Embed Size (px)
Citation preview

Landscape of North-South and South-South Initiatives for Local Pharmaceutical
Production and Technology Transfer
By Suerie MoonResearch Fellow and Doctoral Candidate
Sustainability Science Program, Center for International Development
Kennedy School of Government, Harvard University
Comments & questions welcome at: [email protected]
LATIN AMERICAN DIALOGUE ON TECHNOLOGY TRANSFER FOR LOCAL MANUFACTURING of DRUGS AND VACCINESOrganised by ICTSD & UNCTAD with the support of WHO and the European Commission18-19 March 2010, Buenos Aires, Argentina

Overview
1. Key questions re: local production
2. Study
3. Findings
4. Key Issues
5. Conclusions
6. Questions for Workshop
6. Questions for Workshop
1. What kind of technology is needed? From whom?
2. What is the biggest barrier to accessing it?
3. What should Latin Am. governments do?
4. What should international community do? (multilaterals, donors, NGOs, foundations, research institutes, firms)
1. Background on Local Production
Global production capacity among LMICs (Ballance et al (1992)):• Sophisticated industry with significant research: 10 countries, 0 LMICs
• Innovative capability: 16 countries, 6 LMICs
• Some production capacity: 97 countries (mostly LMICs)
• Formulation/packaging: 84
• API: 13
• No production capacity: 42 (mostly LMICs)
Recent Developments:• New interest in improving API production capacity
• Some LMIC generics multinational
• Some LMIC generics R&D• Some multinationals acquiring or partnering w/ generics firms
1. Key Questions re: local production
1. Local production = anticipated benefits?
• Improved access to medicines: – Lower prices
– Security of supply
– Quality assurance
– Better-adapted products
• Economic Development: – Foreign exchange or reduced currency-related risk
– Exports
– High-skilled jobs
– Technological capacity
– Technology transfer
1. Key Questions re: local production
2. If so, how can local production best be supported?
• Technological capacity:– Access to/transfer of technology
– Absorptive capacity
• Economic policies:– Investment
– Supportive policies re: procurement, subsidies, taxes, tariffs, and/or trade policies
– Infrastructure
• Legal frameworks– Intellectual property policies
– Regulatory capacity & requirements

2. Study: Objectives
• Identify & outline recent North-South and South-South initiatives for local production & relevant technology transfer (5-10 yrs)
• Analyze gaps & key issues
• Included:• Direct transfer of technology (software/hardware)• Indirect support (eg policy, regulatory)• Investment
• Excluded:• R&D• Initiatives remotely relevant to production• Confidential commercial technology transfer• Reverse engineering
• Considered separately: Voluntary licenses

2. Study: Methodology
• No uniform data source exists• No guarantee of 100% coverage
• Searched and reviewed: • Academic literature• Multilateral agency websites (eg WHO, UNIDO, UNCTAD, etc.) • Donor websites (eg DFID, GTZ, EU, etc.)• Government websites of LMICs with established pharmaceutical industries as
potential transferors (eg India, China, Brazil, etc.)• Pharmaceutical company & industry websites (both patent-based and large
generic firms)• Public-Private Product Development Partnerships (eg. DNDi, Aeras)• Mainstream international and regional media through LexisNexis• Reports of high-income WTO Members on compliance with TRIPS Article 66.2• US Department of Commerce data• Selected interviews and personal referrals

3. Findings: Overview
Wide variation among initiatives, by:• North-South, South-South• Private-private, public*-private, private-public*,
public*-public*• Goals & interests of transferor/transferee• Technical capacity of transferee• Complexity of transferred technology • Technical value of transfer (e.g. gain for transferee)• Economic value of transfer (e.g. product market)• Scale and duration of transfer
*Public=government or not-for-profit entity

3. Findings: Four Types
1. Transfer of technology for production (n=30)
2. Investments (n=27)
3. Voluntary licensing initiatives (n=14)
4. Facilitating production: e.g. support to NRAs, industrial policy advice, IP advice, networking, strategy/planning
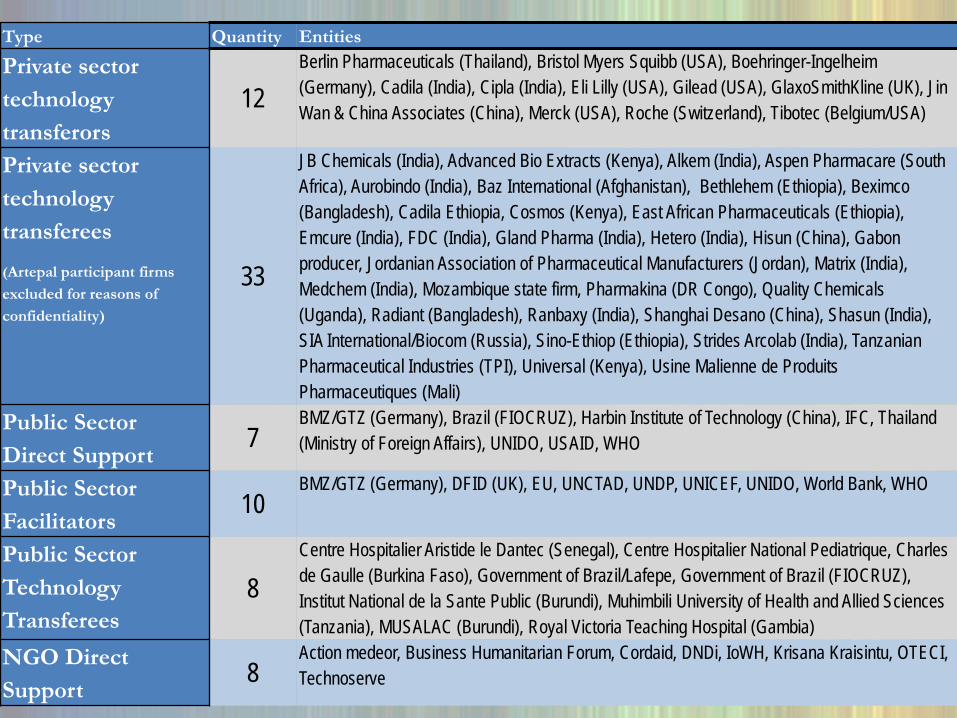
Type Quantity Entities
Private sector technology transferors
12Berlin Pharmaceuticals (Thailand), Bristol Myers Squibb (USA), Boehringer-Ingelheim (Germany), Cadila (India), Cipla (India), Eli Lilly (USA), Gilead (USA), GlaxoSmithKline (UK), Jin Wan & China Associates (China), Merck (USA), Roche (Switzerland), Tibotec (Belgium/USA)
Private sector technology transferees (Artepal participant firms excluded for reasons of confidentiality)
33
JB Chemicals (India), Advanced Bio Extracts (Kenya), Alkem (India), Aspen Pharmacare (South Africa), Aurobindo (India), Baz International (Afghanistan), Bethlehem (Ethiopia), Beximco(Bangladesh), Cadila Ethiopia, Cosmos (Kenya), East African Pharmaceuticals (Ethiopia), Emcure (India), FDC (India), Gland Pharma (India), Hetero (India), Hisun (China), Gabon producer, Jordanian Association of Pharmaceutical Manufacturers (Jordan), Matrix (India), Medchem (India), Mozambique state firm, Pharmakina (DR Congo), Quality Chemicals (Uganda), Radiant (Bangladesh), Ranbaxy (India), Shanghai Desano (China), Shasun (India), SIA International/Biocom (Russia), Sino-Ethiop (Ethiopia), Strides Arcolab (India), Tanzanian Pharmaceutical Industries (TPI), Universal (Kenya), Usine Malienne de ProduitsPharmaceutiques (Mali)
Public Sector Direct Support
7BMZ/GTZ (Germany), Brazil (FIOCRUZ), Harbin Institute of Technology (China), IFC, Thailand (Ministry of Foreign Affairs), UNIDO, USAID, WHO
Public Sector Facilitators
10BMZ/GTZ (Germany), DFID (UK), EU, UNCTAD, UNDP, UNICEF, UNIDO, World Bank, WHO
Public Sector Technology Transferees
8Centre Hospitalier Aristide le Dantec (Senegal), Centre Hospitalier National Pediatrique, Charles de Gaulle (Burkina Faso), Government of Brazil/Lafepe, Government of Brazil (FIOCRUZ), Institut National de la Sante Public (Burundi), Muhimbili University of Health and Allied Sciences (Tanzania), MUSALAC (Burundi), Royal Victoria Teaching Hospital (Gambia)
NGO Direct Support
8Action medeor, Business Humanitarian Forum, Cordaid, DNDi, IoWH, Krisana Kraisintu, OTECI, Technoserve
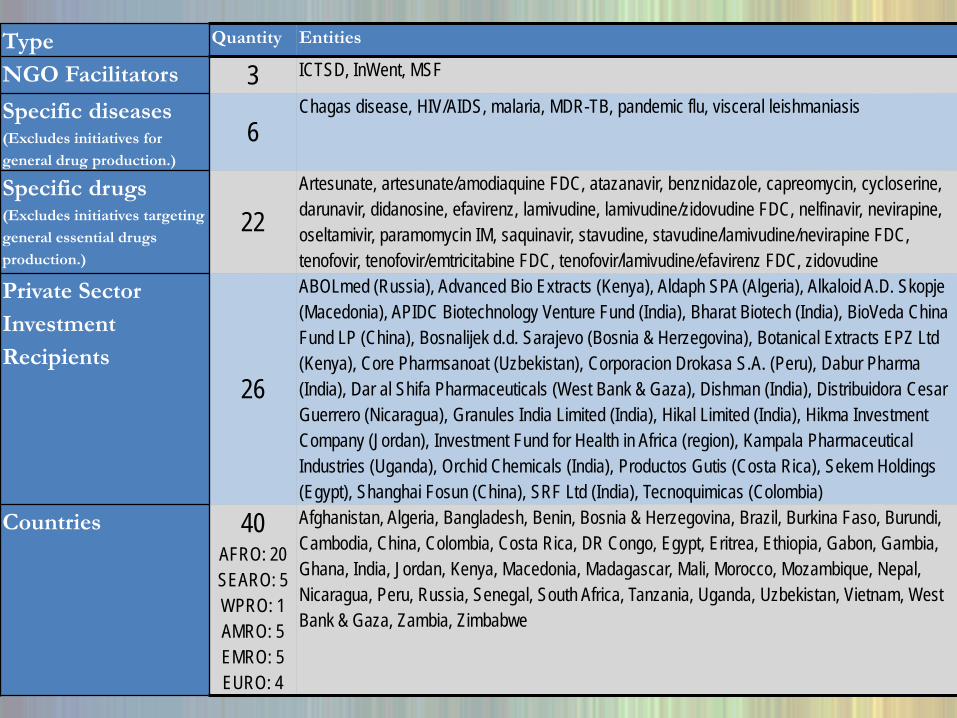
Type Quantity Entities
NGO Facilitators 3 ICTSD, InWent, MSF
Specific diseases (Excludes initiatives for general drug production.)
6Chagas disease, HIV/AIDS, malaria, MDR-TB, pandemic flu, visceral leishmaniasis
Specific drugs(Excludes initiatives targeting general essential drugs production.)
22Artesunate, artesunate/amodiaquine FDC, atazanavir, benznidazole, capreomycin, cycloserine, darunavir, didanosine, efavirenz, lamivudine, lamivudine/zidovudine FDC, nelfinavir, nevirapine, oseltamivir, paramomycin IM, saquinavir, stavudine, stavudine/lamivudine/nevirapine FDC, tenofovir, tenofovir/emtricitabine FDC, tenofovir/lamivudine/efavirenz FDC, zidovudine
Private Sector Investment Recipients
26
ABOLmed (Russia), Advanced Bio Extracts (Kenya), Aldaph SPA (Algeria), Alkaloid A.D. Skopje (Macedonia), APIDC Biotechnology Venture Fund (India), Bharat Biotech (India), BioVeda China Fund LP (China), Bosnalijek d.d. Sarajevo (Bosnia & Herzegovina), Botanical Extracts EPZ Ltd (Kenya), Core Pharmsanoat (Uzbekistan), Corporacion Drokasa S.A. (Peru), Dabur Pharma(India), Dar al Shifa Pharmaceuticals (West Bank & Gaza), Dishman (India), Distribuidora Cesar Guerrero (Nicaragua), Granules India Limited (India), Hikal Limited (India), Hikma Investment Company (Jordan), Investment Fund for Health in Africa (region), Kampala Pharmaceutical Industries (Uganda), Orchid Chemicals (India), Productos Gutis (Costa Rica), Sekem Holdings (Egypt), Shanghai Fosun (China), SRF Ltd (India), Tecnoquimicas (Colombia)
Countries 40AFRO: 20SEARO: 5WPRO: 1AMRO: 5EMRO: 5EURO: 4
Afghanistan, Algeria, Bangladesh, Benin, Bosnia & Herzegovina, Brazil, Burkina Faso, Burundi, Cambodia, China, Colombia, Costa Rica, DR Congo, Egypt, Eritrea, Ethiopia, Gabon, Gambia, Ghana, India, Jordan, Kenya, Macedonia, Madagascar, Mali, Morocco, Mozambique, Nepal, Nicaragua, Peru, Russia, Senegal, South Africa, Tanzania, Uganda, Uzbekistan, Vietnam, West Bank & Gaza, Zambia, Zimbabwe
3. Findings: Therapeutic Areas
• Newer products (some exceptions)• Emphasis on:
– AIDS: antiretrovirals– TB: MDR-TB– Malaria: ACT– Pandemic flu (H5N1 and H1N1): oseltamivir, vaccine– + Some neglected disease:
• Visceral leishmaniasis (kala azar) (paramomycin)• Chagas disease (benznidazole)
• Absent:– Almost no Type 1 disease products (exceptions: joint
ventures in oncology, metabolic)– No biotech drugs– Some traditional medicines but largely commercial

3. Findings: Transferors
Who are the transferors? • Major multinational pharmaceutical companies• Public or non-profit institutions: e.g. NIH, Netherlands Vaccine
Institute, FIOCRUZ• Public-private product development partnerships (PDPs): e.g.
DNDi• NGOs: e.g. action medeor• Individuals: e.g. Dr. Krisana Kraisintu
Out of 30 initiatives:– 20 North-South (2/3)– 10 South-South (1/3)

3. Findings: Transferees
Who are the transferees?• Big generics firms in BRICS: many in India
– All stages of production (raw materials to finished product)• Smaller generics firms in smaller or less developed countries:
e.g. sub-Saharan Africa– Later stages: formulation, packaging, GMP, documentation
• Joint ventures & subsidiaries (limited info): – Wide-range of products and countries,
– Trends in larger developing countries (e.g. India, China)• Universities/research institutes:
– Education, training, small-scale lab production (e.g. Muhimbili (TZ))
3. Findings: “International Community”
• Coordination: – Interagency Pharmaceutical Coordination (IPC) Group: WHO, WB, UNAIDS,
UNFPA, UNICEF– IPC Local Production Sub-group: UNIDO, UNCTAD, UNDP , AfDB, Global Fund
• “Direct” support: firm-level production– WHO: training, technical assistance
– UNIDO: technical assistance to firms
– IFC (World Bank): ~$280 M investment (1997-2009)
– Brazil, EU, Thailand, Germany: technology transfer or financing
– Action medeor, Cordaid, OTECI, Technoserve: technical assistance or financing
• “Indirect” support: policy advice, capacity-building, institutional strengthening, analysis– UNIDO, UNCTAD, World Bank, UNDP, WHO, UNICEF, African Union
– EU, Germany, United Kingdom, United States
– Action medeor, ICTSD, InWent, MSF
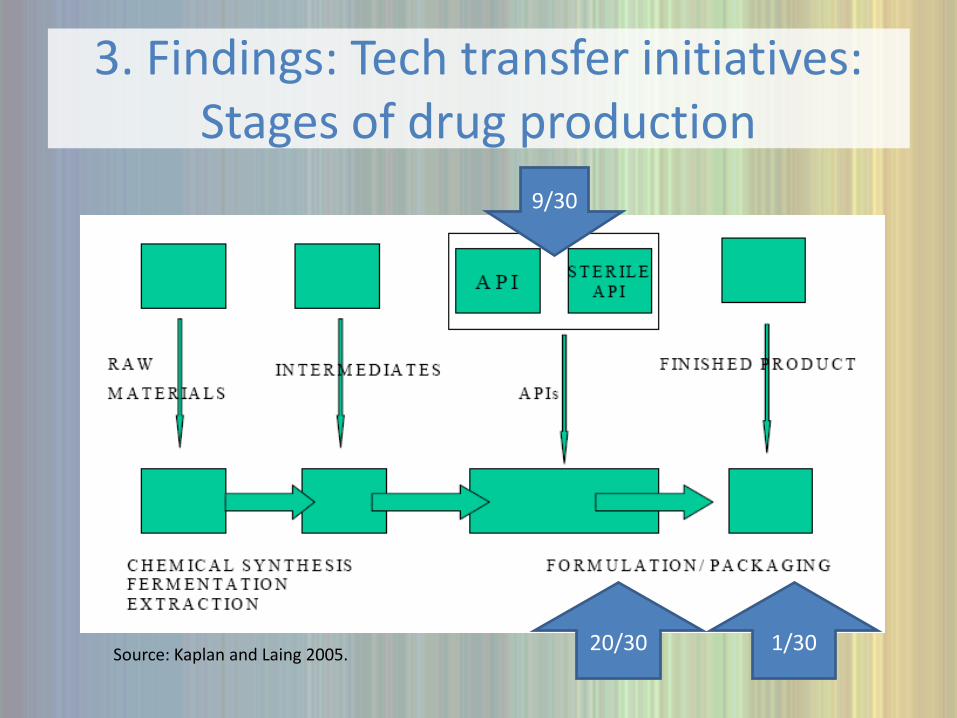
3. Findings: Tech transfer initiatives: Stages of drug production
Source: Kaplan and Laing 2005.
9/30
20/30 1/30
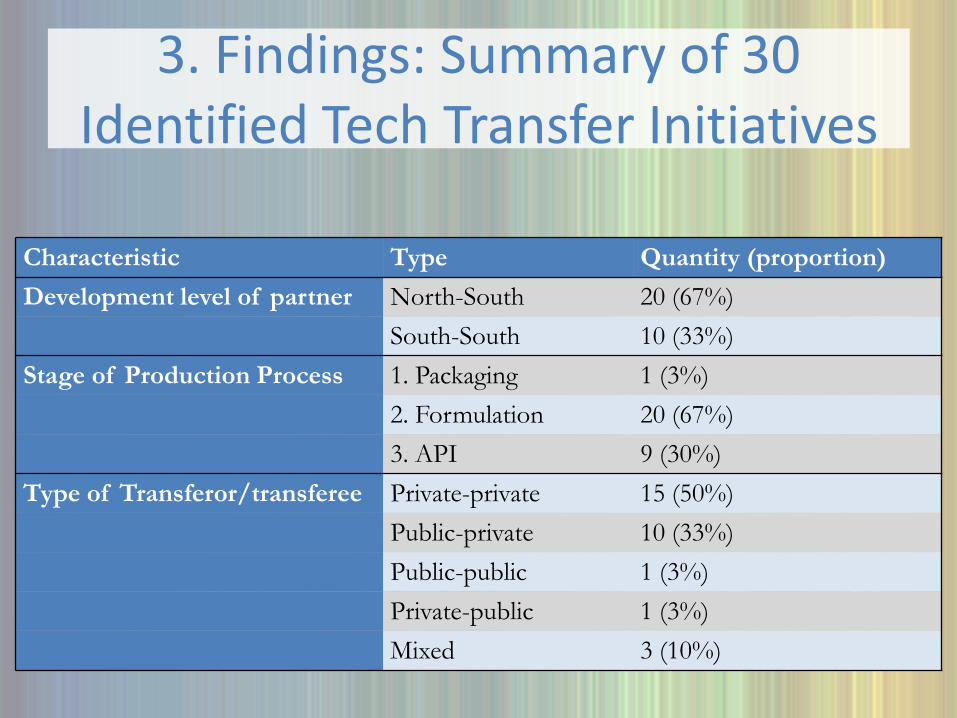
3. Findings: Summary of 30 Identified Tech Transfer Initiatives
Characteristic Type Quantity (proportion)Development level of partner North-South 20 (67%)
South-South 10 (33%)Stage of Production Process 1. Packaging 1 (3%)
2. Formulation 20 (67%)3. API 9 (30%)
Type of Transferor/transferee Private-private 15 (50%)Public-private 10 (33%)Public-public 1 (3%)Private-public 1 (3%)Mixed 3 (10%)

3. Findings: Trends
Start dates of initiatives: 1995-1999 2000-2004 2005-2009
Technology transfer initiatives 0 12 18
Investment initiatives 5 7 15
Voluntary licensing initiatives 0 6 8

4. KEY ISSUES
a. Why transfer?b. Why receive?c. Restrictions in TT Agreementsd. Intellectual property managemente. Economic issuesf. Utility of transferg. Time horizonsh. Quality standards/regulationi. Definition of success?
4. Key issues: Why transfer?
a. Why transfer? :• Commercial: “business case”
– Free up production capacity– Products no longer of commercial interest– Business model does not include high-volume/low-margin
supply– Corporate social responsibility – Avert legal or regulatory action
• Public/non-profit: “mission”– Improve public health through access to medicines– Support economic development– Reduce reliance on imports– Reduce barriers to national adoption of new medicines
4. Key issues: Why receive?
b. Why receive? :• Access to technology, know-how• Reduced time/cost to develop in-house• Employee skills upgrade• Reputational benefits of partnering with major firm/org• Spillovers into other products, distribution networks, business
opportunities
4. Key issues: Restrictions & IP
c. Restrictions in Tech Transfer Agreements • Export markets• Further transfer to third-party• Trade secrets• Monopoly for fixed period• Price floors/ceilings• Royalties
d. Intellectual Property • Patents barrier for more advanced firms or newer products• LDC 2016 deadline = new interest in local production• But many LDCs have not created clear legal space for
production • Strategy needed to manage IP for production & tech transfer

4. Key issues: Economic & Utility
e. Economic issues:1. Finance2. Economic feasibility of local production
• Price competitive?• How much time to get competitive?• Market size sufficient?
3. Failures in technology markets• Information asymmetries search costs• Information asymmetries unequal negotiating power
f. Utility of Transfer• Technology on offer • Advanced vs Less advanced firms

4. Key issues: Timelines & Quality
g. Time horizons• Long-term outlook required• Increased complexity of tech transfer over time
h. Quality standards/Regulation• Which regulatory standards?• Impact of standards on local production• Regulatory capacity critical
4. Key issues: Success?
i. What is success in local production & technology transfer?
1975: UNIDO Goal: 25% pharma production in LMICs by 2000
2000: ~7% pharmaceuticals produced in LMICs
• Project/country/regional perspective:– Access? (price, availability, quality, adaptedness)
– Improved production capacity over status quo?
– Export to region?
• Global perspective– How much local production is ‘enough’?
– How much technology transfer is ‘enough’?

5. Conclusions
1. Methodical, ongoing, centralized public info source2. Broaden therapeutic areas (beyond AIDS, TB,
malaria)3. API: diversify risk of concentrated production4. Extend LDC patent deadline5. Public actors: create incentives for tech transfer6. Define success, articulate goals, set targets7. Mid/long-term comprehensive approach targeting
high-potential countries8. Opportunity & Momentum

6. Questions
1. What kind of technology is needed? From whom?
2. What is the biggest barrier to accessing it?
3. What should Latin Am. governments do?
4. What should international community do? (multilaterals, donors, NGOs, foundations, research institutes, firms)

Gracias, Obrigada, Thank You
Comments & Questions welcome at: [email protected]
Acknowledgments: With thanks to Alyssa Yamamoto for excellent research assistance. Also, special thanks to Malebona Precious Matsoso and Gina Vea at WHO, and to experts Frederick Abbott, Kiyoshi Adachi, Ermias Biadgleng, Padmashree Gehl Sampath, Cheri Grace, Elodie Jambert, Warren Kaplan, Pedro Roffe, and Christoph Spenneman for very helpful guidance and comments. .





























