Embed Size (px)
Citation preview

Leaders in Managing Lipids for
Improved Cardiovascular Health
INVESTOR PRESENTATION
June 2015
Nasdaq: AMRN

2
Forward-Looking Statement and Disclaimer
This presentation contains forward-looking statements, such as those relating to the
commercial potential of Vascepa®, Amarin’s product development, clinical and
regulatory efforts and timelines, potential FDA approvals, intellectual property, cash
flow, and other statements that are predictive in nature and that depend upon or refer
to future events or conditions. These statements involve known and unknown risks,
uncertainties and other factors that can cause actual results to differ materially.
Investors should not place undue reliance on forward-looking statements, which
speak only as of the presentation date of this presentation. Please refer to the “Risk
Factors” section in Amarin’s most recent Quarterly Report on Form 10-Q filed with the
SEC for a more complete description of risks of an investment in Amarin.
Vascepa® (icosapent ethyl) capsules are FDA approved for use as an adjunct to diet
to reduce triglyceride (TG) levels in adult patients with severe (TG >500 mg/dL)
hypertriglyceridemia (commonly known as very high TGs).
This presentation is intended for communication with investors only. Nothing in this
presentation should be construed as marketing the use of Amarin’s product or
product candidates.

3
Amarin: Blockbuster Opportunity and Growing Revenues
Upcoming: Cardiovascular outcomes data on
Vascepa® (>96% ethyl-EPA1) as add-on to statins
REDUCE-IT CV outcomes study >93% enrolled
Events driven study incorporates learnings from positive
JELIS (Japan CV outcomes study of EPA) and others
Leverages strong lipid efficacy & safety profile: two Phase 3s
Studying at-risk patients with persistent elevated triglycerides
CV outcomes results expected 2018, potentially 2016
Today: Marketing Vascepa for very high TGs
U.S. launch in 2013
$54M in revenues in 2014 and growing
Marketing concentrated on top physician targets
Co-promotion partner Kowa Pharmaceuticals America added
in mid-2014 adds to Amarin’s 130 sales reps
Addressing chronic patient condition
1EPA: eicosapentaenoic acid, a unique polyunsaturated omega-3 fatty acid

4
Cardiovascular Risk: Significant Unmet Need
Cardiovascular Disease: #1 cause of death in the United States
>700,000 people die of heart disease in the United States every year
‒ Represents ~1 in every 3 deaths (AHA Heart and Stroke Statistics)
Heart attacks, stroke and other CV disease are expensive to treat
‒ Estimated annual total cost of >$300 billion
Standard of care first therapy beyond diet and exercise: Statins
$40.2 billion annual market at its height
Statins target LDL-C and are reported to have other “pleiotropic” effects such as:
‒ Improving endothelial function
‒ Enhancing the stability of atherosclerotic plaques
‒ Decreasing oxidative stress and inflammation
Statins lower coronary heart disease risk by up to 25 to 40%

5
Seeking Solution to Address Residual Cardiovascular Risk
Limited success in prior CV outcomes studies with statin add-on therapies Ezetimibe (IMPROVE-IT):
‒ ~6% additional risk decline
‒ Focus on additional LDL-C lowering, other lipid reductions
Fenofibrate (ACCORD-Lipid)
‒ No benefit in general population of low HDL-C patients
‒ Benefit trend seen in high TG, low HDL-C subset population
Niacin: HDL-C increase focus (AIM-HIGH and HPS2-THRIVE)
‒ No benefit in the AIM-HIGH general population of low HDL-C patients
‒ In AIM-HIGH, benefit seen in high TG, low HDL-C subset population
‒ No benefit in the HPS2-THRIVE population with half of the patients having low
HDL-C
Exception: 19% to 53% risk reduction in Japan-based study Ethyl-EPA (JELIS):
‒ Benefit shown in general population of statin treated patients
‒ Greater benefit in patient subpopulation with high TG and low HDL-C

6
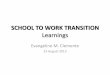
Ethyl-EPA Reduced Coronary Events 19% to 53% on
Top of Statin Therapy in Japan Outcomes Study (JELIS)
Patients Randomized to Statin Alone or Statin + Ethyl-EPA (Epadel) and Followed
for 5 Years with Comparison of Cumulative Incidence of Major Coronary Events
–53%
HR: 0.4795%CI: 0.23-0.98(p=0.043)
0 1 2 3 4 50
1
2
3
4
5
Years5210 3 4
3
0
1
2
4 Control (statin)
EPA (statin+Epadel)
Years
TOTAL COHORTNo pre-specified minimum TG level TG>150 mg/dL and HDL<40 mg/dL
SUB GROUP
N=957
Control (statin)
EPA (statin+Epadel)
Control (statin)
EPA (statin+Epadel)
Source: Yokoyama M. et al, Lancet 2007; 369:1090-1098
P value adjusted for age, gender, smoking, diabetes, and hypertension.
CI=confidence interval.
Source: Saito et al, Atherosclerosis 2008; 200: 135-140
N=18,645(p=0.011)
-–19%
Cum
ula
tive I
ncid
ence o
f M
ajo
r C
oro
nary
Events
(%
)
Cum
ula
tive I
ncid
ence o
f M
ajo
r C
oro
nary
Events
(%
)

7
Ethyl-EPA: Lowers Triglycerides (TGs)
Plus Spectrum of Other Lipid and Pleiotropic Effects
Triglycerides (fat in blood) lowered Studied by Amarin in two Phase 3 studies
‒ MARINE trial: TGs >500mg/dL and ANCHOR trial: TGs 200-499mg/dL on statins
Also significantly lowered other key lipid parameters including total cholesterol,
Non-HDL-C, Apo-B, Apo-CIII, VLDL-C and remnant-like particle cholesterol
Did not increase LDL-C (bad cholesterol)
Pleiotropic effects of EPA beyond lipid improvements1
Improves endothelial function ‒ Alone and in combination with statin therapy
Anti-inflammatory effects ‒ Lowers Lp-PLA2 and hsCRP (>14% and >22% declines, respectively, vs. placebo in
Phase 3 Vascepa studies)
Anti-oxidant effects ‒ More potent antioxidant than historically used TG-lowering therapies and vitamin E
Inhibits formation of cholesterol crystalline domains; disrupts existing domains
‒ No other TG-lowering therapy has been shown to share all these effects
1Pleiotropic effects based on clinical and non-clinical scientific literature

8
Lowering TGs in Patients with Baseline TG>150 mg/dL and low HDL-C in Outcomes Studies Suggests Double Digit Relative Risk Reduction (RRR) on Top of Statin Therapy
Trial
Publication
Year
Therapy
Subgroup
Size
(N)
Statin
Use
Through-
out
Subgroup
PublishedEndpoint
Subgroup
RRR
(p-value)
JELIS
2007EPA 957 Yes
TG ≥150 mg/dL
HDL-C ≤40 mg/dL
Expanded
MACE
-53%(0.043)
ACCORD-
Lipid
2010
Fenofibrate 941
Delayed
start (inflates starting
baselines)
TG ≥204 mg/dL
HDL-C ≤34 mg/dLMACE
-31%(0.0567)
AIM-HIGH
2011Niacin ER 523 Yes
TG ≥ 200 mg/dL
HDL-C <32 mg/dL
Expanded
MACE
-36%(0.032)
HPS2-
THRIVE
2013
Niacin +
Laropiprant4,362 Yes
TG ≥151 mg/dL
HDL-C <35 mg/dL
Major
vascular
events
No
significant
difference
CONFIDENTIAL

9
Genetic Studies: TG Levels Predict Heart Disease (CHD)
Predictor
CHD Risk
Effect Size Perspective P-value
TG 0.40 TGs and LDL-C
levels are
comparably strong
predictors of CHD
<<<0.0001
LDL-C 0.39 <<<0.0001
HDL-C 0.04HDL-C is weak
predictor0.32
Modified from:
Do R et al. Nat Genet. 2013;45(11):1345-1352 (N=86,995);

10
Broad Data Supports Link Between TGs and CV Risk
• Epidemiological, genetic, and clinical data suggest that TGs and the lipoproteins that carry them are within the
causal pathway of CV disease, and that treating elevated TGs may result in reduced CV risk.

11
Amarin: Positioned with First Outcomes Study of Ethyl-
EPA as Add-on to Statin Outside of Japan
Purpose of REDUCE-IT cardiovascular outcomes study: Evaluate effectiveness of Ethyl-EPA (Vascepa) in reducing cardiovascular events
in at risk patients
FDA has strongly urged Amarin to complete REDUCE-IT outcomes study
Addresses unanswered medical questions; 1st outcomes study designed to
prospectively evaluate each of: TG-lowering in patients with elevated TGs despite statin therapy
Ethyl-EPA on top of statins in a broad-based patient population
CV outcomes benefit in REDUCE-IT to be measured by: Randomizing statin treated patients to placebo and to Ethyl-EPA (Vascepa)
Measuring cumulative incidence of major CV events (death, myocardial infarction,
stroke, coronary revascularization and hospitalization for unstable angina)
Comparing cumulative first CV events in active vs. placebo trial arms

12
REDUCE-IT Approaching Key Milestones
DESIGN
SPA Agreement reached with FDA in 2011
– ~8,000 Patients on optimized statin therapy
– Population with CVD or “at Risk,” incl. TGs
>150 mg/dL
– 90% power to detect 15% relative risk
reduction (>95% power to detect >20% relative
risk reduction)
– Amarin blind to ongoing trial results
STATUS
>7,400 patients enrolled (>93% of target)
Enrollment completion anticipated in 2015
– Enrolling in 11 countries at >450 clinical sites
– Safety data reviewed throughout study by DMC
– Mean and median baseline TG of >200 mg/dL
(higher than levels enrolled for recent outcome
studies of other lipid modifying therapies)
TIMING
Complete at 1,612 composite MACE events
– First patient randomized November 2011
– Interim efficacy look ~2016
By independent data monitoring committee, DMC,
pre-specified at 967 events (60% of target events)
– Completion of 100% of target events ~2017
– Publication ~2018
OPPORTUNITY
Incremental risk reduction beyond statin
therapy
Positioned to address patient populations of
>70 million in U.S. alone; billions of dollars
Unique product profile

13
REDUCE-IT and JELIS Study Design Differences
“Enriched” Patient Population in REDUCE-IT
REDUCE-IT: all patients have elevated TG’s and other CV risk factors despite statin therapy
– Mean and median baseline TG’s >200 mg/dL and ~1/2 of patients expected to also have low HDL
JELIS: many patients had normal TG levels and a 19% risk reduction was achieved
– Published subgroup with 53% risk reduction population had TG >150 mg/dL and low HDL
Higher Treatment Dose in REDUCE-IT
REDUCE-IT 4 grams/day of ethyl-EPA (Vascepa); JELIS 1.8 grams/day of ethyl-EPA
In 12-week Phase 3 ANCHOR study, 4 grams/day of Vascepa increased EPA at the plasma
level to the same level as achieved with 1.8 grams/days of ethyl-EPA in JELIS
– Difference likely due to high fish diet in Japan
– EPA levels in REDUCE-IT control likely lower than JELIS due to dietary differences outside Japan
Statin therapy targeted to goal in REDUCE-IT and JELIS
– REDUCE-IT LDL-C target <100 mg/dL; JELIS LDL-C target <130 mg/dL; studies of statin therapy
demonstrated similar outcome results in Japan at <130 mg/dL to Western populations at 100 mg/dL
REDUCE-IT is a Global Study
REDUCE-IT: enrollment in 11 countries including strong participation in the United States;
randomized double blinded study
JELIS: Japan only, mostly women; open label, randomized with blinded endpoint analysis

14
Elevated TGs More Prevalent than Elevated LDL-C
Tens of millions of people have lipid disorders 13.1% of U.S. adults have elevated LDL-C
25.1% of U.S. adults have above normal TGs
Lipid disorders contribute to atherosclerosis,
heart disease, pancreatitis and other health
issues
REDUCE-IT: Focused on statin treated patients
with persistently elevated TG levels and other
CV risk factors
Seeking right to promote Vascepa as add-on to
statin therapy, not replace statin therapy
0%
5%
10%
15%
20%
25%
30%
LDL-C>130
mg/dL
TG>150
mg/dL
LDL-C and TG Prevalence in Adults
(U.S.)
Source: NHANES 2009-2012

15
67%
15% 16%
2%
0-149 mg/dL 150-199 mg/dL 200-499 mg/dL 500-2000 mg/dL
Large Underpenetrated Market Opportunities
150 Million
People
34 Million
People
36 Million
People3.8 Million
People
MARINEStudy
Only 3.6% Treated with Rx Meds
>100M People in Top 7 Global Markets for Initially-Targeted Indications
Source: Datamonitor and Archives of Internal Medicine, 2009;169(6):572-578
ANCHOR Study
Current
Indication*
REDUCE-IT
Outcomes Study
Includes Statin-treated
Patients in Ongoing
U.S. Adult Population Stratified Based on TG Levels
*Current indication for Vascepa; same as Lovaza®
TG levels:
U.S
. Ad
ult
Po
pu
lati
on

16
TGs
LDL-C
Vascepa: Potential to Redefine Lipid Management Therapies
Vascepa: New Paradigm in Cardiovascular Health
Traditional Cholesterol
Management Priority
Historically Limited TG
Treatment Options
New Generation
TG Lowering w/o LDL-C Increase(LDL-C decrease in ANCHOR vs. placebo)
LDL-C
HDL-C
LDL-CTGs
LIPID
PARAMETERS
KEY
TREATMENTS Statins, Niacin, Fibrates Fibrates, Other Prescription
Omega-3 which contain DHA
Amarin’s
FOCUS
Note: Arrows show direction only—not to scale
®

17
Vascepa: Lowers TGs and Other Lipid Markers
Very High TGs (≥500 mg/dL)
◼ All Primary Endpoints Achieved
◼ Favorable Safety and Tolerability Profile
◼ Favorable Effect on Other Endpoints (Total Cholesterol, VLDL-C)
-33%
-18%
-2%*
Phase 3 Results: MARINE Trial (4g/day dose)
Supported FDA Approved Indication (median placebo-adjusted data)
TG Non-HDL-C LDL-CTG >750
mg/dL
-45%
Note: median % change versus placebo at week 12 *=not significant
Ref: American Journal of Cardiology 2011; 108:682–690.
Apo B
-9%
Only reported adverse reaction across the clinical profile for
Vascepa with an incidence > 2% and greater than placebo in
Vascepa treated patients was arthralgia (2.3% for Vascepa,
1.0% for placebo)

18
Vascepa: Lowers TGs and Other Lipid Markers
High TGs (200 – 499 mg/dL) on Statin Therapy
◼ All Primary and Secondary Endpoints Achieved
◼ Favorable Safety and Tolerability Profile
◼ Favorable Effect on Other Endpoints (Total Cholesterol, VLDL-C)
Phase 3 Results: ANCHOR Trial (4g/day dose)
Indication not approved by FDA (median placebo-adjusted data)
TG Non-HDL-C LDL-C
Note: median % change versus placebo at week 12
Apo B
Ref: American Journal of Cardiology 2012;110:984-992
-22%
-14%
-6%
-9%
Only reported adverse reaction across the clinical profile
for Vascepa with an incidence > 2% and greater than
placebo in Vascepa treated patients was arthralgia
(2.3% for Vascepa, 1.0% for placebo)

19
Vascepa: Not Fish Oil, Pure EPA
Additional omega
6, 7 & 9 (100mg)
Other
Omega-3
Acid Ethyl
Esters
(60mg)
Ethyl DHA
(375 mg)
Ethyl EPA
(465 mg)
fatty
acids
~30 mg
Ethyl-EPA
(>960 mg)
APPROVED INDICATION
TG >500 mg/dL Marketed since 2004 (generic 2014) Marketed since 2013
LDL-C effect* Elevated LDL-C over 49% No Elevation (LDL-C reduction in ANCHOR study)
NON-HDL-C effect* Reduced 10.2% Reduced 17.7%
Total cholesterol effect* Reduced 8.0% Reduced 16.3%
Additional biomarkers*Limited, Variable or Not Characterized
in Label for Approved IndicationAdditional Beneficial Effects
Taste/eructation* Fishy Taste / Smell / Burp None
Atrial fibrillation warning* Added to package insert None
OTHER INDICATION POTENTIAL
TG >200 mg/dL and <500 mg/dLStudied, LDL-C Endpoint Not Achieved
(No Outcomes Study for Population)
Biomarker Endpoints Achieved
(Outcomes Benefit Being Studied in REDUCE-IT)
TG >150 mg/dL Not Studied Being Studied in REDUCE-IT
VASCEPA Icosapent Ethyl (Pure EPA)
*median placebo adjusted data and other info from FDA approved package inserts in TG >500 mg/dL patients
Earlier Generation Rx TherapyA Complex Mixture of Fatty Acids

20
Vascepa: Marketed in U.S. for Treating
Patients with Very High TGs (>500 mg/dL)
130 Amarin sales reps target high prescribing
physicians of earlier generation therapy Augmented since mid-2014 with co-promotion by
Kowa Pharmaceuticals America
Wholesale price $221 per month (120 capsules;
daily dose 4 capsules per day) $9 co-pay card for patients
Vascepa price at parity to generics of prior
generation omega-3 on net basis for most payors
>125M lives on tier 2
Competes on a basis of broad efficacy and
placebo-like safety and tolerability Works alone or as add-on to statin therapy
Doesn’t work against LDL-C lowering of statins
>29,000 prescribers
$-
$10
$20
$30
$40
$50
$60
2012 2013 2014
Vascepa Net Revenues (millions)

21
Vascepa Future Growth Potential
Early stages of marketing Vascepa for current indication Prior generation therapy grew to $1B drug based on same indication, despite
it increasing LDL-C
Applying lessons learned from first two years of launch for Amarin (Kowa’s co-
promotion is in early stages)
International expansion In February 2015, executed licensing partnership for Vascepa in China
‒ Received $15M up-front payment with the potential for $154M in additional
milestones plus tiered double digit royalties on future revenues
‒ Partner funding China regulatory approval
Reviewing other ex-US opportunities
Seeking broader opportunities to market Vascepa REDUCE-IT cardiovascular outcomes study
Pursuing judicial authority to promote truthful and non-misleading data to
physicians regarding ANCHOR study and EPA effects on CV risk while
REDUCE-IT is ongoing (1st Amendment suit)

22
Amarin Priorities for 2015
Grow Revenues from Current Vascepa Label
Leverage Vascepa clinical experience and expanded tier 2 coverage
Ensure focus and high sales call volume on highest potential prescribers
Increasing Vascepa experience and outreach from co-promotion partner (Kowa)
Tier 2 coverage for branded Lovaza disappears in 2015; generic Lovaza is expensive
Increase awareness of Vascepa efficacy, safety and tolerability profile
REDUCE-IT Outcomes Study
Complete enrollment in 2015
Prepare for interim look by independent DMC in 2016
Cost-Effectively Advance Other Opportunities
Evaluate additional Ex-US opportunities for Vascepa and consider strategic options
without losing focus on other priorities
Feasibility established for fixed-dose combination of Vascepa with leading statin
(AMR102); work to accelerate closer to completion of REDUCE-IT study
Further document Vascepa patient successes showing positive clinical effect of
switching patients to Vascepa from other TG lowering therapy

23
Capitalization Summary (in Millions)
As of March 31, 2015, except as noted
1 The total remaining cash payments due on this debt are $142.7 million which is a fixed amount and includes the
contractual interest paid quarterly at 10% of Vascepa revenues subject to quarterly maximum amounts. Lower carrying
value reported for accounting purposes per GAAP.2 Total principal of $150.0 million has put provisions for $31 million in Jan 2017 and $119 million in Jan 2019. Notes accrue
3.5% interest, paid semi-annually. Lower carrying value reported for accounting purposes per GAAP. 3 Includes 35.2 million common share equivalents issuable upon conversion of preferred shares issued in March 2015
Cash $161.2M
Debt Obligations
ROYALTY-LIKE DEBT1 $142.7M Carrying value $90.1M for accounting purposes
EXCHANGEABLE SENIOR NOTES2 $150.0M Carrying value $123.2M for accounting purposes
Common Stock and Equivalent Shares (Millions, Except per Share Amounts)
COMMON/PREFERRED SHARES3 212.2 Preferred shares mirror common but non-voting
OPTIONS 12.1 Average Exercise Price of $4.95
RESTRICTED STOCK UNITS 4.1
TOTAL IF ALL EXERCISED 228.4
TAX JURISDICTION (PRIMARY) Ireland12.5% Tax Rate
(Est. Global Blended Rate 15%)

24
Investment Highlights
Leading a New Paradigm in Cardiovascular Health Management
• Multi-billion dollar potential with REDUCE-IT outcomes study
• FDA approved for severe hypertriglyceridemia (TG >500 mg/dL)
• Multiple underserved patient populations with elevated TG levels
Large Global
Sales Potential
Differentiated Product • TG reduction -- no increase, or a decrease, in LDL-C
• Reductions in apo B, non-HDL-C, VLDL-C and total cholesterol
• Safety comparable to placebo
• Growing sales productivity; growing managed care coverage
• Phase 3 trials completed–all primary endpoints achieved
• Recently announced licensing partnership for Vascepa in China
• Outcomes study >93% enrolled and positioned for success
Positive Execution
• Grow revenues through specialty sales focus
• Seek broader promotional opportunities for Vascepa
• Cost-effectively advance other opportunities
Commercialization
Strategy
• Team with history of product development and commercial successes
• Direct sales team of 130 sales representatives, excluding sales managers
• Amarin team supplemented by 250 Kowa sales representatives
Experienced
Management
.

Leaders in Managing Lipids for
Improved Cardiovascular Health
INVESTOR PRESENTATION
June 2015
Nasdaq: AMRN
![Prostaglandins and Other Lipid Mediatorsnlaresourcecenter.lipidjournal.com/Content/PDFs/Bays-Icosapent.pdf · [26,27]. In the Japan EPA Lipid Intervention Study (JELIS), ethyl icosapentate](https://img.pdfslide.us/doc/110x75/5cd6b69488c993ea4e8ddcf8/prostaglandins-and-other-lipid-mediat-2627-in-the-japan-epa-lipid-intervention.jpg)