Embed Size (px)
Citation preview
ARTICLE IN PRESS
Evidence-Based Healthcare & Public Health (2005) 9, 197–199
KEYWORDLegislationPack size;Paracetamoverdose;Before andstudy
1744-2249/$ - sdoi:10.1016/j.e
$Abstractedon poisonings.
www.elsevier.com/locate/ebhph
COMMENTARY
Laws limiting the size of paracetamol packs help toprevent overdose$
Oliver Morgan, MSc MFPH (Commentator)
Imperial College London, UK
S;
ol
after
ee front matter & 2005hbc.2005.03.030
from: Hawton K, SimkiBritish Medical Journal
Question: Does legislation to limit the size of paracetamol packs reduce death, livertransplantation or referral and non-fatal self poisoning?Study design: Before and after study.Main results: In the first 4 years after legislation to limit the size of paracetamolpacks, death from overdose, non-fatal self poisoning and admissions for livertransplant were reduced compared with before legislation. In the first 2 years afterlegislation, listing for liver transplants and actual transplantation rates werereduced compared with before legislation, but there was no significant differenceafter 3 and 4 years (see results tables 1 and 2). Mean pack sizes of paracetamoldecreased significantly from before to after legislation (35 before v 24 after).However, sales rose after legislation, so total numbers of tablets sold were similar(520 million before v 580 million after).Authors’ conclusions: Legislation to limit the size of paracetamol packs reduced therisk of death from overdose, non-fatal self poisoning, admissions and listing for livertransplant and actual transplantation.& 2005 Elsevier Ltd. All rights reserved.
Further details
Setting
Suicide data from the Office for National Statistics in England and Wales, 1993–2001; six liver units inEngland and Scotland, 1996–2002; five general hospitals in Oxford, Manchester, and Derby, 1997–2001; salesdata from Intercontinental Medical Statistics Health UK, 1996–2002.
Participants
People aged 12 years and over who had an adverse outcome related to paracetamol overdose.
Elsevier Ltd. All rights reserved.
n S, Deeks J, et al. UK legislation on analgesic packs: before and after study of long term effect2004; 329: 1076–1079.
ARTICLE IN PRESS
EVIDENCE-BASED HEALTH POLICY198
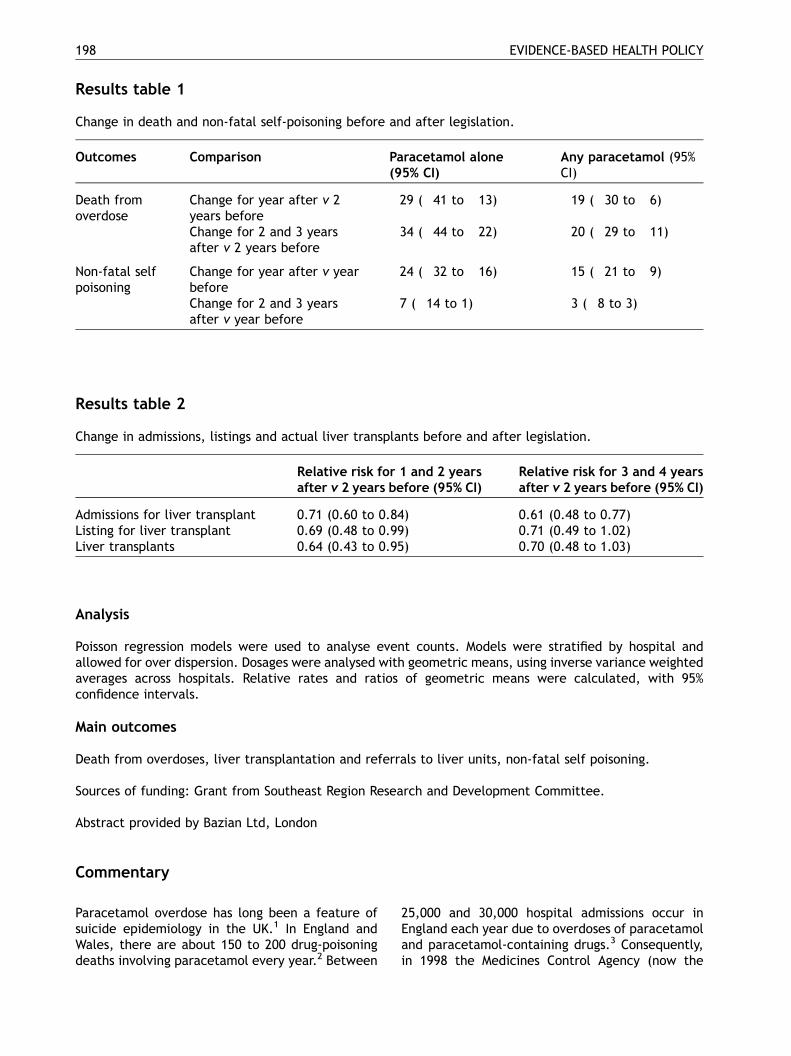
Results table 1
Change in death and non-fatal self-poisoning before and after legislation.
Commentary
Paracetamol overdsuicide epidemioloWales, there are adeaths involving pa
ose has long been a feature ofgy in the UK.1 In England andbout 150 to 200 drug-poisoningracetamol every year.2 Between
25,000 and 30,000 hospitEngland each year due to oand paracetamol-containinin 1998 the Medicines Co
Outcomes
Comparison Paracetamol alone(95% CI)Any paracetamol (95%CI)
Death fromoverdose
Change for year after v 2years before
�29 (�41 to �13)
�19 (�30 to �6)Change for 2 and 3 yearsafter v 2 years before
�34 (�44 to �22)
�20 (�29 to �11)Non-fatal selfpoisoning
Change for year after v yearbefore
�24 (�32 to �16)
�15 (�21 to �9)Change for 2 and 3 yearsafter v year before
�7 (�14 to 1)
�3 (�8 to 3)Results table 2
Change in admissions, listings and actual liver transplants before and after legislation.
Relative risk for 1 and 2 yearsafter v 2 years before (95% CI)
Relative risk for 3 and 4 yearsafter v 2 years before (95% CI)
Admissions for liver transplant
0.71 (0.60 to 0.84) 0.61 (0.48 to 0.77) Listing for liver transplant 0.69 (0.48 to 0.99) 0.71 (0.49 to 1.02) Liver transplants 0.64 (0.43 to 0.95) 0.70 (0.48 to 1.03)Analysis
Poisson regression models were used to analyse event counts. Models were stratified by hospital andallowed for over dispersion. Dosages were analysed with geometric means, using inverse variance weightedaverages across hospitals. Relative rates and ratios of geometric means were calculated, with 95%confidence intervals.
Main outcomes
Death from overdoses, liver transplantation and referrals to liver units, non-fatal self poisoning.
Sources of funding: Grant from Southeast Region Research and Development Committee.
Abstract provided by Bazian Ltd, London
al admissions occur inverdoses of paracetamolg drugs.3 Consequently,ntrol Agency (now the

ARTICLE IN PRESS
Medicines and Healthcare Products RegulatoryAgency) introduced legislation to limit the avail-ability of paracetamol to reduce harm and deathfrom poisoning.4,5 The regulations limit sales atgeneral outlets to a maximum of 16 tablets of500mg (8 g in total). Packets containing 32 tablets(16 g) can be sold at pharmacies and up to 100tablets can be sold at the discretion of a pharma-cist. Specific warnings of the dangers of paraceta-mol are printed on the packets and on leaflets inthe packets. Paracetamol tablets are now also onlyavailable in blister packs. In this study, Hawton andcolleagues assess the impact of these regulationson poisoning death and non-fatal poisoning.
Hawton and colleagues report similar reductionsin severity and death from paracetamol poisoningas reported in their previous study 3 years ago.6
However, the conclusion that ‘Legislation restrict-ing pack sizes of analgesics in the United Kingdomhas been beneficial’ is probably over optimistic.The observational nature of the study makes itdifficult to attribute the decline in poisoning to thereduction in pack sizes. Similar reductions inpoisoning from other drugs such as antidepressantshave occurred over the same time period,7 suggest-ing that the decrease in paracetamol poisoning maybe due to secular trends rather than the regula-tions. And although there has been a noticeablerelative reduction in paracetamol poisoning, theabsolute reduction has actually been fairly modest.In 2002 paracetamol poisoning was still responsiblefor at least 126 deaths in England and Wales2 andabout 25,000 hospital admissions in England.3
The authors’ second conclusion that ‘A furtherreduction in pack sizes could prevent more deaths’is not supported by the study’s results. Instead,many experts are concerned that further reduc-tions in pack sizes may encourage ‘method sub-stitution’, whereby people take drugs that aremore toxic than paracetamol. This may be parti-cularly dangerous because paracetamol is one ofthe few drugs commonly taken in overdose forwhich an effective antidote is available.
Although many studies of the impact of reducingpack size have now been published, the evidencefor a public health benefit is still weak. A trueassessment of the benefit of the regulations mustalso include possible negative consequences, forexample an increased incidence of gastrointestinalhaemorrhage resulting from an increased use ofibuprofen.8 In the UK, paracetamol poisoningremains an important public health issue, repre-senting a notable cause of avoidable mortality anda considerable workload for the NHS. Althoughregulations may possibly prevent some poisonings,a greater reduction in the incidence of paracetamolpoisoning is only likely to be achieved through abroader public health strategy, involving generalpractice and mental health services.
References
1. Flanagan R, Rooney C. Recording acute poisoning deaths.Forensic Sci Int 2002;128:3–19.
2. Office of National Statistics. Deaths related to drug poisoning:results for England and Wales, 1998 to 2002. Health Stat Q2002;21:59–66.
3. Morgan O, Griffiths C, Majeed A. Impact of paracetamol packsize restrictions on poisoning from paracetamol in Englandand Wales: an observational study. J Public Health 2005(advanced access).
4. Medicines Control Agency (Department of Health). Analgesicmedicines available without prescription: proposed changesto product information and sale of supply of paracetamol.London: (MLX321); 1996.
5. Committee on Safety of Medicines (MCA). Paracetamol andaspirin. Curr Problems Pharmacovigilance 1997;23:9.
6. Hawton K, Townsend E, Deeks J, et al. Effects of legislationrestricting pack sizes of paracetamol and salicylate on selfpoisoning in the United Kingdom: before and after study. BrMed J 2001;322:1–7.
7. Morgan O, Griffiths C, Baker A, Majeed A. Antidepressant-related poisoning mortality in England and Wales 1993–2002.Health Stat Q 2004;23:18–24.
8. Sheen C, Dillon J, Bateman N, Simpson K, Macdonald T.Paracetamol pack size restriction: the impact on paracetamolpoisoning and the over-the-counter supply of paracetamol,aspirin and ibuprofen. Pharmacoepidemiol Drug Safety2002;11:329–31.
EVIDENCE-BASED HEALTH POLICY 199





























