Embed Size (px)
Citation preview
Learner’s Workbook Module 6
(c) Commonwealth of Australia 2004
ISBN 0 642 82458 4
This work is copyright. You may download, display, print and reproducethis material in unaltered form only (retaining this notice) for yourpersonal, non-commercial use or use within your organisation. Apart fromany use as permitted under the Copyright Act 1968, all other rights arereserved. Requests for further authorisation should be directed to theCommonwealth Copyright Administration, Intellectual Property Branch,Department of Communications, Information Technology and the Arts, GPOBox2154, Canberra ACT 2601 Australia ,or posted athttp://www.dcita.gov.au/cca.
Opinions expressed in this publication are those of the authors and do notnecessarily represent those of the Australian Government Department ofHealth and Ageing.
Publications approval number 3451
Project Outline
This project, an initiative of the National Illicit Drug Strategy, has developedteaching and learning resources to assist frontline workers address the needof young people on issues relating to illicit drugs. They will support a trainingorganisation in the delivery of training. The modules explore work with youngpeople, drug use and suitable intervention approaches.
Project Management
The development of the resources has been managed by:
• New South Wales Technical and Further Education Commission (TAFENSW) through the Community Services, Health, Tourism and HospitalityEducational Services Division
• Drug and Alcohol Office (Western Australia)• The Northern Territory Health Service.
Acknowledgements
The original consultations, writing, practitioner review and revision of thematerials has involved a large number of services including:
Alison Bell ConsultancyCentre for Community Work Training, Association of Children’s WelfareAgencies (NSW)Community and Health Services (Tas)Community Education and Training (ACT)Curtin UniversityDepartment of Community Services (NSW)Department of Juvenile Justice (NSW)Drug and Alcohol Office (WA)Health Department of NSWNational Centre for Education and Training in AddictionsNew England Institute of TAFE, Tamworth CampusNorthern Territory Health ServiceNSW Association for Adolescent HealthTed Noff’s Foundation (NSW)The Gap Youth Centre (NT)Turning Point (Vic)Youth Substance Abuse ServiceYouth Action Policy Association (Vic)
This project was funded and supported by the National Illicit DrugsStrategy through the Australian Government Department of Health andAgeing.
The Materials
The final product, provided for distribution on CD-Rom, consists of:
• a facilitator and learner guide for 12 modules,• a support text for workplace learning.• Overhead transparencies using Microsoft PowerPoint for each module to
support facilitators who choose face-to-face delivery.
Each document has been provided in
• Acrobat (pdf) format to ensure stability• A Microsoft Word version to enable organisations to amend, add and
customise for local needs
The primary user would be a facilitator/trainer/training organisation thatwould distribute the learning materials to the learners. They can be used intraditional face to face or through a supported distance mode.
Materials have been prepared to allow direct colour laser printing orphotocopying depending on the size and resources of the organisation. It isnot envisaged that learners would be asked to print materials.
Assessment
Where assessment of competence is implemented training organisations arereminded of the basis principles upon which assessment should be based:
Assessment is an integral part of learning. Participants, throughassessment, learn what constitutes effective practice.
Assessment must be reliable, flexible, fair and valid.
• To be reliable, the assessment methods and procedures must ensurethat the units of competence are applied consistently.
• To be flexible, assessment should be able to take place on-the-job, off-the-job or in a combination of both. They should be suitable for a varietyof learning pathways including work-based learning and classroombased learning.
• To be fair, the assessment must not disadvantage particular learners• To be valid, the assessment has to assess what it claims to assess.
2Learner’s Workbook – Section A
Contents
Background .....................................................................................3
Target occupational groups .............................................................3
Approaches to service delivery........................................................4
Project resources ............................................................................7
Developing your learning plan .......................................................12
Using the Learner Workbook.........................................................13
Information for distance and work-based learners – yourfacilitator’s role ..............................................................................14
3Learner’s Workbook – Section A
Training Frontline Workers:Young People, Alcohol
and Other Drugs
Background
The project Training Frontline Workers – Young People,Alcohol and Other Drugs is part of a broad strategy tosupport the educational and training needs of frontline workers.The training and support needs of frontline workers notdesignated as alcohol and other drug workers to enable themto work confidently with young people on illicit drugs is wellrecognised. This project attempts to meet this need. It wasfunded by the Australian Government Department of Healthand Ageing under the National Illicit Drug Strategy (NIDS).
Target occupational groups
This training resource has been developed specifically for thefollowing groups of frontline workers:
• Youth Workers• Accommodation and crisis workers• Counsellors (including school based)• Primary and community health and welfare workers• Juvenile justice workers• Teachers• Police
4Learner’s Workbook – Section A
Approaches to service delivery
The development of the resources brings together twoapproaches to service delivery:
• work with young people
• alcohol and other drug work
The two approaches which underpin these resources aresummarised as follows:
Working with young people
A systems approach is the most appropriate model tounderstand and work with young people. A systems approachassumes that no aspect of behaviour occurs in isolation,rather it occurs within a wider context. In other words, tounderstand young people we need to consider the individual,their family, the wider community and society as a whole aswell as how they interact with each other.
The systemic youth-focused approach assumes that:
• Young people deal with challenges in ways similar toother people in society (some well, others not so well).Young people develop their coping strategies and skills bylearning from others around them, through their ownpersonalities and through trial and error.
• The term ‘youth’ is a social construction. Societal valuesand beliefs about young people determine the way inwhich they are treated within society (for example, youngpeople are viewed differently in different cultures).
• Young people are not a homogenous group. Althoughyoung people share some common developmental issues,their backgrounds, experiences and cultures are asdiverse as the rest of the population.
• Young people participate actively in their lives, makechoices, interact with others, initiate changes andparticipate in our society. They are not passive victims ofa dysfunctional society, family or peer group.
5Learner’s Workbook – Section A
The following social justice principles guide work withyoung people:
• Access - equality of access to goods and services
• Equity - overcoming unfairness caused byunequal access to economic resourcesand power
• Rights - equal effective legal, industrial andpolitical rights
• Participation - expanded opportunities for realparticipation in the decisions whichgovern their lives.
6Learner’s Workbook – Section A
Alcohol and other drug work
Harm minimisation is the most appropriate approach forworking with alcohol and illicit drug issues. The goal of harmminimisation is to reduce the harmful effects of drugs onindividuals and on society. Harm minimisation assumes thatwhile we cannot stop drug use in society, we can aim toreduce the harm related to using drugs. Harm minimisationhas three components: harm reduction, supply reduction anddemand reduction.
A variety of drugs, both legal and illegal, are used in society.There are different patterns of use for drugs and not all druguse is problematical.
Large proportions of young people try alcohol or other drugs,including illicit drugs, without becoming regular or problemdrug users.
Drug use is a complex behaviour. Interventions that try todeal with single-risk factors or single-risk behaviours areineffective.
Drug use represents functional behaviour for both youngpeople and adults. This means that drug use can best beunderstood in the broader context of the lives of the youngpeople using them. Any interventions need to take thebroader context into account.
Training approach
These training resources are based on the followingprinciples:
• Training is consistent, supports a national qualificationand provides a pathway to a qualification.
• Training is based on adult learning principles. It should:− build on learners’ existing knowledge, skills and
experience− utilise problem-based learning and skills practice, and− develop critical thinking and reflection.
• Training is to be flexible and available through a variety ofmethods. Examples include workshops, self-directedlearning, distance learning supported by a mentor/facilitator and work-based learning.
7Learner’s Workbook – Section A
• Work-based learning provides participants with theopportunity to reflect on current work practices, apply theirlearning to the work situation and to identify opportunitiesfor organisational change and development in theirworkplaces.
• A key learning strategy of the resources, supported byindividual, group and work-based activities, is reflection:alone and with peers and supervision. To reflect upon andevaluate one’s own work, the types of intervention usedand the assumptions they are based on is crucial toworking more effectively.
Project resources
The Young People, Alcohol and Other Drugs programaims to provide the core skills and knowledge that frontlineworkers need to respond to the needs of young people withalcohol and drug issues, particularly illicit drugs.
This training resource, which comprises 12 modules, hasbeen developed to provide a qualification and/or specific unitsof competence. The resource can also be used as a test orreference document to support the development of a specificknowledge or skill.
Each module (except Module 1) comprises a LearnerWorkbook and a Facilitator Guide. Each Learner Workbook isa self-contained resource that can be used for both distanceand work-based learning or to support face-to-face learning(including workshops).
Relationship to the Community Services TrainingPackage (CHC02)
The training modules were initially developed to support fourunits of competence from the Community Services TrainingPackage (CHC99). These were:
CHCYTH1A Work effectively with young people
CHCAOD2A Orientation to the alcohol and otherdrugs sector
CHCAOD5A Provide support services to clientswith alcohol and other drugs issues
CHCAOD6A Work with clients who areintoxicated.

8Learner’s Workbook – Section A
Following the release of the revised Community ServicesTraining Package (CHC02) in April 2003, the modules wererevised to support the following units of competence from therevised Training Package:
Unit ofCompetence Module
CHCYTH1CWork effectively withyoung people
• Perspectives on Working withYoung People
• Young People, Risk and Resilience• Working with Young People
CHCAOD2BOrientation to thealcohol and otherdrugs sector
• Young People, Society and AOD• How Drugs Work• Frameworks for AOD Work
CHCCS9AProvide supportservices to clients
• Helping Young People Identify theirNeeds
• Working with Young People onAOD Issues
• Working with Families, Peers andCommunities
• Young People and Drugs – Issuesfor Workers
CHCAOD6BWork with clientswho are intoxicated
• Working with Intoxicated YoungPeople
The twelfth module Planning for Learning at Work is designedto support participants in their learning.
The four units of competence listed above contribute to nationalqualifications in both Youth Work and Alcohol and Other DrugWork and are electives in a range of other qualifications. Sincethese units by themselves will not deliver a qualification, theadditional units listed in the Community Services TrainingPackage Qualification Framework would need to be completed.
To achieve any of the above units a learner must complete all themodules comprising that unit and be assessed by a qualifiedassessor from a registered Training Organisation. While it ispossible to complete individual modules, this will not enable youto achieve a unit of competence. Individual modules willcontribute towards gaining the unit of competence and over aperiod of time all modules needed for the unit could be completed.

9Learner’s Workbook – Section A
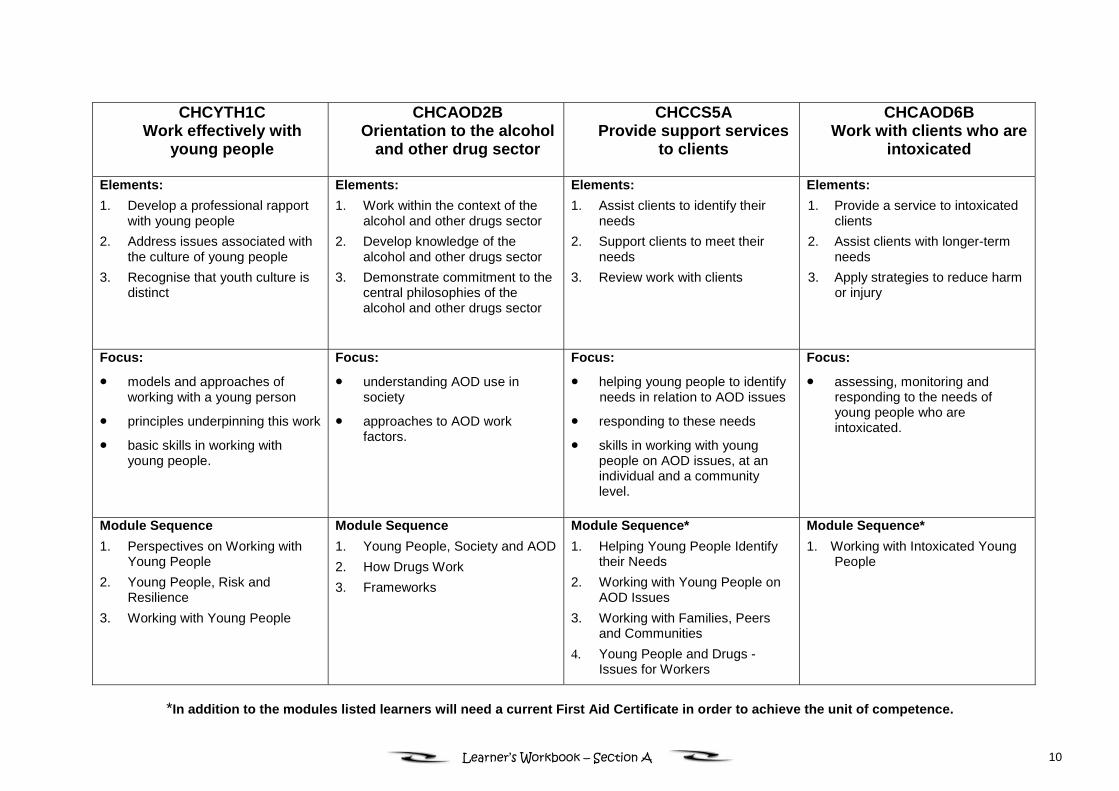
Each of the units of competence has a different focus andhas been customised within national guidelines to meet theneeds of frontline workers in working with young people withillicit drug issues. The modules each provide a learningpathway with stated learning outcomes to help achieve eachparticular unit of competence.
Since the modules associated with each unit of competenceprogressively build on each other, they can be delivered andassessed in an integrated manner. This provides learnerswith a ‘total view’ of the essential theory and required skillsfor their work roles.
10Learner’s Workbook – Section A
CHCYTH1CWork effectively with
young people
CHCAOD2BOrientation to the alcohol
and other drug sector
CHCCS5AProvide support services
to clients
CHCAOD6BWork with clients who are
intoxicated
Elements:1. Develop a professional rapport
with young people2. Address issues associated with
the culture of young people3. Recognise that youth culture is
distinct
Elements:1. Work within the context of the
alcohol and other drugs sector2. Develop knowledge of the
alcohol and other drugs sector3. Demonstrate commitment to the
central philosophies of thealcohol and other drugs sector
Elements:1. Assist clients to identify their
needs2. Support clients to meet their
needs3. Review work with clients
Elements:1. Provide a service to intoxicated
clients2. Assist clients with longer-term
needs3. Apply strategies to reduce harm
or injury
Focus:
• models and approaches ofworking with a young person
• principles underpinning this work
• basic skills in working withyoung people.
Focus:
• understanding AOD use insociety
• approaches to AOD workfactors.
Focus:
• helping young people to identifyneeds in relation to AOD issues
• responding to these needs
• skills in working with youngpeople on AOD issues, at anindividual and a communitylevel.
Focus:
• assessing, monitoring andresponding to the needs ofyoung people who areintoxicated.
Module Sequence1. Perspectives on Working with
Young People2. Young People, Risk and
Resilience3. Working with Young People
Module Sequence1. Young People, Society and AOD2. How Drugs Work3. Frameworks
Module Sequence*1. Helping Young People Identify
their Needs2. Working with Young People on
AOD Issues3. Working with Families, Peers
and Communities4. Young People and Drugs -
Issues for Workers
Module Sequence*1. Working with Intoxicated Young
People
*In addition to the modules listed learners will need a current First Aid Certificate in order to achieve the unit of competence.
11Learner’s Workbook – Section A
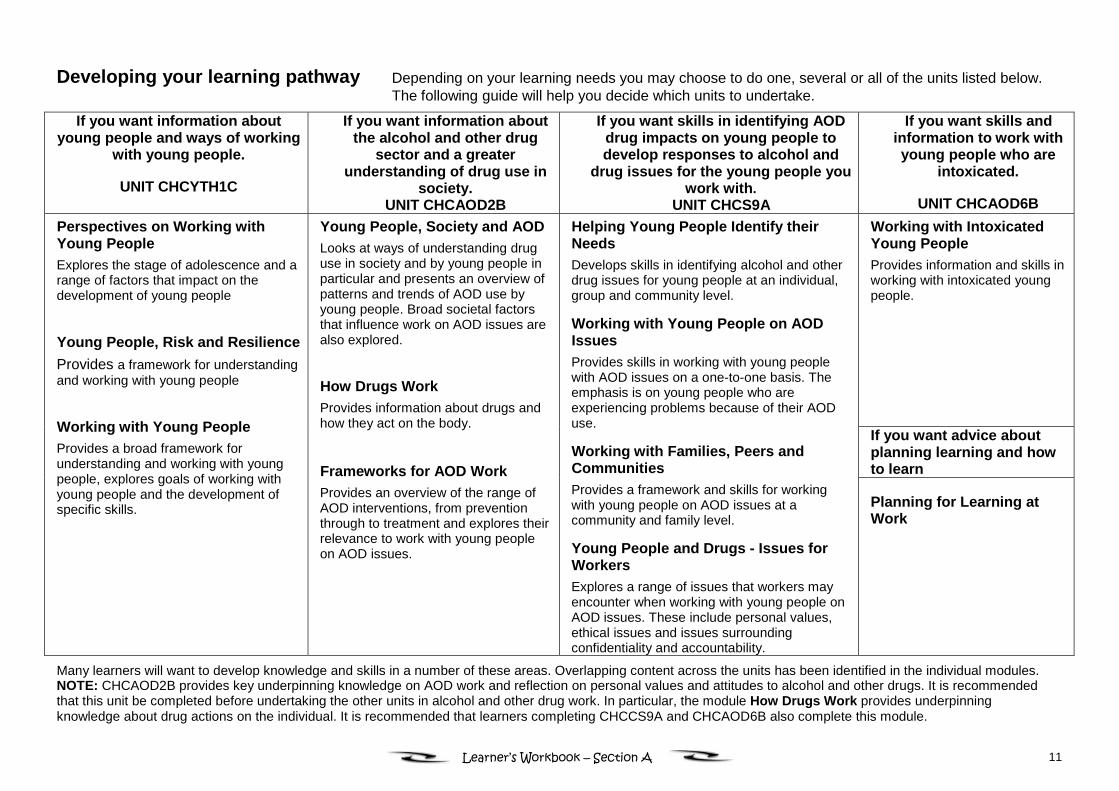
Developing your learning pathway Depending on your learning needs you may choose to do one, several or all of the units listed below.The following guide will help you decide which units to undertake.
If you want information aboutyoung people and ways of working
with young people.
UNIT CHCYTH1C
If you want information aboutthe alcohol and other drug
sector and a greaterunderstanding of drug use in
society.UNIT CHCAOD2B
If you want skills in identifying AODdrug impacts on young people todevelop responses to alcohol and
drug issues for the young people youwork with.
UNIT CHCS9A
If you want skills andinformation to work withyoung people who are
intoxicated.
UNIT CHCAOD6BWorking with IntoxicatedYoung PeopleProvides information and skills inworking with intoxicated youngpeople.
If you want advice aboutplanning learning and howto learn
Perspectives on Working withYoung PeopleExplores the stage of adolescence and arange of factors that impact on thedevelopment of young people
Young People, Risk and ResilienceProvides a framework for understandingand working with young people
Working with Young PeopleProvides a broad framework forunderstanding and working with youngpeople, explores goals of working withyoung people and the development ofspecific skills.
Young People, Society and AODLooks at ways of understanding druguse in society and by young people inparticular and presents an overview ofpatterns and trends of AOD use byyoung people. Broad societal factorsthat influence work on AOD issues arealso explored.
How Drugs WorkProvides information about drugs andhow they act on the body.
Frameworks for AOD WorkProvides an overview of the range ofAOD interventions, from preventionthrough to treatment and explores theirrelevance to work with young peopleon AOD issues.
Helping Young People Identify theirNeedsDevelops skills in identifying alcohol and otherdrug issues for young people at an individual,group and community level.
Working with Young People on AODIssuesProvides skills in working with young peoplewith AOD issues on a one-to-one basis. Theemphasis is on young people who areexperiencing problems because of their AODuse.
Working with Families, Peers andCommunitiesProvides a framework and skills for workingwith young people on AOD issues at acommunity and family level.
Young People and Drugs - Issues forWorkersExplores a range of issues that workers mayencounter when working with young people onAOD issues. These include personal values,ethical issues and issues surroundingconfidentiality and accountability.
Planning for Learning atWork
Many learners will want to develop knowledge and skills in a number of these areas. Overlapping content across the units has been identified in the individual modules.NOTE: CHCAOD2B provides key underpinning knowledge on AOD work and reflection on personal values and attitudes to alcohol and other drugs. It is recommendedthat this unit be completed before undertaking the other units in alcohol and other drug work. In particular, the module How Drugs Work provides underpinningknowledge about drug actions on the individual. It is recommended that learners completing CHCCS9A and CHCAOD6B also complete this module.
12Learner’s Workbook – Section A
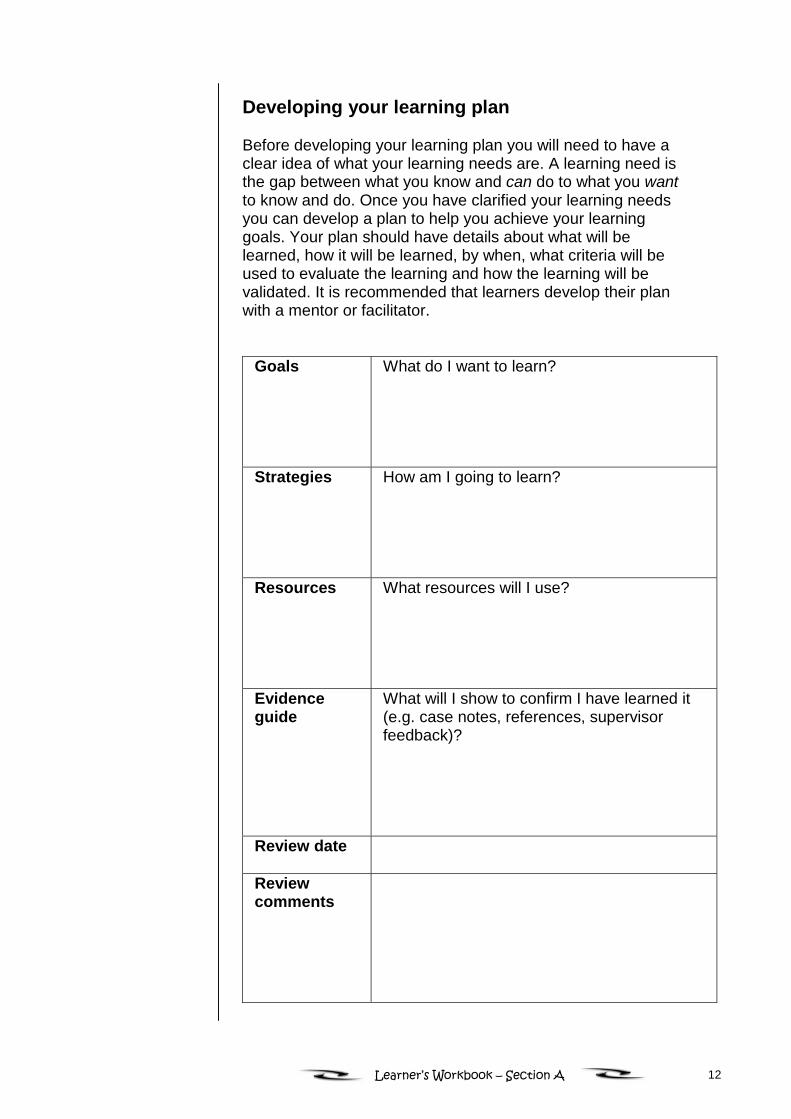
Developing your learning plan
Before developing your learning plan you will need to have aclear idea of what your learning needs are. A learning need isthe gap between what you know and can do to what you wantto know and do. Once you have clarified your learning needsyou can develop a plan to help you achieve your learninggoals. Your plan should have details about what will belearned, how it will be learned, by when, what criteria will beused to evaluate the learning and how the learning will bevalidated. It is recommended that learners develop their planwith a mentor or facilitator.
Goals What do I want to learn?
Strategies How am I going to learn?
Resources What resources will I use?
Evidenceguide
What will I show to confirm I have learned it(e.g. case notes, references, supervisorfeedback)?
Review date
Reviewcomments
13Learner’s Workbook – Section A
The module Planning for Learning at Work providesdetailed information on identifying your learning needs,developing a learning plan and strategies that will assist youto learn.
Once you have identified your needs you can match them upwith the units of competence and the resources available.
Assessment
If part of your learning plan is to achieve particular units ofcompetence you will need to clarify how you will be assessedand by whom. Your facilitator will provide you with informationon assessment activities and requirements.
Recognition
If you think that you already have skills and knowledge thatare contained in a particular module, you may be eligible toapply for recognition of prior learning. You will need todiscuss this with your facilitator who will inform you of thenecessary requirements.
Using the Learner Workbook
The Learner Workbook is a comprehensive, workbook-styledocument. It can be used for distance and work-basedlearning modes as well as supporting face-to-face learning.
The Learner Workbook provides an overview of the moduleand the learning outcomes which will help you to plan andguide your learning. The content is divided into topic areasproviding information for you to read, topics for research,activities that can be completed alone, in groups or in yourworkplace. A glossary and a list of references and resourcesare also provided in each module.
14Learner’s Workbook – Section A
Information for distance and work-basedlearners – your facilitator’s role
It is recommended that these resources be used in supporteddistance mode. This means that learning occurs outside of aclassroom workshop setting with the support and guidance ofa qualified facilitator. If you are a distance learner it isimportant for you to clarify your learning needs and what youhope to achieve with your facilitator. This person will help youidentify your needs, develop goals, match your needs to theunits of competence and the relevant modules and developyour learning plan. Your facilitator will clarify how you will beassessed and by whom and will contact you at prearrangedtimes to assist and support you as you complete theWorkbook.
As a distance learner much of your learning is self-directed.This means that you are responsible for setting your ownlearning goals and organising your learning so that youachieve these goals. The module Planning for Learning atWork is a good resource for distance learners. As well ashelping you to develop a learning plan, it provides a range ofstrategies to assist you with self-directed and work-basedlearning as well as helping you to identify how you learn best.
Managing your learning
Your Workbook contains a range of learning activities. Theseactivities involve self-assessment and will assist you in yourlearning and your preparation for formal assessment.
The following study links will assist you in managing yourlearning:
• Managing time − You will need to plan time to undertakeyour learning. This may be a regular time each week oryou may prefer to do blocks of learning.
• Managing activities − The Workbook contains a rangeof activities some of which will require you to have accessto a phone and a computer and sources of data in theworkplace.
• Managing your learning materials − Organise yourmaterials so that you can easily keep track of theresources you need.

15Learner’s Workbook – Section A
• People who can help you learn − Remember that arange of people can help you with your learning includingyour facilitator, your supervisor, work colleagues and yourpeers. These people can provide support, assistance andinformation and assist you in completing activities such asrole plays.
16Learner’s Workbook – Section A
Icons
A range of icons is used in the Learner Guide to assist you inusing the resources. The following icons are used:
Facilitator direction
Workplace learning activity
Case study
Task
Writing exercise
Group activity
Links to other modules
Web resources
Video
Question
Answer
A good point for student to contact facilitator
Brainstorm
Suggested time
Overhead transparency
2
Contents
Topic 1 Introduction...................................................................3
Topic 2 Introduction to how drugs work.....................................5
Topic 3 Classifying drugs ........................................................15
Topic 4 How psycho-active drugs act on the body ..................22
Topic 5 How drugs move through the body.............................26
Topic 6 Drug effects ................................................................31
Topic 7 Effects of specific psycho-active drugs.......................36
Topic 8 Key issues in pharmacology .......................................42
Topic 9 Managing overdose ....................................................55
Topic 10 Management of withdrawal.........................................65
Topic 11 Reducing drug-related harm .......................................73
Topic 12 Summary and conclusion ...........................................84
References ...................................................................................87
Key terms ...................................................................................89
3
Topic 1
Introduction
Overview
In this module you will learn about key issues inpharmacology. You will explore how mind-alteringdrugs affect young people and how to apply thisknowledge to achieve an effective working relationshipwith them.
1.2 Learning outcomesWhen you have completed this module you should beable to:
Classify common psycho-active drugsaccording to their effect on the central nervoussystem (CNS)
Outline the major short and long-term effectsof psycho-active drugs
Discuss key issues in pharmacology such astolerance, withdrawal, overdose, dependenceand interaction
Describe the harmful effects on young peopleresulting from AOD use.
It is suggested that you remind yourself of theselearning outcomes as you work through the module.At different stages ask yourself whether you think youhave achieved each of the learning outcomes. Thiswill help you keep track of your progress, and whatyou still need to learn to successfully complete themodule.
4
1.3 Assessment events
Your facilitator will provide you with information on anyassessment activities you might be required to undertake. If youare not provided with assessment information when youcommence this module, make sure you ask your facilitator ifthere are any assessment requirements for module completion.
5
Topic 2
Introduction tohow drugs work
2.1 What ispharmacology?
Pharmacology is a branch of science that deals withthe study of drugs and their actions on living systems −that is, the study of how drugs work in the body(sometimes referred to as ‘drug actions’). Tounderstand this we need to consider what a drug is,how it affects our physical, emotional andpsychological wellbeing, the type of drug being used,the modes of administration, how the drug is absorbedand the characteristics of the person taking the drug.
This module will focus on psycho-pharmacology whichconcerns the action of mind-altering or psycho-activedrugs. Psycho-active drugs are substances that altermood, thoughts or behaviour as a result of changes inthe functioning of the brain. In this module, the term‘drug’ will be used to include all psycho-active drugsincluding alcohol and other psycho-active substances(e.g. petrol).
Common examples of psycho-active drugs includealcohol, nicotine and cannabis.
What ispharmacology?
Why is pharmacologyimportant?
The limitations ofpharmacologicalknowledge
Finding moreinformation abouthow drugs work?
Adhikari, P, & Summerill, A (2000)
6
Give three examples of psycho-active drugs and threeexamples of non-psychoactive drugs. (Hint: Think aboutmedication that affects parts of the body other than the brain.)
Psycho-active drug Non-psycho-active drug
1.
2.
3.
1.
2.
3.

7
2.2 Why is pharmacologyimportant?
Since alcohol and other drug (AOD) use is a part of youthculture, it is important to understand how drugs work if you workwith young people.
Case studies
William is a 19-year-old student at a TAFE college. He wasdriving home the morning after a Bachelor and Spinster’s Ball,where he drank about 12 cans of beer. When he arrived back intown, 50km away, he was tested by police with a random breathtesting unit. His blood alcohol reading was 0.09 percent,although he had slept in his car for eight hours before drivinghome.
Uma, 15, was arrested for stealing a handbag. Twelve hoursafter her arrest, while still in custody, she begins to shiver andcomplains of feeling sick.
Matthew is a 16-year-old Aboriginal boy attending school nearBroome in Western Australia. His teacher has noticed a rapiddeterioration in the quality of his school work. His memory ismuch worse than it used to be and he often complains ofheadaches.
Emily, 17, is a regular resident of an accommodation service foryoung people in the inner city. Following a six-week break fromheroin while on a rehabilitation program, she returned to therefuge, and that evening used heroin. She collapsed outside thehouse and was taken by ambulance to hospital.
Kayla, 18, is a student at university. She lives with a couple ofother friends in the city. Last week she went out with her friendsfor lunch and drove her car to the pub where they had a countermeal. On the way home she was involved in a minor car crashas she failed to give way at an intersection. When the policeattended the scene Kayla was pale, shaking, with slurredspeech and disorientated.
8
Do you think all the young people in the casestudies are experiencing AOD-related problems?
(Write your answer here, then check the answers on the nextpage.)
9
Your initial impression might lead you to guess that all theyoung people in the above case studies were under theinfluence of AOD which led to some problems. In fact, Kaylawas the one exception to the rule. Her presentation after theaccident seems to be consistent with being substance-affected.However, Kayla suffers from diabetes and had consumed toomuch sugar at lunch time.
While it is important to recognise the effects of drug use onyoung people’s behaviour, it is also important NOT to ASSUMEthat they are under the influence of a drug without gathering allthe facts first.
(Answer the following questions, then check the possible answers onthe next page.)
How do you think some knowledge of how drugswork could assist a police officer, teacher oryouth worker to help young people like William,Uma, Matthew, Emily or Kayla?
How might one of these young people experiencemore harm from their drug use if the staff and/orpolice working with them had no suchknowledge?
10
An understanding of how drugs can affect a young personis important to know so that workers can:
• provide accurate information to young people andparents who want to know more about drugs and druguse
• build a better rapport and have more confidencewhen dealing with young people who use alcohol andother drugs
• develop a better understanding of factors influencingthe young person
• take appropriate action in critical situations thatmay save a young person’s life or reduce risk of harm.
• provide emergency service workers with accurateinformation about the state of a young person shouldmedical care be required (e.g. Ambulance Officer or000 Operator)
• meet their obligations in regard to duty of care toyoung people
• provide a safe and healthy work environment andmeet Occupational Health and Safety legislationrequirements.
11
2.3 The limitations ofpharmacological
knowledge
Pharmacists are very knowledgeable about drug actions, butthey might not be able to understand drug use in young people.This is because understanding youth drug use requires muchmore than technical knowledge.
What other knowledge and skills might assist youto understand and work with young AOD users?
(Write your answer here, then check the possible answerson the next page.)
12
Possible answers include:
Knowledge of pharmacology is useful when dealing withyoung people. However, this needs to be supplementedby:
• knowledge of the developmental processes that occur
during adolescence
• skills in communicating with young people
• alcohol and other drug intervention skills andknowledge
• an understanding of the social context of drug use,such as the influence of peers etc
• an understanding of street terms and slang languageassociated with young people and AOD use.
13
2.4 Finding moreinformation about
how drugs work?
You can find more information about how drugs work from:
• Posters• Brochures• Books, journals and other publications• Internet sites such as:
− www.mentalhealth.com− www.ceida.net.au− www.connexions.com.au− www.ndarc.com.au− www.adin.com.au− www.adf.org.au− www.health.usyd.edu.au− www.druginfo.nsw.gov.au
• Clients and personal experience• Colleagues• Libraries• Hospitals and other health services• Young people• Youth centres and youth services• Schools, TAFE colleges and universities.
This list is not exhaustive. Find out which agency/ies inyour local area provide information about how drugs work.
14
• Pharmacology is the study of how drugs work in the body.
• Psycho-active drugs commonly affect a person’s mood,behaviour or thinking ability and act upon the brain.
• Other drugs that are purely medicinal do not have apsycho-active effect (e.g. cholesterol loweringmedication).
• Young people are the largest consumers of drugs in ourcommunity so it is necessary for frontline workers tounderstand how drugs work.
15
Topic 3
Classifying drugs
3.1 Classifying drugsby their effect on
the centralnervous system
Drugs can be classified in many ways. For example,they can be classified according to:
• uses (medicinal or recreational)• effect on the body (the specific effect on the central
nervous system)• source of the substance (synthetic or plant)• legal status (legal/illegal)• risk status (dangerous/safe).
One of the most common and useful ways ofclassifying a drug is by the effect that it has on aperson’s central nervous system. The brain is themajor part of the central nervous system, and this iswhere psycho-active drugs have their main effect.
The following table summarises the majorclassifications of drugs including stimulants,depressants and hallucinogens. The group ‘others’includes those psycho-active drugs that do not fitneatly in any other category. Some drugs can beclassified in a number of categories, e.g. cannabis andecstasy.
Classifying drugs bytheir effect on thecentral nervoussystem
Names of drugs
The legality of drugs
16
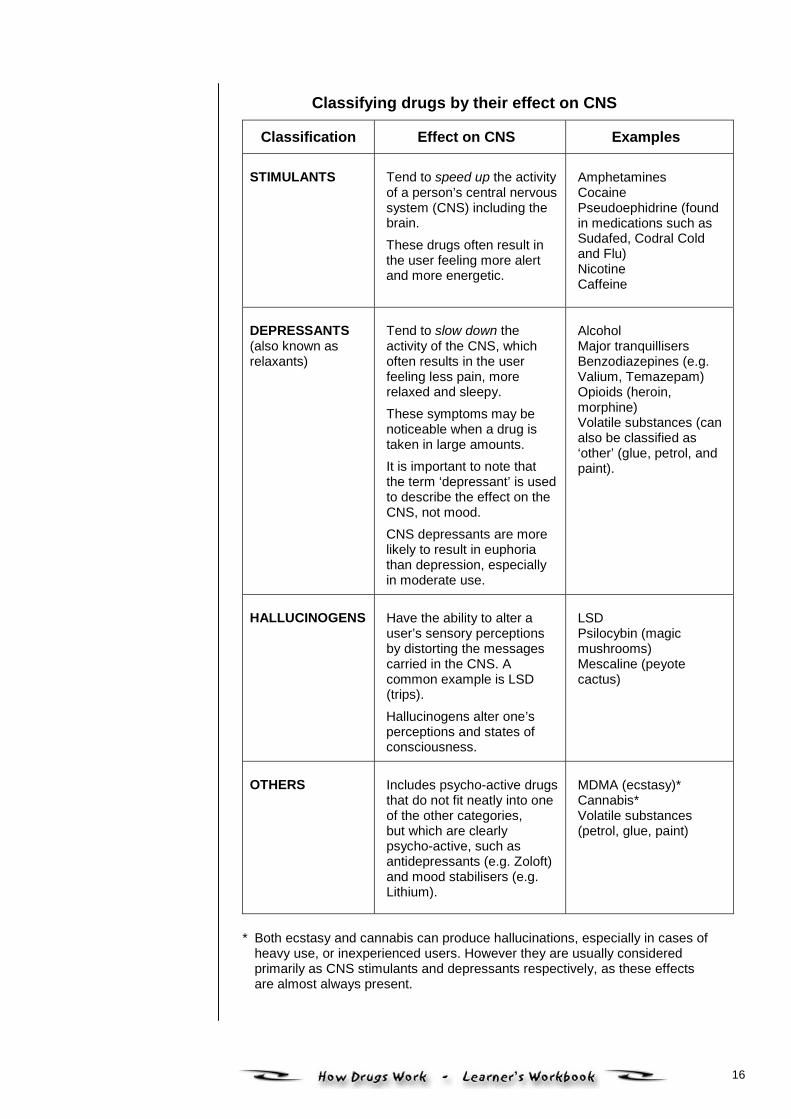
Classifying drugs by their effect on CNS
Classification Effect on CNS Examples
STIMULANTS Tend to speed up the activityof a person’s central nervoussystem (CNS) including thebrain.These drugs often result inthe user feeling more alertand more energetic.
AmphetaminesCocainePseudoephidrine (foundin medications such asSudafed, Codral Coldand Flu)NicotineCaffeine
DEPRESSANTS(also known asrelaxants)
Tend to slow down theactivity of the CNS, whichoften results in the userfeeling less pain, morerelaxed and sleepy.These symptoms may benoticeable when a drug istaken in large amounts.It is important to note thatthe term ‘depressant’ is usedto describe the effect on theCNS, not mood.CNS depressants are morelikely to result in euphoriathan depression, especiallyin moderate use.
AlcoholMajor tranquillisersBenzodiazepines (e.g.Valium, Temazepam)Opioids (heroin,morphine)Volatile substances (canalso be classified as‘other’ (glue, petrol, andpaint).
HALLUCINOGENS Have the ability to alter auser’s sensory perceptionsby distorting the messagescarried in the CNS. Acommon example is LSD(trips).Hallucinogens alter one’sperceptions and states ofconsciousness.
LSDPsilocybin (magicmushrooms)Mescaline (peyotecactus)
OTHERS Includes psycho-active drugsthat do not fit neatly into oneof the other categories,but which are clearlypsycho-active, such asantidepressants (e.g. Zoloft)and mood stabilisers (e.g.Lithium).
MDMA (ecstasy)*Cannabis*Volatile substances(petrol, glue, paint)
* Both ecstasy and cannabis can produce hallucinations, especially in cases ofheavy use, or inexperienced users. However they are usually consideredprimarily as CNS stimulants and depressants respectively, as these effectsare almost always present.
17
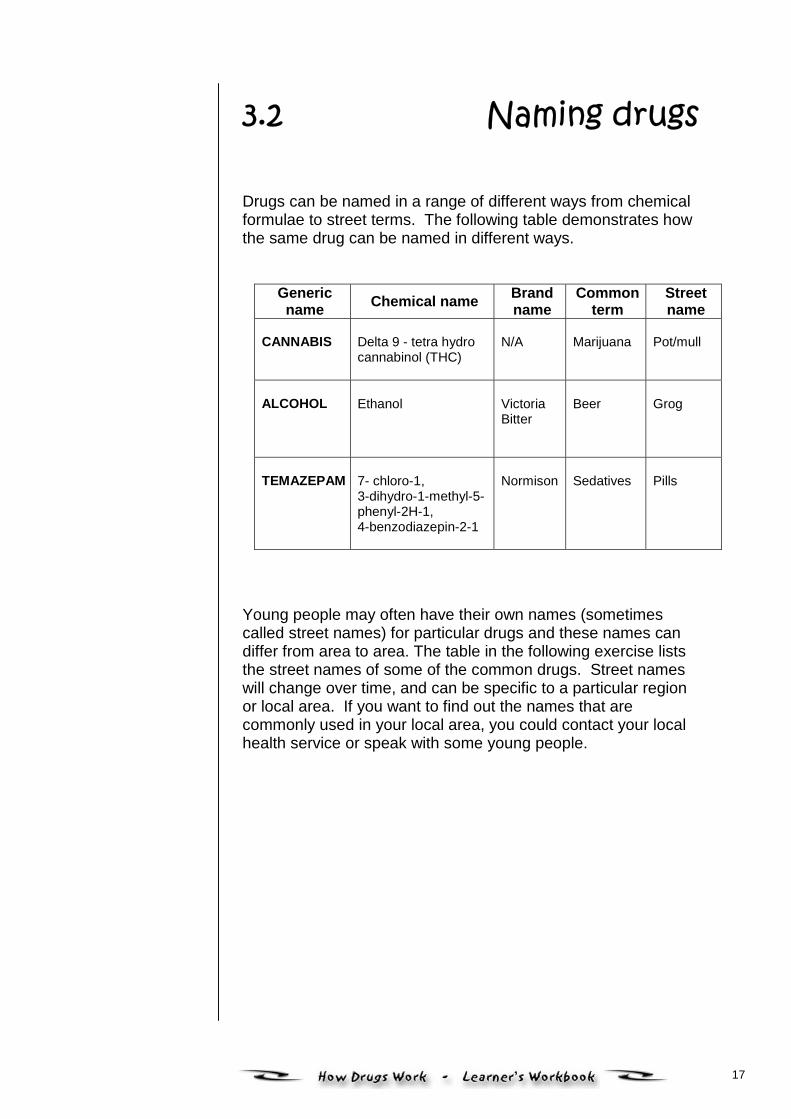
3.2 Naming drugs
Drugs can be named in a range of different ways from chemicalformulae to street terms. The following table demonstrates howthe same drug can be named in different ways.
Genericname Chemical name Brand
nameCommon
termStreetname
CANNABIS
Delta 9 - tetra hydrocannabinol (THC)
N/A
Marijuana
Pot/mull
ALCOHOL Ethanol
VictoriaBitter
Beer
Grog
TEMAZEPAM 7- chloro-1,3-dihydro-1-methyl-5-phenyl-2H-1,4-benzodiazepin-2-1
Normison
Sedatives
Pills
Young people may often have their own names (sometimescalled street names) for particular drugs and these names candiffer from area to area. The table in the following exercise liststhe street names of some of the common drugs. Street nameswill change over time, and can be specific to a particular regionor local area. If you want to find out the names that arecommonly used in your local area, you could contact your localhealth service or speak with some young people.
18
What are street names in your local area for:• Cannabis .........................................................
• Inhalants ..........................................................
• Benzodiazepines ............................................
• Ecstasy ............................................................
• Amphetamines ................................................
• Hallucinogens .................................................
• Opioids ............................................................
• Cocaine ............................................................
19
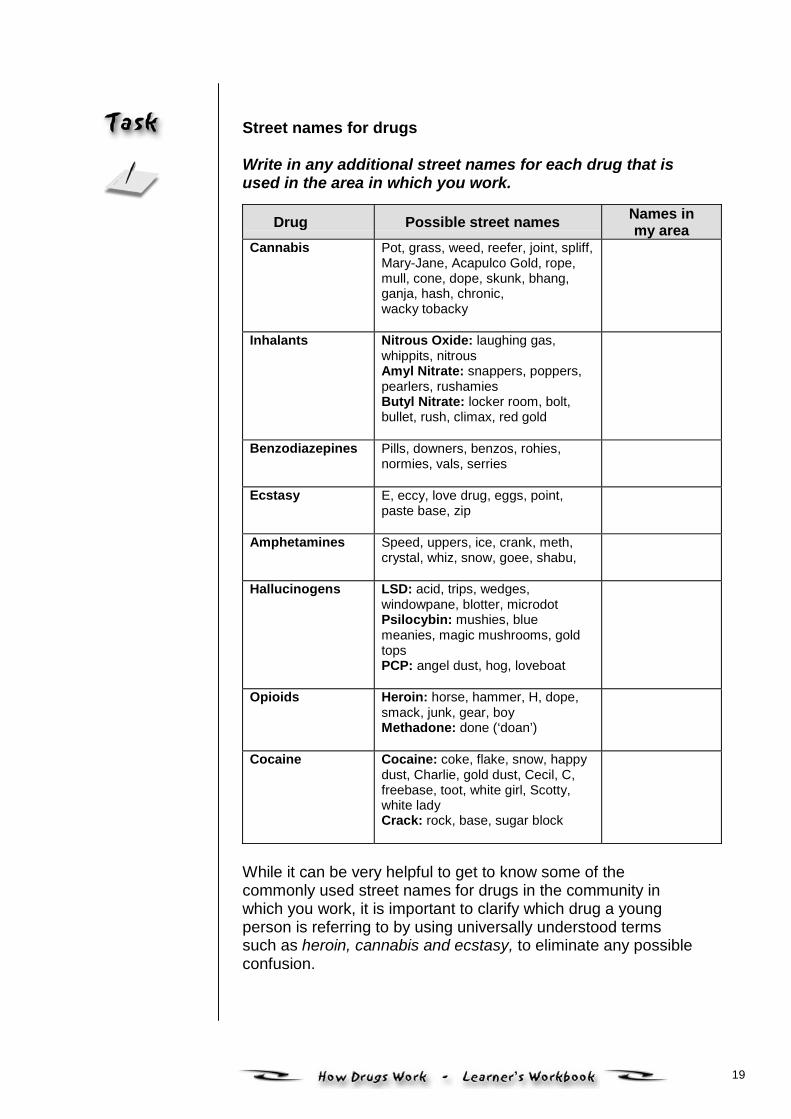
Street names for drugs
Write in any additional street names for each drug that isused in the area in which you work.
Drug Possible street names Names inmy area
Cannabis Pot, grass, weed, reefer, joint, spliff,Mary-Jane, Acapulco Gold, rope,mull, cone, dope, skunk, bhang,ganja, hash, chronic, wacky tobacky
Inhalants Nitrous Oxide: laughing gas,whippits, nitrous Amyl Nitrate: snappers, poppers,pearlers, rushamies Butyl Nitrate: locker room, bolt,bullet, rush, climax, red gold
Benzodiazepines
Pills, downers, benzos, rohies,normies, vals, serries
Ecstasy
E, eccy, love drug, eggs, point,paste base, zip
Amphetamines
Speed, uppers, ice, crank, meth,crystal, whiz, snow, goee, shabu,
Hallucinogens LSD: acid, trips, wedges,windowpane, blotter, microdot Psilocybin: mushies, bluemeanies, magic mushrooms, goldtops PCP: angel dust, hog, loveboat
Opioids
Heroin: horse, hammer, H, dope,smack, junk, gear, boy Methadone: done (‘doan’)
Cocaine Cocaine: coke, flake, snow, happydust, Charlie, gold dust, Cecil, C,freebase, toot, white girl, Scotty,white lady Crack: rock, base, sugar block
While it can be very helpful to get to know some of thecommonly used street names for drugs in the community inwhich you work, it is important to clarify which drug a youngperson is referring to by using universally understood termssuch as heroin, cannabis and ecstasy, to eliminate any possibleconfusion.
20
3.3 The legality of drugs
Drugs can also be classified in terms of their legal status. Thereare a variety of reasons why some recreational drugs are legalwhile others are illegal. The legal status of drugs is often due tohistorical and political factors rather than their harmful nature.For example, penalties are imposed for the use of some drugs,such as heroin, which only a small proportion of the populationuse, while others of apparently equal or greater danger arewidely used, accepted and promoted, such as alcohol.
Formal sanctions such as laws that prohibit the use of certainsubstances can deter people from using those drugs. However,they do not necessarily stop use altogether. Prescriptions areanother way of influencing the use and availability of drugs.
Legality of drugs Write the names of at least two or more psycho-activedrugs in each category below.
Legally availableto adults
Legal withprescription Illegal to use
Over the counterpainkillers Ritalin Cocaine
21
Distance learners should take time now to reflect on theirlearning, check in with their facilitator and determine theirprogress.
• The most useful system of classifying drugs is by theireffect on the central nervous system
− Stimulants speed up the CNS− Depressants slow down the CNS− Hallucinogens distort the message carried in the CNS− Other − those drugs that do not easily fit into the other
groups.
• Some drugs such as cannabis and ecstasy can fit into morethan one category.
22
Topic 4
How psycho-activedrugs act
on the body
Drugs produce their effect on the body through twomajor processes. The first is the effect of the chemicalproperties of the drug on the central nervous system(CNS) which includes the brain and the spinal cord.This process is called pharmacodynamics. Thesecond is how the drugs enter, are metabolised, andabsorbed by the body. This process is known aspharmacokinetics. These two processes worktogether to produce a certain effect.
Pharmacodynamic processes
Neurons
A psycho-active drug must find its way to thebloodstream to have an effect on the brain. Once thedrug reaches the brain, it can lodge on to specificreceptor sites on the neurons which are sensitive toparticular types of drugs. Each drug affects specificneurons in a number of parts of the brain. There are13 billion neurons or nerve cells in each person’sbrain.
The effect of drugson the centralnervous system (CNS)
www.wnet.org/closetohome describes the biology of drugeffects and dependence with easy-to-understand animationsof the brain.
23
Neurotransmitters
Many drugs seem to imitate neurotransmitters, the naturalchemicals that facilitate or inhibit the transfer of electricalimpulses between neurons. For example, opiate drugs such asheroin are thought to exert their drug action by mimickingendorphins which are naturally occurring proteins that reducepain.
Drug action
Like neurotransmitters, drugs can speed up (CNS stimulants) orslow down (CNS depressants) the transfer of electro-chemicalmessages between neurons in the brain. Messages betweenneurons can also be distorted when hallucinogenic drugs aretaken.
Pleasure centre
In addition to affecting the transfer of messages betweenneurons, drugs appear to act directly on ‘pleasure centres’ in thebrain, which may explain the euphoria experienced by users ofmany different types of drugs. It is believed that the effect on thepleasure centre is highly rewarding for many young people andis crucial to the development of drug dependence.
24
Review Quiz
Complete the following quick quiz which reflects yourlearning so far.
A. Pharmacology is:a) a branch of science that deals with emotionsb) the study of how drugs workc) the study of living things
B. Circle the drug that is not psycho-active.a) alcoholb) petrolc) steroids
C. A neuron is a:a) chemical in the brainb) gap between nerve cellsc) nerve cell
D. Drugs work by:a) imitating neurotransmittersb) destroying brain cellsc) creating dysfunctional neural pathways
E. The euphoria (good feeling) that drug use can promote, iscaused by:
a) the distortion of electrochemical messagesbetween neurons
b) stimulation of pleasure centres in the brainc) elimination of withdrawal symptoms
F. Drugs can be classified by their effect on the CNS. What arethe three major groups called? Provide two examples of drugsthat fit in each of these categories.
Group 1Group Name ..............................................................Example 1. .................................................................Example 2 ..................................................................
Group 2Group name ..............................................................Example 1 ..................................................................Example 2 .................................................................
Group 3Group name ...............................................................Example 1Example 2 ..................................................................
G. Why is it necessary to have a fourth group called ‘others’?
(Check your answers on the following page.)
25
A. (b) B. (c) C. (c) D. (a)
E. (b)
F. Group 1 Group Name: DepressantExamples: Alcohol
Heroin
Group 2 Group Name: StimulantExamples: Tobacco
Cocaine
Group 3 Group Name: HallucinogensExamples: LSD
Magic Mushrooms
G. Drugs classified as ‘others’ may not fit neatly into any onecategory. For example marijuana can be classified as ahallucinogen and/or a depressant. Ecstasy can be classified aseither an hallucinogen or stimulant because of their properties andtheir effect on neurotransmitters.
26
Topic 5
How drugs movethrough the body
5.1 Methods of drugadministration
To affect the brain, a psycho-active drug must enterthe body and reach the bloodstream in a processcalled pharmacokinetics. There are a variety ofways of administering drugs to allow them to enterthe body.
The most common methods of drug administrationinclude:
• injecting
• smoking
• inhaling
• snorting
• swallowing.
Each of these methods will be described more fullylater in this topic.
Methods of drugadministration
Speed of drug effect
Elimination of drugsfrom the body anddrug half-life
27
What are three of the most popular methods ofadministering drugs for young people you workwith? What could be some of the advantages anddisadvantages that young people might perceivefor each of these methods of drug administration?
Method of
administration Advantages Disadvantages 1.
2.
3.
(Check your answers on the following page.)
28
Method of administration Advantages Disadvantages
Swallowing
Easy Effects can be slow
Smoking
Familiar, can haverapid effect
Can be detectedeasily
Snorting
Rapid effect Can damage nostrils
29
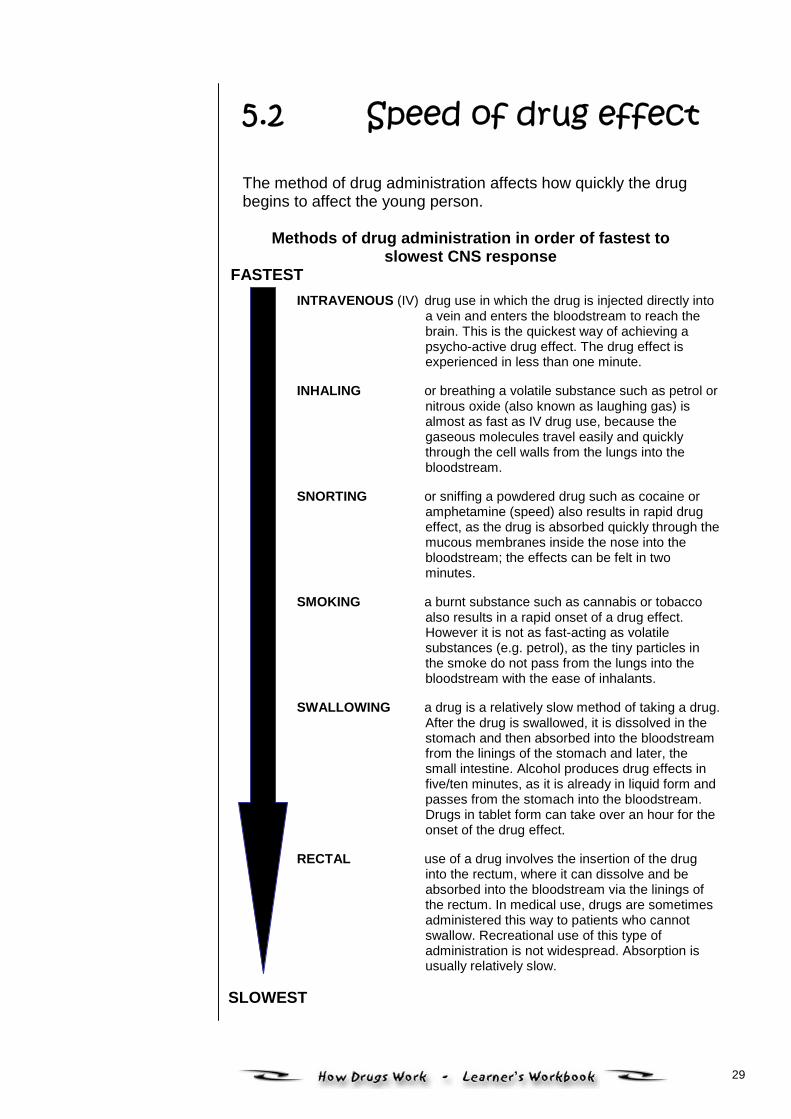
5.2 Speed of drug effect The method of drug administration affects how quickly the drugbegins to affect the young person.
Methods of drug administration in order of fastest toslowest CNS response
FASTEST
INTRAVENOUS (IV) drug use in which the drug is injected directly intoa vein and enters the bloodstream to reach thebrain. This is the quickest way of achieving apsycho-active drug effect. The drug effect isexperienced in less than one minute.
INHALING or breathing a volatile substance such as petrol ornitrous oxide (also known as laughing gas) isalmost as fast as IV drug use, because thegaseous molecules travel easily and quicklythrough the cell walls from the lungs into thebloodstream.
SNORTING or sniffing a powdered drug such as cocaine oramphetamine (speed) also results in rapid drugeffect, as the drug is absorbed quickly through themucous membranes inside the nose into thebloodstream; the effects can be felt in twominutes.
SMOKING a burnt substance such as cannabis or tobaccoalso results in a rapid onset of a drug effect.However it is not as fast-acting as volatilesubstances (e.g. petrol), as the tiny particles inthe smoke do not pass from the lungs into thebloodstream with the ease of inhalants.
SWALLOWING a drug is a relatively slow method of taking a drug.After the drug is swallowed, it is dissolved in thestomach and then absorbed into the bloodstreamfrom the linings of the stomach and later, thesmall intestine. Alcohol produces drug effects infive/ten minutes, as it is already in liquid form andpasses from the stomach into the bloodstream.Drugs in tablet form can take over an hour for theonset of the drug effect.
RECTAL use of a drug involves the insertion of the druginto the rectum, where it can dissolve and beabsorbed into the bloodstream via the linings ofthe rectum. In medical use, drugs are sometimesadministered this way to patients who cannotswallow. Recreational use of this type ofadministration is not widespread. Absorption isusually relatively slow.
SLOWEST
30
5.3 Elimination of drugsfrom the body
and drug half-life
Once drugs enter the body, the process of leaving the body orelimination begins. In order for drugs to leave the body, mostdrugs need to be metabolised. This is a chemical process inwhich the liver transforms the drug into a substance called ametabolite that can be passed out of the body.
While drugs and their metabolites are mostly excreted by thekidneys into urine, drugs can also leave the body in othermethods, such as breath and sweat, hence the noticeable smellof alcohol on someone who has been drinking very heavily.Drugs can also leave the body in very small quantities via salivaand breast milk.
Drug testing often detects the metabolites of specific drugs inthe urine of a person, rather than the drug itself.
Distance learners should take time now to reflect on theirlearning, check in with their facilitator and determine theirprogress.
• Various methods of drug administration including:InjectingSmokingInhalingSnortingSwallowing
• Intravenous drug use and inhaling the fumes of asubstance are the two fastest methods of achievingpsycho-active drug effect.
31
Topic 6
Drug effects
6.1 Factorsinfluencing
drug effects
The effect of any drug on an individual is the resultof three interacting factors:
1. the drug itself2. the individual user3. the environment in which drug use occurs.
In this topic we will be focusing on the factorsrelating to the drug itself.
The effect that a drug has on a person is determinedby many factors. The primary factors that influencedrug effect are the type of drug and the quantityused.
Other factors include:
• the time taken to consume the drug (10 minutesvs 10 hours)
• the user’s tolerance (e.g. regular cannabissmoker vs naïve smoker)
• the user’s gender, size and amount of muscle
Young People, Society and AOD
Factors influencingdrug effects
How drugs affectyoung peopledifferently
32
• other psycho-active drugs in the person’s bloodstream(poly-drug use)
• the mood or attitude of the user (e.g. angry vs calm,confident vs fearful)
• the user’s expectation of the drug effect (e.g. expecting apowerful drug effect vs expecting a modest drug effect)
• the setting or environment in which the drug is consumed(e.g. wild party vs quiet night at home).
Unexpected drug effect
Recall a time when a drug (psycho-active or not)had an unexpected effect on you or someone youknow. Briefly outline the situation, and identifywhich of the above factors may have contributed tothe drug effect.
33
6.2 How drugsaffect young
people differently
Age is one of the factors that determine how a drug will affect auser.
Drugs can affect young people differently for many reasons. Forexample:
• Having less experience with a drug means a person is lesslikely to have developed a tolerance for it. The drug will havetherefore have a greater effect.
• The social context (e.g. excitement at a party) in whichyoung people take drugs has an influence.
• Since the brain continues to develop until a young personreaches approximately 18 years of age, they can be morevulnerable to the harmful effects of drugs.
How drugs affect young people differently
What are some possible reasons why drugs mightaffect young people differently from adults? (Write your answers here, then check the possible answerson the next page.)
34
Possible answers include:
• smaller body size• placebo effect• poor judgement due to immaturity
Natasha and Samantha go to a party
Natasha is a 16-year-old girl, slightly built and 150cm tall. Shewent to a party that a friend was hosting and was very excitedbecause Jay, a boy she liked, was going to be there too. She didnot have much experience in drinking alcohol and her parentsnever allowed her to drink alcohol at home.
Arriving at the party at 7 pm, she drank five vodka drinks in thefirst hour. Later in the evening, Jay turned up to the party with hisarm around another girl. Natasha continued to drink three morevodka drinks and by 10 pm she became tearful and verballyabusive towards Jay and others at the party. After vomiting, shefell asleep around 11.30 pm.
One of Natasha’s friends is 16-year-old Samantha with anaverage build and 170cm tall. She had been to a few partieswhere alcohol was available and had been tipsy on severaloccasions. Her parents allow her to drink a glass of wine at dinnertime. While she was looking forward to the party, she was quiterelaxed about it. Samantha arrived with Natasha and drank threevodka drinks in the first hour, and then slowed down to one drinkper hour. By midnight, when people started to leave the party,Samantha was tipsy, but felt good, having danced most of thenight.
Using the table below, specify which factors ledNatasha to get very drunk and Samantha to justfeel tipsy?
Natasha SamanthaTotal amountof alcohol used
Average drinksper hour
Body size
Mood
Other factors
35
Drugs affect young people in ways that may be differentfrom adults. This may be due to:
• smaller body size
• placebo effect
• lack of experience and judgement
• lowered tolerance
• social context (excitement of the party)
• the brain is still developing
• peer influence
• strong expectations.
36
Topic 7
Effects of specificpsycho-active drugs
7.1 Short-termand long-termdrug effects
The effect of a drug is determined by many factorsin addition to the type and amount of the drug taken.However, each psycho-active drug does havespecific and often predictable effects on the user’sbehaviour, mood and thoughts, and often on bodilyfunctioning.
Short-term and long-term drug effects
In completing the following exercise, use the fact sheets(or other resources (such as www.ceida.net.au) referredto in the references section of this Workbook.
www.ceida.net.au
Short-term and long-term drug effects
The placebo effect
37
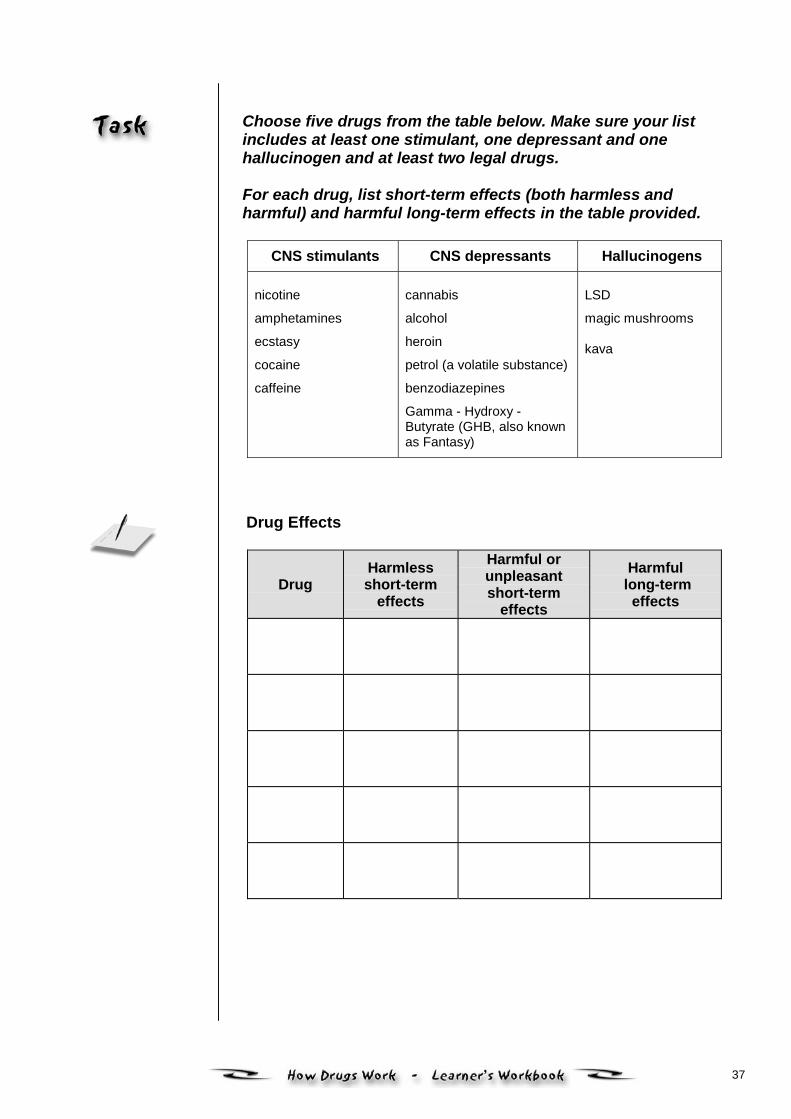
Choose five drugs from the table below. Make sure your listincludes at least one stimulant, one depressant and onehallucinogen and at least two legal drugs.
For each drug, list short-term effects (both harmless andharmful) and harmful long-term effects in the table provided.
CNS stimulants CNS depressants Hallucinogens
nicotine
amphetamines
ecstasy
cocaine
caffeine
cannabis
alcohol
heroin
petrol (a volatile substance)
benzodiazepines
Gamma - Hydroxy -Butyrate (GHB, also knownas Fantasy)
LSD
magic mushrooms
kava
Drug Effects
DrugHarmlessshort-term
effects
Harmful orunpleasantshort-term
effects
Harmful long-term
effects
38
SANDY
Sandy is a 14-year-old female who attends your service. Shehas been drinking and smoking cannabis just prior to her arrival.
What are the likely effects of this drug use onSandy’s behaviour?
How would you determine whether Sandy had beendrinking and smoking cannabis?
Which other drugs could possible lead to similareffects and symptoms?
39
Think of a young person you have worked with whom youbelieved was affected by drugs.
With reference to the table on drug effects state:
1) What indicators you noticed that led you tobelieve they were affected by the drug/s?
2) Which drugs could possibly produce similareffects?
You may have noticed that some drugs can lead to similareffects.
40
7.2 The placebo effect
The placebo effect is the well-known phenomenon in which aperson takes a substance which has no pharmacological orpsycho-active properties (usually a sugar pill) yet claims toexperience a drug effect. This effect is based on theexpectations of the person.
Doctors have sometimes used a placebo drug with somepatients claiming excellent results from their placebomedication, or alternatively intolerable side effects! (Of coursethe patients did not realise the medication was merely a sugarpill.)
The placebo effect can have a powerful influence when peopleuse psycho-active drugs.
Why might young people be particularly influencedby the placebo effect when they use psycho-activedrugs?
(Write your answer here, then check the possible answerson the next page.)
41
Many young people are inexperienced users and thereforetheir expectations can influence the effect of psycho-activedrugs.
• The effect of a drug is determined by many factors(not just type and amount of drug)
• Drugs can have short-term and long-term effects
• The placebo effect can have a powerful influencewhen young people use psycho-active drugs.
42
Topic 8
Key issues inpharmacology
8.1 Intoxication
A number of key terms are used in pharmacology todescribe and explain the range of effects that drugscan have on the body. Workers are in a betterposition to assess the impact of drug use on theindividual if they understand these processes.
How would you define the term‘intoxication’?
(Write your answer here, then check theanswers on the next page.)
Intoxication
Tolerance
Physical andpsychologicaldependence
Drug interactions
www.ceida.net.au
43
Intoxication is the term used to describe any change inperception, mood, thinking processes and motor skills thatresults from the effect of a drug(s) on our central nervoussystem.
Often intoxication is thought of in extreme terms, whensomeone is 'drunk' or 'off their head' with drugs. In fact,some degree of intoxication occurs with any single dose ofalcohol or other drugs. Risky activities of all sorts increase,even with low levels of intoxication.
Whatever problems and risks are associated with beingintoxicated, there is also much pleasure to be gained. Thisis an important principle to remember in our work withyoung people, as it will help us to understand theirmotivation for drug use and intoxication.
What are some of the changes in behaviouryou might notice in a young person who isintoxicated with cannabis? (Write your answer here, then check the possible answers onthe next page.)
44
Possible answers include:
• placid
• talkative
• hungry
What are some of the changes in behaviour youmight notice in a young person who is intoxicatedwith alcohol?
(Write your answer here, then check the possible answerson the next page.)
45
Possible answers include:
• loud
• boisterous
• sleepy

46
8.2 Tolerance
What is your understanding of the term ‘tolerance’in relation to AOD issues?
(Write your answer here, then check the possible answerson the next page.)
47
Tolerance occurs when a regular user of a drug graduallybecomes less responsive to the drug. This can often lead to theperson taking larger amounts of the drug to achieve the sameeffect.
A new user of a drug has no tolerance to it and will be affectedmore than an experienced user. For example, while a youngperson who has never consumed alcohol may become quiteintoxicated from having one standard drink, another person ofthe same age and gender may require three or more drinks toexperience the same effect.
Tolerance develops via two main mechanisms:
1. The liver increases the level of enzymes to metabolise thedrug, so it becomes more effective at eliminating the drug.
2. The brain’s receptors respond to the regular presence ofthe drug by becoming less sensitive to the drug’s effects.
Is the concept of tolerance relevant to youngpeople? If so, how?
(Write your answer here, then check the possible answer onthe next page.)
48
Young people will become tolerant to most drugs withregular use. However, tolerance can develop rapidly withregular use of some drugs such as amphetamines,ecstasy, heroin and benzodiazepines. Other drugs such asnicotine do not appear to demonstrate tolerance, except forthe initial effects such as nausea and headache for naïveusers.
JOHN
John is a 17-year-old who was arrested for theft and sent to ajuvenile correctional facility. At the time of his arrest, he wasusing two to three $50 shots of heroin per day, and his toleranceto heroin was quite high.
John spent three months in the juvenile facility, during whichtime he did not use heroin. He ingested rohypnol tablets onthree occasions during his first week there, but since then, hadnot used any other drugs.
John was released from the juvenile facility, and went to therefuge accommodation that a social worker had arranged forhim. He wasn’t happy there and went out to find some of thefriends he used to hang out with prior to his arrest.
What might happen to John if he used a $50 shot ofheroin again that evening?
What factors might influence whether Johnexperienced an overdose or not? (Hint: See topic ondrug effects).
49
8.3 Physical andpsychologicaldependence
Dependence on a drug can be physical, psychological or both.Many daily drug users demonstrate signs of both. The physicaland psychological aspects of drug dependence are closelyrelated and can be difficult to separate (often workers in theAOD field talk only of dependence). However, there are somedifferences.
What do you understand by the term ‘physicaldependence’? (Write your answer here, then check the possible answerson the next page.)
50
Physical dependence to a drug can be demonstrated bythe presence of withdrawal symptoms when the drug is nottaken. That is, the person depends on the drug to avoidwithdrawal symptoms and to function normally. This isknown as ‘addiction’, a term not so widely used in recenttimes. Physical dependence on a drug often follows heavydaily use over several weeks or longer.
GEMMA Gemma uses about $100 worth of heroin per day, in two to fourinjections, four to twelve hours apart. When she goes for longerthan twelve hours without the drug, she feels sick in thestomach, anxious, and has very strong cravings for the drug. Physical dependence
Consider a young person physically dependent onalcohol, sedatives or cannabis. What sort ofphysical symptoms might they demonstrate if theygo without that substance for a significant period oftime?
What do you understand by the term ‘psychologicaldependence’?
(Write your answer here, then check the possible answerson the next page.)
51
Psychological dependence occurs when a drug becomescentral to a person’s thoughts, emotions and activities. Itcan be demonstrated by a strong urge to use the drug,despite being aware of its harmful effects. A preoccupationwith acquiring the drug and/or compulsive use of the drugmay also be evident. Another determining factor may berelapse or recurrent use of the drug.
While not all drugs are considered capable of leading tophysical dependence, it is possible for any drug to lead topsychological dependence.
THOMAS Thomas sniffs petrol with his friends. He often goes withoutsniffing for a few days with no withdrawal symptoms. However,when he has not sniffed for a week or more, he can feel astrong urge to sniff, despite knowing the dangers of petrolsniffing. The urge to sniff can be very strong if he feelsdepressed or bored.
Psychological dependence
Describe another example of a young person psychologicallydependent on amphetamines, ecstasy or alcohol.
52
From your experience, what sort of physicalsymptoms might a physically dependent persondemonstrate if they go without that substance for asignificant period of time?
What sort of symptoms might a psychologicallydependent person demonstrate if they go withoutthat substance for a significant period of time?
53
8.4 Drug interactions
Drug interaction occurs when a drug acts on the body along withanother drug. This interaction can change the effect of one orboth drugs on the body. When two drugs of a similar typeinteract, the overall effect of one or both of the drugs canincrease. Mixing drugs (often referred to as poly-drug use), cantherefore be a very risky activity. Some drug interactions can be very dangerous − especiallywhen any combination of the following drugs are taken together: • alcohol• heroin• benzodiazapines
It is interesting to note that many heroin users who have died ofdrug overdoses had also consumed alcohol and/or prescriptiondrugs in addition to heroin. Drugs can act together so that the overall effect is far greaterthan the two added together. Their effect can be multiplied. Thisis called potentiation.
What is the relevance of knowing about druginteractions for workers? (Write your answer here, then check the possible answerson the next page.)
54
Many heroin users who have died of drug overdoses hadalso consumed alcohol and/or prescription drugs inaddition to heroin.
Some of the key issues in pharmacology include:
• intoxication
• tolerance
• dependence (both physical and psychological)
• drug interaction
• potentiation.
55
Topic 9
Managingoverdose
9.1 Overdose andidentifying those
who are at high risk
The term ‘overdose’ is often associated with thefatal or life-threatening effect of using too much of adrug. However, overdose refers to any unpleasantand unintended effect of a drug.
The amount needed to reach an overdose dependson the tolerance of the person as well as the amountand type of drug. For example, while a 13-year-oldcan overdose on drawing back her first puff of acigarette (causing her to cough and feel unwell), itmight require two bottles of bourbon consumed over24 hours for a heavy drinker to overdose (vomitingor falling unconscious). An overdose can thus beviewed as short-term, unpleasant or harmful effects.
Overdose andidentifying those whoare at high risk
Management ofoverdose
Heroin overdose –a special case
56
Overdoses are more likely to occur in some environments thanothers but there is always a possibility that a young person mayhave a serious drug overdose while they are in your care. Allworkers with young people should be prepared to deal with suchan emergency as this preparation could help to save someone’slife.
What should you do if you suspect an overdose hasoccurred?
(Write your answer here, then check the possible answerson the next page.)
57
Possible answers include:
Seek medical assistance then monitor the following indicators:
• decreasing levels of consciousness• breathing difficulties• abnormal pulse (irregular or below 60 bpm
or above 120 bpm)• convulsions• increasing agitation• changing mental state – hallucinations, panic or deep
depression.
Some people are at higher risk of experiencing overdose thanothers. Some risk factors related to overdose include:
• heroin use• poly-drug use (mixing drugs)• past overdoses• recent release from a correctional centre• age• using drugs alone.
Being aware of these risk factors can help identify those peoplewho may be at highest risk so that risk management strategiesmight be implemented. While there may be a risk of overdosewith the presence of one or more of these factors it cannot beassumed that everyone who is a poly-drug user, for example,will necessarily experience an overdose.
What factors might affect the seriousness of anoverdose?
(Write your answer here, then check the possible answerson the next page.)
58
Possible answers include:
• type of drug• amount used• how administered• poly-drug use• time consumed• tolerance level• mood• physical/psychological status• gender• age• weight• expectations.
59
9.2 Managementof overdose
Many media reports focus on fatal overdoses. However it isimportant to note that not all overdoses are fatal or life-threatening. Nevertheless you should always seek medicaladvice if you suspect an overdose has occurred. You shouldalso know your agency’s policy regarding the management ofoverdose and/or critical situations.
Overdose types
Overdose can be divided into two main types: potentially life-threatening and non-life threatening.
Potentially life-threatening overdose When a young person’s life seems in danger as a result of anoverdose (e.g. when the person has collapsed or stoppedbreathing) the following steps are recommended:
• call an ambulance
• ensure the safety of yourself and others in your care orsupervision
• administer first aid
• take young person to the emergency department of thenearest Medical Centre
• thoroughly document the incident and your involvement. Non life-threatening If you are experienced in dealing with overdose managementand feel confident that the overdose is not life-threatening, thefollowing strategies are recommended:
• make contact with a health professional and seek a secondopinion
• observe young person − don’t let them go home until theyare OK

60
• if young person goes home, try to have a someone stay withthem
• thoroughly document the incident and your involvement.
Remember that while you are working with young people, youwill always be subject to legal obligations that relate to youngpeople and their drug use while they are in your care orsupervision.
61
9.3 Heroin overdose− a special case
The vast majority of fatal illicit drug overdoses involve the use ofheroin. This is because, in Australia, heroin is usually injected.This results in a quick and intense effect. Large enoughamounts of heroin will not only cause the user to loseconsciousness (pass out), but will act on the brain stem to stopthe person from breathing. The dangerous effects of heroin canbe exaggerated by the use of other CNS depressant drugs,such as alcohol or benzodiazepines in conjunction with heroin.
One of the common interventions used for heroin and otheropiate overdose is the intravenous use of Naloxone (Narcan).This drug is an opiate antagonist, which reverses the effect ofheroin and other opiates within seconds. The person will wakeup immediately and often experience withdrawal symptoms.Naloxone works by dislodging the opiates from the receptorsites in the brain. It has a short half-life, and wears off quickly.This means that if a person has another shot of heroin, the firstshot of heroin can ‘kick in’ again, leading to another overdose.
62
Planning for the management of overdose
Does your organisation have any policy orprocedure documents relating to how you mightmanage a young person’s overdose or a policyrelating to critical incidents? (If so, obtain a copy anduse it to assist you in completing the followingquestions. If not, complete the questions, and thendiscuss with your manager or supervisor).
Are there any work situations that you can think ofwhere you might come across a young person whohas overdosed (either life threatening or non-lifethreatening)? (e.g. streetwork, residential care setting,court house etc.)
Are there likely to be other workers or youngpeople present at that work situation? If so, whatoccupational groups might be present? (e.g. policeat a courthouse or young people together in astreetwork setting?)
63
What would be your role would be in managingsuch a situation?
If there are likely to be other workers there, whatwould their role be in managing such a situation?
What sort of issues might arise if there are otheryoung people present and how might you assist inmanaging them?
64
Review the general steps for managing overdoseoutlined earlier in this module. Would they assistyou in managing that situation? If not, what elsemight you be required to do?
Are your colleagues (both in your own agency andother relevant agencies) aware of how to manageoverdose?
What are some ways that you could encourageother workers to consider and plan for managing anoverdose situation?
Distance learners should take time now to reflect on theirlearning, check in with their facilitator and determine theirprogress.
65
Topic 10
Management ofwithdrawal
10.1 Withdrawalsymptoms and the
rebound effect
Withdrawal symptoms
Withdrawal symptoms can occur when a person usinga drug over a prolonged period of time reduces orstops using altogether. In much the same way as theeffects of a drug are highly variable, the symptoms,severity and duration of withdrawal from a drug aredifficult to predict. Some differences in withdrawal arevery difficult to explain and are probably due tobiological and psychological differences in people.However there are factors − apart from the amountand duration of the drug used − that can affect theseverity and duration of withdrawal.
A substance as common as coffee can producewithdrawal symptoms in certain circumstances. If youare usually a heavy coffee drinker and then go awaycamping for a week (without taking coffee with you!)you might well experience headaches and otherunpleasant symptoms which are the result ofwithdrawal from caffeine.
Withdrawal symptoms for most drugs last for lessthan two weeks. Some drugs are likely to producemore severe withdrawal symptoms.
Withdrawal symptomsand the reboundeffect
Assisting youngpeople withdrawingfrom drugs
66
Withdrawal
Heroin
Branco used $100 heroin per day for four years andexperienced quite mild withdrawal symptoms when he wentthrough detoxification. He did not require medication or an in-patient stay. In comparison, Robbie had very severewithdrawal symptoms after ceasing a $50-a-day heroin habitwhich had continued over a six-month period.
Cannabis Tara and Rebecca had both been smoking five to ten cones ofhydro cannabis (a more potent form than leaf) daily for about ayear. As a New Year’s resolution, the girls agreed to give upcannabis for at least a month. While Tara coped relatively well,and did not experience any serious withdrawal symptoms,Rebecca had ten days of ‘hell’ experiencing insomnia,depression, irritability, anxiety and sweating.
What are some reasons that might explain thedifferences in the withdrawal symptomsexperienced by Branco and Robbie and Tara andRebecca? (Write your answer here, then check the possible answers onthe following page.)
67
Possible answers include: • expectation − If someone expects to have a very severe
withdrawal, it is more likely they will have one.
• general physical health − A person who is less healthy ismore likely to experience serious withdrawal symptoms
• general psychological health − Someone prone to anxietyor depression is more likely to experience serious withdrawalsymptoms.
• social supports − that the person is able to rely upon.
68
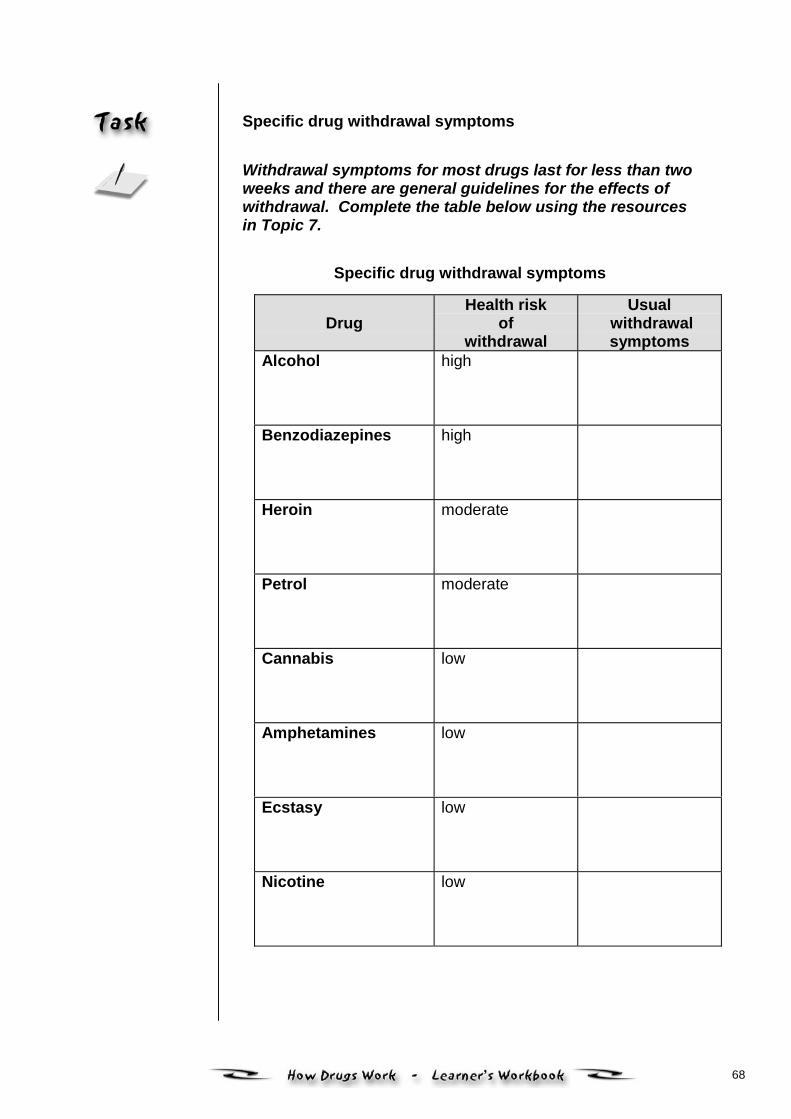
Specific drug withdrawal symptoms
Withdrawal symptoms for most drugs last for less than twoweeks and there are general guidelines for the effects ofwithdrawal. Complete the table below using the resourcesin Topic 7.
Specific drug withdrawal symptoms
Drug Health risk
ofwithdrawal
Usual withdrawalsymptoms
Alcohol
high
Benzodiazepines
high
Heroin
moderate
Petrol
moderate
Cannabis
low
Amphetamines
low
Ecstasy
low
Nicotine
low
69
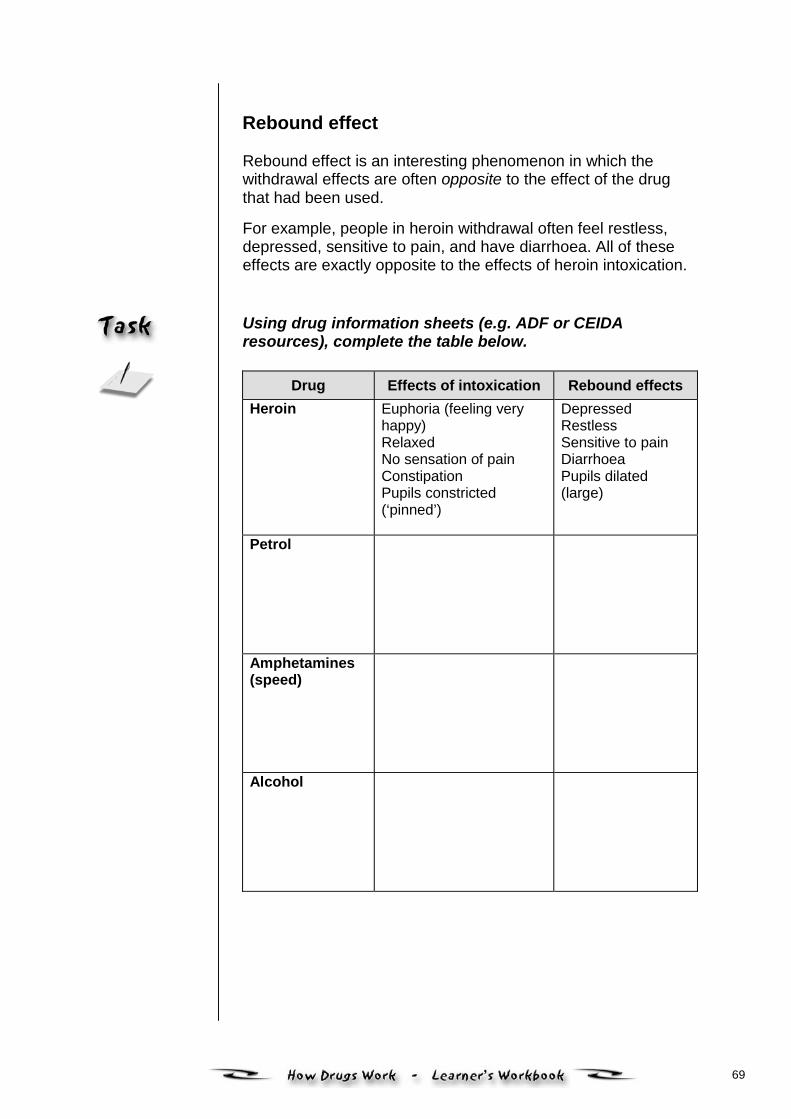
Rebound effect
Rebound effect is an interesting phenomenon in which thewithdrawal effects are often opposite to the effect of the drugthat had been used.
For example, people in heroin withdrawal often feel restless,depressed, sensitive to pain, and have diarrhoea. All of theseeffects are exactly opposite to the effects of heroin intoxication. Using drug information sheets (e.g. ADF or CEIDAresources), complete the table below.
Drug Effects of intoxication Rebound effectsHeroin Euphoria (feeling very
happy)RelaxedNo sensation of painConstipationPupils constricted(‘pinned’)
DepressedRestlessSensitive to painDiarrhoeaPupils dilated(large)
Petrol
Amphetamines(speed)
Alcohol
70
10.2 Assisting youngpeople withdrawing
from drugs
Managing withdrawal symptoms
Withdrawal from any drug is almost always an unpleasantexperience. The person’s body has developed a physicaldependence and now needs the drug to function normally.However, many young people can successfully withdraw fromalcohol or other drugs without formalised treatment such ashospitalisation or medication.
As with the management of overdose, many frontline workerswill not be required to assist someone withdrawing from drugs.While youth workers in a residential facility may come acrossthis issue, other frontline workers may not.
Even so, in your work you may come across someone who iswithdrawing from drugs. You should therefore be able torecognise possible withdrawal symptoms and have somestrategies to assist the person that are appropriate to your workrole. You may need to work with an AOD worker to help theyoung person through this experience.
While some drugs can often be managed without the need formedication, it is sometimes required to reduce the mostuncomfortable symptoms and assist people to sleep. However, other drugs are likely to produce more severewithdrawal symptoms. For example, alcohol can produce life-threatening withdrawal symptoms known as delerium tremens(DTs), which can require urgent hospital treatment, includingmedication.
Medical professionals should provide details of any medicationthat may be required for a young person undergoingdetoxification. If in doubt, you should always consult a medicalprofessional before dispensing medications to a young person.
Check your organisational policies and procedures regardingyour role in managing withdrawal and dispensing medication toyoung people.
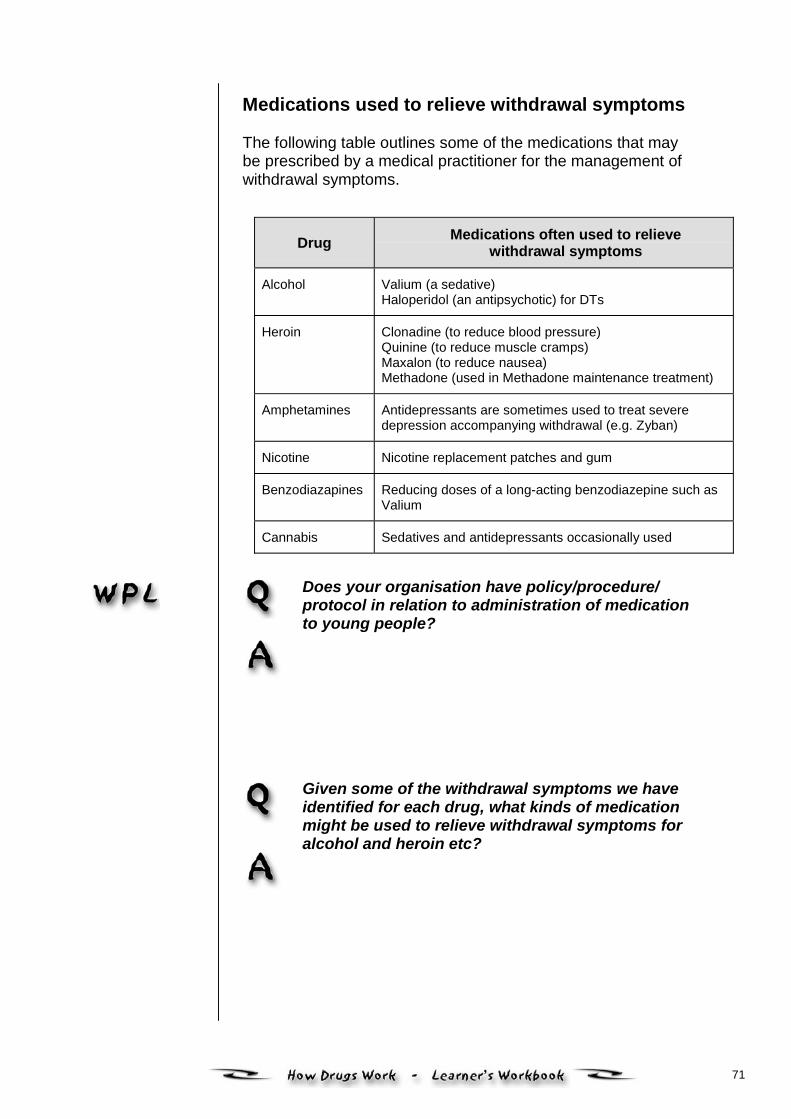
71
Medications used to relieve withdrawal symptoms
The following table outlines some of the medications that maybe prescribed by a medical practitioner for the management ofwithdrawal symptoms.
Drug Medications often used to relievewithdrawal symptoms
Alcohol Valium (a sedative)Haloperidol (an antipsychotic) for DTs
Heroin Clonadine (to reduce blood pressure)Quinine (to reduce muscle cramps)Maxalon (to reduce nausea)Methadone (used in Methadone maintenance treatment)
Amphetamines Antidepressants are sometimes used to treat severedepression accompanying withdrawal (e.g. Zyban)
Nicotine Nicotine replacement patches and gum
Benzodiazapines Reducing doses of a long-acting benzodiazepine such asValium
Cannabis Sedatives and antidepressants occasionally used
Does your organisation have policy/procedure/protocol in relation to administration of medicationto young people?
Given some of the withdrawal symptoms we haveidentified for each drug, what kinds of medicationmight be used to relieve withdrawal symptoms foralcohol and heroin etc?
72
Withdrawal:
• is the set of symptoms a daily user of a drugexperiences when they stop taking that drug
• symptoms can be difficult to predict
• with the rebound effect, symptoms are oftenopposite to the effect of the drug that has beenused.
73
Topic 11
Reducingdrug-related harm
11.1 Understandingdrug-related harm
As we have seen in the previous topics the effectsof drugs on the individual user is complex.Sometimes alcohol and other drug use can beharmful for the user. The harm may be a directresult of the effect of the drug on the body or it maybe a result of broader factors related to drug use,such as the way the drug is administered oraccidents that occur while under the influence of thedrug.
The Public Health model can be used to understanddrug-related harm. According to this model threeareas determine the drug experience: the drug, theindividual and the environment. Harm from druguse can fall into each of these three areas. This canbe a helpful way of identifying the range of harmsthat young people can experience due to their druguse. Similarly each of these areas can be the focusof strategies to reduce harm related to drug use.This approach is also referred to as the InteractionModel.
Young People, Society and AODWorking with Families, Peers and Communities
Understanding drug-related harm
Thorley’s model ofdrug-related harm
The Four L’s model
Harm minimisation
Specific harmsrelated to drugs anddrug use
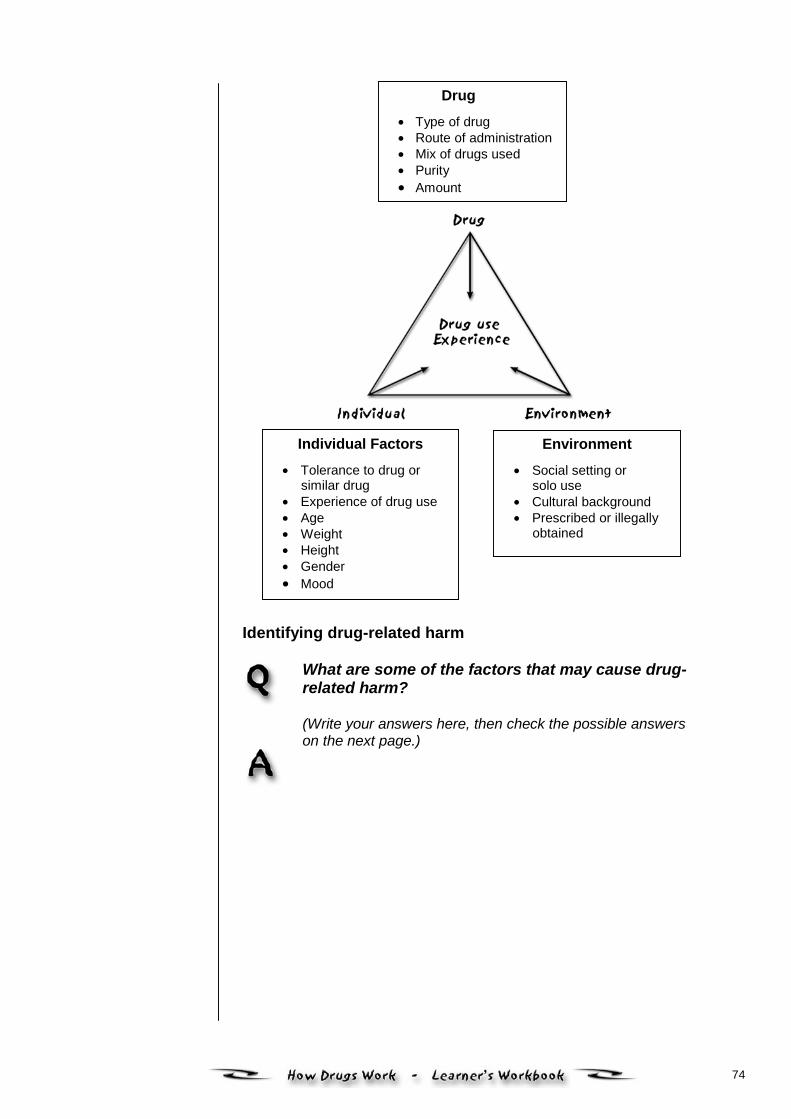
74
Identifying drug-related harm
What are some of the factors that may cause drug-related harm?
(Write your answers here, then check the possible answerson the next page.)
Drug• Type of drug• Route of administration• Mix of drugs used• Purity• Amount
Individual Factors• Tolerance to drug or
similar drug• Experience of drug use• Age• Weight• Height• Gender• Mood
Environment• Social setting or
solo use• Cultural background• Prescribed or illegally
obtained
75
Possible answers include:
• The drug and type of drug used: Harms related toinjecting drugs, overdose
• The individual and individual factors: Aggressivebehaviour, depression, money problems, dependency,tolerance
• The environment (or context) in which drugs areused: Legal problems, friends using, problems withfamily, homelessness.
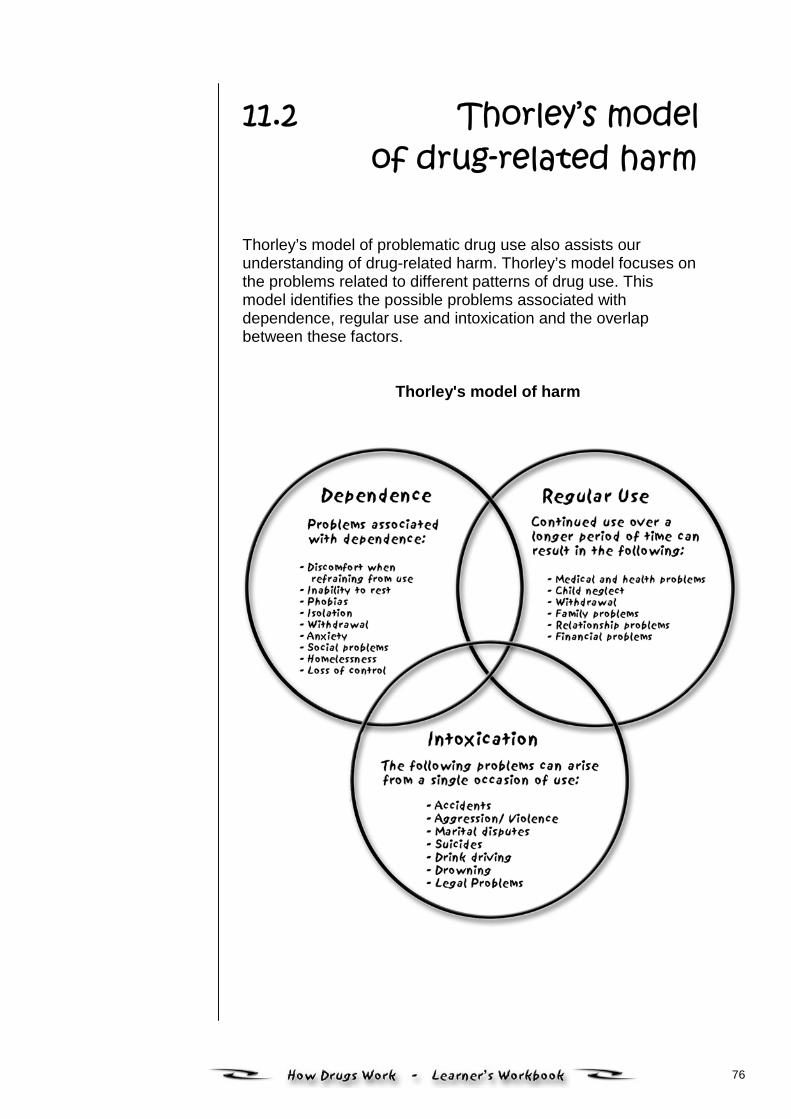
76
11.2 Thorley’s modelof drug-related harm
Thorley’s model of problematic drug use also assists ourunderstanding of drug-related harm. Thorley’s model focuses onthe problems related to different patterns of drug use. Thismodel identifies the possible problems associated withdependence, regular use and intoxication and the overlapbetween these factors.
Thorley's model of harm
77
While there may be some overlap between the type of use andassociated harms, there are also many separate issues relatedto the different types of use. It is important to remember that the majority of young people willnot experience problems related to dependent use. Most oftheir difficulties will arise from intoxication (using at hazardouslevels) or regular use (e.g. a couple of drinks of alcohol eachnight with friends). However, a smaller proportion of long-term excessive users willexperience some dependence-related problems as they developa tolerance to the drug and a need to use for both psychologicaland physical reasons.
78
11.3 The Four L’s model
Another useful model for understanding the nature and extent ofdrug-related difficulties considers the actual nature of thedifficulties experienced. Thorley’s model looks at patterns of useand related problems whereas the Four L’s model, (adapted byRoizen) considers the impact of drug use on four major sphereson a young person’s life. These are:
Liver: Anything to do with a person’s health – eitherphysical, psychological or emotional healthproblems
Lover: Problems associated with a person’srelationships, family, friends, children, loversetc.
Lifestyle/ Problems which relate accommodation,livelihood work, finances, education, recreation etc.
Legal: Any problems associated with the law –either criminal or civil proceedings.
Like Thorley’s model, the Four L’s model is extremely useful forfrontline workers in that it assists you to work out the types ofproblems or difficulties being experienced by a young person.This model can be applied during an initial or morecomprehensive assessment of a young person as it helps you toidentify the most urgent areas for intervention. If a young personis experiencing difficulties in all four spheres of life it mayindicate that they are dependent upon drugs. Once drug useaffects every aspect of daily life it is a major issue of concernand will require further exploration with the young person.
79
11.4 Harm minimisation
Harm minimisation aims to reduce the harmful health, social andeconomic consequences of alcohol and other drugs onindividuals and society. It is based on the Public Health model.Goals and strategies for harm minimisation are wide ranging.The approach is broad enough so that the goals of safer druguse, controlled use and abstinence can all be accommodated.
Harm minimisation is accepted Commonwealth policy.
Harm minimisation strategies can be categorised into threeareas:
• Harm reduction − Strategies that aim to reduce the harmfrom drugs for both individuals and communities. Thesestrategies do not necessarily aim to stop drug use. Examplesinclude needle syringe services, methadone maintenance,brief interventions, peer education and education for saferdrug use.
• Supply reduction − Strategies aimed at reducing theproduction and supply of illicit drugs. Examples includelegislation and law enforcement.
• Demand reduction − Strategies aimed at preventing theuptake of harmful drug use. Examples include communitydevelopment projects and media campaigns.
In this module, as we are focusing on the drug itself we willemphasise harm reduction strategies.

80
11.5 Specific harmsrelated to drugs
and drug use
The table below will help you identify possible harms related toparticular drugs and harm reduction strategies that can be usedto reduce these harms. One example has been provided. • Fill in the rest of table focusing on drugs that young people
in your area commonly use.
Drug Drug related harm Harm reductionstrategies
Ecstasy Dehydration
Drinking appropriatelevels of water
Most young people do not inject drugs. However, there areharms related to injecting drug use that it is important to befamiliar with. These include: • fatal overdose due to respiratory depression (a large dose
of CNS depressants can cause the person’s brain to ‘forget’to breathe)
• blood-borne viruses (e.g. HIV and Hepatitis C) spread bysharing needles or other injecting equipment with aninfected person
• other medical problems (e.g. skin sores, bruising, bloodclots, blood infections) caused by injecting practices, such aspoor hygiene and overusing the same injecting site.
81
Strategies to reduce harm
Some strategies that reduce the harm related to injecting druguse include:
• Following infection control procedures
• Never re-using syringes or needles
• Using sterile ‘fit kits’ provided by health services andselected chemists. (The fit kit provides injecting drug userswith sterilised needles and a disposal receptacle to reducerisk of stab wounds to others. The kit is available throughhospitals at no cost.)
• Disposing of needles in sterile bins.
82
MATT
Matt is a 16-year-old male in Year 11 at school. His parentshave recently called the school counsellor, concerned becausehe is drinking large amounts of alcohol on weekends with hisfriends. More recently he has begun arriving home early onSunday morning (after a Saturday night out) extremelyintoxicated, to the point where he vomits and has difficultyspeaking or even walking.
A few weeks ago, Matt arrived home later than usual, minus hiseyebrows because they were shaved off by his mates after he‘passed out’ after drinking too much. Although Matt’s parentsaccept ‘heavy drinking’ as a relatively normal part of growing up,they are concerned that Matt’s drinking is happening morefrequently. They also suspect that he may be using othersubstances as well. Whenever they have tried to discuss theirconcerns with Matt, or impose limits on his going out, hebecomes extremely agitated and tells his parents that they don’tunderstand and that they are being over protective. Mattbelieves that he is just doing what his mates do and that there isnothing wrong with his behaviour.
His teachers have noticed no recent decline in his grades.Although Matt has never been a top student, he has consistentlyobtained B/C grades and has always planned on going touniversity to study business. Indeed, as long as his currentgrades are maintained, he may achieve this goal (although inorder to do so it is important that his grades do not fall).
What sort of harm might Matt be experiencing fromthe effects of alcohol?
83
If the school counsellor adopted a harm reductionapproach, what might they recommend to Matt andhis parents?
What activities could cause harm to young peoplethat you work with?
Reflect on any harm reduction strategies youcurrently use in your work with young people. Doyou think these strategies work well for theseyoung people? Consider the reasons for yourresponse.
What research harm reduction strategies orservices do other agencies in your area use in theirwork with young people?
84
Topic 12
Summary andconclusion
12.1At this point you should speak with your facilitatorand together assess whether you can:
• Classify common psycho-active drugs accordingto their effect on the central nervous system
• Outline the major short and long-term effects ofpsycho-active drugs
• Discuss key issues in pharmacology such astolerance, withdrawal, overdose, dependenceand interaction
• Describe the harmful effects on young peopleresulting from AOD use.
If you have any concerns about meeting theselearning outcomes you should speak further withyour facilitator.
Before you contact your facilitator, complete theReflection Activity in this topic.
Remember that if you want to know more about anyof the topics covered in this module, a range ofreferences are provided at the end of this module.
You could also contact your local health service oryouth service for further information.

85
12.2 Summary of contents
In this module you have explored how mind-altering drugs ofdifferent types act on young people. Some key issues inpharmacology have been covered that may help you respondmore appropriately to the needs of young people with alcoholand other drug problems.
86
12.3 Self-reflectionactivity
Take some time to reflect on what you have gained from yourlearning. You may wish to share your insights with otherlearners or colleagues, if possible.
What aspect of this module do you feel is mostrelevant and useful in your work practice?
What kinds of issues has this module raised for youin your work?
Have you identified any further learning needs as aresult of completing this module?
If so, what are some ways you can achieve theselearning needs?
87
References
Australian Institute of Health and Welfare 2002. (2001). NationalDrug Strategy Household Survey: First results. AIHW Cat No.PHE 35. Canberra: AIHW (Drug Statistics Series No 9).
Commonwealth Department of Human Services and Health(1995). Handbook on alcohol and other drug problems formedical practitioners and other health care workers. Australia:Australian Government Publishing Service.
Julien, R. (1995) Primer of Drug Action. New York: W.H. Freeman.
MIMS Australia, published by Medimedia, is monthly and annualguide used by health professionals to find information onpharmaceuticals. While these guides are not generally availableto the general public, they can often be sourced from hospitallibraries and medical practitioners.
Ryder, D., Salmon, A. & Walker, N. (2001). Drug Use and Drug-related Harm: A delicate balance. IP Communications Pty Ltd.
Upfal, J, (1998) The Australian Drug Guide, 4th ed. Melbourne,Australia: Bookman Press.
Websites
National Institute on Drug Abuse. Slide Teaching Packet 1, ForHealth Practitioners, Teachers and Neuroscientists entitled‘The Brain and the Actions of Cocaine, Opiates, and Marijuana’.www.clubdrugs.org
An excellent website, with details descriptions of majordisorders and links to many high quality mental health andAOD-related siteswww.mentalhealth.com
Devoted to the psychopharmacology with a very wide range oflinks: academic, lay and weirdwww.biopsychiatry.com/refs
www.aidscouncil.org.au
www.hepatitisc.org.au
www.ceida.net.au
88
www.mims.com.au
www.psychnet-uk.com/addictions_and_drugs/psychopharmacology1.htm
http://165.112.78.61/Teaching/Teaching.html
Drug Info Clearinghouse – The drug prevention networkhttp://druginfo.adf.org.au
The Australian Drug Foundation (ADF):www.adf.org.au/index.htm
The Centre for Youth Drug Studies is within the ADF:www.adf.org.au/cyds/index.html
The Alcohol and Other Drug Council of Australia (ADCA):www.adca.org.au/
The National Drug and Alcohol Research Centre (NDARC):www.med.unsw.edu.au /ndarc/
The Centre for Education and Information on Drugs and Alcohol(CEIDA): www.ceida.net.au/
The Network of Alcohol and Drug Agencies (NADA):www.nada.org.au
Drug Arm (This site is particularly focused on youth issues):www.drugarm.org.au
The Australian Drug Information Network:www.adin.com.au
89
Key terms
Abstinence Refraining from drug use.
Amphetamine Behavioural stimulant.
Antabuse Trade name for disulfiram, a drug that interferes with thebreakdown of alcohol, resulting in the accumulation ofacetaldehyde.
Antagonist Drug that attaches to a receptor and blocks the action of either anendogenous transmitter or an agonist drug.
Antidepressant Drug that is useful in treating mental depression in depressedpatients but does not produce stimulant effects in normal persons.
AOD Alcohol and/or other drugs
Barbiturates Class of chemically related sedative-hypnotic compounds thatshare a characteristic six-membered ring structure.
Benzodiazepines Class of chemically related sedative-hypnotic agents of whichchlordiazepoxide (Librium) and diazepam (Valium) are examples.
Bipolar disorder Affective disorder characterised by alternating bouts of mania anddepression. Previously referred to as manic-depressive illness.
Brand name Unique name licensed to one manufacturer of a drug. Contrastswith generic name, the name under which any manufacturer maysell a drug.
Caffeine Behavioural and general cellular stimulant found in coffee, tea, coladrinks and chocolate.
Cannabis Plant that contains marijuana.
Central nervoussystem (CNS)
Brain and spinal cord.
Cirrhosis Serious, usually irreversible liver disease. Usually associated withchronic excessive alcohol consumption.
90
Key terms (continued)
Cocaine Behavioural stimulant.
Codeine Sedative and pain-relieving agent found in opium. Structurallyrelated to morphine but less potent.
Crack Street name for a smokable form of potent, concentrated cocaine.
Deliriumtremens
Syndrome of tremulousness with hallucinations, (DT’s, ‘rum fits’)psychomotor agitation, confusion and disorientation, sleepdisorders and other associated discomforts, lasting several daysafter alcohol withdrawal.
Depressants Drugs that slow down the brain and central nervous system.
Detoxification Process of allowing time for the body to metabolise and/or excreteaccumulations of a drug. Usually a first step in drug abuseevaluation and treatment.
Drug Within the context of this course, a drug is a substance thatproduces a psycho-active effect (i.e. changes in mood or behaviourdue to alterations in brain function).
Drug absorption Mechanism by which a drug reaches the bloodstream from theskin, lungs, stomach, intestinal tract, or muscle.
Drugdependence
Occurs when a drug becomes central to a person’s thoughts,emotions and activities. A dependent person finds it difficult to stopusing the drug or even to cut down on the amount used.Dependence has physiological and psychological elements.
Drug half-life The time it takes for 50 percent of a drug to be metabolised into aninactive substance and/or eliminated from a person’s body.
Drug interaction Modification of the action of one drug by the concurrent or prioradministration of another drug.
Drug misuse Use of any drug (legal or illegal) for a medical or recreationalpurpose when other alternatives are available, practical, orwarranted or when drug use endangers either the user or others.
91
Key terms (continued)
Generic name Name under which any manufacturer may sell a drug.
Hallucinogens Drugs that act on the brain to distort perception, (i.e. sight, taste,touch, sound or smell).
Harmminimisation
Harm minimisation is the primary principle underpinning theNational Drug Strategy and refers to policies and programs aimedat reducing drug-related harm. It encompasses a wide range ofapproaches including abstinence-oriented strategies. Both legaland illegal drugs are the focus of Australia’s harm minimisationstrategy. Harm minimisation includes preventing anticipated harmand reducing actual harm.
Harm reduction Harm reduction aims to reduce the impact of drug related harm onindividuals and communities. It includes those strategies designedto reduce the harm associated with drug use without necessarilyreducing or stopping use.
Hashish Extract of the hemp plant (Cannabis sativa) that has a higherconcentration of THC than does marijuana.
Heroin Semisynthetic opiate produced by a chemical modification ofmorphine.
Intoxication Any change in our perception, mood, thinking processes and motorskills as a result of the impact of a drug(s) on our central nervoussystem.
Majortranquillizer
Drug used in the treatment of psychotic states (antipsychotictranquillizer).
Marijuana Mixture of the crushed leaves, flowers, and small branches of boththe male and female hemp plant (Cannabis sativa).
Morphine Major sedative and pain-relieving drug found in opium, comprisingapproximately 10 percent of the crude opium exudate.
Neuron The basic nerve cell of the nervous system which transmits nerveimpulses to and from the body and the brain.
Neurotransmitter Endogenous chemical released by one neuron that alters theelectrical activity of another neuron.
92
Key terms (continued)
Nicotine Behavioural stimulant found in tobacco which is responsible for thepsychedelic effects of tobacco and for tobacco dependence
Opioid Natural or synthetic drug that exerts actions on the body similar tothose induced by morphine, the major pain- relieving agentobtained from the opium poppy (Papaver somniferum).
Opium Rude resinous exudate from the opium poppy.
Overdose Use of a drug in an amount that causes acute adverse physical ormental effects. Overdose may produce transient or lasting effectsand can sometimes be fatal.
Pharmaco-dynamics
Study of the interactions of a drug and the receptors responsible forthe action of the drug in the body.
Pharmacokinetics Study of the factors that influence the absorption, distribution,metabolism, and excretion of a drug.
Pharmacology Branch of science that deals with the study of drugs and theiractions on living systems.
Physicaldependence
State in which the use of a drug is required for a person to functionnormally. Confirmed by withdrawing the drug and noting theoccurrence of withdrawal symptoms (abstinence syndrome).Characteristically, withdrawal symptoms can be terminated byreadministration of the drug.
Placebo Pharmacologically inert substance that may elicit a significantreaction largely because of the mental ‘set’ of the patient or thephysical setting in which the drug is taken.
Poly-drug use The use of more than one psycho-active drug, simultaneously or atdifferent times. The term ‘poly-drug user’ is often used todistinguish a person with a varied pattern of drug use fromsomeone who uses one kind of drug exclusively.
Potency Measure of drug activity expressed in terms of the amount requiredto produce an effect of a given intensity. Potency varies inverselywith the amount of drug required to produce this effect − the morepotent the drug, the lower the amount required to produce theeffect.
93
Key terms (continued)
Psychologicaldependence
Compulsion to use a drug for its pleasurable effects. Suchdependence may lead to a compulsion to misuse a drug.
Psycho-pharmacotherapy
Clinical treatment of psychiatric disorders with drugs
Receptor Location in the nervous system at which a neurotransmitter or drugbinds in order to exert its characteristic effect
Route ofadministration
Method used to take drugs into the body. Includes oral (via themouth); injection (intravenous, intramuscular, subcutaneous);inhalation (via the lungs); mucous membrane absorption (nasal,under the tongue, anal/rectal); dermal/topical (skin patches orcream).
Side effect Drug-induced effect that accompanies the primary effect for whichthe drug is administered.
Stimulants Drugs that speed up the brain and nervous system.
Tolerance Occurs when a person needs increased doses of a drug to obtainthe same effect as the body adapts to the presence of the drug.Tolerance develops more quickly if use is frequent and heavy.
Toxic effect Adverse drug-induced effect (temporary or permanent) on anyorgan or system of an animal or person. Includes both therelatively minor side effects that invariably accompany drugadministration and the more serious and unexpectedmanifestations that occur in only a small percentage of patientswho take a drug.
Withdrawalsymptoms
Symptoms that can occur when a person using a drug over aprolonged period reduces or ceases use.
![Home [] · Web view2020. 8. 29. · Dear TeacherProvided herewith is a Learner’s Project Workbook and a set of Teacher’s Project Notes for the School- Based Assessment (SBA)](https://img.pdfslide.us/doc/110x75/614944f7080bfa6260148079/home-web-view-2020-8-29-dear-teacherprovided-herewith-is-a-learneras.jpg)




























