Embed Size (px)
Citation preview

Left Stellectomy in the Prevention of VentricularFibrillation Caused by Acute Myocardial Ischemia
in Conscious Dogs with Anterior Myocardial Infarction
PETER J. SCHWARTZ M.D., AND H. LOWELL STONE, PH.D.
SUMMARY The potential of left stellectomy in reducing the incidence of ventricular fibrillation associatedwith acute myocardial ischemia was investigated in a new animal model for sudden death. Thirty-two dogs hadan anterior myocardial infarction produced by ligation of the left descending coronary artery. One week laterthey were randomly allocated to a control or to an experimental group that underwent left stellectomy. Onemonth after ligation while the dogs were conscious, a balloon occluder previously positioned around the cir-cumflex coronary artery was inflated and the ensuing coronary occlusion was maintained for 10 minutes. Ven-tricular fibrillation occurred in 11 of 17 (65%) control dogs, compared with five of 15 (33%) (p < 0.05) in theexperimental group. Among the survivors the incidence of arrhythmias was less in the experimental group com-pared with the control group. Infarct size (21 ± 2% vs 20 ± 2%), resting heart rate (143 beats/min vs 127beats/min) and QT, (347 ± 11 msec vs 349 13 msec) were similar between control and experimental groups.The dogs that died had a greater increase in heart rate at 1 minute postocclusion than survivors and also hadsignificantly longer QT intervals.Our study indicates that left stellectomy exerts a major protective effect in reducing the incidence of ven-
tricular fibrillation when conscious dogs with a previous anterior myocardial infarction undergo acute myocar-dial ischemia. This simple and safe surgical procedure may be considered for a clinical trial in subgroups ofpatients with ischemic heart disease at very high risk for sudden death.
SUDDEN DEATH is most often caused by ven-tricular fibrillation.' The importance of neuralmechanisms, particularly the sympathetic nervoussystem, in precipitating ventricular fibrillation hasbeen shown experimentally, confirmed clinically and isgenerally accepted.2 7 Therefore, a rational approachtoward the prevention of sudden death is representedby interventions that increase electrical stability andinterfere with the effects of increases in sympatheticactivity. We propose that left stellectomy may be oneof these interventions.We have shown that ablation of the left stellate
ganglion results in a reduced incidence of arrhythmiaseither directly or indirectly, by changes in hemo-dynamic variables relevant to the genesis of cardiacarrhythmias. Briefly, left stellectomy reduces the inci-dence of arrhythmias associated with transient coro-nary occlusion,8 markedly increases the threshold forventricular fibrillation,9 prolongs the ventricular re-fractory period,'0 and increases the capability of thecoronary bed to dilate at rest" and during exercise.12Two considerations have guided the design of our
experimental model: (1) Patients with a previousanterior myocardial infarction, when challenged by anew episode of acute ischemia, represent one of thegroups at very high risk for sudden death. (2) If the
From the Istituto di Ricerche Cardiovascolari e Centro RicercheCardiovascolari C.N.R., Universita di Milano, Milan, Italy, andthe Department of Physiology and Biophysics, University ofOklahoma, Oklahoma City, Oklahoma.
Supported in part by grant HL-18798, NIH.Address for correspondence: Peter J. Schwartz, M.D., Istituto
Ricerche Cardiovascolari, dell' Universita di Milano, 20122Milano, Italy.
Received August 31, 1979; revision accepted April 20, 1980.Circulation 62, No. 6, 1980.
results are to be transposed into the clinical setting,the experimental intervention has to be appropriatelytimed in consideration of the two cardiac events thatcreated the risk factor and that may induce suddendeath.
Therefore, we studied the incidence of ventricularfibrillation during acute myocardial ischemia in twogroups of conscious dogs in which an anterior myocar-dial infarction had been produced 4 weeks earlier; theexperimental group of dogs had a left stellectomy per-formed 1 week after the myocardial infarction.Preliminary results have been reported."' 14
Methods
Surgical Procedure and Protocol
Sixty-four mongrel dogs, ranging in weight from17-25 kg were anesthetized with sodium pentothal (30mg/kg i.v.) and intubated. The level of anesthesia wasmaintained with a mixture of oxygen, nitrous oxideand halothane. The heart was exposed through thefourth intercostal space. The left circumflex anddescending coronary arteries were dissected free fromsurrounding tissue for approximately 1.0 cm, carefullyavoiding damage to the pericoronary nerves. Ahydraulic balloon occluder was positioned around thecircumflex coronary artery and secured in place. Acatheter attached to the balloon was brought out ofthe chest and tunneled to the dorsal surface of the neckwhere it exited from the skin.The left stellate ganglion, the ansa subclavia and the
rami communicantes from Ti to T4 were identified. Anylon monofilament suture was placed around thecaudal portion of the ganglion near the point wherethe T, ramus enters the sympathetic chain and a sec-ond suture was placed around the ansa subclavia at the
1256
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from
LEFT STELLECTOMY AND SUDDEN DEATH/Schwartz and Stone
cranial portion of the ganglion. Both sutures were
buried subcutaneously near the vertebrae on the leftside. Care was taken to make sure that the suturesremained loose around the ganglion to prevent unduetension.The left descending coronary artery was occluded,
by means of the Harris two-stage procedure,15 ap-proximately 1.5-2.0 cm from its origin. The ECG was
monitored before and after occlusion for 1 hour. If toomany ventricular ectopic complexes occurred,lidocaine (5 mg i.v.) was usually given. In the lastgroup of dogs, we also often applied lidocainetopically on the left stellate ganglion. One hour aftercoronary artery occlusion the chest was closed and thedogs were returned to their cages.The dogs alive 1 week after the production of the
anterior myocardial infarction were randomlyallocated to an experimental (LSGx) group or to acontrol group. The dogs in the experimental groupwere lightly anesthetized with sodium pentothal (30mg/kg i.v.), and through an incision in the skin, thenylon sutures passed around the left stellate ganglionwere suddenly pulled, resulting in the destruction ofthe ganglion itself. The final part of the study was per-formed 3-4 weeks after myocardial infarction wasproduced. The dogs were conscious while the balloonoccluder positioned around the circumflex coronaryartery was inflated, producing acute ischemia. Theocclusion was maintained for 10 minutes and thenreleased.A postmortem examination was performed in all
dogs. The heart was removed and the clearly demar-cated infarct was excised from normal tissue, weighedand expressed as a percentage of the total heartweight.
Measurements
The ECG (lead 2) was recorded on an eight-channelBeckman direct-writing oscillograph and was used totrigger a cardiotachometer for measurement of theheart rate. The signals were also recorded on a
magnetic tape (Ampex FR-1300) for later analysis.The QT interval was measured and corrected for
heart rate using the classic Bazett's formula QT, =
QT/VRR. QT, was calculated from five cardiaccycles in each dog and a mean value was then ob-tained.
Data Analysis
The final study with occlusion of the circumflexartery was performed only if the dogs were afebrileand had no arrhythmias. If at postmortem examina-tion the infarct size was less than 10% of total heartweight, the dogs were eliminated from the study. Theeffectiveness of the coronary occlusion was manifestedby ECG signs of acute ischemia and usually bytachycardia.
Statistical analysis was done using the chi-squaretest and t test for paired and unpaired observations.All values are expressed as mean -SEM.
Results
An anterior myocardial infarction was produced in64 dogs. Thirteen dogs died on the surgical tablewithin 2 hours of total occlusion of the anteriordescending coronary artery. Thirteen dogs diedpostoperatively within 1 week after surgery; they wereall found dead in the cage and were, with one excep-tion, in fair condition the day before their death. Onedog died just after induction of anesthesia with sodiumpentothal when the sutures around the left stellateganglion had to be pulled. Five dogs were eliminatedfrom the study, three because of a small infarct (< 10%of total heart weight), one because the balloon occluderaround the circumflex artery ruptured at the time ofocclusion and one because of persistent ventriculartachycardia up to 46 days after myocardial infarction.
Thus, the data were obtained from 32 dogs (50% ofthe initial number) that met our criteria; 17 were in thecontrol group and 15 in the LSGx group. The overalldata are shown in table 1.
TABLE 1. Summary of Data in 32 Dogs with Anterior Myocardial InfarctionInitial HR HR at 1 min. QT0
n VF (%) Mortality Infarct size (beats/min) postocclusion (msec)
Controls 17 11 (65%) 12 (71%)' 21 2% 143 8 201 - 9 347 11X * > * 5 NS NS NS NS
LSGx 15 5 (33%) 6 (40%) 20 2% , 127 5 193- 7 349 19)Survivors 14 - 18 2% 130 5') 178- 5) 318 13
NS NS > *Deceased 18 87% 100% 22 1% } 139 8 210 - 7 371 13,)C surv 5 -- 18=g5% 126 3 172 14 311 14
C dec 12 92% 100% 22 2% 149 10 210 9 363 12
LSGx surv 9 18 3% 132 7 181 4 322 20
LSGx dec 6 83% 100% 22 1% 118 8 211 14 386 31
*p < 0.05.tP < 0.01.Abbreviations: C 2 controls; surv = survived; dec = deceased; LSGx = left stellectomy; VF = ventricular fibrillation.
1257
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from
VOL 62, No 6, DECEMBER 1980
Arrhythmias
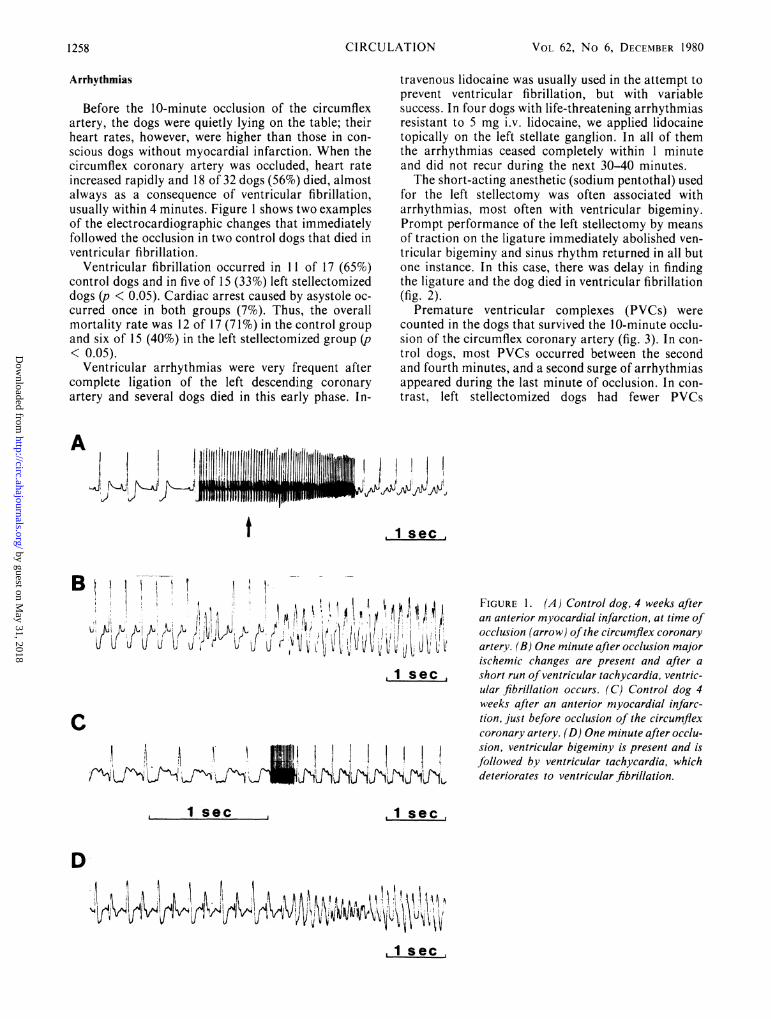
Before the 10-minute occlusion of the circumflexartery, the dogs were quietly lying on the table; theirheart rates, however, were higher than those in con-scious dogs without myocardial infarction. When thecircumflex coronary artery was occluded, heart rateincreased rapidly and 18 of 32 dogs (56%) died, almostalways as a consequence of ventricular fibrillation,usually within 4 minutes. Figure 1 shows two examplesof the electrocardiographic changes that immediatelyfollowed the occlusion in two control dogs that died inventricular fibrillation.
Ventricular fibrillation occurred in 11 of 17 (65%)control dogs and in five of 15 (33%) left stellectomizeddogs (p < 0.05). Cardiac arrest caused by asystole oc-curred once in both groups (7%). Thus, the overallmortality rate was 12 of 17 (7 1%) in the control groupand six of 15 (40%) in the left stellectomized group (p< 0.05).
Ventricular arrhythmias were very frequent aftercomplete ligation of the left descending coronaryartery and several dogs died in this early phase. In-
travenous lidocaine was usually used in the attempt toprevent ventricular fibrillation, but with variablesuccess. In four dogs with life-threatening arrhythmiasresistant to 5 mg i.v. lidocaine, we applied lidocainetopically on the left stellate ganglion. In all of themthe arrhythmias ceased completely within 1 minuteand did not recur during the next 30-40 minutes.The short-acting anesthetic (sodium pentothal) used
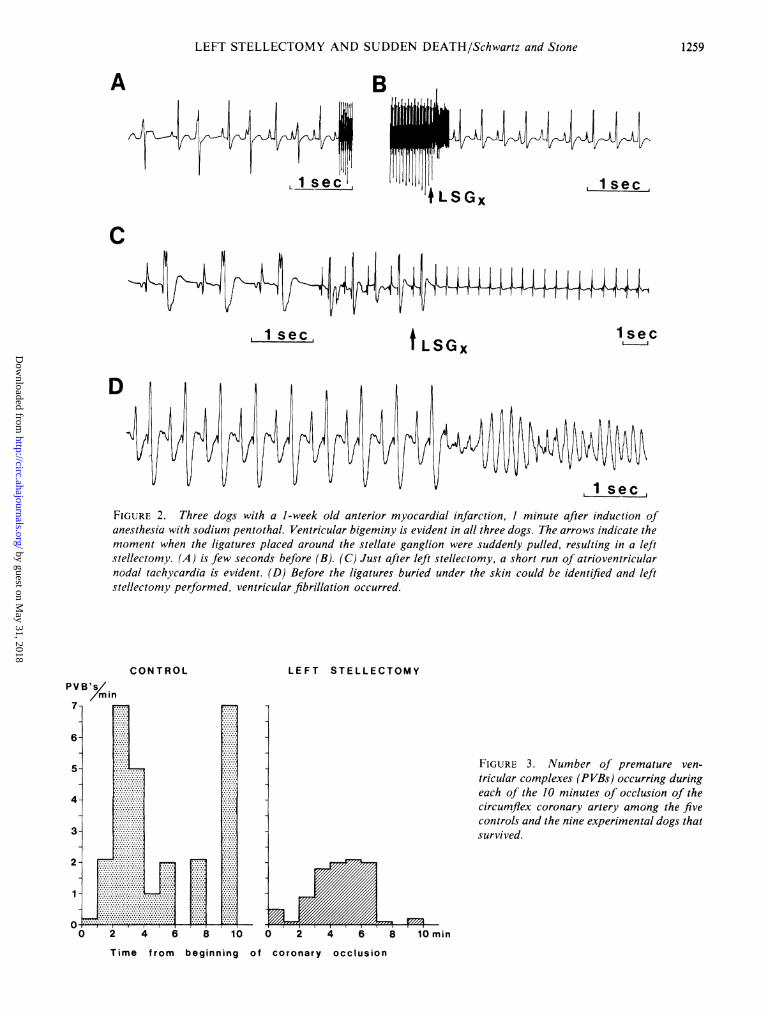
for the left stellectomy was often associated witharrhythmias, most often with ventricular bigeminy.Prompt performance of the left stellectomy by meansof traction on the ligature immediately abolished ven-tricular bigeminy and sinus rhythm returned in all butone instance. In this case, there was delay in findingthe ligature and the dog died in ventricular fibrillation(fig. 2).
Premature ventricular complexes (PVCs) werecounted in the dogs that survived the 10-minute occlu-sion of the circumflex coronary artery (fig. 3). In con-trol dogs, most PVCs occurred between the secondand fourth minutes, and a second surge of arrhythmiasappeared during the last minute of occlusion. In con-trast, left stellectomized dogs had fewer PVCs
A
t
~~ ~ ~ ~ ~ ~ ~ ~ e
fvl~~i'lI if j~U"l 411- 'l
FIGURE 1. (A) Control dog, 4 weeks afteran anterior myocardial infarction, at time ofocclusion (arrow) ofthe circumflex coronaryartery. (B) One minute after occlusion majorischemic changes are present and after ashort run of ventricular tachycardia, ventric-ular fibrillation occurs. (C) Control dog 4weeks after an anterior myocardial infarc-tion, just before occlusion of the circumflexcoronary artery. (D) One minute after occlu-sion, ventricular bigeminy is present and isfollowed by ventricular tachycardia, whichdeteriorates to ventricular fibrillation.
isec sec
D-
.1 sec
1258 CIRCULATION
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from
LEFT STELLECTOMY AND SUDDEN DEATH/Schwartz and Stone
B
i
C
1 secT LSGx
D
FIGURE 2. Three dogs with a 1-week old anterior myocardial infarction, 1 minute after induction ofanesthesia with sodium pentothal. Ventricular bigeminy is evident in all three dogs. The arrows indicate themoment when the ligatures placed around the stellate ganglion were suddenly pulled, resulting in a leftstellectomy. (A) is few seconds before (B). (C) Just after left stellectomy, a short run of atrioventricularnodal tachycardia is evident. (D) Before the ligatures buried under the skin could be identified and leftstellectomy performed, ventricular fibrillation occurred.
/ min
.............
,..
........
.....
...... W..............
LEFT STELLECTOMY
FIGURE 3. Number of premature ven-tricular complexes (PVBs) occurring duringeach of the 10 minutes of occlusion of thecircumflex coronary artery among the fivecontrols and the nine experimental dogs thatsurvived.
0 2 4 6 8 10 min
of coronary occlusion
A
PVE
7-
6-
5-
4-
3-
2
1-
0*-r0 2 4 6
Time from
8 10
beginning
1259
......f---
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from
VOL 62, No 6, DECEMBER 1980
throughout the entire occlusion (p < 0.05). The com-parison was made only in the surviving dogs, so thegreater incidence of deaths in the control group doesnot affect this observation. Thus, left stellectomyreduced the incidence not only of ventricular fibrilla-tion, but also of PVCs in the dogs that survived the 10minutes of circumflex coronary artery occlusion.
Infarct Size
Infarct size was similar in the two groups, 21 ± 2%in the control group and 20 ± 2% in the LSGx group.The difference in infarct size between the survivors (18± 2%) and nonsurvivors (22% ± 1) was not significant.
A
C
HR 150
HR 155
Heart Rate
Heart rate before occlusion of the circumflexcoronary artery was higher in the control group thanin the experimental group (143 ± 8 beats/min vs 127± 5 beats/min) (NS). Heart rate in the dogs withmyocardial infarction was considerably higher thanthat observed in the same laboratory in previousstudies of normal conscious dogs (91 ± 7 beats/min).At 1 minute after the beginning of occlusion, heart
rate increased significantly (p < 0.001) in both groups(201 ± 9 beats/min in the control group and 193 ± 7beats/min in the LSGx group). This is at variancewith that observed by Thames et al."' in anesthetizeddogs without myocardial infarction. A large andsignificant difference (p < 0.05) was found when the
B 3'
D 2'
HR 115
HR 120
AFTER ATROPINE
HR 235 F 30" HR 230
J&i
G 2' HR 187 H 8' HR 200
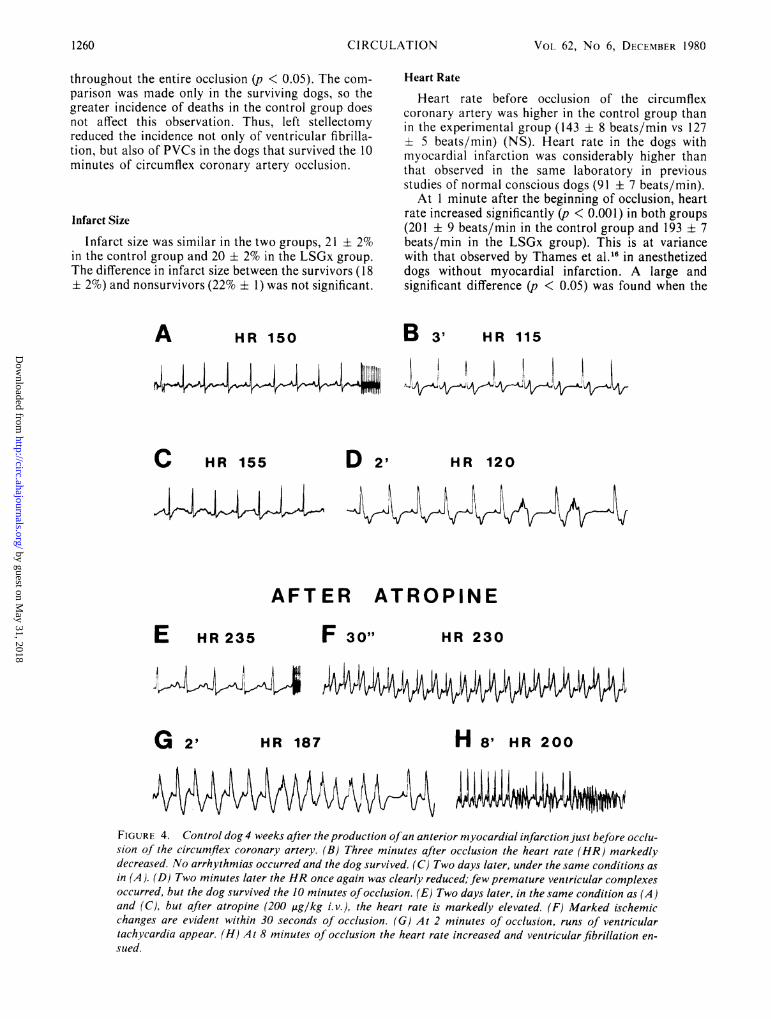
FIGURE 4. Control dog 4 weeks after the production ofan anterior myocardial infarction just before occlu-sion of the circumflex coronary artery. (B) Three minutes after occlusion the heart rate (HR) markedlydecreased. No arrhythmias occurred and the dog survived. (C) Two days later, under the same conditions asin (A). (D) Two minutes later the HR once again was clearly reduced; few premature ventricular complexesoccurred, but the dog survived the 10 minutes ofocclusion. (E) Two days later, in the same condition as (A)and (C), but after atropine (200 ,ug/kg i. v.), the heart rate is markedly elevated. (F) Marked ischemicchanges are evident within 30 seconds of occlusion. (G) At 2 minutes of occlusion, runs of ventriculartachycardia appear. (H) At 8 minutes of occlusion the heart rate increased and ventricular fibrillation en-
sued.
E
1260 CIRCULATION
p ..,%A,
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from
LEFT STELLECTOMY AND SUDDEN DEATH/Schwartz and Stone
changes in heart rate in the first minute of occlusionwere compared between survivors (from 130 ± 5 to178 ± 5 beats/min) and nonsurvivors (from 139 + 8 to210 i 7 beats/min). The heart rate in the dogs thatdied reached the same level in both groups (210 + 9 inthe control group and 211 + 14 beats/min in the LSGxgroup). Detailed information on heart rate before andat 1 minute of occlusion is presented in table 1.
In four dogs, the heart rate decreased after theocclusion of the circumflex artery. Two of these dogsdied in asystole and two survived. (The figures onheart rate reported above do not include them.) Figure4 shows the relationship between vagal reflexes, heartrate and survival in one of the latter two. This dog sur-vived two occlusions that lasted 10 minutes each,always associated with a decreased heart rate; afterpretreatment with atropine the coupling of myocardialischemia with increased heart rate resulted in ven-tricular fibrillation.
QTcECGs recorded while the dogs were conscious were
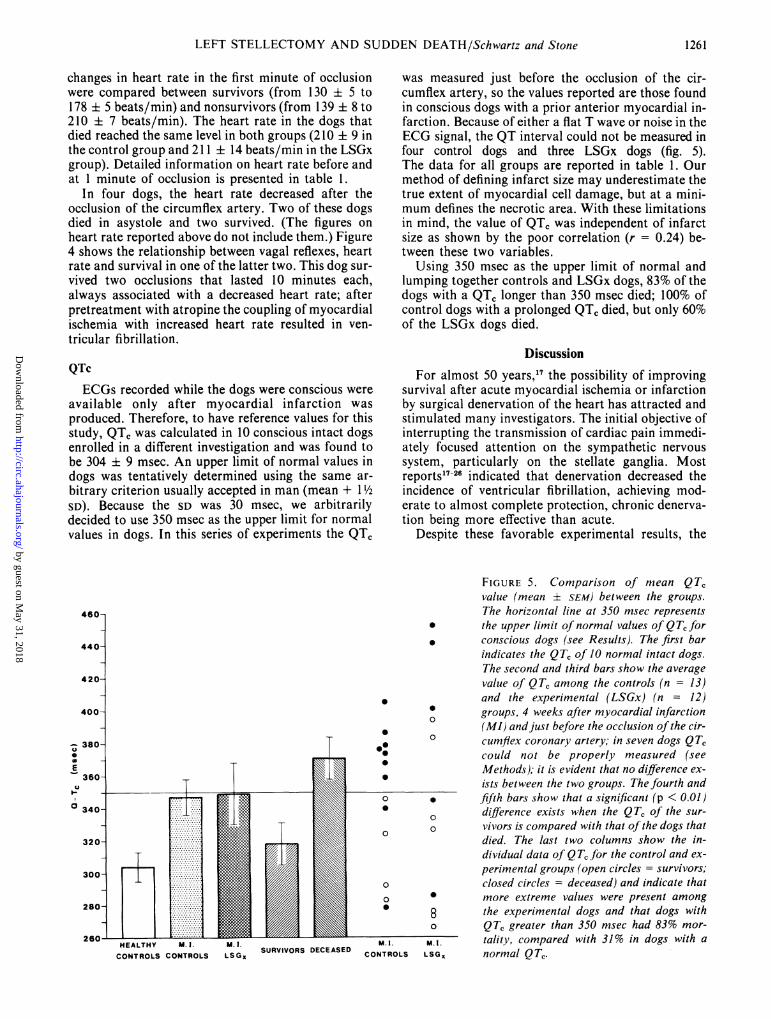
available only after myocardial infarction wasproduced. Therefore, to have reference values for thisstudy, QT, was calculated in 10 conscious intact dogsenrolled in a different investigation and was found tobe 304 + 9 msec. An upper limit of normal values indogs was tentatively determined using the same ar-bitrary criterion usually accepted in man (mean + 1 ½/2SD). Because the SD was 30 msec, we arbitrarilydecided to use 350 msec as the upper limit for normalvalues in dogs. In this series of experiments the QT,
0
0.
0
000.
0
0
0
0
0
.............
HEALTHY M. 1. M. 1.SURVIVORS DECEASED
M. 1.
CONTROLS CONTROLS LSG, CONTROLS L
was measured just before the occlusion of the cir-cumflex artery, so the values reported are those foundin conscious dogs with a prior anterior myocardial in-farction. Because of either a flat T wave or noise in theECG signal, the QT interval could not be measured infour control dogs and three LSGx dogs (fig. 5).The data for all groups are reported in table 1. Ourmethod of defining infarct size may underestimate thetrue extent of myocardial cell damage, but at a mini-mum defines the necrotic area. With these limitationsin mind, the value of QT, was independent of infarctsize as shown by the poor correlation (r = 0.24) be-tween these two variables.
Using 350 msec as the upper limit of normal andlumping together controls and LSGx dogs, 83% of thedogs with a QT, longer than 350 msec died; 100% ofcontrol dogs with a prolonged QT, died, but only 60%of the LSGx dogs died.
DiscussionFor almost 50 years,17 the possibility of improving
survival after acute myocardial ischemia or infarctionby surgical denervation of the heart has attracted andstimulated many investigators. The initial objective ofinterrupting the transmission of cardiac pain immedi-ately focused attention on the sympathetic nervoussystem, particularly on the stellate ganglia. Mostreports17-26 indicated that denervation decreased theincidence of ventricular fibrillation, achieving mod-erate to almost complete protection, chronic denerva-tion being more effective than acute.
Despite these favorable experimental results, the
FIGURE 5. Comparison of mean QT,value (mean ± SEM) between the groups.The horizontal line at 350 msec represents
* the upper limit of normal values of QT for* conscious dogs (see Results). The first bar
indicates the QT, of 10 normal intact dogs.The second and third bars show the averagevalue of QT, among the controls (n = 13)and the experimental (LSGx) (n = 12)
0 groups, 4 weeks after myocardial infarction(MI) andjust before the occlusion of the cir-
o cumflex coronary artery; in seven dogs QT,could not be properly measured (seeMethods); it is evident that no difference ex-ists between the two groups. The fourth and
* fifth bars show that a significant (p < 0.01)O difference exists when the QTC of the sur-o vivors is compared with that of the dogs that
died. The last two columns show the in-dividual data of Q T, for the control and ex-perimental groups (open circles = survivors;closed circles = deceased) and indicate that
* more extreme values were present among8 the experimental dogs and that dogs witho QT, greater than 350 msec had 83% mor-
M.l. tality, compared with 31% in dogs with aL.SGX normal Q T.
1261
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 62, No 6, DECEMBFR 1980
clinical interest in sympathectomy, usually performedto relieve anginal pain, has progressively decreased, fortwo main reasons: (1) bilateral thoracic sympathec-tomy constitutes rather extensive surgery; and (2) theadvent of 3-adrenergic blocking agents, which werethought to duplicate the effects of surgical sympathec-tomy, seemed to supersede surgical denervation.
Recent experimental evidence, however, has shiftedthe focus of interest from bilateral thoracic sympa-thectomy to unilateral left stellectomy.
Critique of the Experimental Model
Large differences still exist between the experi-mental models for sudden cardiac death and the clin-ical situation; a major one is that the diseased, largelyatherosclerotic and ischemic hearts of most patientswho die suddenly27' 28 are not comparable to the intacthearts of the animals used in laboratory experiments.Previous studies, although often very carefully con-ducted26 or analyzed,21 25 suffer because coronaryartery occlusion was performed (1) during anesthesia,(2) at the same time or too shortly after denervation,(3) in otherwise completely intact hearts, and/or(4) after a complete, and therefore clinically unrealis-tic, denervation.Our interest in the potential clinical importance of
our results guided the design of our protocol. The ex-periments had to be performed in conscious animals.To study the effects of denervation in a heart that wascompletely normal until the very moment of coronaryocclusion is of modest clinical interest because a sur-gical denervation would, of course, be inconceivable inpatients with a normal heart, but may be consideredfor patients at high risk of sudden death. Patients withanterior myocardial infarction constitute one of thesehigh-risk groups, so we decided to study dogs with aprevious anterior myocardial infarction during anepisode of acute ischemia. Furthermore, a patientwould be considered for surgery only some time afterthe myocardial infarction, yet early enough to protecthim from life-threatening arrhythmias that are morelikely to occur during the first 6 months after dis-charge from the hospital; accordingly, we scheduledthe left stellectomy 1 week after infarction and theepisode of acute ischemia 3 weeks later. The durationof the occlusion of the circumflex coronary artery, (10minutes) was decided arbitrarily in an attempt tosimulate the occurrence of a major ischemic insult; werealize, however, that this 10-minute occlusion,coupled with the previous ligature of the left anteriordescending coronary artery, may have been over-whelming for many dogs. This may have affected ourresults by decreasing the relative importance of thesympathetic nervous system compared with pumpfunction; if so, our data may actually underestimatethe protective effect of left stellectomy.
Sudden Death
The high mortality (71 %), mostly the result ofventricular fibrillation (65%), indicates that our modelis indeed very effective in producing sudden cardiac
Our main finding is that left stellectomy, performed1 week after an anterior myocardial infarction and 3weeks before a 10-minute occlusion of the left cir-cumflex coronary artery, significantly reduces the in-cidence of ventricular fibrillation in conscious dogs.The minor difference in heart rate before the occlusionand the similar infarct size stress the fact that the onlyimportant difference between the two groups was thepresence or absence of the left stellate ganglion.
Arrhythmias
Among the survivors, the control dogs had morearrhythmias than the LSGx dogs, again confirmingthe antiarrhythmic effect of left stellectomy.8 Theburst of arrhythmias during the last minute of occlu-sion in the control dogs suggests that in this group themortality might have been higher if the occlusion wasmaintained for 1-2 more minutes; in contrast, in theLSGx group the few PVCs during the first part of theocclusion had almost completely subsided by theseventh minute.The observation that topical application of
lidocaine on the left stellate ganglion suppressed,within seconds, ventricular arrhythmias resistant tofull doses of lidocaine given intravenously, pointsagain to the critical role played by the nerve fiberstraversing the left stellate ganglion in the genesis ofthe ventricular arrhythmias that occur during theearly phase of myocardial ischemia. In 1955, Milch etal.22 found that the incidence of sudden death afterligation of the left anterior descending coronary arteryin anesthetized dogs was reduced by bilateral thoracicsympathetic ganglionectomy to 39%, (compared with62% in control dogs), and to 16% by injecting procainein the left stellate ganglion.
Heart Rate
High heart rates in the early stage of acute myo-cardial ischemia may precipitate ventricular fibrilla-tion.29-31 The sympathetic control of heart rate is pri-marily exerted by the right stellate ganglion'2' 32 andimportant differences between control and LSGx dogswould not be expected. The resting heart rates were in-deed similar and did not seem to play an importantrole, being slightly higher (16 beats/min) in the con-trols compared with the LSGx dogs. The main andmost significant difference was the peak value reachedat the first minute of occlusion in the dogs that sur-vived compared with those that did not. The fact thatthe dogs that died reached the same heart rate at 1minute postocclusion (210 beats/min), irrespective ofwhether they belonged to control or LSGx groups,suggests that very high heart rates may overcome theprotective effect of left stellectomy. Hope et al.33similarly showed that the antiarrhythmic effect ofpropranolol was lost if the hearts of dogs with cor-onary artery occlusion were paced to 184 beats/min.However, major and dangerous increases in rate oc-curred much more frequently among control dogs.Why left stellectomized dogs had a reduced tendencyto increase heart rate to a major extent during acuteischemia is not clear, but a tentative explanation is
CI RCU LATION1262
death in control dogs.
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from
LEFT STELLECTOMY AND SUDDEN DEATH/Schwartz and Stone
possible. The heart rate response to ischemia is com-plex and depends on many factors, one of them beinga component of the cardio-cardiac sympathetic re-flex34' 3 with the efferent limb mostly through the rightstellate ganglion and the afferent limb probablythrough both right and left sympathetic afferentfibers.36 Left stellectomy would eliminate part of theafferent information, thus limiting the full expressionof this reflex.
In dogs with an intact heart, occlusion of the cir-cumflex coronary artery is often associated withbradycardia,l' dependent upon activation of vagalafferent fibers.37 38 In only four of our dogs with aprevious myocardial infarction did heart ratedecrease. The role of vagal reflexes during acutemyocardial ischemia is controversial5' 7' 3 and bothprotective and detrimental effects have been claimed.Some enhancement in vagal tone may be beneficial bypreventing excessive tachycardia, thus preserving un-derperfused tissue from advancing ischemia.5However, when the increase in vagal tone is excessive,it may produce hypotension, further reducing cor-onary flow to the ischemic areas and eventuallyresulting in either ventricular fibrillation or asystole.Why some dogs show such an overwhelming vagal ac-tivity is still unclear. Yet, it seems reasonable topostulate that the critical factor may be the existinglevel of sympathetic tone: if it is high enough, thevagal reflex may prevent excessively high heart rateswithout the detrimental effects that occur if the in-creased vagal activity is left completely unopposed.From what is known about the neural pathwaysthrough which the sympathetic nervous system exertsits control on heart rate,'2' 32 it is evident thatthe sympathetic nerves that are critically impor-tant in counteracting vagal reflexes in the setting ofacute ischemia are those that originate from the rightstellate ganglion. Their function would be annulled bybilateral stellectomy or fl-adrenergic blocking agentsbut would remain unimpaired after left stellectomy.The balance between sympathetic and parasym-pathetic efferent activity may be a key to survival dur-ing acute myocardial ischemia.
QT Interval
In a study40 among patients with a myocardialinfarction who had an ECG recorded every 2 monthsfor 7 years, prolongation of the QT interval (QTC > 440msec) was found to be more frequent (57% vs 18%)among those who died compared with those who sur-vived, and 77% of patients with prolonged QT intervaldied suddenly. These findings have been con-firmed.41' 42As in humans, dogs with myocardial infarction had
a greater QT, than control dogs; the most interestingfinding, however, was that the QT, was remarkablylonger in dogs that died than in dogs that survived, asin the clinical study.42 We have no ready explanationfor the cause of QT prolongation. It is tempting tospeculate that, because right sympathetic nerves aremainly distributed to the anterior ventricular surface,an anterior myocardial infarction would damage or
destroy adrenergic terminals mostly innervated byright-sided nerves, thus mimicking, to some extent,the results of right stellectomy, which is associatedwith prolongation of the QT interval43 and ventriculararrhythmias.' 9 The dogs with the greater involvementof right-sided neural terminals would be those with thelonger QT and the greater vulnerability to ventricularfibrillation.
Rationale for Left Stellectomy
The rationale for evaluating the potential of leftstellectomy in reducing the incidence of sudden deathdue to ventricular fibrillation lies mainly in the notionsconcerning (1) the sympathetic reflexes elicited byischemia, (2) the dominant role played by left-sidednerves in the genesis of life-threatening arrhythmiasand (3) some recent findings related to the neural con-trol of coronary circulation.
Cardiac sympathetic sensory endings with myeli-nated and unmyelinated fibers are excited by ische-mia36' 44 and are capable of eliciting a cardio-cardiacsympathetic reflex.35 This sympathetic reflex, whichtakes place within a few seconds after the onset of is-chemia, plays an important role in the genesis of theearly ventricular arrhythmias.45 The excitation of car-diac sympathetic afferents can also reflexly inhibit theactivity of efferent vagal cardiac fibers,46 with thepotential of impairing the maintenance of an optimalheart rate,31 thus facilitating the occurrence of adangerous tachycardia. The afferent limbs of mostcardio-cardiac sympathetic reflexes seem to be prefer-entially distributed through left-sided nerves, whichmakes these reflexes dependent to a major extent on anintact left stellate ganglion.47' 48 Thus, left stellectomywould not only reduce the effects of the tonic sympa-thetic effects on the heart, but would also largely pre-vent the occurrence of cardio-cardiac sympatheticreflexes.
Recent studies dealing with unilateral stellectomyhave shown some unexpected results49 and have in-dicated that left-sided sympathetic nerves play an un-expected role in the genesis of life-threateningarrhythmias. When left cardiac sympathetic activity ispotentiated by right sympathectomy and a conditionof imbalance with left dominance is created, the heartbecomes more vulnerable to ventricular arrhythmias,during control states,9 ischemia,6 psychologic stress14or exercise,'2' 1' in dogs,8' 12, 50 cats34 and nan.51, 52 Leftstellectomy eliminates the possibility that the synmpa-thetic activity would reach the heart through the ar-rhythmogenic left-sided nerves.
It has been recently shown that the coronary cir-culation is under autonomic and metabolic control"' 53
and that sympathetic tone limits, through av-adrener-gic effects, the capability of the coronary bed todilate." This vasoconstrictor activity is almost elimi-nated by left stellectomy, which is as effective as sys-temic a-adrenergic blockade; and is potentiated byadrenergic fA blockade, which leaves unopposed thea-adrenergic tone." Left stellectomy, by improvingthe capability of coronary bed to dilate, may limit theischemic area, particularly by improving the perfusion
1263
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 62, No 6, DECEMBER 1980
of the border zone, and decrease the potential for life-threatening arrhythmias, and may contribute to thepreservation of ventricular function.
Left stellectomy, probably because it does notproduce a major catecholamine depletion,54 is notfollowed by post-denervation supersensitivity.55
Clinical Implications
Although experimental results must be interpretedcautiously, this study suggests that left stellectomy (inman, high thoracic left sympathectomy7) may reducethe incidence of sudden cardiac death in patients withischemic heart disease. This procedure, which is per-formed extrapleurally and carries practically no risk,has been very successfully used in 23 patients affectedby the long QT syndrome who were refractory tomedical treatment.56-58 It is relevant that cardiac per-formance is not affected by left stellectomy, as shownby findings during exercise studies both with59 andwithout infarction in dogs12 and in man.5'The observation that the QT interval is prolonged
just before the occurrence of coronary spasm,60 whichsuggests a unilateral or dominant left sympathetic dis-charge, coupled with our findings of a vasoconstrictoractivity primarily dependent on the left stellate gangli-on, leads us to speculate that left stellectomy might beappropriate in preventing coronary spasm and itsdangerous complications" in patients with variantangina.
Considering the simplicity and the safety of this sur-gical intervention, we believe that its potential forreducing the incidence of ventricular fibrillation isworthy of further investigation.
Acknowledgment
We thank Gerald Todd and Delvin Knight for their excellenttechnical assistance in conducting these experiments and EileenSpain for typing the manuscript.
References
1. Lown B: Sudden cardiac death: the major challenge confront-ing contemporary cardiology. AmJ Cardiol 43: 313, 1979
2. Lown B, Wolf M: Approaches to sudden death from coronaryheart disease. Circulation 44: 130, 1971
3. Lown B, Verrier RL: Neural activity and ventricular fibrilla-tion. N Engl J Med 294: 1165, 1976
4. Lown B, Verrier RL, Rabinowitz SH: Neural and psychologicmechanisms and the problem of sudden cardiac death. AmJCardiol 39: 890, 1977
5. Verrier RL: Neural factors and ventricular electrical instability.In Sudden Death, edited by Wellens HJJ, Kulbertus HE. TheHague, M Nijhof, p 137, 1980
6. Schwartz PJ, Brown AM, Malliani A, Zanchetti A (eds):Neural Mechanisms in Cardiac Arrhythmias. New York,Raven Press, 1978, p 442
7. Malliani A, Schwartz PJ, Zanchetti A: Neural mechanisms inlife-threatening arrhythmias. Am HeartJ 100: 705, 1980
8. Schwartz PJ, Stone HL, Brown AM: Effects of unilateralstellate ganglion blockade on the arrhythmias associated withcoronary occlusion. Am HeartJ 92: 589, 1976
9. Schwartz PJ, Snebold NG, Brown AM: Effects of unilateralcardiac sympathetic denervation on the ventricular fibrillationthreshold. AmJ Cardiol 37: 1034, 1976
10. Schwartz PJ, Verrier RL, Lown B: Effect of stellectomy and
vagotomy on ventricular refractoriness in dogs. Circ Res 40:536, 1977
11. Schwartz PJ, Stone HL: Tonic influence of the sympathetic ner-vous system on myocardial reactive hyperemia and on coronaryblood flow distribution in dogs. Circ Res 41: 51, 1977
12. Schwartz PJ, Stone HL: Effects of unilateral stellectomy uponcardiac performance during exercise in dogs. Circ Res 44: 637,1979
13. Schwartz PJ, Stone HL: Left stellectomy and ventricularfibrillation during myocardial ischemia in conscious dogs with aprevious myocardial infarction. (abstr) Circulation 56 (supplIII): 111-79, 1977
14. Schwartz PJ, Stone HL: Unilateral stellectomy and suddendeath. In Neural Mechanisms in Cardiac Arrhythmias, editedby Schwartz PJ, Brown AM, Malliani A, Zanchetti A. NewYork, Raven Press, 1978, p 107
15. Harris AS: Delayed development of ventricular ectopicrhythms following experimental coronary occlusion. Circula-tion 1: 1318, 1950
16. Thames MD, Klopfenstein HS, Abboud FM, Mark AL,Walker JL: Preferential distribution of inhibitory cardiacreceptors with vagal afferents to the inferoposterior wall of theleft ventricle activated during coronary occlusion in the dog.Circ Res 43: 512, 1978
17. Leriche R, Herman L, Fontaine R: Ligature de la coronairegauche et fonction du coeur apres enervation sympathique. C RSoc Biol 107: 547, 1931
18. Cox WV, Robertson HF: The effect of stellate ganglionectomyon cardiac function of intact dogs. Am Heart J 12: 285, 1936
19. Schauer G, Gross L, Blum L: Hemodynamic studies in ex-perimental coronary occlusion. Am Heart J 14: 669, 1937
20. McEachern CG, Manning GW, Hall GE: Sudden occlusion ofcoronary arteries following removal of cardiosensory pathways:an experimental study. Arch Intern Med 65: 661, 1940
21. Harris AS, Estandia A, Tillotson RF: Ventricular ectopicrhythms and ventricular fibrillation following cardiac sym-pathectomy and coronary occlusion. Amn J Physiol 165: 505,1951
22. Milch E, Zimdahl WT, Egan RW, HsiaTW, Anderson AA,David J: Experimental prevention of sudden death from acutecoronary artery occlusion in the dog. Am Heart J 50: 483, 1955
23. Skelton RB, Gergely N, Manning GW, Coles JC: Mortalitystudies in experimental coronary occlusion. J Thorac Car-diovasc Surg 44: 90, 1962
24. Schaal SF, Wallace AG, Sealy WC: Protective influence of car-diac denervation against arrhythmias of myocardial infarction.Cardiovasc Res 3: 241, 1969
25. Ebert PA, Vanderbeek RB, Allgood RJ, Sabiston DCJr: Effectof chronic cardiac denervation on arrhythmias after coronaryartery ligation. Cardiovasc Res 4:141, 1970
26. Fowlis RAF, Sang CTM, Lundy PM, Ahuja SP, Colhoun H:Experimental coronary artery ligation in conscious dogs sixmonths after bilateral cardiac sympathectomy. Am HeartJ 88:748, 1974
27. Cobb LA, Baum RS, Alvarez H III, Schaffer WA: Resuscita-tion from out-of-hospital ventricular fibrillation: 4 years follow-up. Circulation 52 (suppl III): 111-223, 1975
28. Baroldi G, Falzi G, Mariani F: Sudden coronary death. A post-mortem study in 208 selected cases compared to 97 "control"subjects. Am HeartJ 98: 20, 1979
29. Scherlag BJ, Helfant RH, Haft JI, Damato AN: Elec-trophysiology underlying ventricular arrhythmias due to cor-onary ligation. AmJ Physiol 219: 1665, 1970
30. Kent KM, Smith ER, Redwood DR, Epstein SE: Thedeleterious electrophysiological effects produced by increasingheart rate during experimental coronary occlusion. Clin Res 20:379, 1972
31. Chadda KD, Banka VS, Helfant RH: Rate dependent ven-tricular ectopia following acute coronary occlusion. Circulation49: 654, 1974
32. Randall WC, Rohse WG: The augmentor action of the sym-pathetic cardiac nerves. Circ Res 4: 470, 1956
33. Hope RR, Williams DO, El-Sherif N, Lazzara R, Scherlag BJ:The efficacy of antiarrhythmic agents during acute myocardialischemia and the role of heart rate. Circulation 50: 507, 1974
1264 CIRCULATION
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from
LEFT STELLECTOMY AND SUDDEN DEATH/Schwartz and Stone
34. Malliani A, Parks M, Tuckett RP, Brown AM: Reflex in-creases in heart rate elicited by stimulation of afferent cardiacsympathetic nerve fibers. Circ Res 32: 9, 1973
35. Malliani A, Schwartz PJ, Zanchetti A: A sympathetic reflexelicited by experimental coronary occlusion. Am J Physiol 217:703, 1969
36. Malliani A, Recordati G, Schwartz PJ: Nervous activity ofafferent cardiac sympathetic fibres with atrial and ventricularendings. J Physiol 229: 457, 1973
37. Recordati G, Schwartz PJ, Pagani M, Malliani A, Brown AM:Activation of cardiac vagal receptors during myocardialischemia. Experientia 27: 1423, 1971
38. Thoren P: Vagal reflexes elicited by left ventricular C-fibresduring myocardial ischemia in cats. In Neural Mechanisms inCardiac Arrhythmias, edited by Schwartz PJ, Brown AM,Malliani A, Zanchetti A. New York, Raven Press, 1978, p 179
39. Corr PB, Gillis RA: Autonomic neural influences on thedysrhythmias resulting from myocardial infarction. Circ Res43: 1, 1978
40. Schwartz PJ, Wolf S: QT interval prolongation as predictor ofsudden death in patients with myocardial infarction. Circula-tion 57: 1074, 1978
41. Haynes RE, Hallstrom AP, Cobb LA: Repolarization abnor-malities in survivors of out-of-hospital ventricular fibrillation.Circulation 57: 654, 1978
42. Ahne S, Helmers C, Lundman T, Rehnqvist N, Sjogren A: QTcinterval in acute myocardial infarction: first year prognosticimplications. Clin Cardiol 3: 303, 1980
43. Yanowitz F, Preston JB, Abildskov JA: Functional distributionof right and left stellate innervation to the ventricles: productionof neurogenic electrocardiographic changes by unilateralalterations of sympathetic tone. Circ Res 18: 416, 1966
44. Casati R, Lombardi F, Malliani A: Afferent sympathetic un-myelinated fibres with left ventricular endings in cats. J Physiol292: 135, 1979
45. Schwartz PJ, Foreman RD, Stone HL, Brown AM: Effect ofdorsal root section on the arrhythmias associated with coronaryocclusion. Am J Physiol 231: 923, 1976
46. Schwartz PJ, Pagani M, Lombardi F, Malliani A, Brown AM:A cardiocardiac sympatho-vagal reflex in the cat. Circ Res 32:215, 1973
47. Malliani A, Pagani M, Recordati G, Schwartz PJ: Spinal sym-pathetic reflexes elicited by increases in arterial blood pressure.Am J Physiol 220: 128, 1971
48. Pagani M, Schwartz PJ, Banks R, Lombardi F, Malliani A:
Reflex responses of sympathetic preganglionic neurones ini-tiated by different cardiovascular receptors in spinal animals.Brain Res 68: 215, 1974
49. Schwartz PJ: Unilateral stellectomy and dysrhythmias. CircRes 43: 939, 1978
50. Randall WC, Thomas JX, Euler DE, Rozanski GJ: Cardiacdysrhythmias associated with autonomic nervous system im-balance in the conscious dog. In Neural Mechanisms in CardiacArrhythmias, edited by Schwartz PJ, Brown AM, Malliani A,Zanchetti A. New York, Raven Press, 1978, p 123
51. Austoni P, Rosati R, Gregorini L, Bianchi E, Bortolani E,Schwartz PJ: Stellectomy and exercise in man. Am J Cardiol43: 399, 1979
52. Crampton RS: Preeminence of the left stellate ganglion in thelong Q-T syndrome. Circulation 59: 769, 1979
53. Feigl EO: Control of myocardial oxygen tension by sym-pathetic coronary vasoconstriction in the dog. Circ Res 37: 88,1975
54. Hertting G, Schiefthaler Th: The effect of stellate ganglion exci-sion on the catecholamine content and the uptake of 3-norepinephrine in the heart of the cat. Int J Neuropharmacol 3:65, 1964
55. Schwartz PJ, Stone HL: Post-denervation supersensitivity andleft stellectomy. Am J Cardiol 43: 381, 1979
56. Schwartz PJ, Periti M, Malliani A: The long Q-T syndrome.Am Heart J 89: 378, 1975
57. Moss AJ, Schwartz PJ: Sudden death and the idiopathic longQ-T syndrome. Am J Med 66: 6, 1979
58. Schwartz PJ: The long Q-T syndrome. In Sudden Death, editedby Wellens HIJ, Kulbertus HE. The Hague, M. Nijhof, 1980,p 358
59. Schwartz PJ, Gwirtz PA, Stone HL: Cardiac performance be-fore and after left stellectomy in dogs with an anterior myo-cardial infarction. Proc 8th European Congress of Cardiology.Paris, 1980, p 121
60. Ricci DR, Orlick AE, Cipriano PR, Guthaner DF, HarrisonDC: Altered adrenergic activity in coronary arterial spasm: in-sight into mechanism based on study of coronary hemody-namics and the electrocardiogram. Am J Cardiol 43: 1073,1979
61. Maseri A, L'Abbate A, Baroldi G, Chierchia S, Marzilli M,Ballestra AM, Severi S, Parodi 0, Biagini A, Distante A,Pesola A: Coronary vasospasm as a possible cause of myocar-dial infarction. A conclusion derived from the study of "prein-farction" angina. N Engl J Med 293: 1271, 1978
1265
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from

P J Schwartz and H L Stoneischemia in conscious dogs with anterior myocardial infarction.
Left stellectomy in the prevention of ventricular fibrillation caused by acute myocardial
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1980 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.62.6.1256
1980;62:1256-1265Circulation.
http://circ.ahajournals.org/content/62/6/1256the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 31, 2018
http://circ.ahajournals.org/D
ownloaded from





























