance is being discharged.Although we do not have direct observations to
determine precise anatomic localization of coronary
capacitance, we are able to speculate on the localizationaccording to the resistance distribution in the coronaryvascular tree reported by Chilian et al.27 Before vasodi-lation, approximately 25% of total coronary resistance
is distributed in the coronary arteries and arterioles thatare more than 170±40 gm in diameter. Less than 10%of the resistance is distributed in the venules and veinsthat are more than 150±30 ,am in diameter. Aftervasodilation, approximately 40% of the resistance isdistributed in arterioles and arteries of the same size,and 30% of the resistance is distributed in venules andveins of the same size. The top panel of Fig 10 showsthis distribution schematically. The present results mayindicate that intramyocardial coronary capacitance islocated mainly between coronary arterioles (170±40gm) and venules (150±30 gm) when coronary tone isintact. After vasodilation, the distribution of coronaryresistance indicates that intramyocardial coronary ca-
pacitance redistributed to the distal portion and mightbe located mainly at the small venules and/or small
TABLE 6. Effects of Increased Left Ventricular Diastolic Chamber Stiffness on theLocalization and Magnitude of Intramyocardial Coronary Capacitance
Control Hypoxic Perfusion P Adjusted LVDP P
RPOST, mm Hg * min1 * mL-' 0.11±0.02 0.25±0.04 <.01 0.21±0.03 <.01
RPRE, mm Hg -min-' *mL-1 0.42±0.05 0.45±0.05 NS 0.46±0.07 NS
RPRE+RPOST, mm Hg* min1 * mL-' 0.52±0.06 0.70±0.08 <.05 0.67±0.08 <.05
RposT/(RPRE+RPoST) 0.21 ±0.05 0.36±0.06 <.05 0.33±0.05 <.05
Tc, s 1.70±0.31 2.19±0.35 NS 1.82±0.24 NS
CIM-GCV, mL/mm Hg 0.18±0.11 0.09±0.06 <.05 0.08±0.04 <.05
CIM-LV, mL. mm Hg-1 100 g-' 0.32±0.12 0.17±0.04 <.05 0.16±0.03 <.05
LVDP indicates left ventricular diastolic pressure; RPOST and RPRE indicate the precapacitance andpostcapacitance coronary resistance, defining the localization of the intramyocardial capacitance bythe ratio of RPOST/(RPRE+RPOST); Tc .time constant of the decay of the great cardiac vein flow; CiM-GCV,magnitude of the intramyocardial capacitance calculated from Tc and RPOSr; and CM-LV is thecapacitance normalized by the total left ventricular mass. P values show statistical difference fromcontrol. (See text for detail.)
A200
150 hc-4E%.4.-3
aI4IL'p
C-
100
50
I
l~~~~~~~~~~lIII
#ir~~~~~~~~~I
00 25 50
CORONARY PRESSURE - Hg
2937
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

2938 Circulation Vol 88, No 6 December 1993
Coronary Reslitance distribution170±40 pum 150±30 pm
Artery _ Vein
Intact 25% '10%
Vasodliation 40% 30%
Intact RPRE C0M 0.09 RpOST66% Fl
0.24
Vasodliation 77% 23%
ExtravwCompro
ascular 0.16
*esalon an s 33%
FIG 10. Top, Schematic presentation of coronary resis-tance distribution reported by Chilian et al.27 Bottom,Effects of vasodilation (Table 2) and increased extravas-cular compression (hypoxic perfusion-induced rise inmyocardial stiffness; Table 6) on the magnitude andlocalization of intramyocardial coronary capacitance (CIMin mL mm Hg-1 * 100 g-'). The precapacitance andpostcapacitance resistance (RPRE and RPOST) are pre-sented as percent of the total resistance.
veins, as shown schematically in Fig 10. Although wecannot clarify the mechanism of the changes in themagnitude and localization of the intramyocardial cor-onary capacitance, it is likely that an increase in venouspressure after vasodilation27 may play some role in thesechanges. Thus, the venous system, which should bemore compliant than the arterial system,3 would cometo play a greater role in the intramyocardial coronarycapacitance after vasodilation because of increased di-astolic transmural pressure of the venous system.Lee and Downey16 reported that the ratio of the
postcapacitance resistance to the total resistance de-creased from 0.63+0.05 to 0.43 ±0.04 after vasodilation.Although our data showed a directionally similarchange (0.35±0.02 and 0.23±0.02 before and aftervasodilation, respectively), their absolute values wereclearly higher than ours, implying that the localizationof the intramyocardial coronary capacitance might dis-tribute in the more proximal portion of coronary tree(Fig 10). These differences might be caused in part bymethodological differences. They calculated precapaci-tance resistance from the coronary arterial pressure-flow relation during a rapid change in CPP, withoutdistinguishing the epicardial coronary capacitance fromthe intramyocardial coronary capacitance. Therefore,the slope of coronary arterial pressure-flow relationmay have been overestimated,12,2829 resulting in under-
estimation of the precapacitance resistance and overes-timation of the resistance ratio mentioned above.Spaan et a13 reported that the ratio (RPRE/total resis-
tance) was 0.63 in intact hearts from an analysis ofperipheral pressure distal to coronary occlusion. Theirvalues and ours (0.65 before adenosine) are similardespite different approaches. They regarded the decaycurve of peripheral coronary pressure between 0.5 and3 seconds after occlusion as being determined by dis-charge of intramyocardial coronary capacitance into thevenous direction. In the present study, the second lineardecline of the pressure-flow relation started approxi-mately 0.5 second after occlusion (Fig 4), and weapplied a linear fit to this declining portion. Thus, ourmethod of assessing Pc is similar to that of Spaan et alin terms of using a relatively late phase of PDIS; theeffects of the epicardial coronary capacitance should beminimized using these approaches. In this regard, bothgroups have obtained similar values concerning RPREand RPOST distribution.
Effect of Perfusion Pressure on IntramyocardialCoronary CapacitanceThe present results (Fig 6 and Table 3) did not show
any changes in the magnitude and localization of intra-myocardial coronary capacitance when CPP before theocclusion was varied over a wide range (40 to 100mm Hg). Some investigators26 have reported a signifi-cant dependence of coronary capacitance on perfusionpressure. However, their measurements were based oncoronary artery input pressure and inflow, and againthey might reflect the capacitance of the relatively largearteries in which intraluminal pressure might vary di-rectly with CPP. Kajiya et als reported significant per-fusion pressure dependency of intramyocardial coro-nary capacitance derived from GCVF analysis. As onepotential explanation of the difference between theirfinding and ours, they included epicardial coronarycapacitance in the coronary capacitance that they pre-sented. In contrast, Salisbury et a130 reported a near-linear relation between coronary blood volume andperfusion pressure in the range from 30 to 120 mm Hg.Thus, this issue remains controversial depending on themethod of assessing coronary capacitance.
If intramyocardial coronary capacitance is distributedmainly distal to arterial resistance vessels, perfusionpressure might have little effect on the magnitude ofintramyocardial capacitance because a change in coro-nary arterial pressure would be greatly attenuated bythe high coronary resistance of precapacitance vessels.In our results, the second linear portion of the coronarypressure-venous flow relation started from a coronarypressure of less than 30 mm Hg (Fig 6). Thus, wecalculated the magnitude of CIM in the perfusion pres-sure range that most likely corresponds to the actualpressure within CIM-related intramyocardial vessels. Inthis regard, we have reported that coronary venouspressure was an important determinant of the coronaryerectile effect.31 A change in coronary venous pressuremay be a strong determinant of intramyocardial bloodvolume because venous pressure may transmit directlyto the CIM-related vessels through low resistance ofpostcapacitance vessels.
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

Watanabe et al Intramyocardial Coronary Capacitance 2939
Effect of Left Ventricular Diastolic Volume onIntramyocardial Coronary Capacitance
Increased ventricular diastolic volume should trans-mit an increased force into the myocardial wall19,20 andmay change the magnitude and localization of intramyo-cardial coronary capacitance by extravascular compres-sion. The present data (Table 4) show that the postca-pacitance resistance (RPOST) increased significantly withincreased LV preload and the magnitude of CIM de-creased significantly. Precapacitance coronary resis-tance (RPRE) did not change, and the ratio of RPOST toRPRE+RPOST increased slightly. Thus, the effect of in-creased intraventricular volume was heterogenous andappeared to be greater on postcapacitance resistancevessels (which may correspond to the venules and smallveins) than on precapacitance resistance vessels. Someinvestigators32-34 have reported that increased LV pre-load changed the slope of the diastolic coronary arterialpressure-flow relation by less than 20% when LVdiastolic pressure was changed within nearly the samerange (0 to 30 mm Hg), and CPP was nearly in the samerange (60 to 70 mm Hg). This may support the conclu-sion that increased ventricular preload has only smalleffects on the arterial resistance vessels in thesesituations.
Effect of Left Ventricular Diastolic Chamber Stiffnesson Intramyocardial Coronary CapacitanceWhen LV diastolic chamber stiffness was increased by
hypoxic perfusion, postcapacitance resistance increasedsignificantly; however, precapacitance resistance did notchange (Table 6), and the magnitude of CIM decreasedsignificantly. These changes were still significant afteradjustment of LV diastolic pressure to the control levelby decreasing LV balloon volume, indicating that anincrease in LV diastolic pressure per se was not a majordeterminant of this change. Most likely, the factorsresponsible for the increased myocardial stiffness, suchas impaired diastolic myocardial relaxation and/or myo-cardial edema, result in an important extravascularcompressive factor. The results indicate that increasedmyocardial stiffness reduced intramyocardial coronarycapacitance and shifted it to a relatively proximal por-tion (Fig 10) of the coronary vascular bed. Thus,increased myocardial stiffness mainly affects postcapac-itance resistance vessels and the intramyocardial capac-itance vessels (which may correspond to venules andsmall veins) and has qualitatively similar effects oncoronary vessels as does an increase in LV preload. Inthe present study, both impaired diastolic relaxationand interstitial edema may be responsible for an in-crease in ventricular myocardial stiffness and shouldincrease extravascular compression in pathophysiologi-cal conditions such as severe ischemia and/or reperfu-sion. We were unable to separate these two effects inthe present study.Although the hypoxic perfusion of our experiments
may affect the tone of coronary vessels, this did notappear to have had a major role in the present resultssince the precapacitance resistance (which probablycorresponds roughly to arterial resistance vessels) didnot increase with hypoxic perfusion (Table 6) despitethe abundant smooth muscle of the arterial resistancevessels. In fact, the precapacitance resistance decreased
after adenosine-induced vasodilation. Nevertheless, dif-ferential effects of hypoxia on arterial versus venoustone may have occurred and could account in part forthe decline in CIM and increase in RPOST during hypoxicperfusion.The present results indicate that the distribution of
precapacitance and postcapacitance coronary resis-tance is altered after vasodilation and extravascularcompression. This redistribution of resistance may playan important role in determining coronary diastolicinflow. Thus, diastolic coronary flow appears to occuractually between the coronary ostium and the site of theintramyocardial coronary capacitance. Therefore, pre-capacitance coronary resistance may be the effectivediastolic coronary resistance rather than the total cor-onary resistance. In the next step, we should apply thismodel to the systolic period to assess whether intramyo-cardial capacitance can explain the systolic behavior ofcoronary circulation.
In conclusion, the effects of vasodilation and extravas-cular compression on the coronary circulation werecharacterized by changes in the magnitude and localiza-tion of intramyocardial coronary capacitance. The cor-onary pressure-venous flow relation presented in thisstudy should provide a useful method for the assessmentof factors influencing the interaction of CBF, resistance,and capacitance.
AcknowledgmentsSupported in part by a grant (RO-1-HL-44431) from the
National Heart, Lung, and Blood Institute and by NationalResearch Service Award (M.J.L.) HL-07870-02. We thank MrAlvin Franklin for his technical assistance and Ms PatriciaAllen for her excellent secretarial help.
References1. Stein PD, Badeer HS, Schuetle WH, Glaser JF. Pulsatile aspects of
coronary sinus blood flow in closed-chest dogs. Am Heart J. 1969;78:331-337.
2. Kajiya F, Tsujioka K, Goto M, Wada Y, Tadaoka S, Nakai M,Hiramatsu 0, Ogasawara Y, Mito K, Hoki N, Tomonaga G. Eval-uation of phasic blood flow velocity in the great cardiac vein by alaser doppler method. Heart Vessels. 1985;1:16-23.
3. Spaan JAE. Coronary diastolic pressure-flow relationship and zeroflow pressure explained on the basis of intramyocardial com-pliance. Circ Res. 1985;56:293-309.
4. Chilian WM, Marcus ML. Coronary venous outflow persists aftercessation of coronary arterial inflow. Am J Physiol. 1984;247:H984-H990.
5. Kajiya F, Tsujioka K, Goto M, Wada Y, Chen XL, Nakai M,Tadaoka S, Hiramatsu 0, Ogasawara Y, Mito K, Tomonaga G.Functional characteristics of intramyocardial capacitance vesselsduring diastole in the dog. Circ Res. 1986;58:476-485.
6. Harrison DG, Florentine MS, Brooks LA, Cooper SM, MarcusML. The effect of hypertension and left ventricular hypertrophy onthe lower range of coronary autoregulation. Circulation. 1988;77:1108-1115.
7. Vanhoutte PM, Luscher TF, Graser T. Endothelium-dependentcontractions. Blood Vessels. 1991;28(1-3):74-83.
8. Harrison DG, Marcus ML, Dellsperger KC, Lamping KG,Tomanek RJ. Pathophysiology of myocardial perfusion in hyper-tension. Circulation. 1991;83(suppl 3):III-14-III-18.
9. Bronzwaer JGF, de Bruyne B, Ascoop CAPL, Paulus WJ. Com-parative effects of pacing-induced and balloon coronary occlusionischemia on left ventricular diastolic function in man. Circulation.1991;84:211-222.
10. Wyman RM, Farhi ER, Bing OHL, Johnson RG, Weintraub RM,Grossman W. Comparative effects of hypoxia and ischemia in theisolated, blood perfused dog heart: evaluation of left ventriculardiastolic chamber distensibility and wall thickness. Circ Res. 1988;64:121-128.
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

2940 Circulation Vol 88, No 6 December 1993
11. Caroll JD, Hess OM, Hirzel HO, Krayenbuehl HP. Exercise-induced ischemia: the influence of altered relaxation on earlydiastolic pressures. Circulation. 1983;67:521-528.
12. Apstein CS, Mueller M, Hood WB Jr. Ventricular contracture andcompliance changes with global ischemia and reperfusion and theireffect on coronary resistance in the rat. Circ Res. 1977;41:206-217.
13. Gaascb WH, Bing OHL, Franklin A, Rhodes D, Bernard SA,Weintraub RM. The influence of acute alterations in coronaryblood flow on left ventricular diastolic compliance and wallthickness. Eur J Cardiol. 1978;7(suppl):147-161.
14. Steiner C, Kovalik ATW. A simple technique for production ofchronic heart block in dogs. JAppl Physiol. 1968;25:631-635.
15. Dole WP, Bishop VS. Influence of autoregulation and capacitanceon diastolic coronary artery pressure-flow relationships in the dog.Circ Res. 1982;51:261-270.
16. Lee J, Chambers DE, Akizuki S, Downey JM. The role of vascularcapacitance in the coronary arteries. Circ Res. 1984;55:751-762.
17. Kajiya F, Tsujioka K, Ogasawara Y, Wada Y, Hiramatsu 0, GotoM, Nakai M, Tadaoka S, Matsuoka S, Sha Y. Effect of packed cellvolume on diastolic coronary artery pressure-flow relations in thedog. Cardiovasc Res. 1988;22:545-554.
18. Vergroesen I, Noble MIM, Spaan JAE. Intramyocardial bloodvolume changes in first moments of cardiac arrest in anesthetizedgoats. Am J Physiol. 1987;253:H307-H316.
19. Archie JP Jr. Transmural distribution of intrinsic and transmittedleft ventricular diastolic intramyocardial pressure in dogs. Car-diovasc Res. 1978;12:255-272.
20. Heineman FW, Grayson J. Transmural distribution of intramyo-cardial pressure measured by micropipette technique. Am JPhysiol. 1985;249:H1216-H1223.
21. Ellis AK, Klocke FJ. Effects of preload on the transmural distri-bution of perfusion and pressure-flow relationships in the caninecoronary vascular bed. Circ Res. 1980;46:68-77.
22. Goto M, Jansen CMA, Stork MM, Flynn AE, Coggings DL,Husseini W, Hoffman JIE. Effects of myocardial contraction onintramyocardial vessels. Circulation. 1989;80(suppl 2):II-212.
23. Judd RM, Levy BI. Effects of barium-induced cardiac contractionon large- and small-vessel intramyocardial blood volume. Circ Res.1991;68:217-225.
24. Hanley FL, Messina LM, Grattan MT, Hoffman JIE. The effect ofcoronary inflow pressure on coronary vascular resistance in theisolated dog heart. Circ Res. 1984;54:760-772.
25. Marcus ML. The Coronary Circulation in Health and Disease. NewYork: McGraw-Hill; 1983:15-21.
26. Canty JM Jr, Klocke FJ, Mates RE. Characterization ofcapacitance-free pressure-flow relationships during single diastoles indogs using an RC model with pressure dependent parameters. CircRes. 1987;60:273-282.
27. Chilian WM, Layne SM, Klausner EC, Eastham CL, Marcus ML.Redistribution of coronary microvascular resistance produced bydipyridamole. Am J PhysioL 1989;256:H383-H390.
28. Eng C, Jentzer JH, Kirk ES. The effects of the coronary capac-itance on the interpretation of diastolic pressure-flow rela-tionships. Circ Res. 1982;55:10-17.
29. Klocke FJ, Mates RE, Canty JM, Ellis AK. Coronary pressure-flowrelationships: controversial issues and probable implications. Circ Res.1985;56:310-323.
30. Salisbury PF, Cross CE, Rieben PA. Physiological factors influ-encing coronary blood volume in isolated dog hearts.Am J Physiol.1961;200:633-636.
31. Watanabe J, Levine MJ, Bellotto F, Johnson RG, Grossman W.Effects of coronary venous pressure on left ventricular diastolicdistensibility. Circ Res. 1990;67:923-932.
32. Aversano T, Klocke FJ, Mates RE, Canty JM Jr. Preload-inducedalterations in capacitance-free diastolic pressure-flow relationship.Am J Physiol. 1984;246:H410-H417.
33. Watanabe J, Maruyama Y, Satoh S, Keitoku M, Takishima T.Effects of the pericardium on the diastolic left coronarypressure-flow relationship in the isolated dog heart. Circulation.1987;75:67-675.
34. Satoh S, Watanabe J, Keitoku M, Itoh N, Maruyama Y, TakishimaT. Influences of pressure surrounding the heart and intracardiacpressure on the diastolic coronary pressure-flow relation in excisedcanine heart. Circ Res. 1988;63:788-797.
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from

J Watanabe, M J Levine, F Bellotto, R G Johnson and W Grossmanisolated dog hearts.
Left ventricular diastolic chamber stiffness and intramyocardial coronary capacitance in
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1993 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.88.6.2929
1993;88:2929-2940Circulation.
http://circ.ahajournals.org/content/88/6/2929World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 18, 2018
http://circ.ahajournals.org/D
ownloaded from













![1210 DIASTOLIC Hypertension[2]](https://img.pdfslide.us/doc/110x75/577cdd4a1a28ab9e78acb724/1210-diastolic-hypertension2.jpg)