Embed Size (px)
Citation preview

Clinical Radiology (1990) 42, 188-191
Left Coronary Angiography in the Pre-operative Diagnosis of Thrombosis of the Left Atrium or its Appendage in Rheumatic Mitral Stenosis S. SHARMA,* M. V. K U M A R , t V. M. REDDY~, U. KAULt , M. RAJANI* and P. VENUGOPAL~
Departments o f* Cardiovascular Radiology, ~ Cardiology and ~ Cardiothoracic and Vascular Surgery, Cardiothoraeic Centre, All India Institute o f Medical Sciences, New Delhi, India
We studied the utility of pre-operative selective left coronary angiograms for detecting thrombosis in the left atrium or its appendage in 81 patients with rheumatic mitral stenosis, who subsequently underwent open-heart surgery. Thrombus was predicted by the angiographic demonstration of neovascularity seen as a bunch of small vessels arising from the circumflex branch of the left coronary artery coursing superiorly to the region of the left atrial appendage and terminating in a network of smaller vascular channels with a blush of contrast n~dium coalescing into small 'lakes'. This pooling of contrast medium was considered esseJitial for positive angiographic diagnosis. Based on these criteria, the angiographic diagnosis of thrombus was made in 27 patients. Thrombus was found in 33 patients at surgery. Selective left coronary angiography had a sensitivity of 72.7%, specificity of 92.7% and predictive value of 88.8% for detecting thrombi in the left atrium or its appendage. Coronary angiography should be performed in all the patients with mitral stenosis who are undergoing cardiac catheterization especially if balloon mitral valvoplasty or closed mitral valvotomy are planned. Sharma, S., Kumar, M.V., Reddy, V.M., Kaul, U. Rajani, M. & Venugopal, P. (1990). Clinical Radiology 42, 188 191. Left Coronary Angiography in the Pre-operative Diagnosis of Thrombosis of the Left Atrium or its Appendage in Rheumatic Mitral Stenosis
Thrombosis of the left atrium or its appendage is common in rheumatic mitral stenosis and occurs in 22% of patients at surgery and in 35.8% of patients at autopsy (Nichols et al., 1962; Wallach et al., 1963). Pre-operative localization of thrombus is important since its presence necessitates open heart surgery. Various imaging techniques including angiocardiography, computed tomography, transthora- cic and transoesophageal echocardiography, and scinti- graphy are utilized for the pre-operative detection of left atrial thrombus; and advantages and limitations of these techniques are well documented (Soloff and Zatuchni, 1956; Swanson and Steinberg, 1964; Lewis et al., 1965; Parker et al., 1965; Baue et al., 1968; Spanglar and Okin, 1975; Colman et al., 1981 ; Cipriano and Guthaner, 1978; Nair et al., 1981; Schweizer et al., 1981; Shrestha et al., 1983; Tomoda et al., 1983; Eriksson et al., 1984; Yamada et al., 1984; Aschenberg et al., 1986; Hubbard et al., 1987; Shuaile, 1988).
The finding of ~neovascularity in the region 0f the left atrium has been described at selective left: coronary arteri0graphy in patients with mitral stenosis and throm- bosis of the left atrium or its appendage (Colman et al., 1981). The presence of neovascularity and coronary artery-left atrial fistula associated with acquired heart disease was first reported by Marshall et al. (1969) and the same angiographic findings were correlated later with the presence of an organized left atrial thrombus in a patient with mitral valve disease (Standen, 1975). Since then, reports have differed in their view of the utility of this method in detecting left atrial thrombi: (Cipriano and Guthaner, t978; Esplugas et al., 1978; Bochna and Falicov, 1980; Colman et al., 1981; Hubbard et al., 1987). Our experienceof 81 consecutive patients with rheumatic
Correspondence to: Dr Sanjiv Sharma, Department of Radiodiag- nosis, All India Institute of Medical Sciences, New Delhi- 110029, India.
mitral stenosis, who underwent selective left coronary angiograms prior to open heart surgery, has shown some interesting results and led us to modify the criteria for positive angiographic diagnosis. The angiographic-surgi- cal correlation forms the subject of this paper.
MATERIALS AND METHODS
During the last 4 years, 81 consecutive patients with dominant rheumatic mitral stenosis underwent selective left coronary angiography during their pre-operative investigation. The indications for coronary angiography included clinical suspicion of left atrial thrombus due to the presence of paroxysmal or persistent atrial fibrilla: tion, a history of systemic embolization and assessment of coronary arterial anatomy in the patients over 40 years of age.
Angiograms were performed using a Polydiagn0st (Philips) o r Angio t ron GMP (Siemens) unit utilizing single plane radiography and 35 mm cinefilm. All studies were undertaken by percutaneous transfemoral puncture utilizing Seldinger's technique and preshaped Judki~¢s catheters: 9 ml of an ionic, water-soluble contrast medium (Urografin 370, Schering) was injected at a flow rate 0f3 ml/s by a power injector and angiograms were obtained in the right and left anterior oblique projections.
All angiograms were analysed independently by two observers. Angiographic criteria for the presence of thrombus included demonstration o f neovascularity seen as a bunch of small vessels arising from the coronary artery, coursing superiorly to the region of left atrial appendage and terminating in a network of small vascular channels; this is seen as a blush of contrast mediur~ coalescing into small 'lakes'.
All the patients subsequently underwent open-heart surgery. Surgical and angiographic findings were corre
CORONARY ANGIOGRAPHY FOR DETECTION OF LEFT ATRIAL THROMBI 189
lated to evaluate the diagnostic value of left coronary -io-raphy in detecting thrombosis of the left atrium or aIl~ e,
its aPP endage m the following manner:
Sensitivity
True positive
True positives + False negatives x 100
Specificity
True negatives
True negatives + False positives x 100
True positives predictive x 100 value True positives + False positives
RESULTS
There were 45 males and 36 females with an age range between 16 and 68 years (mean age=39.5 years). The duration of symptoms ofmitral stenosis ranged between 8 months and 7 years (mean 3.2 years). All these patients were receiving long term anti-coagulation at the time of angiographic evaluation and subsequent surgery. Parox- ysmal or persistent atrial fibrillation was seen in 74
(a)
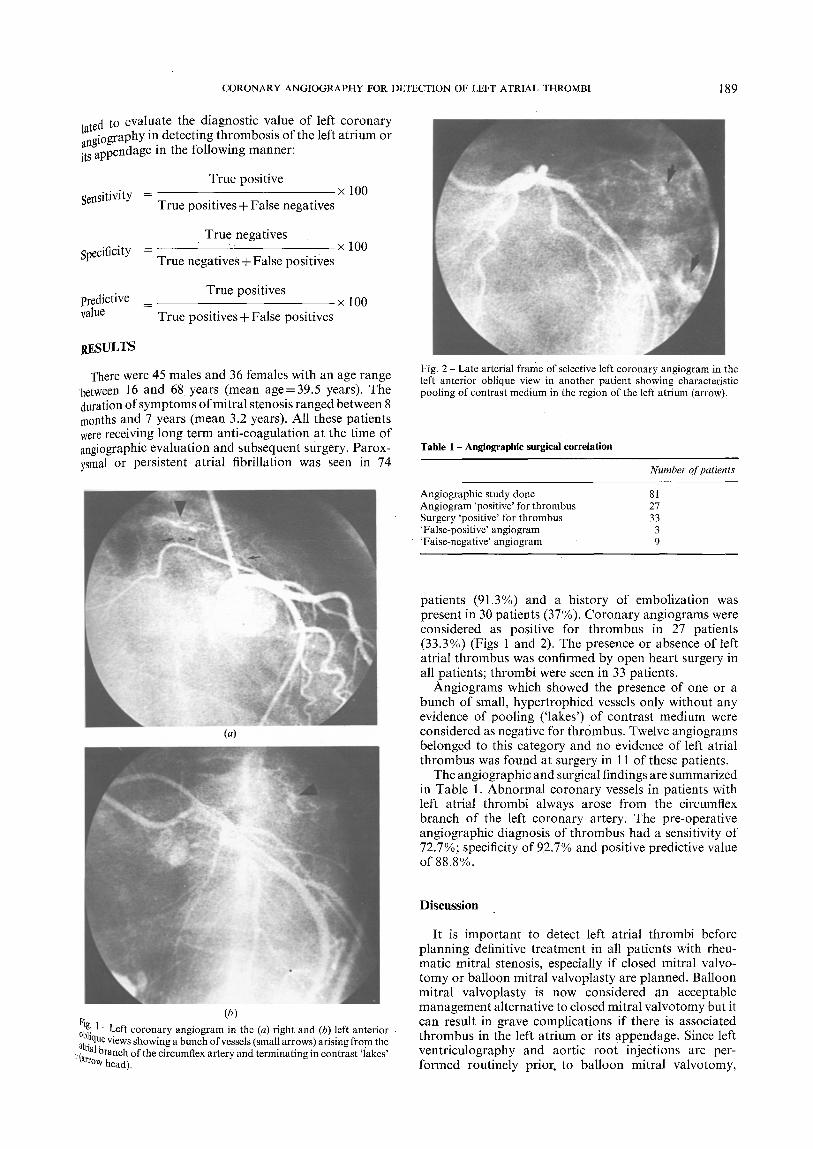
Fig. 2 Late arterial frame of selective left coronary angiogram in the left anterior oblique view in another patient showing characteristic pooling of contrast medium in the region of the left atrium (arrow).
Table 1 - Angiographic surgical correlation
Number of patients
Angiographic study done Angiogram 'positive' for thrombus Surgery 'positive' for thrombus 'False-positive' angiogram 'False-negative' angiogram
81 27 33
3 9
patients (91.3%) and a history of embolization was present in 30 patients (37%). Coronary angiograms were considered as positive for thrombus in 27 patients (33.3%) (Figs 1 and 2). The presence or absence of left atrial thrombus was confirmed by open heart surgery in all patients; thrombi were seen in 33 patients.
Angiograms which showed the presence of one or a bunch of small, hypertrophied vessels only without any evidence of pooling ('lakes') of contrast medium were considered as negative for thrombus. Twelve angiograms belonged to this category and no evidence of left atrial thrombus was found at surgery in 11 of these patients.
The angiographic and surgical findings are summarized in Table 1. Abnormal coronary vessels in patients with left atrial thrombi always arose from the circumflex branch of the left coronary artery. The pre-operative angiographic diagnosis of thrombus had a sensitivity of 72.7%; specificity of 92.7% and positive predictive value of 88.8%.
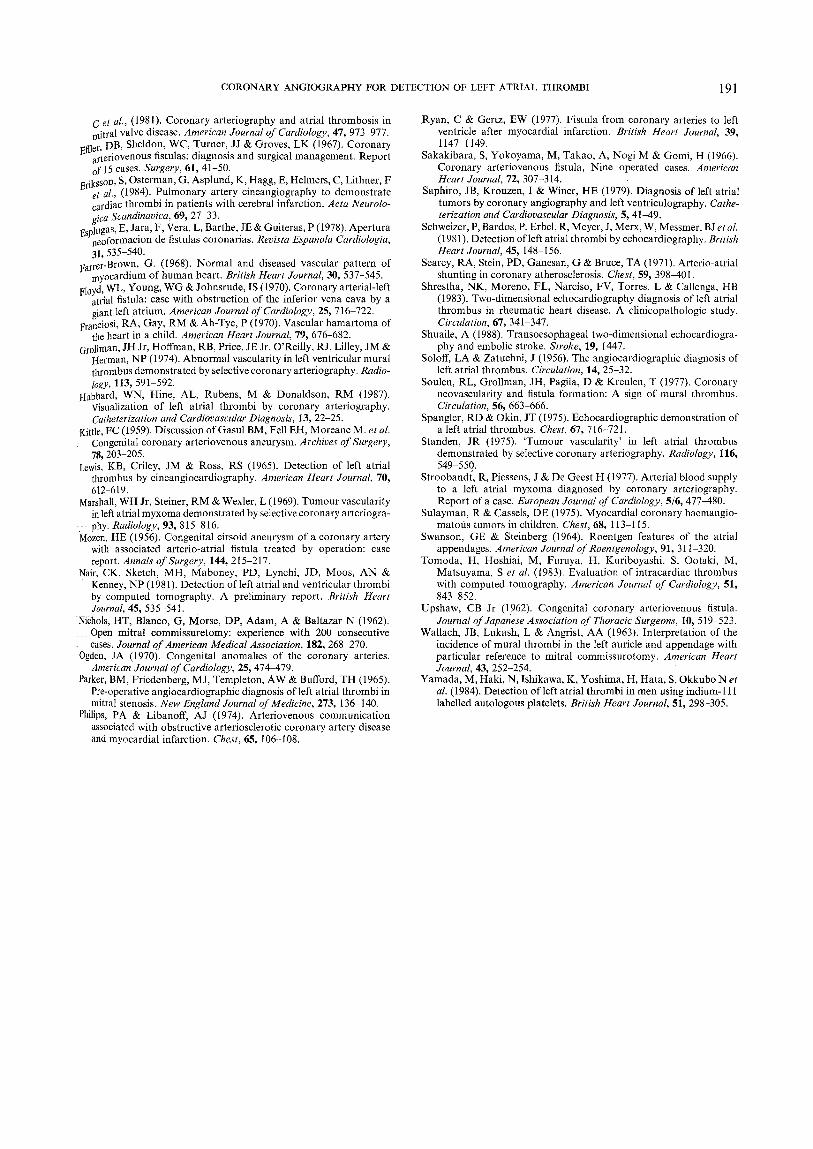
(b) g: 1 - Left coronary angiogram in the (a) right and (b) left anterior
a,°!Nue views showing a bunch of vessels (small arrows) arising from the ~rlal branch of the circumflex artery and terminating in contrast 'Sakes' t rrow head).
Discussion
It is important to detect left atrial thrombi before planning definitive treatment in all patients with rheu- matic mitral stenosis, especially if closed mitral valvo- tomy or balloon mitral valvoplasty are planned. Balloon mitral valvoplasty is now considered an acceptable management alternative to closed mitral valvotomy but it can result in grave complications if there is associated thrombus in the left atrium or its appendage. Since left ventriculography and aortic root injections are per- formed routinely priol: to balloon mitral valvotomy,

190 CLINICAL RADIOLOGY
additional left coronary angiography will not signifi- cantly increase the procedure time or cost. At the same time, important information regarding the presence or absence of left atrial thrombosis can be obtained.
Previously reported studies on the efficacy of selective coronary angiography in detecting left atrial thrombi have shown conflicting results (Bochna and Falicov, 1980; Colman et al., 1981). Bochna and Falicov (1980) found that neovascularity in the region of the left atrium was a highly sensitive sign for the presence of thrombus. However, Colman et al. (1981) showed that although this sign was very specific for the diagnosis of thrombus (98.8 %), it had a very low sensitivity of only 32.8 % and a predictive value of 83.3%. This is at variance with our study when this radiographic sign had a sensitivity of 72.7 %, specificity of 92.7 % and predictive value o f 88.8 %; this is probably related to the fact that we included only those angiograms showing definite 'pooling' of contrast medium as positive for thrombus. The mere presence of one or a bunch of small, hypertrophied vessels in the region of the left atrial appendage in the absence of pooling of contrast material in the form of'lakes' does not constitute a radiological sign for left atrial thrombus.
There is no correlation between the size or age of the thrombus and angiographic grade of neovascularity (Colman et al., 1981). Neovascularity is probably related to the local inflammatory reaction that occurs secondary to an effort to reabsorb the thrombus. Subsequent partial necrosis of the thrombus may result in fistula formation into the left atrium (Standen, 1975). These angiographic abnormalities are observed mainly in the narrow area of implantation of thrombus to the atrial wall (Cipriano and Guthaner, 1978). The presence of false positive angio- grams can be explained by this hypothesis since even after embolization, the remaining fibrous tissue can still have enough of these peculiar blood vessels to be visualized at angiography. This was confirmed at histology in one patient by Colman et al., (1981).
Abnormal vascular channels arising from the coronary arteries and mimicking neovascularity have also been described in congenital intracardiac fistulae, atheroscler- otic coronary artery disease, myxomas and other cardiac tumours (Mozen, 1956; Kittle, 1959; Upshaw, 1962; Sakakibara et al., 1966; Effler et al., 1967; Fa/'rer-Brown et al., 1968; Floyd et al., 1970; Franciosi et al., 1970;
Table 2 - Angiographic differential diagnosis o f left atrial thrombus
Clinical condition Angiographic features
Congenital fistulae 1 Rare; usually drain into right heart chambers
2 Communications often large, and may cause haemodynamic disturbance
3 Pooling ('lakes') of contrast not seen
Atherosclerotic coronary 1 Fistulae that drain into cardiac artery disease chambers are associated with hypertro-
phied collateral vessels especially in subendocardial region
2 Atherosclerotic coronary arterial lesions are present
Ventricular thrombus after Fistulae drain into the ventricular cavity myocardial infarction
Left atrial myxoma 1 Vessels usually arise from the right cor- onary artery
2 Positional change in neovascularity may be seen at angiography
Ogden, 1970; Searcy et al., 1971; Grollman~et al., 1974; Philips and Libanoff, 1974; Sulayman and Cassels, 1975; Ryan and Gertz, 1977; Stroobandt et al., 1977; Saphiro et al., 1979). The important distinguishing radiographic features are summarized in Table 2. Left atrial myxomais the only condition which closely mimics left atrial thrombus. The characteristic clinical and echocardi0. graphic features of myxoma, however, are very helpful in establishing the diagnosis.
Conventional chest radiography, fluoroscopy, echo. cardiography, computed tomography and scintigraphy have been variously utilized for the non-invasive pre. operative detection of left atrial thrombi (Swanson and Steinberg, 1964; Spangler and Okin, 1975; Nair et al., 1981; Shrestha et al., 1983; Schweizer et al., 1981; Tomoda et al., 1983; Yamada et al., 1984). Conventional chest radiographs and fluoroscopy are very poor predie. tots of the presence of left atrial thrombus. Trans. thoracic echocardiography is associated with an unaccep. tably low sensitivity and specificity (Spangler and Okin, 1975; Schweizer et al., 1981; Shrestha et al., 1981). In addition, it is particularly unreliable in detecting thromb[ in the atrial appendage, the site of thrombus formation in as many as 84% of patients (Swanson and Steinberg; 1964; Schweizer et al., 1971; Shrestha et al., 1983). Transoesophageal two-dimensional echo-cardiography, a recently introduced technique, can readily visualize the left atrial appendage and may prove helpful in patients in whom left atrial thrombi are suspected, especially those in whom a conventional transthoracic two-dimensional echocardiogram is non-diagnostic (Shuaile, 1988). Aschenberg et al. (1986) recently performed transoes0~ phageal echocardiograms in 21 patients with mitral stenosis and detected left atrial thrombi in six patients. The findings were confirmed at subsequent surgery in all patients. These thrombi had not been earlier noticed in any patient at transthoracic echocardiography. Recently, computed tomography and scintigraphy have also shown encouraging results in this regard (Nair et al., 1981; Tomoda et al., 1983; Yamada et al., 1984).
We conclude that selective left coronary angiographyis a reliable method for detecting left atrial thrombi. It should be performed in all the patients with a clinical suspicion of thrombus in the left atrium or its appendage, especially if closed mitral valvotomy or balloon mitrai valvoplasty are planned. Angiographic demonstration of pooling of contrast material ('lakes') is an essential sign for the study to be considered as positive for thrombus. Its presence should lead to further careful search for throrn" bus, either by precordial or trans-oesophageal echocar" diography or if necessary at surgery.
R E F E R E N C E S
Aschenberg, W, Schluter, M, Kremer, P. Schroder, E, Siglow, V & Bleifeld, W (1986). Transoesophageal two-dimensional echocardi° i graphy for the detection of left atrial appendage thrombus. Journa of American College of Cardiology,.7, 163-166.
Baue, AE, Baum, S, Wallace, HW, Blakemore, WS & Zinsser, I-IF (1968). The diagnosis of left atrial thrombus by cineangiograPhY' Archives of Surgery, 97, 976 983. ..~
Bochna, AJ & Falicov, RE (1980). Diagnosis of intracardiac thromb11/ mitral stenosis and left ventricular dysfunction. Archives oflnterna Medicine, 140, 759-762.
Cipriano, PR & Guthaner, DF (1978). Organized left atrial mural thrombus demonstrated by coronary arteriography. AmeriCatt Heart Journal, 96, 166-169.
Colman, T, Ubago, JLM, Figueroa, A, Pomar, JL, Gallo, G, Mortera,
CORONARY ANGIOGRAPHY FOR DETECTION OF LEFT ATRIAL THROMBI 191
C et al., (1981). Coronary arteriography and atrial thrombosis in r~itral valve disease. American Journal of Cardiology, 47, 973-977.
l~ffler, DB, Sheldon, WC, Turner, JJ & Groves, LK (1967). Coronary arteriovenous fistulas: diagnosis and surgical management. Report of 15 cases. Surgery, 61, 41-50.
13rikSSOn, S, Os!erman, G, Asplund, K, Hagg, E, Helmers, C, Lithner, F et al., (1~,+). rmmonary artery cineangiography to demonstrate cardiac thrombi in patients with cerebral infarction. Acta Neurolo- gica Scandinavica, 69, 27-33.
13splugas, E, Jara, F, Vera, L, Barthe, JE & Guiteras, P (1978). Apertura neoformacion de fistulas coronarias. Revista Espanola Cardiologia, 31, 535-540.
Farrer-Brown, G. (1968). Normal and diseased vascular pattern of nayocardium of human heart. British Heart Journal, 30, 537-545.
Floyd, WL, Young, WG & Johnsrude, IS (1970). Coronary arterial-left atrial fistula: case with obstruction of the inferior vena cava by a giant left atrium. American Journal of Cardiology, 25, 716 722.
Franciosi, RA, Gay, RM & Ah-Tye, P (1970). Vascular hamartoma of the heart in a child. American Heart Journal, 79, 676-682.
Grollman, JH Jr, Hoffman, RB, Price, JE Jr. O'Reilly, R J, Lilley, JM & Herman, NP (1974). Abnormal vascularity in left ventricular mural thrombus demonstrated by selective coronary arteriography. Radio- logy, 113, 591 592.
Hubbard, WN, Hine, AL, Rubens, M & Donaldson, RM (1987). Visualization of left atrial thrombi by coronary arteriography. Catheterization and Cardiovascular Diagnosis, 13, 22-25.
Kittle, FC (1959). Discussion of Gasul BM, Fell EH, Moreane M. et al. Congenital coronary arteriovenous aneurysm. Archives of Surgery, 78, 203-205.
Lewis, KB, Criley, JM & Ross, RS (1965). Detection of left atrial thrombus by cineangiocardiography. American Heart Journal, 70, 612 619.
Marshall, WH Jr, Steiner, RM & Wexler, L (1969). Tumour vascularity in left atrial myxoma demonstrated by selective coronary arteriogra- play. Radiology, 93, 815-816.
Mozen, HE (1956). Congenital cirsoid aneurysm of a coronary artery with associated arterio-atrial fistula treated by operation: case report. Annals o f Surgery, 144, 215-217.
Nair, CK, Sketch, MH, Maboney, PD, Lynchi, JD, Moos, AN & Kenney, NP (1981). Detection of left atrial and ventricular thrombi by computed tomography. A preliminary report. British Heart Journal, 45, 535-541.
:Nichols, HT, Blanco, G, Morse, DP, Adam, A & Baltazar N (1962). Open mitral commissuretomy: experience with 200 consecutive eases. Journal of American Medical Association, 182, 268 270.
Ogden, JA (1970). Congenital anomalies of the coronary arteries. American Journal of Cardiology, 25, 474 479.
Parker, BM, Friedenberg, M J, Templeton, AW & Bufford, TH (1965), Pre-operative angiocardiographic diagnosis of left atrial thrombi in mitral stenosis. New England Journal of Medicine, 273, 136-140.
Philips, PA & Libanoff, AJ (1974). Arteriovenous communication associated with obstructive arteriosclerotic coronary artery disease and myocardial infarction. Chest, 65, 106-108.
Ryan, C & Gertz, EW (1977). Fistula from coronary arteries to left ventricle after myocardial infarction. British Heart Journal, 39, 1147 1149.
Sakakibara, S, Yokoyama, M, Takao, A, Nogi M & Gomi, H (1966). Coronary arteriovenous fistula, Nine operated cases. American Heart Journal, 72, 307-314.
Saphiro, JB, Kronzen, I & Wirier, HE (1979). Diagnosis of left atrial tumors by coronary angiography and left ventriculography. Cathe- terization and Cardiovascular Diagnosis, 5, 41-49.
Schweizer, P, Bardos, P, Erbel, R, Meyer, J, Merx, W, Messmer, BJ et al. (1981). Detection of left atrial thrombi by echocardiography. British Heart Journal, 45, 148 156.
Searcy, RA, Stein, PD, Ganesan, G & Bruce, TA (1971). Arterio-atriaI shunting in coronary atherosclerosis. Chest, 59, 398 401.
Shrestha, NK, Moreno, FL, Narciso, FV, Torres, L & Callenga, HB (1983). Two-dimensional echocardiography diagnosis of left atrial thrombus in rheumatic heart disease. A clinicopathologic study. Circulation, 67, 341-347.
Shuaile, A (1988). Transoesophageal two-dimensional echocardiogra- phy and embolic stroke. Stroke, 19, 1447.
Soloff, LA & Zatuchni, J (1956). The angiocardiographic diagnosis of left atrial thrombus. Circulation, 14, 25-32.
Soulen, RL, Grollman, JH, Pagila, D & Kreulen, T (1977). Coronary neovascularity and fistula formation: A sign of mural thrombus. Circulation, 56, 663-666.
Spangler, RD & Okin, JT (1975). Echocardiographic demonstration of a left atrial thrombus. Chest, 67, 716-721.
Standen, JR (1975). 'Tumour vascularity' in left atrial thrombus demonstrated by selective coronary arteriography. Radiology, 116, 549-550.
Stroobandt, R, Piessens, J & De Geest H (1977). Arterial blood supply to a left atrial myxoma diagnosed by coronary arteriography. Report of a case. European Journal of Cardiology, 5/6, 477-480.
Sulayman, R & Cassels, DE (1975). Myocardial coronary haemangio- matotis tumors in children. Chest, 68, 113-115.
Swanson, GE & Steinberg (1964). Roentgen features of the atrial appendages. American Journal of Roentgenology, 91, 311 320.
Tomoda, H, Hoshiai, M, Furuya, H, Kuriboyashi, S, Ootaki, M, Matsuyama, Se t al. (1983). Evaluation of intracardiac thrombus with computed tomography. American Journal o f Cardiology, 51, 843 852.
Upshaw, CB Jr (1962). Congenital coronary arteriovenous fistula. Journal o f Japanese Association o f Thoracic Surgeons, 10, 519 523.
Wallach, JB, Lukash, L & Angrist, AA (1963). Interpretation of the incidence of mural thrombi in the left auricle and appendage with particular reference to mitral commissurotomy. American Heart Journal, 43, 252-254.
Yamada, M, Haki, N, Ishikawa, K, Yoshima, H, Hata, S, Okkubo Ne t al. (I 984). Detection of left atrial thrombi in men using indium- 111 labelled autologous platelets. British Heart Journal, 51, 298-305.