Embed Size (px)
Citation preview

mop
pvmsddtdi
tibaisbhs
bucr
R1
2
3
4
5
6
7
8
J6
Tmlitcic
R
l
s
S
j
©
0
d
2374 PANFACIAL FRACTURES AND LATE VASCULAR INJURIES
embers suggests a sporadic mutation affecting onef the genes responsible for bone homeostasis in thisatient.Cranial nerve compression has been described in
atients’ with van Buchem disease; however, cerebro-ascular accidents have not been identified com-only in these patients. Although the patient de-
cribed some disturbance in facial sensation andisplayed skull bone thickening radiographically, it isifficult to say whether the condition contributed tohe cerebrovascular accidents without radiologic evi-ence of compression of the brain or vascular canals
n the skull base.Previous reports of surgical intervention on pa-
ients with van Buchem disease and ADO4-6,8 havendicated normal healing although no comments haveeen made on longer term recurrence at surgically-ddressed sites. We were concerned about the heal-ng capacity of the bone and carried out more limitedurgery at the first intervention. These fears seem toe unfounded and, ironically with the wisdom ofindsight, the history of palmidronate infusions
hould have caused greater concern.Frank Newman, DDS, MS,* and
catatlf
R
aEdhbgufbtwoi:10.1016/j.joms.2008.06.035
The recurrence of the bony exostoses at the lowerorder of the mandible in this case indicate that thenderlying process is still active. Patients with similaronditions should be advised of the possibility ofecurrence before surgical intervention.
eferences. Janssens K, Van Hul W: Molecular genetics of too much bone.
Hum Mol Genet 11:2385, 2002. Van Hul W: Recent progress in the molecular genetics of scle-
rosing bone dysplasias. Pediatr Pathol Mol Med 22:11, 2003. Van Wesenbeeck L, Cleiren E, Gram J, et al: Six novel missense
mutations in the LDL receptor-related protein 5 (LRP5) gene indifferent conditions with an increased bone density. Am J HumGenet 72:763, 2003
. Schendel SA: Van Buchem disease: Surgical treatment of themandible. Ann Plast Surg 20:462, 1988
. Ruckert EW, Caudill RJ, McCready PJ: Surgical treatment of vanBuchem’s disease. J Oral Maxillofac Surg 43:801, 1985
. Renton T, Odell E, Drage NA: Differential diagnosis and treat-ment of autosomal dominant osteosclerosis of the mandible. Br JOral Maxillofac Surg 40:55, 2002
. Balemans W, Patel N, Ebeling M, et al: Identification of a 52 kbdeletion downstream of the SOST gene in patients with vanBuchem disease. J Med Genet 39:91, 2002
. Vanhoenacker FM, De Beuckeleer LH, Van Hul W, et al: Scleros-
ing bone dysplasias: Genetic and radioclinical features. EuroRadiol 10:1423, 2000Oral Maxillofac Surg6:2374-2377, 2008
Late Vascular Complication AssociatedWith Panfacial Fractures
Joseph E. Cillo, Jr, DMD†
he occurrence of late post-traumatic aneurysm fromaxillofacial injuries is a rare complication of maxil-
ofacial trauma.1-5 False aneurysms of facial vesselsnvolved may include the superficial temporal artery,6
he maxillary artery,5,7 and the facial artery.8-10 Theseonditions may generally manifest themselves clin-cally through facial swelling, hemorrhaging, or de-reased hematocrit, and can be confirmed with
eceived from the Division of Oral and Maxillofacial Surgery, Al-
egheny General Hospital, Pittsburgh, PA.
*Chief Resident.
†Associate Program Director.
Address correspondence and reprint requests to Dr Cillo: Divi-
ion of Oral and Maxillofacial Surgery, Allegheny General Hospital,
uite 0107, 320 East North Avenue, Pittsburgh, PA 15212; e-mail:
2008 American Association of Oral and Maxillofacial Surgeons
278-2391/08/6611-0030$34.00/0
omputed tomography and computed tomographyngiograms. Many treatment options have been at-empted to resolve ruptures vessels, including tampon-de, direct ligation, hemostatic agents, and emboliza-ion. This case report will detail the management of aate vascular complication associated with panfacialractures.
eport of a Case
A 49-year-old Caucasian female fell 80 feet from a bridgend was transported to the Allegheny General Hospitalmergency Department with extensive facial and orthope-ic injuries. On arrival to the Emergency Department, shead a Glasgow coma scale of 6 and was subsequently intu-ated then later underwent tracheotomy. Clinical and radio-raphic facial examination showed a comminuted mandib-lar symphysis fracture, bilateral mandibular subcondylarractures, multiple fractured teeth, a Le Fort II fracture,ilateral comminuted zygomaticomaxillary complex frac-ures, and a type II naso-orbital ethmoid fracture. There
ere no major vascular injuries and hemostasis was well
cdfa
hrav1s(trlmtteblb3iqwami
ratttmwi1lteaab
Fi
Nr
Nr
Fmm
NEWMAN AND CILLO 2375
ontrolled during her initial presentation. The patient un-erwent open reduction and internal fixation of panfacialractures through multiple surgical approaches by the oralnd maxillofacial surgery service without complications.
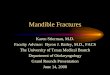
Her initial postoperative course was unremarkable as sheealed uneventfully. Due to multiple orthopedic injuriesequiring bed rest, the patient had been placed on oralnticoagulation therapy by the primary service for deepein thrombosis prophylaxis that consisted of warfarin0 mg/day by mouth. At the 4-week postoperative period,he developed a spontaneous and sudden left facial swellingFig 1). The swelling was indurated, nonfluctuant, nonery-hematous, nonpulsatile, and extended from the left tempo-al region down to the mandibular region with subsequentimited mandibular mobility and deviation to the right of
idline. There were no intraoral or extraoral signs of infec-ion and the patient remained afebrile. Clear saliva was ableo be obtained from the left parotid gland. Her neurologicxamination had remained unchanged from a GCS of 15efore the occurrence of the facial swelling. She did report
eft-sided headache, pulsation, and tinnitus. She did notecome hypotensive, had a slight drop in hematocrit from8 to 36, a slight drop in hemoglobin from 14 to 12, and her
nternational normalization ratio (INR) was 2.3. She subse-uently underwent head and neck computed tomographyith contrast (Figs 2, 3) and carotid angiogram that showedpseudoaneurysm of the left superficial temporal arteryeasuring 3.5 cm and extravasation from a transected left
nternal maxillary artery. The left occipital, ascending pha-
IGURE 1. Left facial swelling 4 weeks after open reduction andnternal fixation of panfacial fractures.
ewman and Cillo. Panfacial Fractures and Late Vascular Inju-ies. J Oral Maxillofac Surg 2008.
Nr
yngeal, lingual, and facial arteries were normal. Remoteppearing hematomas were reported surrounding the ex-ravasations measuring 6.6 cm. These were in the mastica-or space and infratemporal fossa surrounding the angle ofhe mandible with superior extension along the temporalisuscle with mass effect of the temporal soft tissues. Thearfarin was stopped and she was given 5.0 mg vitamin K1
ntravenously and fresh frozen plasma to lower her INR to.1. Once INR had been normalized, she underwent embo-
ization by the Department of Interventional Radiology withwo 2-�m fiber coils placed distally within the distal leftxternal carotid artery and the proximal internal maxillaryrtery. Subsequent follow-up angiogram showed static flowt the site of coil placement. After completion of the em-olization, the patient underwent evacuation of the hema-
FIGURE 2. Axial CT scan of left-sided facial swelling.
ewman and Cillo. Panfacial Fractures and Late Vascular Inju-ies. J Oral Maxillofac Surg 2008.
IGURE 3. Coronal CT scan of left-sided facial swelling showingass effect of extravasation having medially displaced the leftandibular condyle to the cranial base.
ewman and Cillo. Panfacial Fractures and Late Vascular Inju-ies. J Oral Maxillofac Surg 2008.

tb
rc
D
tivtshpvaow
swubaditdpsiabtctfpssfuttt
papsLpicthtp2oIrhmbth2icmtcI
Ff
Nr
2376 PANFACIAL FRACTURES AND LATE VASCULAR INJURIES
oma via intraoral incision under general anesthesia. Nolood transfusions were required.At the 6-month follow-up appointment, the patient had
esolution of her facial swelling with no neurologicalhanges from before the hemorrhaging (Fig 4).
iscussion
Vascular injuries to facial arteries are rare sequelaeo blunt facial trauma with a reported incidence rang-ng from 1.25% to 11%.11 Nasal bleeding has been theascular complication reported most commonly inhe early phase after facial injury.1-4 Management ofevere nasal bleeding associated with facial fracturesas been managed with procedures ranging from tam-onade to transcatheter arterial embolization. Lateascular complications, those occurring days or weeksfter facial fractures, are also rare. Clinical symptomsf late hemorrhaging of the facial arteries often start
IGURE 4. Six months postoperative showing resolution of leftacial swelling.
ewman and Cillo. Panfacial Fractures and Late Vascular Inju-ies. J Oral Maxillofac Surg 2008.
ith increased facial swelling, which may persist for i
everal days to weeks, and may lead to possible air-ay compromise. Late vascular complications aresually the result of pseudoaneurysm formation inranches of the carotid artery. Pseudoaneurysms aren outpouching of the artery involving a traumaticefect in the 2 innermost tissue layers, the tunica
ntima and tunica media. The outermost layer, theunica adventia, may be intact, or all 3 layers may beamaged with bleeding contained by a blood clot orroduction of a hematoma in the confines of theurrounding soft tissue.7 A true aneurysm, in contrast,s a vascular outpouching containing all 3 layers of thertery. Hematoma size in a pseudoaneurysm is limitedy the equilibrium between hematoma pressure andhe vessel. Within days, liquefaction of the hematomaenter as well as pseudointima production of connec-ive tissue along the outer wall occurs. Further lique-action of the center, causes the pseudoaneurysm torogressively evolve and enlarge. The increased pres-ure on the surrounding tissue may rupture and causeevere hemorrhaging.7 As a result of pseudoaneurysmormation, severe hemorrhaging may not be achievedntil days or weeks after the initial injury. This situa-ion can be further complicated with deep veinhrombosis (DVT) prophylaxis with the administra-ion of warfarin.
Postoperative anticoagulation therapy for DVT pro-hylaxis is generally recommended for patients whore older than 40 years, have prolonged immobility oraralysis, history of DVT, or who underwent majorurgery (eg, abdomen, pelvis, lower extremity, etc).ow molecular-weight heparin is used widely in theerioperative setting for DVT prophylaxis. However,
n this situation, the patient was placed on oral anti-oagulation therapy of warfarin by the primaryrauma service because it was believed that she was aigh risk for DVT and would benefit from warfarinherapy.12 International normalization ratio for DVTrophylaxis in these cases is desired to be between.0 and 3.0.13 Warfarin acts by inhibiting the synthesisf functional vitamin K-dependent coagulation factorsI, VII, IX, and X. The effective half-life of warfarinanges from 20 to 60 hours, with a mean of about 40ours and a duration of effect of 2 to 5 days. As theost common complication of warfarin therapy is
leeding, close monitoring of the INR must be main-ained. Several studies have shown that the risk ofemorrhaging doubled as the INR increased from.0–2.9 to 3.0–4.4, and quadrupled when the INR
ncreased to 4.5–6.0. Another study showed an in-rease in INR by 0.5 multiplied the absolute risk ofajor bleeding (mostly intracranial) by 1.43.11,13 Al-
hough the bleeding risk increases as the INR in-reases, 50% of bleeding episodes occur while theNR is less than 4.0.14 In situations where hemorrhag-
ng occurs and the INR is required to be lowered,
waivhf
estiameielmnbaswbi
mtfoca
R
1
1
1
1
1
1
Tpk
T
c
G
B
b
GRAHAM, SMYTH, AND LANGTON 2377
arfarin is discontinued and intravenous vitamin K1
nd fresh frozen plasma can be administered. Admin-stration of vitamin K1 reverses warfarin’s effect of theitamin K-dependent coagulation factors in about 24ours whereas the fresh frozen plasma has all theseactors and has a more immediate effect.
Treatment options for vascular lesions could beither surgical or nonsurgical. When surgical options,uch as ligation of the proximal and distal portions ofhe artery, are not feasible, nonsurgical, minimally-nvasive treatment options, such as embolization, are more practicable option. This endovascular treat-ent is usually achieved by the femoral route; a cath-
ter guide is positioned enabling microcatheters to benserted.1 Microcatheters allow insertion of differentmbolization materials, such as particles, coils, bal-oons, or liquids like cyanoacrylate or alcohol.6 Coils
ay be placed for permanent occlusion of the exter-al carotid artery and internal maxillary arteries. Em-olization of pseudoaneurysms of the facial arteriesfter trauma and elective surgery has been manageduccessfully in the past.4,6,15 The procedure is notithout risks, however, including a 1% risk of a cere-rovascular accident from the passage of particles or
njected liquids through vessels to the brain.6
This case illustrates that late vascular complicationsay occur in the maxillofacial region after facial frac-
ures. Follow-up should be maintained with panfacialracture patients to ensure that vascular injuries do notccur, particularly in anticoagulated patients. If late vas-ular complications do occur, early diagnosis and man-
gement is warranted to prevent additional injury.Stephen G. Langton, F
ovw
urn Hospital, Blackburn, UK.
D
G
y
©
0
d
eferences1. Ardekian L, Samet N, Shoshani Y, et al: Life-threatening bleed-
ing following maxillofacial trauma. J Craniomaxillofac Surg21:336, 1993
2. Yang WG, Tsai TR, Hung CC, et al: Life-threatening bleeding ina facial fracture. Ann Plast Surg 46:159, 2001
3. Murakami R, Kumazaki T, Tajima H, et al: Transcatheter arterialembolization as treatment for life-threatening maxillofacial in-jury. Radiat Med 14:197, 1996
4. Mehrotra ON, Brown GE, Widdowson WP, et al: Arteriographyand selective embolization in the control of life-threatening hem-orrhage following facial fractures. Br J Plast Surg 37:482, 1984
5. Schwartz HC, Kendrick RW, Pogorel BS: False aneurysm of themaxillary artery. An unusual complication of closed facialtrauma. Arch Otolaryngol 109:616, 1983
6. Sanchez F, Delgado F, Ramos M: Pseudoaneurysm of the super-ficial temporal artery treated by embolization: Report of a case.J Oral Maxillofac Surg 58:819, 2000
7. Krishman D, Marashi A, Malik A: Pseudoaneurysm of internalmaxillary artery secondary to gunshot wound managed byendovascular techniques. J Oral Maxillofac Surg 62:500, 2004
8. Pettiti L, Jenning HB: False aneurysm of the facial artery. U SArmed Forces Med J 3:781, 1952
9. Ghenini AJ, Horde DR, Hesse CJ: False aneurysm of the facialartery. Calif Med 95:312, 1961
0. Cooperband BR, Friedel W, Bhatt GM, et al: False aneurysm ofthe facial artery. J Oral Maxillofac Surg 47:1327, 1989
1. Ho K, Hutter JJ, Eskridge J, et al: The management of life-threatening hemorrhage following blunt facial trauma. J PlastReconstr Aesthet Surg 59:1257, 2006
2. Colwell CW Jr, Annenberg Center for Health Sciences andQuadrant Medical Education: Thromboprophylaxis in orthope-dic surgery. Am J Orthop Suppl:1, 2006
3. Bynoe RP, Kerwin AJ, Parker HH 3rd, et al: Maxillofacial inju-ries and life-threatening hemorrhage: Treatment with trans-catheter arterial embolization. J Trauma 55:74, 2003
4. Bishop B, Wilson AG, Post D, et al: A pilot study of home treat-ment of deep vein thrombosis with subcutaneous once-dailyenoxaparin plus warfarin. J Manag Care Pharm 12:70, 2006
5. The Stroke Prevention in Reversible Ischemia Trial (SPIRIT)Study Group: A randomized trial of anticoagulants versus aspi-rin after cerebral ischemia of presumed arterial origin. Ann
Neurol 42:857, 1997J Oral Maxillofac Surg66:2377-2379, 2008
Intraorbital Wooden Foreign BodyRichard M. Graham, FDSRCS, MRCS,*
Katherine L. Smyth, FRCOphth,† and
DSRCPS, FRCS‡
here have been many previous reports of unusualenetrating orbital injuries—for example, with anife,1 firearm projectile,2 bicycle hand brake,3 and
*Formerly, Specialist Registrar in Oral and Maxillofacial Surgery,
he Royal Blackburn Hospital, Blackburn, UK; and Currently, Spe-
ialist Registrar in Oral and Maxillofacial Surgery, North Manchester
eneral Hospital, Crumpsall, UK.
†Consultant in Ophthalmology, The Royal Bolton Hospital,
olton, UK.
‡Consultant in Oral and Maxillofacial Surgery, The Royal Black-
thers. We present a similar case; this, however, in-olved an intraorbital wooden foreign body (WFB)4
ith unusual features.
Address correspondence and reprint requests to Mr Graham:
epartment of Oral and Maxillofacial Surgery, North Manchester
eneral Hospital, Crumpsall, M8 5RB, UK; e-mail: grahamrm2@
ahoo.co.uk
2008 American Association of Oral and Maxillofacial Surgeons
278-2391/08/6611-0031$34.00/0
oi:10.1016/j.joms.2007.12.044

![CaseReport ... · chanical complication rate of the GUEPAR®prosthesis in-cluding femoral and tibial stem fractures, severe bushing wear,andahingefracture[11]. Incontrasttootherprostheses,literaturedatashowthat](https://img.pdfslide.us/doc/110x75/5f9ed2f31b08c43834634ba0/casereport-chanical-complication-rate-of-the-gueparprosthesis-in-cluding-femoral.jpg)