Embed Size (px)
Citation preview
a report on the Local Exercise Action Pilots
Learning from LEAPLE
AP
Loca
l Exe
rcis
e A
ctio
n P
ilots
The Local Exercise Action Pilotsprogramme is jointly funded by
Executive Summary
1.0 Introduction and Background
2.0 The Local Exercise Action Pilots
3.0 Evaluation Methodology
4.0 Key Findings
• Who was engaged in LEAP?
• Did the participants in LEAP interventions increase their levels ofphysical activity?
• The different intervention types
• Costs and cost effectiveness of the physical activity interventions
5.0 Lessons from LEAP
• Design characteristics of successful physical activity interventions
• Good practice in evaluating physical activity interventions
6.0 Conclusions and Recommendations
Appendices
A - Overview of LEAP interventions and priority groups
B - MET thresholds for physical activity participation categories
Contents
3
5
7
11
13
13
14
15
20
22
22
24
26
28
30
Learning from LEAP
We would like to thank all of the individuals andorganisations that have been involved in the management,delivery and evaluation of LEAP including the 10 pilot sites andtheir lead agencies, project managers, delivery teams andparticipants; Sport England; Natural England (formerly theCountryside Agency); Department of Health Physical ActivityTeam; The Carnegie Research Institute at Leeds MetropolitanUniversity; Matrix; MORI and Yew Consulting Ltd.

The Chief Medical Officer’s (CMO)report ‘At Least Five a Week’ setsout the strength of evidence for the role physical activity canplay in preventing and treating a range of disease conditions andrecommends minimum levels ofparticipation in physical activity foryoung people and adults to conferthe health benefits. 70% ofadults, 30% of boys and 40% ofgirls are not currently achievingthe recommended levels, givingcause for public concern.
Although the evidence base onthe health benefits of physicalactivity is convincing, moreinformation is needed to identifythe most effective interventionsfor getting people physicallyactive. The Local Exercise ActionPilots (LEAP) were commissionedto collect evidence on theeffectiveness of physical activityinterventions and to disseminatelearning and good practice. Their overall aim was toencourage people, in particularthose from priority groups, toparticipate in physical activity and to achieve an activity levelthat meets or exceeds theDepartment of Health guidelines.
The evaluation of the LEAPinterventions has provided arobust set of qualitative andquantitative data that contributessignificantly to the evidence base currently available in theUnited Kingdom related to shortterm physical activity behaviourchange and the effectiveness ofphysical activity interventions. Key findings from LEAP include:
• A broad range of people were attracted to the LEAPinterventions and engaged inphysical activity, includingpeople who were sedentary, at risk of particular healthconditions and from prioritygroups. 40% of participantswere sedentary or lightly activei.e. not meeting the CMOrecommended guidelines forphysical activity at the start ofthe LEAP interventions. 60%were already moderately orhighly active. Careful planning is required to ensure that theinactive and those at risk ofparticular health conditions are effectively targeted wheninterventions are planned and implemented.
• The majority of participants who took part in the physicalactivity interventions increasedtheir physical activity levels. A comparison of 1051participants who provided both baseline and interventionphysical activity data showed a positive intervention effect.The median increase acrossparticipants equates toapproximately 75 minutes of additional brisk walking per week.
• Increases in physical activitywere greatest amongparticipants who were sedentaryand lightly active at the start of the intervention. 80% of LEAP participants who weresedentary at baseline and 63%of those who were lightly activeat baseline moved up at leastone physical activity category i.e.from sedentary to lightly active,moderately active or highlyactive; or from lightly active tomoderately active or highly active.
70% of adults, 30% of boys and 40% of girls are notcurrently achieving therecommended levels, givingcause for public concern.
Executive Summary LEAP interventions were cost effective to implement.The cost per quality adjustedlife year gained from thephysical activity interventionswas significantly lower thanthe threshold for investing in medical interventionsimplied from decisions madeby the National Institute forHealth and Clinical Excellence.
• The LEAP interventions alsodemonstrated that the potentialcost savings to the NationalHealth Service exceeded thecosts per participant ofimplementing the intervention.
The LEAP evaluation confirmedthat the way that interventions areplanned, delivered and managedcan make a significant differenceto their overall effectiveness inboth attracting people frompriority groups and the extent towhich physical activity changetakes place. Design characteristicscontributing to the success of the LEAP projects in engagingparticipants and bringing aboutphysical activity change includedlinking the physical activityintervention into local strategiesand existing programmes;undertaking outreach workbefore the intervention starts;putting in place simple referralprotocols; tailoring theprogrammes provided to meet theneeds of individual participants;connecting people into more thanone intervention to help them get
and stay active; locating thephysical activity intervention inenvironments that are local andfamiliar to the target audience;recruiting dedicated and skilledstaff and volunteers thatunderstand the needs of prioritygroups they will be targeting;building capacity as part of theintervention and identifyingsustainable exit routes early in the intervention.
The LEAP research and evaluationdemonstrated that appropriatelydesigned physical activityinterventions can attract andengage a broad range of peopleand increase their physical activitylevels in the short term. The mostsignificant positive change inphysical activity levels will occuramong people who are sedentaryor lightly active at the start of theintervention. The LEAP projectshave also demonstrated thatphysical activity interventions can be cost effective.
Based on the evidenceavailable from LEAP therecommendations forcommissioning agencies are:
• to commission physical activityinterventions, in particularexercise referral (according to NICE guidelines) andmotivational interviewing, to engage and help facilitatepositive change in the physicalactivity levels of priority groups
and especially among peoplewho are currently sedentary or lightly active;
• to commission pilot projects for classes and groups and other types of physical activityintervention best suited to thepriority group being targetedand to confirm their impact onphysical activity levels throughadditional evaluation prior tolarge scale implementation;
• to undertake further evaluationand longitudinal research toexplore how engagement andchange can be translated intolonger term maintenance of the CMO guidelines.
The recommendations for delivery and evaluationagencies are:
• to develop physical activityinterventions in partnership with a range of otherorganisations from the health,physical activity and sportssectors who can provideresource, advice and knowledgeas well as sustainable exit routes for participants;
• to ensure that the objectives of the physical activityintervention are agreed prior to commencement and to apply the design characteristicsof successful physical activity interventions and good practice in evaluations identified by LEAP.
Learning from LEAP 0403
60% of participants who wereclassified as either sedentary or lightly active at baselineachieved the CMO recommendedguideline of being moderatelyactive after participating in LEAP.
The median increase across LEAP participants inphysical activity equated toapproximately 75 minutes of additional brisk walking per week.

1.1 The Chief Medical Officer’s(CMO) report ‘At Least Five aWeek’1 sets out the strength ofevidence for the role physicalactivity can play in preventing and treating a range of diseaseconditions including obesity,cardiovascular disease, diabetes,some types of cancer and mental health.
1.2 To obtain such health benefitsthe Department of Healthrecommends minimum levels ofparticipation in physical activity for young people and adults:
• Young people should achieve a total of at least 60 minutes of at least moderate intensityactivity each day.
• Adults should achieve a total of at least 30 minutes of at least moderate intensity physicalactivity, on 5 or more days a week.
1.3 Current levels of participationin physical activity give cause forpublic concern. 70% of adults,30% of boys and 40% of girls2
are not currently achieving therecommended levels. As a resultgovernment policies andchallenging targets3 have been set for increasing participation in physical activity over the nextfew years.
1.4 The CMO report and otherresearch4 confirms that althoughthe evidence base on the healthbenefits of physical activity isconvincing, more information isneeded to identify the mosteffective interventions for gettingpeople physically active. The LocalExercise Action Pilots (LEAP) werecommissioned in 2004 to collectevidence over a two year periodon the effectiveness of physicalactivity interventions and todisseminate learning and good
practice about such interventionsamong the health and physicalactivity community.
1.5 The overall aim of the LEAPinterventions was to encouragepeople, in particular those frompriority groups, to participate inphysical activity and to achieve anactivity level that meets or exceedsthe Department of Healthguidelines.
1.6 The evaluation of the LEAPinterventions has providedimportant quantitative andqualitative data related to shortterm physical activity behaviourchange and the effectiveness ofphysical activity interventions. This report introduces the LEAPprojects, reports the key findingsand conclusions and providesrecommendations for the future.It is aimed at commissioners,purchasers and providers ofphysical activity interventions.
Learning from LEAP
1.0 Introduction and background
1 At Least Five a Week, Chief Medical Officer,
Department of Health, 2004
2 At Least Five a Week, Chief Medical Officer,
Department of Health, 2004 and the Health
Survey for England, Department of
Health, 2002
3 Game Plan targets are for 70% of adults to
achieve the recommended levels of physical
activity by 2020, with an interim target of
50% by 2011. Department for Culture,
Media and Sport/Strategy Unit, 2002
4 National Institute of Health and Clinical
Excellence, 2006; Centre of Disease Control,
Kahn, 2002
0605
Current levels of participation inphysical activity give cause for public concern. 70% of adults, 30% of boys and 40% of girls are notcurrently achieving the Department of Health recommended minimumlevels of participation to obtain health benefits .

2.1 LEAP was commissioned andmanaged by a partnershipconsisting of the Department ofHealth, Natural England and Sport England. It was delivered at a local level by Primary CareTrusts (PCTs) working with localpartner agencies, or by localauthority or local leisure Trustsworking with the PCT and otherpartner agencies.
2.2 One LEAP site was located ineach of the nine English regions,with the exception of the SouthWest region which had two pilots.The pilot sites were:
• Ashton, Wigan and Leigh: North West
• Durham Dales: North East
• Dudley, Beacon and Castle:West Midlands
• Great Yarmouth: East
• Hastings St Leonard’s: South East
• Wandsworth: London
• Nottingham City: East Midlands
• North Kirklees: Yorkshire
• Plymouth: South West 1
• West of Cornwall: South West 2
2.3 Each pilot targeted one ormore priority group to engage inthe physical activity interventions.Participants living in areas withhigh levels of deprivation andhealth inequalities were a priorityalong with other groups with lowlevels of physical activityparticipation and that face thegreatest barriers to becomingactive5. This included children andyoung people; older people; blackand minority ethnic groups andadults with health conditions or at risk of health conditions such as obesity, heart disease or mentalhealth problems.
2.0 The Local Exercise Action Pilots
The Wandsworth Active LivingMap was developed for theresidents of Wandsworth,highlighting easy routes to localphysical activity opportunities. The aim was to bring togetherexisting maps, routes and leafletsto form a single resource,emphasizing low cost activitiesand areas for recreation such asparks, commons and open spaces.The maps were targeted atinactive residents living or workingin the Borough of Wandsworth,primarily those in recognised areasof deprivation such as the wardsaround the rivers Wandle andThames, although all residents
could obtain a map. The mapswere developed in partnershipwith Wandsworth CyclingCampaign, Wandsworth BoroughCouncil (Transport departmentand Parks Service) and Sustrans.10,000 maps were initially printedand proved to be a popular anduseful resource; with all mapsquickly distributed to residentsaround the borough. Of thosethat completed an evaluation71% reported it had helped themto be more active. Many positivecomments were received:
“It has shown me a new greenWandsworth that I knew
existed just didn't know how to use it”“Very clear and colourful,inspiring”“I've become moreindependent”Due to the great success andpopularity of the mapWandsworth Council funded the printing of another 10,000maps in January 2006. Thesecontinue to be distributed toresidents around the borough.
For more information contact: Liz Kellow:[email protected]
The ‘Stepping Out’ project in theBorough of Wigan developed anintegrated programme of physicalactivity opportunities to addressthe needs of older people(50+years), particularly thoseliving in deprived communities.This included a number ofdifferent interventions:
• talks, taster sessions andexercise courses provided by an outreach worker at localcommunity venues across the Borough;
• a sports, dance and activityprogramme;
• the ‘Steps to Health’ exercisereferral programme and ‘NewWeighs’ course of exercise andnutritional information;
• the ‘Healthwalks’ programmewhich included weekly healthwalks, an annual borough walkand pedometer challenges;
• a falls prevention initiativewhere frail, older peopleparticipated in specific exercise classes;
• a peer mentoring/buddyingprogramme where a regular
participant of an activity buddiesup with a new starter;
• ‘Moving more often’ training for residential and nursing homestaff and assistants on how toprovide light exercises and arange of motion activities fortheir residents; and
• a communication and marketingcampaign.
Over 2,500 people participated in the interventions betweenSeptember 2004 and December2005 ranging from 50 to 104 years of age. The leadorganisation for the programmewas Ashton, Wigan and LeighPrimary Care Trust who workedwith the Active Living Team of the Wigan Leisure and CultureTrust. Other partners includedAge Concern, Wigan CouncilAdult Services and theWrightington, Wigan and LeighNHS Trust. The University ofSalford were involved as the localevaluators of the project.
For further information contactCarol Southern:[email protected]
In Hastings the LEAP interventionsfocused particularly on youngpeople and included:
• ‘Girlz Gettin Active’, designed by girls for girls. The projectinvolved a range of fitnessactivities and games and usedproactive marketing techniquestargeted specifically at youngwomen to attract participants;
• street dance clubs, with tasterclasses in schools followed up bycommunity based street dancesessions;
• ‘Walk to school week’campaign, run in partnershipwith school P.E departments,which involved promotionalresources being distributed inschools to promote the messagethat walking is good for you and gave young people anopportunity to participate inpower walking in a PE session;
• ‘Extend your life’ theatreproduction, run by Theatre inEducation, which educatedyoung people about how toachieve 60 minutes of moderateintensity physical activity andfollow an active lifestyle;
• the ‘Active Attitude’ summerprogramme combining physicalactivity and healthy eatingtargeted at overweight andsedentary children; and
• ‘Young Mums’ Activityproviding affordable exerciseclasses with childcare provision.This included four differentweekly groups operating indeprived wards.
2925 young people engaged inthe LEAP interventions and over500 sessions were run. The leadorganisation for the programmewas Hastings and Rother PrimaryCare Trust, with a wide range ofpartners including local schools.
For further information contact:Hayley Martin:[email protected]
Stepping Out Ashton, Wigan and Leigh
Active HastingsHastings, St Leonard’s
Active Living MapWandsworth Primary Care Trust and Wandsworth Council
Learning from LEAP 0807
5 Department of Health, 2004; HealthEducation Authority, 1999

In Nottingham the ‘Get Moving’project was implemented with the aim of increasing physicalactivity and decreasing sedentarybehaviour amongst the city'sresidents aged 50 years and over,particularly those living in themost deprived areas of the city of Nottingham. A multicomponent campaign wasimplemented consisting of sixrelated interventions:
• mapping and consultation –an audit of local provision to identify where gaps oropportunities were located andconsulting people to identifysupportive factors and barriersto becoming active;
• advertising campaign –a community wide campaign tohelp raise awareness of thebenefits of physical activity, the ‘Get Moving’ Nottingham
projects and local opportunitiesto become physically active;
• involving people in physicalactivity – working withcommunity groups to developgroup based activity sessionsbased on need;
• senior peer mentoring – avolunteer programme helpingpeople aged 50 and over tobecome more active byproviding them with supportand encouragement in the formof a mentor on positive ways to become more active;
• physical activity associateadvisor training – trainingworkers who support peopleaged 50 and over in briefinterventions to encourage andadvise clients on how they canlead more active lives; and
• specialist physical activityadvisors – employing specialistphysical activity advisors whouse motivational interviewingtechniques to support clients in becoming more active.
The lead organisation for theprogramme was NottinghamPrimary Care Trust who workedwith a wide range of partnersincluding Nottingham YMCA,Nottingham City Council – LeisureServices, Age Concern – First Link,Communities for Health – GetMoving Nottingham, The NiftyFifties, Bulwell Healthy LivingCentre, various communitygroups and individual volunteers.
For further information contact:Paul.dodsley@nottinghamcity-pct.nhs.ukwww.getmovingnottingham.nhs.uk
2.4 The interventions weredeveloped and delivered in bothcommunity and health settings bya range of partners. This included:
• Primary Care and NHS Trusts
• GP’s and other healthprofessionals
• Local authorities, including sport and leisure, children’s and adult services
• Schools
• Youth organisations and groups
• Community and voluntarygroups and trusts
• Sports clubs and sportspartnerships
2.5 LEAP sites used one or more of the following types of physicalactivity intervention to engageparticipants:
• Exercise Referral: This involvedthe referral of a participant by an allied professional, usually ina health, education or youthsetting, to a physical activityintervention undertaken withinthe local community e.g. afitness session in a local gym, an exercise class or a walkinggroup. Participation by theindividual in physical activity was then undertaken on a oneto one basis or in a groupsituation, but was normallytailored to their individual needs.Exercise referral interventionstook place at 5 LEAP sites.
• Peer Mentoring: This involvedthe engagement of participantsin dialogue and interaction with a peer of the same age group.
The dialogue aimed to promotephysical activity and develop thecapacity of the participant tobecome physically active eitherindependently or within a classsituation external to peermentoring. Peer mentoringinterventions took place at 3LEAP sites.
• Classes and Groups:This involved the engagement of a participant in a structured or unstructured physical activityintervention involving otherpeople. This was normally in acommunity setting and includeda variety of different modes of physical activity both indoorsand outdoors e.g. swimmingsessions, dance and exerciseclasses, after school sportsactivities, walking groups etc.Classes and groups took place at 8 LEAP sites.
• Campaigns and Directories:This involved the engagement of a participant through a rangeof media which promotephysical activity. It includedconsultation, needs assessment,advertising, promotion anddissemination of information on physical activity and healthylifestyles e.g. through schools orcommunity groups. Campaignsand directories took place at 6 LEAP sites.
• Motivational Interviewing:This involved the engagement ofa participant in a series of one toone interviews with a trainedadvisor. These took place in thehealth or community setting andaimed to help the participantdevelop capacity to engage in
physical activity. Motivationalinterviewing took place at 4 LEAP sites.
• Outdoors and Transport:This involved the engagement of a participant in anunstructured or a structuredintervention of physical activityin the outdoors e.g. walking or cycling. Outdoor activitiestook place at 2 LEAP sites.
• Training Leaders and Co-ordinators: This involvedthe engagement of voluntary or paid leaders in a programmeof training, support andeducation who then facilitatethe implementation of physicalactivity interventions forparticipants e.g. training for care workers or staff who workwith the over 50s. Training ofleaders and co-ordinators tookplace at 2 LEAP sites.
2.6 At many sites more than oneintervention was used to helpengage people in physical activityand to increase or maintain theirparticipation levels. For exampleengagement in taster sessions wasused to refer some ‘at risk’participants to an exercise referralscheme and individuals involved in motivational interviewing wenton to take part in LEAP exerciseclasses or outdoor activities.
2.7 Further information on thedifferent types of intervention, the setting in which they tookplace and the priority groupstargeted for each LEAP site areprovided in Appendix A.
‘Get Moving’Nottingham
Learning from LEAP 1009

3.1 In order to determine theeffectiveness of LEAP in bringingabout physical activity change acomprehensive evaluationprogramme was implemented.Data for the evaluation wascollected at a local level using a number of differentmethodologies, then analysed andinterpreted at a national level6.
• Attendance anddemographic data onparticipants was collected using attendance registers, self report tools7 and throughshort questionnaires tailored to particular interventions. This identified how many peopleparticipated in the interventionsand the demographic profile of participants.
• Physical activity data wascollected using self-report tools6
from LEAP participants for atypical week prior to theintervention beginning (baselineactivity) and for a series oftypical weeks during and at the end of the intervention(intervention activity). 1051 datasets were collected. The datawas then used to determinemultiples of resting metabolic
rate values (METS values)8 andthe volume of physical activityfor each participant per week.This enabled both adultparticipants and young peopleto be categorised as:
- Sedentary
- Lightly active
- Moderately active
- Highly active
By comparing participants activitycategories at baseline andintervention the extent of physicalactivity change could bedetermined. A description of theMETS values associated with eachactivity category is provided inAppendix B.
• Qualitative data was collected to supplement the quantitativedata and add depth to theevaluation. Participant views onthe interventions and the impacton their physical activity levelswere collected through focusgroups and semi structuredinterviews during and at the endof interventions. Interventionstaff and partner organisations’views on the interventions, theimpact on participant physical
activity levels and on the designcharacteristics of successfulinterventions were collectedthrough a series of structuredinterviews that were repeated at key points in the LEAPprogramme. Over 380 recorded practitioner interviewstook place.
• Cost data was collected frominterviews with the interventionpersonnel at each LEAP site to establish the costs ofimplementing physical activityinterventions and to enable anassessment of the costeffectiveness of interventions totake place. The data obtainedwas entered onto a spreadsheetand exported for analysis.
• A Community Survey of 4000people at 5 LEAP sites and afurther 800 people at a controlsite was also completed prior tothe interventions in November2003 and towards the end ofthe interventions in November2005. This was undertaken toidentify whether the LEAPinterventions had an impact onthe wider community, inparticular where a communitywide campaign was proposed.
3.2 The overall conclusions thathave been reached about LEAP and the physical activityinterventions implemented arebased on all of the availablesources of data being analysedand reviewed. Overall the LEAPprogramme has provided a robustset of qualitative and quantitativedata. This contributes significantlyto the evidence base currentlyavailable in the United Kingdomrelated to short term physicalactivity behaviour change and the effectiveness of physicalactivity interventions.
3.3 The research findings shouldbe interpreted with the followingpoints in mind:
• The LEAP interventions were for a relatively short period oftime9 and can only demonstrateshort term behaviour change. It is likely that increasedparticipant attrition would have occurred over a longerintervention period10.
• Allowance has not been madefor seasonal variations, whichare known to influenceparticipation rates.
• Small sample sizes in someinterventions limit the ability togeneralise some results11. Whenreporting on the findings in thisreport the sample sizes, shownas (N=) may vary.
• Not all LEAP participants werewilling to be involved in theevaluation or provide data. This may have resulted in underrepresentation of the impact onparticipants from some prioritygroups e.g. black and minorityethnic communities, and fromindividuals classified withinlower physical activity categoriesat baseline.
• Much of the data provided isbased on participants self report.Individuals may over-report their level of physical activity and some have difficulty inaccurately recalling physicalactivity behaviour. In additionsome sites invested time inimproving the accuracy of datacaptured over the interventionlife which made it less likely thata positive intervention effectwould be found12.
• Where interventions weredelivered in a community settingit has not been possible tocontrol for factors that may haveinfluenced behaviour. Factorsbeyond the LEAP interventions,such as individual capacity andthe provision of safe andaccessible opportunities to beactive, also contribute to theintervention effects.
6 The Carnegie Research Institute at Leeds Metropolitan University, withcontributions from MATRIX and MORI, undertook the nationalevaluation for LEAP.
7 These included the International PhysicalActivity Questionnaire (IPAQ) for adults
and adapted versions of the BristolPhysical Activity Diary (Cooper, 2003)and Cale’s Physical Activity Diary (Caleand Harris, 2005) for young people.
8 METS are multiples of resting metabolicrate with one MET equal to a person’srate of energy expenditure when at rest.
To calculate weekly volumes thefollowing equation was used: Frequency(days) x duration (minutes) x intensity(METS threshold). Intensity values wereset at 3.0 METS for moderate intensityactivity and at 6.5 METS for the highlyactive intensity activity, in line with thephysical activity literature.
9 LEAP interventions ran between April2004 and December 2005. Not allinterventions ran for the whole of this period.
10 Buckworth and Dishman 2002demonstrated that as many as 50% of participants who initiated physicalactivity interventions dropped outwithin 6-9 months.
11 All interventions were requested to provide data on attendance,demographics (age, gender, ethnicity,socio-economic status) and physicalactivity levels from all participants atthe start and during the intervention.Only some interventions weresuccessful in collecting such data.Further information is available in the full report available from theDepartment of Health.
12 Some sites invested time in workingwith both participants and researchersto improve the accuracy of datacaptured over the intervention life. This made it less likely that a positiveintervention effect would be foundwhen more accurate (and usuallylower) physical activity levels were selfreported later in the intervention thanhad been recorded at baseline.
3.0 Evaluation Methodology
Learning from LEAP 1211

Who was engaged in LEAP?
4.1 A total of 10,433 participantswere recorded as attending LEAPinterventions. This figure excludesa wider audience who may havebeen exposed to a LEAP physicalactivity campaign or awarenessraising intervention.
4.2 Data from participants of theinterventions indicates that theyattracted a mix of people,including those from the prioritygroups specifically targeted by the LEAP projects:
• Sedentary and lightly activeparticipants (N=2783). 39.9%of participants were sedentaryor lightly active i.e. not meetingthe CMO recommendedguidelines for physical activity at the start of the LEAPinterventions. 60.1% werealready moderately or highlyactive, graph 1 below.
• Age groups (N=4835). TheLEAP interventions attractedboth adults and young people,including a high proportion of older adults 50+. This reflects that a number of theinterventions sought to reacholder adults as a key prioritygroup.
• Gender (N=4835). Amongadults more women than menwere attracted to the physicalactivity interventions, often in a 2:1 ratio. Among youngpeople the male and female split was broadly equal.
• Ethnic group (N=5202). 94%of LEAP participants were whiteBritish participants.
• Social group (N= 2646). Thedata collected on social groups13
was collapsed into four social
groups based on occupation.The largest participant groupwere categorised as professional(54.9%) with the remaindersemi-routine (22%); routine(22%) and students (1.1%).
4.3 The demographic datademonstrates that a broad rangeof different audiences can beattracted to physical activityinterventions, but confirms theneed for a highly targetedapproach if truly hard to reachgroups and people who aresedentary are to be engaged.Whilst it is likely that there is some under representation of theextent to which inactive peopleand other priority groups such aspeople from black and ethnicminority groups did participate in LEAP14 it is clear that physicalactivity interventions, even whentargeted at a particular audience,will still attract and engage a highproportion of people who arealready physically active and fromnon priority groups. If physical activity interventions are to beseen as effective in reaching the
inactive and those at risk ofparticular health conditions, muchgreater attention may need to begiven at the start of interventionsto the engagement mechanismsused.
4.4 Although reaching theinactive and at risk groups is apriority it should be noted that the LEAP interventionsdemonstrated that mixing activeand inactive people has itsbenefits15. The physical activityinterventions helped alreadyactive people to maintain theirphysical activity levels, ensuredthat the interventions were notstigmatised in any way (avoidingthe ‘kids fat camp’ syndrome) andprovided the newly active peoplewith support and role models. It may therefore be both realisticand appropriate for someinterventions to contain a mix of sedentary and already activeparticipants, whilst not takingaway the importance of findingappropriate ways of engaging the priority target audiences.
13 In order to investigate the socio-economicstatus of participants, the ward that theparticipant came from was obtainedthrough their postcode. Using an approachadapted from the Centre for RegionalEconomic & Social Research at SheffieldHallam University. "Census, key statisticsfor postcode sectors” were then used inorder to investigate the occupation thatthe majority of individuals within the ward
undertook. This occupation was recorded as that of the ward, from whichthe participant came and allowed anassumption of the socio-economic class or social grouping of that participant to be made.
14 Intervention managers reported difficultiesin persuading some categories ofparticipants, including people from black
and ethnic minority communities, peoplefrom lower social groups and people whowere sedentary, to provide demographicand activity data for evaluation purposes. It is possible that the numbers attendingfrom those groups is higher than thefigures demonstrate.
15 Qualitative data from interventionmanager interviews.
Did the participants in LEAPinterventions increase theirlevels of physical activity?
4.5 A comparison of the overallMETS values of 1051 participantswho provided both baseline andintervention data showed apositive intervention effect(p<0.001) with a median increaseacross participants of 223METS/week. This equates toapproximately 75 minutes ofadditional brisk walking per week.
The median increase across LEAP participants inphysical activity equated to approximately 75 minutes of additional brisk walking per week.
4.6 Analysis of the activitycategories of participants atbaseline and intervention furtherdemonstrates positive change inphysical activity levels, particularlyamong those who are sedentaryand lightly active. 80.3% of LEAPparticipants who were sedentaryat baseline and 63% of those whowere lightly active at baselinemoved up at least one physicalactivity category.
4.7 Graph 2 below shows thepercentage of participantsclassified in each activity categoryfollowing their involvement inLEAP (intervention) compared toat the start (baseline).
4.8 Column 1 shows that amongthe participants who werecategorised as sedentary at thestart of the LEAP interventions,19.8% remained sedentaryfollowing the intervention, 31.9%became lightly active; 19.8%became moderately active and28.6% became highly active.
4.9 Column 2 demonstrates thatamong those that were lightlyactive 7.4% reduced their activitylevels following the LEAP
intervention and becamesedentary; 29.7% stayed as lightly active; 32.1% becamemoderately active and 30.9%became highly active.
59.9% of participants whowere classified as eithersedentary or lightly active atbaseline achieved the CMOrecommended guideline ofbeing moderately active afterparticipating in LEAP.
4.10 The impact on the physicalactivity levels of participants who were already classified asmoderately or highly active atbaseline is not as strong. Column3 demonstrates that among thosewho were moderately active atbaseline 36.5% increased theiractivity levels, with 35.2%remaining moderately active and28.3% reducing their activitylevels. Among those who werehighly active at baseline, column4, 66.8% remained highly active,with 33.2% reducing their activity levels.
4.11 These findings indicate thatthe relative impact of engagementin a physical activity interventionfor already active participants is
less than for sedentary or lightlyactive participants. The reasonsfor participants reducing theiractivity levels are likely to bevaried16 and were not fullyexplored as part of this study.
4.12 Further evidence of thephysical activity change thatoccurred as a result ofengagement in LEAP wasevidenced by data collected froma larger number of participants17
at baseline (N=2783) and atintervention (N=1521). Thisshowed a median increase of+480 METS/wk, equating toapproximately 160 minutes ofadditional brisk walking per week,and supports the positive trend inincreasing physical activityparticipation.
4.13 Analysis of physical activitychange among the key audienceof people who were sedentary or lightly active at baselinedemonstrated that the extent ofpositive change varied dependingon the demographic profile ofparticipants18.
16 Reductions in physical activity levelsamong participants who were classifiedas moderately or highly active at baselineare likely to have occurred for a numberof reasons such as ill health, work andfamily commitments or may haveoccurred as a result of inaccuracies in selfreporting by participants (under or over
estimating their activity levels at baselineand/or at intervention). This was notexplored in detail for this study.
17 This includes data from participantsprovided at only one point of collectioni.e. only at baseline or only atintervention.
18 Care needs to be taken in utilising thisdata due to small sample sizes for somegroups. Sample sizes are young people178; adults 18-49 years 25; adults 75 and over 25; white British 318; black andethnic minority 56; semi-routine 54;routine 61, professional 126; students 13.
Learning from LEAP
4.0 Key Findings
35
30
25
20
15
10
5
0
sedentary lightly active moderately active highly active
(%)
11.5%
28.4% 28.5%
31.7%
Graph 1: The physical activity category of participants at basesline
sedentary at baseline
19.8%
31.9%
19.8%
28.6%
lightly active at baseline
7.4%
29.7%
32.1%
30.9%
moderately active at baseline
25.4%
35.2%
36.5%
highly active at baseline
10.2%
20.4%
66.8%
Graph 2: Change in activity categories from baseline to intervention
1413
Highly active
Moderately active
Lightly active
Sedentary

Positive change among sedentaryor lightly active people was:
• higher for males (66.3%) thanfor females (55.7%);
• higher for adults aged 18-49years (84%), 50-64 years (70%)and 65-74 years (80%) than forolder adults 75 years and over(48%) or young people (42%);
• higher for black and ethnicminority participants (85.7%)than for white British participants (61.9%); and
• higher for individuals classified as professional (74.6%), routine(79.4%) and students (85.7%)than for those in semi-routineoccupations (50%).
4.14 Care needs to be taken in generalizing from this due to the small sample sizes for somegroups. However the datahighlights the need to considercarefully who interventions aretargeting and how the differingneeds of participants who aresedentary or lightly active can bemet if widespread positive changein physical activity is to take place.
4.15 Overall the physical activitydata demonstrates that physicalactivity interventions can assistindividuals to increase or maintaintheir physical activity levels andthat the greatest effect occursamong adults who are sedentaryor lightly active at the time ofengagement.
The different intervention types
4.16 Taking both quantitative and qualitative data into accountsome observations can be madeon the effectiveness of differentintervention types, although itmust be recognised that sincedelivery was not standardisedvariations in the way they weredesigned and delivered will alsohave contributed to who attendedand physical activity change.
4.17 The conclusions that can be drawn are based on theeffectiveness of interventions in engaging and sustainingparticipation in the short term. The extent to which theinterventions are effective insustaining recommended levels of physical activity participationover longer time frames requiresfurther investigation.
Exercise referral
4.18 The majority of participants in exercise referral interventionswere over the age of 50. Exercisereferral interventions attractedmore women than men althoughhigher rates of positive changewere found for males (81.5%)than for females (55.4%). Thelargest social group amongexercise referral participants was ‘professional’.
4.19 Calculation of the mediandifferences in exercise referralparticipants METS values betweenbaseline and interventiondemonstrated a positiveintervention effect of +405METS/week, equating toapproximately 135 minutes of additional brisk walking per week. (N=460).
4.20 67.6% of participants inexercise referral interventions who were sedentary or lightlyactive at baseline were achievingor exceeding the CMOrecommended levels of physicalactivity at intervention.
4.21 Qualitative data fromparticipants and practitionerssupported the positive effect on physical activity brought about by engagement in exercisereferral schemes. Exercise referralparticipants self reported positivefeelings of physical and mentalwell being as a result of taking part in the intervention.
4.22 Overall the data supports theview that exercise referral is aneffective intervention for initially
engaging and facilitating physicalactivity change in adults and olderadults not meeting the CMOrecommended guidelines forphysical activity.
Classes and groups
4.23 The majority of participants in classes and groups were youngpeople under 18 years of age and 62% were female. Of all theinterventions classes and groupshad the most diverse mix ofdifferent social groups, with thelargest category participants fromthe ‘routine’ social group19.
4.24 Calculation of the mediandifferences in classes and groupsparticipants METS values betweenbaseline and interventiondemonstrated a negativeintervention effect of minus 36.9 METS/week for allparticipants (N=464), although a small positive intervention effect of +30 METS/week, equating toapproximately 10 minutes ofadditional brisk walking per week,was identified when adults wereanalysed separately from youngpeople20 (N=97).
4.25 50.7% of participants inclasses and groups interventionswho were sedentary or lightlyactive at baseline were achievingor exceeding the CMOrecommended levels of physicalactivity at intervention.
4.26 Qualitative data fromparticipants and practitionerssupported the positive effect onphysical activity brought about by engagement in classes andgroups. Participants reported thatthe interventions helped addresstheir barriers to participating inphysical activity including lack ofconfidence and competence, low self efficacy, fear of failure,concerns over appearance and a lack of knowledge of thedifferent types of activity that they could participate in and how to become involved.
The Weight ManagementProgramme (WMP) was designedas a holistic health intervention for obese patients from three GPsurgeries located in areas of socialand economic deprivation in theBorough of Great Yarmouth. The programme consisted of a 12-week combination ofsupervised physical activity,alongside dietetic group supportand behavioural change support.103 people were referred to thescheme and 58% completed the full course. The localevaluation reports encouragingphysiological changes made by those who completed thescheme and positive feedbackfrom participants:
“I feel fitter, healthier, happier and more confident.When I look in the mirror I'mno longer horrified by what I see, but most importantly for me, I no longer feel guiltywhen I eat”
“I felt the need to findsomething else to help memanage my depression andhopefully not to have to rely on medication unlessabsolutely necessary. I wouldencourage everyone to go to the gym, because I have my life back”
“The scheme has given me the tools with which tosuccessfully control my weightand well-being. This will giveme the confidence I lack totackle other issues in my life”
Two measures of change, Body Mass Index and waistcircumference were used tomeasure progress. Thesedemonstrated that average BMI reductions after the first fewmonths were 2.8% whereasaverage waist circumferencereductions were 9.5%. The studyconcluded that obese people who
undertake a lifestyle programmethat includes physical activity mayfind their Body Mass Index doesnot reduce considerably in the firstthree months. For many obesepeople who take up activity frombeing sedentary their muscle massincreases as the muscles have towork hard in moving the totalbody mass during these first fewmonths, which appears to masksthe fact that considerable fat lossis occurring. However waistcircumference does reduceconsiderably over the sameperiod. An effective measure ofsuccess in the early stages of aweight management programme,and one that is more likely tomaintain patients motivation, maytherefore be waist circumference.
For more information contact:[email protected]
19 See paragraph 4.2
20 The majority of participants involved inclasses and groups were young peopleand the data collection process did
encounter some problems withaccurately measuring their physicalactivity levels. This is likely to havecontributed to the overall negativeintervention effect.
Weight Management ProgrammeGreat Yarmouth Primary Care Trust
Learning from LEAP 1615
“I feel fitter, healthier,happier and moreconfident. When I look in the mirror I'm no longerhorrified by what I see, but most importantly for me, I no longer feelguilty when I eat”

One of the larger LEAPinterventions in classes andgroups was the free swimmingintervention for young people in Plymouth. The local evaluationreport, based on questionnairescompleted by 334 young people, states:
“Overall the programme was well received and liked by theyoung people. For many it was a chance to be morephysically active without extracost being involved. As well asincreasing participants selfreported activity levels it hasalso changed their views onphysical activity generally byhelping young people to enjoyphysical activity and makingthem realise that it can be fun.It appears that LEAP has madethe young people more awareof their health and fitnesswhich was reflected in thenumber of participants whothought they were activeenough to stay fit as well assome of the participantschanging their eating habits
as a response to informationthey had received from LEAP.Being part of the freeswimming programme hadmade many of the participantsfeel fitter and healthier as well as increased their selfconfidence. In a nutshell theprogramme has made themajority of the young peoplemore aware of the time theyspend doing physical activitiesas well as encouraging them to enjoy being active. LEAPparticipants’ views about theprogramme are very positive,they like the programme and ithas been instrumental to themas a way of being able toexercise without extra cost."
In North Kirklees motivationalinterviews were used in twointerventions: to increaseparticipation in physical activity by adults and older people withdiabetes and to increaseparticipation in physical activitywith overweight and obese youngpeople. In both interventions themotivational interview wasconducted by a Physical ActivityDevelopment Officer whose key role was to:
• seek to understand theindividual’s frame of referenceusing reflective listening;
• express acceptance andaffirmation;
• reinforce the individual’s selfmotivational statements i.e.problem recognition, concerns,desire and ability to change;
• monitor readiness to change; and
• support the individual’s choicesand their identified changes, as appropriate.
Motivational interviews usuallylasted one hour and were held ina variety of venues across NorthKirklees such as hospitals, leisurefacilities and community venues.The young people were
encouraged to bring aparent/guardian with them, with the adults and older peopleable to bring a partner, friend orcarer. Interviews were offered on a frequency to suit theindividual, however most seemedto have them at the start of theintervention, ten weeks, twentyfive weeks and forty five weeks.Weekly support via a drop inopportunity along with telephonesupport Monday – Friday, 9.00 – 5.00 pm was also offered.
Very positive feedback wasreceived from participants andsignificant changes in behaviourand health shown. One of theadult participants started theintervention overweight and withtype two diabetes, hypertensionand high cholesterol. This clientset goals of reducing weight andincreasing physical activity levels.Within a twelve month period themeasured outcomes werereduced weight, blood pressureand blood glucose levels and theclient self reported being able tobreathe easier, that everyday lifeseemed easier and participation inphysically active five or more timesper week for 30 minutes or more.
“I didn’t feel I could makethese changes but I did! Theinterviews I had with Helenmade me believe I could do itand showed me how. When Iwas down there was someoneto help me. I have met newpeople and now have a newlease of life and I don’t have togo to the doctors as much.”
An obese young person, aged 14, engaged in the programmefor a 12 month period. At the first interview he was at the‘contemplative’ stage of the cycleof change and reported his onlyphysical activity as taking part in school PE twice each week. By interview 4 his activity hadincreased to 7 times per weekincluding joining 3 activitiesoutside of school and the localrugby club. His body fat decreasedfrom 44% to 35% and hishappiness, confidence and fun to be with ratings increased. The young person’s parents alsoreported an increase in his selfesteem/confidence and sociability.At the end of the programme hewas at ‘maintenance’ on the cycle of change.
For further details contact:[email protected]
Free SwimmingPlymouth
Motivational Interviewing North Kirklees
4.27 Overall the data offerscautious support for the positiveeffects of classes and groups inengaging and initially facilitatingphysical activity change amongthose not meeting the CMOrecommended guidelines forphysical activity. Further research is required to enable firmconclusions to be reached.
Motivational Interviewing
4.28 The majority of participants in motivational interviewing wereover 50, with the largest age
group those who were between65-74 years old. More femalesthan males participated and the majority were from the‘professional’ social group. Of allthe interventions motivationalinterviewing had the highestparticipation by people from black and ethnic minorities.
4.29 Calculation of the mediandifferences in participants involvedin motivational interviewing METSvalues between baseline andintervention demonstrated apositive intervention effect of
+360 METS/week, equating toapproximately 120 minutes ofadditional brisk walking per week. (N=77)
4.30 86% of participants involvedin motivational interviewing whowere sedentary or lightly active at baseline were achieving orexceeding the CMOrecommended levels of physicalactivity at intervention.
Learning from LEAP 1817
4.31 Qualitative data fromparticipants and practitionerssupported the positive effect onphysical activity that motivationalinterviewing can have. Participantsreported that motivationalinterviewing helped to providesolutions to their own personalbarriers to participation andbrought improved feelings of well being, increased confidenceand sociability.
4.32 Overall the data supports the view that motivationalinterviewing can be effective at
engaging and initially facilitatingphysical activity change in adults and older adults not meeting theCMO recommended guidelines for physical activity.
Other interventions
4.33 The other intervention typesof peer mentoring, campaigns and directories, outdoors andtransport and training allexperienced difficulties incollecting physical activity data.With a lack of data, or very smallsample sizes, robust conclusions
cannot be drawn on theireffectiveness or otherwise at engaging and initiallyfacilitating physical activitychange. The qualitative data collected did howeverprovide cautious support for all of the different interventionshaving a positive effect.
The local evaluations of the seniorpeer mentoring programme inNottingham concluded that peermentoring programmes supportpeople and bring about behaviourchange. A case study involving a68 year old female participantdemonstrates the positive impactit can have:
“Meeting my Mentor andgoing along with him to thegym turned out to be one ofthe best days of my life. I’d lostconfidence and he made it somuch easier to go along andjoin in. He introduced me to hisfriends at the gym and justgave me the confidence to tryit out. He just made it fun. Ionly needed his help a couple
of times, but since then I’vebeen going along to the gymregularly... Physically I feel likea different person, I’m walkingmore, can carry things betterand can enjoy getting down on the floor and playing withthe grandchildren again... I’mdetermined to keep activenow, and not only that, I’veenrolled myself in the PeerMentor training to become a Mentor myself. I want to be able to help others as I was helped.”
For further information contact:Paul.dodsley@nottinghamcity-pct.nhs.ukwww.getmovingnottingham.nhs.uk
Costs and cost effectiveness of the physical activityinterventions
4.34 The monthly cost ofimplementing the LEAPinterventions varied significantly,with the lowest cost £500 permonth and the highest £9,200 per month. The reasons behindthe variations in cost were notfully explored as part of this study,but the nature and design ofintervention are likely to have had an impact21 .
4.35 The cost per participant ofLEAP interventions ranged from£50 to £3,400 and the cost perparticipant who improved theirphysical activity category rangedfrom £260 to £2,790.
4.36 To determine whether LEAP was a worthwhileinvestment an economic modelwas applied to calculate a cost per ‘quality adjusted life year’gained by participants of the LEAP interventions, as well as any potential future NHS savings.Underpinning the model is theidea that as people become more
physically active the likelihood ofthem experiencing illness such as CHD, stroke, type two diabetesand colon cancer reduces. Thisincreases their life expectancy andtheir quality of life in each yearthat they live. In addition if theyremain healthy then they do notrequire medical treatment and sothere is a potential cost saving tothe NHS.
4.37 The cost per quality adjustedlife year gained from the LEAPinterventions ranged from £50 to £510. This was then comparedto the threshold for investing inmedical interventions impliedfrom decisions made by theNational Institute for Health andClinical Excellence (NICE). Theanalysis revealed that the cost perquality adjusted life year gainedfrom the LEAP interventions issignificantly lower than this£30,000 threshold.
The cost per ‘Quality AdjustedLife Year’ for LEAP wassignificantly below thethreshold for investing inmedical interventions impliedfrom decisions taken by the
National Institute for Healthand Clinical Excellence.
4.38 The future cost savings to the NHS per LEAP participant were compared to the cost perparticipant of implementing LEAP.The analysis demonstrated thatthe savings per participant rangedfrom £770 to £4,900 and for all interventions exceeded thecurrent cost per participant(ranging from £50 to £3,400).
The LEAP interventionsdemonstrated that thepotential cost savings to theNHS exceeded the costs perparticipant of implementingthe intervention.
4.39 These two findings suggestthat the LEAP interventions werecost effective to implement.
21 Based on qualitative data collectedthough interviews with interventionmanagers.
Senior Peer MentoringNottingham City
“Meeting my mentor and going along with him to the gym turned out to be one of the bestdays of my life. I’d lostconfidence and he madeit so much easier to go along and join in.”
Learning from LEAP 2019

5.1 The LEAP evaluationconfirmed that the way thatinterventions are planned,delivered and managed can makea significant difference to theiroverall effectiveness in bothattracting people from prioritygroups and the extent to whichphysical activity change takesplace. Some of the proposed LEAPinterventions did not get beyond aplanning stage or after startingdid not continue due to difficultiesin engaging and meeting theneeds of their target audience orin recruiting and retaining theright staff or volunteers. Othersdemonstrated that positive resultscan be achieved with earlyplanning, a sound understandingof the needs of participants andan inclusive approach.
Design characteristics ofsuccessful physical activityinterventions
5.2 The following designcharacteristics were identified bythe LEAP projects as key factorsthat contributed to their success
in engaging participants andbringing about physical activity change:
• Link the physical activityintervention into localstrategy and existingprogrammes – understand howthe physical activity interventioncan help deliver the key strategicobjectives and targets of localorganisations and agencies andcomplement what is alreadytaking place. This will help toengage partners andparticipants for the interventionand potentially open up accessto other human and financialresources. Explore if a physicalactivity intervention can be‘bolted on’ to existingprogrammes or projects in orderto avoid having to create entirelynew infrastructures that can becostly to set up and maintain.
• Outreach work – undertakeoutreach work with potentialparticipants, communitynetworks and referral partnersbefore the intervention starts.This helps gather information on
participants’ motives, intentionsand barriers to physical activityto inform the planning anddevelopment of interventions. It also helps raise awareness ofthe intervention, buildsrelationships and provides anopportunity for questions to beasked about the interventionbefore anyone commits toattending and means that whena participant attends anintervention for the first time,they already know at least one‘friendly face’.
• Referral protocols – where an intervention receivesreferrals, put a simple referralprotocol in place with only alimited number of stages anddevelop it in conjunction withthe individuals or organisationsthat will be using it. This is mostlikely to result in participantsbeing put forward and helpsminimise refused referrals.
Active Attitude was set-up as asummer holiday programme foryoung people who weresedentary or participated inlimited physical activity. It used arange of fun physical activity andsport opportunities and healthyeating workshops to motivate andenthuse the participants and tobuild self-esteem and self-efficacyfor being active. The project didnot focus or refer to weight loss,though this was a personal goalfor some participants and theirparents. The young people wererecruited through targetedinvitations from school nurses inassociation with school teachersand a paediatric dietician. Theywere offered 10 full days of multi-activities across the summerholidays including: bench-ball,basketball, football, hockey,rounders, street dance,swimming, tennis, horse-ridingand a ‘Walking Bus’. Active day-trips where they were able to trymore adventurous activities suchas canoeing, trampolining or lasergames, as well as a visit to theScience Museum’s Sport ScienceExhibition, helped to inspire theirimagination and interest in sport.
Families of the young people were also invited to attend someevents. Exit routes into communitybased activities were developed by inviting community coachesand workers into the project tooffer taster sessions e.g. throughlinking with the Hastings andRother School Sport Partnership a weekly multi-skills club wasoffered to the young peoplefollowing the summerprogramme. The young peopleand their parents reportedincreased confidence, motivation,self-esteem, enthusiasm andenjoyment for physical activity.
“Generally I’ve started doingmore since I started cominghere…I’ve started watchingtelly less and playing out withmy friends and I walk homefrom school now” Participant
“I really enjoy the games weplay, they listen to what welike doing.” Participant
“It has helped build herconfidence and now she seems a lot happier. She alsoseems motivated to want tolose a bit of weight and she has realistic goals now which I think helps.” Parent
91% of the young people havesince joined new activities andsome reported enjoying andparticipating more in PE at school.Some participants achievedweight loss and reported that theywere bullied less in school. Whilethis was not a project objective itwas viewed as a benefit to thequality of life of the childrenconcerned. The partners in theproject were Hastings and StLeonards PCT, Paediatric Dietician,School Nurses, 5 a Day Project,Hastings Borough Council SportsDevelopment team, ExcellenceCluster, Hastings and RotherSchool Sports Partnership, CentreParcs and Pontins. The partnershipwith the paediatric dieticianparticularly added to the successof the project with families andparents of the participantssuggesting that she addedcredibility to healthy eatinginformation, helped the childrento want to make changes andprovided support to parents.
For further information contact:[email protected]
Learning from LEAP
5.0 Lessons From LEAP
2221
The ‘Active Attitude’ ProjectHastings, St Leonard’s

• A tailored approach – tailorthe programmes provided andthe advice given to meet theneeds of individual participants.This ensures that their specificbarriers and fears can beaddressed and that the exerciseactivity recommended is the one most likely to deliver theirpersonal objectives and fit intotheir lifestyle. Develop clientcentred materials and resourcese.g. information directories,pedometers, activity diaries,matched to the participant’sstate of readiness to engage inphysical activity.
• Join up interventions – ifappropriate connect people intomore than one intervention to
help them get and stay active.For example develop peermentoring alongsidemotivational interviewing so that they receive practicalsupport.
• Use varied, local and familiarlocations for physical activity – Where possible locatethe physical activity interventionin a range of environments thatare local and familiar to thetarget audience. This may beformal locations such as localhealth centres, communitycentres or parks or informallocations such as green spacesor supermarket car parks. Thiscan help reduce barriers toparticipation that might
otherwise arise due to perceiveddifficulties related to access,safety or cost.
• Use trained and skilled staffand volunteers – recruitdedicated and skilled staff andvolunteers that understand theneeds of priority groups they willbe targeting and have the skillsto be able to build positiveworking relationships. Ensureintervention leaders andmentors receive training andeducation in a range ofbehaviour change and physicalactivity topics and have aworking knowledge of the local area and physical activityopportunities. Recognise thatmore than one skill set, or
different specialist knowledge,may be required within physicalactivity interventions and buildup a network of other expertswho can be called upon when required.
• Build capacity – where possiblebuild capacity as part of theintervention. Raise awarenessamong other service providers ofsome of the barriers preventingparticipation and of the supportneeded by new participants.Encourage participants of theinterventions to become futurephysical activity leaders, whethervoluntary or paid, and to act asadvocates for physical activitywith their peers.
• Identify sustainable exitroutes early – actively engageparticipants in shaping their ownsustainable exit routes frominterventions and ensure thatparticipants are givenappropriate information andsupport to enable them to joinmainstream sport and physicalactivity groups andorganisations. Developrelationships with otherprogrammes and organisationsat the start of the intervention tohelp with this process.
Good practice in evaluatingphysical activity interventions
5.3 The LEAP projects alsohighlighted the difficulty thatexists in collecting data from
participants of physical activityinterventions in order to evidencetheir impact. Some participants,often those from the prioritygroups, were not willing to providepersonal information or take partin research and a requirement todo so was in itself a barrier toparticipation. Gaining consent toenable young people to beincluded in research wasproblematic. Participants who didprovide physical activity data onoccasion found it difficult toaccurately recall the frequency andintensity of activity.
The ‘Over 50’s Leisure Weeks’were run by the Cornwall and Islesof Scilly Primary Care Trusts LEAPActive project in partnership withPenwith and Kerrier DistrictCouncils. During the leisureweeks’ a wide range of free tastersessions were offered by activityproviders, sports clubs and leisurecentres including: archery,shooting, tai-chi, walking, pilates,tennis, golf, bowls, sailing, cricketand cycling. These providedparticipants aged 50+ with anopportunity to try a number ofdifferent activities and to find outhow to further their participationoutside of the leisure weeksessions e.g. by joining the club orchanging their lifestyle. The leisureweeks were widely marketedthrough promotional materialsdesigned to appeal to differentaudiences and word quickly
got around in the local communitythat the over 50’s Leisure Weekswere something to be part of. Over 1000 people have nowregistered on the over 50’sdatabase, in excess of 40organisations are involved inproviding activities and more than 700 people participated inactivities held during 2006.Following a celebration evening a steering group was formedconsisting of participants and clubrepresentatives. This group haveplayed a significant role in thesuccess of the latest leisure weeksand in their future developmentand promotion.
For further information contact:Tracey Barter/Lewis Jones,LEAP activators:[email protected].
The ‘Active Choice’ LEAP projectin the Durham Dales was aimed atencouraging inactive youngpeople to become more physicallyactive. It provided alternativephysical activity choices outside ofthose already taking place in aschool or community setting andincluded three main interventions:
• residential summer camps,where young peopleparticipated in adventurous andoutdoor activities such as gorgewalking, raft making, kayakingand assault courses, as well asmusic, drama and dance;
• a school and community activityprogramme, which includedactive games as part of breakfastclubs and circuit sessions outsideof the school day; and
• a physical activity focus group,drawn from young peopleattending the summer campsand other activities, whereparticipants commented onactivities they would like to doand actively participated in arange of different communitybased events includingmountain biking, a communitydisco and the Great North Walk.
The emphasis of the interventionswas on participation, fun, thedevelopment of confidence andself esteem among the youngpeople with the aim of bringingabout behaviour and lifestylechange.
One of the interventions was anextra curricular circuits class foryear 5 and 6 pupils at St Andrew’sprimary school in Bishop Aucklandwhich involved a range of fun,non competitive but structuredactivities using equipment that thechildren were familiar with such asspace hoppers, balls, hoops etc.Some of the children at the schoolhad physical and psychologicalconditions including obesity,diabetes and attention deficithyperactivity disorder. In thecircuit sessions the children wereencouraged to set their ownpersonal exercise goals, to achieveboth at home and at school, andto lead and adapt the activitysessions that took place. The localevaluation of the project identifiedthat both staff and pupils at theschool felt that participation by the young people in the circuit sessions had a number of positive benefits.
“All of the children in thecircuits group have reallyimproved their fitness andhave had loads of funexercising every week. Theirconfidence has improved andtheir health image hasimproved. The benefits ofcircuits are affecting theirwhole life now” Teacher
“Before circuits I wasn’t reallyconfident in taking part insport but now I am” Participant
“I enjoy circuits because I amexercising and having fun atthe same time” Participant
“Before I started circuits Ididn’t really feel fit but nowthat I’ve done it for quite awhile I feel more fit andhealthy” Participant
The circuit programme has raisedthe profile of health and fitnesswithin the school and the classesare continually being adapted anddeveloped to maintain the youngpeople’s interest.
For further information contact:Dave Allen:[email protected]
Over 50’s Leisure WeeksWest of Cornwall
Active Choice Durham Dales
Learning from LEAP 2423

5.4 With respect to the evaluators,sites sometimes under estimatedthe resource required to deliverthe evaluation data or found that without a specialist evaluatoras part of their team they did not have the right evaluationskills. These and a range of otherfactors, set out in the full report,made evidence collectionchallenging.
5.5 In overcoming thesechallenges LEAP has identifiedrecommended approaches andgood practice that can be sharedwith other providers of physicalactivity interventions who maywish to undertake a robustevaluation of impact. Thisincludes:
• Appoint designatedevaluators with the rightskills and experience – appointevaluation specialists, such asuniversities or researchcompanies, or provide staff withappropriate training to enablethem to take on an evaluationrole. Ensure that those who will be responsible for datacollection and evaluation areinvolved in the planning stagefor the intervention, includingselecting the evaluation tools,understand the complexities ofthe project and have sufficienttime allocated within their workprogrammes or contract to fulfil their evaluation role.Where data collection is to beundertaken by project leaders,including volunteers, and/orinput by data processors ensurethat they are also properlytrained and motivated andprovided with ongoing support.
• Understand the barriers toparticipant involvement inresearch – wherever possibleconsult ahead of the projectwith potential participants fromthe priority group that theintervention will be targeting, or with informed individual’sworking with such groups, to try to identify reasons whyparticipants may not want toparticipate or be able toparticipate in an evaluationprogramme. Plan to minimisesuch barriers.
• Adopt simple validation tools – use validation tools thatcan be simply administered andunderstood by participants andpractitioners at a project level.Where appropriate be preparedto adapt tools or use alternativeapproaches to enable data to be collected from users withparticular needs. Adopt a rangeof different collection methods ifrequired. Provide data collectionguidance and protocols to helpwith consistency acrossinterventions and understandingof what is required.
• Obtain specialist advice onethics and obtaining ethicalclearance, if it is required –Seek advice on how evaluationscan be conducted ethicallythroughout the project includingon issues such as participantempowerment and rights, datastorage and export, feedbackand reporting. If ethicalclearance is required build insufficient time into the projectplanning stage to make anapplication and, if there is not inhouse expertise, seek specialistadvice to assist with completingthe application.
• Plan ahead as to howinformed consent will beobtained, if it is required –if young people are to beconsulted then recognise andplan for the difficulties inobtaining informed consent.Build in to project plans the timerequired to gain parentalconsent, including to allow forfollow ups to get consent formsreturned. If research is takingplace within a school dayexplore the possibility of thehead teacher providinginformed consent.
• Build in quality assurancechecks – particularly if physicalactivity data is being collected,undertake quality assurancechecks of the data early in theprocess so that any problems ordifficulties can be addressed inthe way data is being collectedor recorded.
• Maintain regularcommunications – if localinterventions are contributing to a wider evaluation, whetherat a local level or national level,ensure that the evaluators atboth levels engage in frequentdialogue. Regular meetings andtraining sessions, supported bytelephone support, ensure thatevaluators can discuss issues andproblems as they arise and sharepotential ideas and solutions.Dialogue between the overallproject manager or steeringgroup and the evaluator is alsoessential to ensure that the databeing collected will provide theevidence required.
6.1 The Local Exercise ActionPilots research and evaluation has demonstrated thatappropriately designed physicalactivity interventions can attractand engage a broad range ofpeople in physical activity,including people who are notmeeting the CMOrecommendations for physicalactivity and from other at risk or priority groups. Interventionswill also attract people who arealready moderately physicallyactive and who are not frompriority groups. Careful planningprior to the start of theintervention, including outreachwork and the development ofreferral networks, can help ensurethat the right mix of people areengaged in interventions and that the people who will benefitthe most, in particular those who sedentary and lightly active,take part.
6.2 The physical activity data from LEAP confirmed that themajority of participants willmaintain or increase their physicalactivity levels in the short term.The most significant positivechange in physical activity levelswill occur among people who aresedentary or lightly active at thestart of the intervention. Keyfactors that impact on the successof the interventions in bringingabout positive physical activitychange include using local venuesand appropriately trained staffand volunteers, providing tailoredsupport that meets the individualneeds of new participants and the early identification ofsustainable exit routes.
6.3 The LEAP interventions havedemonstrated that physicalactivity interventions can be costeffective. The cost per qualityadjusted life year gained fromphysical activity interventions issignificantly lower than the value for money threshold implied
from NICE recommendations for investing in medicalinterventions. They also offerpotential cost savings to the NHS through reducing thelikelihood that physically activeindividuals will suffer adversehealth states in the future.
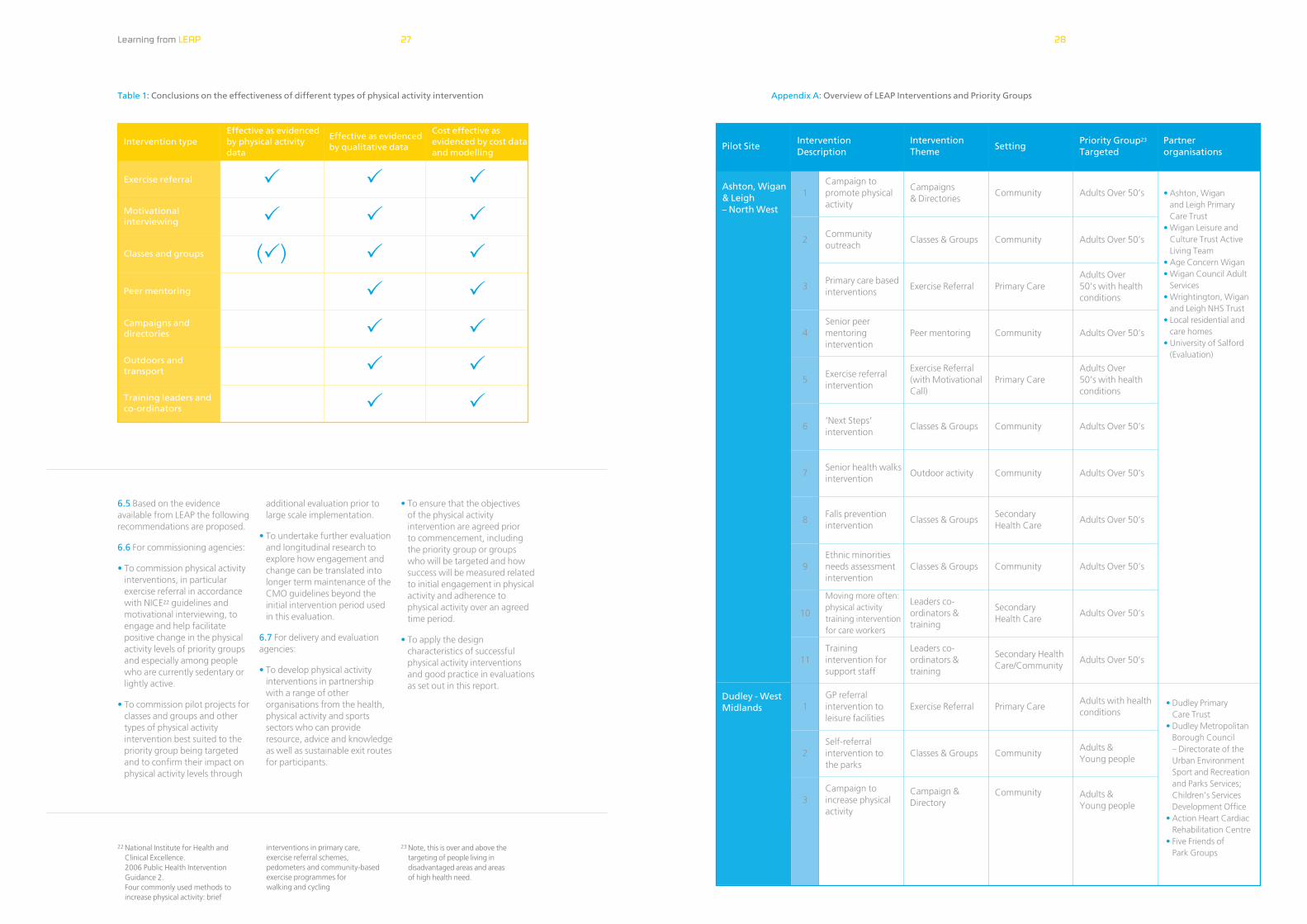
6.4 A range of quantitative andqualitative evidence has beencollected on the different types of physical activity interventionand their effectiveness. Howeverthe lack of substantive physicalactivity data for some interventiontypes has meant it is not possibleto confirm that some of theinterventions are or are noteffective interventions to use and further research is required.Table 1 below summarises theconclusions that can be drawnfrom LEAP by intervention type.
A number of the LEAP projectsencountered difficulties in obtainingdata from participants for evaluationpurposes and so had to find alternativeapproaches to that originally planned.One of the projects faced resistancewhen a male research assistant wantedto collect data from young Asianwomen. As an alternative members ofproject staff known to the womeninvolved were trained to undertakefocus groups. Another project faced
difficulties with getting young peopleto complete activity diaries through alack of willingness on their behalf and in some instances due to literacyproblems. Rather than lose theirexperiences altogether, a researchassistant collected data through a seriesof focus groups and the data collectedwas cross referenced with findings from self report methods in similarpriority groups.
Learning from LEAP
6.0 Conclusion and Recommendations
2625
Exercise referral
1
6.5 Based on the evidenceavailable from LEAP the followingrecommendations are proposed.
6.6 For commissioning agencies:
• To commission physical activityinterventions, in particularexercise referral in accordancewith NICE22 guidelines andmotivational interviewing, toengage and help facilitatepositive change in the physicalactivity levels of priority groupsand especially among peoplewho are currently sedentary orlightly active.
• To commission pilot projects forclasses and groups and othertypes of physical activityintervention best suited to thepriority group being targetedand to confirm their impact onphysical activity levels through
additional evaluation prior tolarge scale implementation.
• To undertake further evaluationand longitudinal research toexplore how engagement andchange can be translated intolonger term maintenance of theCMO guidelines beyond theinitial intervention period used in this evaluation.
6.7 For delivery and evaluationagencies:
• To develop physical activityinterventions in partnership with a range of otherorganisations from the health,physical activity and sportssectors who can provideresource, advice and knowledgeas well as sustainable exit routesfor participants.
• To ensure that the objectives of the physical activityintervention are agreed prior to commencement, includingthe priority group or groups who will be targeted and howsuccess will be measured relatedto initial engagement in physicalactivity and adherence tophysical activity over an agreedtime period.
• To apply the designcharacteristics of successfulphysical activity interventionsand good practice in evaluationsas set out in this report.
Learning from LEAP
Intervention type
Motivationalinterviewing
Classes and groups
Peer mentoring
Campaigns anddirectories
Outdoors andtransport
Training leaders and co-ordinators
P
P
(P)
P
P
P
P
P
P
P
P
P
P
P
P
P
P
Effective as evidenced by physical activitydata
Effective as evidenced by qualitative data
Cost effective asevidenced by cost dataand modelling
Campaign topromote physicalactivity
Campaigns & Directories
Community Adults Over 50’s
Communityoutreach
Classes & Groups Community Adults Over 50’s
Primary care basedinterventions
Exercise Referral Primary CareAdults Over 50’s with healthconditions
Senior peermentoringintervention
Peer mentoring Community Adults Over 50’s
Exercise referralintervention
Exercise Referral(with MotivationalCall)
Primary CareAdults Over 50’s with healthconditions
‘Next Steps’intervention
Classes & Groups Community Adults Over 50’s
Senior health walksintervention
Outdoor activity Community Adults Over 50’s
Falls preventionintervention
Classes & GroupsSecondary Health Care
Adults Over 50’s
Ethnic minoritiesneeds assessmentintervention
Classes & Groups Community Adults Over 50’s
Moving more often:physical activitytraining interventionfor care workers
Leaders co-ordinators &training
Secondary Health Care
Adults Over 50’s
Trainingintervention forsupport staff
Leaders co-ordinators &training
Secondary HealthCare/Community
Adults Over 50’s
GP referralintervention to leisure facilities
Exercise Referral Primary CareAdults with healthconditions
Self-referralintervention to the parks
Classes & Groups CommunityAdults & Young people
Campaign toincrease physicalactivity
Campaign &Directory
Community Adults & Young people
• Ashton, Wigan and Leigh Primary Care Trust
• Wigan Leisure andCulture Trust ActiveLiving Team
• Age Concern Wigan• Wigan Council Adult
Services • Wrightington, Wigan
and Leigh NHS Trust• Local residential and
care homes• University of Salford
(Evaluation)
• Dudley Primary Care Trust
• Dudley MetropolitanBorough Council – Directorate of theUrban EnvironmentSport and Recreationand Parks Services;Children’s ServicesDevelopment Office
• Action Heart CardiacRehabilitation Centre
• Five Friends of Park Groups
Ashton, Wigan & Leigh – North West
Pilot SiteIntervention Description
Intervention Theme
SettingPriority Group23
TargetedPartner organisations
2
3
4
5
6
7
8
9
10
11
1
2
3
Dudley - WestMidlands
22 National Institute for Health and Clinical Excellence. 2006 Public Health Intervention Guidance 2.Four commonly used methods toincrease physical activity: brief
interventions in primary care, exercise referral schemes, pedometers and community-basedexercise programmes for walking and cycling
23 Note, this is over and above thetargeting of people living indisadvantaged areas and areas of high health need.
2827
Appendix A: Overview of LEAP Interventions and Priority GroupsTable 1: Conclusions on the effectiveness of different types of physical activity intervention
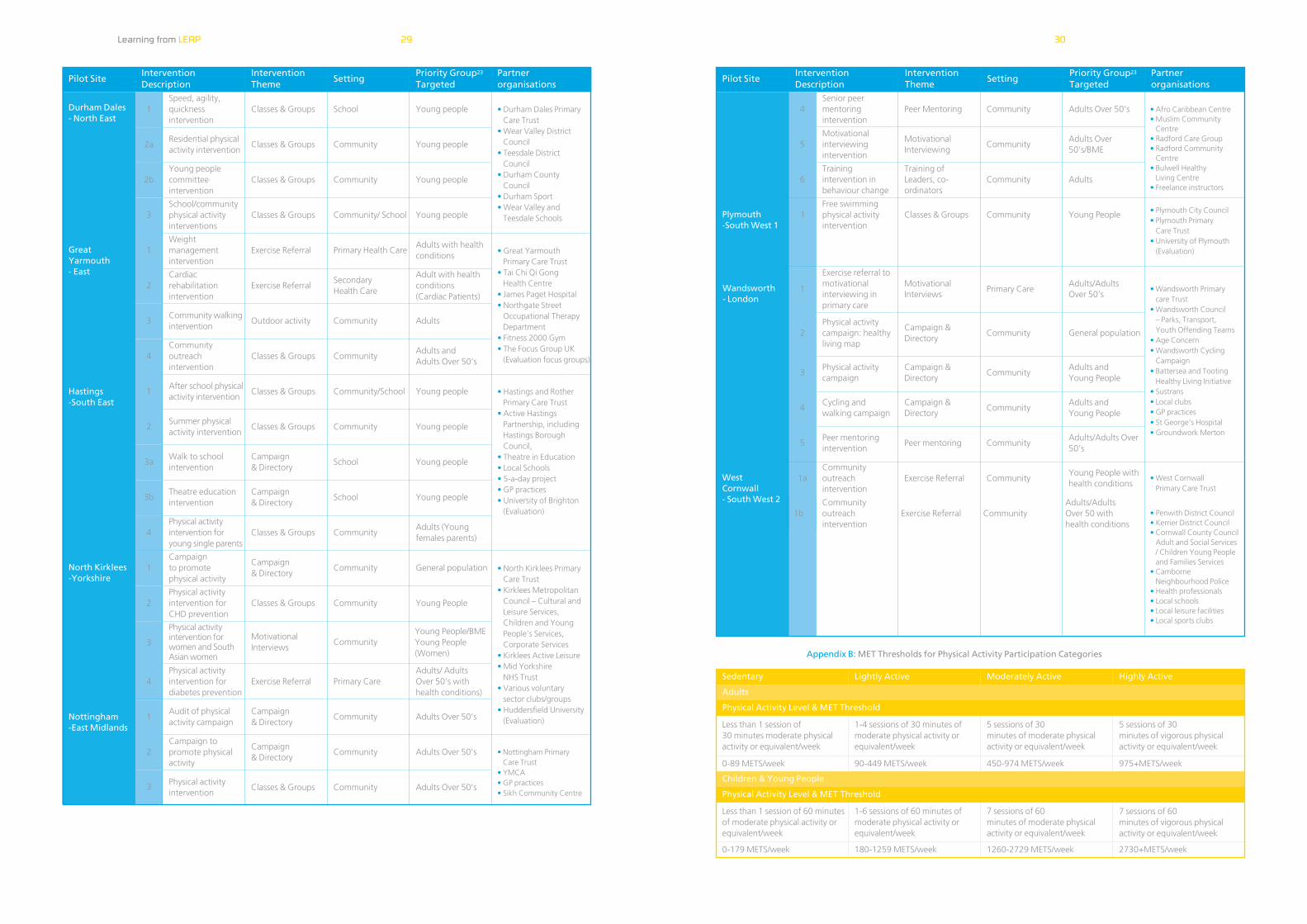
Pilot SiteIntervention Description
Intervention Theme
SettingPriority Group23
TargetedPartner organisations
Pilot SiteIntervention Description
Intervention Theme
SettingPriority Group23
TargetedPartner organisations
Physical activityintervention forwomen and SouthAsian women
MotivationalInterviews
CommunityYoung People/BMEYoung People(Women)
Physical activityintervention fordiabetes prevention
Exercise Referral Primary CareAdults/ Adults Over 50’s withhealth conditions)
Audit of physicalactivity campaign
Campaign & Directory
Community Adults Over 50’s
Campaign topromote physicalactivity
Campaign & Directory
Community Adults Over 50’s
Physical activityintervention
Classes & Groups Community Adults Over 50’s
• Afro Caribbean Centre• Muslim Community
Centre• Radford Care Group• Radford Community
Centre• Bulwell Healthy
Living Centre• Freelance instructors
• Plymouth City Council• Plymouth Primary
Care Trust• University of Plymouth
(Evaluation)
• Wandsworth Primary care Trust
• Wandsworth Council – Parks, Transport,Youth Offending Teams
• Age Concern• Wandsworth Cycling
Campaign• Battersea and Tooting
Healthy Living Initiative• Sustrans• Local clubs• GP practices• St George’s Hospital• Groundwork Merton
• West Cornwall Primary Care Trust
• Penwith District Council• Kerrier District Council• Cornwall County Council
Adult and Social Services/ Children Young Peopleand Families Services
• CamborneNeighbourhood Police
• Health professionals• Local schools• Local leisure facilities• Local sports clubs
1
Less than 1 session of 30 minutes moderate physicalactivity or equivalent/week
1
2
3
Learning from LEAP
Appendix B: MET Thresholds for Physical Activity Participation Categories
1
2a
2b
3
1
2
3
4
1
2
3a
3b
4
1
2
3
4
1
2
3
Speed, agility,quicknessintervention
Classes & Groups School Young people
Residential physicalactivity intervention
Classes & Groups Community Young people
Young peoplecommitteeintervention
Classes & Groups Community Young people
School/communityphysical activityinterventions
Classes & Groups Community/ School Young people
Weightmanagementintervention
Exercise Referral Primary Health CareAdults with healthconditions
Cardiacrehabilitationintervention
Exercise ReferralSecondary Health Care
Adult with healthconditions (Cardiac Patients)
Community walkingintervention
Outdoor activity Community Adults
Communityoutreachintervention
Classes & Groups CommunityAdults and Adults Over 50’s
After school physicalactivity intervention
Classes & Groups Community/School Young people
Summer physicalactivity intervention
Classes & Groups Community Young people
Walk to schoolintervention
Campaign & Directory
School Young people
Theatre educationintervention
Campaign & Directory
School Young people
Physical activityintervention foryoung single parents
Classes & Groups CommunityAdults (Youngfemales parents)
Campaign to promote physical activity
Campaign & Directory
Community General population
Physical activityintervention forCHD prevention
Classes & Groups Community Young People
Durham Dales - North East
GreatYarmouth - East
Senior peermentoringintervention
Peer Mentoring Community Adults Over 50’s
Motivationalinterviewingintervention
MotivationalInterviewing
CommunityAdults Over50’s/BME
Trainingintervention inbehaviour change
Training ofLeaders, co-ordinators
Community Adults
Free swimmingphysical activityintervention
Classes & Groups Community Young People
Exercise referral tomotivationalinterviewing inprimary care
MotivationalInterviews
Primary CareAdults/Adults Over 50’s
Physical activitycampaign: healthyliving map
Campaign &Directory
Community General population
Physical activitycampaign
4Cycling and walking campaign
5Peer mentoringintervention
1aCommunityoutreachintervention
Campaign &Directory
CommunityAdults and Young People
Campaign &Directory
CommunityAdults and Young People
Peer mentoring CommunityAdults/Adults Over50’s
Exercise Referral CommunityYoung People withhealth conditions
1bCommunityoutreachintervention
Exercise Referral CommunityAdults/Adults Over 50 with health conditions
Hastings-South East
North Kirklees-Yorkshire
Nottingham-East Midlands
4
5
6
Plymouth-South West 1
Wandsworth- London
1-4 sessions of 30 minutes ofmoderate physical activity orequivalent/week
5 sessions of 30 minutes of moderate physicalactivity or equivalent/week
5 sessions of 30 minutes of vigorous physicalactivity or equivalent/week
90-449 METS/week 450-974 METS/week 975+METS/week
Adults
Sedentary Lightly Active Moderately Active Highly Active
Less than 1 session of 60 minutesof moderate physical activity orequivalent/week
1-6 sessions of 60 minutes ofmoderate physical activity orequivalent/week
7 sessions of 60 minutes of moderate physicalactivity or equivalent/week
7 sessions of 60 minutes of vigorous physicalactivity or equivalent/week
0-179 METS/week 180-1259 METS/week 1260-2729 METS/week 2730+METS/week
0-89 METS/week
WestCornwall- South West 2
• Durham Dales PrimaryCare Trust
• Wear Valley DistrictCouncil
• Teesdale District Council
• Durham County Council
• Durham Sport• Wear Valley and
Teesdale Schools
• Great Yarmouth Primary Care Trust
• Tai Chi Qi Gong Health Centre
• James Paget Hospital• Northgate Street
Occupational TherapyDepartment
• Fitness 2000 Gym• The Focus Group UK
(Evaluation focus groups)
• Hastings and RotherPrimary Care Trust
• Active HastingsPartnership, includingHastings BoroughCouncil,
• Theatre in Education• Local Schools• 5-a-day project• GP practices• University of Brighton
(Evaluation)
• North Kirklees PrimaryCare Trust
• Kirklees MetropolitanCouncil – Cultural andLeisure Services, Children and YoungPeople’s Services,Corporate Services
• Kirklees Active Leisure• Mid Yorkshire
NHS Trust• Various voluntary
sector clubs/groups• Huddersfield University
(Evaluation)
• Nottingham Primary Care Trust
• YMCA• GP practices• Sikh Community Centre
1
Children & Young People
Physical Activity Level & MET Threshold
Physical Activity Level & MET Threshold
3029
For further information:www.sportengland.org/LEAPwww.naturalengland.org.ukwww.dh.gov.uk
For the full evaluation report:www.dh.gov.uk
Author: Yvonne Barker, Yew Consulting Ltd www.yewconsulting.co.uk
Stock code number SE-0506-015
LEA
PLo
cal E
xerc
ise
Act
ion
Pilo
ts