Embed Size (px)
Citation preview
2017Vol.8 No.5:224
Review Article
DOI: 10.21767/2171-6625.1000224
iMedPub Journalswww.imedpub.com
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
1© Under License of Creative Commons Attribution 3.0 License | This article is available in: www.jneuro.com
Alberto J Mimenza Alvarado1*, Carlos G Cantú Brito2, Gustavo C Roman3, Pietro Gareri4, Sara G Aguilar Navarro1, Jose L Ruiz Sandoval5, Juan M Calleja Castillo6, Carolina Velazquez7, Gustavo Pradilla Ardila8, María S Caceres Merino9, Juan C Duran Quiroz10, Nilton C Capuñay11, Ciro Gaona12, Jose S Ramírez13, Carlos Arteaga Vasquez14, Hector Franco15, Felipe Villareal16, Hector Orrego Castellanos17, Xinia M Jiménez Campos18 and Julio J Secades19
1 DepartmentofGeriatric,InstitutoNacionaldeCienciasMédicasyNutriciónSalvadorSubirán,México
2 DepartmentofNeurology,InstitutoNacionaldeCienciasMédicasyNutriciónSalvadorZubirán,México
3 DepartmentofNeurology,MethodistNeurologicalInstitute,USA
4 AmbulatoryCenterforCognitivedisorders,GeriatricianASPCatanzaro,Italy
5 DepartmentofNeurology,HospitalCivildeGuadalajara"FrayAntonioAlcalde",México
6 DepartmentofNeurology,InstitutoNacionaldeNeurologiayNeurocirugia,México
7 NewHeightsChristianSchool/EscuelaNuevasAlturasLambare,Paraguay,Paraguay
8 UnitofNeurology,IndustrialUniversityofSantander,Colombia
9 SociedaddeGeriatríayGerontologíadeChile,EnvejecimientoActivoChile,ClínicaDávila,Chile
Latin American Delphi Consensus on Vascular Cognitive Impairment: Definitions,
Clinical Features, Pathophysiology, Prevention and Treatment
AbstractCerebralvasculardisease(CVD)representsthesecondcauseinyearsoflifelost,accordingto theGlobalBurdenofDiseaseStudy2015study.Theglobal reportonAlzheimer'sdisease2015estimatesthatinLatinAmericathereare9.2millioncasesofdementia,withaprevalenceof8.2%.Undoubtedly,Alzheimer'sdiseaseisthemostfrequentcause,followedbyvasculardementia(VD)with15%ofthecases,althoughglobaldataareunknowninLatinAmerica.
Objective: To analyze and present the current evidence on the classification,pathophysiology,diagnosisandtreatmentofvascularcognitiveimpairment.
Methodology:AgroupofexpertsmetinMiami,Florida,inApril2016.ThegroupincludedNeurologists,GeriatriciansandPsychiatristsfromthefollowingcountries:Mexico,Guatemala,ElSalvador,CostaRica,Peru,Spain,Bolivia,Chile,Paraguay,Colombia, Panama, Venezuela, Italy, the United States, Dominican Republic,Honduras and Nicaragua. The Delphi method was used to review availableinformation(providedmonthsbeforethemeeting),inrelationtoassignedtopics:definitionofCognitiveVascular Impairment(CVI), riskfactors,pathophysiology,diagnosis(neuropsychologicalandimaging)andtreatment.Fortheallocationofevidenceandrecommendationofavailabletreatments,theGRADEsystemwasused.
TheworkinggroupsanalyzedanddiscussedavailableevidenceonCVIconcerningproposed definitions, risk factors and diagnostic elements. Subsequently, theconclusionsofeachoftheworkinggroupsweredrafted,whichwerereviewedbyeachoftheauthorsandbytherestofthestudygroupsuntilaglobalconsensuswasreached.Oncethisprocesswascompleted,theprocessofexternalvalidationandpreparationofthefinaldocumentwascarriedout.
Theresultsofthisconsensusallowtheincorporationoftheopinionandexperienceof physicians of different specialties in Latin America regarding the vascularcognitiveimpairment.
Keywords: Depression; Chronic inflammation; Chronic renal failure; Systemicarterialhypertension;Diabetesmellitus
Received:October06,2017; Accepted: October27,2017;Published: October30,2017
IntroductionAccording to the Global Burden of Disease Study 2015 [1],cerebrovascular disease (CVD) represents the second cause ofyearsof life lostandoneofthemajorcausesofdisability.Thisdisability includes not only physical limitations and functional

2017Vol.8 No.5:224
2 This article is available in: www.jneuro.com
ARCHIVOS DE MEDICINAISSN 1698-9465
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
impairment,butalsocognitive issueshavingsubstantial impacton the patient’s quality of life. Latin America is not excludedfromtheworldwidepopulationagingprocess;thisexplainstheincreaseincardiovascularriskfactorsand,consequently,higherprobabilityofoccurrenceofCVD.
Therehasbeenmajorprogressintheunderstandingofcognitiveimpairmentrelatedtovascularpathology.Theseadvanceshavemadeitpossibletobetterdefinevascularcognitiveimpairment(VCI), and to improve our knowledge of the pathophysiologyaccordingtothetypeofvesselaffected(largeorsmall).Also,thewideruseofcognitivescreening tests for thedetectionofVCI,even in the early stages, hasmade it possible to establish thediagnosisinpreclinicalstages,withthepurposeofcontrollingriskfactors.
TheWorldwide Report on Alzheimer’s Disease 2015 estimatesthat there are 9.2million cases of dementia in Latin America,withaprevalenceof8.2%[2].Certainly,themostfrequentcauseof dementia is Alzheimer’s disease (AD), followed by vasculardementia(VD)with15%ofdementiacases[3].TherearenodatabycountryinLatinAmerica.
The main objective of this consensus was to analyze andsummarize current evidence on definition, classification,pathophysiology,diagnosisand treatmentofvascularcognitiveimpairment from a Latin America perspective by a group ofHispanicspecialists.
EpidemiologyStrokeisaleadingcauseofcognitiveimpairment,disabilityandmortalityinLatinAmerica,althoughinformationregardingstrokeand vascular dementia in the region is limited [4-7]. Incidenceratesofstrokereported inLatinAmericanstudies (alladjustedfor Segi’s world population) range from 76.5 to 110 first-everstrokesper100000peryear[8-11].Strokeprevalenceper1000population,basedondoor-to-door surveys, ranges from1.7 inrural areas to 8.7 among predominantly urban population. Inolder patients, (aged ≥60), prevalence of stroke ranges from18.2 to 46.7 per 1000 [12-14]. Considering the high incidenceand prevalence of stroke in Latin America, cerebral vascularinjury shouldbeexpected tobea commoncauseofdementiaand of milder forms of cognitive dysfunction. The prevalenceofdementiainLatinAmericaiscomparabletothatreportedinNorthAmerica.Areviewof8studiesondementiafrom6LatinAmerican countries (Uruguay, Chile, Brazil, Venezuela, Cuba,Peru) reported an overall prevalence of 7.1% (with AD as themostfrequentcause),withoutdescribingvascularetiology[15].A reporton theglobalepidemiologyofdementia indevelopedand underdeveloped countries, reported a prevalence of 1.9%(1.0-3.0) in Cuba, 0.9% (0.06-1.78) and 2.2% (1.6-2.7) in Brazil[16]. InMexico, a study of 110 patientswith first-ever stroke,reportedaprevalenceofvasculardementia(threemonthsaftertheCVA)of12%,withahigherprevalence in illiteratepatientsandlowereducation[17].
Given the fast and increasing knowledge in this field, it isimportant to obtain accurate up-to-date data. For this reason,
10 EspecialistaenNeurología,UniversidadMayordeSanAndrés,Bolivia
11 DirectorMédicoenInstitutoPeruanodeNeurociencias,Perú
12 LaboratoriodeNeurociencias,UniversidaddelZulia,Venezuela
13 AcadémicoDirector,SantoDomingo,DominicanRepublic
14 NationalUniversityofSanMarcos,Perú15 ClínicaNeurología,UniversidaddeSan
CarlosdeGuatemala,Guatemala16 Neurologist,CiudaddePanamá,Panamá.
BrindalosserviciosdeEstudiosdeEEG,CRCVPanama,Panama
17 Neurologist,HospitalNacionalRosales-UniversidaddeElSalvador,ElSalvador
18 UniversidadLatinadeCostaRica,Alajuela,CostaRica
19 DepartamentofNeurosurgery,ScientificDepartmentGrupoFerrer,Barcelona,Spain
*Corresponding author: AlbertoJoseMimenzaAlvarado
InstitutoNacionaldeCienciasMédicasyNutriciónSalvadorZubirán,VascodeQuiróga#15,Tlalpan,CiudaddeMéxico.
Tel: 5554166463
Citation: MimenzaAAJ,CantúBCG,RomanGC,GareriP,AguilarNSG,etal.(2017)LatinAmericanDelphiConsensusonVascularCognitiveImpairment:Definitions,ClinicalFeatures,Pathophysiology,PreventionandTreatment.JNeurolNeurosci.Vol.8No.5:224
a group of experts in cerebrovascular pathology, includingneurologists, geriatricians and psychiatrists from several LatinAmerican countries, analyzed the information available in thisregion,aswellasworldwidedataregardingcognitiveimpairmentofvascularetiology.Thegoalofthestudygroupwastoestablishdefinitions, diagnosis, classification and recommendations forthepreventionandtreatmentofvascularcognitiveimpairment(VCI).
Methodology for Study Group’s RecommendationsA meeting was held on April 2016 in Miami, Florida, USA,

2017Vol.8 No.5:224
3
ARCHIVOS DE MEDICINAISSN 1698-9465
© Under License of Creative Commons Attribution 3.0 License
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
includingagroupofHispanic specialists (vascularneurologists,geriatricsandpsychiatrists)of the followingcountries:Mexico,Guatemala,ElSalvador,CostaRica,Peru,Bolivia,Chile,Paraguay,Colombia, Panama, Venezuela, Dominican Republic, HondurasandNicaragua.Likewise,Hispanicexperts invasculardementia(Spain,ItalyandUnitedStates)alsoparticipatedintheconsensus.
TheDelphi[18]methodwasusedbytheexperts,whoreviewedtheinformationavailable(providedmonthsbeforethemeeting)related to assigned topics: definition of VCI, risk factors,pathophysiology, neuropsychological and imaging diagnosis,and treatment. TheGrade [19] Systemwas used for assigningtheevidenceandrecommendationofavailabletreatments.ThediscussionpanelsanalyzedanddiscussedtheavailableevidenceonVCIforproposeddefinitions,riskfactorsanddiagnosticitems.Subsequently, the conclusions of each panel were written,and study groups reviewed themuntil a global consensuswasreached.Once this processwas completed, thepreparationofthefinaldocumentwascarriedout.
Definition from mild vascular cognitive impairment to vascular dementiaIn1988,Reisbergetal.[20]introducedtheGlobalDeteriorationScale(GDS)inwhichstageGDS3indicatedthemildprogressionofcognitive impairment. Itwasnotuntil1999,however,whenPetersenetal. [21] consolidated theconceptofmild cognitiveimpairment (MCI). MCI emerges then as a prodromal stageof AD, characterized as an interim cognitive stage betweennormal cognition and dementia. Since then, it is establishedthat to cross the borderline between MCI and dementia, thegrade of cognitive dysfunction should be one that impacts onfunctionality. Therefore, investigations were conducted in thisregard,othercausesofMCIadditionallytoADwererecognized,a sub-classification depending on the combination of involvedcognitive domains was created, and an attempt was made toassociateitwithaspecificcause(includingthevascularcause)asthefollowingstepinthediagnosticprocess[22].
The expansion of spectrum of cognitive impairment with acerebrovascular origin arises in this way, not only in terms ofetiologybutalsofortheseverity.Severaltermsareusedtorefertoprodromalstagesofvasculardementia:mildvascularcognitiveimpairment (M-VCI), preclinical vascular cognitive impairment,vascular pre-dementia, and non-dementia vascular cognitiveimpairment [23], referring basically to the same condition butwithsmalldifferences intheoperationaldefinitionofthetermconferringagreatheterogeneityaboutinformationofthisentity.In 2009, the first special symposium was held at the fourthedition of the Congress of International Society for VascularBehavioral and Cognitive Disorders (VASCOG), in which theterm vascular cognitive impairment (VCI) is proposed to nameany cognitive dysfunction with a vascular cause, regardless ofitsspecificetiologyandgradeofseverity,sub-dividingthistermintoMajorVascularCognitiveImpairment(equivalenttovasculardementia) andMild Vascular Cognitive Impairment (similar toVCI).Inthisway,thespectrumbecomesmorecompleteinallitsdimensionsandtheprodromalstageofdementiawithavascular
causeisbetterdelimitedunderthenameMildVascularCognitiveImpairment [23].On the other hand, theAmerican PsychiatricAssociation, inDSM-5,callsitminorneurocognitivedisorder[24].Thecriteriondifferentiatingaminorfromamajordisorderisthatcognitive difficulties should not influence a person’s capabilitytoperformactivitiesofdailylife(ADL).ItisconsideredamajorneurocognitivedisorderwhenitaffectsADL.
Theterm“cognitiveimpairment”isclassicallyusedforthisentity,while the term “neurocognitive” used in DSM-5 emphasizesa conditioncharacterizedbycognitive failuresnot causedbyapsychiatricdisorder,suchasmajordepressionorschizophrenia,butresultingfroman“organic”etiology[24].Thus,VCIisbeginningto be recognized as encompassing many diseases, each withdifferentseverityandimpairmentpatterns.Therecognitionthatadeclineinpriorcognitiveabilityhasoccurred,asdocumentedby longitudinaldataor inferredfromapremorbidreference, isimplicitintheterm.
VASCOGrecognizesthattherearetworequirementsfordiagnosisof a cognitive disorder: a subjective report and objectiveevidencesofalterations.Aclinical visit foracognitivedisorderasthereasonforconsultationusuallyresultsfromaconcernbythepatientand/oran informantwhohasobservedadecreaseinthecognitivefunction.InvasculardementiaormajorVCI,thesubjective report will typically be that the individual dependsonother toplanormakedecisions, hashad to leave complexprojects, repeats the same conversation, needs remindersto perform a task, has significant difficulties with expressiveor receptive language, has problems to navigate a familiarenvironment,orhasclearalterationinbodyschema,capabilitytocalculate,readorwrite[23].
RecommendationsTheconceptofVCIisaconstructcoveringtheentirespectrumofcognitivedisordersrangingfrommildcognitiveimpairment(MCI)through fullydevelopeddementia,duetoall formsofvascularbraininjury.Itincludesvasculardiseaseasasingleetiology,butalsoincombinationwithothercausesofcognitiveimpairment,mainly neurodegenerative disorders. Two requirements fordiagnosis of a cognitive disorder include a subjective reportand objective evidence of cognitive impairment. The criterionto distinguish aminor from amajor disorder is that cognitivedifficultiesdonot influence the subject’s capability toperformADLs, whereas these are involved in a major neurocognitivedisorder.
Diagnostic Criteria for Vascular Cognitive ImpairmentThemost commonlyusedcriteria for thediagnosisof vasculardementiaarethosestatedbytheNationalInstituteofNeurologicalDisordersandStrokeandtheAssociationInternationalepourlaRecherche et l’Enseignement enNeurosciences (NINDS-AIREN)[25],thoseadoptedbytheStateofCaliforniaAlzheimer’sDiseaseDiagnostic and Treatment Centers (ADDTC) [26], and thosecontainedinDSM-5andCIE-10.InthelastmeetingoftheVASCOG

2017Vol.8 No.5:224
4 This article is available in: www.jneuro.com
ARCHIVOS DE MEDICINAISSN 1698-9465
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
in 2013, itwas recognized that cognitive disorders of vascularetiology are a heterogeneous set of alterations with differentetiologiesandclinicalmanifestations,allofwhichareconsideredunder the term “vascular cognitive disorders” [23]. There aretwocriticalareasforthediagnosisofvasculardementia:one,thecertaintyof thepresenceofacognitivedisorder,and two, thedeterminationthatvasculardisease is thedominant, ifnot theonlypathology,whichaccountsforthecognitivedisorder.
Clinical characteristics of cognitive syndromeTo clinically establish a predominantly vascular etiology for acognitive disorder, VASCOG recommends that the followingcharacteristicsshouldbeconsideredinadditiontothesubjectivereport and objective evidences of cognitive alterations. Thealterationofexecutivefunctions,unlikememorydisturbances,isoftenthemostoutstandingfeatureofvasculardementia.Memoryimpairmentmay not be present in some cases; in others, thedisorder inepisodicmemory is typical (althoughnotexclusive)of vascular dementia. The heterogeneity of pathology in VCIsuggests that cognitive deficits will vary according to involvedbrainareaandthewayinwhichlesionsappear.Thispatternistime-related to strokes, hemorrhages or other vasculopathies[23,24]. However, sometimes it is difficult to establish thistemporal relation clinically. For example, cognitive impairmentisatitshighestlevelshortlyafterabrainhemorrhageanditmayshowasignificantimprovementoverthenextthreemonths;butpersistencebeyond thisperiod is considerednecessary for thediagnosisofcognitiveimpairment.VCIwithagradualonsetandslowprogression is usually due to small-vessel disease leadingto lesions in thewhitematter, basal ganglia, and/or thalamus[25].Thisgradualprogression isoftenmarkedbyacuteeventsthat leave subtle neurological deficits such as focal weakness,unilateral incoordination, asymmetrical reflexes, instability,short-stepgait,orsignsofParkinsonism[26].Cognitivechangesmaybeattributedtointerruptionofcortico-subcorticalcircuits,and it is likely that speed of information processing, complexattentionandexecutivefunctionsmaybeinvolved.Whitematterischemiclesionsarecommonlyassociatedwithfrontalexecutivedeficits,regardlessoftheirdistributioninthebrain[27].Vascularlesionsmaydisruptthalamus-cortical,striatal-corticalandbasalganglia-prefrontalcortexpathways,aswellascorticalandlimbicstructures; therefore, VCI is often associated with behavioralandemotionaldisturbances.Astheseneuropsychiatricfeaturesarenotspecifictovascularetiology,theyarenotconsideredascore characteristics in thediagnosis [28].A clinical history andanappropriateneurologicalexaminationmayprovideadditionalinformation,ormaybetheonlyobjectivesourceofevidence,intheabsenceofneuroimaging.Thus,awell-documentedhistoryof acute stroke is solid evidence of cerebrovascular disease,eitherfromlarge-vesseldisease,orfromembolism.Additionally,evidence isalsoprovidedbyneurologicalexaminationshowingtypical stroke signs, including hemiparesis, facial asymmetry,sensorydisorderincludingvisualfielddefectsandpseudobulbarsyndrome (supranuclear weakness in facial muscles, tongueand pharynx, spastic dysarthria, difficult swallowing and lossof emotional control) [23]. The following criteria support the
presenceofCVD,butarenotenoughbythemselvestoestablishvasculardiseaseasaprobablecauseofVCI:
1. Earlypresenceofagaitdisorder.
2. Urinary urgency or incontinence and other urinarysymptoms not explained by urological or non-cognitiveneurologicaldisease.
3. Changes in personality and mood, abulia, depression,emotional incontinence, or other subcortical deficits,including psychomotor retardation and abnormalexecutivefunction[23,25,26].
Determination of significant cerebrovascular disease (CVD)This part of the diagnostic process is based on clinical historyand neuroimaging. The demonstration of vascular lesionsin neuroimaging is essential for higher diagnostic certainty.Absence of neuroimaging data may lead to inaccuratediagnosis. Neuroimaging is also important to rule out lesscommoncauses,suchasabraintumororthenormalpressurehydrocephalus (NPH) syndrome [29]. In addition, imaging isimportant indeterminingthevascularcontributiontoADortofrontotemporal degeneration, as amixed etiology of cognitiveimpairment[30].Ingeneral,theevidenceofsignificantvascularpathology isbasedoncomputed tomography (CT)ormagneticresonanceimaging(MRI),thelatterbeingthemostsensitiveforthispurpose.Neuroimagingfindingsshouldbeinterpretedintheclinicalcontextandtheirnature,severityand locationmustbedetermined. Attempts have beenmade to define the numberof vascular lesions required to support a vascular etiology ofcognitive impairment (see section 9.3.1 below, Neuroimaging-supportedcriteria)[31,32].
Two levels of certainty are recommended for a clinical VCIdiagnosis: “probable” and “possible”. For a “probable” VCIdiagnosis, both clinical and neuroimaging criteria should bemet. Although rare, evidence of a genetic cerebrovasculardisorder will support a “probable” level of certainty [33,34].Examples include cerebral autosomal dominant arteriopathywith subcortical infarcts and leukoencephalopathy (CADASIL);cerebral autosomal recessive arteriopathy with subcorticalinfarcts and leukoencephalopathy (CARASIL); hereditaryendotheliopathy with retinopathy, nephropathy and stroke(HERNS); pontine autosomal dominant microangiopathy andleukoencephalopathy (PADMAL); retinal vasculopathy withcerebralleukodystrophy(RVCL),andtypeIVA1collagendisorder(e.g., mutations of COL4A1 gene) as well as familial forms ofcerebralamyloidangiopathy(CAA)[35].Ifclinicalcriteriaaremetbutneuroimagingisnotavailable,thecertaintyleveloftheVCIdiagnosisremains“possible.”Byobtainingcerebralimaging,thediagnosisprogressestoagreatercertaintylevel(“probable”VCI).The definitive level of diagnosis certainty is obtained throughpostmortemneuropathologicalexamination.However,theterm“definitive”VCIisnotproposedinVASCOGrecommendationsastheserecommendationsareintendedtoestablishclinicalcriteria[23].
2017Vol.8 No.5:224
5
ARCHIVOS DE MEDICINAISSN 1698-9465
© Under License of Creative Commons Attribution 3.0 License
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
Differential diagnosisGiventhat incidentalstrokesandvascularleukoencephalopathyare common in the brain of elderly people, it is important toconsiderotherpossibleetiologieswhen thepatient’s cognitiveimpairment is assessed. When a non-vascular etiology of thedementia is provided by clinical history, physical examination,and/or laboratory investigations then VCI should not be theprimary diagnosis but a contributing factor. Often, VCI is animportantcontributortoseveralneurodegenerativeetiologiesofdementia.
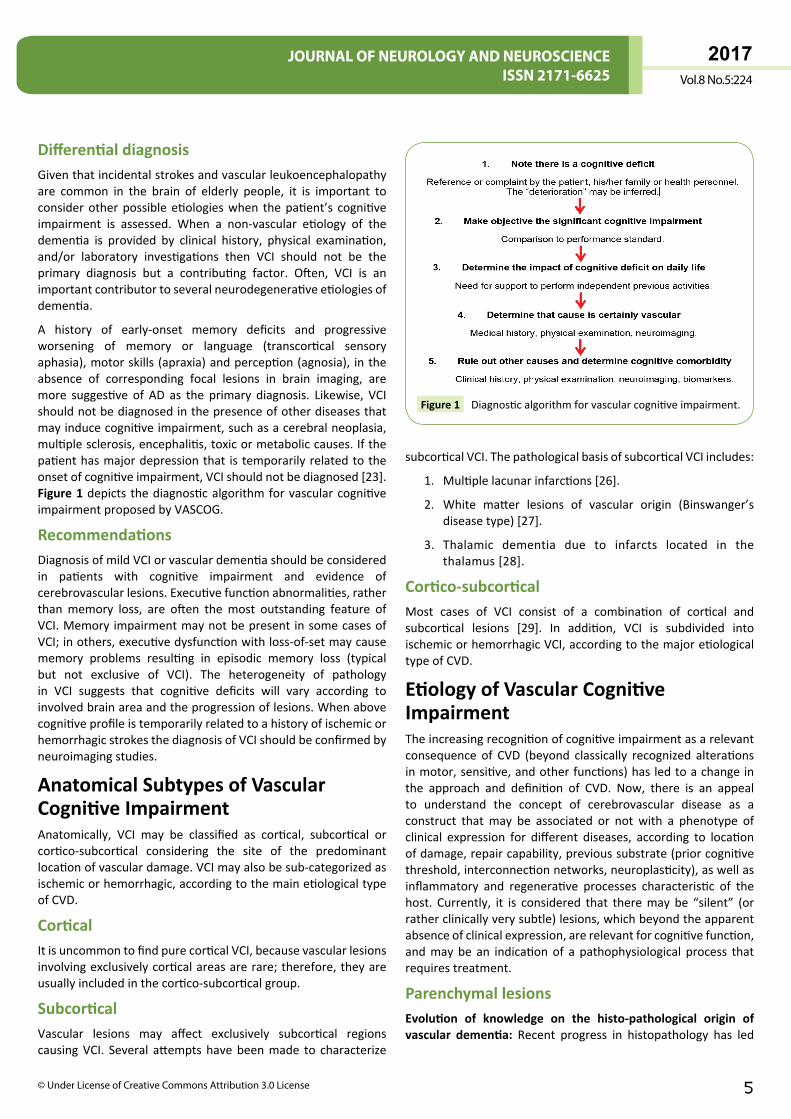
A history of early-onset memory deficits and progressiveworsening of memory or language (transcortical sensoryaphasia),motorskills(apraxia)andperception(agnosia), intheabsence of corresponding focal lesions in brain imaging, aremore suggestive of AD as the primary diagnosis. Likewise, VCIshouldnotbediagnosedinthepresenceofotherdiseasesthatmayinducecognitiveimpairment,suchasacerebralneoplasia,multiplesclerosis,encephalitis,toxicormetaboliccauses.Ifthepatienthasmajordepressionthat is temporarilyrelatedtotheonsetofcognitiveimpairment,VCIshouldnotbediagnosed[23].Figure 1depicts thediagnosticalgorithmforvascularcognitiveimpairmentproposedbyVASCOG.
RecommendationsDiagnosisofmildVCIorvasculardementiashouldbeconsideredin patients with cognitive impairment and evidence ofcerebrovascularlesions.Executivefunctionabnormalities,ratherthanmemory loss, are often themost outstanding feature ofVCI.Memoryimpairmentmaynotbepresent insomecasesofVCI;inothers,executivedysfunctionwithloss-of-setmaycausememory problems resulting in episodic memory loss (typicalbut not exclusive of VCI). The heterogeneity of pathologyin VCI suggests that cognitive deficits will vary according toinvolvedbrainareaandtheprogressionoflesions.WhenabovecognitiveprofileistemporarilyrelatedtoahistoryofischemicorhemorrhagicstrokesthediagnosisofVCIshouldbeconfirmedbyneuroimagingstudies.
Anatomical Subtypes of Vascular Cognitive ImpairmentAnatomically, VCI may be classified as cortical, subcortical orcortico-subcortical considering the site of the predominantlocationofvasculardamage.VCImayalsobesub-categorizedasischemicorhemorrhagic,accordingtothemainetiologicaltypeofCVD.
CorticalItisuncommontofindpurecorticalVCI,becausevascularlesionsinvolvingexclusivelycorticalareasarerare;therefore,theyareusuallyincludedinthecortico-subcorticalgroup.
SubcorticalVascular lesions may affect exclusively subcortical regionscausingVCI. Several attemptshavebeenmade to characterize
subcorticalVCI.ThepathologicalbasisofsubcorticalVCIincludes:
1. Multiplelacunarinfarctions[26].
2. White matter lesions of vascular origin (Binswanger’sdiseasetype)[27].
3. Thalamic dementia due to infarcts located in thethalamus[28].
Cortico-subcorticalMost cases of VCI consist of a combination of cortical andsubcortical lesions [29]. In addition, VCI is subdivided intoischemicorhemorrhagicVCI,accordingtothemajoretiologicaltypeofCVD.
Etiology of Vascular Cognitive ImpairmentTheincreasingrecognitionofcognitiveimpairmentasarelevantconsequence of CVD (beyond classically recognized alterationsinmotor,sensitive,andotherfunctions)hasledtoachangeinthe approach and definition of CVD. Now, there is an appealto understand the concept of cerebrovascular disease as aconstruct thatmay be associated or not with a phenotype ofclinical expression for different diseases, according to locationofdamage,repaircapability,previoussubstrate(priorcognitivethreshold,interconnectionnetworks,neuroplasticity),aswellasinflammatory and regenerative processes characteristic of thehost. Currently, it is considered that theremay be “silent” (orratherclinicallyverysubtle)lesions,whichbeyondtheapparentabsenceofclinicalexpression,arerelevantforcognitivefunction,andmaybe an indicationof a pathophysiological process thatrequirestreatment.
Parenchymal lesionsEvolution of knowledge on the histo-pathological origin of vascular dementia: Recent progress in histopathology has led
Diagnosticalgorithmforvascularcognitiveimpairment.Figure 1
2017Vol.8 No.5:224
6 This article is available in: www.jneuro.com
ARCHIVOS DE MEDICINAISSN 1698-9465
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
to the emergence of new concepts of cerebrovascular diseaserelevanttocognition.ThedimensionsandlocationoflesionsarerelevantparametersforVCIexpression:
Size of lesion:ItisrecognizedthatVCImayoccurwithavolumeofdamagedtissueofat least100mm3 regardlessthe location,orwith a lower volume depending on location [30]. Thus, theconceptofastrategically-localizedinfarctarises,inwhichalowervolumemayhaveagreatercognitiveimpactduetoitslocation[31,32]. However, the number of infarcts and the volume ofdamagedtissuecorrelatewithdementiadegree (mild=3cm3, moderate=29cm3,severe=63cm3)[33].
Location of lesion:Beyondthevolumeofdamagedtissue,thereare cerebral structures that becauseof theirmodular functionperforming a cognitive task or their importance as pathwaysconnectingtwocorticalareasrelevantforcognitivefunctionmaycauseVCIafterrelativelysmall lesions.Thefollowingareasarerecognizedasstrategiclesionsites[28,29,34,36,37]:
1. Limbic, paralimbic, frontal and parietal associativeheteromodalcortex.
2. Subcorticalstructuressuchasbasalforebrain,amygdala,(anterior,paramedian)thalamus,basalnuclei.
3. Papezmemorycircuit.
4. Frontal-subcortical circuits. In particular, prefrontal-caudatenucleus/thalamus/prefrontalcircuits.
5. Whitemattersubstance(subcortical,deep).
6. Cortico-corticalassociationfibers.
7. Cortico-subcorticalfibers.
8. Commissural fibers (corpus callosum, anteriorcommissure).
9. Lesionsduetodisconnectionofthepreviousmentionedstructures.
Types of vascular lesion causing cognitive impairmentIn the classical concept, major or minor vascular cognitiveimpairmentmay be secondary to lesion in small vessels, largevesselsoranassociationofboth.
Lesions in large vessels: They are most commonly caused byanatherothrombosisorcardioembolismwithocclusionoflargecerebralarteries,eitherextracranial(mainlycarotidarteries)oraffectingthemainintracranialarteries(middlecerebral,anteriorcerebralandposteriorcerebralarteries).Thisobstructioncausesmiddle or large-sized strokes causing signs of a neurologicaldisconnection decoupling modules required for the cognitiveprocess.Itmayalsooccurduetothepresenceofmultipleinfarctsin different locations,which cause a great cortical dysfunctionand a loss of different basic functions for cognition (language,memory,executivefunction,etc.).
Lesions in small vessels: These are classically consideredsecondary to lipohyalinosis, thickening of arteriolar walls
(arteriolosclerosis),andocclusionofperforatingarteriescausingasmallinfarctarea(microinfarcts,lacunes),usuallyinsubcorticalwhitematterareasorbasalganglia. Ithasalsobeendescribedassociatedwithmicroatheromatosisintheoriginofperforatingarteries.Smallvesseldiseaseisamajorriskfactorfordevelopingcognitiveimpairmentanddementia.Thefollowingtypesofsmallcerebralvessellesionsarerecognized:
1. Lacunar infarct (lacune): There isnoaconsensusaboutthe number and location of lacunes required for VCIdiagnosis.Possibly,1or2lacunesdonotcausecognitiveimpairmentinolderpeople,andtheycouldbeincidentalfindings. More than two lacunes should be considerednecessarytosupporttheVCIdiagnosis,exceptforsinglelacunesinstrategicareas.
2. Hyperintensity of the white matter:Itisassociatedwithsilentneurologicalandcognitivesymptoms.
3. Perivascular space: The general enlargement ofperivascular spaces is associated with white matterhyperintensity and lacunar infarcts. Some studies haveassociatedthemostprominentperivascularspaceswithaworsecognitivefunction.
4. Microbleeds: Lobular microbleeds have been includedin theresearchcriteria forcerebralamyloidangiopathy.New studies show an association betweenmicrobleedsandcognitiveimpairment.
In the definition of VCI neuropathological substrates, theNewcastle classification considers the following vascularalterations[35]:
1. Large infarcts or several infarcts:Aresult fromvasculardamage >50mL of infarcted brain tissue. They includemulti-infarctdementia.
2. Lacunar infarcts or multiple microinfarcts: Thoseleaving gliosis and small areas of cavitation. At least 3infarctswith aminimum sizeof 0.5mmare thought tobe necessary. This item includes microbleeds, cerebralamyloidangiopathyanddiffuseleukoencephalopathy.
3. Strategic infarcts:Theyarepresentinregionsofthalamusandhippocampus,withalowervolumebutahighimpactoncognitivefunction.
4. Cerebral hypoperfusion with hippocampal sclerosis, ischemic anoxic damage, laminar cortical necrosis, or watershed infarcts: In older subjects, hippocampalsclerosisisaccompaniedbyTDP-43proteindeposits.
5. Brain hemorrhages:eitherintracerebral(mainlylobar)orsubarachnoid.
6. Mixed dementia: Presence of cerebrovascular changeswithADpathology.
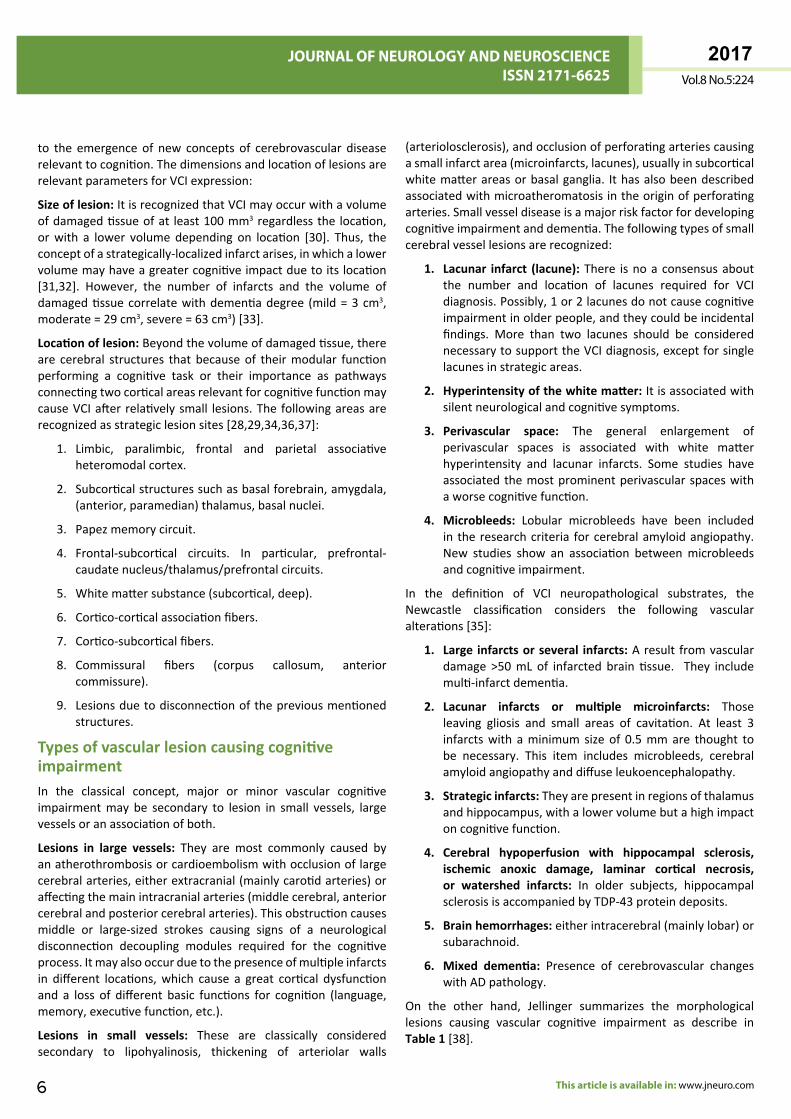
On the other hand, Jellinger summarizes the morphologicallesions causing vascular cognitive impairment as describe inTable 1[38].
2017Vol.8 No.5:224
7
ARCHIVOS DE MEDICINAISSN 1698-9465
© Under License of Creative Commons Attribution 3.0 License
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
CerebralmicrobleedsareeasilyidentifiedwithgradientechoorSwanMRI sequences; these are histopathologically defined asextravasationofbloodintotheperivascularspace.Whenlocatedinlobarregions,theyarerelatedtocerebralamyloidangiopathy,with accumulationof amyloidprotein in thewall of arterioles,whichbecomeweakandpronetorupture.Occasionally,usuallyin the context of a genetic alteration, a patient may havehundreds of microbleeds and their presence is a predictor ofcognitiveimpairment[39].
RecommendationsIt is critical toestablish the sizeand locationofvascular injuryin all patientswith CVD. It is also necessary to determine thetypeofvesselaffected(largeorsmall),sincethedamageofthelatterincludeslacunarinfarcts,microbleeds,hyper-intensitiesorperivascularspaces,whichhaveanimpactontheprognosisandtreatmentofcognitivedisorder.
Risk Factors of Vascular Cognitive Impairment Demographic and genetic factorsThemostimportantdemographicpredictorforVCIisage;thus,theagingofLatinAmericanpopulationsprobablywill leadtoahigher incidenceofVCI. There isnoanapparentdifferenceby
sexorethnicfactors,andthereisaneedforreliablegeographicalstudiesinLatinAmerica[40-42].
Regardinggenetic factors, the roleofApoEepsilon-4hasbeenstudiedforitsrelevanceinAlzheimer’sdisease,butnoassociationwithVCIhasbeenestablished[43,44].Amonggeneticdiseases,CADASIL standsout,beinganon-amyloidsmallvesselsdiseaseassociatedwithcognitiveimpairmentandevidenceofalterationinNOTCHgene[45,46].
Lifestyle factorsDiet:Ithasbeenproposedthattheintakeofantioxidantsasthosecontained in vitamin E, vitamin C and beta carotenes in dietsincludingfruitsandvegetables,orassupplements,mayreducetheriskofVCI[47-49].However,controlledclinicaltrialsdonotshowbenefitofconsumingtheseantioxidantsinthepreservationof cognitive function or its impairment reduction [50-52]. TheN-3polyunsaturatedfattyacidsinfishhaveantioxidantandanti-inflammatoryproperties,andtheyarealsothemajorcomponentsofphospholipidsofbraincellmembranes.Investigationsinthisrespecthaveshownthattheintakeoffishforseveralyears(3-6years)isassociatedwithlesserdeclineincognitivefunction[53-59].Therefore,adietrichinpolyunsaturatedfattyacidsinfishoilis recommended. The so-calledMediterraneandiet has shownincreasingevidencethatmayreducecognitiveimpairment,anditisreasonabletorecommendit[60-63].
Multifocal Disease
Largevessels(largearteriesdementia)Dementia caused by multiple infarcts:MultipleinfarctsWatershedinfarcts
Smallvessels(smallvesselsdementia)
Due to subcortical infarcts:MultiplelacunarinfarctswithperipherallesionsinthewhitematterGranularatrophyofcortex(multifocalcorticalmicroinfarcts)LacunarinfarctsandmultilacunarstateBinswanger’ssubcorticalleukoencephalopathySubcorticalangiopathies(CADASILandothers)Due to subcortical plus cortical affection: small multiple infarcts caused by:HypertensiveoratheroscleroticangiopathyCerebralamyloidangiopathywithorwithouthemorrhageCollagenorvascularinflammatorydisease(systemicorprimaryvasculitisofnervoussystem,fibromusculardysplasia)Hereditaryformsofcerebralamyloidangiopathy
Duetohypoperfusionorhypoxia/ischemia
IncompletewhitematterinfarctsIschemiarelatedtoantiphospholipidsyndromeHypoxic-ischemicencephalopathy(corticallaminarnecrosis,postcardiacarrest,hypotension)
Associatedwithvenousinfarcts LargehemorrhagicvenousinfarctsduetovenousthrombosisofsuperiorsagittalsinusorgreatveinofGalen
Hemorrhagicorigin
SubduralhematomaSubarachnoidhemorrhageIntracerebralhemorrhageMultiplemicrobleeds,especiallythosesubcortical
Focal Disease due to Strategic Lesions
Smallinfarctslocatedinfunctionallyimportantregionssuchas:
Mesial temporal CaudalandthalamicinfarctsFronto-cingularinfarctsAngulargyrusinfarctsStrategicareasofwhitematter
Table 1Morphologicallesionscausingvascularcognitiveimpairment[11].

2017Vol.8 No.5:224
8 This article is available in: www.jneuro.com
ARCHIVOS DE MEDICINAISSN 1698-9465
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
Obesity:Bodymass index(BMI) isdirectlyassociatedwithVCI.The Framingham Offspring Study showed that the higher thewaist-hip ratio was the lower cognitive function during a 12-yearfollow-up.Itisreasonabletorecommendthebodyweightcontrolforpreservingcognitivefunction[64-68].AnincreaseofBMI is associatedwithobstructive sleep apnea (OSA), a factorof vascular risk, and a frequent cause of cognitive functionimpairment.OSA causes subcortical lesions inwithematterbylesionsinsmallbrainvessels[69].
Exercise:Regular,long-termphysicalactivity,includingvigorousexerciseandwalking,hasbeenassociatedwithbettercognitivefunctionandlessimpairmentwithage.AlthoughtheLIFE studydidnotyieldpredictedresultsformoderatephysicalactivityandcognitionimprovementinsedentaryadultsaged70-89years,itdidshowthatthoseat80yearsandolderexperiencedbenefitsinexecutivefunction[70].Physiciansshouldencouragepatientsofallagestooptimizetheirlevelsofphysicalactivityfortheentirelifetoreducetheriskofdevelopingconditionsaffectingcognitionandotherdiseases[71].Therefore,thereisafavorableevidencetorecommendroutinephysicalactivityasapreventivestrategyinVCI[72-82].
Smoking: This is a well-known risk factor for ischemic andhemorrhagiccerebrovascularevents.Severalprospectivestudieshaveconfirmedhigherriskofcognitiveimpairmentinsmokers,particularlyforsomecognitivedomains.TheevidenceindicatesthatsmokingdiscontinuationisessentialforindividualsatriskofVCI[83-88].
Alcohol: Some investigations have shown certain benefit incognitionforalcoholusers,especiallyinlowtomoderateamount,compared to thosewhodonotdrinkordo itoccasionally. Forsomeauthors,thebenefitwouldoccurprimarilyinoldersubjects.However,thereisnoconclusivedataontheamountofalcohol,genderorcognitivedomainsimpacted.AlcoholabuseisassociatedwithalltypesofCVD.AlthoughmoderatealcoholconsumptionisrecommendedinpatientswithVCI[89-95],theexperienceshowsthatitisimpossibletolimitalcoholconsumptioninpatientswithcognitivedeficitwithamnesicpredominance;thus,alcoholtotalabstinenceisadvisableinthesepatients.
DepressionDepression may be a comorbidity, a prodromal factor or aconsequence of VCI rather that a factor leading to cognitiveimpairment [96-99].TheThree-City studydidnotdemonstratean association between VCI and major depression during afour-yearfollow-up[100].TheCardiovascular Health Study also couldnotconfirmit[101].Therefore,depressionisnotcurrentlyconsideredasariskfactorforVCI.Late-lifedepression(definedasthatbeginningafterage60)inacross-sectionalstudyshowedthat individuals with depression were more likely (20%) todevelopvasculardementia[102].
Chronic inflammationInflammation is a cardinal process associated with many riskfactors of neuronal and vascular damage. Plasma levels ofinflammatoryproteins,specificallyalpha-anti-chymotrypsinand
C-reactive protein (CRP), increased prior to the developmentofvasculardementiaafter8yearsof follow-up; theCRP levelsarehighupto25yearsbeforetheonsetofvasculardementia.Inanotherstudywith4-year follow-up, itwasestablished thatacombinationofhighCRPandinterleukin-6levelsresultedina3-foldincreasedriskofdevelopingvasculardementia[103-105].
Chronic renal failureSeveralstudieswithdifferentpopulationssuggestthatpatientswith moderate and severe chronic renal disease have anincreasedprevalenceofcognitiveimpairmentaffectingmultipledomains. Chronic renal failure is associated with hypertensiveencephalopathyand increasedriskofCVD.Acloserelationshipbetween the reduction of glomerular filtration rate and thepresenceofVCIhasbeendemonstrated. In theCardiovascularHealth Study [106], moderate chronic renal disease wasassociated with a higher incidence of vascular dementia.However, the association between chronic renal disease andcognitive impairmentmay be confounded because they sharevascularriskfactorsforsmall-vesseldisease[107-109].
Systemic arterial hypertensionHypertension is the main risk factor for ischemic andhemorrhagicCVD.Therelationshipbetweenbloodpressureandcardiovascular risk is consistent and independent of other riskfactors.Morethantwothirdsofpeopleover65areknowntobehypertensive.Appropriatecontrolofbloodpressurecontributesnot only to prevent CVD but also to reduce cardiac and renaldamage.Antihypertensive treatmenthasbeenassociatedwitha reduction in the incidenceofCVD from44%to35%.Systolichypertension is recognized as a risk factor to developVCI anddementia, not only of vascular type but also degenerativedementiasuchasAlzheimerdisease.Hypertensionexposesthecerebralmicrovasculaturetopulsatileflowandpressureleadingtoendothelialdamagewhichcauseslipohyalinosisandfibrinoidnecrosis. The resulting disruption of perfusion leads to thedevelopmentof lacunar infarctsor chronic ischemiaexpressedasasubcorticalvascularlesion(leukoaraiosis).Thereareseveralcross-sectional and cohort studies demonstrating the closerelationshipbetweensystolicordiastolicarterialhypertensionintheperson’shalf-lifeandthedevelopmentofvascularcognitiveimpairment[110-112].
Studieshaveshownthatthereisa“J”or“U”relationship,wheretheeffectofcontrollinghypertensiontopreventthedevelopmentofVCIiseffectivewhenthisisdonefromthemiddleofthelife,butnotwhenitistreatedlateatanadvancedage.
Diabetes mellitusPeople with diabetes mellitus (DM) have an increased riskof developing CVD, with a relative risk between 1.8 and 6dependingon the typeandseverityofDM.Also,patientswithDMareabouttwiceaslikelytodevelopdementia.SubjectswithDMhavelowerscoresintestsofmemory,processingspeedandexecutivefunctions;thesearemoreapparentwithpoorglycemiccontrol. MRI studies have shown that patients with DM havemore lacunar infarcts and hippocampal atrophy. DM is likely

2017Vol.8 No.5:224
9 This article is available in: www.jneuro.com
ARCHIVOS DE MEDICINAISSN 1698-9465
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
to influence cognitive impairment, independentlyof its roleasa vascular risk factor. Hyperglycemia acts through advancedglycation terminal products that have been found in neuriticplaquesandneurofibrillarytanglesintheearlystagesofAD.TheRotterdamstudy indicates thatDMdoubles the riskofADandVCI,particularlyinsubjectswithAPOE-4genotype.Thepresenceof repeatedand intermittenthypoglycemicepisodes in insulin-treatedpatientcauseshippocampalatrophyandcognitivedeficit[113-115].
DyslipidemiaThe role of lipid disorders on VCI remains controversial.Dyslipidemias are likely toparticipate inVCI indirectly throughthe development of atherosclerosis. Autopsy studies haverevealedthatpatientswithADshowatherosclerosisinthecircleofWillisin77%ofcases.However,mostofthestudiesassessingtheeffectivenessof statins inpatientswithdementia shownoimprovement[116,117].
Subclinical atherosclerosisSubclinicalatherosclerosisisnoninvasivelydetected,primarilybyhigh-resolutionultrasoundmeasurementofcarotidintima-mediathickening (IMT). Itmay also be assessed through studies thatmeasurearterial stiffness (essentially thecarotid-femoralpulsewavevelocity). IMThasbeenrelatedwithmostofthevascularrisk factors and the development of vascular events (CVD,coronary). A significant inverse relationship between IMT andcognitivefunctionhasbeenobserved;thegreatertheIMT,thelowerthecognitivecapacityregardlessofage,sexandtraditionalvascularriskfactors.Likewise,studiesusingcarotidpulsewavevelocity have found greater arterial stiffness in subjects withcognitiveimpairment[118,119].
Cardiovascular diseaseVCI risk has been associated with atrial fibrillation (AF), heartfailure,chronicrenaldiseaseandcoronaryandperipheralarterialdisease.AFimpactsonthedevelopmentofVCInotonlythroughthe production of cardioembolic ischemic cerebral events,but alsowith an increased risk of AD and VCI, independently,although themechanism is unknown. It has been shown thatcerebral volume in subjects with AF is lower than in controlswithout AF. It has been stated that this is a consequence ofhypoperfusion when AF has a rapid ventricular response orbecauseof thepresenceofmicroembolism.Oneof the causalfactorsofAF isunsuspectedanduntreatedOSA.On theotherhand, the reduction of cardiac output has been associatedwith a decrease in cognitive functions, in particular executivefunctions. It has been proposed that chronic hypoperfusion isthemajor contributor butmore studies should be conducted.CoronaryarterydiseaseisalsoassociatedwithanincreasedriskofVCI [120,121]. Inaddition,coronaryarterybypasssurgery isassociated with early cognitive impairment (post-surgery) andincreasedriskofdementiainthemedianterm.Finally,peripheralarterial diseasemeasured through the ankle-arm index is alsoassociatedwithahigherriskofvasculardementia[122,123].
Sleep disordersFromNurses’HealthStudy [124], itwasobserved thatwomenwhosleep5hoursor lessorthosewhosleep9hoursormoreatnighthadahigherriskofMCIcomparedtowomenwhosleep7hours.OSA isoneof the risk factorsmost frequentlymissedwhenevaluatingpatientswithVCI[125].
HyperhomocysteinemiaSeveral studies have shown that high levels of homocysteineare associatedwith an increased risk of cardiovascular events,either coronary or cerebrovascular. There is also evidencethat hyper- homocysteinemia is related to VCI, either throughcerebrovascular damage or directly. Hyperhomocysteinemiamaybedeterminedbygenetic-environmentalfactors,mutationsincriticalmetabolismenzymes,mainlymetylentetrahydrofolato-reductase(MTHFR)anddeficiencyorlowlevelsofvitaminsinvolvedinmetabolismsuchasvitaminB12andfolicacid.SomefamilieswithMTHFRgenemutationsmayhaveahistoryofdepression,suicideandalcoholism,aswellaselevatedhomocysteine.Thetreatmentofhyperhomocysteinemiawithcobalamin(vitaminB12),pyridoxine(vitamin B6) and folic acid (vitamin B9) in patients withminimalcognitive deficit stops the progression to dementia and cerebralatrophytypicalofAD[126-128].
Recommendations VCIhasbeenassociatedwith several preventable vascular riskfactorssuchashypertension,sedentarylifestyle,obesity,smoking,diabetes mellitus, hypercholesterolemia and obstructive sleepapnea. Management of these risk factors remains a practicalapproachtoreducingVCI.
Diagnostic Methods for Vascular Cognitive ImpairmentDiagnostic neuropsychological tests in vascular cognitive impairmentCognitiveimpairmentischaracterizedbyawiderangeofcognitivedeficits, but there is a predominance of executive dysfunction[129,130]. Therefore, the neuropsychological protocols shouldbesensitivetovariousdomains,withanemphasisonexecutivefunction assessment. For Latin American population, it isimportant toconsider severalaspects toconduct thecognitiveassessment: (a)education level; (b)standardizedandvalidatedtestsforstudypopulation;(c)timetoconductit,and(d)personnelwhowillconductassessments(doctor,psychologist).
There are no specific and universally accepted tests for VCIdiagnosis. There are three recommended protocols lasting 60minutes,30and10minutes.The60-minutetestmaybeusedinstudiesrequiringadetailedanalysisofcapabilitiesinthecognitivedomains.Physiciansmayusethefollowingtestsduringvisits:
30-minute tests: The clinical screening tools in patients withsuspectedVCIincludethefollowing[131]:
1. Phonologicalfluency

2017Vol.8 No.5:224
10
ARCHIVOS DE MEDICINAISSN 1698-9465
© Under License of Creative Commons Attribution 3.0 License
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
2. Semanticfluency
3. MontrealCognitiveAssessment(MoCA)
4. Digitsinregression
5. Mini-MentalStateExamination(MMSE)
6. TrialMakingTestAandB(TMTAandB)
7. HopkinsVerbalLearningTest(HVLT-R)
10-minute tests: Theseare instruments tobeusedbyprimarycare physicians, nurses, and other healthcare professionals, toallowrapiddetectionofVCI:
1. Mini-Mental State Examination (MMSE):Thisisawidelyused method to estimate the intellectual status butinsufficient to assess the executive function; its 3-wordmemorytest is insensitivetoearlydetectionofmemoryimpairmentinpatientswithVCI.
2. MoCA (Montreal Cognitive Assessment):Thisshort testdesignedtodetectcognitiveimpairmentinolderadultshasamaximumscoreof30points.TheMoCAtestissensitiveto subcortical damage. Itmay also be administered viatelephone [132,133]. The MoCA in Spanish (MoCA-S)has been validated in some countries of Latin America.In Mexico, validation showed a sensitivity of 80% andspecificityof75%,withcut-offpointof26forMCI(areaunderthecurve0.886p<.001).Forthedementiagroup,itshowedasensitivityof98%andspecificityof93%,withcut-offpointof24.(Areaunderthecurve0.998p<0.001)[134]. InColombianelderlysubjectswithloweducation,theMoCA-Shadahighreliabilitybutscoreswerestronglydependent on years of education, social and culturalfactors[135].Acompensationof3-4pointswasneededforsubjectswith<6yearsofeducation[136].
Neuropsychological tests proposed for VCI, by cognitive domainExecution/activation (planning, decision making, workingmemory,responsetofeedbackorerrorcorrections, inhibition/predominanthabits,mentalflexibility):
1. Semantic fluency [137]: A test related to left posteriorparietal-temporalregion.
2. Phonological fluency [138]: Reflecting integrity of leftdorsolateralfrontalregion.
3. Wechsler Adult Intelligence Scale (WAIS) – Digits: It evaluatesprocessingspeedandactivation.
4. Trail Making: It is a test of exploration, visual-motortracking, divided attention and cognitive flexibility.The test is very sensitive to the presence of cognitiveimpairment[139].
5. Hopkins Verbal Learning Test (HVLT-R) [140]: It may provide strategic learning measures reflecting thedorsolateral frontal function in addition to episodicmemoryrates.
6. Frontal Assessment Battery (FAB): It includes sixsubtests, which correlate with frontal lobe function.The performance in these six subtests may give acompositeglobalscore,whichassessestheseverityofthedysexecutivesyndrome[141].
7. Clock drawing test [142,143]: The common errors inexecutive function showed in this test include incorrectplacementofthehands,graphicproblems(diffuselines,smallcircle,correctionattempts)anddifficultiesinspacingnumbers.
Visuospatial (visoconstructive skills, visual perception): Thisneuropsychological test is performed through Rey-Osterreithcomplexfigure[144].Thistaskrequiresorganizationandvisuo-perceptual skill. The primary visuospatial test is administeredbycopyingtheRey-Osterreithfigure,andthememorytestwasselectedasasupplementarymeasure.
Language: Evaluation includes expressive language such asnaming objects, finding words, fluency, grammar and syntax,aswellasreceptivelanguage. Commonlanguagetestsarethefollowing:
1. The Boston Naming Test (BNT) [145]: It diagnoses thepresence and type of aphasic deficit, allowing globalassessment of difficulties in all the areas of language.Evaluationofnamingcapabilityisbyvisualconfrontation.
2. Semantic fluency:Itmayserveasalessstructuredlexicalretrievaltask.
Learning and memory: It includes immediatememory, recentmemory, free recall, evoked recall and recognition, as well aslong-term semantic and autobiographicalmemory and implicitlearning.Testsinclude:
1. HVLT-R (Hopkins Verbal Learning Test – Revised): Thisis the preferred learning test. Its strengths include amultiple-choice form and a short administration time.TheHVLT-Rdoesnotincludeaninterferencelistorakeyrecall. Clinical studieshaveshownthat it is sensitivetocognitiveimpairmentrelatedtoVCI.
2. Wechsler Memory Scale: Itallowsassessmentofverballearning capability, short- and long-term retention andrecognition capability, as well as other more specificaspects such as the interference effect or the trend torespondwithfalsepositives;itissensitivetoVCI[146,147].
3. RAVLT (Rey Auditory Verbal Learning Test) or Rey test for verbal and auditory learning:Itassessesrecognition,interference, learning curve, immediate and delayedmemory.
To establish a difference between static cognitive deficitsfollowingacerebrovasculardiseaseandtheprogressivedementiasyndrome, it is advisable to conduct serial neuropsychologicaltests,usuallyafterayearofevolution.
1. California Verbal Learning Test-II: Useful for evaluatingepisodicverballearningandmemory[148].

2017Vol.8 No.5:224
11 This article is available in: www.jneuro.com
ARCHIVOS DE MEDICINAISSN 1698-9465
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
RecommendationsThere are no specific and universally accepted tests for thediagnosisofVCI. Thereisnoidealneuropsychologicaltestandthe assessment should include sensitive tests for each type ofcognitivedisorder.MoCAisasensitivescreeningtesttodetectVCI and shouldbeused todetect early formsof this disorder.Other recommended tests include those of semantic andphonological fluency, FAB and clock test. All the tests shouldbe standardized and validated for the study population. Theassessmentof illiterateor loweducationpatients isaproblemthatrequirestheurgentdevelopmentofappropriateevaluationmethodsinLatinAmerica.
Neuroimaging studiesThe main neuroimaging choices to study VCI are MRI and CTscan.MRI isparticularlysensitive intheevaluationofcognitivedisorders characterized by small-vessel lesions. The minimumacceptable field strength is 1.0 Tesla, but ≥ 1.5 T is preferred.The following sequences are required: weighted in T1 andT2, FLAIR, and gradient echo. The first 3 sequences provideinformationontheanatomy,thepresenceofaninfarctandotherpathologies,while thegradientecho identifies thepresenceofbleeding, including small, chronic and/or acute hemorrhages.Neuroimagingfindingsshouldbeinterpretedinaclinicalcontextconsideringtheinfarctnature,severityandlocation.TheuseofArterial Spin Labeling (ASL) imaging for cerebral blood flow innon-contrastMRIisapromisingtechniqueinVCI.
Neuroimaging-supported criteria to determine vascular dementia: Although it is accepted that VCI may rarely occurwithoutevidenceofcerebralinfarctsintheneuroimagingstudies,theselesionsareusuallypresent.AsinglestrategicstrokeoranextensivestrokehavingeffectsinseveralcognitivedomainsmaybenecessarytocauseaVCI.Ifmultiple-strokediseaseisacauseofVCI,atleastoneshouldoccuroutsidethecerebellum.Ideally,there should be a temporary association between the strokeand theonsetof cognitive impairment, in suchaway that theischemic lesionprecedesthe impairmentwithinpreviousthreemonths,andthatthisimpairmentextendsbeyondthisperiod.
California criteria [26]: Two or more ischemic infarcts, withat least one of them outside the cerebellum, are required todiagnosevasculardementia.
NINDS-AIREN criteria [25]: Multiple large vessel infarcts or astrategic infarct (occurred at angular gyrus, thalamus, basalforebrain, or in the posterior or anterior carotid region) orlacunarinfarctsinthewhitematterorbasalganglia,orextensiveperiventricularlesionsinthewhitematterarerequired.
Newcastle criteria [35]: The presence of >3 lacunar infarctsshouldbeappropriateevidenceofcausality,especiallywithco-existingwhitematterdisease.
Characteristics of lacunar infarcts in neuroimaging [149]: LacunarinfarctisbetterdetectedwithaFLAIRsequenceinMRI,whichshowsthelesionasasmallhypointenseareasurroundedbyahyperintensehalo,althoughthefluidinthecentralcavityis
notsuppressedinFLAIRsometimesandmayappearcompletelyhyperintense.Lacunarinfarctiscommonlyconsideredasa3-15mmlesion,butdefinitionsvarywithmaximumdiametersof2cm.TheVCIharmonizationgrouprecommendsconsider“lacunes”upto1cm,with themaincharacteristicofbeing ischemic lesionsorsmallhemorrhagesinthedeepwhitematterofaperforatingarteriole.Giventheirsmallsize,theMRIsequencewithadjacentslices≤4mmisrequiredtodetectadequatelytheselesions.InCT,lacunarinfarctsaresmallhypodenselesions(i.e.,welldefined),but given the poor CT spatial resolution, these lacunar lesionsmayremainunnoticed.ItisimportantnotconfuselacunarlesionswithVirchow-Robinperivascularspaces,althoughthesefindingsmayreallyrepresentandearlystageofsmallvesseldiseasewithanunderlyingmicrovasculardegeneration.
Vascular lesions in sub-cortical white matter: In CT, whitematter lesions are hypodensities (leukoaraiosis). In MRI, theyare hypointense areas in T1 and hyperintense in T2-weightedimages. Subcortical vascular leukoencephalopathy may befocalormultifocal,andasthesetypesof lesionsbecomemoreextensive,theymayconvergeandinvolvealargeareaofwhitematter. Basal ganglia and thalamus also show these lesions.Whenvascularleukoencephalopathyismild,theselesionsappearassmall“caps”infrontaloroccipitalhornsoflateralventricles,orasthin“rings”surroundingthesestructures[150].However,theseimagesarenotspecifictovascular leukoencephalopathy,ascomparablepatternsmaybeobservedinseveralpathologies,includingmultiple sclerosis, cerebral edema, neurosarcoidosis,brain lesion caused by radiation, etc. Despite the diverselisting of differential diagnoses, there is clinical evidence andpathologicaldatasuggestingthatmostofthesebrainlesionsinoldersubjectshaveanischemicorigin.Theselesionsarecausedbyarteriolosclerosis,lipohyalinosisandfibrinoidnecrosisofthesmallvessels,andparticularlyalongtheperforatingarteries,withor without occlusion. Vascular leukoencephalopathy is highlyprevalent in the brains of older people and evenmiddle-agedindividuals;thus,onlyextensivelesionsareclinicallysignificant.IfvascularleukoencephalopathyisfocalandvisibleonlyinT2,itisunlikelytobesignificantenoughtoexplainthedevelopmentofcognitivedisorder.Someresearchershavesuggestedthatatleast 25%of totalwhitematter should be affected to supporta vasculardementiadiagnosis. Therefore, it is difficult tohaveprecise rules for relating leukoencephalopathy to mild VCI orvascular dementia. A general rule is that these lesions shouldbe extensive and confluent and the above descriptions areconsideredaspatternsofsubcorticalvascularinvolvement.WiththedevelopmentofnewMRItechniquessuchasdiffusiontensorimaging, it has been shown that white matter that appearsnormal in T2mayalsohave anisotropyor abnormal diffusivitymatchingwith theneuropathology andbe relevant to supportthe presence of cerebrovascular damage in the presence ofcognitivealterations[151,152].
Intracranial hemorrhagic lesions: Cognitive disorders havebeen associated with intracerebral hemorrhage, subarachnoidhemorrhage, and subdural hematoma. VCI has also beenassociated with cortical and subcortical microbleeds, whichmayberelatedtohypertensionorcerebralamyloidangiopathy.

2017Vol.8 No.5:224
12
ARCHIVOS DE MEDICINAISSN 1698-9465
© Under License of Creative Commons Attribution 3.0 License
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
Thisangiopathy isaconsequenceof theaccumulationofAβ40(different from A42 that forms the plaques in AD), which isdepositedintheintimaandthemediaofthevessel,producingfragilityandhemorrhage,butalsopredisposestothickeningoftheartery,whichcausesischemia[153].Theselesionsarebettervisualized in MRI Eco-GRE sequence. Microbleeds associatedwithhypertensionare in thedeepbrainnuclei andbrainstem,whilethoseassociatedwithamyloidangiopathyandAlzheimer’sdisease has usually a lobar location. As microbleeds are notuncommonincognitivelynormalolderadults,theattributionofVCItomicrobleedsshouldbedoneonlywhentheselesionsarenumerousandaftercarefulexclusionofothercausesofcognitiveimpairment.
Cerebrovascular assessment by other studies: Doppler ultrasonographytechnologyprovidesuseful informationonthestate of cervical and intracranial arteries, complementing theinformationofparenchymalbrainlesionidentifybyneuroimagingstudies.TranscranialDopplerisadynamicstudyofcerebralbloodflowvelocitiesthathelpstodeterminefunctionalcharacteristicsandtodeducestructuralaspectsaswell.BrainperfusionisalsoassessedthroughsinglephotonemissioncomputedtomographyandCTwithxenoncontrast.Positronemissiontomography(PET)allows imaging throughregionalglucosemetabolic rates,using18F-fluorodeoxyglucose(FDG-PET).Itisusefulforestablishingthedifferentialdiagnosisofsometypesofcognitivedisorders.Thereisno characteristicpattern inpatientswith vasculardementia,anditscurrentusefulnessistoruleoutanothertypeofdementia[154].Morerecently,amyloidimagingwithcompoundssuchasradiolabeledPittsburghCompoundB(C-PIB)hasgainedagreatinterestandhasbeenproposedasabiomarkerforADimaging.ASL imaging in brain MRI measures cerebral blood flow in anoninvasiveway,itdoesnotrequireanycontrastinjection,anddoesnotexposethepatienttoradiation;furthermore,thereisagoodcorrelationbetweenASLandFDG-PET.
RecommendationsItisessentialtohaveaneuroimagingstudywhenassessingthepatientwithcognitiveimpairmentforprobablevascularetiology.BrainCT shouldbeperformed inall cases.CerebralMRI is theidealstudytocharacterizesmall-vessellesionsanditshouldberequested considering the individual clinical context for eachpatient.
Genetic and inflammatory biomarkers and their neuropathological correlation in vascular cognitive impairmentInpatientswithVCI,severalbiomarkershavebeeninvestigatedfor early detection, to discriminate neuropathological findings,to estimate prognosis and to monitor disease progression ortherapeuticresponse[155,156].Inthesecircumstances,markersrelatedtogeneticfactorsandinflammatorymediatorsinvolvedintheetiopathogenesisofVCIareofinterest.
The analysis of cerebrospinal fluid (CSF) biomarkers, alongwith clinical and neuroimaging information, may enhancethe diagnosis of different brain disorders causing cognitive
impairment[156].VasculardementiaisgenerallyrelatedtothefollowingbiomarkersinCSF:
Total tau: It is a dynamic marker of the intensity of axonaldegeneration/damage. Its levels increase in Creutzfeld-Jakobdisease,and itmayalsobe found indementiaassociatedwithVCI, cerebral trauma and AD [157-159]. The usefulness of tauproteininthediagnosisofvasculardementiaistoexcludeotheretiologies,sothattherearenocut-offpointsforthediagnosisofvascularpathology[160].
Light sub-unit of neurofilament protein:ItisthebestbiomarkerinCSFforsubcorticalaxonaldamage/degeneration.Itoccursathighconcentrationsinvasculardementia,frontotemporaldementiaanddifferentinflammatorydisorders(multiplesclerosis,dementia-AIDScomplex).ThecombinationwithanADbiomarkerindicatesthepresenceofmixeddementia[155,161-164].
CSF and serum albumin concentration index: It is the mostdefinedbiomarkerofintegrityoftheblood-brainbarrier.Thereisusuallyanelevationofthisratioinpatientswithvasculardementia(particularlyduetosubcorticalvesseldisease)[156,159,164].
Levels of tumor necrosis factor alpha (TNF-α): Thisproinflammatory cytokine mediates myelin damage. Its levelsincrease in patients with subcortical vascular dementia andcorrelatetosulfatidelevels(awhitematterdegradationmarker).Itisfoundpotentiallyhighinsubcorticalvasculardementia[165].
Sulfatides:Theyidentifypossiblewhitematterdemyelination.
Metaloproteases [166]:Theyincreasewhenthereisvascularorwhitematterdamage.Ithasbeendemonstratedthathighlevelsof some of them allow prediction of the evolution of vascularimpairment. High levels of metalloproteinase MMP-9 areassociatedwithworseprognosisforVCIcomparedtothosewitha stable disease and lowMMP-9 levels. According to imagingstudies,thereisalsoapositivecorrelationbetweenMMP-9meanvaluesandthevolumeofinfarctorischemia.MMP-9andMMP-2levelsdependontheocclusiontimeofvascularbed,whichmayextend,expandorcauseworsevasculardamage.
Other cytokines:TheassessmentofinterleukinIL-1isconsideredimportant, along with tumor necrosis factor alpha. It may beassociatedwithworsening of vascular impairment. They couldalso be correlated to the measurement of IL-10 and IL-1ra(IL-1 receptor antagonist interleukin) by exerting a potentialneuroprotective effect. IL-6 is present in acute ischemia andreflects theextentof the infarct; itcouldalsobecorrelatedtoseverityofvasculardamageinthepatientwithVCI.
Anti-inflammatory prostaglandin 15-Dpgj2: The high levels ofthis prostaglandin may correlate with better prognosis in theevolutionofVCI.
Homocysteine: Its persistent elevation matches with thepotential presence of a deleterious inflammatory process thatmay perpetuate and enhance the vascular damage with thecorrespondingprogressionofcognitiveimpairment[167].
C-reactive protein: It is known to be associated with a poorlong-termfunctionalprognosiswhenitisincreasedintheacute

2017Vol.8 No.5:224
13 This article is available in: www.jneuro.com
ARCHIVOS DE MEDICINAISSN 1698-9465
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
phaseofthecerebrovascularevent.Althoughthismarkercannotpredict the stroke progression, it is an excellent, independentpredictorofmortalityandmorbidityinCVDevolvingintoVCI.
Non-specific biomarkers used for distinctive diagnosis of vascular cognitive impairment:ThefindinginCSFoflowlevelsofamyloidbeta 42 amino acids, with high levels of hyperphosphorylatedtau, or biochemical signs of neuro-inflammation (increasedwhite blood cells, production of IgG or IgM) indicates non-vascular dementia and may be useful as negative biomarkersfor the diagnosis of pure vascular dementia. However, theimplementationofCSFbiomarkers in thediagnosticprocessofvasculardementiarequiresstandardmethodsinthecollection,storageandmeasurementofthesample[155-157].
RecommendationsAt present, there is no biomarker capable of establishing thediagnosisofVCI.Theutilityofthesebiomarkersistoconfirmthepresenceofneuronaldamageorinflammation.MorestudiesareneededtoidentifyasensitiveandspecificmarkertoestablishtheearlydiagnosisofVCI.
Mixed DementiaThe concept of mixed dementia refers to the coexistence ofa typical degenerative disease (e.g., Lewy body dementia,frontotemporal dementia, Alzheimer’s disease) and vasculardementia.Alzheimer’sdiseaseshowsthestrongestevidenceofitsinterrelationwithvascularlesions.
The term mixed dementia represents a challenge forclinicians and even for neuropathologists, and expressesthe increasing difficulty to isolate a “pure” type of dementia(vascular versus Alzheimer’s), especially in preclinical stages.At the sametime, it represents amodel for the studyof two-way interaction between vascular lesions of different types(atherosclerosis, arteriolosclerosis, amyloid angiopathy) andneuronal degeneration [168]. Vascular lesions can cause bothneurodegenerationand its typicalmarkers (e.g.,neurofibrillarytangles,β-amyloid),assimilarlyneurodegenerativepathologycanaccumulate β-amyloid compromising the cerebral vasculatureandcausevascular lesions.As longastheclassificationofpureneurodegenerativeorvascularformsremainsastheinitialsteptoclassifydementias,wewillbeforcedtodefinea“hybrid”called“mixeddementia”.TheproposedapproachfortheclassificationisdescribedinFigure 2 andconsistsofdeterminingfirstwhetherdementia (meeting the accepted criteria) is associated or notwith overt cerebrovascular lesions, to rule out pure forms inthisway.Subsequently,adistinctionisestablishedamongthoseshowingevidenceofvascular lesion,thosehavingmoreclinicaland paraclinical features of degenerative dementia despitevascularlesions,andthosehavingmoreclinicalandparaclinicalcharacteristics of vascular dementia but alsowith evidence ofneurodegenerativepathology.
Association between cerebrovascular disease and Alzheimer’s diseaseEpidemiological studies show that Alzheimer’s disease and
cerebrovascular disease share similar risk factors includinghypertension, diabetes, smoking, apolipoprotein E epsilon 4isoforms, hypercholesterolemia, chronic nephropathy and,mainly, age [169,170]. Cardiac risk factors, in particular atrialfibrillationandcongestiveheartfailure,havealsobeenassociatedwith the pathogenesis and progression of Alzheimer’s disease[168-177].
A study in Mexican patients with Alzheimer's disease andmixed dementia demonstrated aftermultivariate analysis thathypertension (OR: 1.92, p= 0.009), white matter disease (OR:3.61,p=0.001)andlacunarinfarcts(OR:3.35,p=0.014),wereassociatedwithmixeddementia[178].
Different studies have documented the overlapping ofcerebrovasculardiseaseandAlzheimer’sdisease,anassociationeven stronger in Braak stages with a lower density ofneurofibrillarytangles.Theautopsystudywith5,715casesoftheNationalAlzheimer’sCoordinatingCenterconfirmeddataontheprevalenceofcerebrovasculardiseaseandAlzheimer’sdisease,and the deleterious additive or interacting effect of vascularpathologyandAlzheimer’sdiseaseoncognition[179-181].
Likewise, aging itself has a deleterious effect on the cerebralvasculature similar to that caused by Alzheimer’s disease,as when drainage of soluble β-amyloid is affected it leads toaccumulationinvascularwallsandparenchyma,withthealreadyknownconsequencesonhomeostasisofneuronalenvironmentand cerebral perfusion [106,182]. In addition, the presence ofcerebrovasculardiseasehasbeenassociatedwithworsecognitiveperformanceinpatientswithAD,andneuropathologicalstudieshave documented that cerebrovascular disease reduces thedementia threshold in subjects with pathological diagnosis ofAD[183,184].Thus, ithasbeenproposedthatCVDcontributesto neuropathological changes of AD, including selectivecerebral atrophy and accumulation of abnormal proteins suchasβ-amyloid.On theotherhand, subcorticalADandCVDmayindependentlyaffectcorticalatrophy[185-187].
Type of vascular lesions more associated with mixed dementiaInbrainswithADandmildCVD(primarilydegenerativedementia),mostofthecerebrovascularlesionsarelacunarinfarctsinbasal
Dementia (meets criteria)
Dementia with overt vascular lesion
Dementia without overt vascular lesion
Pura vascular dementia (Vascular lesions included in criteria already described)
Dementia meeting criteria for AD with evidence of relevant vascular lesion (including evidence of amyloid angiopathy such as microbleeds)
Vascular dementia with elements characteristic of AD (e.g., marked temporal atrophy, demonstration of tau protein, β-amyloid)
Degenerative dementias
Mixed dementia
Classificationofvasculardementia.Figure 2

2017Vol.8 No.5:224
14
ARCHIVOS DE MEDICINAISSN 1698-9465
© Under License of Creative Commons Attribution 3.0 License
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
ganglia and white matter, with multiple microinfarcts. Thispattern of topographic distribution of cerebrovascular lesionsis very similar to that observed in “pure” vascular dementia(vascular dementiawithout histopathology of AD greater thanexpected for the age). Sixty-eight percent are lacunar infarctsinvolvingthalamusorhippocampus,andonly32%areextensivecortico-subcorticalinfarcts.
In contrast, mixed dementia may be accompanied by lobarinfarcts and multiple cortico-subcortical lesions (57%) ratherthansubcorticallacunarinfarctsorstrategicinfarcts(43%).Thissuggests different pathogenicmechanisms between these twoentities, which give greater importance tomicroangiopathy inpurevasculardementiaorADwithmildcerebralvasculardiseasethaninmixeddementia,asdescribedinTable 2,whichcomparescommonlesionsinAD,VDandmixeddementia[188].
The combination of two or more pathological processes mayinfluence the severity of cognitive impairment in such a waythatcerebrovascularlesionsmayunmaskdementiaatpreclinicalstageinpatientswithAlzheimer’sdisease.However,apparentlysmall cerebrovascular lesions occurring in 10-50%of the adultpopulationwithoutcognitiveimpairmentcannotcausedementiabythemselves.
Physiopathogenesis proposed for mixed dementia MicrovascularchangesinthebrainofolderpeopleandADinducecerebralperfusionalteration,inparticular,adecreaseinregionalbloodflow,reductionofglucosetransportandutilization,withlossofvascularinnervationandaspecialimpactonthedeficitsincholinergicneurotransmissioninthecaseofAD.Likewise,thereis damage in neurovascular regulation, ultrastructural changesin capillaries and basement membranes due to depositionof β-amyloid, with disruption of the blood-brain barrier andalterationofβ-amyloidclearance.Thesuccessionoftheseeventsandotherdeleteriouseffectscreateaviciouscircle,whichfinallyproduces structural disintegration through infarcts, lacunarlesionsandvascularlesionsinwhitematter,whichcompromiseneuronal metabolism, with mitochondrial energy deficit andoxidativestress,promotingthedegradationofproteins,lesionsincytoskeletonwithformationofneuriticplaquesanddepositionof β-amyloid. These factors induce cerebral atrophy and theconsequentcognitiveimpairment.
On the other hand, atherosclerosis and amyloid angiopathycausechangesintheself-regulationofmicrovasculature,leadingtolossofmyelin,frequentlyobservedinelderlypeople’sbrains,suggesting shared risk factors for all pathological changesobservedinADandcerebrovasculardisease.Whitematterlesionscanbecausedbybothcerebralvasculardisease(hypoperfusion)andAD (retrogradedegeneration).These lesionsprogresswithage,representaconsiderableriskfactorforcognitiveimpairmentand lead to impairment in frontal functions regardlessof theirlocation[189-191].
Themostcommonclinicalexpressioninneuropsychologicaltestsis combined; i.e., they exhibit characteristics of a subcortical
cognitive profile, aswell as of cortical. However, regardless ofthepredominanceoftheclinicalpatternshowedbythepatient,inalmostallthecasesthereisaclearcompromiseoffrontalandprefrontalfunctions.
Diagnostic criteria for mixed dementiaThe clinical criteria for the diagnosis of mixed dementia arediverseandposedifficultiesforthestudyofthisconditionasanindependententity.The InternationalClassificationofDiseases(ICD-10) does not consider mixed dementia an isolated entitybutincludesitintheADsection“G30.8:OtherAlzheimer’s-typeDiseases(atypicalandmixedforms)”.
The classificationby theConsortium to Establish a Registry for Alzheimer’s Disease (CERAD) [192] does not consider mixeddementiainitsclassification,whilethecriteriaoftheAlzheimer’s Disease Diagnostic and Treatment Centers (ADDTC) requiretheevidenceofaCVDcloselyrelatedtodementia(referredtowithoutatimeframework),inadditiontothetypicalpathologyof AD [26]. The NINDS-AIREN criteria suggest to demonstratean evidence of memory compromise and at least two othercognitive areas, in addition to an evidence of cerebrovascularlesion(focalneurologicalsignsandinfarcts/lesioninbrainwhitematterimaging),andthattheonsetofdementiaoccurswithin3monthsfromtheoccurrenceofthecerebrovascularevent[25].
In2011,theAHA/ASArecognizedthatvascularanddegenerativepathologies are frequent and coexisting disorders in elderlypeople,andthatseparatelyeachaddstotheotherthepossibilityofdevelopingcognitiveimpairmentanddementiawithoverlappingclinical and neuroimaging phenotypes. Additionally, there isa need to resolve the concerns by establishing a relationshipbetweenneuroimagingfindingsandpostmortemstudies[169].First, by improving the resolution capacity of neuroimagingstudies, as they currently can detect macroscopic infarcts ofmore than 3 mm, but fail to detect microscopic infarcts andsmallvesselsdisease (suchasarteriolosclerosis).Second,somevascular pathologies may represent vascular or degenerativeprocess, as degeneration of white matter, measured in FLAIRsequence and by diffusion, as well as microbleeds, measuredbyecho-gradient sequence, areassociatedwithboth cognitivevasculardisorderandAD[193-195],andpathologystudieshave
Pathology AD (%) VD (%) Mixed dementia (%)
Totalinfarcts 10-20 100 30-40Small vessel disease Approx.50 >50 >50Lacunarinfarcts 30-46 70 60-70
Whitematterpathology 40 80 70-80Intracerebralhemorrhage 10-15 15 10
Cerebralamyloidangiopathy 98 30 Approx.90Lossofcholinergicmarkers 75 40 Approx.70
Atherosclerosis 45-60 60 Approx.60AD:Alzheimer’sDisease;VD:VascularDementia.
AdaptedfromJellingerKA,AttemsJ(JNeurolSci2007,257:80-87).
Table 2 Vascular lesions comparison between AD, VD and mixeddementia.

2017Vol.8 No.5:224
15 This article is available in: www.jneuro.com
ARCHIVOS DE MEDICINAISSN 1698-9465
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
shown that white matter degeneration and microbleeds arerelatedtolipohyalinosis[196,197].
On the other hand, changes in hippocampal volume may berelated to AD-type or vascular pathology [198] in such a waythat the atrophy of hippocampusmay occur in response to adegenerative or vascular process [199]. The different criteriaused so far formixeddementiaaround theworldaredetailedcomparativelyinTable 3[24-26,200-202].
Gold et al. [203] compared the clinical findings to theneuropathologicaldiagnosisin113elderlysubjectswithdementiaundergoing autopsy. The subjects were neuropathologicallyclassifiedwithmixed dementia if theymet the criteria for ADandforvasculardementia.Alltheclinicalcriteriaexaminedhadadifferentbehaviorwhendiagnosingmixeddementiabehavior.The proportion of cases neuropathologically diagnosed withmixeddementiawhichhavebeenclinicallyclassifiedasvasculardementiawas54%forADDTC,29%fortheNINDS-AIRENcriteria,and18%fortheHachinskiscale.TheHachinskiscaleallowedtoexcludemorecasesofmixeddementiabutfailedtoidentifymanycasesofvasculardementia.TheADDTCandNINDS-AIRENcriteriaweremoresensitivetodetectvasculardementia,but lessabletodistinguishbetweenvasculardementiaandmixeddementia.Mixed dementia was better excluded with NINDS-AIREN thanwithADDTC. The authors reported thatmixeddementiahas asignificant effect on the acuity of the diverse clinical criteria.Recentdata from the samegrouphave confirmed that clinicalcriteria for vascular dementia are not equivalent to those formixedfementiaandworkverydifferentlywithrespecttomixeddementiadetection.Furthermore,restrictivecriteriasuchasICD-10ortheprobablecategoryofADDTCandNINDS-AIRENdonotcorrelate significantly tohistopatological diagnoses. In ameta-analysis,Moroneyetal.foundthatHachinskiscaledistinguishedwell between AD and VD, but it had difficulties with mixeddementiadiagnosis[204].
From the above mentioned, we conclude that there are novalidated and accepted clinical-pathological criteria for thediagnosis of mixed dementia and therefore there are onlyrecommendations for its diagnosis, many of them based onhistopathological findings. Jellinger considers the followingsuggestions[188]:
1. National Institute of Aging(NIA)criteriaassessingplaques(including diffuse plaques as neuritic-NPs) in neocortexandhippocampusperunit,correctedforage.
2. Criteria based in the semi-quantitative assessment ofplaquesandNFTsinneocortexandhippocampus.
3. CERAD criteria using the semi-quantitative NPs countadjustedforage,towhichtheclinicalhistoryofdementiaisaddedtoestablishtheprobabilityofAD.
4. Topographic categorization of neuritic (neurofibrillary)changes,with6stages:entorhinal(1and2),hippocampal(3and4)andneocortical(5and6).
5. Quantitative criteria of the University ofWashington, amodificationoftheNIAconsensuscriteria1985.
6. TheguidesofNIAandRonaldandNancyReaganResearchInstitute of theAlzheimer’s Association (NIA-RI)make apostmortemdiagnosisofADbycombiningtheCERADandBraakcriteria.Thisleadsustoestablishalowprobability(CERAD=0-A,Braak=1-2),mediumprobability (CERADB,Braak3-4)orhighprobability(CERADC,Braak5-6)thatdementiaiscausedbyAD.
7. VD/VCIclusterallthecaseswherecognitivecompromisecanbeattributedtocerebrovasculardisease(CVD)anditisgreaterthanthatexpectedfornormalaging.VDwouldbe a type located at the end of VCI, where cognitivecompromiseissevereenoughtointerferewithsocialandoccupationalactivities.
VCI is a “continuum” emerging from the initial appearanceof vascular risk factors, which generate CVD and thencerebrovascular damage, which according to its locationcauses different types of cognitive compromise. CVD includesarteriolosclerosis, atherosclerosis, amyloid angiopathy andCADASIL,whilecerebrovasculardamagerelatestoabrainlesioncaused by CVD,whichwill depend on the size of the involvedartery, i.e., lesion in largearteriesandlesions insmallarteries.In the first case, it can cause total occlusion andwewill haveaninfarct,withadeficientclinicalpicture,generallymotor,thatalongthemonthsmayevolveintocognitiveimpairment,whichis known as post-VCD dementia (or post-stroke dementia). Inthecaseofcerebrovasculardamagecausedby lesionsofsmallarteries, we have two probable settings, which finish in theclassic lacunar state syndromes and Binswanger syndrome,depending on complete or incomplete artery occlusion. Thus,apathologicalexaminationis importantfor,first,confirmingordetecting cerebral vascular damage, especially for lesions thatcannotbedetectedbyneuroimagingtechniques(smallinfarcts,selective neuronal loss, microinfarcts); second, confirmingor identifying the type of underlying CVD (arteriolosclerosis,amyloidangiopathy,etc.);and third, toassess thepresenceormatchingextensionofanAD-typepathology.Jellingerproposes
Source Criteria
HachinskiscaleScalebasedonclinicaldata:≤4=AD,≥7=VD;middlescoreof5or6=MD
InternationalClassificationofDiseases(ICD10thedition) CasesmettingcriteriaforADandVD.
Diagnostic and Statistical ManualofMentalDisorders(DSM-V)
CaseswithcriteriaforAlzheimer-typeprimary degenerative dementia andclinicalorneuroimagingdataforVD.
Alzheimer’sDiseaseDiagnosticandTreatmentCenters(ADDTC)
Presenceofisquemiccerebrovasculardisease and a second cerebral orsystemicdisorder.
National Institute of NeurologicalDisordersandStrokeandAssociationInternationalepourlaRecherche´etl’Enseignement en Neurosciences(NINDS-AIREN)*
Typical AD data associated withclinicalandradiologicalevidenceofcerebrovasculardisease.
AD:Alzheimer’sDisease;VD:VascularDementia.MD:MixedDementia.*TheydonotcallitMDbutADwithcerebrovasculardisease.
Table 3Criteriaformixeddementia.

2017Vol.8 No.5:224
16
ARCHIVOS DE MEDICINAISSN 1698-9465
© Under License of Creative Commons Attribution 3.0 License
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
a combination of autopsy-proven AD and multiple lacunarinfarcts or lesions causing cerebrovascular damage in cortex,basal ganglia, thalamus, hippocampus and white matter, withapproximately30-50mLofinfarctedcerebralvolume.
Due to the difficulty to make available technological devices(MRIwithmoreTeslaunits,PittsburghcompoundB,etc.)andahistopathologyinmostofthecases,anoperating definition for mixeddementiaisrecommendedtouseit inasteppedwayasfollows:
1. Carrierofcardiovascularandcerebrovascularriskfactors,eitherknownornotbythepatientat thetimeof initialevaluation.
2. Defined diagnosis of dementia,without considering theneuropsychologicalphenotype.
3. MRneuroimagingwith1.5Teslaorgreaterdemonstratingvascularlesionsotherthan:
• Lobarinfarctorhemorrhage
• Strategiclesions(e.g.:thalamic)
• Extensivevascularlesions(Fazekasscale3)
• Age,whichhasagreaterimportanceinthepathophysiologyof both diseases. The detection at early stages, at ayoungerage,hasagreaterrelevanceasaftertheageof85mostofthecasesaredefinedandadvanced,andeventhecases of degenerative dementiawill already have a notnegligible“lesionburden”.Ontheotherhand,hereditaryforms of Alzheimer’s disease have an early onset. Forexample,themeanageatonsetis46.8years(range:36-42years)withanaveragedurationofupto8yearswithafataloutcomeinpatientswithdominantE280Amutationofthepresenilin-1genepresentinAntioquia(Colombia).Thesecasesarecharacterizedbythepresenceofminimalcerebrovascularlesions,incontrasttoformsoflate-onsetAD[205].
Strategies to Prevent Vascular Cognitive ImpairmentThere are several therapeutic interventions that can prevent,delay the onset or slow down the progression of vascularcognitiveimpairment,whicharedescribedinTable 4[206-208]:
The main impact on the modification of natural history ofcognitive alterations related to cerebrovascular disorders isachievedwhentherapeuticinterventionsareappliedintheearlystagesofcognitiveimpairment[209],butespeciallywhentheyareconductedbeforeVCIdevelops.ThesemeasuresnotonlyhelptopreventVCIbutalsohavefavorableresultsinneurodegenerativedisorderssuchasAlzheimer’sdisease.
Health care efforts should be focused on primary preventivemeasures, including the modification of known vascular riskfactors[206,207,210,211].Thedirectimpactontheimprovementof cognitive functions through the appropriate control ofsmoking, hypertension [212,213] and the Mediterranean diet
[60-63]isespeciallyrelevant.
Different studies and systematic reviews have demonstratedthatcognitivetrainingisaneffectivewaytoobjectivelyimprovethecognitivefunction.ACochranereview in2012[214]pointsoutthatcognitivestimulationprogramsdemonstratedbenefitsin the treatment of patients with mild MCI and moderatedementia.Arelationbetweenmentalactivitydevelopedearly,inthemiddleandlatelife,andasignificantreductionofdementiahasbeenobservedintheadvancedage(OR:0.54).AmultivariateapproachtoreducingriskforcognitivedeclinewastestedintheFINGER study (Finnish Geriatric Intervention Study to PreventCognitiveImpairmentandDisability)[215].Authorsfoundoverallthatcognitiveperformanceimprovedsignificantlywithamulti-component lifestyle intervention involving physical activity,nutritional guidance, cognitive training, and social activities, aswellasmanagementofvascularriskfactors.
RecommendationsIn the absence of a disease-modifying treatment or cure forCVI, reducing the risk of developing vascular dementia takeson added importance. There is sufficiently strong evidence toconcludethatahealthydiet,managementofmodifiablevascularrisk factors (diabetes,obesity, smoking,andhypertension)andlifelong learning and cognitive trainingmay reduce the risk ofcognitivedeclineandmayreducetheriskofdementia.
Pharmacological TreatmentThe main randomized controlled trials in patients with VCItreatedwithpharmacologicinterventionsshowsomebenefitforimproving cognition. However, none have received regulatoryapprovalparticularlybecausethelowereffectsizescomparedtoAD.Consideredthepreviousaspects,themaindrugsarebrieflyreviewed[216].
InterventionsEvidence
quality (GRADE System)
Strategy recommendations
Lifestyle factorsSmokingdiscontinuation B1 ReasonableModeratealcoholintake B1 Itcanbereasonable
Weightcontrol B1 ItcanbereasonablePhysicalactivity A1 Advisable
Mediterranean diet B1 AdvisablePhysiological factors
Treatmentofhypertension A1 AdvisableTreatmentofhyperglycemia B1 Itcanbereasonable
Treatmentofhypercholesterolemia B1 Itcanbereasonable
Other interventionsVitaminsupplements A2 Not demonstratedCognitivestimulation B1 Advisable
Multimodalintervention B1 Advisable
Table 4 Strategies for therapeutic intervention in vascular cognitiveimpairment.

2017Vol.8 No.5:224
17 This article is available in: www.jneuro.com
ARCHIVOS DE MEDICINAISSN 1698-9465
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
DonepezilIt is a specific and reversible acetylcholinesterase (AChE)inhibitor that increases acetylcholine (ACh) levels. Severalstudiesusingdonepezilforvasculardementiahavebeenpublished. Two randomized, double blind, controlled studiesin 1219 patients with possible or probable vascular cognitiveimpairmentshouldbementioned; inthem,5or10mgdailyofthedrugwereadministeredfor6months,comparedtoplacebo.Significant benefits were found in cognition, global functionand functionality in activities of daily life in patients receivingdonepezil,therebyinferringitseffectiveness[217,218].
Recommendation Grade:A1
RivastigmineThis pseudo-irreversible inhibitor of acetylcholinesterase andbutyrylcholinesterase, facilitates cholinergic neurotransmissionbyslowingdegradationofacetylcholinereleasedbyfunctionallyintactcholinergicneurons.
A double-blind, randomized clinical trial assessed theeffectivenessofrivastigminetreatment(3-12mg/day)comparedtoplaceboinpatientswithvasculardementiafor6months.Theresultsdidnotprovideconsistentefficacy[219].Theothertrialcomparedrivastigmine(9mg/day)withplaceboinpatientswithmildcognitiveimpairmentfor6monthsoftreatment,providingsomebenefitintheexecutivefunctioning[220].
Recommendation Grade:B2
GalantamineIt is a competitive, reversible acetylcholinesterase inhibitor. Itshows allostericmodulation of the nicotinic receptor (nAChR),andbonds tonAChR inaplaceother thanacetylcholine (ACh).When it merges simultaneously with ACh at their respectivebindingsites, thepresynapticnicotinicreceptorbecomesmoresensitivetoAChandamplifiesitsresponse.
Galantamine has been assessed in two clinical trials crucial toknowthebenefitsofthisdrug.Adouble-blind,randomizedclinicaltrialusedgalantamine(24mg/day)in592patientswith“pure”vascular dementiaas “mixed” vascular dementia for 6monthsoftreatment,showingabenefitoverplaceboincognition,globalassessment, activities of daily life and behavioral symptoms[221]. The other trial in 788 patients diagnosed with “pure”vascular dementia assessed the effectiveness of galantaminetreatmentwith24mg/day,comparedtoplacebofor26weeks.Theresultsshowedabenefitincognitionandexecutivefunctionswithgalantamine[222,223].
Recommendation Grade:B1
MemantineItisanon-competitive,voltage-dependent,antagonistwithlow/moderate affinity for NMDA (N-methyl-D-aspartate) receptors;it blocks the excitotoxic effects of pathologically increasedglutamatetoniclevelsthatmaycauseneuronaldysfunction.
Twoclinicaltrialscomparedmemantine(20mg/day)toplaceboin mild to moderate vascular dementia for 28 weeks. Dataanalysisshowedanimprovementincognitivefunctions,butnotintheglobalclinicalimpressionnorintheactivitiesofdailylife,inthosetreatedwithmemantine[224,225].
Recommendation Grade:B2
NimodipineItbindstoL-typecalciumreceptorsandreducesthenumberofopenchannelstransportingcalciumionsthroughcellmembrane.Ithasavasodilatingactiononarteriolesandcanmodulateothercalciumdependentprocessessuchasthereleaseofacetylcholine.Thebindingsitesare inneuronsandcerebrovascularcells,andtheir action can influence both neural conduction and brainbloodflow.
ACochrane2002reviewanalyzedthreestudiesusingnimodipine(90mg/day)between12and24weeksinpatientswithvasculardementia,andabenefitwasfoundinsomecognitionandglobalassessmentscales[226]Amulticenter,double-blind,randomizedstudy comparing nimodipine (90 mg/day) to placebo for thetreatment of subcortical vascular dementia for 52 weeks waspublished,withoutfindingabenefitinthecognitionscales[227].
Recommendation Grade:B2
CiticolineIt stimulates the biosynthesis of structural phospholipids inthe neuronal membrane. It inhibits the activation of certainphospholipases (A, A2, C and D) and preserves the neuronalenergyreserve,inhibitingapoptosisandstimulatingthesynthesisof acetylcholine. It improves the brain function by interactingwithseveralneurotransmittersandreceptors,aswellasduetoitsvasoactiveandantibindingproperties.
AsystematicCochrane2005reviewincluded14clinicaltrials;theeffectsofciticolineonthetreatmentofcognitive,emotionalandbehavioral deficits associated with chronic cerebral disordersin older people were analyzed. There were difficulties due toheterogeneity of the articles, but even with these technicaldifficulties there was evidence of certain benefit for memory,behaviorandglobalclinicalimpressioninthemediumandshortterm,especiallyinpatientswithcognitivedeficitsassociatedwithcerebrovascular disorders [228]. Subsequently, a randomized,open-labelstudycomparingciticolinetoplacebofor12monthswas published to assess the effectiveness of citicoline inpreventing post-stroke cognitive impairment in patients whohadafirstischemicstrokeevent;benefitsinexecutivefunctionandguidancewerefound[229,230].Simultaneously,theIDEALEstudywaspublished,comparingoralciticoline(1000mg/day)toplaceboformildVCIfor9months.Theresultsobtainedshowedaslightbutnon-significantdifferenceinthegeriatricdepressionscalescore,andalsothatMMSEscoreremainedunalteredoverthetime[17,231].Atwo-yeartreatmentandfollow-upstudywithciticolinepublishedin2016havingasobjectivetomeasurethequalityoflifeandcognitivestatusinpatientswhohadsufferedafirststrokedemonstratedthatciticoline(1g/day)isassociated

2017Vol.8 No.5:224
18
ARCHIVOS DE MEDICINAISSN 1698-9465
© Under License of Creative Commons Attribution 3.0 License
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
with an improved quality of life (EuroQol-5D) in both elderlyand young patients, and significantly improved the cognitivestatus(p=0.005)aftertwoyearsoftreatment,followingafirststroke.Inaddition,onlytheciticolinetreatedgroup(vs.standardmeasures)sustainedcognitiveimprovementafterthefirstyearoftreatment[232].
Recommendation Grade:B2
EGB 761 (Ginkgo biloba). Ginkgo bilobahasantioxidant,vasoactiveandneurotransmitter-modulatingproperties.
IntheCochrane2002review,itwasconcludedthatthebenefitof Ginkgo biloba (unspecified dose) for people with dementiaor cognitive impairment is inconsistent and unreliable.Subsequently, a multicenter, double-blind, randomized studywasconductedtodemonstratetheeffectivenessofGinkgo biloba (240mg/day) compared to placebo in 410 patientswithmild-moderatedementia(vasculardementiaorAlzheimer’sdisease)for24weeks.TheresultsshowedabenefitofusingGinkgo biloba comparedtoplacebo incognition,psychopathology, functionalmeasuresandqualityoflifeforpatientsandcaragivers[233].
Recommendation Grade:B2
CerebrolysinIthasneurotrophicmechanismssuchasantiapoptopicactivity,modulation of anti-inflammatory response, reduction of freeradicals,modulationofCDK5andGSK3βactivity,neuroplasticityandneurogenesis.
In a randomized, double-blind, prospective clinical trialconducted with cerebrolysin in 242 patients over 50 years ofage diagnosed with mild-moderate vascular dementia, 20 mLintravenous cerebrolysin were administered once daily for24 weeks, comparing to placebo. The cerebrolysin treatmentshowed that cognitive function, overall function, daily lifeactivities and executive functions improved significantly[234,235].Subsequently,aCochrane2013reviewwaspublishedandanalyzed6studiesusing10-30mLintravenouscerebrolysindailywithavariableduration(agerange:60-71years)inpatientsdiagnosedwithmild-moderatevasculardementia,andabenefitin some scales of cognition and global assessment was found[236].
Recommendation Grade: C2
PiracetamItisacyclicderivativeofgamma-aminobutyricacid(GABA)thatcancrosstheblood-brainbarrierandisselectivelyconcentratedinthecerebralcortex.Itrestoresthefluidityinthecellmembrane,inducingthelipidreorganizationandstimulatingthesynthesisofmembranephospholipidsandcholineuptake in themuscariniccholinergicnerveendings.Atlowdoses,piracetamincreasestheutilizationofoxygenandglucosethroughtheenergypathwaysofadenosinetriphosphate(ATP).Athigherdoses,itopposestoplateletaggregationandhasantithromboticeffects.
TheCochrane2001reviewdidnotdemonstrateanybenefitwithpiracetaminpatientswithdementiaorcognitiveimpairment[237].
Recommendation Grade: C2
PropentophyllineThis acts on the blood-brain barrier by blocking adenosineand inhibiting the phosphodiesterase enzyme; it also inhibitsthe production of free radicals and reduces the activation ofmicroglialcells.
A Cochrane 2003 meta-analysis concluded that there is nosufficient evidence to demonstrate beneficial effects with thisdrugon cognition, global function and activitiesof daily life inpeoplewithAlzheimer’sdiseaseand/orvasculardementia[238].
Recommendation Grade: C2
RecommendationsTreatments of vascular cognitive impairment have shownmodest cognitive improvements with donepezil, galantamineandmemantine, although these improvements haveuncertainclinicalsignificance.
ConclusionThereisinsufficientdatatorecommendtheuseofthesedrugsinageneralizedwayinpatientswithvascularcognitiveimpairment,sotheirindicationmustbeindividualized.
References1 GBD 2015 Mortality and Causes of Death Collaborators (2016)
Global, regional, and national life expectancy, all-cause mortality,andcause-specificmortalityfor249causesofdeath,1980–2015:asystematicanalysisfortheGlobalBurdenofDiseaseStudyof2015.Lancet388:1459-1554.
2 PrinceM,WimoA,GuerchetM,AliG,WuY,etal. (2015) InformeMundialsobreelAlzheimer2015.Lasconsecuenciasdelademenciaanálisis de prevalencia, incidencia, coste y tendencias. Londres:Alzheimer’sDiseaseInternational.
3 O'BrienJT,ThomasA(2015)Vasculardementia.Lancet386:1698-1706.
4 DeCarvalhoJJ,AlvesMB,VianaGA,MachadoCB,DosSantosBF,etal.(2011)Strokeepidemiology,patternsofmanagement,andoutcomesinFortaleza,Brazil:ahospital-basedmulticenterprospectivestudy.Stroke42:3341-3346.
5 PorcelloMarroneLC,DiogoLP,DeOliveiraFM,TrentinS,ScalcoRS,etal. (2013)Risk factorsamongstrokesubtypes inBrazil. J StrokeCerebrovascDis22:32-35.
6 Saposnik G, Del Brutto OH (2003) Stroke in South America: A

2017Vol.8 No.5:224
19 This article is available in: www.jneuro.com
ARCHIVOS DE MEDICINAISSN 1698-9465
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
systematic review of incidence, prevalence, and stroke subtypes.Stroke34:2103-2107.
7 Marquez-RomeroJM,ArauzA,Gongora-RiveraF,BarinagarrementeriaF,CantuC(2015)TheburdenofstrokeinMexico.IntJStroke10:251-252.
8 BahitMC,CoppolaML,RiccioPM,CiprianoLE,RothGA,etal.(2016)First-everstrokeandtransientischemicattackincidenceand30-daycase-fatalityrates inapopulation-basedstudy inArgentina.Stroke47:1640-1642.
9 Lavados PM, Sacks C, Prina L, Escobar A, Tossi C, et al. (2005)Incidence, 30-day case-fatality rate, and prognosis of stroke inIquique,Chile:a2-yearcommunity-basedprospectivestudy(PISCISproject).Lancet.365:2206-2215.
10 Cabral NL, Cougo-Pinto PT,Magalhaes PS, Longo AL,Moro CH, etal.(2016)Trendsofstrokeincidencefrom1995to2013inJoinville,Brazil.Neuroepidemiology46:273-281.
11 Cantu-BritoC,MajersikJJ,SanchezBN,RuanoA,QuiñonesG,etal.(2010)HospitalizedstrokesurveillanceinthecommunityofDurango,Mexico: thebrain attack surveillance inDurango study. Stroke41:878-884.
12 Cantu-BritoC,MajersikJJ,SanchezBN,RuanoA,Becerra-MendozaD,etal.(2011)Door-to-doorcaptureofincidentandprevalentstrokecases inDurango,Mexico:thebrainattacksurveillanceinDurangostudy.Stroke42:601-606.
13 MelconCM,MelconMO(2006)PrevalenceofstrokeinanArgentinecommunity.Neuroepidemiology27:81-88.
14 ThriftAG,CadilhacDA,ThayabaranathanT,HowardG,HowardVJ,etal.(2014)Globalstrokestatistics.IntJStroke9:6-18.
15 Nitrini R, Bottino CM, Albala C, Custodio Capuñay NS (2009)Prevalence of dementia in Latin America: a collaborative study ofpopulation-basedcohorts.InterPsychogeriatr21:622–630.
16 RizziL,RossetI,RorizCM(2014)Globalepidemiologyofdementia:Alzheimer'sandvasculartypes.BiomedResInt2014:908915.
17 ArauzA,RodríguezAY,SosaAL,ChávezM,PazF,etal.(2014)Vascularcognitive disorders and depression after first-ever stroke: theFogarty-MexicoStrokeCohort.CerebrovascDis38:284-289.
18 FerriCP,PrinceM,BrayneC,BrodatyH, Fratiglioni L, et al. (2005)Global prevalence of dementia: A Delphi consensus study. Lancet3667:2112-2117.
19 AlonsoCP,OxmanAD,MobergJ,BrignardelloPR,AklEA,etal.(2016)GRADE Evidence to Decision (EtD) frameworks: A systematic andtransparentapproachtomakingwell informedhealthcarechoices.2:ClinicalpracticeguidelinesBMJ.353:i2089.
20 ReisbergB, Ferris SH, KlugerA, FranssenE,Wegiel J, et al. (2008)Mild cognitive impairment (MCI): A historical perspective. IntPsychogeriatr20:18-31.
21 PetersenRC,SmithGE,WaringSC,IvnikRJ,TangalosEG,etal.(1999)Mildcognitiveimpairment:Clinicalcharacterizationandoutcomes.ArchNeurol56:303-308.
22 Petersen RC, Roberts RO, KnopmanDS, Boeve BF, Geda YE, et al.(2009)Mildcognitive impairment:Tenyears later.ArchNeurol66:1447-1455.
23 Sachdev P, Kalaria R, O’Brien J, Skoog I, Alladi S, et al. (2014)Diagnostic criteria for vascular cognitive disorders: a VASCOGstatement.AlzheimerDisAssocDisord28:206–218.
24 American Psychiatric Association (2013) Diagnostic and Statistical
ManualofMentalDisorders(5thedn)(DSM-5).AmericanPsychiatricPublishing,Washington,DC,USA.
25 Román GC, Tatemichi TK, Erkinjuntti T, Cummings JL, Masdeu JC,et al. (1993) AIREN International Workshop. Vascular dementia:diagnosticcriteriaforresearchstudies.ReportoftheNINDS-AIRENInternationalWorkshop.Neurology43:250-260.
26 ChuiHC,VictoroffJI,MargolinD,JagustW,ShankleR,etal.(1992)CriteriaforthediagnosisofischemicvasculardementiaproposedbytheStateofCaliforniaAlzheimer'sDiseaseDiagnosticandTreatmentCenters.Neurology42:473-80.
27 Roman GC (1987) Senile dementia of the Binswangeer type: Avascularfromofdementiaintheelderly.JAMA258:1782–1788.
28 CarreraE,BogousslavskyJ(2006)Thethalamusandbehavior:Effectsofanatomicallydistinctstrokes.Neurology66:1817-1823.
29 ZekryD,DuyckaertsC,BelminJ,GeoffreC,HerrmannF,etal.(2003)Thevascularlesionsinvascularandmixeddementia:theweightoffunctionalneuroanatomy.NeurobiolAging24:213-219.
30 DelSerT,BermejoF,PorteraA,ArredondoJM,BourasC,etal.(1990)Vasculardementia:Aclinicopathologicalstudy.JNeurolSci96:1-17.
31 TomlinsonBE,BlessedG,RothM(1970)Observationsonthebrainsofdementedoldpeople.JNeurolSci11:205-242.
32 Brun A (1994) Pathology and pathophysiology of cerebrovasculardementia:Puresubgroupsofobstructiveandhypoperfusiveetiology.Dementia5:145-147.
33 ErkinjunttiT,HaltiaM,PaloJ,SulkavaR,PaetauA(1988)Accuracyoftheclinicaldiagnosisofvasculardementia:aprospectiveclinicaland post-mortem neuropathological study. J Neurol NeurosurgPsychiatry51:1037-1044.
34 SkrobotOA,O'BrienJ,BlackS,ChenC,DeCarliC,etal.(2017)TheVascular Impairment of Cognition Classification Consensus Study.AlzheimersDement13:624-633.
35 KalariaRN,KennyRA,BallardCG,PerryR,InceP,etal.(2004)Towardsdefining the neuropathological substrates of vascular dementia. JNeurolSci226:75-80.
36 Lanna ME, Alves CE, Sudo FK, Alves G, Valente L, et al. (2012)Cognitive disconnective syndrome by single strategic strokes invasculardementia.JNeurolSci322:176-183.
37 Catani M, Mesulam M (2008) The arcuate fasciculus and thedisconnectiontheme in languageandaphasia:historyandcurrentstate.Cortex44:953-961.
38 JellingerKA(2013)Pathologyandpathogenesisofvascularcognitiveimpairment–Acriticalupdate.FrontAgingNeurosci5:17.
39 Van der Flier WM, Cordonnier C (2012) Microbleeds in vasculardementia:Clinicalaspects.ExpGerontol47:853-857.
40 RinconF,WrigthCB(2013)Vascularcognitive impairment.CurrentOpinioninNeurology26:29-36.
41 ChuiHC(2007)Subcorticalischemicvasculardementia.NeurolClin25:717-740.
42 Leyds D, Hénon H,Mackowiak-CordolianiaMA, Pasquier F (2005)Poststrokedementia.LancetNeurol4:752-759.
43 Kim KW, Youn JC, Han MK, Paik NJ, Lee TJ, et al. (2008) Lack ofassociation between apolipoprotein E polymorphism and vasculardementiainKoreans.JGeriatrPsychiatryNeurol21:12-17.
44 KullerLH,LopezOL,JagustWJ,BeckerJT,DeKoskyST,etal.(2005)

2017Vol.8 No.5:224
20
ARCHIVOS DE MEDICINAISSN 1698-9465
© Under License of Creative Commons Attribution 3.0 License
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
Determinants of vascular dementia in the cardiovascular healthcognitionstudy.Neurology64:1548-1552.
45 ChabriatH,BousserMG(2003)CADASIL:Cerebralautosomaldominantarteriopathywithsubcorticalinfarctsandleukoencephalopathy.AdvNeurol92:147-150.
46 OpherkC, PetersN,Herzog J, LuedtkeR,DichgansM (2004) Longterm prognosis and causes of death in CADASIL: a retrospectivestudyin411patients.Brain127:2533-2539.
47 Cherubini A, Martin A, Andres LC, Di Iorio A, Lamponi M, et al.(2005)VitaminElevels,cognitiveimpairmentanddementiainolderpersons:theInCHIANTIstudy.NeurobiolAging26:987-994.
48 JamaJW,LaunerLJ,WittemanJC,DenBreeijenJH,BretelerMM,etal.(1996)Dietaryantioxidantsandcognitivefunctioninapopulation-basedsampleofolderpersons:theRotterdamstudy.AmJEpidemiol144:275–280.
49 Morris MC, Evans DA, Tangney CC, Bienias JL, Wilson RS (2006)Associations of vegetable and fruit consumption with age-relatedcognitivechange.Neurology67:1370–1376.
50 KangJH,GrodsteinF(2008)Plasmacarotenoidsandtocopherolsandcognitivefunction:aprospectivestudy.NeurobiolAging29:1394–1403.
51 Kang JH, CookNR,Manson JE, Buring JE, Albert CM, et al. (2009)VitaminE,vitaminC,betacarotene,andcognitivefunctionamongwomenwithoratriskofcardiovasculardisease:thewomen'santi-oxidantandcardiovascularstudy.Circulation119:2772–2780.
52 HeartProtectionStudyCollaborativeGroup(2002)MRC/BHFHeartProtectionStudyofantioxidantvitaminsupplementationin20,536high-risk individuals:Arandomisedplacebo-controlledtrial.Lancet360:23-33.
53 BourreJM(2006)Effectsofnutrients(infood)onthestructureandfunctionofthenervoussystem:Anupdateondietaryrequirementsforbrain,part2:Macronutrients.JNutrHealthAging10:386-399.
54 ChewEY,ClemonsTE,AgrónE,LaunerLJ,GrodsteinF,etal.(2015)Effect of omega-3 fatty acids, lutein/zeaxanthin, or other nutrientsupplementation on cognitive function. The AREDS2 randominzeclinicaltrial.JAMA314:791-801.
55 KalmijnS,FeskensEJ,LaunerLJ,KromhoutD(1997)Polyunsaturatedfattyacids,antioxidants,andcognitivefunctioninveryoldmen.AmJEpidemiol145:33-41.
56 HeudeB,DucimetièreP, BerrC (2003)Cognitivedecline and fattyacid compositionoferythrocytemembranes: theEVAStudy.Am JClinNutr77:803-808.
57 BeydounMA,KaufmanJS,SatiaJA,RosamondW,FolsomAR(2007)Plasma n-3 fatty acids and the risk of cognitive decline in olderadults:theAtherosclerosisRiskinCommunitiesStudy.AmJClinNutr85:1103-1111.
58 KalmijnS,vanBoxtelMP,OckeM,VerschurenWM,KromhoutD,etal.(2004)Dietaryintakeoffattyacidsandfishinrelationtocognitiveperformanceatmiddleage.Neurology62:275-280.
59 VandeRestO,SpiroA,Krall-KayeE,GeleijnseJM,DeGrootLC,etal.(2009) Intakesof (n-3) fattyacidsand fattyfisharenotassociatedwith cognitive performance and 6-year cognitive change in menparticipating in theVeteransAffairsNormativeAgingStudy. JNutr139:2329-2336.
60 Scarmeas N, Stern Y,Mayeux R,Manly JJ, Schupf N, et al. (2009)Mediterraneandietandmildcognitiveimpairment.ArchNeurol66:
216-225.
61 Féart C, Samieri C, Rondeau V, Amieva H, Portet F, et al. (2009)Adherence to aMediterranean diet, cognitive decline and risk ofdementia.JAMA.302:638-648.
62 Tangney CC, KwasnyMJ, Li H,Wilson RS, Evans DA, et al. (2011)AdherencetoaMediterraneandietandage-relatedcognitivedeclinearandomizedclinicaltrial.AmJClinnNutr93:601-607.
63 Valls-PedretC,Sala-VilaA,Serra-MirM,CorellaD,DelaTorreR,etal. (2015)Mediterraneandiet andage-related cognitivedecline: arandomizedclinicaltrial.JAMAInternMed175:1094-1103.
64 GustafsonDR,KarlssonC,SkoogI,RosengrenL,LissnerL,etal.(2007)Mid-life adiposity factors relate to blood-brain barrier integrity inlatelife.JInternMed262:643-650.
65 Beydoun MA, Beydoun HA, Wang Y (2008) Obesity and centralobesity as risk factors for incident dementia and its subtypes: asystematicreviewandmeta-analysis.ObesRev9:204-218.
66 FitzpatrickAL,KullerLH,LopezOL,DiehrP,O'MearaES,etal.(2009)Midlifeandlate-lifeobesityandtheriskofdementia:cardiovascularhealthstudy.ArchNeurol66:336-342.
67 StewartR,MasakiK,XueQL,PeilaR,PetrovitchH,etal. (2005)A32-year prospective study of change in bodyweight and incidentdementia:TheHonolulu-AsiaAgingStudy.ArchNeurol62:55-60.
68 WolfPA,BeiserA, EliasMF,AuR,VasanRS, et al. (2007)Relationofobesitytocognitivefunction: importanceofcentralobesityandsynergisticinfluenceofconcomitanthypertension:TheFraminghamHeartStudy.CurrAlzheimerRes4:111–116.
69 Román GC (2011) Pathogenesis of cerebral small-vessel diseasein obstructive sleep apnea. In: CulebrasA, (ed) Sleep, Stroke, andCardiovascularDisease,Chapter8.CambridgeUniversityPress,NewYork,USA.pp:97-113.
70 SinkKM,EspelandMA,CastroCM,ChurchT,CohenR,etal.(2015)LIFE Study Investigators. Effect of a 24-month physical activityinterventionvshealteducationoncognitiveoutcomesinsedentaryolderadults.TheLIFERandomizedTrial.JAMA34:781-790.
71 GillSD,SeltzDP(2015)Lifestylesandcognitivehealth.Whatolderindividualscandotooptimizecognitiveoutcomes.Editorial. JAMA314:774-775.
72 WeuveJ,KangJH,MansonJE,BretelerMM,WareJH,etal.(2004)Physical activity, includingwalking, andcognitive function inolderwomen.JAMA292:1454–1461.
73 SturmanMT,MorrisMC,MendesdeLeonCF,BieniasJL,WilsonRS,etal.(2005)Physicalactivity,cognitiveactivity,andcognitivedeclineinabiracialcommunitypopulation.ArchNeurol62:1750-1754.
74 LarsonEB,WangL,BowenJD,McCormickWC,TeriL,etal. (2006)Exerciseisassociatedwithreducedriskforincidentdementiaamongpersons65yearsofageandolder.AnnInternMed144:73-81.
75 RavagliaG,FortiP, LucicesareA,PisacaneN,RiettiE,etal. (2008)Physical activity and dementia risk in the elderly: findings from aprospectiveItalianstudy.Neurology70:1786-1794.
76 AngevarenM,AufdemkampeG,VerhaarHJ,AlemanA,Vanhees L(2008)Physical activityandenhancedfitness to improvecognitivefunction in older people without known cognitive impairment.CochraneDatabaseSystRev16:CD005381.
77 SoumaréA,TavernierB,AlpérovitchA,TzourioC,ElbazA(2009)Across-sectional and longitudinal studyof the relationshipbetween

2017Vol.8 No.5:224
21 This article is available in: www.jneuro.com
ARCHIVOS DE MEDICINAISSN 1698-9465
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
walkingspeedandcognitivefunctionincommunity-dwellingelderlypeople.JGerontolABiolSciMedSci64:1058-1065.
78 Yaffe K, Fiocco AJ, Lindquist K, Vittinghoff E, Simonsick EM, et al.(2009)Predictorsofmaintainingcognitivefunctioninolderadults:theHealthABCstudy.Neurology72:2029-2035.
79 VergheseJ,CuilingW,KatzMJ,SandersA,LiptonRB(2009)Leisureactivitiesandriskofvascularcognitiveimpairmentinolderadults.JGeriatrPsychiatryNeurol22:110-118.
80 LiuAT,EngJJ,BoydLA, JacovaC,Davis JC,etal. (2010)Promotionof the mind through exercise (PROMoTE): a proof-of-conceptrandomized controlled trial of aerobic exercise training in olderadultswithvascularcognitiveimpairment.BMCNeurol10:14.
81 BakerLD,FrankLL,Foster-SchubertK,GreenPS,WilkinsonCW,etal.(2010)Effectsofaerobicexerciseonmildcognitiveimpairment:acontrolledtrial.ArchNeurol67:71–79.
82 SofiF,ValecchiD,BacciD,AbbateR,GensiniGF,etal.(2011)Physicalactivityandriskofcognitivedecline:Ameta-analysisofprospectivestudies.JInternMed269:107-117.
83 KalmijnS,VanBoxtelMP,VerschurenMW,JollesJ,LaunerLJ(2002)Cigarettesmokingandalcoholconsumptioninrelationtocognitiveperformanceinmiddleage.AmJEpidemiol156:936-944.
84 AnsteyKJ,VonSandenC,SalimA,O'KearneyR (2007)Smokingasariskfactorfordementiaandcognitivedecline:ameta-analysisofprospectivestudies.AmJEpidemiol166:367-378.
85 SabiaS,MarmotM,DufouilC,SinghMA(2008)Smokinghistoryandcognitive function inmiddle age from theWhitehall II study.ArchInternMed168:1165-1173.
86 Poorthuis RB, Goriounova NA, Couey JJ, Mansvelder HD (2009)Nicotinic actions on neuronal networks for cognition: generalprinciples and long-term consequences. Biochem Pharmacol 78:668-676.
87 SabiaS,ElbazA,DugravotA,HeadJ,ShipleyM,etal.(2012)Impactof smoking on cognitive decline in early old age: theWhitehall IIcohortstudy.ArchGenPsychiatry69:627-635.
88 North TL, Palmer TM, Lewis SJ, Cooper R, Power C, et al. (2015)Effectofsmokingonphysicalandcognitivecapabilityinlaterlife:amulticohortstudyusingobservationalandgeneticapproaches.BMJOpen5:e008393.
89 Elias PK, Elias MF, D'Agostino RB, Silbershatz H, Wolf PA (1999)AlcoholconsumptionandcognitiveperformanceintheFraminghamHeartStudy.AmJEpidemiol150:580-589.
90 GanguliM,VanderBiltJ,SaxtonJA,ShenC,DodgeHH(2005)Alcoholconsumption and cognitive function in late life: a longitudinalcommunitystudy.Neurology65:1210–1217.
91 StampferMJ,KangJH,ChenJ,CherryR,GrodsteinF(2005)Effectsofmoderatealcoholconsumptiononcognitivefunction inwomen.NEnglJMed352:245-253.
92 StottDJ,FalconerA,KerrGD,MurrayHM,TrompetS,etal. (2008)Does low to moderate alcohol intake protect against cognitivedeclineinolderpeople?JAmGeriatrSoc56:2217-2224.
93 KimJW,LeeDY,LeeBCH,JungMH,KimH,etal.(2012)Alcoholandcognitionintheelderly:Areview.PsychiatryInvestig9:8-16.
94 BernardinF,Maheut-BosserA,PailleF(2014)Cognitiveimpairmentsinalcohol-dependentsubjects.FrontPsychiatry5:78.
95 Sameer J, Marshall EJ, Smith ID (2014) Alcohol and cognitiveimpairment.BJPsychAdvances20:304-313.
96 YaffeK,BlackwellT,GoreR,SandsL,ReusV,etal.(1999)Depressivesymptomsandcognitivedeclineinnondementedelderlywomen:aprospectivestudy.ArchGenPsychiatry56:425-430.
97 GanguliM,DuY,DodgeHH,RatcliffGG,ChangCC(2006)Depressivesymptoms and cognitive decline in late life: a prospectiveepidemiologicalstudy.ArchGenPsychiatry63:153-160.
98 HammarA,ArdalG(2009)Cognitivefunctioninginmajordepression-Asummary.FrontiersinHumanNeuoscience3:26.
99 GodinO,DufouilC,RitchieK,Dartigues JF,TzourioC,etal. (2007)Depressive symptoms,major depressive episode and cognition intheelderly:thethree-citystudy.Neuroepidemiology28:101-108.
100 Papazacharias A, Nardini M (2012) The relationship betweendepression and cognitive deficits. Psychiatria Danubina 24:S179-S182.
101 Barnes DE, Alexopoulos GS, Lopez OL, Williamson JD, Yaffe K(2006)Depressivesymptoms,vasculardisease,andmildcognitiveimpairment: findings from the Cardiovascular Health Study. ArchGenPsychiatry63:273-279.
102 CankurtaranM,YavuzBB,CankurtaranES,HalilM,Ulger Z, et al.(2008)Riskfactorsandtypeofdementia:VascularorAlzheimer?.ArchGerontolGeriatr47:25-34.
103 EngelhartMJ,GeerlingsMI,MeijerJ,KiliaanA,RuitenbergA,etal.(2004) Inflammatoryproteins inplasmaandtheriskofdementia:theRotterdamstudy.ArchNeurol61:668-672.
104 SchmidtR, SchmidtH,Curb JD,MasakiK,White LR, et al. (2002)Early inflammation and dementia: a 25-year follow-up of theHonolulu-AsiaAgingStudy.AnnNeurol52:168–174.
105 RavagliaG,FortiP,MaioliF,ChiappelliM,MontesiF,etal. (2007)Blood inflammatorymarkers and risk of dementia: the ConseliceStudyofBrainAging.NeurobiolAging28:1810-1820.
106 Seliger SL, SiscovickDS, Stehman-Breen CO,GillenDL, FitzpatrickA, et al. (2004)Moderate renal impairment and riskofdementiaamongolder adults: the CardiovascularHealth Cognition Study. JAmSocNephrol15:1904-1911.
107 Etgen T, Sander D, Chonchol M, Briesenick C, Poppert H, et al.(2009)Chronickidneydiseaseisassociatedwithincidentcognitiveimpairmentintheelderly:theINVADEstudy.NephrolDialTransplant24:3144-3150
108 KurellaM, Yaffe K, ShlipakMG,Wenger NK, ChertowGM (2005)Chronic kidney disease and cognitive impairment in menopausalwomen.AmJKidneyDis45:66–76.
109 EliasMF, Elias PK, Seliger SL, Narsipur SS, Dore GA, et al. (2009)Chronic kidney disease, creatinine and cognitive functioning.NephrolDialTransplant24:2446–2452.
110 Int Veld BA, Ruitenberg A, Hofman A, Stricker BH, Breteler MM(2001) Antihypertensive drugs and incidence of dementia: TheRotterdamStudy.NeurobiolAging22:407-412.
111 LaunerLJ,RossGW,PetrovitchH,MasakiK,FoleyD,etal. (2000)Midlife blood pressure and dementia: The Honolulu-Asia agingstudy.NeurobiolAging21:49-55.
112 Skoog I, Nilsson L, Persson G, Palmertz B, Andreasson LA, et al.(1996)15-yearlongitudinalstudyofbloodpressureanddementia.Lancet347:1141-1145.
113 ChengG,HuangC,DengH,WangH(2012)Diabetesasariskfactor

2017Vol.8 No.5:224
22
ARCHIVOS DE MEDICINAISSN 1698-9465
© Under License of Creative Commons Attribution 3.0 License
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
for dementia and mild cognitive impairment: A meta-analysis oflongitudinalstudies.InternMedJ42:484–491.
114 McCrimmonRJ,RyanCM,FrierBM(2012)Diabetesandcognitivedysfunction.Lancet379:2291-2299.
115 SaediE,GheiniMR,FaizF,AramiMA(2016)Diabetesmellitusandcognitiveimpairments.WorldJDiabetes7:412-422.
116 AnsteyKJ,LipnickiDM,LowLF(2008)Cholesterolasariskfactorfordementiaandcognitivedecline:Asystematicreviewofprospectivestudieswithmeta-analysis.AmJGeriatrPsychiatry16:343-354.
117 RichardsonK,SchoenM,FrenchB,UmscheidC,MitchellM,etal.(2013) Statins and cognitive function: A systematic review. AnnInternMed159:688–697.
118 FeinkohlI,KellerM,RobertsonCM,MorlingJR,WilliamsonRM,etal.(2013)Clinicalandsubclinicalmacrovasculardiseaseaspredictorsof cognitive decline in older patients with type 2 diabetes: TheEdinburghType2DiabetesStudy.DiabetesCare36:2779-2786.
119 Hajjar I, Goldstein FC, Martin GS, Quyyumi AA (2016) Roles ofarterial stiffness and blood pressure in hypertension-associatedcognitivedeclineinhealthyadults.Hypertension67:171-175.
120 Rosano C, Naydeck B, Kuller LH, Longstreth WT Jr, Newman AB(2005) Coronary artery calcium: associationswith brainmagneticresonanceimagingabnormalitiesandcognitivestatus.JAmGeriatrSoc53:609-615.
121 VidalJS,SigurdssonS,JonsdottirMK,EiriksdottirG,ThorgeirssonG,etal.(2010)Coronaryarterycalcium,brainfunctionandstructure:theAGES-ReykjavikStudy.Stroke41:891–897.
122 LaurinD,MasakiKH,WhiteLR,LaunerLJ(2007)Ankle-to-brachialindex and dementia: the Honolulu-Asia Aging Study. Circulation116:2269-2274.
123 NewmanAB,FitzpatrickAL, LopezO, JacksonS, LyketsosC,etal.(2005)DementiaandAlzheimer'sdiseaseincidenceinrelationshiptocardiovasculardiseaseintheCardiovascularHealthStudycohort.JAmGeriatrSoc53:1101–1107.
124 Devore EE, Grodstein F, Duffy JF, StampferMJ, Czeisler CA, et al.(2014)Sleepdurationinmidlifeandlaterlifeinrelationtocognition.JAmGeriatrSoc62:1073-1081.
125 ChangWP,LiuME,ChangWC,YangAC,KuYC,etal. (2013)Sleepapneaandtheriskofdementia:Apopulation-based5-yearfollow-upstudyinTaiwan.PLoSOne8:e78655.
126 WaldDS,LawM,MorrisJK(2002)Homocysteineandcardiovasculardisease:evidenceoncausalityfromameta-analysis.BrMedJ325:1202–1206.
127 KalmijnS,LaunerLJ,LindemansJ,BotsML,HofmanA,etal.(1999)Total homocysteine and cognitive decline in a community-basedsampleofelderly subjects. TheRotterdamStudy.Am JEpidemiol150:283-289.
128 Quadri P, Fragiacomo C, Pezzati R, Zanda E, Forloni G, et al.(2004) Homocysteine, folate, and vitamin B-12 in mild cognitiveimpairment,Alzheimerdisease,andvasculardementia.AmJClinNutr80:114–122.
129 Garrett KD, Browndyke JN, Whelihan W, Paul RH, DiCarlo M, etal. (2004) The neuropsychological profile of vascular cognitiveimpairment–no dementia: Comparisons to patients at riskfor cerebrovascular disease and vascular dementia. Arch ClinNeuropsychol19:745-757.
130Nyenhuis DL, Gorelick PB, Geenen EJ, Smith CA, GenchevaE, et al. (2004) The pattern of neuropsychological deficits invascular cognitive impairment-no dementia (vascular CIND). ClinNeuropsychol18:41-49.
131 Hachinski V, Iadecola C, Petersen RC, Breteler MM, NyenhuisDL, et al. (2006) National Institute of Neurological Disorders andStroke-Canadian Stroke Network vascular cognitive impairmentharmonizationstandards.Stroke37:2220-2241.
132 NasreddineZS,PhillipsNA,BédirianV,CharbonneauS,WhiteheadV,etal.(2005)TheMontrealCognitiveAssessment,MoCA:abriefscreeningtoolformildcognitiveimpairment.JAmGeriatrSoc53:695-699.
133 PendleburyST,MarizJ,BullL,MehtaZ,RothwellPM(2012)MoCA,ACE-R, and MMSE versus the National Institute of NeurologicalDisordersandStroke-CanadianStrokeNetworkVascularCognitiveImpairment Harmonization Standards Neuropsychological BatteryafterTIAandstroke.Stroke43:464-469.
134 AguilarNS,MimenzaAA,PalaciosGA, SamudioCA,GutiérrezGL,etal.(2017)ValidezyconfiabilidaddelMoCA(MontrealCognitiveAssessment)paraeltamizajedeldeteriorocognoscitivoenMéxico.RevistaColombianadePsiquiatria.
135 Gómez F, Zunzunegui M, Lord C, Alvarado B, García A (2013)ApplicabilityoftheMoCA-StestinpopulationswithlittleeducationinColombia.IntJGeriatrPsychiatry28:813-820.
136 ZhouY,OrtizF,NuñezC,ElashoffD,WooE,etal.(2015)UseoftheMoCAinDetectingEarlyAlzheimer'sDiseaseinaSpanish-SpeakingPopulationwithVariedLevelsofEducation.DementGeriatrCognDisExtra5:85-95.
137 Carew TG, Lamar M, Cloud BS, Grossman M, Libon DJ (1997)Impairment in category fluency in ischemic vascular dementia.Neuropsychology11:400-412.
138 LamarM,PriceCC,DavisKL,KaplanE,LibonDJ(2002)Capacitytomaintainmentalsetindementia.Neuropsychologia40:435-445.
139 AlexanderMP,StussDT,ShalliceT,PictonTW,GillinghamS(2005)Impaired concentration due to frontal lobe damage from twodistinctlesionsites.Neurology65:572-579.
140 EslingerPJ,GrattanLM(1994)Alteredserialpositionlearningafterfrontallobelesion.Neuropsychologia32:729–739.
141 DuboisB,SlachevskyA,LitvanI,PillonB(2000)TheFAB:AFrontalAssessmentBatteryatbedside.Neurology55:1621-1626.
142 ShulmanKI(2000)Clock-drawing:Isittheidealcognitivescreeningtest?.IntJGeriatrPsychiatry15:548-561.
143 Eknoyan D, Hurley RA, Taber KH (2012) The clock drawing task:common errors and functional neuroanatomy. J NeuropsychiatryClinNeurosci24:260-265.
144 OsterriethPA(1944)Letestdecopied’unefigurecomplexe.ArchPsychologie30:206-356.
145 Franzen M, Haut M, Rankin E, Keefover R (1995) Empiricalcomparison of alternative forms of the Boston naming test. ClinNeuropsychol9:225-229.
146 Suades-GonzálezE,Jódar-VicenteM,Pérdrix-SolàsD(2009)Memorydeficit in patients with subcortical vascular cognitive impairmentversusAlzheimer-type dementia: The sensitivity of the 'word list'subtestontheWechslerMemoryScale-III.RevNeurol49:623-629.
147 O’Sullivan M, Morris RG, Markus HS (2005) Brief cognitive

2017Vol.8 No.5:224
23 This article is available in: www.jneuro.com
ARCHIVOS DE MEDICINAISSN 1698-9465
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
assessmentforpatientswithcerebralsmallvesseldisease.JNeurolNeurosurgPsychiatry.76:1140-1145.
148 Delis DC, Kramer JH, Kaplan E, Ober BA (2000) California VerbalLearning Test – (2nd edn), Adult version. Manual. PsychologicalCorporation,SanAntonio,Texas,USA.
149 WardlawJM,SmithEE,BiesselsGJ,CordonnierC,FazekasF,etal.(2013)StandardsforReportingVascularchangesonnEuroimaging(STRIVEv1).Neuroimagingstandardsforresearchintosmallvesseldisease and its contribution to ageing and neurodegeneration.LancetNeurol12:822-838.
150WahlundLO,BarkhofF,FazekasF,BrongeL,AugustinM,etal.(2001)EuropeanTaskForceonAge-RelatedWhiteMatterChanges.Anewratingscaleforage-relatedwhitematterchangesapplicabletoMRIandCT.Stroke32:1318–1322.
151 BrownWR,Moody DM, Thore CR, Challa VR, Anstrom JA (2007)Vascular dementia in leukoaraiosis may be a consequence ofcapillarylossnotonlyinthelesions,butinnormal-appearingwhitematterandcortexaswell.JNeurolSci257:62-66.
152 Hilal S, SikkingE, ShaikMA,ChanQL,VanVeluwSJ, et al. (2016)Cortical cerebral microinfarcts on 3T MRI: A novel marker ofcerebrovasculardisease.Neurology87:1583-1590.
153 Zipfel GJ, Han H, Ford AL, Lee JM (2009) Cerebral amyloidangiopathy:progressivedisruptionoftheneurovascularunit.Stroke40:S16-S19.
154 Marcus C, Mena E, Subramaniam RM (2014) Brain PET in thediagnosisofAlzheimer'sdisease.ClinNuclMed39:e413-e422.
155 MoorhouseP,RockwoodK (2008)Vascular cognitive impairment:Currentconceptsandclinicaldevelopments.LancetNeurol7:246-255.
156 Zetterberg H, Mattsson N, Blennow K (2010) Cerebrospinal fluidanalysisshouldbeconsideredinpatientswithcognitiveproblems.IntJAlzheimersDis2010:163065.
157 Hesse C, Rosengren L, Andreasen N, Davidsson P, VandersticheleH,etal.(2001)Transientincreaseintotaltaubutnotphospho-tauinhumancerebrospinalfluidafteracutestroke.NeurosciLett297:187-190.
158 OstM, Nylén K, Csajbok L, Ohrfelt AO, TullbergM, et al. (2006)InitialCSFtotaltaucorrelateswith1-yearoutcomeinpatientswithtraumaticbraininjury.Neurology67:1600-1604.
159 Samgård K, Zetterberg H, Blennow K, Hansson O, Minthon L, etal. (2010)Cerebrospinalfluidtotal tauasamarkerofAlzheimer'sdiseaseintensity.IntJGeriatrPsychiatry25:403-410.
160 Abdalla B, Bishara B, William N, Muhamad O, Mustafa Y (2015)Candidate Biomarkers and CSF Profiles for Alzheimer’s Disease andCADASIL.InternationalJournalofBrainandCognitiveSciences4:15-27.
161 PetzoldA,KeirG,WarrenJ,FoxN,RossorMN(2007)Asystematicreview and meta-analysis of CSF neurofilament protein levels asbiomarkersindementia.NeurodegenerDis4:185-194.
162 AbdulleS,MellgrenA,BrewBJ,CinqueP,HagbergL,etal. (2007)CSF neurofilament protein (NFL) -a marker of active HIV-relatedneurodegeneration.JNeurol254:1026-1032.
163 Gisslen M, Hagberg L, Brew BJ, Cinque P, Price RW, et al.(2007) Elevated cerebrospinal fluid neurofilament light proteinconcentrationspredictthedevelopmentofAIDSdementiacomplex.JInfectDis195:1774-1778.
164 WallinA,SjögrenM(2001)Cerebrospinalfluidcytoskeletonproteins
in patientswith subcorticalwhite-matterdementia.MechAgeingDev122:1937-1949.
165 TarkowskiE,TullbergM,FredmanP,WikkelsöC(2003)CorrelationbetweenintrathecalsulfatideandTNF-alphalevelsinpatientswithvasculardementia.DementGeriatrCognDisord15:207-211.
166 BjerkeM,ZetterbergH,EdmanA,BlennowK,WallinA,etal.(2011)Cerebrospinalfluidmatrixmetalloproteinasesandtissue inhibitorofmetalloproteinasesincombinationwithsubcorticalandcorticalbiomarkers in Vascular Dementia and Alzheimer's Disease. JAlzheimersDis27:665-676.
167 RománGC (2015)MTHFRGeneMutations:Apotentialmarkeroflate-onsetAlzheimer'sdisease?.JAlzheimersDis47:323-327.
168 Kling MA, Trojanowski JQ, Wolk DA, Lee VM, Arnold SE (2013)Vasculardiseaseanddementias:Paradigmshiftstodriveresearchinnewdirections.AlzheimersDement9:76-92.
169 GorelickPB,ScuteriA,BlackSE,DecarliC,GreenbergSM,etal.(2011)Vascular contributions to cognitive impairment and dementia: astatement for healthcare professionals from the American HeartAssociation/AmericanStrokeAssociation.Stroke42:2672-2713.
170 Casserly I, Topol E (2004) Convergence of atherosclerosis andAlzheimer’s disease: inflammation, cholesterol, and misfoldedproteins.Lancet363:1139–1146.
171 ToledoJB,ToledoE,WeinerMW,JackCRJr,JagustW,etal.(2012)Cardiovascularriskfactors,cortisol,andamyloid-betadepositioninAlzheimer’sDiseaseNeuroimagingInitiative.AlzheimersDement8:483-489.
172 Polidori MC, Pientka L, Mecocci P (2012) A review of the majorvascularriskfactorsrelatedtoAlzheimer’sdisease.JAlzheimersDis32:521-530.
173 AhtiluotoS,PolvikoskiT,PeltonenM,SolomonA,TuomilehtoJ,etal. (2010) Diabetes, Alzheimer disease, and vascular dementia: apopulation-basedneuropathologicstudy.Neurology75:1195-1202.
174 HelznerEP,LuchsingerJA,ScarmeasN,CosentinoS,BrickmanAM,etal.(2009)ContributionofvascularriskfactorstotheprogressioninAlzheimerdisease.ArchNeurol66:343–348.
175 KivipeltoM,NganduT,LaatikainenT,WinbladB,SoininenH,etal.(2006) Risk score for the prediction of dementia risk in 20 yearsamongmiddleagedpeople:Alongitudinal,population-basedstudy.LancetNeurol5:735-741.
176 MielkeMM, Rosenberg PB, Tschanz J, Cook L, Corcoran C, et al.(2007) Vascular factors predict rate of progression in Alzheimerdisease.Neurology69:1850-1858.
177 QiuC,XuW,WinbladB,FratiglioniL(2010)VascularriskprofilesfordementiaandAlzheimer’sdiseaseinveryoldpeople:apopulation-basedlongitudinalstudy.JAlzheimersDis20:293-300.
178 Moreno CC,Mimenza AA, Aguilar NS, Alvarado ÁP, Gutiérrez GL,etal.(2015)Factoresasociadosademenciamixtaencomparacióncon la demencia tipo Alzheimer en adultos mayores mexicanos.Psicogeriatría5:125-130.
179 ToledoJB,ArnoldSE,RaibleK,BrettschneiderJ,XieSX,etal.(2013)Contribution of cerebrovascular disease in autopsy confirmedneurodegenerative disease cases in the National Alzheimer’sCoordinatingCentre.Brain.136:2697-2706.
180 Arvanitakis Z, Leurgans SE, Barnes LL, Bennett DA, Schneider JA(2011) Microinfarct pathology, dementia, and cognitive systems.
2017Vol.8 No.5:224
24
ARCHIVOS DE MEDICINAISSN 1698-9465
© Under License of Creative Commons Attribution 3.0 License
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
Stroke42:722-727.
181 BennettDA,WilsonRS,ArvanitakisZ,BoylePA,DeToledo-MorrellL,etal.(2013)Selectedfindingsfromthereligiousordersstudyandrushmemoryandagingproject.JAlzheimersDis33:S397-S403.
182 HawkesCA,SullivanPM,HandsS,WellerRO,NicollJA,etal.(2012)Disruption of arterial perivascular drainage of amyloid-beta fromthebrainsofmiceexpressingthehumanAPOEepsilon4allele.PLoSOne.7:e41636.
183 Ladecola C (2010) The overlap between neurodegenerative andvascularfactorsinthepathogenesisofdementia.ActaNeuropathol120:287-296.
184 RiekseRG,LeverenzJB,McCormickW,BowenJD,TeriL,etal.(2004)Effect of vascular lesions on cognition in Alzheimer’s disease: acommunity-basedstudy.JAmGeriatrSoc52:1442–1448.
185 Zlokovic BV (2005) Neurovascular mechanisms of Alzheimer’sneurodegeneration.TrendsNeurosci28:202-208.
186 ZlokovicBV(2011)NeurovascularpathwaystoneurodegenerationinAlzheimer’s disease andother disorders.Nat RevNeurosci 12:723-738.
187 DuAT, SchuffN, Chao LL, Kornak J, Ezekiel F, et al. (2005)Whitematter lesions are associated with cortical atrophy more thanentorhinalandhippocampalatrophy.NeurobiolAging26:553-559.
188 JellingerKA,AttemsJ(2007)Neuropathologicalevaluationofmixeddementia.JNeurolSci257:80-87.
189 Schmidt R, Schmidt H, Haybaeck J, Loitfelder M, Weis S, et al.(2011) Heterogeneity in age-related white matter changes. ActaNeuropathol122:171-185.
190 ArteroS,TiemeierH,PrinsND,SabatierR,BretelerMM,etal.(2004)Neuroanatomicallocalisationandclinicalcorrelatesofwhitematterlesionsintheelderly.JNeurolNeurosurgPsychiatry75:1304-1308.
191 Ihara M, Polvikoski TM, Hall R, Slade JY, Perry RH, et al. (2010)Quantificationofmyelinlossinfrontallobewhitematterinvasculardementia, Alzheimer’s disease, and dementia with Lewy bodies.ActaNeuropathol119:579-589.
192 MirraSS,HeymanA,McKeelD,SumiSM,CrainBJ,etal.(1991)TheConsortiumtoEstablishaRegistryforAlzheimer'sDisease(CERAD).Part II. Standardization of the neuropathologic assessment ofAlzheimer'sdisease.Neurology41:479-486.
193 Kirsch W, McAuley G, Holshouser B, Petersen F, Ayaz M, et al.(2009)SerialsusceptibilityweightedMRImeasuresbrain ironandmicrobleedsindementia.JAlzheimersDis17:599-609.
194 CordonnierC,VanderFlierWM,SluimerJD,LeysD,BarkhofF,etal.(2006)Prevalenceandseverityofmicrobleeds inamemoryclinicsetting.Neurology66:1356-1360.
195 LeeDY,FletcherE,MartinezO,OrtegaM,ZozulyaN,etal. (2009)RegionalpatternofWhitemattermicrostructuralchangesinnormalaging,MCI,andAD.Neurology73:1722-1728.
196 Fazekas F, KleinertR,RoobG,KleinertG,KapellerP, et al. (1999)Histopathologicanalysisoffociofsignallossongradient-echoT2*-weighted MR images in patients with spontaneous intracerebralhemorrhage: evidence of microangiopathy-related microbleeds.AmJNeuroradiol20:637-642.
197 Tanaka A, Ueno Y, Nakayama Y, Takano K, Takebayashi S (1999)Smallchronichemorrhagesandischemiclesionsinassociationwithspontaneousintracerebralhematomas.Stroke30:1637-1642.
198 JagustWJ,ZhengL,HarveyDJ,MackWJ,VintersHV,etal. (2008)Neuropathologicalbasisofmagneticresonanceimagesinaginganddementia.AnnNeurol63:72-80.
199 Zarow C, Sitzer TE, Chui HC (2008) Understanding hippocampalsclerosis in the elderly: epidemiology, characterization, anddiagnosticissues.CurrNeurolNeurosciRep8:363-370.
200World Health Organization (1993) The ICD-10 classification ofmentalandbehaviouraldisorders:Diagnosticcriteriaforresearch.En The ICD-10 classificationofmental andbehavioural disorders:Diagnosticcriteriaforresearch.WorldHealthOrganization.
201HachinskiVS, IliffLD,ZilkhaE,DuBoulayGH,McAllisterVL,etal.(1975)Cerebralbloodflowindementia.ArchNeurol32:632-637.
202 Loeb C, Gandolfo C (1983) Diagnostic Evaluation of degenerativeandvasculardementia.Stroke14:399-401.
203GoldG,BourasC,CanutoA,BergalloMF,HerrmannFR,etal.(2002)Clinicopathologicalvalidationstudyoffoursetsofclinicalcriteriaforvasculardementia.AMJPsychiatry159:82-87.
204Moroney Jt, Bagiella E, Desmond DW, Hachinski VC, Molsa PK,et al. (1997) Meta-analysis of the Hachinski ischemic score inpathologicallyverifieddementias.Neurology49:1096-1105.
205 LoperaF,ArdillaA,MartínezA,MadrigalL,Arango-VianaJC,etal.(1997)Clinicalfeaturesofearly-onsetAlzheimerdiseaseinalargekindredwithanE280Apresenilin-1mutation.JAMA277:793-799.
206 KivipeltoM,HelkalaEL,HanninenT,LaaksoMP,HallikainenM,etal. (2001)Midlife vascular risk factors and late-lifemild cognitiveimpairment:Apopulation-basedstudy.Neurology56:1683-1689.
207GorelickPB,NyenhuisD(2013)Understandingandtreatingvascularcognitiveimpairment.Continuum(MinneapMinn)19:425-437.
208 RománGC, Boller F (2014) Vascular factors in neurodegenerativediseases:Apathtowardstreatmentandprevention.FunctNeurol29:85-86.
209 Román G, Pascual B (2012) Contribution of neuroimaging to thediagnosisofAlzheimer'sdiseaseandvasculardementia.ArchMedRes43:671-676.
210 Cukierman-YaffeT,GersteinHC,WilliamsonJD,LazarRM,LovatoL,et al. (2009) Relationship between baseline glycemic control andcognitive function in individuals with type 2 diabetes and othercardiovascularriskfactors:theactiontocontrolcardiovascularriskin diabetes-memory in adiabetes (ACCORD-MIND) trial. DiabetesCare32:221-226.
211 RománGC,NashDT,FillitH (2012)Translatingcurrentknowledgeintodementiaprevention.AlzheimerDisAssocDisord26:295-299.
212 Reitz C, Tang MX, Manly J, Mayeux R, Luchsinger JA (2007)Hypertension and the risk of mild cognitive impairment. ArchNeurol64:1734-1740.
213 BirnsJ,KalraL(2009)Cognitivefunctionandhypertension.JHumHypertens23:86-96.
214 WoodsB,AguirreE,SpectorAE,OrrellM(2012)Cognitivestimulationtoimprovecognitivefunctioninginpeoplewithdementia.CochraneDatabaseSystRev2:CD005562.
215 Ngandu T, Lehtisalo J, Solomon A, Levälahti E, Ahtiluoto S, et al.(2015)A2yearmultidomaininterventionofdiet,exercise,cognitivetraining, and vascular risk monitoring versus control to preventcognitivedecline inat-riskelderlypeople (FINGER):a randomisedcontrolledtrial.Lancet385:2255-2263.

2017Vol.8 No.5:224
25 This article is available in: www.jneuro.com
ARCHIVOS DE MEDICINAISSN 1698-9465
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
216 Smith EE, Cieslak A, Barber P, Chen J, Chen YW, et al. (2017)TherapeuticStrategiesandDrugDevelopmentforVascularCognitiveImpairment.JAmHeartAssoc6:e005568.
217 RománGC,WilkinsonDG,DoodyRS,Black SE, Salloway SP, et al.(2005)Donepezil in vasculardementia: combinedanalysisof twolarge-scaleclinicaltrials.DementGeriatrCognDisord20:338-344.
218 Román GC (2014) Vascular Cognitive Disorders. In, Gabbard’sTreatmentsofPsychiatricDisorders.DSM-5Edition.pp:977-985.
219 Ballard C, Sauter M, Scheltens P, He Y, Barkhof F, et al. (2008)Efficacy,safetyandtolerabilityofrivastigminecapsulesinpatientswithprobablevasculardementia:theVantagEstudy.CurrMedResOpin24:2561-2574.
220NarasimhaluK,EffendyS,SimCH,Lee JM,Chen I,etal. (2010)Arandomizedcontrolledtrialofrivastigmineinpatientswithcognitiveimpairmentnodementiabecauseofcerebrovasculardisease.ActaNeurolScand121:217-224.
221 Erkinjuntti T, Kurz A, Gauthier S, Bullock R, Lilienfeld S, et al.(2002)Efficacyofgalantamine inprobablevasculardementiaandAlzheimer's disease combined with cerebrovascular disease: Arandomisedtrial.Lancet359:1283-1290.
222 AuchusAP,BrashearHR,SallowayS,KorczynAD,DeDeynPP,etal.(2007)GAL-INT-26StudyGroup.Galantaminetreatmentofvasculardementia:Arandomizedtrial.Neurology69:448-458.
223 RománG,PascualB(2012)DemenciaVascularyDeterioroCognitivode Origen Vascular. Revista Neuropsicología, Neuropsiquiatría yNeurociencias12:203-213.
224 Orgogozo JM, Rigaud AS, Stoffler A,Mobius HJ, Forette F (2002)Efficacyandsafetyofmemantineinpatientswithmildtomoderatevasculardementia:a randomized,placebo-controlled trial (MMM300).Stroke33:1834-1839.
225 WilcockG,MobiusHJ,StofflerA,MMM500group(2002)Adouble-blind,placebo-controlledmulticentrestudyofmemantineinmildtomoderatevasculardementia(MMM500).IntClinPsychopharmacol17:297-305.
226 López-Arrieta JM, Birks J (2002) Nimodipine for primarydegenerative, mixed and vascular dementia. Cochrane DatabaseSystRev3:CD000147.
227 PantoniL,DelSerT,SoglianAG,AmigoniS,SpadariG,etal.(2005)Efficacyandsafetyofnimodipineinsubcorticalvasculardementia:arandomizedplacebo-controlledtrial.Stroke36:619-624.
228 Fioravanti M, Yanagi M (2005) Cytidinediphosphocholine (CDP-choline)forcognitiveandbehaviouraldisturbancesassociatedwithchroniccerebraldisorders in theelderly.CochraneDatabaseSystRev2:CD000269.
229 Alvarez-SabínJ,OrtegaG,JacasC,SantamarinaE,MaisterraO,etal.(2013)Long-termtreatmentwithciticolinemayimprovepoststrokevascularcognitiveimpairment.CerebrovascDis35:146-154.
230Mimenza-AlvaradoA,Aguilar-NavarroS,Ávila-FunesJA(2013)GuíaPráctica de Demencias para diagnóstico y tratamiento. México:CorporativoIntermédica(EditorialCorinter)pp.61-92.
231 Cotroneo AM, Castagna A, Putignano S, Lacava R, Fantò F, etal. (2013) Effectiveness and safety of citicoline in mild vascularcognitiveimpairment:theIDEALEstudy.ClinIntervAging8:131-137.
232 Alvarez-SabínJ,SantamarinaE,MaisterraO,JacasC,MolinaC,etal. (2016) Long-term treatmentwith citicoline prevents cognitivedecline and predicts a better quality of life after a first ischemicstroke.J.etal.IntJMolSci17:390.
233 HerrschaftH,NacuA,LikhachevS,SholomovI,HoerrR,etal.(2012)GinkgobilobaextractEGb761®indementiawithneuropsychiatricfeatures: A randomised, placebo-controlled trial to confirm theefficacyand safetyofadailydoseof240mg. JPsychiatrRes46:716-723.
234 Guekht AB,Moessler H, Novak PH, Gusev IE (2011) Cerebrolysinin vascular dementia: improvement of clinical outcome in arandomized, double-blind, placebo-controlled multicenter trial. JStrokeCerebrovascDis20:310-318.
235 Pearce LA,McClure LA,AndersonDC, JacovaC, SharmaM,et al.(2014) Effects of long-term blood pressure lowering and dualantiplatelettreatmentoncognitivefunctioninpatientswithrecentlacunar stroke: A secondary analysis from the SPS3 randomisedtrial.LancetNeurol13:1177-1185.
236 ChenN,YangM,GuoJ,ZhouM,ZhuC,etal.(2013)Cerebrolysinforvasculardementia.CochraneDatabaseSystRev1:CD008900.
237 Flicker L, Evans G (2001) Piracetam for dementia or cognitiveimpairment.CochraneDatabaseSystRev2:CD001011.
238 Frampton M, Harvey RJ, Kirchner V (2003) Propentofylline fordementia.CochraneDatabaseSystRev2:CD002853.

![Vascular parkinsonism · Vascular parkinsonism – REVIEW future science groupfuture science group 239 20%) suffered from parkinsonism with strong evidence of CVD [23]](https://img.pdfslide.us/doc/110x75/5c12e69c09d3f208438bb500/vascular-parkinsonism-vascular-parkinsonism-review-future-science-groupfuture.jpg)



























