Embed Size (px)
Citation preview

Journal of Cardiac Failure Vol. 20 No. 4 2014
Latent Obstruction and Left Atrial Size Are Predictorsof Clinical Deterioration Leading to Septal Reduction
in Hypertrophic Cardiomyopathy
GHERARDO FINOCCHIARO, MD,1 FRANCOIS HADDAD, MD,1,4 ALEKSANDRA PAVLOVIC,1 GIANFRANCO SINAGRA, MD,2
INGELA SCHNITTGER, MD,1 JOSHUA W. KNOWLES, MD, PhD,1,4 MARCO PEREZ, MD,1,4 EMMA MAGAVERN,1
JONATHAN MYERS, PhD,3 AND EUAN ASHLEY, MRCP, DPhil1,4
Trieste, Italy; and Palo Alto, California
From the 1Divicine, Stanford Unidiovascular DepaTrieste, Italy; 3VeCalifornia and 4S
Manuscript recDecember 11, 201
Reprint requesvascular Medicineþ4407506900809
Funding: Biotrolar Disease.
See page 242 f1071-9164/$ - s� 2014 Elseviehttp://dx.doi.org
ABSTRACT
Background: Exercise echocardiography is a reliable tool to assess left ventricular (LV) dynamicobstruction in hypertrophic cardiomyopathy (HCM). The aim of this study was to determine the role ofexercise echocardiography in the evaluation of latent obstruction and in predicting clinical deteriorationin HCM patients.Methods and Results: We considered 283 HCM patients studied with exercise echocardiography. Theend point was clinical deterioration leading to septal reduction (myectomy or alcohol septal ablation).LV latent obstruction was present at enrollment in 67 patients (24%). During a mean follow-up of42 6 31 months, 42 patients had clinical deterioration leading to septal reduction therapy: in 12/67(22%) patients with a latent obstruction at enrollment, in 28/84 (33%) patients with obstruction at rest,and in 2/132 (1.5%) with obstruction neither at rest or during stress. Multivariate analysis identified thefollowing variables as independently associated with the end point: LV gradient O30 mm Hg at rest (haz-ard ratio [HR] 2.56, 95% CI 1.27e5.14; P5 .009), LV gradientO30 mm Hg during stress (HR 4.96, 95%CI 1.81e13.61; P 5 .002), and indexed left atrial volume (LAVi ) O40 mL/m2 (HR 2.86, 95% CI1.47e5.55; P5 .002). In patients with a latent obstruction, the strongest independent predictor of outcomewas LAVi O40 mL/m2 (HR 3.75, 95% CI 1.12e12.51; P 5 .032).Conclusions: Assessment of LV gradient during stress with exercise echocardiography is an importanttool for the evaluation of latent obstruction in HCM and may have a role in risk stratification of these pa-tients. (J Cardiac Fail 2014;20:236e243)Key Words: Hypertrophic cardiomyopathy, exercise echocardiography, left ventricular obstruction.
Intracavitary left ventricular (LV) obstruction, typicallyacross the left ventricular outflow tract (LVOT), is animportant pathophysiologic feature of hypertrophic
sion of Cardiovascular Medicine, Department of Medi-versity School of Medicine, Palo Alto, California; 2Car-rtment, Ospedali Riuniti and University of Trieste,terans Affairs Palo Alto Health Care System, Palo Alto,tanford Cardiovascular Institute, Palo Alto, California.eived August 3, 2013; revised manuscript received3; revised manuscript accepted January 23, 2014.ts: Gherardo Finocchiaro, MD, Division of Cardio-, Stanford University, 34100 Palo Alto, California. Tel:. E-mail: [email protected] Italia and Stanford Center for Inherited Cardiovascu-
or disclosure information.ee front matterr Inc. All rights reserved./10.1016/j.cardfail.2014.01.014
236
cardiomyopathy (HCM).1 Twenty-five percent to 30% ofpatients with HCM have a significant LVOT gradient atrest.2 In patients with HCM, LVOT obstruction at rest isconsidered to be a strong independent predictor of progres-sion to severe symptoms of heart failure and death.3
The presence of a significant intraventricular gradientidentifies a subgroup of patients in whom septal reductioninterventions, such as surgical myectomy or alcohol septalablation, are considered as therapeutic options.4,5 It is nowrecognized that a sizable proportion of patients with mini-mal or absent LVOT gradients at rest develop significantgradients after exercise or provocative maneuvers. Thesepatients may be minimally symptomatic or asymptomatic.6
However, the burden of latent obstruction is variable in thedifferent series analyzed, and its prognostic role is not clear.
The first aim of the present study was to describe theprevalence and features of patients with latent obstruction

Exercise Echocardiography in Hypertrophic Cardiomyopathy � Finocchiaro et al 237
in a large population of patients with HCM studied with ex-ercise echocardiography. The second aim was to assesswhether latent obstruction is associated with a higher likeli-hood of worsening symptoms and exercise intolerance lead-ing to septal reduction therapy.
Methods
Study Population
From the population of patients with HCM enrolled in the Stan-ford registry for inherited cardiovascular disease, 283 patients(mean age 50 6 16 years, male sex 60%) referred for evaluationat Stanford University from January 2000 to January 2012 under-went exercise echocardiography at enrollment. For the presentanalysis we excluded 16 patients with ‘‘pure’’ apical HCMwithout significant intraventricular gradient at rest or stress.The diagnosis of HCM was based on the presence of significant
LV hypertrophy (end-diastolic wall thickness O15 mm with M-mode or 2-dimensional [2D] echocardiography) in the absenceof other etiologies according to international criteria, or wallthickness of 13e15 mm in the presence of an abnormal electrocar-diogram or familial history of inherited cardiomyopathies.7 Pa-tients with left ventricular (LV) systolic dysfunction atenrollment were included in the study if there was a clear docu-mented history of HCM and preserved LV ejection fraction(LVEF) from earlier echocardiographic examinations performedat other institutions.All subjects were stable and receiving optimal medical therapy
at the time of testing. Written informed consents were obtainedwith the use of a protocol approved by the Stanford UniversityInstitutional Review Board. The investigation conformed withthe principles outlined in the Declaration of Helsinki8 and locallegal requirements and was approved by the Institutional ReviewBoard at Stanford University.
Echocardiographic and Doppler Study
Echocardiographic images were acquired with the use of PhilipsIE 33 or HP 5500 systems depending on the period of enrollment(Andover, Massachusetts). We considered only the examinationperformed at enrollment. HCM was classified according to ven-tricular morphology as: 1) hypertrophy with reverse septal curva-ture; 2) hypertrophy with proximal septal bulge; 3) concentrichypertrophy with normal shape (symmetric); or 4) indefinite ifthe morphology did not fit any of the other subgroups.9 UsingM-mode and 2D, we measured LV diameters and shortening frac-tion, thickness of the interventricular septum (IVS) and LVposterior wall (PW), and left atrial end-systolic diameter; all mea-surements were performed according to recommendations of theAmerican Society of Echocardiography (ASE).10,11 With the useof 2D, the sites and maximal extent of ventricular hypertrophywere assessed and measured in end-diastole. LV volumes andEF were assessed from the apical 4-chamber view, with the useof the biplane method of discs. LVEF was considered to bedepressed when it was !50%.At Doppler examination, the systolic intraventricular gradient
was quantified with the use of the continuous-Doppler technique.A peak gradient of O30 mm Hg at rest was considered to be sig-nificant. LV filling was assessed by pulsed Doppler interrogationat the level of mitral opening tips. In accordance with earlierstudies and with ASE guidelines,12,13 the pattern of LV fillingwas classified as: 1) restrictive filling pattern: E-deceleration
time !120 ms or an E/A $2 associated with E-decelerationtime !160 ms; 2) abnormal relaxation: E/A !1 associated withE-deceleration timeO220 ms; or 3) normal (or ‘‘pseudonormal’’):intermediate filling pattern. Mitral and tricuspid valve regurgita-tion were assessed according to the ASE guidelines.14
Left ventricular myocardial performance index (MPI) wasmeasured from mitral inflow and LV outflow Doppler tracings,as previously described by Tei et al.15 From tissue Doppler imag-ing we considered peak myocardial early diastolic velocitymeasured at the lateral mitral annulus and the assessment of trans-mitral to TDI early-diastolic velocity ratio (E/e0).16 Tricuspidannular plane systolic excursion (TAPSE) was measured fromthe systolic excursion of the tricuspid lateral annulus. In accor-dance with ASE guidelines, right ventricular systolic dysfunctionwas considered to be present when fractional area contraction(apical 4-chamber view) was !35% and/or TAPSE was !16mm.17 We defined the development of new wall motion abnormal-ities as the presence of alterations in segmental kinesis notobserved during resting echocardiography and worsening of mitralregurgitation (MR) from mild to moderate/severe or from moder-ate to severe MR, according to ASE guidelines.18
Patients were stressed with the use of the ramp Bruce protocol.The Borg scale19 and the peak respiratory exchange ratio (RER)were used as measures of adequate stress. After the treadmill ex-ercise test, patients were immediately placed in the left lateral de-cubitus position. Imaging was performed by an experiencedtechnician. The peak gradient was measured first, and degrees ofMR were then assessed.Patients were classified according to the presence of a signifi-
cant gradient at rest and/or during stress in the following 3 groups:group 1: patients nonobstructive either at rest or stress; group 2:patients obstructive only at stress (latent obstruction); and group3: patients obstructive at rest.
Follow-Up Assessment
Patients were periodically followed with clinical/laboratoryassessment. The frequency of evaluations was established ac-cording to the clinical needs of a given patient. The end pointof the study was clinical deterioration leading to septal reductiontherapy (surgical myectomy or alcohol septal ablation). Clinicaldeterioration was defined as an evolution from a conditionconsidered to be manageable with medications to severe symp-toms (New York Heart Association [NYHA] functional classIIIeIV) despite optimal medical therapy (OMT). Septal reduc-tion therapy during follow-up was considered only when signif-icant symptoms (NYHA functional class IIIeIV) despite OMT,associated with a significant resting LVOT gradient, occurred.The patients that at enrollment were symptomatic (NYHA func-tional class III) showing a significant obstruction at rest and/or atstress were initially medically treated with closer follow-up. In-formation regarding study end points was obtained directly fromthe clinical follow-up evaluations or by telephone interview withthe patient, their relatives, or general practitioner or obtained bythe residence birth/death registries. For patients without events,the end of follow-up was considered to be June 1, 2012. Duringfollow-up, 3/67 (4%) in group 2, 5/84 (6%) in group 3 and 7/132(5%) in group 1 died or underwent heart transplantation (P 5NS). We did not consider this end point for the present study,focusing our attention on clinical deterioration leading to septalreduction.

238 Journal of Cardiac Failure Vol. 20 No. 4 April 2014
Statistical Analysis
Results are expressed as mean6 SD for continuous variables oras number of cases and percentage for categoric variables. Com-parisons between groups were made with the use of the analysisof variance test on continuous variablesdusing the Brown-Forsythe statistic when the assumption of equal variances didnot holddand the chi-square test for discrete variables, usingYates correction when necessary. Cox proportional hazards anal-ysis was used to determine factors independently associatedwith a higher likelihood of clinical deterioration leading to septalreduction (we included in the multivariate analysis only the vari-ables most strongly associated with outcomes on univariate anal-ysis). Cox proportional hazard models in the subgroup with latentobstruction were adjusted for age and sex (we included in themultivariate analysis only the variables most strongly associatedwith outcomes on univariate analysis). To determine intra- and in-terreader variability, the studies were blindly read by the sameinvestigator as well as by a separate investigator. A random sampleof 25 studies was chosen to calculate the intra- and interreadervariability. Intra- and interreader variability was quantified withthe use of mean differences and intraclass correlation coefficients,
Table 1. Baseline Characteristics of
Total Population(n5283)
NonobstrGroup 1 (
Demographic and clinicalAge 50 6 16 49 6Male, n (%) 171 (60) 77 (5BSA, m2 2.0 6 0.2 2.0 6NYHA III, n (%) 24 (8) 5 (4AFib, n (%) 12 (4) 9 (7Borg scale 17.2 6 1.2 17.4 6RER 1.13 6 0.12 1.15 6
MorphologySeptal converse, n (%) 22 (8) 10 (8Septal reverse, n (%) 164 (58) 66 (5Symmetric, n (%) 52(18) 32 (2Indefinite, n (%) 46 (16) 25 (1
EchocardiographyIVS, mm 18 6 5 16 6Indexed IVS, mm/m2 9 6 3 8 6PW, mm 12 6 3 11 6LVEF (%) 68 6 9 65 6LVEF!50%, n (%) 13 (5) 10 (8E/A!1, n (%) 95 (33) 39 (2Restrictive pattern, n (%) 15 (5) 10 (8LVMPI 0.58 6 0.18 0.59 6LAVi O40 ml/m2, n (%) 114 (40) 41 (3SAM n (%) 141 (50) 33 (2Moderate-severe MR, n (%) 15 (5) 2 (2E/e0 12 6 8 10 6E0 8 6 3 9 6RVSP on 175 pts, mmHg 31 6 9 30 6Development of WMA, n (%) 10 (4) 4 (3Worsening MR during exercise, n (%) 10 (4) 3 (2
TherapyBeta-blockers 148 (52) 63 (4Calcium channel Blocker, n (%) 64 (23) 26 (2Ace Inhibitors, n (%) 44 (16) 28 (2Diuretics, n (%) 28 (10) 17 (1
LV, left ventricle; BSA, body surface area; EDD, end-diastolic diameter; IVSejection fraction; LA, left atrium; LAVi, indexed left atrium volume; MPI, myoRVSP, right ventricle systolic pressure.
*P ! .05 between group 3 and group 1.yP ! .05 between group 2 and group 1.zP ! .05 between group 2 and group 3.
and no significant difference (P 5 .89) between the 2 readers wasobserved. Statistical analysis was performed with the use ofPASW software (v18.0; Chicago, Illinois).
Results
Patient Characteristics
Clinical and demographic characteristics for the studypopulation at baseline are summarized in Table 1. Meanage was 50 6 16 years; 171 patients (60%) were male.Twenty-nine patients (10%) were in NYHA functional classIII. Maximal LV wall thickness was 18 6 5 mm (9 6 3mm/m2). Seventeen patients (6%) had an earlier septalreduction (5 with septal alcohol ablation and 12 with septalmyectomy). The average Borg scale was 17.2 6 1.2, andthe average peak exercise RER was 1.13 6 0.12. In 2 pa-tients the Borg scale was !15 and in 5 the peak exerciseRER was !0.9.
283 Study Patients With HCM
uctive:n5132)
Latent Obstructive:Group 2 (n567)
Obstructive at Rest:Group 3 (n584) P
16 50 6 18 52 6 15 .398) 54 (81)y 40 (48)z !.0010.2 2.0 6 0.2z 1.9 6 0.3* .02) 2 (3)z 17 (20)* !.001) 2 (3) 1 (1) .121.3 17.1 6 1.2 17.2 6 1.2 .690.14 1.12 6 0.12 1.13 6 0.11 .09
) 6 (9) 6 (7) .910) 41 (61) 57 (68)* .034) 10 (15) 10 (12)* .059) 10 (15) 11 (13) .49
5 18 6 4* 19 6 6y !.0012 9 6 2 10 6 3* !.0013 12 6 2* 13 6 3 !.00110 70 6 9 71 6 7* ! .001) 2 (3) 1 (1) .079) 24 (36) 32 (38) .61) 4 (6) 1 (1) .120.18 0.61 6 0.17z 0.53 6 0.19* !.0011) 26 (39) 47 (56)* .0015) 38 (57)* 70 (83)z !.001) 3 (4) 10 (12)* .0046 10 6 5z 16 6 9* !.0014 9 6 3z 7 6 3* !.0018 31 6 7 34 6 10 .06) 2 (3) 4 (5) .77) 1 (1) 6 (7) .10
8) 32 (48) 53 (63) .060) 15 (22) 23 (27) .421) 9 (13) 7 (8)* .033) 2 (3) 9 (11) .08
, interventricular septum; PW, posterior wall; AFib, atrial fibrillation; EF,cardial performance index; MR, mitral regurgitation; RV, right ventricle;

Table 2. Baseline Characteristics of the Total PopulationAccording to Outcomes
PrimaryOutcome(n 5 42)
NoPrimaryOutcome(n 5 241)
PValue
Demographic and clinicalAge 52 6 13 50 6 17 .34Male, n (%) 21 (50) 150 (62) .13AFib, n (%) 1 (2) 11 (5) .49
MorphologySeptal converse, n (%) 3 (7) 19 (8) .87Septal reverse, n (%) 25 (60) 139 (58) .82Symmetric, n (%) 6 (14) 46 (19) .46Indefinite, n (%) 8 (19) 38 (16) .59
EchocardiographyIVS, mm 19 6 5 17 6 5 .006Indexed IVS, mm/m2 10 6 3 9 6 3 .01PW, mm 13 6 3 12 6 3 .03RWT 0.82 6 0.21 0.67 6 0.25 !.001LVEF, % 70 6 8 68 6 10 .14LVEF !50%, n (%) 1 (2) 12 (5) .46Restrictive pattern, n (%) 3 (7) 12 (5) .61LAVi O40 mL/m2, n (%) 29 (69) 85 (35) !.001Moderate-severe MR, n (%) 4 (10) 11 (5) .19LV gradient O30 mm Hg atrest, n (%)
28 (67) 56 (23) !.001
Exercise Echocardiography in Hypertrophic Cardiomyopathy � Finocchiaro et al 239
Prevalence of LV Obstruction and Differences Betweenthe Subgroups
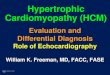
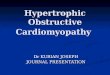
At baseline, out of the 283 HCM patients considered, 67(24%) had a latent obstruction, 84 (30%) an obstruction atrest, and 132 (47%) no obstruction at rest or during stress(Fig. 1). Echocardiographic quantification of LV gradientwas evaluated by 2 physicians for all of the patients.Patients with obstruction at rest showed greater IVS and
PW thicknesses than other groups (16 6 5/11 6 3 in group1 vs 18 6 4/12 6 2 mm in group 2 vs 19 6 6/13 6 3 ingroup 3; P ! .001/P ! .001) and greater LA size (LAViO40 mL/m2 present in 31%, 39%, and 56% in groups 1,2, and 3, respectively; P ! .001). In addition, patientsbelonging to group 3 were more symptomatic (NYHAfunctional class III was present in 4%, 10%, and 20% of pa-tients in groups 1, 2, and 3, respectively; P ! .001). Pa-tients with latent obstruction were more frequently male(prevalence of male sex was 58%, 81%, and 48% in groups1, 2, and 3, respectively; P ! .001) and were characterizedby a higher LV myocardial performance index (0.59 6 0.18in group 1 vs 0.61 6 0.17 in group 2 vs 0.53 6 0.19 ingroup 3; P ! .001).
LV gradient O30 mm Hg atstress, n (%)
37 (88) 106 (44) !.001
RV dysfunction, n (%) 1 (2) 14 (6) .36E/e0 15 6 8 11 6 7 .01E0 7 6 2 9 6 3 .001
Therapy, n (%)Beta-blockers 29 (69) 19 (49) .02Calcium channel blocker 11 (26) 53 (22) .55ACE inhibitors 2 (5) 42 (17) .04Diuretics 2 (5) 26 (11) .23
RWT, relative wall thickness; LV, left ventricular; RV, right ventricular;other abbreviations as in Table 1.
Outcomes and Prognostic Predictors in the TotalPopulation
During a mean follow-up of 42 6 31 months, 42 patientshad a clinical deterioration leading to septal reduction ther-apy, including 33 who underwent septal myectomy and 9septal alcohol ablation. All of the patients that had septalreduction developed a clear indication for the procedure:LV gradient at rest associated with a clear clinical deterio-ration not manageable with optimal medical therapy. At thepreassessment for the procedure, 34 patients (81%) were inNYHA functional class III and 8 (19%) were in ambulatoryNYHA functional class IV. In these patients, a mean clin-ical deterioration of NYHA functional class of 1.6 6 0.3from baseline was observed.Table 2 presents baseline features of the patients accord-
ing to outcomes. Patients that underwent septal reductiontherapy were characterized at baseline by a greater IVSand PW thickness (IVS: 19 6 5 vs 17 6 5 mm [P 5
Fig. 1. Prevalence of left ventricular gradient at rest or stress.Group 1: patients without obstructivon; group 2: patients withobstruction at rest; group 3: patients with latent obstruction.
.006]; PW: 13 6 3 vs 12 6 3 [P 5 .030]), a greater LAsize (LAVi O40 mL/m2 present in 69% vs 35%, respec-tively; P ! .001), and a higher E/e0 (15 6 8 vs 11 6 7;P 5 .011).
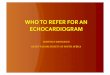
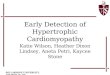
The end point occurred in 12/67 (22%) in group 2, 28/84(33%) in group 3, and 2/132 (1.5%) in group 1. Event-freesurvival at 12, 24 ,and 60 months was 89%, 86%, and 84%in group 2, 73%, 67%, and 62% in group 3, and 98%, 98%,and 98% in group 1; P ! .001 (Fig. 2).
Table 3 presents the outcome predictors from the base-line data with univariate and multivariate analysis. Themodel both including and not including presence ofobstruction with stress (IV gradientO30 mm Hg) is shown.In the model considering exercise echocardiography assess-ment of LV gradient, the independent predictors of clinicaldeterioration leading to septal reduction during follow-upwere: LV gradient O30 mm Hg at rest (hazard ratio [HR]2.56, 95% CI 1.27e5.14; P 5 .009), LV gradient O30mm Hg at stress (HR 4.96, 95% CI 1.81e13.61; P 5.002), and LAVi O40 mL/m2 (HR 2.86, 95% CI1.47e5.55; P 5 .002).
An analysis excluding the patients that had an earlierreduction therapy was performed with similar results and

Fig. 2. Kaplan-Meier curves of nonobstructive (group 1), obstruc-tive at rest (group 2), and latent obstructive (group 3) subgroups.
240 Journal of Cardiac Failure Vol. 20 No. 4 April 2014
a significant difference between survival free from clinicaldeterioration in the 3 groups (P ! .001).
Prognostic Predictors in the Latent ObstructionPopulation
Univariate and multivariate predictors of events in thissubgroup (n 5 67) are presented in Table 4. The strongestpredictor of clinical deterioration was LAVi O40 mL/m2
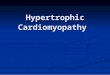
(HR 3.75, 95% CI 1.12e12.51; P 5 .032). We did notobserve a direct relationship between the magnitude ofLV gradient and the occurence of clinical deterioration(Fig. 3A), although we found a significant association be-tween LA size and the end point during follow-up(Fig. 3B).
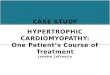
Figure 4 shows event-free survival according to presenceof LAVi O40 mL/m2 in this subgroup. Patients with LAViO40 mL/m2 showed a significantly lower event-free sur-vival; 85%, 71%, and 63% vs 93%, 89%, and 89%, at 12,24, and 60 months, respectively, P ! .001).
Table 3. Univariate and Multivariate Predicto
Univariate Analysis
HR (95% CI) P Value
Age (y) 1.01 (0.99e1.03) .41Male sex 0.64 (0.35e1.67) .14Indexed IVS O10 mm/m2 2.22 (1.18e4.18) .01PW (mm) 1.01 (1.01e1.21) .02RWT 5.91 (2.18e16.06) !.001LV gradient O30 mm Hg at rest 5.88 (3.09e11.18) !.001LV gradient O30 mm Hg during
stress8.56 (3.36e21.8) !.001
LVEF (%) 1.03 (0.99e1.06) .14E/e0 1.04 (1.01e1.07 .01E0 0.83 (0.75e0.93) .002S0 0.80 (0.67e0.95) .01LAVi O40 mL/m2 3.67 (1.90e7.07) !.001
Abbreviations as in Tables 1 and 2.
Discussion
Prevalence of LV Obstruction
In this study we considered a large series of patientswith HCM evaluated with exercise echocardiography atbaseline, focusing on the prevalence of latent obstructionand its prognostic impact. More than 50% of the samplewas characterized by an obstruction at rest and/or at stress.The principle novel finding of our study is that the presenceof latent obstruction or a significantly enlarged left atrialvolume are associated with a high prevalence of clinicaldeterioration leading to septal reduction therapy duringfollow-up.
The results underscore the main role of exercise echocar-diography in the overall assessment and prognostic stratifi-cation of HCM patients.
An intracavitary LV gradient, typically across the LVOT,is an important pathophysiologic feature of HCM.2 Inearlier studies, 25%e30% of patients with HCM had a sig-nificant LVOT gradient at rest.6 Exercise or maneuvers thatdecrease cardiac load can also unmask significant obstruc-tion. The presence and the magnitude of the LV gradient areaffected by several variables, including the loading condi-tions of the patient at the moment of the exam and strokevolume.20
In a study by Maron et al6 among 201 symptomaticand asymptomatic patients with peak instantaneous gradi-ents !50 mm Hg at rest, 106 (53%) developed mechanicalobstruction after exercise. Shah et al21 studied 87 symptom-atic HCM patients with a resting peak gradient !30 mmHg and reported that LVOT obstruction developed in 54 pa-tients (62%) during exercise echocardiography. In addition,they observed that patients with latent obstruction weremore likely to have systolic anterior motion of the mitralvalve at rest (relative risk 2.1, 95% CI 1.2e3.8; P 5 .01)than patients with nonobstructive HCM.
rs of Outcome in the Overall Population
MultivariateAnalysis
(Not IncludingAssessment of LV
GradientDuring Stress)
MultivariateAnalysis
(Including Assessmentof LV GradientDuring Stress)
HR (95% CI) P Value HR (95% CI) P Value
4.86 (2.53e9.35) !.001 2.57 (1.27e5.14) .0094.95 (1.81e13.56) .002
2.75 (1.42e5.36) .003 2.86 (1.47e5.55) .002

Table 4. Univariate and Multivariate Predictors of Outcome in Latent Obstructive Population (n 5 67)
Univariate Analysis Multivariate Analysis
HR (95% CI) P Value HR (95% CI) P Value
Age (y) 1.01 (0.98e1.03) .48Male sex 0.73 (0.19e2.70) .64Indexed IVS O10 mm/m2 3.30 (1.05e10.51) .04PW (mm) 1.28 (1.02e1.61) .03LAVi O40 mL/m2 3.75 (1.22e12.51) .03 3.75 (1.12e12.51) .032E/e0 1.14 (1.05e1.22) .001S0 0.46 (0.29e0.72) .001
Abbreviations as in Table 1.
Exercise Echocardiography in Hypertrophic Cardiomyopathy � Finocchiaro et al 241
It is well known that there are several physiologic ma-neuvers that can provoke an LVOT gradient in HCM. Exer-cise echocardiography is considered to be a reliable methodfor the detection and quantification of exercise-induced dy-namic LV obstruction in patients who have a resting peakinstantaneous gradient #30 mm Hg (according to currentguidelines, it has a class IIa recommendation, level of evi-dence B).7 Exercise echocardiography is also a useful toolfor symptoms evaluation and determination of exercise ca-pacity, and if a provocable obstruction is detected it justifiesthe use of medications aimed at decreasing the obstructionand symptom relief.In the present population, patients with latent obstruction
at baseline showed an increased LV wall thickness, morefrequently systolic anterior motion of the mitral valve, anda larger LA size compared with nonobstructive patients.
Latent Obstruction as a Prognostic Predictor in HCM
Several studies have demonstrated that resting LVOTobstruction is associated with a moderate increase in overallmortality in patients with HCM.5,22 Maron et al3 studied alarge population of HCM patients (n5 1,101) and observedthat a resting LVOT peak instantaneous gradient $30 mm
Fig. 3. (A) Prevalence of various grades of left ventricular obstruc-tion at stress and events in the latent obstruction subgroup. (B)Prevalence of various grades of left atrial dilation (left atrial vol-ume index) and events in the latent obstruction subgroup.
Hg was independently associated with an increased riskof both cardiac death (relative risk 1.6; P 5 .02), progres-sion to NYHA functional class III or IV, or death from heartfailure or stroke (relative risk 2.7; P 5 .001). Autore et al23
in a population of 526 HCM patients demonstrated thatpresence of LV obstruction was an important predictor ofcardiovascular death, particularly in patients who wereasymptomatic or mildly symptomatic.
Septal myectomy and alcohol septal ablation are reason-able options for the treatment of eligible patients with HCMwith severe drug-refractory symptoms and LVOTobstruction.1,4,24
To the best of our knowledge, only 1 earlier study hasanalyzed echocardiographic factors associated with riskfor clinical deterioration leading to septal reduction in asample of patients with HCM studied with exercise echo-cardiography. Vaglio et al25 analyzed a cohort of 415 pa-tients (20% in NYHA functional class IIIeIV) withlatent obstruction. Almost 20% of patients in that referralseries required invasive therapy for relief of symptoms.Although LVOT gradient at rest was the strongest multi-variate predictor of septal reduction during follow-up,LVOT-provoked gradient did not reach statistical signifi-cance. Our study considered a large population of bothobstructive and nonobstructive HCM patients to compareoutcomes according to the presence of a significantgradient at rest and/or during stress. Our results suggest
Fig. 4. Kaplan-Meier curves according to the presence of eft atrialvolume index (LAVi) O40 mL/m2 in the latent obstructionpopulation.

242 Journal of Cardiac Failure Vol. 20 No. 4 April 2014
that a significant proportion of patients with latentobstruction at baseline ultimately require surgical ornonsurgical septal reduction, whereas patients nonobstruc-tive at rest/stress almost never show clinical deteriorationthat warrants intervention by septal reduction. It is note-worthy that during follow-up in both the latent obstructiveand in the obstructive subgroup similar percentages (12%and 13%, respectively) showed clinical deterioration lead-ing to septal reduction from a less advanced baselineNYHA functional class (IeII). The nonobstructivesubgroup was less clinically impaired at baseline, andonly 1 patient experienced worsened clinical conditionrequiring a reductive therapy.
LV gradient O30 mm Hg during exercise emerged asthe strongest independent predictor of clinical deteriora-tion leading to septal reduction during follow-up in thetotal population. This is probably due to the fact thatthe stress evaluation unmasks a significant proportion ofpatients defined as nonobstructive by rest echocardiogra-phy only. Our findings are consistent with an increasedrate of events during follow-up even in patients with astress LV gradient of 30e50 mm Hg. This observationis in contrast to some evidence that considers only astress gradient O50 mm Hg to be clinically significant,and it is important not to underestimate the clinical valueof a ‘‘mild’’ stress LV gradient.
In the subgroup with latent obstruction, the factor moststrongly associated with clinical deterioration leading toseptal reduction during follow-up was LA size. Variousgrades of atrial dilatation were previously associated withworse outcomes in HCM.26,27 Considering that LA sizemirrors LV pressures in several cardiac diseases, in the cur-rent context it is likely that patients with larger atria werecharacterized by a relatively constant state of elevatedfilling pressures that led to a worsening of clinical status.Overall, LA size seems to be a red flag in the generalassessment of HCM patients.
Study Limitations
There are several limitations in our study, includingreferral bias in our sample, due to the fact that Stanford Uni-versity is a major center for the evaluation of cardiomyopa-thies. In addition, we considered only echocardiographicdata at baseline and before the procedure of septal reduction,rather than throughout the whole follow-up; therefore, we donot have data on echocardiographic progression of disease.The indication to reductive therapy was assessed by thephysician according to the clinical status and the presenceof a significant gradient. Advanced NYHA functional classwas considered to be an indicator of clinical deterioration,as was exercise test in some patients, though performed inonly a minority of the patients in the preassessment for septalreduction therapy. Therefore, an objective measure of clin-ical impairment was not available and consequently notconsidered for the present study.
Conclusion
The present study underscores the important role of exer-cise echocardiography in the assessment of patients withHCM. Unmasking a significant LV gradient in patientswith HCM with the use of exercise echocardiography islikely to be helpful in selecting patients that should be fol-lowed more carefully. Left atrial size and latent obstructionare the main predictors of clinical deterioration leading toseptal reduction therapy in HCM patients.
Disclosures
Dr Finocchiaro is funded by Biotronik Italia. EmmaMag-avern has been funded by Sarnoff Cardiovascular ResearchFoundation.
References
1. Maron BJ, Maron MS, Wigle ED, Braunwald E. The 50-year history,
controversy, and clinical implications of left ventricular outflow
tract obstruction in hypertrophic cardiomyopathy from idiopathic hy-
pertrophic subaortic stenosis to hypertrophic cardiomyopathy: from
idiopathic hypertrophic subaortic stenosis to hypertrophic cardiomy-
opathy. J Am Coll Cardiol 2009;54:191e200.2. Argulian E, Chaudhry FA. Stress testing in patients with hypertrophic
cardiomyopathy. Prog Cardiovasc Dis 2012;54:477e82.
3. MaronMS, Olivotto I, Betocchi S, Casey SA, Lesser JR, Losi MA, et al.
Effect of left ventricular outflow tract obstruction on clinical outcome in
hypertrophic cardiomyopathy. N Engl J Med 2003;348:295e303.
4. Ommen SR, Maron BJ, Olivotto I, Maron MS, Cecchi F, Betocchi S,
et al. Long-term effects of surgical septal myectomy on survival in pa-
tients with obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol
2005;46:470e6.
5. Maron BJ, Maron MS. Hypertrophic cardiomyopathy. Lancet 2013;
381:242e55.6. Maron MS, Olivotto I, Zenovich AG, Link MS, Pandian NG,
Kuvin JT, et al. Hypertrophic cardiomyopathy is predominantly a dis-
ease of left ventricular outflow tract obstruction. Circulation 2006;114:
2232e9.7. Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, LinkMS, et al.
2011ACCF/AHAguideline for the diagnosis and treatment of hypertro-
phic cardiomyopathy: executive summary: a report of the American
College of Cardiology Foundation/American Heart Association Task
Force on Practice Guidelines. J Am Coll Cardiol 2011;58:2703e38.
8. RickhamPP. Human experimentation. Code of ethics of theWorldMed-
ical Association. Declaration of Helsinki. Br Medical J 1964;2:177.
9. Binder J, OmmenSR,GershBJ,VanDriest SL,TajikAJ,NishimuraRA,
et al. Echocardiography-guided genetic testing in hypertrophic cardio-
myopathy: septal morphological features predict the presence ofmyofil-
ament mutations. Mayo Clin Proc 2006;81:459e67.10. SahnDJ,DeMariaA,Kisslo J,WeymanA.Recommendations regarding
quantitation in M-mode echocardiography: results of a survey of echo-
cardiographic measurements. Circulation 1978;58:1072e83.11. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E,
Pellikka PA, et al. Recommendations for chamber quantification: a report
from the American Society of Echocardiography’s Guidelines and Stan-
dards Committee and the Chamber QuantificationWriting Group, devel-
oped in conjunctionwith the EuropeanAssociation of Echocardiography,
a branch of the European Society of Cardiology. JAm Soc Echocardiogr
2005;18:1440e63.

Exercise Echocardiography in Hypertrophic Cardiomyopathy � Finocchiaro et al 243
12. Nishimura RA, Tajik AJ. Evaluation of diastolic filling of left ventricle
in health and disease: Doppler echocardiography is the clinician’s Ro-
setta Stone. J Am Coll Cardiol 1997;30:8e18.
13. Nagueh SF, Appleton CP, Gillebert TC,Marino PN, Oh JK, Smiseth OA,
et al. Recommendations for the evaluation of left ventricular diastolic
function by echocardiography. JAmSocEchocardiogr 2009;22:107e33.
14. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD,
Levine RA, et al. Recommendations for evaluation of the severity of
native valvular regurgitation with two-dimensional and Doppler echo-
cardiography. J Am Soc Echocardiogr 2003;16:777e802.
15. Tei C, Dujardin KS, Hodge DO, Bailey KR, McGoon MD, Tajik AJ,
et al. Doppler echocardiographic index for assessment of global right
ventricular function. J Am Soc Echocardiogr 1996;9:838e47.
16. Yu CM, Sanderson JE, Marwick TH, Oh JK. Tissue Doppler imaging a
new prognosticator for cardiovascular diseases. J Am Coll Cardiol
2007;49:1903e14.
17. Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD,
Chandrasekaran K, et al. Guidelines for the echocardiographic assess-
ment of the right heart in adults: a report from the American Society of
Echocardiography endorsed by the European Association of Echocar-
diography, a registered branch of the European Society of Cardiology,
and the Canadian Society of Echocardiography. J Am Soc Echocar-
diogr 2010;23:685e713.18. Douglas PS, Khandheria B, Stainback RF, Weissman NJ, Peterson ED,
Hendel RC, et al. ACCF/ASE/ACEP/AHA/ASNC/SCAI/SCCT/SCMR
2008 appropriateness criteria for stress echocardiography: a report of the
American College of Cardiology Foundation Appropriateness Criteria
Task Force, American Society of Echocardiography, American College
of Emergency Physicians, AmericanHeart Association, American Soci-
ety of Nuclear Cardiology, Society for Cardiovascular Angiography and
Interventions, Society of Cardiovascular Computed Tomography, and
Society for Cardiovascular Magnetic Resonance endorsed by the Heart
Rhythm Society and the Society of Critical Care Medicine. J Am Coll
Cardiol 2008;51:1127e47.
19. Borg G. Psychophysical scaling with applications in physical work
and the perception of exertion. Scand J Work Environ Health 1990;
16(Suppl 1):55e8.
20. Joshi S, Patel UK, Yao SS, Castenada V, Isambert A, Winson G, et al.
Standing and exercise Doppler echocardiography in obstructive hyper-
trophic cardiomyopathy: the range of gradients with upright activity. J
Am Soc Echocardiogr 2011;24:75e82.
21. Shah JS, Esteban MT, Thaman R, Sharma R, Mist B, Pantazis A, et al.
Prevalence of exercise-induced left ventricular outflow tract obstruc-
tion in symptomatic patients with nonobstructive hypertrophic cardio-
myopathy. Heart 2008;94:1288e94.22. Elliott PM, Gimeno JR, Tome MT, Shah J, Ward D, Thaman R, et al.
Left ventricular outflow tract obstruction and sudden death risk in pa-
tients with hypertrophic cardiomyopathy. Eur Heart J 2006;27:1933e41.
23. Autore C, Bernabo P, Barilla CS, Bruzzi P, Spirito P. The prognostic
importance of left ventricular outflow obstruction in hypertrophic car-
diomyopathy varies in relation to the severity of symptoms. J Am Coll
Cardiol 2005;45:1076e80.
24. Olivotto I, Ommen SR, Maron MS, Cecchi F, Maron BJ. Surgical
myectomy versus alcohol septal ablation for obstructive hypertrophic
cardiomyopathy. Will there ever be a randomized trial? J Am Coll Car-
diol 2007;50:831e4.
25. Vaglio JC Jr, Ommen SR, Nishimura RA, Tajik AJ, Gersh BJ.
Clinical characteristics and outcomes of patients with hypertro-
phic cardiomyopathy with latent obstruction. Am Heart J 2008;
156:342e7.
26. Nistri S, Olivotto I, Betocchi S, Losi MA, Valsecchi G, Pinamonti B,
et al. Prognostic significance of left atrial size in patients with hyper-
trophic cardiomyopathy (from the Italian Registry for Hypertrophic
Cardiomyopathy). Am J Cardiol 2006;98:960e5.27. Finocchiaro G, Pinamonti B, Merlo M, Brun F, Barbati G, Sinagra G.
Prognostic role of clinical presentation in symptomatic patients with
hypertrophic cardiomyopathy. J Cardiovasc Med (Hagerstown) 2012;
13:810e8.