Embed Size (px)
Citation preview

Late Re...opening of Macular Holes after Initially Successful Treatment with Vitreous Surgery
JayS. Duker, MD,l Robert Wendel, MD,2 Arun C. Patel, MD,2
Carmen A Puliafito, MD1
Background: In more than 50% of eyes with idiopathic, full-thickness macular holes, vitrectomy results in clinical closure of the hole and improvement in visual acuity. Other than cataract formation, late complications of the procedure have not been reported.
Methods: Over a 4-year period, 167 eyes underwent successful vitreous surgery for idiopathic macular holes documented by clinical closure of the hole and an improvement in visual acuity of at least two Snellen lines. The authors retrospectively studied eight of these eyes. All initially had successful surgery; however, they subsequently had spontaneous late re-opening of the macular hole with acute diminution in vision.
Results: Late re-opening developed in these eyes between 2 and 22 months after initial surgery. The mean time for re-opening was 12.5 months. Three of eight eyes underwent a second vitrectomy, which was successful in improving visual acuity in two eyes. Another patient manifested the growth of an epiretinal membrane that apparently sealed the re-opened macular hole and improved vision.
Conclusion: Late re-opening can complicate initially successful macular hole surgery and may occur in at least 4.8% (8 of 167) of initially successful operations. Re-opening has been documented as late as 22 months after initial surgery. Repeat vitrectomy with gas injection may result in reclosure of the hole and improvement in vision. Ophthalmology 1994; 101:1373-1378
In 1991, Kelly and Wendel1 initially reported that vitreous surgery can improve the visual acuity in some eyes with acute, idiopathic macular holes. Their surgical technique included a pars plana vitrectomy followed by careful engagement, elevation, and removal of the intact posterior hyaloid from the edges of the hole. A complete air-fluid exchange followed by injection of a dilute concentration of a long-acting inert gas was performed.
In their initial series of 52 treated eyes, 42% showed a visual acuity improvement of two or more Snellen lines
Originally received: November 15, 1993. Revision accepted: March 3, 1994. 1 New England Eye Center, New England Medical Center, Tufts University School of Medicine, Boston. 2 Mercy Eye Foundation, and Retinal Consultants, Sacramento. Presented at the American Academy of Ophthalmology Annual Meeting, Chicago, November 1993. Reprint requests to Jay S. Duker, MD, New England Medical Center, Tufts University, 750 Washington St, Box 450, Boston, MA 02111.
after surgery. 1 A higher percentage of eyes (58%) were considered anatomic successes, which was defined as disappearance of the surrounding cuff of subretinal fluid. Wendel et al's2 subsequent series showed that anatomic success could be achieved in 73% of eyes, with 55% improving two or more Snellen lines. Best results were obtained when surgery was performed within 6 months of visual loss. Documented surgical complications included intraoperative enlargement of the macular hole and postoperative retinal pigment epithelial (RPE) alterations in the area of the macular hole. 1- 3 Well-recognized complications of vitreous surgery with peeling of the posterior hyaloid and gas injection include peripheral retinal breaks and retinal detachment, as well as cataract formation in phakic eyes.
We recently observed a previously unreported complication of vitrectomy for idiopathic macular holes. In several eyes with full-thickness macular holes that were both anatomic and visual successes after vitreous surgery, spontaneous re-opening ofthe macular holes subsequently
1373

Ophthalmology Volume 101, Number 8, August 1994
developed in the late postoperative period. We undertook a retrospective analysis to identify the incidence of this complication and elucidate any possible risk factors for thts late re-opening.
Patients and Methods
All charts of all patients undergoing vitreous surgery for idiopathic macular hole at the New England Eye Center, Boston, Massachusetts, and Associated Retinal Consultants, Sacramento, California, between January 1989 and December 1992 (4 years) were reviewed.
Preoperatively, all patients received a complete ophthalmologic evaluation, including best-~orre_cted
Snellen visual acuity. All patients had a preoperative vtsual acuity of 20/50 or worse and a full-thickness macular hole on examination. Macular holes were diagnosed on contact lens examination when a full-thickness retinal defect was seen surrounded by a cuff of subretinal fluid. Macular holes were staged according to the classification of Gass and Johnson.4'5
The surgical procedure has been outlined in detail elsewhere.1·2 Briefly, all procedures were performed under local anesthesia, unless general anesthesia was requested by the patient. A standard three-port vitrectomy was completed, followed by engagement and elevat~on of the posterior hyaloid with a silicone-tipped extrus10n needle. At this juncture, epiretinal membrane (ER~), ifpresent, was peeled using a sharp instrument. An au-flmd exchange was performed, and 20% to 25% sulfur hexafluoride (S~6) gas was placed in the v~treous cavity. Pat_i~nts. were mstructed to maintain stnct face-down pos1t10nmg for at least 7 days postoperatively.
Anatomic success was determined between 2 and 4 weeks after surgery, when the gas bubble had completely resorbed. Anatomic success was defined as a complete disappearance of the cuff of subretinal fluid surrounding the macular hole. In most instances, when this occurred the edges of macular hole were opposed to the RPE, rendering identification of the macular hole difficult.
Visual success was defined as an improvement in postoperative visual acuity ofa minimum oftwo Snel~en l_ines over preoperative acuity on two or more exammatwns prior to re-opening. No eyes had visual success that did not also have anatomic success. A total of 167 eyes were considered both anatomic and visual successes.
Results
Of the 167 eyes that were considered successes, late reopening was observed to have occurred in eig_ht_~yes (4.8%). All eight eyes were document~d to _have tmtlally successful anatomic results as well as vtsualtmprovement of two or more Snellen lines on at least two examinations; however, they subsequently manifested a delayed drop in visual acuity with coincident anatomic re-opening of the macular hole.
In this group of eight patients, there were four women and four men. The mean age was 68.6 years (range, 6276 years). Six right eyes and two left eyes were affected. Three of the eight patients had bilateral macular holes. Two additional patients were noted to have lamellar macular holes in the fellow eye with essentially normal visual acuity.
The initial visual acuity was 20/80 or worse in all eight eyes. As previously stated, all eight eyes improved at least two Snellen lines; however, the mean improvement was considerably better: 4.8 Snellen lines. Visual acuity in four of eight eyes improved to 20/50 or better before re-o~ening. At the time ofthe initial vitrectomy, three ofthe etght eyes underwent significant ERM peeling. The other five had no identifiable ERM.
The mean time until re-opening was 12.5 months after initial vitrectomy (range, 2-22 months). Seven patients noted an abrupt drop in visual acuity, prompting an unscheduled visit for five of these patients. The eighth patient described a gradual loss of vision over several weeks. Visual acuity in all eight eyes after re-opening was 20/100 or worse. Four of the eight eyes had one line less Snellen visual acuity after re-opening than before the original surgery. Three of the eight eyes were noted clinically to have significant ERM growth at the time of re-opening. One of these eyes had undergone significant ERM peeling at the initial operation.
Three of eight eyes underwent cataract surgery after initial vitrectomy for macular hole before the re-opening of the hole. The mean time for re-opening after cataract surgery in these three patients was 8 months (range, 312 months). None of the cataract surgeries were associated with intraoperative or postoperative complications, and no new cystoid macular edema was detected. A fourth eye underwent uncomplicated cataract extraction after re-opening, whereas a fifth eye had cataract surgery after a second vitrectomy.
Three ofeight patients underwent a second vitrectomy operation to repair the re-opened macular hole. This second procedure consisted of peeling of ERM (in 2 eyes), air-fluid exchange, and SF6 injection, followed by facedown positioning. Two of the three operations were anatomically successful, and in both eyes visual acuity improved two or more Snellen lines. One of these eyes regained vision to the best visual acuity after initial vitrectomy (20/40) after eventual cataract removal. Ofthe eight eyes, five eventually underwent cataract extraction ~fter initial vitrectomy. The clinical characteristics of the etght patients are summarized in Table 1.
Selected Case Reports
Case 1. A 63-year-old woman noted an abrupt onset of decreased vision in the left eye. Evaluation 2 months later showed a full-thickness macular hole with visual acuity of 20/200 (Fig 1). Pars plana vitrectomy with peeling of the posterior hyaloid and injection of25% SF6 was performed. No ERM was removed.
Six weeks later, visual acuity improved to 20/60, and the hole appeared closed (Fig 2). One year later, there was gradual
1374

Duker et al · Macular Holes after Vitreous Surgery
Table 1. The Clinical Characteristics of Patients with Late Reopening of Macular Holes after Initially Successful Vitrectomy Surgery
Initial Successful Patient Age (yrs)/ Visual Visual
No. Race/Sex Eye Acuity Acuity
1 63/W/F OS 20/200 20/60 2 62/W/F OS 20/200 20/25 3 70/W/M OD 20/400 20/50 4 69/W/M OD 20/80 20/60 5 70/W/F OD 20/400 20/40 6 66/W/M OD 20/100 20/70 7 73/W/M OD 20/200 20/70 8 76/W/F OD 20/400 20/40
W = white; OS = left eye; NA = not applicable; OD = right eye.
decrease in visual acuity with a worsening nuclear sclerotic cataract. Visual acuity was 20/ I 00, and the macular hole remained closed. Potential acuity meter testing showed potential improvement in visual acuity to 20/60. An uncomplicated phacoemulsification with insertion of posterior chamber intraocular lens was performed. Postoperatively, best-corrected visual acuity improved to 20/60.
Reopen Visual Acu· Interval Visual ity after
(mos) Acuity Reoperation Reoperation
17 20/200 No NA 6 20/400 No NA
15 20/400 No NA 2 20/100 Yes 20/50
16 20/200 No NA 22 20/200 Yes 20/400 5 20/200 No NA
17 20/200 Yes 20/40
Three months later, 17 months after the original vitrectomy, the patient noted an abrupt decrease in vision. Best-corrected visual acuity was 20/200, and the macular hole was patent again, surrounded by a cuff of subretinal fluid (Fig 3). The re-opened hole appeared larger than the original. No further surgery was performed. With 18 months of follow-up, the appearance and vision are stable.
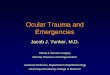
Top left, Figure 1. Case 1. Appearance of the macular hole before vi· trectomy. Visual acuity was 20/200.
Top right, Figure 2. Case 1. Appearance of the macular hole 3 months after vitrectomy. Visual acuity was 20/60.
Bottom, Figure 3. Case 1. Two months after cataract extraction, 17 months after the vitrectomy, the macular hole re-opened. Visual acuity declined to 20/400.
1375

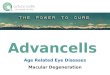
Top left, Figure 4. Case 2. Before vitrectomy, a small, stage 3 macular hole with surrounding cuff of fluid was present. Visual acuity was 20/ 200.
Top right, Figure 5. Case 2. Five weeks after vitrectomy, visual acuity was 20/25, and the hole was no longer visible.
Second row left, Figure 6. Case 2. Six months after vitrectomy, the macular hole re-opened, with a decline in visual acuity to 20/200. Notice the mild growth of an epiretinal membrane temporal to the hole, resulting in tortuosity and displacement of the superior arteriole compared with Figure 5 (arrow). An artifact is present nasal to the re-opened hole.
Second row right, Figure 7. Case 2. Three months after cataract extraction, 9 months after vitrectomy, visual acuity spontaneously improved to 20/40. Notice obvious growth of epiretinal membrane temporal to the fovea with change in the appearance of the macular hole.
Third row left, Figure 8. Case 3. A full-thickness macular hole, with visual acuity of 20/400, is seen in the right eye.
1376

Duker et al · Macular Holes after Vitreous Surgery
Case 2. A 62-year-old woman noted an abrupt diminution in vision in the left eye. Her ocular history was unremarkable. Results of examination showed visual acuity of 20/25 in the right eye and 20/200 in the left. Her right macula had a lamellar macular hole, whereas a stage 2 macular hole was noted in the left eye. She declined surgery and was observed for the next 6 months.
After this time period, the patient elected to undergo vitrectomy. Preoperatively, best-corrected visual acuity was 20/200, and the stage 2 hole had progressed to a small stage 3 hole (Fig 4). Pars plana vitrectomy was performed with peeling of the posterior hyaloid and injection of 25% SF6 gas. No ERM was peeled.
At 5 weeks after surgery, visual acuity improved to 20/25, · and the hole had disappeared (Fig 5). The hole spontaneously re-opened 5 months later, accompanied by the growth of a mild ERM (Fig 6). Visual acuity at this time was 20/200. The patient became increasingly symptomatic due to a nuclear sclerotic cataract with a further decline in visual acuity to counting fingers. She underwent an uncomplicated phacoemulsification with insertion of a posterior chamber intraocular lens. Two months after cataract surgery, best-correct visual acuity was 20/200.
Three months after cataract surgery, the patient returned with a spontaneous improvement in visual acuity to 20/40, which was associated with significant progression ofthe ERM. Although the hole was still visible (Fig 7), it was irregularly shaped, similar to a pseudo hole. No subretinal cuff of fluid was evident. Visual acuity has remained stable at 20/40 for 6 additional months.
Case 3. A 70-year-old man with a history of open-angle glaucoma noted blurry vision in the right eye for 2 weeks. Results of initial examination showed visual acuity of 20/400 in the right eye and 20/25 in the left. A full-thickness macular hole was noted in the right eye (Fig 8).
Three weeks later, an uncomplicated vitrectomy with peeling of the posterior hyaloid and injection ofSF6 gas was performed. Eight weeks later, visual acuity was 20/50, and the macular hole appeared closed (Fig 9). Five months after surgery, visual acuity was 20/70, which was associated with increasing nuclear sclerosis. The hole remained closed, and the potential acuity meter test showed a potential visual acuity of 20/50.
Fifteen months after the original surgery, the patient noted a gradual drop in vision in the right eye. Results of repeat examination showed visual acuity of 20/400 with improvement to 20/200 on the potential acuity meter test. A moderate nuclear sclerotic cataract was present, and the macular hole had reopened. No significant ERM was visible (Fig 10). The appearance and vision are stable with another 7 months of follow-up.
Discussion
Before the report by Kelly and Wendel, 1 idiopathic macular hole was considered an untreatable condition. It is now apparent that vitreous surgery can improve visual acuity for many patients with macular holes. As in any relatively new procedure, surgical indications, visual re-
suits, and complications still are being evaluated. Known complications of macular hole surgery include cataract formation, retinal tears and rhegmatogenous detachment, RPE alterations in the macula, and intraoperative enlargement of the macular hole. 1- 3 As shown by the clinical course of these patients, late re-opening of the macular hole with a subsequent drop in visual acuity can occur as a surgical complication as well.
It is possible that in more than 4.8% of the patients who are anatomic and visual successes with macular hole surgery late re-opening may eventually develop. Because of the retrospective nature of this study, the lack of consistent follow-up, and the possibility that late re-opening may continue to be observed for years after the vitreous surgery, the 4.8% incidence documented in the current group of patients may prove to be a low estimate. Further prospective studies with longer follow-up are necessary to document the true incidence of late re-opening after successful macular hole surgery.
The precise mechanism by which vitrectomy with gas injection improves visual acuity in idiopathic macular hole remains unknown. It currently is hypothesized that vitrectomy with peeling of the posterior hyaloid relieves the tangential traction induced by the intact cortical hyaloid, which is the cause of the elevation of the edges of a macular hole. I-s The presence of the gas bubble postoperatively helps re-oppose the edges of the macular hole to the RPE by preventing vitreous fluid passage into the subretinal space. This allows the natural adhesion between photoreceptors and RPE to be restored. It is also possible that the growth of a thin layer of glial cells across the macular hole plays a role in the success of some patients as well. In a patient with bilateral macular holes successfully treated with vitreous surgery, a glial ERM was documented in one eye studied in clinicopathologic correlation, although the second eye studied showed minimal glial tissue growth. 6
We hypothesize that, in at least some of the eyes undergoing late re-opening of originally successfully treated macular holes, the growth of an ERM plays a role in the re-opening. New tangential traction by the developing ERM would serve to re-elevate the edges of the holes, leading to new subretinal fluid accumulation. Three of eight eyes in this series showed new ERM postoperatively. It is possible that a clinically undetected ERM was present in the other eyes; however, without clinicopathologic correlation, this remains conjecture. In previous pathologic studies of macular holes, clinically undetected ERM was not an uncommon finding. 7 In a recent case of a successfully treated macular hole that underwent spontaneous late re-opening not in this series, ERM removed at the time ofre-operation was noted to contain Miiller cells on
Third row right, Figure 9. Case 3. After surgery, the macular hole is no longer visible. Visual acuity improved to 20/50.
Bottom, Figure 10. Case 3. Fifteen months after surgery, the macular hole re-opened, with a drop in visual acuity to 20/400. An artifact is present nasal to the macular hole.
1377

Ophthalmology Volume 101, Number 8, August 1994
histopathologic examination (Green WR, personal communication).
In case 2, a prominent ERM developed that coincided with the re-opening of the macular hole. The ERM continued to progress and, apparently, led to eventual reclosure of the hole. This sequence of events is similar to the case reported by Lewis and collaborators,7 in which the growth of an ERM was observed to seal a macular hole, improving visual acuity from 20/70 to 20/30. It is believed that the development ofa posterior vitreous detachment plays an etiologic role in the formation of ERM.9 It is, therefore, not surprising that ERM formation is observed in eyes undergoing vitrectomy for macular hole, because a critical aspect of the surgical procedure is the intraoperative creation of a posterior vitreous detachment.
Glaser and collaborators10·11 have presented intriguing evidence that the use of a biologic material to promote local fibrosis, transforming growth factor-beta 2, significantly increases both the anatomic and visual success of macular hole surgery. Transforming growth factor-beta 2 is a potent stimulator of wound healing. Its effectiveness in macular hole surgery is hypothesized to be due to its ability to induce a chorioretinal adhesion in the vicinity of the macular hole. 12 However, the long-term effects of this substance on the growth of ERM after vitrectomy still need to be elucidated. Ongoing prospective randomized trials of macular hole surgery both with and without transforming growth factor-beta 2 will help to answer questions concerning the role of postoperative ERM in both the initial success of macular hole surgery as well as in the occurrence oflate re-opening ofa successfully closed macular hole.
Indications for macular hole surgery remain controversial.13·14 Because of this, indications for re-operation after late re-opening after initial surgery are unsettled. Three of the eight eyes in this report did undergo re-operation, at the patients' request, which was successful in two eyes (67%). Obviously, the patients believed that the visual improvement they experienced after initial macular hole surgery was sufficient to warrant undergoing a reoperation. Although repeat pars plana vitrectomy with complete air-fluid exchange was performed as a re-operation, it is possible that simple outpatient gas injection alone, followed by face-down positioning, may reclose at least some re-opened macular holes. Theoretically, if significant tangential traction from ERMis present, gas injection alone may not be sufficient to re-close the macular hole.
It is interesting that Bonnet and Semiglia15 recently reported six cases of highly myopic eyes with retinal detachments associated with macular holes. All six eyes underwent initially successful retinal detachment repair; however, they subsequently had redetachment due to late re-opening of the macular holes. The authors found that the mean time for redetachment was 13.4 months, and one eye redetached as late as 78 months after the initial
surgery. Although the pathogenesis of retinal detachment due to macular hole in a patient with high myopia differs from the pathogenesis ofan idiopathic macular hole, similarities may exist in the etiology of late re-opening in both conditions.
In summary, late re-opening of initially successful macular holes after vitreous surgery can occur. Initial retrospective data indicate that 4.8% of initially successful patients may be at risk for this complication. Future prospective data may find that the percentage is higher. Repeat vitrectomy can result in improved visual acuity in some eyes, although the indications and surgical approach for re-operation remain to be settled.
References
I. Kelly NE, Wendel R T. Vitreous surgery for idiopathic macular holes. Results of a pilot study. Arch Ophthalmol 1991; 109:654-9 0
2. Wendel RT, Patel AC, Kelly NE, et al. Vitreous surgery for macular holes. Ophthalmology 1993;100:1671-6.
3. Poliner LS, Tornambe PE. Retinal pigment epitheliopathy after macular hole surgery. Ophthalmology 1992;99:16717.
4. Gass JDM. Idiopathic senile macular hole. Its early stages and pathogenesis. Arch Ophthalmol 1988;106:629-39.
5. Johnson RN, Gass JDM. Idiopathic macular holes. Observations, stages of formation, and implications for surgical intervention. Ophthalmology 1988;95:917-24.
6. Funata M, Wendel RT, de la Cruz Z, Green WR. Clinicopathologic study of bilateral macular holes treated with pars plana vitrectomy and gas tamponade. Retina 1992; 12: 289-98.
7. Lewis H, Cowan GM, Straatsma BR. Apparent disappearance of a macular hole associated with development of an epiretinal membrane. Am J Ophthalmol 1986; 102:172-5.
8. Guyer DR, Green WR, de Bustros S, Fine SL. Histopathologic features of idiopathic macular holes and cysts. Ophthalmology 1990;97: 1045-51.
9. Wiznia RA. Posterior vitreous detachment and idiopathic preretinal macular gliosis. Am J Ophthalmol 1986; I 02: 1968.
10. Lansing MB, Glaser BM, Liss H, et al. The effect of pars plana vitrectomy and transforming growth factor-beta 2 without epiretinal membrane peeling on full-thickness macular holes. Ophthalmology 1993; 100:868-72.
II. Glaser BN, Michels RG, Kuppermann BD, et al. Transforming growth factor-{J2 for the treatment of full-thickness macular holes. A prospective randomized study. Ophthalmology 1992;99:1162-73.
12. Smiddy WE, Glaser BM, Green WR, et al. Transforming growth factor beta. A biologic chorioretinal glue. Arch Ophthalmol 1989;107:577-80.
13. Fine SL. Vitreous surgery for macular hole in perspective. Is there an indication [editorial]? Arch Ophthalmol 1991; 109:635-6.
14. Weingeist TA. Surgical management of idiopathic macular holes [editorial]. Ophthalmology 1993; 100:1607-8.
15. Bonnet M, Semiglia R. Late recurrences after successful surgery for retinal detachment with macular hole. Graefes Arch Clin Exp Ophthalmol 1993;231:347-50.
1378