Embed Size (px)
Citation preview

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
in collaboration with:
MULTIDISCIPLINARYAPPROACH
Lebanese Societyof MedicalOncology (LSMO)National Forum
16th
LOP: 11 CME Order of Nurses: 12 CNE

ZYTIGA® as first-line therapy in mCRPC and mHSPC delivers remarkable overall survival benefits without compromising quality of life, so your patients can stay active for longer.
FIRST NOVEL HORMONAL AGENT IN mCRPC*1
4.4 months median life extension vs prednisone alone in post-ADT (HR 0.81; 95% CI 0.70–0.93; P=0.0033)**2
4.6 months median life extension in post-chemotherapy patients (HR 0.74; 95% CI 0.64–0.86; P<0.0001)3
FIRST IN NEWLY DIAGNOSED HIGH-RISK mHSPC*1 Superior median overall survival vs ADT alone (HR 0.62; 95% CI 0.51–0.76; P<0.001)†4
SINCE 2011
FOR MAXIMUM IMPACT, USE ZYTIGA® PLUS PREDNISONE FIRST-LINE IN mCRPC AND mHSPC
Time for life
mCRPC=metastatic castration-resistant prostate cancer; mHSPC=metastatic hormone-sensitive prostate cancer; ADT=androgen deprivation therapy * ZYTIGA® approved for mCRPC post-chemotherapy in September 2011, mCRPC post-ADT in December 2012 and for newly diagnosed high-risk mHSPC in November 2017 ** Asymptomatic or mildly symptomatic patients with mCRPC post-ADT † Median time not reached for ZYTIGA® group

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
Welcome Letter
On behalf of the LSMO Organizing Committee, It gives me great pleasure to invite you all to participate in the “16th Lebanese Society of Medical Oncology National Forum LSMO” which will be held from 11-13 April 2019 at Phoenicia Hotel in Beirut Lebanon.
The objective of this unique conference is to promote the highest standards of healthcare in the management and support of patients with cancer. The program aims at equipping healthcare professionals with knowledge about recent developments, advance the effectiveness of healthcare practice and delivery and increase the quality of patient care.
The congress will provide both a forum for exchange on cutting-edge scientific and clinical information and will facilitate interactions among physicians, researchers, scientists, clinicians and other healthcare professionals from around the world to navigate the various challenges faced in further refining the health outcomes of patients suffering from cancer.
The scientific program contains a series of high-profile plenary presentations, symposia and concurrent sessions. Our aim is to bridge gaps and pave the future by hosting several international speakers from North America, Europe and the region who will be giving lectures on the recent updates in primary care, share valuable scientific knowledge in oncology, ranging from diagnostic and therapeutic tools and techniques to cutting-edge research.
I sincerely hope that this conference will deliberate and discuss all the different facets of oncology and come up with recommendations that will lead to a better, healthier world. The LSMO congresses have been very successful & well attended congresses with outstanding scientific programs where we can ensure that the 16th Annual Congress will not be an exception. We will put together another milestone on the way to success, focusing on the most important instrument to further improve our society: multiplying knowledge by sharing it with each other.I am convinced, the program will provide you with new information, better knowledge in oncology, provide ideas on how to improve your research and results and it will be a stimulus to further harmonize our medical standards and to successfully compete with our neighboring disciplines. Looking forward to a successful and fruitful congress and hoping to see you all there!
Nizar Bitar, MDLSMO President

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
Scientific Committee PresidentRoger Khater, MD
Past PresidentJoseph Makdessi, MD
TreasurerTherese Abou Nasr, MD
PresidentNizar Bitar, MD
President ElectRoger Khater, MD
General SecretaryOussama Jradi, MD
LSMO PresidentNizar Bitar, MD
Ahmad Awada, MDJeffrey Gregg, MDPeter Niehoff, MDPeter Schmid, MDRuben Cabanillas, MD
Scientific Committee
Executive Board
International Faculty
Members
Ali Shamseddine, MDArafat Tfayli, MDFadi Nasr , MD
MembersHanane Yassine, MD Mohamad Haidar, MDNaji Amro, MD
Rita Murr , MDWalid Moukadem, MD
Hazem Assi, MD Jad Wakim, MD Joseph Kattan, MD
Joseph Makdessi, MDRita Murr , MD Therese Abou Nasr , MD
Sana Al-Sukhun, MDShouki Bazarbachi, MDStephan Chia, MDSuayib Yalcin, MDYohann Loriot, MD

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
Thursday, April 11, 201908:00 Registration
Moderator: Fadi EL Karak
09:00 - 09:45 Optimizing Management of Pre/Post Menopausal Women with HR+ve ABC Patients
Novartis Symposium
Stephen Chia
09:45 - 10:30 Current Practice and Opportunities in the Management of HR+/HER2- mBC: Optimizing the Role of CDK4/6 Inhibitors in Clinical Practice
Pfizer Symposium
Hady Ghanem
10:30 - 10:50 Coffee Break
10:50 - 11:35 Are all CDK4/6i the same? How Abemaciclib was Designed to be Different
Lilly Symposium
Hazem Assi
11:35 - 12:05 Opening CeremonyMaster of CeremonyAddress of the President of LSMO Prof. Nizar Bitar
Address of AMACC General SecretaryProf. Sami Khatib
Address of the President of The Lebanese Order of Physicians in BeirutProf. Raymond Sayegh
Address of the President of the Lebanese RepublicGeneral Michel Aoun

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
Thursday, April 11, 2019
Moderator: Nizar Bitar
12:05 - 12:50 Current Questions on Why, When and How to Treat Non-Metastatic Castration-Resistant Prostate Cancer
Janssen Symposium
Marwan GhosnMichel Jabbour
12:50 - 13:50 Lunch Break
13:50 - 14:50 General SessionModerators: Ali Youssef - Zahera Fahed
13:50 - 14:15 Sequence of Treatment in Advanced Neuroendocrine Tumors
Ali Shamseddine
14:15 - 14:40 Role of Checkpoints Inhibitors in the Adjuvant and Neoadjuvant Settings of Solid Tumors
Ahmad Awada
14:40 - 15:25 Reshaping the Management Paradigm of ALK/ROS1 Positive Non-Small Cell Lung Cancer (NSCLC)
Pfizer Symposium
Arafat Tfayli
15:25 - 15:45 Coffee Break
Moderators: Nizar Bitar - Arafat Tfayli
15:45 - 16:30 The Role of Denosumab for Prevention of Skeletal Related Complications in Multiple Myeloma
Georges Chahine
Denosumab for the Prevention of Skeletal-Related Events in Patients with Bone Metastasis fromSolid Tumors
Amgen Symposium
Sana Al-Sukhun

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
Thursday, April 11, 2019
16:30 - 18:30 Breast SessionModerators: Georges El Hachem - Clemence Matta - Riwa Sakr - Sami El Khatib
16:30 - 16:50 Genomic Expression Profiling and Selection ofAdjuvant Systemic Therapy in Early Breast Cancer
Stephen Chia
16:50 - 17:10 Optimizing Adjuvant Therapy Decisions for HER2-Positive Early Breast Cancer
Nagi Saghir
17:10 - 17:30 Neoadjuvant Treatment in Primary Operable Breast Cancer: A More Individualized Approach to Systemic Therapies
Stephen Chia
17:30 - 17:50 Beyond HER2 and CDK4/6 Agents in Advanced Breast Cancers: Molecular Aberrations, New Targets and New Molecular Agents
Ahmad Awada
17:50 - 18:10 Targeting Immune Checkpoints in TNBC Hazem Assi
18:10 - 18:30 Adjuvant Endocrine Therapy in Early HR-Positive Breast Cancer, the Controversy of Duration
Sana Al-Sukhun
18:30 - 19:15 Role of Immunotherapy in mTNBC Roche Symposium
Peter Schmid

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
Friday, April 12, 2019
08:30 - 10:10 Lung CancerModerators: Rita El Murr - Ali Youssef - Ali Monzer
08:30 - 08:55 Local Ablation Techniques in Early Stage NSCLC Nadim Muallem
08:55 - 09:20 Immunotherapy in Non-Mutation Driven Advanced NSCLC Fadi Karak
09:20 - 09:45 Advances in the Management of SCLC Ghazi Nsouli
09:45 - 10:10 Approach to Patients with EGFR or ALK Mutated NSCLC Arafat Tfayli
10:10 - 10:35 Mesothelioma: New Treatment Options Therese Abi Nasr
10:35 - 10:55 Coffee Break
10:55 - 11:40 The Promise of Immunotherapy in Melanoma
BMS Symposium
Hady Ghanem
11:40 - 12:40 Head & NeckModerators: Mouin Moubarak - Marcel Massoud - Abdel Fattah Kheir
11:40 - 12:00 Immunotherapy in Head and Neck Cancers Hady Ghanem
12:00 - 12:20 Approach to Patients with Iodine-Refractory Thyroid Cancer Marwan Ghosn
12:20 - 12:40 Chemotherapy/Radiation vs. Cetuximab/Radiation Bassem Youssef
12:40 - 13:25 Pembrolizumab, Redefining the Standard of Care inMetastatic Non-Small Cell Lung Cancer
MSD Symposium
Ziad Salem
13:25 - 14:25 Lunch Break
14:25 - 15:25 Cancers in Young AdultsModerators: Hanane Yassine - Abir El Ahmadie
14:25 - 14:45 Bone Sarcoma Treatment in 2020: Current Advances Raya Saab
14:45 - 15:05 Surgery for Bone Sarcomas:Tumor Control and Functional Outcome
Johnny Abdel Nour
15:05 - 15:25 Role of Radiation Therapy in Bone Sarcomas Caroline Jabbour

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
Friday, April 12, 2019
15:25 - 16:10 Implementing a Treatment Strategy in ManagingGastric and GEJ Cancer Eli Lilly Symposium
Ali Shamseddine
16:10 - 16:30 Coffee Break
16:30 - 17:15 Looking Beyond Second-Line Treatment in Metastatic Colorectal Cancer
Servier Symposium
Joseph KattanFadi Nasr
17:15 - 18:15 GI SessionModerators: Oussama Jradi - Sally Tamraz - Haifa Dbouk
17:15 - 17:35 Recent Management of Advanced Cholangiocarcinoma Shouki Bazarbashi
17:35 - 17:55 Adjuvant and Neoadjuvant Treatment in Gastric Cancer Suayib Yalcin
17:55 - 18:15 Is Total Neoadjuvant Therapy is Becoming the Standard of Care for Locally Advanced Rectal Cancer
Ali Shamseddine
18:15 - 19:00 Pancreatic Session; Management of Resectable Pancreatic CancerModerators: Mahmoud Wehbe - Evelyne Helou
18:15 - 18:30 The role Of Hepatobiliary Surgery on Outcome Claude Tayyar
18:30 - 18:45 Adjuvant and Neoadjuvant Therapy in PancreaticCancer
Fadi Farhat
18:45 - 19:00 Impact of Radiation Therapy on Survival in PancreaticCancer
Yousef Zaidan
Moderator: Nizar Bitar
19:00 - 20:15 Unlocking the Potential in Precision Medicine Roche Launching Symposium
Ruben CabanillasJeffrey Gregg
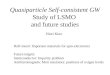
In advanced gastric/GEJ adenocarcinomaAdding CYRAMZA to paclitaxel significantly increased OS vs paclitaxel alone1
you’ve gotI need everything
I don’t want a
fairy tale
CYRAMZA Summary of Product Characteristics:CYRAMZA® is a human vascular endothelial growth factor receptor 2 Antagonist indicated • as a single agent or in combination with paclitaxel, for treatment of advanced gastric or gastro-esophageal junction adenocarcinoma, with disease progression on or after prior fluoropyrimidine- or platinum-containing chemotherapy. • in combination with docetaxel, for treatment of metastatic nonsmall cell lung cancer with disease progression on or after platinum-based chemotherapy. Patients with EGFR or ALK genomic tumor aberrations should have disease progression on FDA-approved therapy for these aberrations prior to receiving CYRAMZA.• in combination with FOLFIRI, for the treatment of metastatic colorectal cancer with disease progression on or after prior therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine. DOSE AND ADMINISTRATION: For intravenous infusion only. Do not administer as an intravenous push or bolus. Gastric Cancer• The recommended dose of CYRAMZA either as a single agent or in combination with weekly paclitaxel is 8 mg/kg every 2 weeks. Non-Small Cell Lung Cancer• Administer CYRAMZA at 10 mg/kg intravenously on day 1 of a 21-day cycle prior to docetaxel infusion. Colorectal Cancer • Administer CYRAMZA at 8 mg/kg intravenously every 2 weeks, prior to FOLFIRI administration. DOSAGE FORMS AND STRENGTHS: Injection: 100 mg/10 mL (10 mg per mL) solution, single-dose vial and 500 mg/50 mL (10 mg per mL) solution, single-dose vial. CONTRAINDICATIONS None. WARNINGS AND PRECAUTIONS • Arterial Thromboembolic Events (ATEs): Serious, sometimes fatal ATEs have been reported in clinical trials. Discontinue CYRAMZA for severe ATEs.• Hypertension: Monitor blood pressure and treat hypertension. Temporarily suspend CYRAMZA for severe hypertension. Discontinue CYRAMZA for hypertension that cannot be medically controlled. • Infusion-Related Reactions: Monitor for signs and symptoms during infusion.• Impaired Wound Healing: Withhold CYRAMZA prior to surgery.• Clinical Deterioration in Patients with Cirrhosis: New onset orworsening encephalopathy, ascites, or hepatorenal syndrome canoccur in patients with Child-Pugh B or C cirrhosis.• Reversible Posterior Leukoencephalopathy Syndrome: Discontinue CYRAMZA.• Proteinuria Including Nephrotic Syndrome: Monitor proteinuria. Interrupt CYRAMZA for urine protein levels ≥2 g/24 hours. Permanently discontinue CYRAMZA for urine protein levels>3 g/24 hours or for nephrotic syndrome. • Thyroid Dysfunction: Monitor thyroid function during treatment with CYRAMZA. • Embryofetal Risk: Can cause fetal harm. ADVERSE REACTIONS • The most common adverse reactions observed in single-agent CYRAMZA-treated patients at a rate of ≥10% and ≥2% higher than placebo were hypertension and diarrhea. • The most common adverse reactions observed in patients treated with CYRAMZA plus paclitaxel at a rate of ≥30% and ≥2% higher than placebo plus paclitaxel were fatigue, neutropenia, diarrhea, and epistaxis.• The most common adverse reactions observed in patients treatedwith CYRAMZA plus docetaxel at a rate of ≥30% and ≥2% higher than placebo plus docetaxel were neutropenia, fatigue/asthenia, and stomatitis/mucosal inflammation. • The most common adverse reactions observed in patients treated with CYRAMZA plus FOLFIRI at a rate of ≥30% and ≥2% higher than placebo plus FOLFIRI were diarrhea, neutropenia, decreased appetite, epistaxis, and stomatitis.
For further information about Lilly and Lilly products please contact us on the below address:Lebanon: Jisr el Wati, Sin El Fil, Fouad Ammoun Street, Plot #2252, 4th & 5th Floors, POB: 55-158Tel: (961) 1 504 700, Fax: (961) 1 504 701
For adverse events and safety reporting, please send an email to the following email address : [email protected].
PP-R
B-LB
-001
1
40 %40.1% (34.7, 45.5)
(n=330)In the placebo + paclitaxel arm
n=335), OS rate was 30.2%(25.1, 35.3) at 1 year.
1-yearOS rate
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
OS
PR
OB
AB
ILIT
Y
TIME FROM RANDOMIZATION (MONTHS)
CYRAMZA+ paclitaxel
(n=330)
Placebo+ paclitaxel(n=335)
9.6MONTHS(8.5, 10.8)
7.4MONTHS
(6.3, 8.4)
1.0
0.8
0.6
0.4
0.2
0.0
CYRAMZA+ paclitaxel
Placebo+ paclitaxel
330 308 267 228 185 148 116 78 60 41 24 13 6 1 0
335 294 241 180 143 109 81 64 47 30 22 13 5 2 0
NUMBER AT RISK
CYRAMZA + paclitaxel
Placebo+ paclitaxel
CI=confidence interval; GEJ=gastroesophageal junction; HR=hazard ratio; OS=overall survival. References: 1. Wilke H, Muro K, Van Cutsem E, et al; for the RAINBOW Study Group. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol. 2014;15(11):1224-1235.

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
In advanced gastric/GEJ adenocarcinomaAdding CYRAMZA to paclitaxel significantly increased OS vs paclitaxel alone1
you’ve gotI need everything
I don’t want a
fairy tale
CYRAMZA Summary of Product Characteristics:CYRAMZA® is a human vascular endothelial growth factor receptor 2 Antagonist indicated • as a single agent or in combination with paclitaxel, for treatment of advanced gastric or gastro-esophageal junction adenocarcinoma, with disease progression on or after prior fluoropyrimidine- or platinum-containing chemotherapy. • in combination with docetaxel, for treatment of metastatic nonsmall cell lung cancer with disease progression on or after platinum-based chemotherapy. Patients with EGFR or ALK genomic tumor aberrations should have disease progression on FDA-approved therapy for these aberrations prior to receiving CYRAMZA.• in combination with FOLFIRI, for the treatment of metastatic colorectal cancer with disease progression on or after prior therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine. DOSE AND ADMINISTRATION: For intravenous infusion only. Do not administer as an intravenous push or bolus. Gastric Cancer• The recommended dose of CYRAMZA either as a single agent or in combination with weekly paclitaxel is 8 mg/kg every 2 weeks. Non-Small Cell Lung Cancer• Administer CYRAMZA at 10 mg/kg intravenously on day 1 of a 21-day cycle prior to docetaxel infusion. Colorectal Cancer • Administer CYRAMZA at 8 mg/kg intravenously every 2 weeks, prior to FOLFIRI administration. DOSAGE FORMS AND STRENGTHS: Injection: 100 mg/10 mL (10 mg per mL) solution, single-dose vial and 500 mg/50 mL (10 mg per mL) solution, single-dose vial. CONTRAINDICATIONS None. WARNINGS AND PRECAUTIONS • Arterial Thromboembolic Events (ATEs): Serious, sometimes fatal ATEs have been reported in clinical trials. Discontinue CYRAMZA for severe ATEs.• Hypertension: Monitor blood pressure and treat hypertension. Temporarily suspend CYRAMZA for severe hypertension. Discontinue CYRAMZA for hypertension that cannot be medically controlled. • Infusion-Related Reactions: Monitor for signs and symptoms during infusion.• Impaired Wound Healing: Withhold CYRAMZA prior to surgery.• Clinical Deterioration in Patients with Cirrhosis: New onset orworsening encephalopathy, ascites, or hepatorenal syndrome canoccur in patients with Child-Pugh B or C cirrhosis.• Reversible Posterior Leukoencephalopathy Syndrome: Discontinue CYRAMZA.• Proteinuria Including Nephrotic Syndrome: Monitor proteinuria. Interrupt CYRAMZA for urine protein levels ≥2 g/24 hours. Permanently discontinue CYRAMZA for urine protein levels>3 g/24 hours or for nephrotic syndrome. • Thyroid Dysfunction: Monitor thyroid function during treatment with CYRAMZA. • Embryofetal Risk: Can cause fetal harm. ADVERSE REACTIONS • The most common adverse reactions observed in single-agent CYRAMZA-treated patients at a rate of ≥10% and ≥2% higher than placebo were hypertension and diarrhea. • The most common adverse reactions observed in patients treated with CYRAMZA plus paclitaxel at a rate of ≥30% and ≥2% higher than placebo plus paclitaxel were fatigue, neutropenia, diarrhea, and epistaxis.• The most common adverse reactions observed in patients treatedwith CYRAMZA plus docetaxel at a rate of ≥30% and ≥2% higher than placebo plus docetaxel were neutropenia, fatigue/asthenia, and stomatitis/mucosal inflammation. • The most common adverse reactions observed in patients treated with CYRAMZA plus FOLFIRI at a rate of ≥30% and ≥2% higher than placebo plus FOLFIRI were diarrhea, neutropenia, decreased appetite, epistaxis, and stomatitis.
For further information about Lilly and Lilly products please contact us on the below address:Lebanon: Jisr el Wati, Sin El Fil, Fouad Ammoun Street, Plot #2252, 4th & 5th Floors, POB: 55-158Tel: (961) 1 504 700, Fax: (961) 1 504 701
For adverse events and safety reporting, please send an email to the following email address : [email protected].
PP-R
B-LB
-001
1
40 %40.1% (34.7, 45.5)
(n=330)In the placebo + paclitaxel arm
n=335), OS rate was 30.2%(25.1, 35.3) at 1 year.
1-yearOS rate
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
OS
PR
OB
AB
ILIT
Y
TIME FROM RANDOMIZATION (MONTHS)
CYRAMZA+ paclitaxel
(n=330)
Placebo+ paclitaxel(n=335)
9.6MONTHS(8.5, 10.8)
7.4MONTHS
(6.3, 8.4)
1.0
0.8
0.6
0.4
0.2
0.0
CYRAMZA+ paclitaxel
Placebo+ paclitaxel
330 308 267 228 185 148 116 78 60 41 24 13 6 1 0
335 294 241 180 143 109 81 64 47 30 22 13 5 2 0
NUMBER AT RISK
CYRAMZA + paclitaxel
Placebo+ paclitaxel
CI=confidence interval; GEJ=gastroesophageal junction; HR=hazard ratio; OS=overall survival. References: 1. Wilke H, Muro K, Van Cutsem E, et al; for the RAINBOW Study Group. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol. 2014;15(11):1224-1235.

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
Saturday, April 13, 2019
08:15 - 09:00 Extend the Possibilities for Multiple Myeloma with NinlaroTakeda Symposium
Colette Hanna
09:00 - 09:45 From Theory to Clinical Practice:Hallmarks of Immunotherapy CombinationsBMS Symposium
Sally Tamraz
09:45 - 10:45 Prostate SessionModerators: Moussa Dhainy - Maha Manachi - Fouad Khoury
09:45 - 10:05 The Paradigm Shift in Metastatic Hormone-Sensitive Prostate Cancer
Yohann Loriot
10:05 - 10:25 Nonsurgical Treatment of Localised Prostate Cancer Peter Niehoff
10:25 - 10:45 PSA Rising in Non-Metastatic Castration ResistantProstate Cancer
Elie Nemr
10:45 - 11:30 mCRPC Management: Clinical Cases Discussion from a Multidisciplinary Perspective
Astellas Symposium
Elie Nemr Deborah Mukherji
11:30 - 12:00 Coffee Break
12:00 - 12:15 An Evolving CLL Treatment Paradigm:VenclextaTM in Relapsed/Refractory CLLLecture Sponsored by Abbvie
Colette Hanna

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
Saturday, April 13, 2019
12:15 - 13:15 Bladder SessionModerators: Anthony Saroufim - Layale Halabi - Rami Nasr
12:15 - 12:35 Immunotherapy in Early Stages Bladder Cancer Joseph Kattan
12:35 - 12:55 Nonsurgical Treatment in Localised Bladder Cancer Peter Niehoff
12:55 - 13:15 The State of the Art in the Treatment of AdvancedBladder Cancer
Yohann Loriot
13:15 - 14:15 Lunch Break
14:15 - 15:00 Maximizing Treatment Benefits in advanced Renal Cell CarcinomaBiologix Symposium
Ali Shamseddine
15:00 - 15:45 Role of Pembrolizumab in Metastatic UrothelialCarcinoma
MSD Symposium
Ghazi Nsouli

HR+/
HER2
– met
asta
ticbr
east
canc
er is
a
DIAG
NOSI
SNo
w’s
the
mom
ent
to d
ecid
e…
W
hat c
omes
nex
t?
STRE
NGTH
COME
S FIR
ST
Afte
r diag
nosis
of H
R+/H
ER2–
m
etas
tatic
brea
st ca
ncer
PO
STME
NOPA
USAL
wom
en w
ith
an A
Ias
initi
al th
erap
y
KISQ
ALI®
Im
porta
nt n
ote:
Bef
ore
pres
crib
ing,
con
sult
full
pres
crib
ing
info
rmat
ion.
Pre
sent
atio
n:
Each
fil
m-c
oate
d ta
blet
con
tain
s 20
0 m
g of
rib
ocic
lib f
ree
base
. In
dica
tions
: K
ISQ
ALI®
is
indi
cate
d in
co
mbi
natio
n w
ith
an
arom
atas
e in
hibi
tor
as
initi
al
endo
crin
e-ba
sed
ther
apy
for
the
treat
men
t of
po
stm
enop
ausa
l wom
en w
ith h
orm
one
rece
ptor
(HR)
-pos
itive
, hum
an e
pide
rmal
gro
wth
fact
or re
cept
or 2
(H
ER2 )
-neg
ative
adv
ance
d or
met
asta
tic b
reas
t ca
ncer
. Do
sage
and
adm
inist
ratio
n: 2
.1 D
osin
g an
d Ad
min
istra
tion
The
reco
mm
ende
d do
se o
f KIS
QAL
I is
600
mg
(thre
e 20
0 m
g fil
m-c
oate
d ta
blet
s) ta
ken
oral
ly, o
nce
daily
for 2
1 co
nsec
utive
day
s fo
llow
ed b
y 7
days
off
treat
men
t res
ultin
g in
a c
ompl
ete
cycl
e of
28
days
. KIS
QAL
I can
be
take
n w
ith o
r with
out f
ood
. Coa
dmin
ister
KIS
QAL
I with
letro
zole
2.5
mg
take
n on
ce d
aily
thro
ugho
ut th
e -2
8day
cyc
le. R
efer
to th
e fu
ll pr
escr
ibin
g in
form
atio
n of
letro
zole
. For
do
sing
and
adm
inist
ratio
n w
ith o
ther
aro
mat
ase
inhi
bito
rs r
efer
to
the
appl
icab
le f
ull
pres
crib
ing
info
rmat
ion.
Pat
ient
s sh
ould
take
thei
r dos
e of
KIS
QAL
I and
letro
zole
at a
ppro
ximat
ely
the
sam
e tim
e ea
ch d
ay, p
refe
rabl
y in
the
mor
ning
. If
the
patie
nt v
omits
afte
r tak
ing
the
dose
, or m
isses
a d
ose,
no
addi
tiona
l dos
e sh
ould
be
take
n th
at d
ay. T
he n
ext p
resc
ribed
dos
e sh
ould
be
take
n at
the
usua
l tim
e.
KISQ
ALI t
able
ts s
houl
d be
sw
allo
wed
who
le (
tabl
ets
shou
ld n
ot b
e ch
ewed
, cr
ushe
d or
spl
it pr
ior
to
swal
low
ing)
. No
tab
let
shou
ld b
e in
gest
ed i
f it
is br
oken
, cr
acke
d, o
r ot
herw
ise n
ot i
ntac
t. D
ose
Mod
ifica
tion
for U
se w
ith S
trong
CYP
3A In
hibi
tors
Avo
id c
onco
mita
nt u
se o
f KIS
QAL
I with
stro
ng C
YP3A
in
hibi
tors
and
con
sider
an
alte
rnat
ive c
onco
mita
nt m
edic
atio
n w
ith le
ss p
oten
tial f
or C
YP3A
inhi
bitio
n. If
a
stro
ng C
YP3A
inhi
bito
r m
ust
be c
oadm
inist
ered
, re
duce
the
KIS
QAL
I dos
e to
400
mg
once
dai
ly. If
the
st
rong
inhi
bito
r is
disc
ontin
ued,
cha
nge
the
KISQ
ALI d
ose
(afte
r at
leas
t 5
half-
lives
of
the
stro
ng C
YP3A
in
hibi
tor)
to th
e do
se u
sed
prio
r to
the
initi
atio
n of
the
stro
ng C
YP3A
inhi
bito
r. Do
se M
odifi
catio
n fo
r He
patic
Im
pairm
ent N
o do
se a
djus
tmen
t is
nece
ssar
y in
pat
ient
s w
ith m
ild h
epat
ic im
pairm
ent (
Child
-Pug
h cl
ass
A).
The
reco
mm
ende
d st
artin
g do
se is
400
mg
KISQ
ALI o
nce
daily
for p
atie
nts
with
mod
erat
e (C
hild
-Pug
h cl
ass
B) a
nd s
ever
e he
patic
impa
irmen
t (Ch
ild-P
ugh
clas
s C)
. R
evie
w th
e Fu
ll Pr
escr
ibin
g In
form
atio
n fo
r th
e ar
omat
ase
inhi
bito
r fo
r do
se
mod
ifica
tions
rel
ated
to
hepa
tic im
pairm
ent.
Cont
rain
dica
tions
: •
None
W
arni
ngs
and
prec
autio
ns:
•Neu
trope
nia
was
m
ost f
requ
ently
rep
orte
d. A
com
plet
e bl
ood
coun
t (CB
C) s
houl
d be
per
form
ed b
efor
e in
itiat
ing
ther
apy.
CBC
sho
uld
be
mon
itore
d ev
ery
2 w
eeks
for
the
firs
t 2
cycl
es,
at t
he b
egin
ning
of
each
of
the
subs
eque
nt 4
cyc
les
then
as
clin
ical
ly in
dica
ted.
Feb
rile
neut
rope
nia
was
repo
rted
in %
1.5
of p
atie
nts
expo
sed
to K
isqal
i and
letro
zole
. Ba
sed
on th
e se
verit
y of
the
neut
rope
nia,
Kisq
ali m
ay re
quire
dos
e in
terru
ptio
n, re
duct
ion,
or d
iscon
tinua
tion.
•In
crea
ses
in A
LT a
nd A
ST h
ave
been
repo
rted,
with
the
maj
ority
of t
hem
with
out c
oncu
rrent
ele
vatio
ns o
f bilir
ubin
. Con
curre
nt e
leva
tions
of A
LT o
r AST
>
3 x
ULN
and
of to
tal b
ilirub
in >
2 x
ULN,
with
nor
mal
alk
alin
e ph
osph
atas
e le
vels
and
no c
hole
stas
is oc
curre
d in
%1.
2 of
pat
ient
s; a
ll pa
tient
s re
turn
ed to
nor
mal
with
in 1
54 d
ays
afte
r di
scon
tinua
tion
of K
isqal
i. Li
ver
func
tion
test
s (L
FTs)
sh
ould
be
perfo
rmed
bef
ore
initi
atin
g th
erap
y w
ith K
isqal
i. LF
Ts s
houl
d be
mon
itore
d ev
ery
2 w
eeks
for t
he fi
rst 2
cyc
les,
at
the
begi
nnin
g of
eac
h of
the
subs
eque
nt 4
cyc
les,
then
as
clin
ical
ly in
dica
ted.
Bas
ed o
n th
e se
verit
y of
tran
sam
inas
e el
evat
ions
, Kisq
ali m
ay re
quire
dos
e in
terru
ptio
n, re
duct
ion,
or d
iscon
tinua
tion.
•Q
T in
terv
al p
rolo
ngat
ion
has
been
repo
rted
with
Kisq
ali.
The
use
of K
isqal
i sho
uld
be a
void
ed in
pat
ient
s w
ho h
ave
alre
ady
or w
ho a
re a
t sig
nific
ant r
isk o
f dev
elop
ing
QTc
pr
olon
gatio
n. T
he E
CG s
houl
d be
ass
esse
d pr
ior
to in
itiat
ion
of tr
eatm
ent.
Trea
tmen
t with
Kisq
ali s
houl
d be
initi
ated
onl
y in
pat
ient
s w
ith
QTc
F va
lues
<45
0 m
sec.
The
ECG
sho
uld
be re
peat
ed a
t app
roxim
atel
y Da
y 14
of t
he fi
rst c
ycle
and
at t
he b
egin
ning
of t
he s
econ
d cy
cle,
then
as
clin
ical
ly in
dica
ted.
App
ropr
iate
mon
itorin
g of
ser
um e
lect
rolyt
es (
incl
udin
g po
tass
ium
, ca
lciu
m,
phos
phor
ous,
and
mag
nesiu
m)
shou
ld b
e pe
rform
ed p
rior t
o in
itiat
ion
of tr
eatm
ent,
at th
e be
ginn
ing
of th
e fir
st 6
cyc
les,
and
then
as
clin
ical
ly in
dica
ted.
Any
abn
orm
ality
sho
uld
be c
orre
cted
be
fore
the
sta
rt of
Kisq
ali t
hera
py.
Base
d on
the
obs
erve
d Q
T pr
olon
gatio
n du
ring
treat
men
t, Ki
sqal
i may
req
uire
dos
e in
terru
ptio
n, r
educ
tion,
or
disc
ontin
uatio
n. P
regn
ancy
, la
ctat
ion,
fem
ales
and
mal
es o
f rep
rodu
ctive
pot
entia
l: Pr
egna
ncy:
It is
pos
sible
that
Kisq
ali c
an c
ause
feta
l har
m w
hen
adm
inist
ered
to a
pre
gnan
t wom
an. T
he p
atie
nt s
houl
d be
adv
ised
of th
e ris
k to
a fe
tus
if Ki
sqal
i is
used
dur
ing
preg
nanc
y or
if th
e pa
tient
bec
omes
pr
egna
nt w
hile
taki
ng K
isqal
i. La
ctat
ion:
A d
ecisi
on s
houl
d be
mad
e w
heth
er to
disc
ontin
ue n
ursin
g or
to d
iscon
tinue
Kisq
ali,
taki
ng in
to a
ccou
nt th
e im
porta
nce
of K
isqal
i to
the
mot
her.
It is
reco
mm
ende
d th
at w
omen
taki
ng K
isqal
i sho
uld
not b
reas
tfeed
for a
t lea
st 2
1 da
ys a
fter t
he la
st d
ose.
Fem
ales
an
d m
ales
of r
epro
duct
ive p
oten
tial:
•Pre
gnan
cy te
stin
g: F
or fe
mal
es o
f rep
rodu
ctive
pot
entia
l the
pre
gnan
cy s
tatu
s sh
ould
be
verifi
ed p
rior t
o in
itiat
ing
treat
men
t with
Kisq
ali.
•Con
trace
ptio
n: S
exua
lly a
ctive
fem
ales
of r
epro
duct
ive p
oten
tial s
houl
d us
e ef
fect
ive c
ontra
cept
ion
(met
hods
that
resu
lt in
< 1
%
preg
nanc
y ra
tes)
whe
n us
ing
Kisq
ali d
urin
g tre
atm
ent a
nd fo
r 21
days
afte
r sto
ppin
g tre
atm
ent w
ith K
isqal
i. •
Infe
rtilit
y: B
ased
on
anim
al s
tudi
es, K
isqal
i m
ay im
pair
ferti
lity
in m
ales
of
repr
oduc
tive
pote
ntia
l. Ad
vers
e dr
ug r
eact
ions
: Ve
ry c
omm
on (
≥%10
): Ur
inar
y tra
ct in
fect
ion,
neu
trope
nia,
leuk
open
ia,
anae
mia
, lym
phop
enia
, de
crea
sed
appe
tite,
hea
dach
e, in
som
nia,
dys
pnoe
a, b
ack
pain
, na
usea
, di
arrh
oea,
vom
iting
, co
nstip
atio
n, s
tom
atiti
s, a
bdom
inal
pa
in,
alop
ecia
, ra
sh,
prur
itus,
fat
igue
, pe
riphe
ral o
edem
a, a
sthe
nia,
pyr
exia
, ab
norm
al li
ver
func
tion
test
s, le
ukoc
yte
coun
t de
crea
sed,
neu
troph
il co
unt
decr
ease
d,
haem
oglo
bin
decr
ease
d,
lymph
ocyt
e co
unt
decr
ease
d,
plat
elet
co
unt
decr
ease
d,
alan
ine
amin
otra
nsfe
rase
in
crea
sed,
as
parta
te
amin
otra
nsfe
rase
inc
reas
ed,
crea
tinin
e in
crea
sed,
pho
spho
rous
dec
reas
ed,
pota
ssiu
m d
ecre
ased
. .
Inte
ract
ions
: •C
onco
mita
nt u
se o
f st
rong
CYP
3A
inhi
bito
rs s
houl
d be
avo
ided
, in
clud
ing
but n
ot li
mite
d to
cla
rithr
omyc
in,
indi
navir
, itr
acon
azol
e, k
etoc
onaz
ole,
lopi
navir
, rit
onav
ir, n
efaz
odon
e, n
elfin
avir,
po
saco
nazo
le, r
itona
vir, s
aqui
navir
, and
vor
icon
azol
e. A
ltern
ative
med
icat
ions
with
less
pot
entia
l to
inhi
bit C
YP3A
sho
uld
be c
onsid
ered
. Pat
ient
s sh
ould
be
mon
itore
d fo
r ADR
s. If
con
com
itant
use
of a
stro
ng C
YP3A
inhi
bito
r can
not b
e av
oide
d, th
e Ki
sqal
i dos
e sh
ould
be
redu
ced
to 4
00 m
g. P
omeg
rana
tes
or p
omeg
rana
te ju
ice
and
gra
pefru
it or
gra
pefru
it ju
ice
shou
ld b
e av
oide
d. •
Conc
omita
nt u
se o
f stro
ng C
YP3A
indu
cers
sho
uld
be a
void
ed, i
nclu
ding
but
no
t lim
ited
to p
heny
toin
, rif
ampi
n, c
arba
maz
epin
e an
d St
Joh
n’s
Wor
t (Hy
peric
um p
erfo
ratu
m).
•Cau
tion
is ad
vised
whe
n Ki
sqal
i is
adm
inist
ered
with
CY
P3A
subs
trate
s w
ith n
arro
w t
hera
peut
ic i
ndex
(in
clud
ing
but
not
limite
d to
alfe
ntan
il, c
yclo
spor
ine,
dih
ydro
ergo
tam
ine,
erg
otam
ine,
eve
rolim
us,
fent
anyl,
pim
ozid
e, q
uini
dine
, siro
limus
, and
tacr
olim
us),
and
thei
r dos
e m
ay n
eed
to b
e re
duce
d. •
Co-a
dmin
istra
tion
of K
isqal
i with
med
icat
ions
with
kn
own
pote
ntia
l to
prol
ong
the
QT
inte
rval
sho
uld
be a
void
ed s
uch
as a
nti-a
rrhyt
hmic
med
icin
es (i
nclu
ding
but
not
lim
ited
to a
mio
daro
ne, d
isopy
ram
ide,
pr
ocai
nam
ide,
qui
nidi
ne, a
nd s
otal
ol),
othe
r med
icin
al p
rodu
cts
know
n to
pro
long
the
QT
inte
rval
incl
udin
g bu
t not
lim
ited
to c
hlor
oqui
ne, h
alof
antri
ne,
clar
ithro
myc
in,
halo
perid
ol,
met
hado
ne,
mox
iflox
acin
, be
prid
il, p
imoz
ide,
and
ond
anse
tron
(i.v)
. Pa
cks
and
pric
es:
Coun
try-s
peci
fic.
Lega
l cl
assifi
catio
n: C
ount
ry-s
peci
fic. L
eafle
t rev
ision
dat
e: M
arch
201
7
March/2019/Kis-Leb/1/Adpage
RA
PID
PO
WER
THA
T R
ED
EFI
NES
FI
RST
LIN
E I
N...
Nova
rtis
Phar
ma
Sevic
es In
c.Fa
ttal,
Daul
phin
Bld
gP.
O B
ox 1
1-34
48Si
n el
Fil,
Leb
anon
Tel +
961
1 4
8248
1Fa
x +
961
1 4
8558
5

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
HR+/
HER2
– met
asta
ticbr
east
canc
er is
a
DIAG
NOSI
SNo
w’s
the
mom
ent
to d
ecid
e…
W
hat c
omes
nex
t?
STRE
NGTH
COME
S FIR
ST
Afte
r diag
nosis
of H
R+/H
ER2–
m
etas
tatic
brea
st ca
ncer
PO
STME
NOPA
USAL
wom
en w
ith
an A
Ias
initi
al th
erap
y
KISQ
ALI®
Im
porta
nt n
ote:
Bef
ore
pres
crib
ing,
con
sult
full
pres
crib
ing
info
rmat
ion.
Pre
sent
atio
n:
Each
fil
m-c
oate
d ta
blet
con
tain
s 20
0 m
g of
rib
ocic
lib f
ree
base
. In
dica
tions
: K
ISQ
ALI®
is
indi
cate
d in
co
mbi
natio
n w
ith
an
arom
atas
e in
hibi
tor
as
initi
al
endo
crin
e-ba
sed
ther
apy
for
the
treat
men
t of
po
stm
enop
ausa
l wom
en w
ith h
orm
one
rece
ptor
(HR)
-pos
itive
, hum
an e
pide
rmal
gro
wth
fact
or re
cept
or 2
(H
ER2)
-neg
ative
adv
ance
d or
met
asta
tic b
reas
t ca
ncer
. Do
sage
and
adm
inist
ratio
n: 2
.1 D
osin
g an
d Ad
min
istra
tion
The
reco
mm
ende
d do
se o
f KIS
QAL
I is
600
mg
(thre
e 20
0 m
g fil
m-c
oate
d ta
blet
s) ta
ken
oral
ly, o
nce
daily
for 2
1 co
nsec
utive
day
s fo
llow
ed b
y 7
days
off
treat
men
t res
ultin
g in
a c
ompl
ete
cycl
e of
28
days
. KIS
QAL
I can
be
take
n w
ith o
r with
out f
ood
. Coa
dmin
ister
KIS
QAL
I with
letro
zole
2.5
mg
take
n on
ce d
aily
thro
ugho
ut th
e -2
8day
cyc
le. R
efer
to th
e fu
ll pr
escr
ibin
g in
form
atio
n of
letro
zole
. For
do
sing
and
adm
inist
ratio
n w
ith o
ther
aro
mat
ase
inhi
bito
rs r
efer
to
the
appl
icab
le f
ull
pres
crib
ing
info
rmat
ion.
Pat
ient
s sh
ould
take
thei
r dos
e of
KIS
QAL
I and
letro
zole
at a
ppro
ximat
ely
the
sam
e tim
e ea
ch d
ay, p
refe
rabl
y in
the
mor
ning
. If
the
patie
nt v
omits
afte
r tak
ing
the
dose
, or m
isses
a d
ose,
no
addi
tiona
l dos
e sh
ould
be
take
n th
at d
ay. T
he n
ext p
resc
ribed
dos
e sh
ould
be
take
n at
the
usua
l tim
e.
KISQ
ALI t
able
ts s
houl
d be
sw
allo
wed
who
le (
tabl
ets
shou
ld n
ot b
e ch
ewed
, cr
ushe
d or
spl
it pr
ior
to
swal
low
ing)
. No
tab
let
shou
ld b
e in
gest
ed i
f it
is br
oken
, cr
acke
d, o
r ot
herw
ise n
ot i
ntac
t. D
ose
Mod
ifica
tion
for U
se w
ith S
trong
CYP
3A In
hibi
tors
Avo
id c
onco
mita
nt u
se o
f KIS
QAL
I with
stro
ng C
YP3A
in
hibi
tors
and
con
sider
an
alte
rnat
ive c
onco
mita
nt m
edic
atio
n w
ith le
ss p
oten
tial f
or C
YP3A
inhi
bitio
n. If
a
stro
ng C
YP3A
inhi
bito
r m
ust
be c
oadm
inist
ered
, re
duce
the
KIS
QAL
I dos
e to
400
mg
once
dai
ly. If
the
st
rong
inhi
bito
r is
disc
ontin
ued,
cha
nge
the
KISQ
ALI d
ose
(afte
r at
leas
t 5
half-
lives
of
the
stro
ng C
YP3A
in
hibi
tor)
to th
e do
se u
sed
prio
r to
the
initi
atio
n of
the
stro
ng C
YP3A
inhi
bito
r. Do
se M
odifi
catio
n fo
r He
patic
Im
pairm
ent N
o do
se a
djus
tmen
t is
nece
ssar
y in
pat
ient
s w
ith m
ild h
epat
ic im
pairm
ent (
Child
-Pug
h cl
ass
A).
The
reco
mm
ende
d st
artin
g do
se is
400
mg
KISQ
ALI o
nce
daily
for p
atie
nts
with
mod
erat
e (C
hild
-Pug
h cl
ass
B) a
nd s
ever
e he
patic
impa
irmen
t (Ch
ild-P
ugh
clas
s C)
. R
evie
w th
e Fu
ll Pr
escr
ibin
g In
form
atio
n fo
r th
e ar
omat
ase
inhi
bito
r fo
r do
se
mod
ifica
tions
rel
ated
to
hepa
tic im
pairm
ent.
Cont
rain
dica
tions
: •
None
W
arni
ngs
and
prec
autio
ns:
•Neu
trope
nia
was
m
ost f
requ
ently
rep
orte
d. A
com
plet
e bl
ood
coun
t (CB
C) s
houl
d be
per
form
ed b
efor
e in
itiat
ing
ther
apy.
CBC
sho
uld
be
mon
itore
d ev
ery
2 w
eeks
for
the
firs
t 2
cycl
es,
at t
he b
egin
ning
of
each
of
the
subs
eque
nt 4
cyc
les
then
as
clin
ical
ly in
dica
ted.
Feb
rile
neut
rope
nia
was
repo
rted
in %
1.5
of p
atie
nts
expo
sed
to K
isqal
i and
letro
zole
. Ba
sed
on th
e se
verit
y of
the
neut
rope
nia,
Kisq
ali m
ay re
quire
dos
e in
terru
ptio
n, re
duct
ion,
or d
iscon
tinua
tion.
•In
crea
ses
in A
LT a
nd A
ST h
ave
been
repo
rted,
with
the
maj
ority
of t
hem
with
out c
oncu
rrent
ele
vatio
ns o
f bilir
ubin
. Con
curre
nt e
leva
tions
of A
LT o
r AST
>
3 x
ULN
and
of to
tal b
ilirub
in >
2 x
ULN,
with
nor
mal
alk
alin
e ph
osph
atas
e le
vels
and
no c
hole
stas
is oc
curre
d in
%1.
2 of
pat
ient
s; a
ll pa
tient
s re
turn
ed to
nor
mal
with
in 1
54 d
ays
afte
r di
scon
tinua
tion
of K
isqal
i. Li
ver
func
tion
test
s (L
FTs)
sh
ould
be
perfo
rmed
bef
ore
initi
atin
g th
erap
y w
ith K
isqal
i. LF
Ts s
houl
d be
mon
itore
d ev
ery
2 w
eeks
for t
he fi
rst 2
cyc
les,
at
the
begi
nnin
g of
eac
h of
the
subs
eque
nt 4
cyc
les,
then
as
clin
ical
ly in
dica
ted.
Bas
ed o
n th
e se
verit
y of
tran
sam
inas
e el
evat
ions
, Kisq
ali m
ay re
quire
dos
e in
terru
ptio
n, re
duct
ion,
or d
iscon
tinua
tion.
•Q
T in
terv
al p
rolo
ngat
ion
has
been
repo
rted
with
Kisq
ali.
The
use
of K
isqal
i sho
uld
be a
void
ed in
pat
ient
s w
ho h
ave
alre
ady
or w
ho a
re a
t sig
nific
ant r
isk o
f dev
elop
ing
QTc
pr
olon
gatio
n. T
he E
CG s
houl
d be
ass
esse
d pr
ior
to in
itiat
ion
of tr
eatm
ent.
Trea
tmen
t with
Kisq
ali s
houl
d be
initi
ated
onl
y in
pat
ient
s w
ith
QTc
F va
lues
<45
0 m
sec.
The
ECG
sho
uld
be re
peat
ed a
t app
roxim
atel
y Da
y 14
of t
he fi
rst c
ycle
and
at t
he b
egin
ning
of t
he s
econ
d cy
cle,
then
as
clin
ical
ly in
dica
ted.
App
ropr
iate
mon
itorin
g of
ser
um e
lect
rolyt
es (
incl
udin
g po
tass
ium
, ca
lciu
m,
phos
phor
ous,
and
mag
nesiu
m)
shou
ld b
e pe
rform
ed p
rior t
o in
itiat
ion
of tr
eatm
ent,
at th
e be
ginn
ing
of th
e fir
st 6
cyc
les,
and
then
as
clin
ical
ly in
dica
ted.
Any
abn
orm
ality
sho
uld
be c
orre
cted
be
fore
the
sta
rt of
Kisq
ali t
hera
py.
Base
d on
the
obs
erve
d Q
T pr
olon
gatio
n du
ring
treat
men
t, Ki
sqal
i may
req
uire
dos
e in
terru
ptio
n, r
educ
tion,
or
disc
ontin
uatio
n. P
regn
ancy
, la
ctat
ion,
fem
ales
and
mal
es o
f rep
rodu
ctive
pot
entia
l: Pr
egna
ncy:
It is
pos
sible
that
Kisq
ali c
an c
ause
feta
l har
m w
hen
adm
inist
ered
to a
pre
gnan
t wom
an. T
he p
atie
nt s
houl
d be
adv
ised
of th
e ris
k to
a fe
tus
if Ki
sqal
i is
used
dur
ing
preg
nanc
y or
if th
e pa
tient
bec
omes
pr
egna
nt w
hile
taki
ng K
isqal
i. La
ctat
ion:
A d
ecisi
on s
houl
d be
mad
e w
heth
er to
disc
ontin
ue n
ursin
g or
to d
iscon
tinue
Kisq
ali,
taki
ng in
to a
ccou
nt th
e im
porta
nce
of K
isqal
i to
the
mot
her.
It is
reco
mm
ende
d th
at w
omen
taki
ng K
isqal
i sho
uld
not b
reas
tfeed
for a
t lea
st 2
1 da
ys a
fter t
he la
st d
ose.
Fem
ales
an
d m
ales
of r
epro
duct
ive p
oten
tial:
•Pre
gnan
cy te
stin
g: F
or fe
mal
es o
f rep
rodu
ctive
pot
entia
l the
pre
gnan
cy s
tatu
s sh
ould
be
verifi
ed p
rior t
o in
itiat
ing
treat
men
t with
Kisq
ali.
•Con
trace
ptio
n: S
exua
lly a
ctive
fem
ales
of r
epro
duct
ive p
oten
tial s
houl
d us
e ef
fect
ive c
ontra
cept
ion
(met
hods
that
resu
lt in
< 1
%
preg
nanc
y ra
tes)
whe
n us
ing
Kisq
ali d
urin
g tre
atm
ent a
nd fo
r 21
days
afte
r sto
ppin
g tre
atm
ent w
ith K
isqal
i. •
Infe
rtilit
y: B
ased
on
anim
al s
tudi
es, K
isqal
i m
ay im
pair
ferti
lity
in m
ales
of
repr
oduc
tive
pote
ntia
l. Ad
vers
e dr
ug r
eact
ions
: Ve
ry c
omm
on (
≥%10
): Ur
inar
y tra
ct in
fect
ion,
neu
trope
nia,
leuk
open
ia,
anae
mia
, lym
phop
enia
, de
crea
sed
appe
tite,
hea
dach
e, in
som
nia,
dys
pnoe
a, b
ack
pain
, na
usea
, di
arrh
oea,
vom
iting
, co
nstip
atio
n, s
tom
atiti
s, a
bdom
inal
pa
in,
alop
ecia
, ra
sh,
prur
itus,
fat
igue
, pe
riphe
ral o
edem
a, a
sthe
nia,
pyr
exia
, ab
norm
al li
ver
func
tion
test
s, le
ukoc
yte
coun
t de
crea
sed,
neu
troph
il co
unt
decr
ease
d,
haem
oglo
bin
decr
ease
d,
lymph
ocyt
e co
unt
decr
ease
d,
plat
elet
co
unt
decr
ease
d,
alan
ine
amin
otra
nsfe
rase
in
crea
sed,
as
parta
te
amin
otra
nsfe
rase
inc
reas
ed,
crea
tinin
e in
crea
sed,
pho
spho
rous
dec
reas
ed,
pota
ssiu
m d
ecre
ased
. .
Inte
ract
ions
: •C
onco
mita
nt u
se o
f st
rong
CYP
3A
inhi
bito
rs s
houl
d be
avo
ided
, in
clud
ing
but n
ot li
mite
d to
cla
rithr
omyc
in,
indi
navir
, itr
acon
azol
e, k
etoc
onaz
ole,
lopi
navir
, rit
onav
ir, n
efaz
odon
e, n
elfin
avir,
po
saco
nazo
le, r
itona
vir, s
aqui
navir
, and
vor
icon
azol
e. A
ltern
ative
med
icat
ions
with
less
pot
entia
l to
inhi
bit C
YP3A
sho
uld
be c
onsid
ered
. Pat
ient
s sh
ould
be
mon
itore
d fo
r ADR
s. If
con
com
itant
use
of a
stro
ng C
YP3A
inhi
bito
r can
not b
e av
oide
d, th
e Ki
sqal
i dos
e sh
ould
be
redu
ced
to 4
00 m
g. P
omeg
rana
tes
or p
omeg
rana
te ju
ice
and
gra
pefru
it or
gra
pefru
it ju
ice
shou
ld b
e av
oide
d. •
Conc
omita
nt u
se o
f stro
ng C
YP3A
indu
cers
sho
uld
be a
void
ed, i
nclu
ding
but
no
t lim
ited
to p
heny
toin
, rif
ampi
n, c
arba
maz
epin
e an
d St
Joh
n’s
Wor
t (Hy
peric
um p
erfo
ratu
m).
•Cau
tion
is ad
vised
whe
n Ki
sqal
i is
adm
inist
ered
with
CY
P3A
subs
trate
s w
ith n
arro
w t
hera
peut
ic i
ndex
(in
clud
ing
but
not
limite
d to
alfe
ntan
il, c
yclo
spor
ine,
dih
ydro
ergo
tam
ine,
erg
otam
ine,
eve
rolim
us,
fent
anyl,
pim
ozid
e, q
uini
dine
, siro
limus
, and
tacr
olim
us),
and
thei
r dos
e m
ay n
eed
to b
e re
duce
d. •
Co-a
dmin
istra
tion
of K
isqal
i with
med
icat
ions
with
kn
own
pote
ntia
l to
prol
ong
the
QT
inte
rval
sho
uld
be a
void
ed s
uch
as a
nti-a
rrhyt
hmic
med
icin
es (i
nclu
ding
but
not
lim
ited
to a
mio
daro
ne, d
isopy
ram
ide,
pr
ocai
nam
ide,
qui
nidi
ne, a
nd s
otal
ol),
othe
r med
icin
al p
rodu
cts
know
n to
pro
long
the
QT
inte
rval
incl
udin
g bu
t not
lim
ited
to c
hlor
oqui
ne, h
alof
antri
ne,
clar
ithro
myc
in,
halo
perid
ol,
met
hado
ne,
mox
iflox
acin
, be
prid
il, p
imoz
ide,
and
ond
anse
tron
(i.v)
. Pa
cks
and
pric
es:
Coun
try-s
peci
fic.
Lega
l cl
assifi
catio
n: C
ount
ry-s
peci
fic. L
eafle
t rev
ision
dat
e: M
arch
201
7
March/2019/Kis-Leb/1/Adpage
RA
PID
PO
WER
THA
T R
ED
EFI
NES
FI
RST
LIN
E I
N...
Nova
rtis
Phar
ma
Sevic
es In
c.Fa
ttal,
Daul
phin
Bld
gP.
O B
ox 1
1-34
48Si
n el
Fil,
Leb
anon
Tel +
961
1 4
8248
1Fa
x +
961
1 4
8558
5
Saturday, April 13, 2019
PARALLEL SESSION | NURSE SESSION CARTHAGE HALL
08:30 - 10:35 Improving Quality CareModerator: Gladys Honein
08:30 - 08:35 Introduction to the Session
08:35 - 08:50 Establishment of A Nurse Navigator Programin Oncology Setting
Wafaa Skaf
08:50 - 09:05 Quality Care Monitoring for Oncology Patients Mariam El Sabae
09:05 - 09:25 Optimizing Drug Safety In Oncology Settings:Clinical Pharmacy Perspective
Aya Kabbani
09:25 - 09:40 Integrated Palliative Care Sarah Lattouf
09:40 - 10:00 Palliation beyond the Traditional:Reaching Out to Patients and Caregivers
Antoine Finianos
10:00 - 10:15 Psychological Support to Cancer Patients Dina Mouzayen
10:15 - 10:30 Benefits of Art Therapy in Managing Oncology Patients Linda Harris
10:30 - 10:35 Wrap-Up Session
10:35 - 11:00 Coffee Break
11:00 - 12:00 Pain ControlModerator: Mona El Ayoubi
11:20 - 11:40 The Cancer Pain Management in Daily Practice Ghassan Mohanna
11:00 - 11:20 Clinical Nurse Specialist Janane Hanna
11:40 - 12:00 Finding Peace Beyond the Pain:The Total Pain Concept
Rana Yamout

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
Notes
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
--------------------------------------------------------------------------------------

MULTIDISCIPLINARY APPROACH
Lebanese Society of Medical Oncology (LSMO)National Forum
April 11-13, 2019 | Phoenicia Hotel - Beirut, Lebanon
Notes
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------
--------------------------------------------------------------------------------------

Organized by: 4th Floor, Qubic CenterDaoud Ammoun StreetHorsh Tabet - Sin El FilP.O. Box: 90-361 BeirutTel: +961 1 510880/1/2/3 Mobile: +961 71 103123
[email protected] | www.infomedweb.com
LEBANON UAE
|DMCC Business CentreAlmas TowerJumeirah Lakes Dubai, United Arab EmiratesUnit No: 3820Mobile: +971 50 9110475
The Lebanese Society of Medical Oncology (LSMO)would like to thank the following companies
for their contribution to the success of its annual congress

Improving lives since 1896.
A tradition of advancing science and medicine. Then, now and in the future.

NOW APPROVED FOR THE FIRST LINE TREATMENT OF PATIENTS WITH aRCC *1,2
®
* intermediate- or poor-risk aRCC patients
HIGHLIGHTS OF PRESCRIBING INFORMATION1
These highlights do not include all the information needed to use OPDIVO® safely and e�ectively. See full prescribing information for OPDIVO®.OPDIVO® (Nivolumab) injection, for intravenous use. Initial U.S. Approval: 2014INDICATIONS AND USAGE OPDIVO® is a programmed death receptor-1 (PD-1) blocking antibody indicated for the treatment of: Patients with BRAF V600 wild-type unresectable or metastatic melanoma as a single agent; with BRAF V600 mutation-positive unresectable or metastatic melanoma as a single agent;a with unresectable or metastatic melanoma, in combination with ipilimumab;a with melanoma with lymph node involvement or metastatic disease who have undergone complete resection, in the adjuvant setting. Patients with metastatic non-small cell lung cancer and progression on or after platinum-based chemotherapy, with EGFR or ALK genomic tumor aberrations should have disease progression on FDA-approved therapy for these aberrations prior to receiving OPDIVO®. Patients with advanced renal cell carcinoma who have received prior anti-angiogenic therapy; with intermediate or poor risk, previously untreated advanced renal cell carcinoma, in combination with ipilimumab. Adult patients with classical Hodgkin lymphoma that has relapsed or progressed after: b autologous hematopoietic stem cell transplantation (HSCT) and brentuximab vedotin; or 3 or more lines of systemic therapy that includes autologous HSCT. Patients with recurrent or metastatic squamous cell carcinoma of the head and neck with disease progression on or after a platinum-based therapy. Patients with locally advanced or metastatic urothelial carcinoma who: b have disease progression during or following platinum-containing chemotherapy or have disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy. Adult and pediatric (12 years and older) patients with microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) metastatic colorectal cancer that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan.b Patients with hepatocellular carcinoma who have been previously treated with sorafenib.a DOSAGE AND ADMINISTRATION Administer as an intravenous infusion over 30 minutes. Unresectable or metastatic melanoma: OPDIVO® 240 mg every 2 weeks or 480 mg every 4 weeks. OPDIVO® with ipilimumab: OPDIVO® 1 mg/kg, followed by ipilimumab on the same day, every 3 weeks for 4 doses, then OPDIVO® 240 mg every 2 weeks or 480 mg every 4 weeks. Adjuvant treatment of melanoma: OPDIVO® 240 mg every 2 weeks or 480 mg every 4 weeks. Metastatic non-small cell lung cancer: OPDIVO® 240 mg every 2 weeks or 480 mg every 4 weeks. Advanced renal cell carcinoma: OPDIVO® 240 mg every 2 weeks or 480 mg every 4 weeks. OPDIVO® with ipilimumab: OPDIVO® 3 mg/kg followed by ipilimumab 1 mg/kg on the same day every 3 weeks for 4 doses, then OPDIVO® 240 mg every 2 weeks or 480 mg every 4 weeks. Classical Hodgkin lymphoma: OPDIVO® 3 mg/kg every 2 weeks or 480 mg every 4 weeks. Recurrent or metastatic squamous cell carcinoma of the head and neck: OPDIVO® 240mg every 2 weeks or 480 mg every 4 weeks. Locally advanced or metastatic urothelial carcinoma: OPDIVO® 240 mg every 2 weeks or 480 mg every 4 weeks. Microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) metastatic colorectal cancer: OPDIVO® 240 mg every 2 weeks. Hepatocellular carcinoma: OPDIVO® 240 mg every 2 weeks or 480 mg every 4 weeks. WARNINGS AND PRECAUTIONS Immune-mediated pneumonitis: Withhold for moderate and permanently discontinue for severe or life-threatening pneumonitis. Immune-mediated colitis: Withhold OPDIVO® when given as a single agent for moderate or severe and permanently discontinue for life-threatening colitis. Withhold OPDIVO® when given with ipilimumab for moderate and permanently discontinue for severe or life-threatening colitis. Immune-mediated hepatitis: Monitor for changes in liver function. Withhold for moderate and permanently discontinue for severe or life-threatening transaminase or total bilirubin elevation. Immune-mediated endocrinopathies: Withhold for moderate or severe and permanently discontinue for life-threatening hypophysitis. Withhold for moderate and permanently discontinue for severe or life-threatening adrenal insu�ciency. Monitor for changes in thyroid function. Initiate thyroid hormone replacement as needed. Monitor for hyperglycemia. Withhold for severe and permanently discontinue for life-threatening hyperglycemia. Immune-mediated nephritis and renal dysfunction: Monitor for changes in renal function. Withhold for moderate or severe and permanently discontinue for life-threatening serum creatinine elevation. Immune-mediated skin adverse reactions: Withhold for severe and permanently discontinue for life-threatening rash. Immune-mediated encephalitis: Monitor for changes in neurologic function. Withhold for new-onset moderate to severe neurological signs or symptoms and permanently discontinue for immune-mediated encephalitis. Infusion reactions: Discontinue OPDIVO® for severe and life-threatening infusion reactions. Interrupt or slow the rate of infusion in patients with mild or moderate infusion reactions. Complications of allogeneic HSCT after OPDIVO®: Monitor for hyperacute graft-versus-host-disease (GVHD), grade 3-4 acute GVHD, steroid-requiring febrile syndrome, hepatic veno-occlusive disease, and other immune-mediated adverse reactions. Transplant-related mortality has occurred. Embryo-fetal toxicity: Can cause fetal harm. Advise of potential risk to a fetus and use of e�ective contraception. ADVERSE REACTIONS Most common adverse reactions (≥20%) in patients were: OPDIVO® as a single agent: fatigue, rash, musculoskeletal pain, pruritus, diarrhea, nausea, asthenia, cough, dyspnea, constipation, decreased appetite, back pain, arthralgia, upper respiratory tract infection, pyrexia, headache, and abdominal pain. OPDIVO® with ipilimumab for melanoma: fatigue, rash, diarrhea, nausea, pyrexia, vomiting, and dyspnea. OPDIVO® with ipilimumab for renal cell carcinoma: fatigue, rash, diarrhea, musculoskeletal pain, pruritus, nausea, cough, pyrexia, arthralgia, and decreased appetite. USE IN SPECIFIC POPULATIONS Lactation: Discontinue breastfeeding.For any additional information or adverse events reporting, please contact Bristol-Myers Squibb Medical Information on http://www.globalbmsmedinfo.coma This indication is approved under accelerated approval based on progression-free survival. Continued approval for this indication may be contingent upon verification and description of clinical benefit in the confirmatory trials. b This indication is approved under accelerated approval based on overall response rate and duration of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.aRCC=advanced renal cell carcinoma
OPDIVO® is indicated for the treatment of patients with intermediate or poor risk, previously untreated advanced renal cell carcinoma, in combination with Ipilimumab1
Bristol-Myers SquibbLaboratory Complex
Dubai Science ParkP.O. Box: 454409, Dubai, UAE
Tel: +971-4-45021001506AE18PR04170-01
References:1. OPDIVO® (Nivolumab) US PI, April 2018 . 2. Motzer RJ, Tannir NM, McDermott DF, et al; Checkmate 214 Investigators. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018;37B(14): 1277-1290.