Embed Size (px)
Citation preview

REVIEW ARTICLEPEDIATRICS Volume 137 , number 6 , June 2016 :e 20153994
Learning Problems in Children of Refugee Background: A Systematic ReviewHamish R. Graham, MBBS, MPH, FRACP, a, b Ripudaman S. Minhas, MD, MPH, FRCPC, c, d Georgia Paxton, MBBS, BMedSci, MPH, FRACPa, e
abstractCONTEXT: Learning problems are common, affecting up to 1 in 10 children. Refugee children
may have cumulative risk for educational disadvantage, but there is limited information on
learning in this population.
OBJECTIVE: To review the evidence on educational outcomes and learning problems in refugee
children and to describe their major risk and resource factors.
DATA SOURCES: Medline, Embase, PubMed, Cumulative Index to Nursing and Allied Health
Literature, PsycINFO, and Education Resources Information Center.
STUDY SELECTION: English-language articles addressing the prevalence and determinants of
learning problems in refugee children.
DATA EXTRACTION: Data were extracted and analyzed according to Arksey and O’Malley’s
descriptive analytical method for scoping studies.
RESULTS: Thirty-four studies were included. Refugee youth had similar secondary school
outcomes to their native-born peers; there were no data on preschool or primary school
outcomes. There were limited prevalence data on learning problems, with single studies
informing most estimates and no studies examining specific language disorders or
autism spectrum disorders. Major risk factors for learning problems included parental
misunderstandings about educational styles and expectations, teacher stereotyping and low
expectations, bullying and racial discrimination, premigration and postmigration trauma,
and forced detention. Major resource factors for success included high academic and life
ambition, “gift-and-sacrifice” motivational narratives, parental involvement in education,
family cohesion and supportive home environment, accurate educational assessment and
grade placement, teacher understanding of linguistic and cultural heritage, culturally
appropriate school transition, supportive peer relationships, and successful acculturation.
LIMITATIONS: Studies are not generalizable to other cohorts.
CONCLUSIONS: This review provides a summary of published prevalence estimates for learning
problems in resettled refugee children, highlights key risk and resource factors, and
identifies gaps in research.
aDepartment of General Medicine, Royal Children’s Hospital, Melbourne, Australia; bCentre for International Child Health, University of Melbourne, Melbourne, Australia; cDepartment
of Pediatrics, St. Michael’s Hospital, Toronto, Canada; dDivision of Developmental Pediatrics, Department of Pediatrics, University of Toronto, Toronto, Canada; and eMurdoch Childrens
Research Institute, Parkville, Victoria, Australia
To cite: Graham HR, Minhas RS, Paxton G. Learning Problems in Children of Refugee Background: A Systematic Review. Pediatrics. 2016;137(6):e20153994
by guest on April 18, 2020www.aappublications.org/newsDownloaded from

GRAHAM et al
BACKGROUND
Conceptual Framework and Terminology
Learning problems are common,
affecting up to 1 in 10 children.1
They may reflect impairments in
intellect, difficulties in a specific
learning domain, behavioral
problems, or difficulties in social
interaction; comorbidities are
common.1 Bioecological system
theory recognizes that a child’s
development occurs in the context of
interactions between different layers
of their “ecology” (eg, individual
attributes, caregivers, family, school,
community, society).2 Integrating
this bioecological perspective
with neurocognitive research
provides an understanding that
learning problems arise from the
interaction of neurodevelopmental
predispositions with environmental
factors and life experience in a
dynamic process.3 This perspective
acknowledges both risk factors
for failure and resource factors
that contribute to developmental
resilience, 1, 3 and it recognizes that
the expression (and experience) of
learning problems will vary across
the life span and between individuals,
communities, and societies.1, 3
For clarity of reporting, we use
contemporary clinical categories
from developmental pediatrics to
describe the prevalence of learning
problems and broad categories to
describe their determinants (negative
risk factors and positive resource
factors). We use the term refugee-
background to describe children
granted humanitarian protection or
seeking asylum and children from
refugee-like backgrounds who have
migrated through other channels
(eg, family reunion).
Refugee Children and Learning
In 2015, the United Nations High
Commissioner for Refugees (UNHCR)
reported the highest numbers of
forcibly displaced people ever
recorded.4 Globally, there are
currently almost 60 million displaced
people, including 13.9 million people
newly displaced in the past year,
19.5 million refugees, and 1.8 million
people who have lodged claims for
asylum.4 More than half of refugees
are children, and the number
of unaccompanied or separated
children seeking asylum is the
highest since records began
(34 300 in 2014).4
Learning and development are
particular concerns for children of
refugee background.5 Displacement
has long-lasting effects on children
and caregivers, often involving
exposure to trauma and disruption
of family structures.6 Relocation
brings additional stressors, as
families negotiate their needs
within foreign social structures and
with limited supports.6 Within this
complex dynamic, a child enters a
new educational environment and
must negotiate multiple transitions,
including transitions in family,
friendships, schooling, community,
language, culture, and identity.6
Although educational success is
critical to overall well-being in
refugee children, 6 there are limited
data on educational outcomes or
learning problems in this group.
Understanding learning problems
and educational needs is essential
to respond to the increasing
populations of forcibly displaced
children and families.
The aim of this study was to review
evidence on educational outcomes
and learning problems among
refugee children, to describe major
risk and resource factors, and
to highlight areas for additional
investigation.
METHODS
We completed a systematic review
by using the search, selection,
extraction, analysis, and reporting
methods described by Arksey and
O’Malley’s framework for scoping
studies.7, 8
Inclusion and Exclusion Criteria
Inclusion and exclusion criteria
were broad, in keeping with the
study question and scoping review
methods. We included studies
if they involved interventional,
observational, or qualitative studies
relating to the prevalence or
determinants of learning problems
in children of refugee background,
available in English. We defined
“determinants” as any demographic,
individual, family, school, or other
factors reported to be associated with
learning problems or educational
outcomes. We excluded single case
reports and non–peer-reviewed
papers.
Data Sources
We completed searches of Medline,
Embase, PubMed, CINAHL, PsycINFO,
and Education Resources Information
Center (ERIC) in January 2015 (see
Supplemental Information), with the
support of a research librarian for
the time period 1996 through 2015
(Table 1). In addition, we searched
key websites, reviewed reference
lists, and contacted people through
refugee health networks in Canada
and Australia.
2
TABLE 1 Medline Search Query
The following search query was used on January 20, 2015 to search Medline; similar search terms used
for the other databases (Embase, PubMed, CINAHL, PsycINFO, ERIC):
1. (exp Refugees/ or “Emigrants and Immigrants”/) and (Learning/ or Learning problem$.af. or exp
Learning Disorders/ or (cognition disorders/ or mild cognitive impairment/) or (exp “attention defi cit
and disruptive behavior disorders”/ or child behavior disorders/ or exp communication disorders/ or
developmental disabilities/ or exp learning disorders/ or intellectual disability/) or Stress Disorders,
Post-Traumatic/)
2. limit 1 to (english language and “all child (0 to 18 years)”), 1996–present.
by guest on April 18, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 137 , number 6 , June 2016
Data Extraction and Synthesis
We systematically extracted data
using a standardized data charting
form, which included information
on study type, location, population,
research methods, outcome
measures, and key findings.
We adopted Arksey and O’Malley’s
descriptive analytical method
for data analysis and reporting, 7 including numerical summary of
included studies to describe the
current state of the literature and
narrative synthesis of findings
using broad categories to describe
educational outcomes, learning
problems, and important risk and
resource factors.
RESULTS
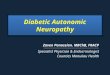
Database searches retrieved 2454
results: Medline 365, Embase
511, CINAHL 278, PsycINFO 543,
ERIC 601, and PubMed 156. After
exclusion of duplicates and addition
of 49 records from other sources,
2021 articles were identified for
screening. Two investigators (H.R.G.,
R.S.M.) independently screened all
titles and abstracts according to
predefined inclusion criteria, then
reviewed 98 full-text papers for
inclusion. Thirty-four articles were
included in the final analysis (Fig 1,
Table 2).
Summary of Included Studies
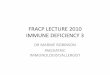
Overall, 34 studies reported on
learning problems in 29 cohorts of
refugee children; half (17/34) were
published since 2010 (Table 3, Fig 2).
The majority (25/34, 74%) reported
results from cohorts in Australia
(11 studies), the United States (7
studies), or Canada (7 studies), with
only 1 study from a low- or middle-
income country (Thailand). Studies
included participants from diverse
regions of origin, and 14 (41%)
included mixed cohorts of children
from multiple regions. Most studies
(30/34, 88%) reported on adolescent
refugees, with 13 studies including
primary school–age children and a
single study on preschool children.
Twenty (59%) studies used
quantitative (or mixed) methods and
reported on educational outcomes
(n = 8), prevalence of learning
problems (n = 14), and risk and
resource factors (n = 9); the
remaining 14 (41%) studies used
qualitative methods and reported on
risk and resource factors.
Educational Outcomes
Eight studies reported educational
out comes for refugee children,
all at secondary school
level10, 18, 23, 28, 30, 33, 35, 40 (Table 4).
Six studies from North America
and Europe reporting on 1197
refugee-background youth from Sub-
Saharan and North Africa, Eastern
Europe, Middle East, Asia, and Latin
America found they had similar
educational outcomes to their peers,
including similar rates of high school
completion (although often at an
older age).10, 18, 30, 33, 35, 40 One study
of 19 unaccompanied minors who
migrated to the United States from
Sudan reported superior performance
to peers, with 100% high school
completion and 79% progression
to college.28 Conversely, a study
involving 102 youth who migrated
from North Korea to South Korea
reported lower academic performance
relative to native-born peers.23
Prevalence of Learning Problems
Fourteen studies provided prevalence
data on developmental or learning
problems in children of refugee back-
ground10, 14, 16, 17, 20, 23–25, 29–31, 34, 39, 41
(Table 5). No studies reported on
autism spectrum disorder, specific
language impairment, dyscalculia, or
dyslexia.
3
FIGURE 1PRISMA 2009 fl ow diagram of literature.
by guest on April 18, 2020www.aappublications.org/newsDownloaded from

GRAHAM et al 4
TABLE 2 Summary of 34 Included Studies on Educational Outcomes and Learning Problems in Refugee Children (1996–2015)
Author Place of Origin Population Method Outcomes
Agbenyega& Klibthong (2013), 9 Australia
Sub-Saharan Africa
(countries not specifi ed)
25 refugee-background
families with a child
attending preschool
Qualitative. Semistructured
interviews with parents
and teachers.
Preschool experiences of
parents and educators.
Berthold (2000), 10 USA Cambodia 144 refugee-background
Khmer secondary school
students, born outside US
(age 14–20 y, mean 16.35 y,
50% male)
Mixed methods. In-depth
interviews, questionnaires
with adolescents and
parents.
Educational outcomes (grade
point average), exposure to
violence, PTSD, depression,
school behavior problems,
perceived social support.
Bitew et al (2008), 11 Australia Ethiopia 16 refugee-background
secondary school students
(age 16–20 y)
Qualitative. Semistructured
interviews with students.
Student experience of school,
cultural differences, needs,
interests.
Bitew et al (2010), 12 Australia Ethiopia 16 refugee-background
secondary school students
(age 16–20 y), 10 teachers,
10 parents
Qualitative. Semistructured
interviews with students,
parents, and teachers.
Parental contact with school,
academic assistance
to child, education
and awareness of
Australian school system,
cultural differences and
expectations.
Brown et al (2006), 13 Australia Sudan 8 refugee-background youth
(age 15–20 y)
Qualitative. Individual
interviews and focus
groups with students.
Subjective school experiences,
and challenges.
Correa-Velez et al (2010), 6
Australia
Sudan, Ethiopia, Liberia,
Uganda, Iraq, Afghanistan,
Iran, Kuwait, Bosnia,
Croatia, Burma
97 refugee-background
students attending English
language school (age
11–19 y) (68% Africa, 27%
Middle East)
Qualitative. Interviews and
questionnaires with
students.
Subjective health and
wellbeing, and wide range of
determinants.
Daud & Rydelius (2009), 14
Sweden
Iraq, Egypt, Morocco, Syria 80 refugee-background
children (age 7–16 y, 50%
male)
Cross-sectional. Standardized
tests (eg, WISC-III, SDQ),
interviews with students
and parents.
ADHD, PTSD, IQ, ODD, CD.
Daud et al (2008), 15 Sweden Iraq, Egypt, Morocco, Syria 80 refugee-background
children (age 7–16 y, 50%
male)
Cross-sectional. Standardized
tests and questionnaires
(eg, WISC-III, SDQ),
interviews with children.
Trauma, PTSD, IQ, self-esteem.
Derluyn & Broekaert (2007), 16 Belgium
41 countries (13% Angola, 7%
DRC, 7% Afghanistan, 7%
Nigeria)
166 recently arrived
“unaccompanied refugee
minors” (age 12–19 y, 63%
male)
Cross-sectional. Standardized
tests and questionnaires
(eg, CBCL, SDQ), children
and social workers.
Behavioral profi les.
Fazel & Stein (2003), 17 UK Balkans, Kashmir, Afghanistan 101 refugee-background
children (age 5–18 y) (plus
202 age- and gender-
matched “minority” and
“white” peers)
Cross-sectional. Standardized
questionnaire (SDQ)
completed by teachers.
Behavioral profi les.
Fox et al (2004), 18 USA Vietnam, Cambodia, Laos 237 refugee-background
students (age 6–17 y, mean
11 y, 47% male)
Cross-sectional. Standardized
tests and questionnaires
(eg, Self-Perception Profi le
for Children) with students.
Educational outcomes (GPA),
self-esteem, depression.
Hatoss et al (2012), 19
Australia
Sudan 30 refugee-background youth
from 6 schools (plus 227
peers)
Qualitative. Focus groups
plus online survey with
students.
Subjective school experiences,
aspirations, and challenges.
Kira et al (2012), 20 USA Iraq, African American 390 children and adolescents
recruited from the
community (age 11–17 y,
mean 13.6 y, 46% male,
52% Iraqi refugee)
Cross-sectional. Standardized
tests and questionnaires
(eg, Cumulative Trauma
Scale, WISC-IV) with
adolescents.
Trauma, PTSD, IQ.
Kira et al (2012), 21 USA Iraq, African American 390 children and adolescents
recruited from the
community (age 11–17 y,
mean 13.6 y, 46% male,
52% Iraqi refugee)
Cross-sectional. Standardized
tests and questionnaires
(eg, Cumulative Trauma
Scale, WISC-IV) with
adolescents.
Trauma, PTSD, IQ.
by guest on April 18, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 137 , number 6 , June 2016 5
Author Place of Origin Population Method Outcomes
Kira et al (2014), 22 USA Iraq, African American 390 children and adolescents
recruited from the
community (age 11–17 y,
mean 13.6 y, 46% male,
52% Iraqi refugee)
Cross-sectional. Standardized
tests and questionnaires
(eg, Cumulative Trauma
Scale, WISC-IV) with
adolescents.
Trauma, PTSD, IQ, race
stressors, bullying
victimization.
Lee et al (2012), 23 South Korea North Korea 102 refugee-background
secondary school students
(age 13–22 y, mean 17 y,
67% male)
Cross-sectional. Standardized
tests and questionnaires
(eg, CBCL) with students.
Educational outcomes,
behavioral profi les.
Mace et al (2014), 24 Australia 24 countries (21% Burma,
11% Afghanistan, 11% Iran)
332 children seen at a
refugee health clinic (mean
age 9.5 y)
Cross-sectional. Retrospective
clinic chart review.
Medical, psychological,
developmental, and learning
issues.
Mollica et al (1997), 25
Thailand
Cambodia 182 refugee-background
adolescents (age 12–13 y),
and their parents
Cross-sectional. Standardized
tests, questionnaires, and
interviews (eg, CBCL) with
adolescents and parents.
Trauma, behavioral profi les.
Naidoo (2009), 26 Australia Africa (countries not
specifi ed)
77 preservice teachers and 9
supervisors working with
the Refugee Action Support
Program
Qualitative. Semistructured
group interviews with
teachers and supervisors.
Teacher experiences and
perceptions of students,
student academic progress
and results.
Nykiel-Herbert (2010), 27 USA Iraq 12 Kurdish refugee-
background primary
school students (age
8–11 y)
Mixed-methods program
evaluation. Class
observation, unstructured
narrative recording,
refl ective practice
techniques, review of
academic records reported
by teachers, caregivers,
and students.
Educational outcomes (literacy,
math), student experience,
teacher experience and
perspectives.
Rana et al (2011), 28 USA Sudan 19 youth who had migrated as
“unaccompanied refugee
minors” (89% male, mean
age 15 y at resettlement
and 22 y at interview), 20
(foster) parents
Qualitative. Semistructured
interviews of youth and
parents.
Educational outcomes (school
completion), determinants
of educational resilience.
Rousseau, Drapeau, & Platt
(2000), 29 Canada
Cambodia, Honduras,
Guatemala, El Salvador
158 secondary school
students (76 Cambodian,
82 Central American)
(mean age 14 y) (plus 67
Quebecois youth)
Cross-sectional. Standardized
tests and questionnaires
(eg, CBCL), interviews with
parents and students.
Behavioral profi les, risk
behaviors.
Rousseau & Drapeau (2000), 30 Canada
Cambodia, Honduras,
Guatemala, El Salvador
158 secondary school
students (76 Cambodian,
82 Central American)
(mean age 14 y)
Cross-sectional. Standardized
tests and questionnaires
(eg, CBCL), interviews with
parents and students,
and review of academic
records.
Educational outcomes
(French, English, math),
trauma, behavioral profi les,
acculturation, parental
depression, and English
profi ciency.
Rousseau et al (1996), 31
Canada
Cambodia, Vietnam,
Honduras, Guatemala, El
Salvador
156 refugee-background
primary school students
(100 from Southeast Asia,
56 Central America (mean
age 10.5 y, 56% male)
Cross-sectional. Standardized
tests and questionnaires
(eg, CBCL), interviews with
teachers and parents,
review of academic
records.
Behavioral profi les, parental
and teacher perceptions.
Shakya et al (2010), 32 Canada Afghanistan, Burma, Sudan 57 refugee-background
youth recruited from the
community (age 16–24 y,
51% male, mean time since
migration 1.9 y)
Qualitative. Focus groups and
interviews with youth.
Educational aspirations,
challenges, barriers, youth
strategies, vulnerability,
empowerment.
TABLE 2 Continued
by guest on April 18, 2020www.aappublications.org/newsDownloaded from

GRAHAM et al
A single Australian study reported
on the prevalence of sensory
impairment (vision, hearing) and
developmental delay in a mixed
cohort of 332 children attending
a refugee health clinic: 7.5% had
a visual impairment, 3.3% had a
hearing impairment, and 6.9%
had developmental delay, most
commonly language (5.7%) or gross
motor (2.1%).24
Two studies from the United States20
and Sweden14 provided information
on intellectual impairment, using
cognitive testing to investigate the
impact of trauma on intelligence.
These studies reported that among
more than 400 Iraqi-background
and African American adolescents,
half (49.4%–56.3%) had low or
borderline IQ scores on the Wechsler
Intelligence Scales for Children
(WISC). Mean IQ for the US cohort
was 84 points (WISC, Fourth Edition
[WISC-IV]), 20 consistent with
WISC-IV results for African American
and other minority populations in the
United States.20
Ten studies reported on behavioral
profiles of refugee children, with
varying results.16, 17, 23, 25, 29–31, 34, 39, 41
A Canadian study of 156 primary
school–age children from Southeast
Asia and Central America reported
an association between problems
identified through behavioral
profiles (especially “externalizing
problems”) and adverse educational
outcomes;31 however, this
association was not found in a
similar adolescent cohort (n =
158).30 Overall, behavioral and
emotional problems were more
common in refugee-background
children compared with their
6
Author Place of Origin Population Method Outcomes
Slodnjak, Kos, & Yule (2002), 33 Slovenia
Bosnia-Herzegovina 430 refugee-background
youth (age 14–15 y) (plus
195 age- and gender-
matched peers)
Cross-sectional. Standardized
questionnaires and
interviews with students
and parents or guardians
(eg, War Trauma
Questionnaire).
Teacher-reported school
outcomes and behavior.
PTSD.
Sourander (1998), 34 Finland Somalia, Ethiopia, Thailand,
Vietnam, Angola, Nigeria,
Burma, Iraq, Zaire
46 unaccompanied minors
(age 6–17 y, mean 14.1 y)
(80% from Somalia)
Cross-sectional. Standardized
questionnaire (CBCL) of
children completed by
support worker.
Behavioral profi les.
Stermac (2012), 35 Canada Multiple (countries not
specifi ed)
219 immigrant youth from
“war-zone” countries (eg,
former Yugoslavia, Middle
East, eastern Africa),
217 from non–war-zone
countries, 222 Canadian-
born (age 18–20 y,
migrated >8 y before)
Cross-sectional. Telephone
survey with youth.
Educational outcomes (math,
language, overall grade),
self-assessed language
ability, work habits,
perceived supports.
Tlhabano & Schweitzer
(2007), 36 Australia
Sudan, Somalia 14 refugee-background youth
(age 16–26 y)
Qualitative. Structured
individual interviews with
youth.
Subjective school experiences,
challenges, and aspirations.
Uptin et al (2013), 37 Australia Burma, Burundi, Sudan, DRC,
Sierra Leone, Togo
12 refugee-background
youth (age 16–19 y), and 1
Sudanese youth worker
Qualitative. Semistructured
interviews and focus
groups with youth and a
youth worker.
School perceptions and
experience.
Usman (2012), 38 Canada Sierra Leone, Liberia 10 refugee-background
primary school students
(Grades 3 and 4)
Qualitative. Interviews with
children, parents, and
teachers. Observation in
classroom and home.
Students’ linguistic heritage,
perspective of teachers on
communication disorders,
teacher approaches to
communication disorders.
Wiegersma et al (2011), 39
Netherlands
Multiple (countries not
specifi ed)
267 children living in asylum
seekers’ centers (age
4–16 y)
Cross-sectional. Standardized
tests and interviews with
parents and children (eg,
SDQ).
Behavioral profi les.
Wilkinson (2002), 40 Canada Yugoslavia, El Salvador,
Afghanistan, Azerbaijan,
Iraq, Vietnam, Somalia,
Guatemala, Pakistan
91 refugee-background youth
(age 15–21 y) recruited
from immigration registry,
and 123 of their parents
Qualitative. Structured
interviews with youth and
parents.
Educational outcomes (based
on grade placement,
secondary school and
postgraduate enrollment
and completion).
Ziaian et al (2013), 41 Australia Afghanistan, Iran, Iraq, Sudan,
Liberia, Bosnia, Serbia
530 refugee-background
children and youth (age
4–17 y)
Cross-sectional. Standardized
tests and interviews with
youth (eg, SDQ).
Behavioral profi les, mental
health service utilization.
CBCL, Child Behavior Checklist; DRC, Democratic Republic of the Congo; GPA, grade point average; SDQ, Strengths and Diffi culties Questionnaire.
TABLE 2 Continued
by guest on April 18, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 137 , number 6 , June 2016
peers, especially in young children
(<10 years old).16, 17, 23, 25, 34, 39,
“Internalizing problems” (ie, anxious,
depressive, and overcontrolled
behavior) were more common
than “externalizing problems”
(ie, aggressive, hyperactive,
noncompliant, and undercontrolled
behavior).16, 17, 23, 25, 34, 39, However,
there is considerable variation in
prevalence estimates, with some
studies reporting no difference to
peers29, 30, 41 and multiple studies
finding marked variation between
self-report, teacher report, and
parent report.16, 25, 29, 39, 41
One study examined the prevalence
of attention-deficit/hyperactivity
disorder (ADHD), involving 80
Middle Eastern refugee children
and adolescents in Sweden.14 There
was high prevalence of ADHD
in students whose parents had
experienced trauma (65% male,
30% female) but low prevalence
in those whose parents had not
(5% male, 10% female).14 Most
(90%) children with ADHD also met
criteria for posttraumatic stress
disorder (PTSD); and lower IQ was
a risk factor for both ADHD and
PTSD.14
Two studies reported on the
prevalence of oppositional defiant
disorder/conduct disorder (ODD/
CD).10, 14 In the Swedish cohort
of adolescent Iraqi refugees, the
prevalence of ODD/CD was 7.5%
in those whose parents had been
exposed to trauma and 0% in
those whose parents did not have
trauma exposure.14 A US study of
144 Khmer adolescents found 30%
had been reported at school for
misconduct (eg, carrying a weapon,
physical assault, swearing, stealing)
and that misconduct was associated
with higher exposure to trauma,
male gender, and lower academic
outcomes.10 The Khmer cohort had
high levels of premigration trauma
(99%), clinical depression (63%),
and PTSD (33%).10
7
Risk and Resource Factors
Twenty-five of the 34 studies (73.5%)
provided qualitative information on
determinants of learning in refugee
children. We describe major risk
and resource factors by using broad
categories: individual child and home
environment, school environment,
migration and trauma experience, and
sociocultural environment (Table 6).
TABLE 3 Characteristics of 34 Included Studies on the Prevalence and Determinants of Learning
Problems in Children of Refugee Background
Characteristic Number (%)
Country of settlement
United States 7 (20.6)
Canada 7 (20.6)
Australia 11 (32.4)
South Korea 1 (2.9)
Thailand 1 (2.9)
Sweden 2 (5.9)
Finland 1 (2.9)
Belgium 1 (2.9)
Netherlands 1 (2.9)
Slovenia 1 (2.9)
United Kingdom 1 (2.9)
Study population region of origin
Sub-Saharan Africa 9 (26.5)
Middle East and North Africa 6 (17.6)
East Asia and Pacifi c 4 (11.8)
Europe and Central Asia 1 (2.9)
Multiple regions 14 (41.2)
Study population age
Preschool age 1 (2.9)
Primary school age 3 (8.8)
Adolescent 20 (58.8)
Primary school age and adolescent 10 (29.4)
Study outcomes reported
Educational outcomes and prevalence of learning problems 19 (55.9)
Prevention of learning problems 14
Educational outcomes 8
Risk and resource factors (solely) 15 (44.1)
Method
Quantitative cross-sectional 20 (58.8)
Qualitative 14 (41.2)
FIGURE 2Included studies by year of publication.
by guest on April 18, 2020www.aappublications.org/newsDownloaded from

GRAHAM et al
Individual Child and Home Environment
Two of the 7 studies reporting
secondary school outcomes in refugee
youth found girls achieved higher
results than boys.10, 35 However,
female academic advantage among
refugee youth was less pronounced
than among their nonrefugee peers
and was limited to language subjects
only.10, 35 A Canadian study of 91
refugee youth from 9 countries found
that younger age at migration, greater
length of time since resettlement, and
urban residence were associated with
better secondary school outcomes.40
This study found no association
between self-reported English
language proficiency and secondary
school outcomes, 40 despite Sudanese
youth reporting English language
difficulties as a common barrier to
success.13, 19, 36
Three studies reported ethnic
differences in educational
outcomes.30, 31, 40 A Canadian study
of 156 refugee children in primary
school found that children from
Central America had more severe
learning difficulties reported by
teachers than their peers from
Cambodia and Vietnam, despite
similar objective academic
outcomes.31 Qualitative data from
this study suggested teachers were
influenced by cultural stereotypes,
leading them to identify Latino
children more readily as having
problems.31 Two studies in
Canadian secondary schools
reported lower school failure rates
for Cambodian-background youth
(compared with Central American
youth) (n = 158)30 and superior
outcomes for Yugoslav compared
with other refugee-background youth
(n = 91).40
Six studies reported that Sudanese-
background refugee youth generally
had high academic aspirations and life
ambition and that this was an effective
motivation for success.13, 19, 28, 32, 36, 37
Indeed, their desires to advance their
education, support relatives and
8
friends left behind, and help rebuild
their country were major motivators
for migration and life.19, 28, 32, 37
Seven studies examined parental
involvement in the education of
refugee children.9, 11, 12, 28, 31, 32, 37
Parental support for education was
identified as a protective factor for
refugee adolescents.28 However,
although they valued education
strongly, parental involvement in
TABLE 4 Educational Outcomes in Refugee-Background Children From Studies Included in This
Review
Educational Level Educational Outcomes
Preschool No studies identifi ed
Primary school No studies identifi ed
Secondary school performance
Failing, defi cient, GPA <2.0, % 21.910
Average, good, excellent, GPA >2.0, % 78.110
Mean GPA (secondary school) “Below peer level, ”23 “At peer level”33
0–4 scale 2.77–3.010, 30
0–5 scale 3.6818
Secondary school completion
Completed or on track, % 80–10028, 35, 40
Behind or dropped out, % 0–2028, 35, 40
Postsecondary school
Pursue postsecondary, % 53–8428, 40
GPA, grade point average.
TABLE 5 Estimated Prevalence of Learning Problems in Refugee-Background Children
Learning Problem Estimated Prevalence (%) Sample Size
Sensory impairment (n = 332)24
Vision 7.524
Hearing 3.324
Developmental delay 6.924
Gross motor 2.124
Fine motor 0.924
Language 5.724
Social 0.624
Cognitive 1.824
Specifi c language impairment,
dyscalculia or dyslexia
No studies identifi ed —
Cognitive function
Mean IQ (WISC-IV FSIQ) 8420 (n = 80)14
IQ <84 (WISC-IV FSIQ) 49.4–56.314, 20 (n = 390)20
IQ <70 (WISC-IV FSIQ) 11.120
Behavioral profi les
Total problems in “clinical
level”
CBCL (carer) 25.2–53.816, 23, 25, 34 (n = 102)11
Internalizing problems 13.9–27.316, 23 (n = 166)20
Externalizing problems 11.6–50.816, 23 (n = 182)22
YSR (self) 26.425 (n = 46)26
SDQ (self) 4.4–9.816, 39, 41
SDQ (carer) 9.0–3816, 17, 39, 41
ADHD 47.5 (M 65, F 30) if trauma14 (n = 80)14
7.5 (M 5, F 10) if no trauma14
ODD/CD 7.5 if trauma14 (n = 80)14
0 if no trauma14
Autism spectrum disorder No studies identifi ed —
Behavior problems 30 (M > F)10 (n = 144)20
Mental health problems (from previous systematic reviews and meta-analysis)
PTSD 11 (7–17) (n = 260)
19–5442 (n = 3003)42
Depression (n = 3003)42
CBCL, Child Behavior Checklist; FSIQ, full-scale IQ; SDQ, Strengths and Diffi culties Questionnaire; YSR, youth self-report.
by guest on April 18, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 137 , number 6 , June 2016
education was limited, with parents
having little contact with school and
providing minimal homework help.11, 12
Parents and teachers perceived
learning problems differently, with
teachers emphasizing language and
family dynamics whereas parents
emphasized the cultural gap of
educational styles and expectations.31
Parents and teachers both recognized
the importance of parent–teacher
communication, 31 but there were
frequent misunderstandings about
education styles, rules, and pathways,
attributed to different cultural
expectations and a lack of familiarity
with education systems.9, 11, 12 Three
studies described the positive effect
of “gift-and-sacrifice” motivational
narratives, whereby parents linked
their struggle with poverty and
migration to the value of educational
opportunity.28, 32, 37
One large US study found a positive
association between parental
education and secondary school
outcomes.35 However, 2 similar-sized
Canadian studies found parental
proficiency in the host country
language to be more important
than parental education per se.30, 40
These Canadian studies also found
no association between household
income and secondary school
outcomes, suggesting that education
was prioritized regardless of the
family’s socioeconomic status.30, 40
However, financial stress was
reported as a major risk factor
for secondary school dropout by
unaccompanied minors, who cited
unique challenges such as obligations
to earn and send money back to
family.28
Three studies reported that family
cohesion and supportive home
environment were associated with
better secondary school outcomes
(particularly for girls).6, 24, 30 Two
studies reported on the association
between parental physical and
mental health and secondary school
outcomes, with 1 finding a positive
association40 and the other finding no
association.30
School Environment
Eleven studies reported on
school transition for refugee
children.28, 31, 40, 11, 13, 32, 36, 37, 26, 27, 38
Accurate educational assessment
and grade placement were major
determinants of educational
success11, 32, 40 but were often
inaccurate.31, 38 Inadequate
appreciation of a child’s educational
experience was reported to result
in inappropriate grade placement
and expectations13, 28, 32, 36, 37, 40 and to
impair remedial educational efforts.38
This discrepancy resulted from either
expectations that were too high (ie,
failing to account for the impact of
interrupted education)13, 36, 40
or too low (ie, failing to recognize
previous learning).28, 37 Teacher
ignorance of linguistic heritage
has resulted in misunderstandings
(eg, misinterpreting respectful
whispering as being shy, unsure,
inattentive, or disrespectful),
misdiagnosis, and counterproductive
remediation attempts (eg, group
reading and public correction creating
a feeling of inadequacy and reinforced
withdrawal).11, 38 Conversely,
teachers’ understanding of a child’s
cultural heritage was associated with
enhanced learning at both primary38
and secondary11 school level.
Low teacher expectations of refugee-
background children were reported
to be common in both primary and
9
TABLE 6 Risk and Resource Factors Infl uencing Learning Outcomes for Refugee Children
Risk Factors Resource Factors
Individual child and home environment
Male gender10, 35 Female gender, 10, 35 younger age at migration, 40
greater length of time since resettlement, 40 and
urban residence40
Latino30, 31 (North American context) Cambodian or Vietnamese, 30, 31 Yugoslav40
English (new) language diffi culties13, 19, 36 High academic aspirations and life ambition13, 19,
28, 32, 36, 37
Financial stress28 Parental involvement in education11, 12, 28
Parental misunderstandings about educational
styles and expectations9, 11, 12, 31
“Gift-and-sacrifi ce” motivational narratives28, 32, 37
Parental education35 (or no association30, 40)
Parental profi ciency in the host country language30,
40
Family cohesion, supportive home environment.6,
24, 30
Parental physical and mental health40 (or no
association30)
School environment
Teacher ignorance of linguistic heritage11, 38 Accurate educational assessment and grade
placement11, 13, 28, 31, 32, 36–38, 40
Low teacher expectations28, 31, 37, 38 Teacher understanding of cultural heritage11, 38
Cultural stereotyping by teachers28, 31, 32, 37, 38 and
peers6, 11, 28, 37
Teachers who believed in child11, 28, 37
Lack of friends28, 37 Culturally appropriate transition program26, 27, 38
Bullying and racial abuse6, 9, 11, 19, 28, 32, 37 Supportive peer relationships6, 11, 13, 28, 37
Migration and trauma experience
Past experience of trauma, 15, 20–22 particularly
abandonment trauma21 and bullying
victimization22
Past experience of trauma33, 35, secondary trauma
(eg, parental war experience)21
Current or past forced detention24
Postmigration trauma (eg, bullying, racial
abuse)10, 15, 20–22, 30, 35, 41
Sociocultural environment
Positive acculturation (whereby there is selective
adoption of new country culture while
maintaining a strong connection with culture
and country of origin)28, 30, 31
by guest on April 18, 2020www.aappublications.org/newsDownloaded from

GRAHAM et al
secondary schools, 28, 31, 37, 38 with the
risk that such expectations would
become a self-fulfilling prophecy.38
Refugee-background youth reported
demotivation from low teacher
expectations and appreciated
teachers who believed in them
and encouraged them to pursue
challenging academic programs.11, 28, 37
Cultural stereotyping of refugee-
background children by
teachers was associated with
prejudiced assessments,
relationships, expectations, and
behavior.28, 31, 32, 37, 38
Three studies reported on school-
based interventions to facilitate
school transition for refugee
children.26, 27, 38 These studies support
the use of intentional transition
programs, culturally relevant
classroom techniques (eg, student-
driven gender segregation, student–
student interaction and assistance)
and explicit attention directed to low
teacher expectations.26, 27, 38 One study
involving a teacher-as-tutor program
reported benefits for both students
(accelerated academic progression)
and teachers (informed beliefs and
attitudes), who became allies in
helping students overcome broader
educational barriers and challenges.26
Five studies reported on the school
social environment in relation to
school success.6, 11, 13, 28, 37, Refugee
youth consistently report that
supportive peer relationships are
academically protective6, 11, 13, 28, 37;
however, difficulty forming such
relationships is the norm, resulting
in significant loneliness and
emotional stress.6, 13, 28, 37 Sport is a
common locus for successful peer
relationships, especially for boys, but
can both encourage and distract from
academic endeavor.13, 28, 37 Cultural
stereotypes strongly influence
social relationships, to the academic
advantage of some and detriment
of others (eg, African boys may be
expected to play sports but
not expected to succeed
academically).6, 11, 28, 37
Six studies found that overt
personal racism, bullying, and
abuse were common, and more
subtle discrimination was the
norm for refugee children and
adolescents, and this discrimination
negatively affected their educational
experience.6, 9, 11, 19, 28, 32, 37 Adolescents
reported feeling identified primarily
by their appearance (especially skin
color) and having to come to terms
with “embodying difference, ” often
experiencing this “otherness” for the
first time when arriving at school.37
Parents of preschool children
reported differential treatment and
derogatory race-based language from
teachers, whereas teachers reported
exclusion by other children.9
Migration and Trauma Experience
Ten studies reported on
the impact of trauma on
learning.10, 15, 20–22, 24, 30, 33, 35, 41 Three
studies involving 793 refugee-
background youth from multiple
countries reported that PTSD
and exposure to war trauma had
negligible10, 35 or positive33 impact on
school outcomes. Canadian students
from war zone countries had similar
academic outcomes to those from
non–war zone countries, and they
had higher academic expectations,
lower truancy, and greater high school
completion rates than their Canadian
peers (although often finishing at older
ages).35 Adolescents from Bosnia–
Herzegovina in Slovenia with greater
trauma exposure and symptoms of
PTSD tended to have higher academic
performance compared with matched
Slovenian-born peers.33
Conversely, 4 studies involving a
total of 319 traumatized children and
adolescents from Cambodia, Iraq, and
the Middle East found that cognitive
function was detrimentally affected
by trauma.15, 20–22 Daud et al15
described intergenerational effects
of trauma on Swedish refugees
from the Middle East, with children
of traumatized parents scoring
lower on cognitive tests despite no
direct experience of trauma (and
independent of whether they had
PTSD). Three studies involving the
same cohort of 200 Iraqi refugee
adolescents in the United States
reported that different types of
trauma had different effects on
cognitive testing (WISC-IV).20–22
“Abandonment trauma” had the
largest impact on all domains (equal
for either maternal or paternal
abandonment), whereas “personal
identity trauma” (eg, personal
assault or rape) affected working
memory, and “survival trauma”
(eg, life-threatening accident)
affected processing speed. “Collective
identity trauma” (eg, genocide or
discrimination) had no impact on
cognitive test results, whereas
“secondary trauma” (eg, parental war
experience) improved reasoning,
processing speed, and working
memory21. “Bullying victimization”
was associated with lower test scores
over and above other traumas.22
Two studies involving 302 refugee
youth from a variety of countries
reported that parental experience
in a refugee camp and parental
separation had no association with
secondary school outcomes.30, 40
Qualitative data from resettled
Sudanese-background refugee youth
demonstrated that thoughts of war
continued to disturb their daily lives,
including their ability to concentrate
and learn.19
Although premigration trauma
is common, there is increasing
recognition that postmigration
trauma is also common and may
have greater impact on both
learning10, 30, 35, 41 and cognitive
function.15, 20–22 Postmigration
trauma exposure was a significant
predictor for behavior problems
and academic failure in a cohort of
Khmer adolescents in the United
States, whereas premigration
trauma exposure did not correlate
with behavioral or educational
outcomes.10 The Australian refugee
health clinic study found that current
10 by guest on April 18, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 137 , number 6 , June 2016
or past mandatory immigration
detention was a significant predictor
for learning and psychological
difficulties among newly arrived
children.24
Sociocultural Environment
Three studies reported better
primary and secondary school
outcomes among refugee children
with greater levels of successful
acculturation (whereby there is
selective adoption of new country
culture while maintaining a strong
connection with culture and country
of origin).28, 30, 31
DISCUSSION
Our review of educational outcomes
and learning problems in refugee-
background children highlights the
complexity of examining learning
in refugee children and identifies
important gaps in the literature.
Overall, there are limited data
on the prevalence of learning
problems in refugee children, with
single studies informing most of
the estimates. There are almost no
studies describing children resettled
in developing countries, despite
the fact that 86% of refugees live in
developing countries.4
Most studies examined outcomes
in adolescent cohorts, there were
few studies on primary school
aged children and only a single
study involving preschool children,
which is concerning given the
importance of early identification for
effective intervention.43 Notably, no
studies reported the prevalence of
autism spectrum disorder, despite
higher rates in other immigrant
populations44–47 and a postulated
association with low vitamin D
levels, 48 which is well described
in resettled refugee populations.49
Similarly, there were no studies on
language impairment, dyscalculia, or
dyslexia, and only 1 study examined
any contribution from sensory
impairment. Only 1 study examined
the prevalence of ADHD, although
these authors highlighted the overlap
in ADHD and PTSD symptoms, which
is an area of particular diagnostic and
therapeutic uncertainty. The majority
of studies were cross-sectional;
the lack of longitudinal data is
a significant limitation, because
learning outcomes and contributing
factors may change over time (both
positively and negatively).
Implications for Practice
Despite significant data gaps, our
review has important implications
for health professionals, educators,
refugee support agencies, and
policymakers.
First, children of refugee background
should be expected and supported to
achieve school outcomes comparable
to those of their peers. Despite
limited data on the preschool or
primary school population, evidence
suggests refugee-background youth
have similar pass rates, completion
rates, and grade point averages to
their peers.10, 18, 28, 30, 33, 35, 40
Population data from other
immigrant populations have often
shown an academic advantage for
migrants compared with native-born
peers after adjusting for variables
such as socioeconomic status, the
so-called immigrant paradox.50, 51
Although the data on refugee-
background children are insufficient
to draw similar conclusions, many
of the same resource factors apply:
strong family ties (although a
significant minority experience
family loss or dislocation),
prioritization of education, “gift-and-
sacrifice” motivational narratives, 52
isolation from negative peer and
social influences, bilingual advantage,
and possible migration bias toward
healthier, wealthier, and more
educated parents.53 This finding
of academic resilience is echoed in
reviews on mental health of refugee
children, 42, 54–59 particularly the
examples of “positive deviance, ”
where children have better mental
health than would be predicted from
their life experiences and social
situation.
Evidence on the impact of trauma
on cognition and school outcomes is
mixed, with several studies indicating
that premigration trauma (and
symptoms of PTSD) has negligible (or
positive) effects on school outcomes.
Possible explanations for this effect
might be survival of past traumatic
experiences contributing to greater
resilience (eg, past trauma becoming
part of individual motivational
narratives), teachers being more
supportive to students who display
signs of PTSD, or survival bias (where
only the most resilient successfully
migrate).
Our review identified substantial
data on educational risk and resource
factors for refugee-background
children (Table 6). Major risk
factors included experience of
trauma, racism, and bullying;
parental misunderstandings about
educational styles and expectations;
and teacher stereotyping, low
teacher expectations, and poor
awareness of linguistic heritage.
Resource factors included high
academic and life ambition, parental
motivational narratives and
involvement in education, family
cohesion and supportive home
environment, accurate educational
assessment and grade placement,
teacher understanding of linguistic
and cultural heritage, culturally
appropriate school transition,
supportive peer relationships, and
successful acculturation. The risk
and resource factors identified in
our review share commonality to
those reported in previous reviews
on resilience in refugee children58
and the educational needs of refugee
students.60 It is clear that, although
premigration experiences do
influence refugee children’s learning,
the most important determinants
of success are located in the
postmigration context, and many of
11 by guest on April 18, 2020www.aappublications.org/newsDownloaded from

GRAHAM et al
these are modifiable in the country of
settlement.
Recommendations
Health professionals, educators,
social support agencies, and
policymakers all have important
roles in providing the individual,
family, community, and structural
support necessary for refugee-
background children to succeed.
Health professionals must identify
potential learning problems early
and work with schools to support
vulnerable children throughout their
educational and social transitions.
Pediatricians have a particular role
in these areas and should tailor their
developmental and educational
assessments to address particular
risk and resource factors. Alongside
health screening and medical
care, this support may include
contributing to accurate grade
placement (including age assessment
where needed), acknowledging
cultural and linguistic heritage,
valuing past educational and life
experience, affirming educational
aspirations, encouraging parental
involvement in school, reassuring
and educating families about
additional language acquisition,
encouraging maintenance of
the families’ first language, and
explicitly inquiring about learning
difficulties, racism experience, and
bullying. Given that some problems
become apparent only after time
in mainstream schooling (and
the dynamic nature of risk and
resource factors), longitudinal care is
important. Clinicians need to revisit
serial screening for school-related
problems as children and families
move through their social and
developmental transitions.6
Educators and schools must provide
inclusive and culturally safe school
environments and be aware that
school represents a major transition
for refugee-background students
and their families.60–62 Positive
supports include dedicated transition
programs, enhancing teacher
linguistic and cultural understanding,
proactively addressing bullying and
racial discrimination, encouraging
parental involvement in school,
incorporating past educational and
life experiences for appropriate
grade placement and individualized
learning plans, and promoting
appropriately high academic
expectations. The finding that
refugee-background students
experience high levels of school-
and peer-based racial abuse and
discrimination is disturbing, and
this will affect not only learning, but
health, well-being, and acculturation
more broadly.6, 49
Support agencies and policymakers
must recognize the importance
of migration transition supports,
including linguistic and educational
transition programs. In the early
postsettlement period, supporting
access to health professionals and
educators who are experienced in
working with refugee-background
children and families is likely to be
of benefit, alongside education and
support for parents to engage with
their children’s schools.
Researchers also have a role in
advancing our understanding of
learning and educational outcomes
in refugee-background students. Key
evidence gaps include longitudinal
assessments of educational and
vocational outcomes and the
influence of risk and resource factors
over time, evaluation of learning in
preschool and primary school–age
populations, directed research
with new population groups, and
comparative evaluations of resettled
populations in different countries
and contexts. Research is also needed
into the validity of assessment tools
in refugee-background populations.
The tools we use to assess
intelligence, behavior, and social and
emotional well-being are culturally
bound, having been developed and
validated in certain population and
language groups (usually European
or North American) and cannot
be assumed to be valid in other
populations.63 Although some of
these tests have been adapted for
use in other specific populations (eg,
WISC tests), they are not validated
for most of the population groups
who become refugees63 or for use
with interpreters. Despite these
obvious limitations, such testing
may be mandated by education
systems when learning problems or
intellectual disability is suspected.
Clinicians working with refugee
children often grapple with
understanding the meaning and
application of cognitive, behavioral,
or language assessments and
deciding which diagnostic labels
most accurately describe clinical
presentations. These clinical
dilemmas highlight the role of
the developmental history and
longitudinal care in supporting
refugee-background students with
learning problems. Additional
research is needed to develop
culturally appropriate assessment
tools, address language difficulties
in assessments, and develop a
nuanced understanding of behavioral
phenotypes in children of refugee
background.
Our review has several limitations.
Although our search strategy
involved multiple databases, we
excluded studies that were not
published in peer-reviewed journals
and studies that were not available
in the English language. Inclusion
criteria required a defined refugee-
background population and excluded
studies that may have included this
population but did not identify them
explicitly (eg, Latino immigrants to
the United States). This criterion
was intended to ensure that the data
better represent forced migration
rather than immigrant populations
more generally. Although included
studies involved children from
various backgrounds, many findings
cannot be generalized to other
refugee-background populations.
12 by guest on April 18, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 137 , number 6 , June 2016
Many studies used convenience
sampling rather than more robust
selection methods. This limitation is
due largely to the methodological,
ethical, and practical challenges of
working with vulnerable populations
and remains an ongoing challenge to
researchers in this field.
CONCLUSIONS
Success at school is critical to well-
being for refugee-background children.
Published data on educational
outcomes and learning problems in
this population are limited, particularly
for younger children and children
in low- or middle-income countries.
Overall, refugee-background children
should be expected (and encouraged)
to achieve comparably to their peers.
Clinicians and educators have an
important role in identifying risk
factors and also acknowledging
the positive resources that refugee
children and families bring to their
education and countries of settlement.
These findings provide practical
guidance to clinicians and educators
working with refugee children and
families, highlight areas for future
research, and inform interventions and
policy to support refugee children to
achieve their developmental potential.
ACKNOWLEDGMENTS
Thanks to Kate Milner for advice on
developmental tools, Shidan Tosif
and Kelly Jurianz for review of the
manuscript, research librarian Poh
Chua for assisting with the search
strategy, and Thivia Jegathesan for
assistance with proofreading and
manuscript revision.
13
ABBREVIATIONS
ADHD: attention-deficit
hyperactivity disorder
CINAHL: Cumulative Index to
Nursing and Allied
Health Literature
ERIC: Education Resources
Information Center
ODD/CD: oppositional defiant
disorder/conduct
disorder
PTSD: posttraumatic stress
disorder
UNHCR: United Nations High
Commission for
Refugees
WISC: Wechsler Intelligence
Scales for Children
WISC-IV: Wechsler Intelligence
Scales for Children,
Fourth Edition
Dr Graham conceptualized and designed the study, conducted the database searches, reviewed articles for inclusion, and drafted the initial manuscript; Dr
Minhas conceptualized and designed the study, reviewed articles for inclusion, and drafted the initial manuscript; Dr Paxton contributed to the conceptualization
and design of the study and reviewed the draft; and all authors approved the fi nal manuscript as submitted.
DOI: 10.1542/peds.2015-3994
Accepted for publication Mar 21, 2016
Address correspondence to Hamish R. Graham, MBBS, MPH, FRACP, Centre for International Child Health, Level 2 East, The Royal Children’s Hospital, 50 Flemington
Rd, Parkville VIC 3052, Australia. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2016 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no fi nancial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential confl icts of interest to disclose.
REFERENCES
1. Goswami U. Foresight Mental Capital and
Wellbeing Project. Learning Diffi culties:
Future Challenges. London, England: The
Government Offi ce for Science; 2008
2. Bronfenbrenner U. The Ecology of
Human Development. Boston, MA:
Harvard University Press; 1979
3. Oberklaid F, Levine MD. Precursors
of school failure. Pediatr Rev.
1980;2(1):5–11
4. UNHCR. World at War: UNHCR
Global Trends: Forced Displacement
in 2014. Geneva, Switzerland:
UNHCR; 2015
5. Crisp J, Talbot C, Cipollone DB. United
Nations High Commissioner for
Refugees G (Switzerland). Learning
for a Future: Refugee Education
in Developing Countries. Geneva,
Switzerland: UNHCR; 2001
6. Correa-Velez I, Gifford SM, Barnett AG.
Longing to belong: social inclusion and
wellbeing among youth with refugee
backgrounds in the fi rst three years
in Melbourne, Australia. Soc Sci Med.
2010;71(8):1399–1408
7. Arksey H, O’Malley L. Scoping
studies: towards a methodological
framework. Int J Soc Res Methodol.
2005;8(1):19–32
8. Levac D, Colquhoun H, O’Brien KK.
Scoping studies: advancing the
methodology. Implement Sci. 2010;5:69
9. Agbenyega J, Klibthong S. Whole
school initiative: has inclusive
education gone astray? Int J Whole
Sch. 2013;9(1):3–22
10. Berthold SM. War traumas and
community violence: psychological,
behavioral, and academic outcomes
among Khmer refugee adolescents. J
Multicult Soc Work. 2000;8(1–2):15–46
by guest on April 18, 2020www.aappublications.org/newsDownloaded from

GRAHAM et al
11. Bitew G, Ferguson P, Dixon M. Ethiopian-
Australian students’ experience of
secondary schooling in the Australian
education system in the State of
Victoria. Australas Rev African Stud.
2008;29(1):78–91
12. Bitew G, Ferguson P. Parental support
for African immigrant students’
schooling in Australia. J Comp Fam
Stud. 2010;41(1):149–165
13. Brown J, Miller J, Mitchell J.
Interrupted schooling and the
acquisition of literacy: experiences
of Sudanese refugees in Victorian
secondary schools. Aust J Lang Lit.
2006;29(2):150–162
14. Daud A, Rydelius P-A. Comorbidity/
overlapping between ADHD and
PTSD in relation to IQ among
children of traumatized/non-
traumatized parents. J Atten Disord.
2009;13(2):188–196
15. Daud A, Klinteberg B af, Rydelius P-A.
Resilience and vulnerability among
refugee children of traumatized
and non-traumatized parents. Child
Adolesc Psychiatry Ment Health.
2008;2(7):2
16. Derluyn I, Broekaert E. Different
perspectives on emotional
and behavioural problems in
unaccompanied refugee children
and adolescents. Ethn Health.
2007;12(2):141–162
17. Fazel M, Stein A. Mental health of
refugee children: comparative study.
BMJ. 2003;327(7407):134
18. Fox PG, Burns KR, Popovich JM,
Belknap RA, Frank-Stromborg M.
Southeast Asian refugee children: self-
esteem as a predictor of depression
and scholastic achievement in
the US. Int J Psychiatr Nurs Res.
2004;9(2):1063–1072
19. Hatoss A, O’Neill S, Eacersall D. Career
choices: linguistic and educational
socialization of Sudanese-background
high-school students in Australia.
Linguist Educ. 2012;23(1):16–30
20. Kira I, Lewandowski L, Yoon J, Somers
C, Chiodo L. The linear and nonlinear
associations between multiple types
of trauma and IQ discrepancy indexes
in African American and Iraqi refugee
adolescents. J Child Adolesc Trauma.
2012;5(1):47–62
21. Kira I, Lewandowski L, Somers CL,
Yoon JS, Chiodo L. The effects of
trauma types, cumulative trauma, and
PTSD on IQ in two highly traumatized
adolescent groups. Psychol Trauma.
2012;4(1):128–139
22. Kira IA, Lewandowski L, Ashby JS,
Somers C, Chiodo L, Odenat L. Does
bullying victimization suppress IQ?
The effects of bullying victimization
on IQ in Iraqi and African American
adolescents: a traumatology
perspective. J Aggress Maltreat
Trauma. 2014;23(5):431–453
23. Lee YM, Shin OJ, Lim MH. The
psychological problems of North
Korean adolescent refugees living
in South Korea. Psychiatry Investig.
2012;9(3):217–222
24. Mace AO, Mulheron S, Jones C, Cherian
S. Educational, developmental and
psychological outcomes of resettled
refugee children in Western Australia:
a review of School of Special
Educational Needs: Medical and Mental
Health input. J Paediatr Child Health.
2014;50(12):985–992
25. Mollica RF, Poole C, Son L, Murray
CC, Tor S. Effects of war trauma on
Cambodian refugee adolescents’
functional health and mental health
status. J Am Acad Child Adolesc
Psychiatry. 1997;36(8):1098–1106
26. Naidoo L. A structuration theory
analysis of the Refugee Action
Support Program in greater
western Sydney. Aust J Teach Educ.
2009;34(4):40–50
27. Nykiel-Herbert B. Iraqi refugee
students: from a collection of aliens to
a community of learners—the role of
cultural factors in the acquisition of
literacy by Iraqi refugee students with
interrupted formal education. Multicult
Educ. 2010;17(3):2–14
28. Rana M, Qin DB, Bates L, Luster
T, Saltarelli A. Factors related to
educational resilience among
Sudanese unaccompanied minors.
Teach Coll Rec. 2011;113(9):2080–2114
29. Rousseau C, Drapeau A, Platt R. Living
conditions and emotional profi les of
Cambodian, Central American, and
Québécois youth. Can J Psychiatry.
2000;45(10):905–911
30. Rousseau C, Drapeau A. Scholastic
achievement of adolescent refugees
from Cambodia and Central America.
Adolescence. 2000;35(138):243–258
31. Rousseau C, Drapeau A, Corin E.
School performance and emotional
problems in refugee children. Am J
Orthopsychiatry. 1996;66(2):239–251
32. Shakya YB, Guruge S, Hynie M, et al.
Aspirations for higher education
among newcomer refugee youth in
Toronto: expectations, challenges, and
strategies. Refuge. 2010;27(2):65–78
33. Slodnjak V, Kos A, Yule W. Depression
and parasuicide in refugee and
Slovenian adolescents. Crisis.
2002;23(3):127–132
34. Sourander A. Behavior problems and
traumatic events of unaccompanied
refugee minors. Child Abuse Negl.
1998;22(7):719–727
35. Stermac L, Elgie S, Clarke A, Dunlap
H. Academic experiences of war-zone
students in Canada. J Youth Stud.
2012;15(3):311–328
36. Tlhabano KN, Schweitzer R. A
qualitative study of the career
aspirations of resettled young
Sudanese and Somali refugees. J
Psychol Afr. 2007;17(1–2):13–21
37. Uptin J, Wright J, Harwood V. “It
felt like I was a black dot on white
paper”: examining young former
refugees’ experience of entering
Australian high schools. Aust Educ Res.
2013;40(1):125–137
38. Usman LM. Communication disorders
and the inclusion of newcomer African
refugees in rural primary schools of
British Columbia, Canada. Int J Prog
Educ. 2012;8(2):102–120
39. Wiegersma PA, Stellinga-Boelen AAM,
Reijneveld SA. Psychosocial problems
in asylum seekers’ children: the
parent, child, and teacher perspective
using the Strength and Diffi culties
Questionnaire. J Nerv Ment Dis.
2011;199(2):85–90
40. Wilkinson L. Factors infl uencing
the academic success of refugee
youth in Canada. J Youth Stud.
2002;5(2):173–193
41. Ziaian T, de Anstiss H, Antoniou G,
Baghurst P, Sawyer M. Emotional
14 by guest on April 18, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 137 , number 6 , June 2016
and behavioural problems among
refugee children and adolescents
living in South Australia. Aust Psychol.
2013;48(2):139–148
42. Bronstein I, Montgomery P.
Psychological distress in refugee
children: a systematic review.
Clin Child Fam Psychol Rev.
2011;14(1):44–56
43. Lazar I, Darlington R, Murray H,
Royce J, Snipper A, Ramey CT. Lasting
effects of early education: a report
from the Consortium for Longitudinal
Studies. Monogr Soc Res Child Dev.
1982;47(2–3):1–151
44. Bolton S, McDonald D, Curtis E, Kelly
S, Gallagher L. Autism in a recently
arrived immigrant population. Eur J
Pediatr. 2014;173(3):337–343
45. Lehti V, Hinkka-Yli-Salomäki S,
Cheslack-Postava K, Gissler M,
Brown AS, Sourander A. The risk of
childhood autism among second-
generation migrants in Finland: a
case–control study. BMC Pediatr.
2013;13:171
46. Haglund NG, Källén KB. Risk factors
for autism and Asperger syndrome.
Perinatal factors and migration.
Autism. 2011;15(2):163–183
47. Dealberto MJ. Prevalence of autism
according to maternal immigrant
status and ethnic origin. Acta Psychiatr
Scand. 2011;123(5):339–348
48. Kočovská E, Fernell E, Billstedt E,
Minnis H, Gillberg C. Vitamin D and
autism: clinical review. Res Dev Disabil.
2012;33(5):1541–1550
49. Paxton G, Smith N, Win AK, Mulholland
N, Hood S. Refugee Status Report.
Department of Education and Early
Childhood Development. Melbourne,
Australia: State Government Victoria; 2011
50. Cobb-Clark DA, Sinning M, Stillman
S. Migrant youths’ educational
achievement: the role of institutions.
Ann Am Acad Pol Soc Sci.
2012;643(1):18–45
51. Coll CG, Marks AK. In: Coll CG, Marks
AK, eds. The Immigrant Paradox
in Children and Adolescents: Is
Becoming American a Developmental
Risk? Washington, DC: American
Psychological Association; 2012
52. Ceballo R, Maurizi LK, Suarez GA,
Aretakis MT. Gift and sacrifi ce: parental
involvement in Latino adolescents’
education. Cultur Divers Ethnic Minor
Psychol. 2014;20(1):116–127
53. Crosnoe R, Turley RN. K–12 educational
outcomes of immigrant youth. Future
Child. 2011;21(1):129–152
54. Porter M, Haslam N. Predisplacement
and postdisplacement factors
associated with mental health of
refugees and internally displaced
persons: a meta-analysis. JAMA.
2005;294(5):602–612
55. Lustig SL, Kia-Keating M, Knight WG,
et al. Review of child and adolescent
refugee mental health. J Am Acad Child
Adolesc Psychiatry. 2004;43(1):24–36
56. Fazel M, Reed RV, Panter-Brick C,
Stein A. Mental health of displaced
and refugee children resettled
in high-income countries: risk
and protective factors. Lancet.
2012;379(9812):266–282
57. Reed RV, Fazel M, Jones L, Panter-Brick
C, Stein A. Mental health of displaced
and refugee children resettled in low-
income and middle-income countries:
risk and protective factors. Lancet.
2012;379(9812):250–265
58. Betancourt TS, Khan KT. The mental
health of children affected by armed
confl ict: protective processes and
pathways to resilience. Int Rev
Psychiatry. 2008;20(3):317–328
59. Fazel M, Wheeler J, Danesh J.
Prevalence of serious mental disorder
in 7000 refugees resettled in western
countries: a systematic review. Lancet.
2005;365(9467):1309–1314
60. McBrien JL. Educational needs
and barriers for refugee students
in the United States: a review
of the literature. Rev Educ Res.
2005;75(3):329–364
61. Brown CS, Chu H. Discrimination,
ethnic identity, and academic
outcomes of Mexican immigrant
children: the importance of
school context. Child Dev.
2012;83(5):1477–1485
62. Kia-Keating M, Ellis BH. Belonging and
connection to school in resettlement:
young refugees, school belonging,
and psychosocial adjustment.
Clin Child Psychol Psychiatry.
2007;12(1):29–43
63. Georgas J. Cross-cultural psychology,
intelligence, and cognitive processes.
In: Georgas J, Weiss LG, van de Vijver
FJR, Saklofske DH, eds. Culture and
Children’s Intelligence: Cross-Cultural
Analysis of the WISC-III. San Diego, CA:
Academic Press; 2003:24–40
15 by guest on April 18, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2015-3994 originally published online May 18, 2016; 2016;137;Pediatrics
Hamish R. Graham, Ripudaman S. Minhas and Georgia PaxtonLearning Problems in Children of Refugee Background: A Systematic Review
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/137/6/e20153994including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/137/6/e20153994#BIBLThis article cites 56 articles, 2 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/immigration_subImmigrationalth_subhttp://www.aappublications.org/cgi/collection/international_child_heInternational Child Healthrning_disorders_subhttp://www.aappublications.org/cgi/collection/cognition:language:leaCognition/Language/Learning Disordersal_issues_subhttp://www.aappublications.org/cgi/collection/development:behaviorDevelopmental/Behavioral Pediatricsfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on April 18, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2015-3994 originally published online May 18, 2016; 2016;137;Pediatrics
Hamish R. Graham, Ripudaman S. Minhas and Georgia PaxtonLearning Problems in Children of Refugee Background: A Systematic Review
http://pediatrics.aappublications.org/content/137/6/e20153994located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2016/05/17/peds.2015-3994.DCSupplementalData Supplement at:
1073-0397. ISSN:60007. Copyright © 2016 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on April 18, 2020www.aappublications.org/newsDownloaded from