-
8/8/2019 Lecture 24 General trauma (cor)
1/16
23.07.2010
1
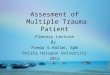
G E N E R A L T R A U M A
Leading causes of injury death by manner of death in the USA
1995. Data from Fingerhut & Warner 1997.5
Initial management of the acutely injured patients.
Priorities.a) the patient may have more than one injury;
b) the obvious injury is not necessarily the most important
one.
Categories of injury:
1. Exigent.These are the most life-threatening
conditions,requiring instantaneous intervention (complete
airway
obstruction).2. Emergency.Those conditions requiring immediate
interventionover a period of few minutes.
. rgent. ose con t ons requ
r
ng ntervent on w t
n t e rst
hour.4. Deferrable.Those conditions that may or may not
immediatelyapparent but will subsequently require treatment
(urethraldisruption).
Steps in initial resuscitation (ABC).
Airway
- removal of debris and the "chin lift" or "jaw thrust"maneuvers
ull the ton ue forward to clean the airwa of lessseverely injured
patients.
Jaw-thrust maneuver. Two hands are placed on the mandibular
ramiand pushed anteriorly, so opening the airway.
Chin-lift maneuver. The tips of the fingers are placed beneath
thepatient's chin and the jaw is lifted anteriorly while the mouth
is
opened by drawing down on the lower lip with the thumb of
thesame hand.
Endotracheal intubation is required at patients with severe
head injury, profound shock.
-
8/8/2019 Lecture 24 General trauma (cor)
2/16
23.07.2010
2
Endotracheal and nasotracheal intubation
Cervical spine injury is always a possibility (ovoid movement of
the neck). Before
intubation the spine should be stabilized until an injury has
been excluded.
Potential spinal injuries. The patient is completely immobilized
on a long
backboard. A rigid cervical collar and paracervical rolls are
placed to protect the
cervical spine.
Consider spine injuryConsider spine injury
In some situations a surgical airway may be required. Surgical
cricothyroidotomy
may be preceded by needle cricothyroidotomy with jet
insufflation to improve
oxygenation.
Surgical airway
Cricothyroidotomy is a preferable emergency procedure.
Technique for cricothyroidotomy. Side view demonstrates that the
cricothyroid
membrane is more superficial than the trachea which makes
performance of a
cricothyroidotomy technically easier than a tracheostomy.
Technique for tracheostomy.
-
8/8/2019 Lecture 24 General trauma (cor)
3/16
23.07.2010
3
Breathing (ventilation)
If there is a decreasedes irator dr ive or an
unstable chest wall, anassisted ventilation isnecessary.
Assisted ventilation may be done using Ambu bag or with a
help of mechanical ventilator.
Most common reasons for ineffective ventilation after
intubation
malposition of endotracheal tube, pneumothorax, and
hemothorax(palpation, auscultation, X-ray to exclude).
In some circumstances (tension pneumothorax) decompression ofthe
chest by needle catheter placement is appropriate prior to
theradiograph.
Circulation (perfusion)
When possible control of the bleeding precedes placement of the
i.v. lines.
(compressive dressing, tourniquet, or placement of pneumatic
antishock
garment (pelvic injuries) may be required. Minimum two i.v.
lines should be
placed percutaneously, or with venous cut-down, or internal
jugular
(subclavian) vein cannulation. Fluid resuscitation begins with a
1000 ml bolus of
LR. Response to therapy is monitored by skin perfusion, UO, or
CVP.
Newly placed central venous catheter via the subclavian access
route.
-
(, , .)
Eye opening:
1 oint - ever
Best verbal response
1 point - no response
A brief examination is done to determine a) level of
consciousness (GCS), b)
pupillary condition c) movement of extremities(paralysis).
Neurologic assessment
2 points - to pain
3 points - to verbal stimuli
4 points - spontaneously
2 points - incomprehensible sounds
3 points - inappropriate words
4 points - disoriented and converses
5 points - oriented and converses
Best motor response:
1 oint - o res onse Total score = 3 - 15;
Less than 10 ointsa at ient
2 points - extension (decerebral rigidity)
3 points - flexion abnormal (decortical rigidity)
4 points - flexion withdrawal
5 points - localized pain
6 points - obey
is serious injury.
15 points - clear consciousness;
13-14 points - stupor;
9-12 points - sopor;
4-8 points - coma;
3 points - death;
-
8/8/2019 Lecture 24 General trauma (cor)
4/16
23.07.2010
4
Examination is done in aead-toe manner
Exposure to complete examination
Reexamine the patientcompletely but expeditiously(diagnosing
other injuries).Examination is done in a head-toe manner, o ta n ng
ancollecting data from laboratoryand radiologic tests. This timeis
also for placement ofadditional lines, catheters (NG,Foley, etc.)
and monitoringdevices.
When the patient is
oxygenating, ventilating, andperfusing adequately a
priorityplane should be established forsubsequent treatment.
Lateral radiograph demonstrating
an L1 burst fracture (arrow).
a priority plane should be established forsubsequent
treatment.
TYPES OF TRAUMATIC INJURIES
Ganglion?Ganglia are cystic, round, usually nontender or
painfulswellings located along tendon sheaths or joint capsules.
Thedorsum of the hand and wrist is a frequent site of
involvement.Flexion of the wrist makes ganglia more prominent;
extensionendsto obscure them. Gan lia ma alsodevelo elsewhere
onthe
hands, wrists, ankles, and feet.
The origin is unclear (overexertion, hereditaryThe origin is
unclear (overexertion, hereditary
predisposition). It grows from a joint and filled
withpredisposition). It grows from a joint and filled withsynovial
fluid like a shellsynovial fluid like a shell
-
8/8/2019 Lecture 24 General trauma (cor)
5/16
23.07.2010
5
Ganglion cyst
Diagnosis is clinical, but XDiagnosis is clinical, but X--ray is
always necessaryray is always necessaryTreatment
is only indicated if ganglion causes severe pain or
limits activity
TreatmentTreatment is only indicated if ganglionis only
indicated if ganglioncauses severe pain or limits activitycauses
severe pain or limits activity
Massage (recurrence)Massage (recurrence)
Aspiration (recurrence)Aspiration (recurrence)
Surgical removal of all theSurgical removal of all the
cyst by orthopedistcyst by orthopedist
Bursitis. Swelling and inflammation of the olecranon (or any
other)bursa may result from trauma. The swelling is superficial to
the
olecranon process. Bony landmarks of the joint may be
attenuateddue to fluid. Also bursitis may affect any other
joints.
Contusion of soft tissuesis characterized by pain, edema,
andbruising as a result of laceration of small vessels of the skin
and
subcutaneous tissue. Trauma to underlying structures must
bepresumed requiring further investigation.
Sprain. Some fibres are torn but the whole ligament is
mechanicallyintact. Pain is provoked by movements in the joint,
localized
tenderness. Bone percussion is painless. Local swelling and
bruisingare common.Treatment:first 24-48 hours ice or chemical cold
pack, elevation,elastic bandage, after two days heat may be used,
NSAID, no weightbearing, removable splint or light cast,
progressive active exercises
after healing
Bivalved cast.The two halves are rejoined
-
8/8/2019 Lecture 24 General trauma (cor)
6/16
23.07.2010
6
Ligament rapture.The ligament is broken in two. Clinical
picture
is the same but accompanied by joint's instability found
duringlocal examination.Medical therapy is the same, immobilization
is necessary. Suture
is done only at some types of rapture (arthroscopic suture of
thecruciate ligament of the knee)
Tendon and muscle rapture. Retraction of ends (muscle
contraction).
Because of the gap the healing does not occur leading to
impairedfunction. The active movements are lost, passive movements
may bepainful. Localized tenderness.Rapture of the insertion of the
quadriceps muscle into the patella
Local swelling and bruising. The gap is visible or palpable.
Lossof active movements may not be obvious if other muscles
take
over the function of the tendon.Rapture of the tendon of the
long head of the left biceps muscle.
When the muscle contracts the long head bunches near the
elbow.
Tendon rapture. Treatment: suturing followed by immobilization
with externalsplintage for 3-6 weeks. Medical treatment is the
same.
Velpeaus bandage can be used.
-
8/8/2019 Lecture 24 General trauma (cor)
7/16
23.07.2010
7
Dislocation and sublaxation
Clicking sound when the dislocation has occurred. Pain
andtenderness, edema and bruising, hemarthrosis, loss of
normaljoint shape. The joint area looks like hollow. The extremity
may
be shortened and loses its normal axis.
Subcoracoid dislocation of the left shoulder
The extremity may beshortened and loses
its normal axis
dislocation of theright shoulder
dislocation of thean e
Treatment of dislocation
Closed joint reduction.
Commonly reduction is done under i.v. sedation. Local anesthesia
(ifused) is done into joints cavity (20 ml 1% lidocaine). Always
assess
neurovascular status.
Ankle dislocation.Assistant helps to stabilize the leg. The foot
istwisted toward the side to which the tallus is dislocated.
23 07 2010
-
8/8/2019 Lecture 24 General trauma (cor)
8/16
23.07.2010
8
Closed joint reduction.
Shoulder joint dislocation. Matsons methodis shown using two
wrappedsheets. Traction and contratraction are applied over a
period of several minutes,
which should reduce the dislocation with a click. After
reduction a shoulder
immobilizer is necessary at position of internal rotation and
adduction.
X-ray confirms reduction.
The arm hangs free off the table with appropriate weights
(approximately
5kg) attached at the wrist (Stimsons method). Usually it takes
20-30
minutes to achieve reduction. Dzhanelidzes methoduses force
produced
by doctors weight.
Motais (left) and Kochers methods of shoulder reduction
Kochers method of reduction of dislocated hip. An assistant
stands
on the side and steadies the pelvis. Traction is applied in the
line ofthe femur. Reduction is achieved with a clunk and is
confirmed byradiology.
Closed reduction of a radial head.The physician holds the
patient injured hand in a hand-shake position.Immobilization
after reduction of dislocation
Positioning used to immobilize a body part
Ankle/foot: 90 0 angle between foot and leg.
Neutraleversion/inversion
Knee: 15-200 flexion
Shoulder: resting at the side of the body Elbow: 900 angle
between forearm and arm. Neutral
pronation/suppination
Wrist: Neutral pronation/suppination, 20-300wristextension
0. ,
300 flexion
Metacarpals, MCP joint, proximal phalanges: wrist positionas
above, MCP joint in 900 flexion, DIP and PIP joints in afull
extension
IP joints middle/distal phalanx: full extension at IP
joints.
23 07 2010
-
8/8/2019 Lecture 24 General trauma (cor)
9/16
23.07.2010
9
Immobilization after reduction of dislocation
Splint padding is done to entire area to be splinted. Evenly,
circular fashion, at
least two layers with extra over bony prominences.Fiberglass
(prefabricated splints can be measured and cut)/plaster (10-15
layers):
generally immobilize one joint above and one joint below
injury.
The splint is applied to the soft roll (after water deepening).
Hold the bandage in
desired position until splint hardens (5-10min with fiberglass,
10-15 min with
aster
Posterior elbow splint(above) and sugar tong forearm
splint(below) are used for
forearm and wrist injuries. Note: the splint reaches the level
of MCP joints
Commercial sling. The elbow is fixed at 900 angle. With the
arm resting across the chest the wrist is elevated higher
whenthe elbow with the thumb pointing upward.
Ulnar gutter splintis used for 4th -5th metacarpal or phalanx
injuries
(above). Radial gutter splint is used for 2nd -3rd metacarpal or
fingers
injuries (below).
Thumb spica splintLong leg splintis used for knee and tibia
injuries (it consists
of two splints for additional stability)
23 07 2010
-
8/8/2019 Lecture 24 General trauma (cor)
10/16
23.07.2010
10
Ankle splintis used at isolated ankle injuries (it consists of
two
splints).
Complications of casts:burns, cast sores, joint contracture
Complications of dislocation:ischemia (vascular compression),
neurologic,
infectious, joint stiffness, instability, recurrent
dislocation.
Range-of-motion exercises for the affected
joint after period of healing and immobilization
Compression of
the popliteal artery
Fractureis a structural break in the normal continuity of the
bone.
bone fracture:
- direct force and indirect
force
Mechanism of cancellous
bone fracture:
- compression and traction
injuries (avulsion).
A) Formation of hematoma; B) after 1 week osteoblasts start to
form as the clotretracts; C) after 3 weeks a procallus begins to
form and stabilize the fracture; D)from 6 to 12 weeks a callus
forms with bone cells; E) in 3 to 4 months osteoclastsbegin to
remodel the fracture site; F) with normal apposition the bone will
becompletely remodeled in 12 months.
Fracture healing (union) Clinical signs
Relative signs:local tenderness, swelling and bruising,
deviationof extremity's axis, disturbance of function of
extremity.
Absolute signs (pathognomonic)to fractures: exposure of the
bonefragments or obvious protrusion of bone fragments under
theintact skin, pathologic mobility, bone crepitation, and
radiologics gns o e rac ure.
Fracture of extremity. Peripheral blood circulation and
nervous
function must be examined (physical examination or
usingadditional tools).
23 07 2010
-
8/8/2019 Lecture 24 General trauma (cor)
11/16
23.07.2010
11
Obvious
deformity ofthe limb
Obvious deformity of the limb
Radiologic confirmation of fracture is absolutely necessary. It
is
done at two planes (AP and lateral view).
Unstable burst fracture of L1 (arrow)
(result of a motor vehicle accident).
Pelvic disruption (arrow).
23.07.2010
-
8/8/2019 Lecture 24 General trauma (cor)
12/16
23.07.2010
12
Description according to fracture line Description according to
displacement ofbone fragments Treatment of fractures
General management
ABC approach Correction of blood loss and shock (pelvic fracture
may
lead to approximately 2 L blood loss)
Pain: splintage and analgesics Coexisting injuries are treated
according to priority plane Tetanus toxoid and AB for o en
fractures
Splintageis done at the scene of injury (to reduce pain
andadditional trauma due to displacement of bone fragments)
Bucks traction may be used for hip
fractures until surgery is performed.
23.07.2010
-
8/8/2019 Lecture 24 General trauma (cor)
13/16
13
Local management
Scheme for fracture management
Define fracture
Detect complications
Does the fracture need reduction?
Is the fracture stable or unstable?
How can the fracture be stabilized?
Does the fracture need immobilization and for how long?
How can the patient best be rehabilitated?
Possible methods of fracture treatment
protection alone
immobilize with external splint without reduction
closed reduction (manipulation or traction) followed
byimmobilization with external splint or traction;
open reduction and external fixation;
excision of fractured fragment and prosthetic replacement
Treatment of open fractureThe aim of surgery is to convert open
fracture to closed one. Tetanus toxoid
and AB are considered.
Wound irrigation. An open fracture of the tibia at initial
operation.
Dissection and excision of tissue as well as lavage with copious
quantities of
fluid (by a jet lavage system). Surgery is finished by closure
of the wound.
Distal superficial femoral artery traumatized at the site of a
fracture of the distal
third of the femur. Blood supply is restored parallel to open
reduction of fracture
Restoration of bone integrity (methods of fracture
reduction)
Gravity methods: collar and cuff, hanging cast
Closed manipulations Traction (fixed or sliding)
Operation
Gravity reduction U-slabwith collar and cuff sling.
Closed manipulations
Fracture reduction using:
23.07.2010
-
8/8/2019 Lecture 24 General trauma (cor)
14/16
14
Fracture reduction using skeletal and skin traction (fixed or
sliding)
The principal elements of sliding
traction: traction and countertractionRussel traction, a form of
skin traction, may
be used for fractures of the hip and femur.
Methods of stabilisation of fractures (immobilization of the
fracture)
External splint: a) plaster of Paris or plastic cast; b)
external fixation;
Internal splint (screws, plate, nail)
Continuous traction a) hanging cast; b) fixed or sliding
traction (skin or
skeletal)
Stabilisation of fractures using Plaster cast
Volkmanns contracture following
fracture of the humerus.A split plaster of Paris cast.
Stabilisation of fractures using external fixation
External fixator applied to a severe lower limb injury, which
was associated with
extensive soft tissue damage with blistering and skin loss. The
fixator provided
early stability and allowed for care of the soft tissues.
Intramedullary nail.The nail stabilizes
a femoral fracture and both proximal
and distal locking help maintain
length, rotation and alignment.
Lumbar fracture-dislocation treated by
posterior spinal instrumentation and
fusion from L2 to L5.
Stabilisation of fractures using internal splints At elderly
patients a surgery should be considered over closed
stabilizationespecially sustained to fracture of the femoral
neck.
Extracapsular fracture of neck of femur fixed by internal
fixation with a
sliding compression screw and six-hole plate
23.07.2010
-
8/8/2019 Lecture 24 General trauma (cor)
15/16
15
Stabilization of fracture usingcontinuous traction
Compound fractures
Severe initial injury
Causes of delayed and nonunion of fractures
Soft tissue interposition
Distraction Infection
Poor blood supply
Inadequate immobilization
Patholo ical fracture
Osteoporosis
Nutritional disorders (malnutrition, vit. D deficit) Metabolic
disorders (uremia, hyperparathyroidism)
Drugs (steroids, cytotoxic drugs)
General rules of bone healing (duration of immobilization)
Fracture of low limb heals twice longer
Fracture in adults heals twice longer
Transverse heals longer then spiral and oblique
Compound and comminuted are particularly slow to unite
No fracture unites in less then 3 weeks
Surgical treatment with open reduction of bone fragments is
indicated at the following situations:
Compound fractures
Reduction of fracture (failure of other types of reduction)
Stabilisation of fracture (failure of other types of reduction)
Management of complications (vascular or head injury)
Soft tissue management
Complications of fractures
Local(nerve, arterial injury followed by acute arterial
ischemia, acute
compartment syndrome (edema of muscle compartments).
Early:skin necrosis, gas gangrene, infection, DVT, embolism;
Late:joint stiffness, osteomyelitis, pseudoarthrosis, deformed
union.
Crash-syndromeis a condition caused by prolonged compressionand
crashing of soft tissues (mainly muscles) resulting
incharacteristic local and general pathologic changes in the
body
developing during and after release of compression
Pathology of the crash-syndromecompression acute arterial
ischemia (compression of arteries, pain is followed
by angiospasm, hypovolemia)
release of compression reperfusion injury (edema of muscle
compartments,
compartment syndrome, and ischemic muscle necrosis)
resorption of toxins from necrotic tissues endotoxicosis
multiple organ
failure
Most common complication of the syndrome are:
- MODS (ARF and AHF) and purulent septic complications
23.07.2010
-
8/8/2019 Lecture 24 General trauma (cor)
16/16
16
Clinical picture
General:early period signs of traumatic shockwith characteristic
hemodinamic
changes.
Local:Initially the skin is warm, PS on arteries is present.
Further an edema
increases, skin necroses appear, and signs of compartment
syndrome develop
(acute arterial ischemia)
Second period is characterized by signs of ARF and poliorganic
failurewith
characteristic clinical and laboratory picture with progress of
fluid-electrolyte
disorders and intoxication.Local changes are less important and
characterized by edema and local septic
complications.
Late periodis accompanied by necrosis and sequestration of dead
muscles,
urulent complications, muscle and joint contractures
At the early period it is very difficult to determine how much
tissues are
devitelized. So an extend of surgery is difficult to
measure.
Treatment
- elastic bandaging (to decrease postischemic edema)
- cooling and splinting of the extremity
- aggressive antishock and detoxication therapy
- , , y , .
Early surgery is indicated at case of steadily progressing edema
and development oflife-threatening ARF
Without aforementioned indications a surgical procedure is done
only after
demarcation of necrotized tissues.
Early surgery fasciotomy, is done to decompress compartment
pressure
Formely used subcutaneous fasciotomy
is currently less popular
Open fasciotomy with or without
necrectomy is a method of choice
A postoperative wound is managed according to commonrules of
untidy wound care preventing cumulation of necrotic
tissues, etc.external fixation is useful if a patient has
coexisting fracture.