Embed Size (px)
Citation preview

Integumentary System

Why is this a system?
What does it do for us?

Functional Review
• Protector and barrier between internal organs and external environment
• Barrier against foreign body intrusions – against invading bacteria and foreign matter
• Transmits sensation – nerve receptors– allows for feelings of temperature, pain, light
touch and pressure

Skin Functions
• Regulates body temperature– regulates heat loss
• Helps regulate fluid balance – prevents excessive water & electrolyte loss. – Slow loss up to 600 ml daily by evaporation
• Immune Response Function– inflammatory process

Skin Functions
• Vitamin production – exposure to UV light allows for the conversion
of substances necessary for synthesizing vitamin D
– Necessary to prevent osteoporosis, rickets

• Wound repair through cell replacement
• Allows excretion of metabolic wastes as
minerals
• Provides identity through skin color and facial
features

The skin is the body's largest
organ, covering the entire body.

Structure of the Integument • The skin is the largest organ of the body
comprising 15 percent of total body weight. • Layers of the skin A. Epidermis B. Dermis C. Subcutaneous tissue

Skin appendages• Hair• Nails• Glands: two types of skin glands:

1. Sweat Gland Eccrine sweat glands: are widely
distributed and open directly onto the skin surface
Apocrine sweat glands: open into hair follicle in axillary and genital areas
2. Sebaceous glands: Produce sebum(oily secretion)

• Epidermis: the most superficial layer, then,
devoid of blood vessels
• Epidermis depends on the underlying dermis
for its nutrition

• The dermis is well supplied with blood. It
contains connective tissue, sebaceous
glands, sweat glands and hair follicles.
• It merges below with subcutaneous or
adipose tissue, also known as fat.



15

The color of normal skin depends on four pigments:
• Melanin
• Carotene
• Oxyhemoglobin
• deoxyhemoglobin

• The amount of melanin, the brownish
pigment of the skin, is genetically
determined and is increased by exposure to
sunlight.
• Carotene is a golden yellow pigment that
exists in subcutaneous fat, palms and sole

• Oxyhemoglobin, a bright red pigment,
predominate in the arteries and capillaries. An
increase in blood flow through the arteries to the
capillaries causes a reddening of the skin, whereas
the opposite change usually produces pallor.
• The skin of light-colored people is normally redder
on the palms, soles, face, neck, and upper chest.

• Deoxyhemoglobin, a darker and somewhat
bluer pigment.
• An increased concentration of
deoxyhemoglobin in cutaneous blood
vessels gives the skin a bluish cast known as
cyanosis.

Hair
Adult have two types of hair:
• Vellus hair: short, fine, and relatively
unpigmented
• Terminal hair: thicker, and usually pigmented
( scalp, eyebrows)

Nails
• Nails protect the distal end of the fingers and toes.
• The firm and usually curving nail plate gets its pink
color from the vascular nail bed to which the plate
is firmly attached.
• One forth of the plate (nail root) is covered by the
proximal nail fold.

• The cuticle extends from the fold and functioning
as a seal, protects the space between the fold and
the plate from external moisture
• Lateral nail folds cover the sides of the nail plate
• Fingernails grow approximately 0.1mm daily;
toenails grow more slowly.



Sebaceous glands
• Sebaceous glands produce sebum, a fatty substance
secreted onto the skin surface through the hair
follicle.
• These glands are present on all the skin surfaces
except the palms and soles.
• The sebum lubricate hair and skin and reduces
water loss through the skin.

sweet glands
Are of two types:
• Eccrine glands: are widely distributed, open
directly onto the skin surface, and by their sweet
production help to control body temperature.
• Apocrine glands: are found chiefly in the auxiliary
and genital regions, usually open into hair follicles

Skin Assessment

1- The health history
The purpose of integumentary history is to identify the following:
• Disease of the skin• Systemic disease that have skin manifestations• Physical abuse• Risk for pressure ulcer• Need for health promotion education regarding skin• Promote wound healing
• Prevent skin breakdown and/or additional wounds

Past History• Are you having experience of skin problem, such as
rashes, lesion• Have you noticed any changed in your ability to feel
pain, pressure, light touch, or temperature changed? • Have you had any hair loss or change in the condition
of your hair?• Have you had any change in the condition or
appearance of your nails? • Describe any previous problem within the skin, hair
or nails ( past history)• Have you ever had any allergic skin reaction to food,
medication, plants?

Family history
• Has anyone in your family had a recent illness, rash, or other skin problem?
• Do any family members have the same or similar symptoms?
• Does anyone have allergies?

Lifestyle and personal habits
• Describe your bathing• Have you changed product brands recently?• Do you wear false nails or wigs?• How much sun exposure do you receive daily?• Diet• Sunscreen

• For example, if the patient report a rash, the nurse can use the OLD CART mnemonic to ask follow-up questions in order to obtain a full description of the condition
• Onset: when did it start?• Location: where is it located?• Duration: how long have you had it?• Characteristic symptoms: describe your rash

• Associated manifestations: does it itch? Is there
any discharge?
• Relieving/ exacerbating factors: have you used
or done anything that seems to make it better:
• Treatment: have you put anything on it to treat
it?

2- Physical Assessment

• Adequate lighting• Good visualization• Explain assessment process to patient• Head-to-toe assessment• Remove necessary cloths while providing
respect, warmth and privacy• Appropriate client positions

Copyright 2002, Delmar, A division of Thomson Learning
Inspection of the Skin
• Follow head-to-toe approach• Supine position to inspect anterior surfaces• Special attention to skin folds• Side-lying position to inspect posterior
surfaces

Technique to examination of skin
• Inspection • Palpation • Olfactory senses

Equipment
• Magnifying glass• Good lighting, natural light preferred• Penlight• Clean gloves• Small centimeter rule

Inspections and palpation of skin Color Moisture Temperature Thickness Turgor Edema Lesions Skin odors are usually noted in the skin fold.
39

Color
• Skin color varies from body part to body part and
from person to person. • Pallor easily perceived in the mouth mucosa
particularly in individuals with dark skin. • Cyanosis readily seen in area of least
pigmentation e.g. lips, nail beds, conjunctiva, soles and palm.
40

• Central cyanosis: if the oxygen level in the arterial
blood is low and indicate decreased oxygenation
in the patient
• Central cyanosis is best identified in the lips, oral
mucosa and tongue

• Peripheral cyanosis: the oxygen level is normal.
occurs when cutaneous blood flow decreases and
slows and tissues extract more oxygen than usual
from the blood. May be a normal response to
anxiety or a cold environment
• Cyanosis of the nails, hand and feet may be
central or peripheral in origin

• Jaundice or Yellow seen in client’s sclera, skin and
conjunctiva.
• Erythema may indicate circulatory changes

44

moisture of skin
• Skin is normally smooth and dry to touch without flaking or
cracking. • Skin folds e.g. axillae are normally moist. • In presence of lesions or ooze fluid, nurse must wear gloves
to prevent exposure to infections • Carefully inspect skin folds where moisture may cause skin
breakdown
• Moisture indicates: Degree of client’s hydration Dryness: Vitamin A def., hypothyroidism Oily: Acne
45

Temperature• Temperature of skin depends on the amount of blood
circulating through dermis.
• Generalized warmth: (Fever, Hyperthyroidism)
• Local warmth: (Inflammation)
• Coolness: (Hypothyroidism, Hypothermia, Shock, Low
cardiac output)
• Palpation of skin with dorsum of the hand.
• Assessment of skin is critical point in some conditions
such as: after cast application, or after vascular surgery. 46

Texture• Note the roughness or smoothness of the skin• Texture of skin normally smooth, soft and flexible
• If any abnormalities in texture found you must ask
the client is he exposed to any recent injury to the
skin?
• Nurse determines whether the client’s skin is
smooth or rough, thin or thick, tight or flexible.
• Rough: (Hypothyroidism)47

Mobility and Turgor
• Turgor: is the skin elasticity diminished by edema or dehydration.
• Assessment of turgor done by lift a fold of skin between the thumb and forefinger and released.
• Note the ease with which it lifts up (mobility) and the speed with which it returns into place (turgor)
• Normally skin return immediately to its position. • Failure of this process means dehydration. • Decreased mobility in edema and Scleroderma • Decrease in turgor predisposes the client to skin
breakdown.

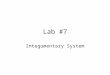
Edema• Edema : "Build up of fluid in the interstitial
spaces“• Inspected for location• may be localized due to injury Or systematic as in
heart failure• Systematic edema most often occurs in the
dependent portions of the body such as feet, legs and sacral area
• Edema may be pitting or nonpitting• The skin appears puffy and feels tight

Edema Scale


Lesions
• Normally skin free of lesions except common freckles.
• If lesion present, inspection must done for their anatomic location and distribution, arrangement, morphology, color and size
• Palpation for lesion’s mobility, contour (flat, raised or depressed) and consistency (soft or hard).
• Cancerous lesions frequently undergo changes in color and size.

Assessment of Lesions
• Color• Shape• Size in cm• Elevation (flat or raised)• Location and distribution on body• Exudate (color, odor)

skin color changes
• Cyanosis• Jaundice• Carotenemia: is the presence in blood of the
orange pigment carotene from excessive intake of carrots or other yellow fruits or vegetables . unlike jaundice it does not affect the sclera, which remain white


• Vitiligo: s a condition that causes depigmentation of parts of the skin. It occurs when skin pigment cells die or are unable to function

Skin lesions- anatomic location and distribution
• Psoriasis: meaning "itching condition" or "being itchy. Appears mainly on extensor surfaces

• atopic eczema or eczema is a type of dermatitis,, relapsing, non-contagious and itchy skin disorder. Appears mainly on flexor surfaces

Skin lesions- pattern and shapes
• Linear : e.g. linear epidermal nevus

• Clustered: herpes simplex

• Annular, arciform: annular lesion of tinea facial

Flat, non palpable lesion with change in skin color
• Macule: small flat spots up to 1 cm.
• Patch: flat spot. 1cm or larger

Mongolian Spot Birthmark: A dense collections of melanocytes
(not a bruise)

Palpable elevations: solid masses
• Papule : up to 1 cm. A papule is a circumscribed, solid elevation of skin with no visible fluid
• Plaque: elevated superficial lesion 1cm or larger, often formed by coalescence of papules


• Nodules: are solid, raised areas in or under the skin that are larger than 0.5 centimeters. Firmer than papule

• Cyst: nodule field with expressible material, either liquid or semisolid
•

• Wheal: somewhat irregular, relatively transient superficial area of localized skin edema

Palpable elevations with fluid-filled cavities
• Vesicle: up to 1 cm, filled with serous fluid

• Bulla: 1cm or larger, filled with serous fluid

• Pustule: filled with pus

Secondary skin lesion
• Scale: a thin flake of dead exfoliated epidermis

• Crust: Crusting is the result of the drying of plasma or exudates (pus or blood) on the skin

• Scars: connective tissue that arises from injury or disease

• Fissure: a linear crack in the skin, often resulting from excessive dryness
• Ulcer: a deeper loss of epidermis and dermis

• Petechia: is a small (1-3 mm) red or purple spot on the skin, caused by a minor hemorrhage (broken capillary blood vessels)

• ecchymosis: is the escape of blood into the tissues from ruptured blood vessels. The term also applies to the subcutaneous discoloration resulting from seepage of blood within the contused tissue. (> 3mm)


Hair and Scalp• Assessment done for distribution, thickness,
texture, and lubrication of the hair.
• Some events which affect the distribution of hair
over the body e.g. client with hormone disorders,
woman with hirsutism
• Amount of hair covering extremities may be
reduced as a result of aging and arterial
insufficiency especially in lower limbs. 79

• Scaliness or dryness of the scalp is frequently
caused by dandruff or psoriasis.
• Color of hair depends on the amount of melanin
present and varies from pale blond to black
• Inspect the scalp for lesions and parasites by
separating the hair

Nails Assessment
• Nails reflect an individual's general state of
health, state of nutrition, and occupation.
• Nails are normally transparent, smooth, and
convex, with a 160 degrees angle between nail
base and skin.

• The surrounding cuticles are smooth, intact and without inflammation.
• Nail bed is normally firm on palpation.
• Nails normally grow at a constant rate.
• Note their color and shape and any lesions

Assessment of Nails
• Shape and contour: slightly curved or flat and smooth, 160 degrees.
• Consistency- surface smooth and regular, not brittle or splitting, uniform thickness.
• Capillary Refill- depress nailbed color blanches , color should return <1-2 seconds

Abnormal condition of nail
84

Anonychia: complete absence of nails

Platunychia: flatting nails

Onycholysis: separation of nail form nail bed (thyrotoxicosis)

Koilonychia : nails like spoon shape (iron deficiencies anemia)
• It refers to abnormally thin nails (usually of the hand) which have lost their convexity, becoming flat or even concave in shape. In a sense, koilonychia is the opposite of nail clubbing.

89

Melanoychia: presence of brown color in nails plate

Leukonychia ( white nails) :white discoloration appearing on nails

• Paronychia: inflammation of tissue surrounding the nail
•

Considerations as the nurse…
•Is the patient nutritionally challenged?
•Is the patient immobile?
•Does the skin appear paper-like or fragile?

Diabetics are at high risk for slow healing wounds due to vascular changes leading to arteriosclerosis (thickening,
loss of elasticity, and calcification of arterial
walls).

Skin Ulcer

Necrotic Toes
What causes this? Decreased/impaired tissue perfusion.

Dry, Scaly Skin

Age Spots:(Liver Spots) Part of the skin’s
normal aging process. Appear as flat gray, brown or black spots. They vary in size and usually appear on the face, hands,
shoulders and arms; areas most exposed to the sun.

Wound Types

Contusions: Bleeding under or within layers of skin

Abrasion:Surface scrape, open wound

Laceration:Tissues torn apart, open wound; edges
often jagged

Puncture or Penetrating: Penetration of skin and underlying tissues; open wound

Copyright 2002, Delmar, A division of Thomson Learning
Wound Evaluation
• Location• Color• Drainage• Odor• Size• Depth• Measure the borders

Copyright 2002, Delmar, A division of Thomson Learning
Safety Tips for the Elderly
• Identify environmental hazards and minimize risk
• Interventions to decrease risk for thermal injuries
• Interventions to maintain skin integrity and prevent damage

Risk factors for pressure sores
People are at risk of developing pressure sores if they have difficulty moving and are unable to easily change position while seated or in bed. Immobility may be due to:
• Generally poor health or weakness• Paralysis• Injury or illness that requires bed rest or wheelchair use• Sedation• Coma

Age. The skin of older adults is generally more
fragile, thinner, less elastic and drier than the
skin of younger adults. Also, older adults usually
produce new skin cells more slowly. These
factors make skin vulnerable to damage.

• Lack of sensory perception. Spinal cord injuries,
neurological disorders and other conditions can
result in a loss of sensation. An inability to feel
pain or discomfort can result in not being aware
of bedsores or the need to change position.

• Weight loss. Weight loss is common during
prolonged illnesses, and muscle atrophy and
wasting are common in people with paralysis.

• Poor nutrition and hydration. People need
enough fluids, calories, protein, vitamins and
minerals in their daily diet to maintain healthy
skin and prevent the breakdown of tissues.

• Excess moisture or dryness. Skin that is moist
from sweat or lack of bladder control is more
likely to be injured and increases the friction
between the skin and clothing or bedding. Very
dry skin increases friction as well

• Bowel incontinence. Bacteria from fecal
matter can cause serious local infections and
lead to life-threatening infections affecting the
whole body.

• Medical conditions affecting blood flow. Health
problems that can affect blood flow, such as
diabetes and vascular disease, increase the risk
of tissue damage.

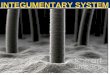
Assessment using the Braden Scale
The Braden scale assesses a patient's
risk of developing a pressure ulcer by
examining six criteria:

1-Sensory perception
This parameter measures a patient's ability to
detect and respond to discomfort or pain
that is related to pressure on parts of their
body.

2- Moisture
• Excessive and continuous skin moisture can
pose a risk to compromise the integrity of the
skin by causing the skin tissue to become
macerated and therefore be at risk for
epidermal erosion. So this category assesses
the degree of moisture the skin is exposed
to.

3- Activity
This category looks at a clients level of physical
activity since very little or no activity can
encourage atrophy of

4- Mobility
This category looks at the capability of a
client to adjust their body position
independently. This assesses the physical
competency to move and can involve the
clients willingness to move.

5- Nutrition
The assessment of a clients nutritional status
looks at their normal patterns of daily
nutrition. Eating only portions of meals or
having imbalanced nutrition can indicate a
high risk in this category.

6- Friction
Friction looks at the amount of assistance a client needs
to move and the degree of sliding on beds or chairs
that they experience. This category is assessed because
the sliding motion can cause shear which means the
skin and bone are moving in opposite directions
causing breakdown of cell walls and capillaries.[5]

• Each category is rated on a scale of 1 to 4, excluding the 'friction category which is rated on a 1-3 scale. This combines for a possible total of 23 points, with a higher score meaning a lower risk of developing a pressure ulcer and vice-versa. The Braden Scale assessment score scale:
• Very High Risk: Total Score 9 or less• High Risk: Total Score 10-12• Moderate Risk: Total Score 13-14• Mild Risk: Total Score 15-18• No Risk: Total Score 19-23