Embed Size (px)
Citation preview

Epilepsy Research (2011) 93, 221—225
journa l homepage: www.e lsev ier .com/ locate /ep i lepsyres
SHORT COMMUNICATION
Laterality and temporal distribution of seizures inpatients with bitemporal independent seizuresduring a trial of responsive neurostimulation
David Spencera,∗, Ryder Gwinnb, Martin Salinskya,1, Jean P. O’Malleyc,2
a Oregon Health & Science University, 3181 SW Sam Jackson Park Rd. CR120, Portland, OR 97239, United Statesb Swedish Neuroscience Institute, 550 17th Ave., Suite 500, Seattle, WA 98122, United Statesc Oregon Clinical and Translational Research Institute, 3181 SW Sam Jackson Park Rd. CR145, United States
Received 8 November 2010; received in revised form 14 December 2010; accepted 21 December 2010Available online 21 January 2011
KEYWORDS Summary We describe seizure laterality and temporal seizure patterns in six subjects with
Epilepsy;Temporal lobeepilepsy;Neurostimulation;Bitemporal epilepsy
bilateral temporal lobe epilepsy (bTLE) implanted with bilateral hippocampal depth electrodesand the NeuroPace RNSTM system over 84 consecutive days. Seizures were disproportionate inlaterality in three subjects and disproportionate in time for two subjects. Clustering of seizuresdid not clearly affect laterality. Some but not all subjects with bTLE displayed nonrandomtemporal or lateral clustering of seizures.
(ta
Published by Elsevier B.V.
Introduction
Epilepsy is a common neurological condition, with a lifetime
prevalence of 0.5—1%. Approximately 2/3 of patients withepilepsy will achieve seizure control with antiepileptic med-ications; 1/3 are possible candidates for epilepsy surgery.Patients with unilateral mesial temporal lobe epilepsy∗ Corresponding author.Tel.: +1 503 494 5682; fax: +1 503 494 6658.
E-mail addresses: [email protected] (D. Spencer),[email protected] (R. Gwinn),[email protected] (M. Salinsky),[email protected] (J.P. O’Malley).
1 Fax: +1 503 494 6658.2 Fax: +1 503 418 0125.
op(g
mmbutdoT2
0920-1211/$ — see front matter. Published by Elsevier B.V.doi:10.1016/j.eplepsyres.2010.12.010
mTLE) are among the best surgical candidates, howeverhere is substantial evidence from pathological, imaging,nd electroencephalographic (EEG) studies that mTLE isften a bilateral disease, and 14—23% of patients show inde-endent seizure onsets from both mesial temporal regionsSo et al., 1989; Hirsch et al., 1991). These patients areenerally not suitable surgical candidates.
Independent bitemporal seizure onset is largely deter-ined by EEG monitoring. Because the duration of EEGonitoring is limited, these studies are prone to samplingias. The number of seizure recordings needed to assurenilateral seizure onset is debated, and depends both on
he proportion of seizures from each temporal lobe and ten-ency to cluster seizures from one temporal lobe as a resultf short interseizure interval or other factors (Blum, 1994;odorov et al., 1994; Haut et al., 1997, 2002; Choi et al.,006).
222 D. Spencer et al.
Table 1 Characteristics of subjects.
Subject Gender Age Age ofseizureonset
Etiology MRI History ofintracranialmonitoring priorto RNS?
Previousepilepsysurgery?
PreviousVNS?
1 F 25 2 Febrile seizures Bilateral MTS No No No2 F 42 15 Febrile seizures Bilateral MTS Yes No No3 F 34 23 Meningo-encephalitis None No No No4 M 50 21 Unknown Left MTS No No Yes5 F 26 9 Meningo-encephalitis None Yes No Yes6 M 34 8 Post-traumatic Bilateral MTS and
bilateralencephalomalacia
Yes No Yes
bepridces
ce
M
S
TjiNoedi
S
Bsta(japp
jltttp
1tnpd
E
Stmsibbuwsoe
D
Aprrsttewot
D
Wssoe
MTS = MRI findings characteristic of mesial temporal sclerosis.
We studied six subjects with known independentitemporal seizure foci and chronically implanted depthlectrodes as part of the NeuroPace RNSTM system trial. Ourrimary objective was to describe the probabilistic tempo-al and laterality patterns of seizure onset in patients withndependent bitemporal seizure onsets using this uniqueata set of long-term ambulatory intracranial electroen-ephalography. A secondary objective was to explore theffect of interseizure interval (ISI) on the laterality of nexteizure.
The results have direct implications for the presurgi-al evaluation of patients with refractory temporal lobepilepsy.
ethods
tudy design
his was a retrospective study of a consecutive series of sub-ects with independent, bitemporal onset seizures and chronicallymplanted hippocampal depth electrodes who were enrolled in theeuroPace RNSTM System trial at Oregon Health & Science Universityr Swedish Medical Center. The RNSTM neurostimulator and depthlectrodes were implanted at least 20 weeks prior to the 84-dayata evaluation period of this study to eliminate any influence ofmmediate postoperative changes.
ubjects
ilateral independent temporal lobe seizures were confirmed in allubjects by standard presurgical evaluation prior to RNSTM implan-ation. Three subjects had long term scalp EEG recordings onlynd three subjects had both scalp and intracranial EEG monitoringTable 1). Subject characteristics are summarized in Table 1. All sub-ects had four contact depth electrodes stereotactically implantedlong the longitudinal axis of each hippocampus. Depth electrodelacement was confirmed by co-registration of pre-implant MRI andost-implant CT imaging.
Enrollment criteria for the RNSTM study required that sub-ects were 18—70 years of age and had medically refractory
ocalization-related epilepsy (disabling simple partial, complex par-ial or secondarily generalized seizures) defined as lack of responseo two or more antiepileptic medications. They had on averagehree or more disabling seizures per month for the three monthsrior to study entry and were on stable antiepileptic medication forwbS
e
2 weeks prior to enrollment. Subjects were excluded from par-icipation if they had primary generalized epilepsy, psychogeniconepileptic events or substantial psychiatric disease in the yearrior to enrollment, a clinically significant or unstable medical con-ition or progressive central nervous system disease.
CoG data
ubjects used a data transmitter daily to upload four, 90 s ECoGso a secure central data repository: the Patient Data Manage-ent System (PDMS). ECoGs were automatically stored for each
eizure containing low-voltage fast activity or rhythmic sharp activ-ty that continued for at least 30 s and was distinct from the ECoGackground activity, based on pre-defined parameters that hadeen optimized over the preceding 20 weeks and that remainednchanged throughout the 84-day data evaluation period. Seizuresere detected and ECoGs stored regardless of clinical symptoms. A
pecific clinical seizure could be marked and stored by the subjectr caregiver by swiping a magnet over the device at the time of thevent.
efinition and identification of seizures
ll ECoG data stored by the RNS over the 84-day data evaluationeriod were reviewed by two board certified electroencephalog-aphers (DS and MS). Determination of whether an ECoG patternepresented a seizure and laterality of each seizure was by consen-us. Most of the recorded seizures were similar in morphology tohose observed during patient-reported seizures. Conservative cri-eria were applied so that repetitive focal spiking and short durationvents (<10 s) were not recorded as seizures. Each identified seizureas described by date and time of onset, and laterality of seizurenset. Interseizure interval (ISI) was determined by calculating theime interval between seizure recordings on PDMS.
ata analysis
e assessed the probability that observed seizures were randomamples from subjects with equal likelihood of seizures from eitheride using a binomial test. To assess whether the laterality sequencef seizures was random, we used the nonparametric run test onach subject’s series of seizures. Temporal distribution of seizures
as assessed by testing the fit of the distribution of time intervalsetween seizures to an exponential distribution with a Kolomogorovmirnov test (Ogburn and Brown, 2003).The relationship between interseizure interval (ISI) and lat-rality of seizure pairs was descriptive in nature due to the

Laterality and temporal distribution of seizures 223
iod.
R
Overall seizure laterality
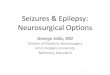
Figure 1 Distribution of seizures in subjects of the study perEach diamond represents a recorded seizure event.
small number of subjects available for analysis. We groupedinterseizure intervals between seizure pairs into quartiles andexamined the relationship between ISI and mean percentconcordance.
Laterality analysis was done using SPSS 16.0. Distribution test-ing was done using SAS 9.2. Adjusted P values reflect a Bonferronicorrection for multiple comparisons.
Tn
X-axis = time (date). Y-axis represents laterality (left or right).
esults
he binomial test showed that overall seizure laterality wason-random in three of six subjects (Fig. 1). Subject 2 had a

224
Fl
gsaa
T
T(4s
L
Ossd
T
AdiIetn
D
Wnnas
sl(t
tredid
stpeacwan2n
ntstwspbbisdws
wnavsirsTuwb
sli
A
Ti
R
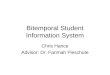
igure 2 Effect of interseizure interval quartile on seizureaterality.
reater proportion of seizures on the right (P < 0.0001 adj),ubject 3 a greater proportion on the left (P < 0.001 adj),nd subject 6 had exclusively right sided seizures (P < 0.003dj).
emporal distribution (clustering) of seizures
emporal clustering was evident in two of six subjectsFig. 1). Subject 2 (P < 0.007, P < 0.042 adj) and subject
(P < 0.001, P < 0.006 adj) showed periods of more activeeizures followed by more quiescent intervals.
aterality sequence
ne subject had a non-random laterality sequence (Fig. 1,ubject 5 P < 0.048), and one subject had seizure arise exclu-ively from one temporal lobe (Fig. 1, subject 6 P notefined).
emporal clustering and laterality
lthough there appeared to be a qualitative trend towardsecreased seizure concordance with increasing interseizurenterval across the first three quartiles (Fig. 2), the longestSI quartile had relatively high concordance, suggesting thatither seizure concordance is not dependent on ISI or thathe relationship is too complex to be modeled with a limitedumber of subjects.
iscussion
e found that some, but not all subjects with bTLE showedonrandom temporal or lateral clustering of seizures. We didot have adequate statistical power to establish or excluden association between ISI or ‘‘temporal clustering’’ andeizure laterality.
Previous work by Van Ness et al. estimated that 17 serialeizures would need to be recorded to confidently estab-ish that fewer than 20% of seizures arise from a second siteVan Ness et al., 1990). Subsequently, Blum et al. used Bayesheorem and selected data from an epilepsy monitoring unit
B
D. Spencer et al.
o constrain the statistical possibilities and estimate thatecording five serial seizures from a single focus confidentlystablishes that site as the sole focus (Blum, 1994). Ourata, with the advantage of long-term intracranial record-ngs in ambulatory patients, showed that five of six subjectsemonstrated bilateral onsets within the first five seizures.
The conclusions of Blum rest on the assumption thateizure clusters do not influence seizure laterality. In fact,here is substantial evidence that seizures may cluster tem-orally (Todorov et al., 1994; Haut et al., 1997, 2002; Choit al., 2006), and that short ISI may influence seizure later-lity (Haut et al., 1997). Haut suggested that recording fiveonsecutive seizures often did not reliably identify patientsith bilateral independent seizure onsets. Choi confirmedn effect of interseizure interval on laterality that was sig-ificant in extratemporal, not TLE patients (Choi et al.,006). Our results support that some mTLE subjects showon-random lateralized sequences of seizures over time.
Despite the advantages of chronic, ambulatory intracra-ial recordings and lack of influence from medication taper,he current study has limitations. Most importantly, thetored ECoGs represent detected events rather than a con-inuous record of all seizures. Although seizure detectionas optimized over 20 weeks, it is possible that some
eizures went undetected or that seizures from one tem-oral lobe were preferentially detected. Storage may haveeen biased towards the collection of non-clustered seizuresecause seizure clusters may saturate the storage capac-ty of the device. Additionally, we studied electrographiceizures. While generally morphologically similar to theefined clinical seizures, the results might have differed hade been able to obtain reliable time course data on clinical
eizures.The study took place during active RNSTM stimulation,
hich could have influenced the results. We studied a smallumber of subjects which limited our ability to statisticallynalyze relationships between seizures, interseizure inter-al, and laterality, and these subjects represent a highlyelected group who qualified for and chose to participaten the RNSTM trial; this limits the external validity of theesults. It is possible that this selected group exhibits morepatial or temporal clustering than other patients with bTLE.hese limitations notwithstanding, the present report offersnique insight into the variable seizure patterns in patientsith bTLE. These patterns are not consistent, and appear toe a unique characteristic of each patient’s epilepsy.
Future studies with more subjects will provide greatertatistical power to illuminate the natural history of seizureaterality in bTLE and the relationship between interseizurenterval and seizure laterality.
cknowledgement
he authors would like to thank Emily Mirro, MS for her helpn data preparation.
eferences
lum, D., 1994. Prevalence of bilateral partial seizure foci andimplications for electroencephalographic telemetry monitoringand epilepsy surgery. Electroencephalogr. Clin. Neurophysiol. 91(5), 329—336.

O
S
T
Laterality and temporal distribution of seizures
Choi, E.J., Kang, J.K., et al., 2006. Effect of interseizure intervalon seizure lateralization in patients with bilateral seizure foci.Seizure 15 (8), 576—581.
Haut, S.R., Legatt, A.D., et al., 1997. Seizure lateralization duringEEG monitoring in patients with bilateral foci: the cluster effect.Epilepsia 38 (8), 937—940.
Haut, S.R., Swick, C., et al., 2002. Seizure clustering during epilepsymonitoring. Epilepsia 43 (7), 711—715.
Hirsch, L.J., Spencer, S.S., et al., 1991. Comparison of bitemporaland unitemporal epilepsy defined by depth electroencephalog-raphy. Ann. Neurol. 30 (3), 340—346.
V
225
gburn, J., Collins, S., Brown, M., 2003. Randomness at the Root ofThings. Phys. Educ. 38 (5), 398.
o, N., Gloor, P., et al., 1989. Depth electrode investigations inpatients with bitemporal epileptiform abnormalities. Ann. Neu-rol. 25 (5), 423—431.
odorov, A.B., Lesser, R.P., et al., 1994. Distribution in time of
seizures during presurgical EEG monitoring. Neurology 44 (6),1060—1064.an Ness, P.C., So, N.K., et al., 1990. Ictal and interictal EEG: whatconstitutes an adequate sample for epilepsy surgery? Epilepsia31 (5), 623.