Embed Size (px)
Citation preview

Lee Ellis, MD, UT MDACC
Anti-VEGF Therapy Goes Mainstream
Lee M. Ellis, MD
UT MD Anderson Cancer Center
Houston, TX
ASCO 2005
“Advancing the science of clinical oncology”

Lee Ellis, MD, UT MDACC
What Have We Learned Today About Anti-VEGF Therapy?
• Bevacizumab (BV) improves effects of chemo in– NSCLC (first line)– mCRC (second line)
• Dosing of BV (10 vs 5 mg/kg) is probably not an issue in mCRC
• BV, as monotherapy, remains unproven in mCRC– Although OS was comparable to FOLFOX, we do not have data
on therapy after progression (PFS of BV < FOLFOX)
• PTK/ZK does not improve the effects of FOLFOX in mCRC front line
• No drug is without toxicity

Lee Ellis, MD, UT MDACC
Points for Discussion
• Biology
• Brief review of trials
• Mechanisms of Action
• PTK/ZK: Why different results than BV
• Toxicities

Lee Ellis, MD, UT MDACC
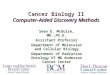
VEGF-A
VEGF-R1(Flt-1)
MigrationInvasion
VEGF-R3(Flt-4)
Lymphangio-genesis
VEGF-R2(KDR/Flk-1)Proliferation
SurvivalPermeability
Cell membrane
VEGF Family and Receptors
PlGF VEGF-B VEGF-C, D
VEGF-R
Functions
NeuropilinSurvivalMigration

Lee Ellis, MD, UT MDACC
Anti-VEGF Therapy is Not Synonymous With Anti-Angiogenic Therapy
Anti-VEGF Anti-angiogenic
Target Endothelial and tumors cells
Endothelial cells
Inhibits permeability Yes ??
Inhibits further blood vessel growth (hard to prove)
Yes TBD
Effects blood flow and function (Nitric oxide?)
Yes TBD

Lee Ellis, MD, UT MDACC
Phase III Trials: Chemo +/- Anti-VEGF Therapy
Trial Year Malignancy Setting Primary Endpoint Met?
Capecitabine +/-BV
2002 mBreast Ca
Refractory NO
Paclitaxel +/- BV 2005 mBreast Ca
Front Line YES
5-FU/LV +/- SU5416
2002 mCRC Front Line NO
IFL +/- BV 2003 (AV2107)
mCRC First Line YES
FOLFOX +/- BV 2005
(ECOG 3200)
mCRC Refractory YES
FOLFOX +/-PTK/ZK
2005
(CONFIRM-1)
mCRC First Line NO
Carbo/Paclitaxel +/- BV
2005
(ECOG 4599)
NSCLC First Line YES
We owe it to our patients to publish the results…good or bad!

Lee Ellis, MD, UT MDACC
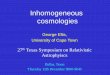
Progression Free Survival
0
1
2
3
4
5
6
7
8
PFS (months)
C + P C + P +BV
FOLFOX FOLFOX+ BV
FOLFOX FOLFOX+ PTK/ZK
ECOG 4599NSCLC
CONFIRM-1mCRC 1st
(Central Rad Review)
ECOG 3200mCRC 2nd
**
* P < 0.05

Lee Ellis, MD, UT MDACC
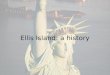
Response Rates
0
5
10
15
20
25
30
35
40
45
50
Response Rates (CR + PR) (%)
C + P C + P +BV
FOLFOX FOLFOX+ BV
FOLFOX FOLFOX+ PTK/ZK
ECOG 4599NSCLC
CONFIRM-1mCRC 1st
(Central Rad Review)
ECOG 3200mCRC 2nd
**
* P < 0.05

Lee Ellis, MD, UT MDACC
Phase III Trials: Chemo +/- BV
Trial Disease Site Front Line or Refractory
RR + BV
Capecitabine +/-BV
mBreast Ca Refractory 10%
Paclitaxel +/- BV mBreast Ca Front Line Monday
IFL +/- BV mCRC First Line 10%
FOLFOX +/- BV mCRC
ECOG 3200
Refractory 13%*
Carbo/Paclitaxel +/- BV
NSCLC
ECOG 4599
First Line 15
* Single agent BV RR in ECOG 3200 = 3%

Lee Ellis, MD, UT MDACC
Points for Discussion
• Biology
• Brief review of trials
• Mechanisms of Action
• PTK/ZK: Why different results than BV
• Toxicities

Lee Ellis, MD, UT MDACC
Proposed Mechanisms of Action of Anti-VEGF Rx
• Anti-angiogenic– Difficult to demonstrate in patients
• How does one explain the increase in RR with chemo when, as a single agent, responses are rare?– “Normalization” of the vasculature with improved
delivery of chemo and O2 (transient)• Jain Science 2005, Yang Cancer 2005
– Vascular “constriction” (Sunday 11:15)
– Direct effect on tumor cells

Lee Ellis, MD, UT MDACC
VEGF-A
VEGF-R1(Flt-1)
MigrationInvasion
VEGF-R3(Flt-4)
Lymphangio-genesis
VEGF-R2(KDR/Flk-1)Proliferation
SurvivalPermeability
Cell membrane
VEGF Family and Receptors
PlGF VEGF-B VEGF-C, D
VEGF-R
Functions
NeuropilinSurvivalMigration

Lee Ellis, MD, UT MDACC
HT
-29
KM
12S
ML
M2
KM
12L
4
SW
480
SW
620
GE
O
RK
O
VEGFR1
-Actin
Parikh et al. Am J Path 2004
VEGFR1
NRP-1
VEGFR1 and NRP-1 on CRC Cells
Fan et al. Oncogene, 2005

Lee Ellis, MD, UT MDACC
Copyright ©2004 by the National Academy of Sciences
Castro-Rivera, Emely et al. (2004) PNAS 101, 11432-11437
Expression of VEGFR-1, VEGFR-2, and NP-1, in
Lung Cancer Cells In Vitro
Anti-VEGF Antibody Decreases Number of Lung
Cancer Cells In Vitro
VEGFR and NRP-1 on Lung Cancer Cells
VEGFR-1
VEGFR-2
Neuropilin-1

Lee Ellis, MD, UT MDACC
Dynamic Effect of Anti-VEGF Therapy
Acute Chronic
• Decreased flow due to vasoconstriction
• Direct effect on tumor cells• Paradoxical transient increase
in chemo delivery
• Inhibition of blood vessel growth

Lee Ellis, MD, UT MDACC
Points for Discussion
• Biology
• Brief review of trials
• Mechanisms of Action
• PTK/ZK: Why different results than BV
• Toxicities

Lee Ellis, MD, UT MDACC
Addition of BV to Chemo Improves EfficacyAddition of PTK/ZK Does Not
• PK?
• Antibody vs TKI?
• VEGF Receptor target profile– TKIs do not target Neuropilin on tumor cells

Lee Ellis, MD, UT MDACC
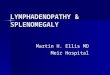
Morgan, B. et al. J Clin Oncol; 21:3955-3964 2003
• Imaging done 2-9 hrs post dosing• Half-life PTK/ZK = 3-6 hrs• How long is the target affected?
With Daily Dosing, We Do Not Know if the Target Was Inhibited for the Entire Dosing Period?
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Pre PTK/ZK Rx Post PTK/ZK Rx(Day 2)
CRC Liver Metastases: DCE-MRI Ki (perfusion/permeability)

Lee Ellis, MD, UT MDACC
Partial Inhibition of VEGFR is Ineffective!! Stress Induction of VEGF
• VEGF-R inhibition (stress) leads to a compensatory increase in VEGF levels– PTK/ZK leads to an increase in plasma VEGF in
Phase I study in a dose dependent manner • Drevs et al. Ann Onc 2005
– Increases in plasma VEGF with VEGFR-2 MoAB• Bocci….Hicklin, Kerbel. Cancer Res 2004

Lee Ellis, MD, UT MDACC
JCO June 20, 2005
Recent studies with TKIs: Longer half-lives or BID dosing

Lee Ellis, MD, UT MDACC
Just because a trial does not meet its primary endpoint does not mean
that the drug is not active!
• Capecitabine +/ BV in refractory breast cancer• PTK/ZK has activity, but in this population with
daily dosing, it did not significantly improve the effects of FOLFOX– LDH as a predictive marker could be explored in
prospective trials, but it is not ready for prime time.• Await OS data, and CONFIRM-2 data
• Consider alternative dosing schedules after validation of PK

Lee Ellis, MD, UT MDACC
Points for Discussion
• Biology
• Brief review of trials
• Mechanisms of Action
• PTK/ZK: Why different results than BV
• Toxicities

Lee Ellis, MD, UT MDACC
Adverse Events in Anti-VEGF + Chemo Trials
• NSCLC (ECOG 4599) C/P +/-BV
– HTN 6%– Hemoptysis and death (5 pts)
• mCRC 2nd line (ECOG 3200) FOLFOX +/-BV vs BV
– HTN 6-7%– Hemorrhage 2-3.5%
• mCRC 1st line (CONFIRM-1) FOLFOX +/- PTK/ZK
– HTN 21%– Dizziness 7-8%
VEGF Plays Important Roles in Physiology!!!
Does HTN contribute to hemorrhage or dizziness, or are they independent effects?

Lee Ellis, MD, UT MDACC
Although Progress Has Been Made, Our Work Is Not Done!!
• Improvements in survival are good, but not good enough (~2 mos) (our patients expect more)
• Identify predictive markers for – efficacy – adverse events
• Determine the role of combination therapy with other biologics– Will the addition of EGFR inhibitors improve efficacy even
further?• BV + cetuximab in mCRC • BV + erlotinib in NSCLC

Lee Ellis, MD, UT MDACC
Take Home Messages• The addition of BV to chemo improves efficacy
– First and second line mCRC– First line NSCLC and Breast Cancer– Be cognizant of HTN, bowel perforations and hemorrhage
(infrequent, but important)
• The role of tyrosine kinase inhibitors targeting VEGFR (PTK/ZK) remains undefined in mCRC– Await overall survival data in CONFIRM-1, and outcomes of
CONFIRM-2 Trials
• Ongoing studies in other malignancies with TKIs– RCC and GIST

Lee Ellis, MD, UT MDACC