Embed Size (px)
DESCRIPTION
Anatomy of the ureters, bladder and urethra
Citation preview

LECTURE 2 - ANATOMY OF THE URETERS, BLADDER AND URETHRA – C. PARSONS
LEARNING OBJECTIVES
To identify and describe structures of the urinary system, from ureters to urethra To become familiar with blood supply, drainage and innervation of these structures To understand the control and process of urination
URETERS
RENAL PELVIS
The ureters begin at the hila of the renal pelvis, called the ureteropelvic junction. The renal pelvis originate from the major calices, which themselves are formed by multiple minor calices.
The ureters are paired muscular tubes 25-30 cm in length that forces the path of the urine into the bladder. They descend on the medial aspect of the psoas major muscle, and at the pelvic brim, they cross the common iliac artery just where it bifurcates into the external and internal iliacs. However sometimes they cross a bit more laterally than that (individual variations) and hence instead cross the external iliac artery. They then curve along the lateral wall of the pelvis, before curving inward anteromedially to enter the bladder.
There are 3 major points of constriction of the ureters, which are of clinical significance because this is usually where kidney stones lodge:
1. Ureteropelvic junction2. Crossing external iliacs3. As ureter traverses the bladder
o The ureters enter the bladder a little bit obliquely through the bladder walls about 2.5 cms apart from one another
BLOOD SUPPLY TO URETERS

Blood supply to the ureters is varied. Branches from the renal artery, gonadal artery, the aorta itself and branches from the internal iliac artery may be commonly involved in the ureter blood supply. Note that branches supplying the abdominal part of the ureters approach medially, while in the pelvis, the vessels approach laterally to the ureters.
Venous drainage in the abdominal region is usually toward the renal and gonadal veins, while venous drainage in the pelvic region is generally towards various venous plexuses, especially the vesical venous plexuses which occupies the fundus region of the bladder.
VENOUS DRAINAGE OF THE PELVIS
Most of the pelvic viscera, other than the blood supply associated with the superior part of the rectum (the superior rectal vein is associated with the inferior mesenteric vein, which is part of the hepatic portal system – this is depicted in purple), is drained through the inferior vena caval system (blue), via the internal iliac.
In many cases the veins are similarly named to the arteries.
PELVIC VENOUS PLEXUSES
These are a fine network of veins surrounding the pelvic viscera:
Rectal Vesical Prostatic Uterine Vaginal
These mostly drain into branches of the internal iliac, but also form anastomoses with veins from the portal system. In cases of liver disease, where you have reduced portal blood flow, alternative routes of blood flow may form through the caval system.
INNERVATION OF URETERS
Nervous supply is from the local autonomic plexuses.
Innervation of the ureters is normally through T11-L1 – which is referred to as ‘above the pelvic pain line’, which spans the upper part of the bladder too.
The pain from the ureters is referred to the ipsilateral lower quadrant, particularly the inguinal region. For example, pain from a kidney stone would be referred pain, and you would perceive it from the ipsilateral lower quadrant – ‘loin to groin pain’.
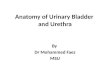
URINARY BLADDER

The bladder has strong muscular walls of detrusor muscle and is highly distensible. It is the reservoir for urine, and varies in size and shape depending on the fullness of the bladder and also other viscera.
In adults, it occupies the lesser pelvis when empty and extends to the abdominal cavity when full. In children less than 6 years old, the bladder is abdominal, and is only truly pelvic during puberty.
The floor of the bladder is firmly anchored or you’d have a floating bladder expelling pee everywhere, whereas the superior surface is surrounded with looser connective fascia and is hence able to expand up into the abdominal cavity.
In its empty state (refer to diagram) it resembles a tetrahedron.
The apex is:o Oriented to the top of pubic symphysiso Urachus (median umbilical ligament) arises from the
apex umbilicus The base is:
o Triangularo Ureters enter at 2 superolateral cornerso The urethra exits at the inferior corner (neck of the
bladder) of the trigone – bounded by the triangle The inferolateral surfaces are:
o Bounded by the levator ani muscles of the pelvic diaphragm and obturator internus muscles
The trigone area is characterised as being a smoother surface that is highly mucosal. The surface is intimately associated with the underlying muscle in the trigone region, and is more loosely connected in areas outside the trigone.
WALL OF BLADDER
Detrusor muscle forms the wall of the bladder. In males the muscle forms the internal urethral sphincter which contracts to prevent ejaculatory reflux of semen back into the bladder – this sphincter usually has some sympathetic tonic contraction in its normal state.
In males, muscles in the neck of the bladder are continuous with fibromuscular tissue of the prostate (which is almost adjacent to the bladder in males). In females, the muscular walls of the bladder are continuous with those of the walls of the urethra.
Loops of the detrusor muscle also form circular sphincter-like rings around the ureteric orifices. When the detrusor muscle is contracted, the circular muscles of the detrusor muscles around the orifices also contract, preventing reflux of the urine back up the ureters in the contracted state.

Above diagram is not important in terms of labels – just shows where things are. The male diagram shows a full bladder while the female one is collapsed. In males, the urethra has 2 curvatures as it runs through the penis. One obvious difference between males and females is that there is a relatively short urethra in females when compared to males. In females it is ~4 cm while in males it is ~20 cm.
ARTERIAL SUPPLY OF THE BLADDER
The bladder is supplied by branches of the internal iliac. The anterosuperior region is supplied by the superior vesicle artery. In males, the fundus and neck are supplied by the inferior vesicular artery, while in females it is supplied by the vaginal arteries. The obturator and inferior gluteal arteries also supply branches to the bladder in a less significant manner.
Venous drainage to the bladder corresponds to arterial supply
MALES FEMALES Vesical venous plexus, which is continuous
with the: Prostatic plexus
o Combined, these plexuses cover the inferior ureter, fundus of bladder, prostate
Vesical venous plexuso Covers the neck of bladder and
associated urethra (pelvic portion)
INNERVATION OF THE BLADDER
The bladder is mainly innervated by the vesical plexus, a plexus which basically lies on the plexus. It is a mixed sympathetic/parasympathetic supply:
Sympathetic:o Inferior thoracic, upper lumbar regions
supply sympathetic fibres to the plexus Parasympathetic::
o Sacral S2-S4 arising from pelvic splanchnic and inferior hypogastric plexus
The external urethral sphincter is under somatic control and there are hence somatic sensory fibres running up from this part of the urethra, eventually joining with the sacral plexus.

URETHRA
MALES
The urethra is a muscular tube about 20 cm long (18-22 cm range). The internal urethral orifice is the beginning of the urethra and the urethra ends at the external urethral orifice. There are four parts:
Intramural or preprostatic urethrao Just at the exit of the bladder,
occupying the internal urethral orifice (?)
Prostatic urethra Internemediate/membranous urethra Spongy urethra
o Basically travels through the length of the penis
The urethra has purposes in both reproduction and voiding of urine. The urethral crest is bordered by the fenestrated prostatic sinuses (2nd
diagram). Through these fenestrations, the prostatic fluid is released in the emission stage, just prior to ejaculation. The ejaculatory duct is where the ductus deferens enters the urethra. It is at the top part of the 2nd diagram at the first schematic constriction that the urethra has its dual purpose.
Entering the urethra are also ducts coming from the bulbourethral glands (bottom of 2nd diagram, near bulb of penis), near the spongy part of the urethra.
BLOOD SUPPLY AND DRAINAGE TO MALE URETHRA
Proximally (area around the prostate gland in the bladder), the urethra is supplied by prostatic branches of the inferior vesicle and middle rectal arteries. It is drained by the prostatic plexus
Distally, the urethra is supplied by the dorsal artery of the penis, which itself is a branch of the internal pudendal artery.
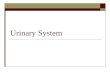
FEMALES
In females the urethra is 4 cm long and 6 mm in diameter (not 6cm as Carl Parsons has written in his lecture). The internal urethral orifice does not have a sphincter. The female urethra is more distensible and hence easier to pass a catheter up through, as it has a lot of elastic fibres incorporated in its walls. The external urethral

orifice lies within the vestibule of the vagina. Vaginal and internal pudendal arteries supply the area, while the veins of the same name drain it.
The image shows the female bladder and urethra. The image shows the external sphincter deep in the perineal pouch, in the floor of the pelvis
CONTROL OF URINATION
Urination is under both reflexive control and voluntary control (both autonomic and somatic). The spinal cord sends reflex loops down to control parts of the bladder – but toilet training means we have voluntary control over the voiding of urine.
There are parasympathetic motor fibres to the detrusor muscle of the bladder, providing contraction of the detrusor muscle. The preganglionic parasympathetic components come from branches of S2-S4. Close to the bladder, we have parasympathetic ganglion, situated close to the bladder. There are mechanoreceptors in the wall, or stretch receptors, which provide an indication of when the bladder is distending. These mechanoreceptors are the nerve endings of cell bodies located within the dorsal root ganglion, which pick up signals from the receptors located in the detrusor muscle. They have the ability to send these signals up into the brainstem (NTS usually involved) hence involving central control of the system.
When we get the filling sensation, it sends outflow through the sympathetic system, which relaxes the detrusor muscle (acting against the parasympathetic system) and also in males, tightens the internal sphincter, providing some tone for the internal sphincter.
When we have a full bladder, the afferent activity increases, and there is a centrally mediated increase in parasympathetic tone which tends to contract the detrusor muscle and bladder, overriding sympathetic signals – there is also a decrease in sympathetic tone. In males, the internal urethral sphincter in males at this time is relaxed, and the only thing that stops the urine from flowing out is the external urethral sphincter, which is under voluntary control. In babies and people lacking voluntary control (e.g. due to high SCI), the urine is stored in the bladder until it reaches tipping point, and then all rushes out – it doesn’t drip out as it is being formed.
SUMMARY
Urine formed in the kidney is conveyed by ureters to the bladder, and voided via urethra Renal caliculi may lodge in narrowings of ureters Arterial supply of the urinary tract shows individual variation, drainage often follows supply Voiding urine involves interplay between autonomic and somatic nervous systems