Embed Size (px)
Citation preview

LC-MS/MS
Ross Molinaro, PhD, MT(ASCP), DABCC, FACB Emory University
Atlanta, GA

Learning Objectives
After this presentation, you should be able to: 1. List requirements for clinical laboratory methodologies. 2. Describe liquid chromatography tandem mass
spectrometry (LC-MS/MS). 3. Discuss advantages and challenges associated with
immunosuppressant testing by immunoassay and LC-MS/MS.
4. Describe the importance of patient comparisons when transitioning between immunoassay and LC-MS/MS for immunosuppressant testing.

Throughput
Automation
Ease of Use Sensitivity
Accuracy
Selectivity
Requirements of Clinical Laboratory Methodology

Choosing Mass Spectrometry
Define your assay requirements
Define your analytes and understand any alternative approaches
Identify a mass spectrometer
Test compounds
Visit other labs

Can You Measure Your Analyte of Interest Using Mass Spectrometry?
• Do you have access to the AOI?
• Have others done this already?
• Does it “fly” (ionization mode)?
• Are the calibrators/IS available?
• Is it financially viable?
• What are the clinical needs?

Immunosuppressants 2003: What Were Other Labs Doing?
Reference Laboratories Methodology Quest HPLC and TDx (by request)
Mayo Labs HPLC + LC- MS/MS
Lab Corp LC- MS/MS ARUP LC - MS/MS
Academic Centers Methodology MUSC LC - MS/MS UNC LC - MS/MS
Univ. of Mich. LC - MS/MS Univ. Penn HPLC (LC - MS for C2 protocols)
Univ. Washington (Seattle) Children’s
TDX
Duke LC - MS/MS

2003 Immunosuppressant Testing
• Rapamycin TAT 1 to 4 days • Expecting volume to increase substantially in future • Each drug is a separate analysis, no opportunity for multiplexing • Total cost to system over 7 years = $1,974,931
Measurand Volume / yr Cost / Analysis Cost / yr
Cyclosporine 7588 $10.80 $81,950 Tacrolimus 13120 $12.00 $157,440 Rapamycin 744 $ 57.45* $42,743
TOTALS 21,452 $282,133 *Sendout-Mayo Labs

LC-MS/MS Proposal
Measurand Volume / yr Cost* / Analysis Cost / yr
Cyclosporine 7588 $6.35 $48,184 Tacrolimus 13120 $6.35 $83,312 Rapamycin 744 $6.35 $4,724
TOTALS 21,452 $136,220 * Cost includes reagents, labor, & instr. depreciation
• All drug TATs within 1 day • Capable of expanding to meet increased need • Runs are multiplexed • Total cost to system over 7 years = $953,540 • Saving to system over 7 years = $1,021,391 • Provides opportunities to do other assays

Process for Developing a Clinical Method
• Method Selection • Selection of Key Operator • Outline/plan methods • Acquisition of materials • Set quality goals • Validation • Monitoring and statistics • SOP preparation, staff training
Make an Implementation Plan Validate the Method
• Imprecision • Recovery • Linearity • Sensitivity • Specificity • Interferences • Specimen • Method Comparison • Assay Calibration

Clarke W, Rhea J, Molinaro R. 2013. Journal Mass Spec (In press)

LC-MS/MS Analyses • Most current methods are Lab Developed Tests (LDT)
– Resources: • Develop from scratch • Previously validated method from colleagues • Literature • Vendors • Most variation between labs related to differences in
methods & standards
• CLIA – High Complexity
NOTE: College of American Pathology (CAP) is now asking labs to list all their LDTs in preparation for their CAP inspections

Useful Resources
CLSI Guidelines – EP10 Preliminary Evaluation of Quantitative Clinical Laboratory
measurement Procedures
– EP15 User Verification of Performance for Precision and Trueness
– EP05 Evaluation of Precision Performance of Quantitative Measurement Methods
– EP06 Evaluation of the Linearity of Quantitative Measurement
– EP09 Method Comparison and Bias Estimation
– GP31 Laboratory Instrument Implementation, Verification, and Maintenance
– EP50 Mass Spectrometry in the Clinical Laboratory
– EP60 (in development)

Issues Unique to LC-MS/MS Analyses • Matrix Effects
• Differential ionization of Internal Standards or Calibrators
• In Source Transformation (fragmentation)
• Isobaric Compounds and Isomers
• Cross-Talk effects
• Chromatographic Resolution
• Carry-Over
Vogeser & Seger, 2010, Clin Chem http://www.clinchem.org/cgi/doi/10.1373/clinchem.2009.138602

High Performance Liquid Chromatography (HPLC)
Detection
Time P
eak
Hei
gh
t
HPLC Column
Mobile phases

MS/MS Detection
HPLC outlet Electrospray
ionization Selected
precursor ion(s)
+ve
+ve
+ve
Selected product ions
Quadrupole 1 select m/z
Quadrupole 2 collision cell
Quadrupole 3 product ion scan
Transitions

Sample Preparation • Matrix: Serum, whole blood, urine
• Pretreatment process
– Protein Precipitation Protocols: Fast & easy however associated with longer periods of ion suppression due to early eluting, low molecular weight matrix constituents
– Solid-Phase Extraction & Liquid-Liquid Extraction: Slower & more chance for error. Do have shorter periods of ion suppression.
Vogeser & Seger, 2010, Clin Chem http://www.clinchem.org/cgi/doi/10.1373/clinchem.2009.138602

In Source Transformation/ Fragmentation: • Fragmentation occurring after
column separation but before collision cell (mycophenolic acid; MPA) – MPA-G > MPA > MPA Fragment – MPA-BE > MPA > MPA Fragment
• Can be a problem with endogenous drug metabolites – Check real patient samples in extended
chromatographic runs

Isobaric Compounds & Isomers • Isobaric: same molecular weight • Extremely important when measuring
endogenous analytes • Mandates complete chromatographic
resolution
Cross-Talk •Occurs when several mass transitions with identical product ions are acquired over a short time interval.
•If collision cell does not empty completely spurious signals can be recorded in a subsequent trace
•Common when several metabolites of a single drug are detected with identical fragment ions
•Solution: Increase interscan delay

Immunosuppressant Drugs by LC-MS/MS – Protocol (circa 2004)
Microfuge tube protocol. 1. In a 1.5mL Eppendorf tube accurately pipette:
50µL Lysis Solution A (0.4M ZnSO4) 200µL whole blood (Calibrators, QCs or patient samples)
2. Briefly vortex mix samples (5 – 10sec)
3. Add 500µL of Precipitating Solution (25ng/mL Ascomycin + 100 ng/mL CycloD in acetonitrile)
4. Vortex mix for approximately 1 minute or until the entire sample is thoroughly mixed
5. Centrifuge for 5 minutes at 14,500rpm
6. Cut top off of micro-centrifuge vial. Place vial into HPLC autosampler
7. Inject 10µL on the LC-MS/MS system. Use C-18 column (4X3mm – Phenemonex)

Immunosuppressant Drugs by LC-MS/MS - Protocol
Compound
Precursor Ion
Product Ion
Cyclosporine A 1220 1203
Tacrolimus 821.5 768.5
Rapamycin 931.6 864.5 Ascomycin 809.5 756.4
Cyclosporine D 1234.1 1217.2

Ascomycin, FK-506, Rapamycin
Cyclosporine A & D
Immunosuppressant Standard (20/20/500 ng/mL)

Immunosuppressant Standard (20/20/500 ng/mL)
Cyclosporine D
Cyclosporine A
Rapamycin
FK-506
Ascomycin

Immunosuppressant Drugs by LC-MS/MS - Limits
Compound
LOD (ng/mL)
LOQ (ng/mL)
Linearity (ng/mL)
Tacrolimus 0.1 0.6 40
Cyclosporine A 3.0 10 1000
Rapamycin 0.3 0.6 40

Immunosuppressant Drugs by LC-MS/MS - Imprecision
Interassay Tacrolimus Cyclosporine A Rapamycin
Concentration (ng/mL)
4 90 4
%C.V. 7 10 13
Intra-assay %C.V. 2 7 9

Matrix effects 1. Prepare extracts on 5 random blood samples from patients not receiving an
IS drug. 2. Prepare 2 extracts using water as matrix. 3. To 500 uL of each extract add 150 ng Cyclo A, 75 ng Cylo D, 15 ng FK-506, 15
ng Rapa, and 20 ng Asco (all in 50ul). 4. Compare whole blood recoveries from water.
FK-506 (Area)
Cyclo A (Area)
Rapa (Area)
Asco (Area)
Cyclo D (Area)
Water 3651 75885 1267 8578 36918
#1 4241 77293 1580 8650 38890
#2 4834 71217 1317 8787 34821
#3 4486 73005 1359 8218 27974
#4 4836 71500 1360 9023 36014
#5 4394 75963 1402 8225 32160
Blood mean 4559 73796 1404 8581 33972
Recovery 125% 97% 111% 100% 92%

AMR & CRR
AMR (ng/mL)
CRR (ng/mL)
Cyclosporine A 100 - 1000 10 - 2000
FK-506 0.3 - 40 0.3 - 80 Rapamycin 0.6 - 40 0.6 - 80

Emory Medical Laboratories Immunosuppressant Monitoring
• Average monthly workload for 2004: » Tacrolimus – 1322 » Cyclosporine A – 732 » Sirolimus – 426
This equals 2480 samples a month or 83 samples per day
• Analysis performed in the Special Chemistry Section, 7 days per week, dayshift only.

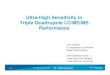
RAPA – Assay Comparison (both LC-MS/MS)
Deming Regression: Emory = 1.006 Mayo + 0.05 R = 0.9903 N = 24 Average Bias = 0.10

Tacrolimus Assay Comparisons
Deming Regression: LC/MS/MS = 1.022 IMx-0.117 R = 0.9380 N = 39 Average Bias = 0.064

HPLC = 1.0056 LCMS + 13.548R2 = 0.9574
0
100
200
300
400
500
600
0 100 200 300 400 500 600
HP
LC
(M
ayo
)(n
g/m
L)
LC/MS/MS (Emory)(ng/mL)
CyclosporineLC/MS/MS vs HPLC
n=19 random patient specimens
LCMS HPLC100 114200 215400 416

How does immunoassay compare to LC-MS/MS?
Pure Compound:
1. LC/MS/MS = 0.912Abbott -2.071, r = 0.912 2. On average the LC/MS/MS value is 9.7% lower than the Immunoassay . 3. Immunoassay Therapeutic Range was 50 to 400 ng/mL 4. From this comparison, LC/MS/MS Therapeutic Range is 43 to 363 ng/mL

Patient Sample Comparison
f / /
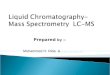
Emory Cyclosporine Assay Comparison (using patient samples)
LC/MS/MS = 0.789TDx - 46.752R2 = 0.9011
0
500
1000
1500
2000
2500
0 500 1000 1500 2000 2500
Immunoassay (Abbott Monoclonal)
LC/M
S/M
S
n=185 patient samples with complete data as of 12/15/03 Therapeutic Range comparable to TDx assay = -7 to 269ng/mL
On average the LC/MS/MS values are 44% lower than the immunoassay values

• Therapeutic drug monitoring is mandated as bioavailability, metabolism, and excretion can differ markedly among individuals.
• Additionally, nephrotoxicity, hepatoxicity, and neurotoxicity can occur with overdosage whereas graft rejection can result from underdosage.
• The current recommendation for CsA monitoring is to analyze trough concentrations of the drug in EDTA whole blood using a method specific for the parent compound. Monitoring of the active metabolites is not currently recommended. (Oellerich et al, Consensus Conference on CsA Monitoring in Organ Transplantation:report of the consensus panel. Ther. Drug Monit. 1995, 17:642-654.)
Cyclosporine

Billboards You’ll Never See:

Update Memo Moving CsA Testing to LC-MS/MS Assay
• “Methodology will change as of 11/24/03”
• “New Therapeutic Range: Specific for parent drug
• “Individual patient levels may vary by as much as 70%”
• “Recommend if see a drop of 30 to 40% and patient is stable, no change. If more than that proceed to increase dose slowly.”

Laboratory Update Memo: Moving CsA Testing to LC-MS/MS Assay
Advantages: – Measures 3 immunosuppressive drugs (CsA, Tacrolimus,
Sirolimus) simultaneously.
– Specific for only parent compound of each drug.
– Corresponds very well to the HPLC method which has been regarded as the “gold standard” method for CsA determinations. (Holt, et al, Ther. Drug Monitor., 24:59-67, 2002)
– Increased lab efficiency, decreased costs, decreased reliance on single vendor of immunoassay.

11/24/03 • Communicated change to physicians
through periodic status updates of conversion
• Due to a distribution problem before go-live, memo not distributed until 11/26/03

Duplicate Patient Testing
• To help transition to the new methodology lab agreed to perform duplicate cyclosporine testing.
• 833 patient specimens were analyzed (12/15/03 thru 01/15/04).
Transplant Type
# Patients Specimens
Heart 82 128
Kidney 231 247
Liver 23 41
Lung 23 243
Stem Cell & Bone
Marrow
8 52
Pancreas 5 42
C2 Protocols
13 45

Total Data Set Cyclosporine Patient Sample Comparisons
12/15/03 thru 01/15/04
LC/MS/MS = 0.6232TDx - 22.659R2 = 0.9629
0
200
400
600
800
1000
1200
1400
1600
1800
2000
0 500 1000 1500 2000 2500 3000
TDx - Immuno Assay(ng/mL)
LC/M
S/MS
(ng/
mL)
LC/MS Immuno 40 100 102 200 227 400 601 1000

Heart Transplant Specimens Heart Transplant Specimens
n=128
LC/MS/MS = 0.5313TDx - 9.3919R2 = 0.9157
0
50
100
150
200
250
300
350
400
450
500
0 100 200 300 400 500 600 700
TDx - Immuno Assay(ng/mL)
LC/M
S/M
S(n
g/m
L)
LC/MS Immuno 44 100 97 200 203 400 522 1 000

Kidney Transplant Specimens Kidney Transplants
n=247
LC/MS/MS = 0.6362TDx - 23.124R2 = 0.9669
0
200
400
600
800
1000
1200
1400
0 200 400 600 800 1000 1200 1400 1600 1800 2000TDx - Immuno Assay (ng/mL)
LC/M
S/MS
(ng
/mL)
LC/MS Immuno 41 100 104 200 231 400613 1000

Individual Patient Data
0
200
400
600
800
1000
1200
1400
12/22/0312/23/03
12/24/0312/25/03
12/26/0312/27/03
12/28/0312/29/03
12/30/0312/31/03
1/1/041/2/04
1/3/041/4/04
1/5/041/6/04
1/7/041/8/04
1/9/041/10/04
1/11/041/12/04
Date
Cyclosp
orine (n
g/mL)
TDx-Immunoassay
LC/MS/MS
Kidney Transplant Patient: PI (10/16/03)
Individual Patient Data
0
50
100
150
200
250
300
350
12/26/0312/27/03
12/28/0312/29/03
12/30/0312/31/03
1/1/041/2/04
1/3/041/4/04
1/5/041/6/04
1/7/041/8/04
1/9/041/10/04
1/11/041/12/04
Date
Cyclosp
orine (n
g/ml)
TDx-Immunoassay
LC/MS/MS
Kidney Transplant Pat: AL (5/1/92)

Conclusions
LC-MS/MS: - may not be as complicated as many techs fear - can be cost-effective - as Lab Developed Tests, require more work on the
lab’s part for implementation - requires a lot of communication with clinicians
So, why isn't every lab running to get LC-MS/MS?


Why isn't every lab running to get a mass spectrometer??
• Challenges – Throughput and Automation – Technology Barriers – Clinical lab workflow incorporation – IAs improving*
Inte
rest
in m
ass s
pect
rom
etry
Time
• Next best thing? – Routine automation – Bar code ready – Common interfacing capabilities

Clarke W, Rhea J, Molinaro R. 2013. Journal Mass Spec (In press)

Why isn't every lab running to get a mass spectrometer??
• Challenges – Throughput and Automation – Technology Barriers – Clinical lab workflow incorporation – IAs improving
Inte
rest
in m
ass s
pect
rom
etry
Time
• Next best things for LC-MS/MS? – Routine automation – Bar code ready – Common interfacing capabilities*

Manual Reporting
Report ~400 mass spectrometry results manually/day
Nominal Human Error Rates For Selected Activities

Thank you!

Self Assessment Questions
1. Which of the following are the units reported by mass spectrometers?
a) Mass to charge ratio b) Charge c) Formula weight d) There are no units

2. A challenge in LC-MS/MS that may be result in analyte fragmentation occurring after column separation but before the collision cell is:
a) Analytical measurement range b) In-source fragmentation c) Dilution effect d) Cross-talk

3. Which of the following is a disadvantage to a protein precipitation pretreatment process for LC-MS/MS?
a) Shorter preparation time b) Ion-suppression c) Less chance of operator error during processing d) In-source fragmentation